Embed Size (px)
Citation preview

Abstract of the thesis entitled
An evidence-based guideline of peer support intervention
in minimizing postnatal depressive symptoms in postnatal women
Submitted by
FONG KAM MUI
For the Degree of Master of Nursing
At the University of Hong Kong
In July 2015
Postnatal depression (PND) is the most common and complicated mental illness
that affects approximately 15% of postnatal women around the world. Many of the
studies documented the detrimental effects of PND, not only on the physical and
psychological aspects of the postnatal women, but also had active and prolonged
negatives effects on their children, family and society.
Although many of the researches were conducted regarding the treatments of
PND, reviews suggested that prevention was much more important than treatment. In
previous literatures, preventive interventions were focused on professional
psychological counseling and cognitive behavioral therapies. Recent researches
documented that psychosocial peer support interventions also significantly reduced
the risk of developing PND in postnatal women.
In this translational research, the current available evidences on the effect of peer
support intervention in minimizing postnatal depressive symptoms in postnatal
women are evaluated. Seven related literatures were retrieved from three electronic
bibliographical databases. Critical appraisals were done to assess the validity and
quality of the selected evidences. Then the implementation potential of the proposed
intervention was assessed by the transferability of the findings, the feasibility of the
implementation and the cost/benefit ratio. A clinical guideline was then developed
based on the evidences from the high standard of literatures identified, followed by
the proposals of the plan of implementation and the conduction of a pilot study plan in
one local MCHC. Finally, a detailed evaluation plan was discussed in this paper.
In conclusion, by evaluating the available evidences regarding the
implementation of new peer support intervention on postnatal women in MCHCs, it is
believed that the postnatal depressive symptoms of the postnatal women will be
minimized and postnatal women will be benefited from the intervention.

An evidence-based guideline of peer support intervention
in minimizing postnatal depressive symptoms in postnatal women
By
FONG KAM MUI
BNurs (Hon) (HKU), RN (HK)
A thesis submitted in partial fulfillment of the requirement
for the Degree of Master of Nursing
at the University of Hong Kong
July 2015
i
Declaration
I declare that this dissertation represents my own work, except where due
acknowledgement is made, and that it has not been previously included in a thesis,
dissertation or report submitted to this University or to any other institution for a
degree, diploma or other qualifications.
Signed:
FONG KAM MUI

ii
Acknowledgement
I would like to express my sincere gratitude to my dissertation supervisor Ms.
Veronica S. F. Lam, for her patient guidance, insightful comments and suggestions,
and expert advice in my dissertation throughout the past two years in my master study.
Without her expert recommendations and supports, I could not be able to finish my
work. Her kindness and patience are surely appreciated. It was my pleasure to be her
student in my master study in the University of Hong Kong.
I would also like to extend my deep gratitude to my Senior Nursing Officer, Ms.
Sally Wan, and Nursing Officers, Ms. Lee Kit Lai and Ms. Cheung Wai Yee, and my
colleages for their unfailing support throughout my two-year master study.
Lastly, warmest thanks to my husband, Mr. Paul Ip, and my mother, Ms. Lo Fung
Chun, for their ongoing love, support, understanding and encouragement in either my
homework or my household matters.
This dissertation definitely would not have been accomplished without the
above-mentioned people’s dedication and contribution.
iii
Table of contents
Page
Declaration …………………………...………………………………………… i
Acknowledgement …………………………………………………………….. ii
Table of contents ……………………………………………………………… iii
List of Abbreviations ………………………………………………………… vi
List of Appendices …………………………………………………………… vii
Chapter 1: Introduction Page
Background ………………………………………………………………….. 1
Prevalence of postnatal depression
Impacts of postnatal depression problem
Affirming the needs …………………………………………………………. 4
Postnatal mental support and services in own setting
Gap in current postnatal mood services
Significance of the peer support intervention ……………………………… 7
Limited peer support service in own setting
Dissertation objectives ……………………………………………………... 8
Research question …………………………………………………………… 8
PICO components …………………………………………………………… 9
Chapter 2: Critical Appraisal
Search strategies ……………………………………………………………. 10
Search date
Inclusion and exclusion criteria
Search results ……………………………………………………………….. 12
Data analysis: table of evidences
Quality assessment …………………………………………………………. 13
Appraising Tool: Scottish Intercollegiate Guidelines Network (SIGN)
Summary of quality assessment of studies
Summary of Results …………………………………………………………. 17
Publication year
Country of study
Sample size
Characteristics of the patient
Peer support intervention
Intensity of intervention

iv
Table of contents (continued)
Page
Peer training
Time for evaluation
Intervention effects
Data synthesis for the new innovation ………………....………………….... 25
Target participants
Peer support intervention
Assessment tool
Evaluation time
Chapter 3: The implementation potential
Transferability of findings …………………………….…………………… 31
Target setting
Target population
Similarity of target setting and target population
Philosophy of care
Patients to be benefited
Implementation plan and evaluation time
Feasibility …………………………………………………………………… 37
Freedom in carrying out the innovation
Organization atmosphere and administrative support
Interference with staff workload
Consensus among the staff
Cost-benefit ratio …………………………………………………………… 40
Potential risks
Potential benefits
Material and non-material costs
Chapter 4: Evidence-based practice (EBP) guideline
Title ……………………………………………………………………….. 44
Purpose of the guideline …………………………………………………… 44
Target group …………………………………………………………….. 44
Recommendations ………………………………………………………... 45
v
Table of contents (continued)
Page
Chapter 5: Implementation Plan
Identification of stakeholders ……………………………………………... 51
Communication plan with potential users ………………………………… 52
Preparatory phase
Implementation phase
Pilot test
Evaluation phase
Chapter 6: Evaluation Plan
Identification of outcome measures ………………………………………. 60
Patients’ outcomes
Healthcare providers’ outcomes
Time and frequency of measurements …………………………………… 62
Nature and Number of clients involved …………………………………… 63
Nature of clients
Number of clients involved
Data analysis ………………………………………………………………... 64
Criteria for effectiveness …………………………………………………… 65
Chapter 7: Conclusion …………………………………………………….. 67
Appendices …………………………………………………………………. 68
References …………………………………………………………………. 113
vi
List of Abbreviations
BDI Beck Depression Inventory
CCDS Comprehensive Child Development Scheme
CES-DS Center for Epidemiological Studies - Depression Scale
EBP Evidence Based Practice
EPDS Edinburg Postnatal Depression Scale
FHS Family Health Service
DH Department of Health
GHQ General Health Questionnaire
IFSC Intergraded Family Service Center
IPV Intimate Partner Violence
MCHC Maternal and Child Health Center
MO Medical Officer
MOSAIC MOther’S Advocates In the Community
NO Nursing Officer
PND PostNatal Depression
PNO Principal Nursing Officer
RCT Randomized Controlled Trial
SIGN Scottish Intercollegiate Guidelines Network
SNO Senior Nursing Officer
SOPC Specialty Out-Patient Clinic
SPSS Statistical Package for Social Science
WHO World Health Organization

vii
List of Appendices
Page
Appendix A Postnatal depression Report of Department of Health, 2013 68
Appendix B Table and Prisma flow diagram for Search Strategies and Results 71
Appendix C Evidence table for relevant studies 73
Appendix D Quality Assessment of selected studies 80
Appendix E Estimated Schedule and Gantt chart for the plan of preparation,
implementation and evaluation of the EBP guideline
102
Appendix F Estimated cost for the proposed program 104
Appendix G Level of Evidence and Grades of Recommendations (SIGN, 2012) 105
Appendix H EBP Protocol: Program flow chart 106
Appendix I Intervention Progress Sheet for nurses to monitor progress of
telephone contacts by peer supporters to postnatal mothers
107
Appendix J Consent form for participants and peer supporters 108
Appendix K Content of the Half-Day Training Workshop for peer supporters 109
Appendix L Surveys for staff 110
Appendix M Survey for participants 111
Appendix N Survey for peer supporters 112

1
Chapter 1: Introduction
Background
Postnatal Depression (PND) is a major depressive disorder which depressive
symptoms appear at the first 4-6 weeks after a woman’s delivery (American
Psychiatric Association, 2013). PND affects postnatal women’s physical and
psychological health (Sadat et al., 2014; Zhang & Jin, 2014), and also brings
detrimental influences to their children and family (Civic & Holt, 2000; Lee et al.,
2004; Patel, DeSouza, & Rodrigues, 2003; Rahman, Iqbal, Bunn, Lovel, & Harrington,
2004). Nowadays, postnatal depression has evoked as the most common and
complicated mental health illness among women at postpartum period.
Prevalence of Postnatal depression
PND has emerged as a globally concerned major public maternal mental health
issue (UNFPA, 2013; WHO, 2008). Its prevalence ranged from 4.5% to 28% in
numerous epidemiological population-based international studies, depending on
different socioeconomic states and cultures (Gavin et al., 2005; Leahy-Warren,
McCarthy, & Corcoran, 2011; Leung et al., 2011; Mallikarjun & Oyebode, 2005;
Lumley, Austin, & Mitchell, 2004; Mao, Li, Chiu, Chan, & Chen, 2012; Mao, Zhu, &
Su, 2011; Patel et al., 2012). In meta-analysis and systematic reviews, PND occurred

2
in an average of 13% of postpartum women by 3 months after delivery in
resource-rich countries, and with an even higher prevalence in resource-poor
countries (Fisher et al., 2012; Gavin et al., 2005; Grigoriadis et al., 2013; Leung &
Kaplan, 2009; Thombs et al., 2014).
In Hong Kong, postnatal depression prevalence ranges from 6.2% to 19.8% in
different epidemiological studies conducted in different years (Chen et al., 2013;
Leung et al., 2011; Leung, Martinson & Arthur, 2005; Mao et al., 2011). According to
the latest statistical data provided by the Family Health Service (FHS) of the
Department of Health (DH), 14.6% of postnatal mothers were identified with
suspected PND in 32 Maternal and Child Health Centers (MCHCs) in Hong Kong in
2013 (Appendix A).
Impacts of postnatal depression problem
The birth of a child is a time of joy for the mother and the family, however, the
occurrence of postnatal depression in postnatal mother brings detrimental effect to her
own physical and mental health (Rahman et al., 2013). Woman suffers from PND is
characterized with symptoms of persistent low mood, tearfulness, fatigue, anxiety,
affected sleep, decreasing appetite, feeling hopeless and guilty, and excessive anxiety
towards their baby (WHO, 2003). Among them, 5-14% of PND women have suicidal

3
ideation and behavior, making suicide be the most leading cause of death among
postpartum depressed women (Lindahl, Pearson, & Colpe, 2005). Nevertheless,
growing evidences have shown that PND reduces mother’s childcare ability and limits
her capacity to engage in positive parenting and child interactions (O'Hara & McCabe,
2013). Hence, the developments of their children are affected. A meta-analysis,
reviewing 193 studies, reported that children of PND women demonstrated higher
levels of misbehaviors and general psychiatric illnesses (Goodman et al., 2011) and
such effects could last for 11 years (Pawlby, Sharp, Hay, & O'Keane, 2008).
Maternal PND also increased the risk of paternal PND as shown by literatures
(Paulson & Bazemore, 2010; Gawlik et al., 2014; Goodman, 2004; Kerstis, Engstrom,
Edlund, & Aarts, 2013; Ramchandani et al., 2011). Potential negative outcomes such
as poor marital relationship and ineffective co-parenting may result (Hickey et al.,
2005; Lee, Taylor, & Bellamy, 2012; Milgrom, Schembri, Ericksen, Ross, & Gemmill,
2011). Therefore, marital relationship and family harmony may be destroyed.
Regarding the detrimental impacts of PND problem, postnatal depression has
also evoked as a global public health problem (Almond, 2009; Dennis & Dowswell,
2013). In the United States, the total health care services expenditures used on
depressed women were significantly higher than non-depressed women (US $1046.3
vs $365.2) (Dagher et al., 2012). Such an increase in health costs would bring

4
financial burden to the future health care system and has posed a major public health
burden in terms of lost productivity (Dagher, McGovern, Dowd, & Gjerdingen, 2012;
Dukhovny et al., 2013). Therefore, according to WHO (2008), maternal mental health
has been set as a fundamental in achieving the Millennium Developmental Goals in
the future (Glavin & Leahy-Warren, 2013) to promote the mental health of postnatal
women.
Affirming the needs
To tackle the problems of PND, routine screening for PND has started in Hong
Kong since 1998 to identify the postnatal women at risk (Lee et al., 1998). Monitoring
of women with PND has been implemented since 2005 in Family Health Service
(FHS) in MCHCs to reduce its severity and impact in future (Department of Health,
2014).
Postnatal mental support and services in own setting
In Hong Kong, family health service is provided by 32 MCHCs of Department of
Health (DH). A community-based Comprehensive Child Development Service
(CCDS) cooperated with the Hospital Authority has been implemented in five pilot
MCHCs since 2005 for early identification of mothers with postnatal depression

5
(PND) to closely monitor their maternal psychological well-being and future child
development (Department of Health, 2014). Since 2012, CCDS program has been
implemented in all 32 MCHCs.
In these MCHCs, all postnatal women are routinely screened for PND at 6 weeks
to 3 months of post-delivery using the Edinburgh Postnatal Depression Scale (EPDS)
questionnaire. If the score of EPDS is >9, a systemic mood assessment about mood
status and the presenting symptoms of PND of the woman will be carried out by
trained nurses. Women with significant depressive symptoms or self harm/baby harm
thoughts/acts will be referred to on-site psychiatric nurse’s assessment and counseling.
Other specialists e.g. pediatrician and social support services referrals will be made
when necessary.
According to the statistical data provided by FHS of DH (Appendix A), 14.6%
(n=6,734) of suspected PND mothers were identified in all MCHCs in 2013 either by
EPDS or clinical interview, in which 78.9% (n=5,311) were recommended to have
their mood to be continued monitoring by nurses during their subsequent MCHC visit
under the CCDS program. At the same time, 38.3% (n=2,579) of these suspected PND
mothers were referred to community social services for social worker counseling and
supports, such as Integrated Family Service Centers (IFSCs) (Appendix A).

6
Gap in current postnatal mood services
MCHC is a great platform for mothers to seek professional and social support.
Last year, 54,656 infants were registered in all MCHCs and 38,113 mothers
completed the PND screening with EPDS in MCHCs (Appendix A). At the moment,
this service targets women with high EPDS scores (EPDS >13) and women with
significant depressive mood symptoms or harmful thoughts. These women will be
referred to doctors or psychiatric nurses for mood counseling or to psychiatric
outpatient clinics in regional hospitals.
However, women with EPDS scores >9, and those with high EPDS scores
(EPDS >13) but with stable mood after the above said professional assessments, will
only have their mood to be monitored and reassessed during their next subsequent
visits in MCHCs. No active nursing intervention services in minimizing their negative
moods will be provided in the setting between their subsequent visits. In conclusion,
although the current CCDS program can identify suspected PND women earlier and
refer them to respective services promptly, no intervention is provided by nurses in
helping these suspected PND women in minimizing their depressive moods at the
moment.
Therefore, there is a gap in providing nursing intervention to this group of PND
patients at risk. It is proposed that the practice of potential nursing intervention be

7
introduced in minimizing the depressive symptoms and improving the mental health
of PND women on the platform of MCHCs.
Significance of the peer support intervention
Given the high prevalence of PND, its tremendous negative effects on the
suffering women, the likelihood of its long term impacts on growth and development
of children and its increasing health care costs to global economic burden, it is worth
to give prompt recognition to the matter. Early prevention and treatments should be
provided at an early stage in order to reduce severity and impact of PND in future.
Limited peer support service in own setting
Peer-based health intervention has been implemented to promote health for more
than forty years (Simoni, Franks, Lehavot, & Yard, 2011) and is commonly used to
improve health of different health outcomes with significant effects, e.g. breastfeeding
(Kaunonen, Hannula, & Tarkka, 2012), smoking cessation (Campbell et al., 2008),
diabetes management (Chan et al., 2014), and depression (DeAndrea & Anthony,
2013) etc.
Since impaired psychosocial functioning is one of the major risk factors leading
to PND (Dennis, 2014), many research findings has consistently highlighted the
8
importance of implementing psychosocial support to PND women (Chen, Kuo, Chou,
& Chen, 2007; Dennis, 2014). The effect of social support has also been found in
Chinese populations, in which women are reported to have fewer depressive
symptoms if being provided with better social supports by family, friends or
community (Lau & Wong, 2008; Zhang & Jin, 2014).
As a result, a new innovation – peer support intervention, which may bring forth
additional benefits (minimizing postnatal depressive symptoms and strengthening
suspected PND mothers’ social support network) is another potential intervention to
be carried out in the MCHC setting to minimize the depressive symptoms in
suspected PND women.
Dissertation objectives
1. To conduct a comprehensive literature search on effectiveness of peer support
intervention in minimizing depressive symptoms in postnatal mothers
2. To critically appraise, summarize and synthesize the relevant research papers
3. To develop an EBP guideline of using peer support intervention in minimizing
postnatal depression symptoms in postnatal women in MCHCs
4. To develop implementation and evaluation plans for a pilot test in a MCHC
Research Question
9
Is peer support intervention effective in minimizing postnatal depressive
symptoms in postnatal women?
PICO Components
Population: Postnatal women
Intervention: Peer support intervention
Comparison: Routine postnatal care service
Outcome: Postnatal depressive symptoms
10
Chapter 2: Critical Appraisal
To review the effectiveness of peer support intervention in minimizing
depressive symptoms in postnatal women, a systemic search and quality assessment
of relevant literatures is performed for the development of an evidence-based peer
support intervention guideline.
Search strategies
A comprehensive literature search was performed in three relevant electronic
databases: PubMed, PsycINFO, and CINAHL Plus.
During the searching process, date of publication was restricted from 1st January
1999 to present, and language was limited to English. Although studies that were done
over 10 years ago (before the year of 2004) were considered too old, not many studies
could be found within the past 10 years. Therefore, to have more relevant studies to
refer to, studies that were done 15 years ago (from January 1999) were included.
Two sets of key search terms were used. The first set was ‘peer support’, ‘social
support’, ‘mentor support’, ‘support group’. The second set was ‘postnatal depression’,
‘postpartum depression’, and ‘perinatal depression’. Complementary search was then
performed with different combination of the key terms of these two sets of keywords.
Potential relevant studies were selected and filtered by limiting to clinical trials,

11
matching titles, abstracts, fulfilling inclusion and exclusion criteria, then full texts
were reviewed. After identification of relevant literatures, manual search was
performed by reviewing the reference lists of selected studies to include extra relevant
studies. The search process and results are described in a search table and a Prisma
flow diagram in Appendix B.
Search date
The latest electronic search was done on 17th
August, 2014.
Inclusion and exclusion criteria
Inclusion criteria
Randomized Controlled Trials (RCTs) / clinical trials
Primary studies on investigating the effects of peer support intervention on
postnatal women
Primary studies that measure maternal depressive symptoms as the outcomes
Primary studies published between 1st January 1999 till 17
th August 2014
Exclusion criteria
Studies that support interventions are provided by health professionals
The target group postnatal women with currently diagnosed psychiatric diseases

12
Studies that the outcome measures are focused on infant and child
Studies that the publication languages are not English
Search Results
After performing electronic search with different combination of key search
terms, 1,934 studies in PubMed, 1,398 studies in PsycINFO and 333 studies in
CINAHL Plus were identified. When limited to clinical trials, 285 studies in PubMed,
57 studies in PsycINFO and 14 studies in CINAHL Plus were identified. With
reference to the inclusion and exclusion criteria and by manual screening of the titles,
abstracts and full texts, finally a total of 9 relevant studies are yielded, all written in
English, in which 7 studies from PubMed, 1 study from PsycINFO and 1 study from
CINAHL Plus were selected. Among the 9 studies yielded, 2 were excluded because
of duplication. Manual searching was then performed by screening the reference lists
of the 7 included studies, but no other relevant literature was yielded in the process.
As a result, 7 relevant eligible studies were included finally for review and
synthesis. All the 7 studies were randomized controlled trials (Chen, Tseng, Chou, &
Wang, 2000; Dennis, 2003; Dennis et al., 2009; Gjerdingen, McGovern, Pratt,
Johnson, & Crow, 2013; Letourneau et al., 2011; Taft et al., 2011; Wiggins et al.,
2005). Details of the systemic search are shown in the search table and the Prisma
13
flow diagram in Appendix B.
Data analysis: table of evidences
The seven studies were reviewed and analyzed. In order to allow systemic and
organized comparison and analysis of the findings, relevant data from the studies was
extracted and represented in a table of evidence. Citation of the study, study type,
characteristics of the patients, intervention(s), comparison, outcome measure(s) and
results were extracted. Evidence level of study was graded in accordance with the
seven-level hierarchies of evidence invented by Melnyk and Fineout-Overholt (2011).
A detail of evidence table for each study is shown in Appendix C.
Quality Assessment
Appraising Tool: Scottish Intercollegiate Guidelines Network (SIGN)
Randomized Controlled Trials (RCTs) Checklist for quality assessment,
developed by the Scottish Intercollegiate Guidelines Network (SIGN) (2008), was
used in appraising the selected literatures. The SIGN checklist provides medical and
nursing health professionals a systemic appraising process of individual literature, in
order to establish an evidence-based practice guideline to improve healthcare quality.
The appraisal criteria are: appropriateness and correct focus of research questions,
14
method of randomization, concealment allocation, blinding, similarity between
intervention and control group, difference in treatment under investigation, validity
and reliability of outcome measurements, dropout rate, intention-to-treat, and
comparable result from different sites.
Ratings for each criterion are responded as ‘well covered’, ‘adequately
addressed’, ‘poorly addressed’, ‘not addressed’, ‘not reported’ and ‘not applicable’.
Based on the SIGN grading system (SIGN, 2008), the level of evidence is graded
“1++”, “1+” and “1-” depending on the fulfillment of criteria. Details of individual
quality assessments of the seven studies using SIGN RCTs checklists are shown in
Appendix D.
Summary of Quality Assessment of studies
All the selected studies addressed an appropriate and clearly focused research
question in relation to the study interest.
Among all seven studies, two studies were cluster RCT. Although all the seven
studies described themselves as RCTs, only four of them clearly described the
methods of randomization in assignment of subjects to treatment groups, e.g.
randomly generated numbers (Dennis, 2003); web-based randomization service
(Dennis et al., 2009); computer generated software program (Wiggins et al., 2005)

15
and random number tables (Gjerdingen et al., 2013). Three studies mentioned and
used concealment methods by using opaque and sealed envelopes (Dennis, 2003;
Letourneau et al., 2011; Taft et al., 2011), while the remaining four studies did not
mention the concealment method (Chen et al., 2000; Dennis et al., 2009; Gjerdingen
et al., 2013; Wiggins et al., 2005).
Blinding is difficult to be carried out in this research design because the
provision of peer support intervention involves manipulation of intervention together
with participants, peers and health care professionals. As a result, none of the studies
was kept triple or double blinded. A single blinding of research assistants or data
entry staff was applied in three studies (Dennis, 2003; Dennis et al., 2009; Wiggins et
al., 2005); two studies did not mention blinding (Chen et al., 2000; Letourneau et al.,
2011) and the remaining two studies were not blinded (Gjerdingen et al., 2013; Taft et
al., 2011).
In five of the studies, the treatment and control groups were similar at the start of
the trial with the only difference between groups being the treatment under
investigation (Chen et al., 2000; Dennis, 2003; Dennis et al., 2009; Letourneau et al.,
2011; Wiggins et al., 2005). Baseline demographic and mental health characteristics
differences were found in the studies of Gjerdingen et al. (2013) and Taft et al. (2011),
in which the intervention groups displayed a higher percentage of mothers with a

16
history of PND in the past. Therefore, potential bias was presented.
All the seven studies used standard, valid and reliable assessment tools to
measure the outcomes. Five studies used Edinburg Postnatal Depression Scale (EPDS)
(Dennis, 2003; Dennis et al., 2009; Letourneau et al., 2011; Taft et al., 2011; Wiggins
et al., 2005), one study used Beck Depression Inventory (BDI) (Chen et al., 2000) and
one study used Center for Epidemiological Studies-Depression Scales (CES-D score)
(Gjerdingen et al., 2013).
Dropout rate ranged from 0% to 23.6% within the studies. Five studies had
maintained the dropout rate below 15% (Chen et al., 2000; Dennis, 2003; Dennis et al.,
2009; Gjerdingen et al., 2013; Letourneau et al., 2011). The dropout rate of the studies
by Wiggins et al. (2005) and Taft et al. (2011) were 20% and 23.6% respectively. It
might be caused by long intervention and long follow up that lasted 12 and 18 months
in Taft et al. (2011) and Wiggins et al. (2005)’s studies respectively. An intention to
treat analysis was used in all seven studies. Two studies were carried out multisite, but
results were not represented separately for comparison in all sites (Dennis et al., 2009;
Taft et al., 2011).
As a conclusion, all study results were applicable to target group identified by
the research question. Two studies were graded “1++” (Dennis, 2003; Dennis et al.,
2009) while the other five studies were graded “1+” (Chen et al., 2000; Gjerdingen et
17
al., 2013; Letourneau et al., 2011; Taft et al., 2011; Wiggins et al., 2005).
Summary of Results
Publication year
Bibliographic citations of the seven studies are cited from 2000 to 2013.
Country of study
Three studies were conducted in Canada (Dennis, 2003; Dennis et al., 2009;
Letourneau et al., 2011); one in the United States of America (Gjerdingen et al., 2013);
one in Australia (Taft et al., 2011); one in the United Kingdom (Wiggins et al., 2005)
and one in Taiwan China (Chen et al., 2000).
Sample size
Sample sizes ranged from 39 (Gjerdingen et al., 2013) to 731 (Wiggins et al.,
2005).
Characteristics of the patient
Postnatal women who delivered a live and healthy baby were recruited in all
studies. All studies recruited postnatal women who were at or above 16 years old and
18
were with a mean age of around 30 years old. A majority of the studies started their
recruitment of participants less than 2 months postpartum. E.g. within 24 hours
(Gjerdingen et al. 2013); 2 weeks (Dennis et al., 2009); 3 weeks (Chen et al., 2000); 8
weeks (Dennis et al., 2009) and 2 months (Wiggins et al., 2005). Over 75% of
mothers were married in five studies (Dennis, 2003; Dennis et al., 2009; Gjerdingen et
al., 2013; Letourneau et al., 2011; Wiggins et al., 2005), over 25% of mothers were
single mothers in one study (Taft et al., 2011), while one study did not measure
marital status of mothers in demographic characteristic (Chen et al., 2000).
For the pre-assessment recruitment screening and post-intervention assessment
comparison, five studies used EPDS (Dennis, 2003; Dennis et al., 2009; Letourneau et
al., 2011; Taft et al., 2011; Wiggins et al., 2005) as the single or one of the assessment
tools; one study used Beck Depression Inventory (BDI) (Chen et al., 2000) and one
study used CES-D depression score (Gjerdingen et al., 2013). The cut-off score were
set at EPDS >9 (Dennis, 2003; Dennis et al., 2009), EPDS >12 (Letourneau et al.,
2011) and BDI ≧9 (Chen et al., 2000) respectively during the pre-assessment
recruitment screening, while the cut-off score in other studies was not mentioned.
The age of the infants of the postnatal mothers ranged between 0 to 5 years old.
Such a large range in infant age was recorded because some mothers had more than
one child (Dennis, 2003; Gjerdingen et al., 2013; Letourneau et al., 2011; Taft et al.,

19
2011). Five studies recruited mothers with infants aged ≦6 months (Chen et al.,
2000; Dennis, 2003; Dennis et al., 2009; Gjerdingen et al., 2013; Wiggins et al., 2005)
and over 50% of them were primiparous in a great majority of the studies (Dennis et
al., 2009; Letourneau et al., 2011; Chen et al., 2000; Gjerdingen et al., 2013; Wiggins
et al., 2005).
Peer support intervention
All the support interventions in the treatment group were provided by peers:
laypeople or non-professionals (Chen et al., 2000; Dennis, 2003; Dennis et al., 2009;
Gjerdingen et al., 2013; Letourneau et al., 2011; Taft e al., 2011; Wiggins et al., 2005).
These supporters or mentors were recruited in the communities through referral from
health professionals in three studies (Chen et al., 2000; Gjerdingen et al., 2013; Taft et
al., 2011); newspaper advertising, and distribution of flyers or by word-of-mouth in
two studies (Dennis, 2003; Dennis et al., 2009); while the method of recruitment was
not mentioned in the remaining two studies (Letourneau et al., 2011; Wiggins et al.,
2005). The peer supporters recruited in four studies were clearly described as
volunteered mothers who had history of PND and had recovered from PND (Dennis,
2003; Dennis et al., 2009; Gjerdingen et al., 2013; Letourneau et al., 2011) while the
nature and characteristics of peer supporters were not described in two studies (Taft et

20
al., 2011; Wiggins et al., 2005).
The way to carry out support intervention varied in the seven studies but the
main strategy was by telephone support provided by peer supporters. Three studies
used solely telephone support (Dennis, 2003; Dennis et al., 2009; Gjerdingen et al.,
2013), two studies used a combination of telephone support with or without home
visiting as decided by the volunteer peer supporter (Letourneau et al., 2011; Wiggins
et al., 2005), one study used group discussion (Chen et al., 2000) and one study used
home visiting or direct meeting with participants in homes or other places (Taft et al.,
2011).
Intensity of intervention
The duration in providing peer support intervention ranged from 1 month (Chen
et al., 2000) to 18 months (Wiggins et al., 2005) and the total time spent on each PND
women ranged from 63.6 minutes (Gjerdingen et al., 2013) to 185.76 minutes (Dennis,
2003) of contacts.
The mean numbers of phone contacts launched were 5.4 (mean 34.4 minutes),
8.8 (mean 14.1 minutes) and 5.6 sessions (11.4 minutes) on each participated mother
in the studies by Dennis (2003), Dennis et al. (2009) and Gjerdingen et al. (2013)
respectively. In the study by Letourneau et al. (2011), each participant received an

21
average of 9 contacts (each lasted more than 20 minutes) of phone calls or visits; and
in the study by Wiggins et al. (2005), a total of 1.5 hours of telephone support or
home visiting were spent on each participant. No specific time spent nor average
number of contacts was reported in Taft et al. (2011)’s study. Instead, it was stated
that 58% of participant received weekly meeting with their peer supporters. In the
study by Chen et al. (2000), 4 weekly sessions (1.5-2 hours) of group discussion was
carried out with 5-6 mothers in a group.
Peer Training
In the studies conducted by Dennis (2003) and Dennis et al. (2009), peers or
mentors took a four-hour training session about the skills in providing telephone
supports and making hospital referrals. A 121-page training manual was given to the
peer supporters. In Letourneau et al. (2011)’s study, peer volunteers received an
eight-hour training about the skills in providing informational and counseling supports,
and practical maternal-infant interaction supports to mothers. In Taft et al. (2011)’s
study, peer supporters were trained with skills in knowledge not only related to
depression, but also Intimate Partner Violence (IPV), parenting, and self-care supports.
They were recruited under the program - Mother’s AdvocateS in the Community
(MOSAIC). Peer supporters in Taft et al. (2011)’s study were provided a five-day
22
training program and an online training manual. In addition, regular sharing sessions
at 1, 4, 8 and 12 month were carried out for peer supporters for inter-peer supports
and experience sharing. In Gjerdingen et al. (2013)’s study, peer telephone supporters
received a half-day training session on PND diagnosis and treatment, suicidal ideation
and techniques for supporting PND women. Periodical meetings were also organized
for supporters to share their experiences. In the study of Wiggins et al. (2005), peer
training was not mentioned.
Time for evaluation
Post-intervention assessments were done after the intervention period in all seven
studies. Three studies measured their intervention effects twice during the
intervention period (Dennis, 2003; Dennis et al., 2009; Wiggins et al., 2005). In the
study of Dennis (2003) and Dennis et al. (2009), EPDS scores were measured in the
middle (4 weeks and 12 weeks of the intervention period) of the study period and at
the end (8 weeks and 24 weeks of the intervention period) of the study period
respectively. In the study of Wiggins et al. (2005), intervention effect was measured at
12 months and 18 months of the intervention period. For the remaining four studies,
post-intervention measurements were taken after the intervention period according to
their length of study: at 4 weeks (Chen et al., 2000); at 12 weeks (Letourneau et al.,

23
2011); at 6 months (Gjerdingen et al., 2013) and at 12 months (Taft et al., 2011).
Intervention Effects
Statistical significance (p<0.05) results were recorded in four studies (Chen et al.,
2000; Dennis, 2003; Dennis et al., 2009; Letourneau et al., 2011) and clinical
significance results were obtained in the remaining three studies (Gjerdingen et al.,
2013; Taft et al., 2011; Wiggins et al., 2005).
In a pilot study conducted by Dennis (2003), lower mean EPDS scores were
obtained from the intervention group at both 4 weeks (p=0.008) and 8 weeks (p=0.006)
of intervention periods. Also, significantly (p=0.008) fewer percentage of mothers
were reported with EPDS score >9 (Intervention group: 35% to Control group: 76.2%)
after 8 weeks of intervention provided.
Another multisite study conducted by Dennis et al. (2009), significant difference
(p=0.02) in EPDS score between intervention and control group after 12 weeks of
intervention period was reported. In the study by Letourneau et al. (2011), EPDS
score significantly decreased by 6.4 in intervention group (p=0.04). In Chen et al.
(2000)’s study, BDI scores of PND women significant reduced by 6.41 after the
one-month intervention period (p<0.01).

24
In Taft et al. (2011)’ study, as the drop-out rate recorded was the highest (23.6%)
among the studies, the insufficient number of participants recruited and included in
the final analysis led to a statistically non-significant result (p=0.09) in the reduction
of EPDS score in the intervention arm. The reason for the high drop-out rate might be
due to long intervention period that lasted 12 months. However, the study did record a
reduction of 6.1 marks in the EPDS score in the intervention group (clinically
significant). Considered its clinical effect, the intervention was still regarded useful.
Instead of using the mean reduction in EPDS score on participants, percentage of
participants scoring EPDS ≧12 and the risk ratio (RR) of developing depression in
postnatal women were used for interpreting the effect of support intervention in the
study by Wiggins et al. (2005). 28% and 30% of participants were recorded EPDS ≧
12, and the RRs of depression were 0.86 and 0.93 in the support group and control
group respectively. A smaller reduction in percentage of participants with EPDS ≧12
in the intervention group recorded might be due to the fact that the uptake of
intervention support was low (only 35 participants out of 184 received supports
offered). As the study was carried out with an intention to treat basis, the result of
the intervention group was significantly diluted. However, the methodology used in
Wiggins et al. (2005)’s study was well designed, and it showed the feasibility in

25
recruiting voluntary peer supporters. Therefore, its results were still considered valid
and useful.
Lastly, in Gjerdingen et al. (2013)’s study, although statistically non-significant
result (p=0.397) was obtained in the reduction of CES-D score in the interventions
groups, the decrease in CES-D score was greater in the intervention group (reduction
of 14.5 marks) when compared to the control group (reduction of 10.1 marks). Such
result obtained was explained and confounded by small sample size (n=39) and the
presence of allocation bias of subjects to treatment groups (larger percentage of
depression history in intervention group).
As a conclusion, all the results of the seven identified studies were effective in
minimizing postnatal depressive symptoms in postnatal women.
Data synthesis for the new innovation
Integrating the collected data and results of the seven selected studies, peer
support intervention is considered feasible to be carried out on PND mothers and is
effective in minimizing postnatal depressive symptoms in PND women.
The recommendation of the new innovation to be carried out in a local setting in
MCHC in Hong Kong is shown below.

26
Target participants
1. Characteristics of mothers
Since a majority of the studies recruited participants is ≧18 years old (Chen et al.,
2000; Dennis, 2003; Dennis et al., 2009; Letourneau et al., 2011; Wiggins et al.,
2005), it is suggested to recruit postnatal mothers who are greater than 18 years
old. Moreover, as all infants in the seven studies were born live and healthily
(Chen et al., 2000; Dennis, 2003; Dennis et al., 2009; Gjerdingen et al., 2013;
Letourneau et al., 2011; Taft et al., 2011; Wiggins et al., 2005); therefore, only
mothers who gave birth to an healthy infant are included. Lastly, based on the
recruitment time of the majority of the studies started at less than three-month
postpartum (Chen et al., 2000; Dennis, 2003; Dennis et al., 2009; Gjerdingen et al.,
2013; Wiggins et al., 2005), mothers who delivered babies within three months are
therefore recruited.
2. EPDS score
A majority of studies used EPDS in the pre- and post- assessment screening and
evaluation (Dennis, 2003; Dennis et al., 2009; Letourneau et al., 2011; Taft et al.,
2011; Wiggins et al., 2005) and three of them set the cut-off score for inclusion as
9 marks. As a result, it is recommended mothers whose EPDS scores >9 should be
invited.
27
3. Exclusion criteria
Based on the exclusion criteria that set in recruitment of participants in a majority
of the studies (Dennis, 2003; Dennis et al., 2009; Letourneau et al., 2011; Taft et al.,
2011), women who have history of or currently diagnosed with major psychiatric
or mental disorders (e.g. schizophrenia, major bipolar disorder, psychosis, chronic
depression) and are currently taking antidepressants or antipsychotic medications;
and women who have history of receiving psychotherapy in the past 1 year are
excluded.
Peer support intervention
Since all the seven studies had either a statistically significant (Chen et al., 2000;
Dennis, 2003; Dennis et al., 2009; Letourneau et al., 2011) or clinically significant
effect (Gjerdingen et al., 2013; Taft et al., 2011; Wiggins et al., 2005) of the peer
support intervention, it implies that such intervention is workable, feasible and
effective in minimizing postnatal depressive symptoms in postnatal women. Since the
supporters who provided the peer support intervention in most of the studies were
trained (Chen et al., 2000; Dennis, 2003; Dennis et al., 2009; Gjerdingen et al., 2013;
Letourneau et al., 2011; Taft et al., 2011), therefore, it is considered training is
essential before the provision of the intervention.

28
Based on the contents and schedule of peer supporter training in a majority of the
studies (Chen et al., 2000; Dennis, 2003; Dennis et al., 2009; Gjerdingen et al., 2013;
Letourneau et al., 2011; Taft et al., 2009), the length of training should last at least 4
hours (Dennis, 2003; Dennis et al., 2009; Gjerdingen et al., 2013; Letourneau et al.,
2011) and the training contents should include information about PND, skills in
providing informational, instrumental, counseling and parenting supports. The
supports to be provided should encompass emotional supports, instrumental
assistances, informational supports and any support that are considered useful to help
participants to cope with their problems.
Moreover, peer supporters from three studies, with statistically significant results,
were those who had history of PND and had recovered from PND (Dennis, 2003;
Dennis et al., 2009; Letourneau et al., 2011), and therefore, they are preferred.
A majority of the studies used telephone contacts to provide peer support (Dennis,
2003; Dennis et al., 2009; Gjerdingen et al., 2013; Letourneau et al., 2011; Wiggins et
al., 2005). As a result, using telephone is preferred in carrying out the peer support
intervention. Since the duration of peer support intervention lasted less than 6 months
in most of the studies (Chen et al., 2000; Dennis, 2003; Dennis et al., 2009;
Gjerdingen et al., 2013; Letourneau et al., 2011), and long intervention period longer
than 12 months might record high dropout and minimize the effectiveness of the

29
intervention in the remaining two studies (Taft et al., 2011; Wiggins et al., 2005).
Therefore, it implies that a six-month intervention period is suitable and effective in
achieving positive results.
Regarding the length of each phone conversation provided by peer supporters to
mothers, an average of 6 contacts of each lasted at least 15 minutes were recordered in
most the studies (Dennis, 2003; Dennis et al., 2009; Letourneau et al.,
2011;Gjerdingen et al., 2013). It is suggested that the peer supporters should provide a
minimum of 6 telephone supports of each lasts more than 15 minutes to the
participants.
Assessment tool
Based on the results of the studies, a majority used EPDS as the assessment tool
in measuring the effectiveness of intervention (Dennis, 2003; Dennis et al., 2009;
Letourneau et al., 2011; Taft et al., 2011; Wiggins et al., 2005). Therefore, EPDS is
considered a valid tool in assessing the intervention effect. In addition, the Chinese
version of EPDS was validated by Lee and his team in 1998 and have been used in
MCHCs to screen suspected PND women during their routine visits at 2-3 months of
post delivery since 1998 (Lee et al., 1998). In conclusion, it is workable to use the
30
10-item Chinese EPDS questionnaire as it is a validated assessment tool in measuring
the effect of the peer support intervention.
Evaluation time
As suggested by a majority of the studies (Chen et al., 2000; Dennis, 2003;
Dennis et al., 2009; Gjerdingen et al., 2013; Wiggins et al., 2005), pre-assessment for
mothers at baseline depressive levels should be carried out at the time when they are
recruited, that is smaller than three-month postpartum. Post-assessment should be
done immediately after the intervention period for six months as suggested by most of
the studies (Chen et al., 2000; Dennis, 2003; Dennis et al., 2009; Gjerdingen et al.,
2013; Letourneau et al., 2011).

31
Chapter 3: The implementation potential
In the previous chapter, evidences from the seven reviewed studies concluded
that peer support intervention was effective in minimizing postnatal depression
symptoms in postnatal women. Therefore, it is worthwhile to translate the current
evidences into real practice and to apply it in the local setting in Hong Kong.
In this chapter, the implementation potential of this peer support intervention was
assessed by the transferability of findings, feasibility of the implementation and the
cost/benefit ratio of the intervention.
Transferability of findings
Target setting
The target setting is one of the 32 MCHCs under DH in Hong Kong. In the target
MCHC, child health and postnatal services are provided to newborn infants and
postnatal mothers accordingly as soon as they are discharged from their delivery
hospital. Routine maternal mood assessment, either by clinical interview or EPDS,
will be done at the first registration and at two-month postnatal period while the baby
will be reviewed respectively.
Target population
32
The target population is postnatal women who have registered in the targeted
MCHC and are identified as suspected PND sufferers after the EPDS screening.
Currently, postnatal woman who completes the EPDS questionnaires and with EPDS
scores >9 or is presented with any self-harm or baby-harm thoughts, will undergo a
systemic mood assessment done by trained nurses. Those with significant depressive
mood problems or psychotic symptoms or with thoughts of harmful behaviors will be
referred to doctors or psychiatric nurse for further assessments. On the other hand,
those postnatal women with EPDS >9 but with stable mood will have their mental
state reviewed again at their next MCHC visit accordingly during their babies’ next
vaccination schedule. And these group of postnatal women with EPDS score >9 and
with stable moods will be our target participants. Mothers who are under 18 years old,
have history of or currently diagnosed with major psychiatric or mental disorder, and
have history of receiving psychotherapy in the past 1 year will be excluded as
suggested by the reviewed studies (Dennis, 2003; Dennis et al., 2009; Letourneau et
al., 2011; Taft et al., 2011).
Similarity of target setting and target population
In all the seven reviewed studies, the recruitment and peer support intervention
were being carried out in a place or clinic which provided services both to infants and

33
mothers (Chen et al., 2000; Dennis, 2003; Dennis et al., 2009; Gjerdingen et al., 2013;
Letourneau et al., 2011;Taft et al., 2011; Wiggins et al., 2005). This is very similar to
our target MCHC which also provides both services to infants and postnatal women.
In addition, the schedule of mood assessment of postnatal mothers in our target
MCHC (at first registration and at 2-3 months after delivery) is also similar with that
from the majority of the reviewed studies (Chen et al., 2000; Dennis, 2003; Dennis et
al., 2009; Gjerdingen et al., 2013; Wiggins et al., 2005). Therefore, it is considered the
target MCHC is a suitable setting for the innovation to fit in.
A vast majority of postnatal mothers that have registered in the target MCHC are
aged between 18-40 years old, which is very similar to those participants recruited in
the reviewed studies, which the mean age range was between 20-35 years (Chen et al.,
2000; Dennis, 2003; Dennis et al., 2009; Gjerdingen et al., 2013; Letourneau et al.,
2011; Taft et al., 2011; Wiggins et al., 2005). Many of the registered postnatal mothers
in the target MCHC have given birth to healthy babies without major complications
within 3 months of post delivery. It is also similar to the patient characteristics
recorded in the reviewed studies (Chen et al., 2000; Dennis, 2003; Dennis et al., 2009;
Gjerdingen et al., 2013; Letourneau et al., 2011; Taft et al., 2011; Wiggins et al.,
2005).

34
Chinese is the main ethnicity in the target population, which is apparently
different from most of the reviewed studies, in which the target participants were
Australian, Canadian and American (Dennis, 2003; Dennis et al., 2009; Gjerdingen et
al., 2013; Letourneau et al., 2011;Taft et al., 2011; Wiggins et al., 2005). Yet, Chen et
al. (2000) demonstrated the innovation was also effective in Chinese populations.
Despite the difference in ethnicity of the target participants, similar PND prevalence
rates are recorded in both Chinese and Westerners. Therefore, the target population is
still considered transferable from the reviewed studies.
Philosophy of care
The core mission of the FHS of DH is to promote a holistic (physical,
psychological, cognitive, social) health and well-being of children and women
through developing evidence-based programs and strategies to empower people the
knowledge and ability to improve health in the community (Family Health Service,
2014). The proposed innovation is an evidence-based intervention that helps to
promote the psychological and social health of postnatal mothers by minimizing their
PND symptoms during the postnatal period by peer supporters in the community,
which comprehensively achieved the mission and value of our target setting in DH.
35
Patients to be benefited
In 2013, a total of 6,734 suspected PND women were identified in all MCHCs in
Hong Kong, in which 5,311 (78.9%) mothers with EPDS >9 were given brief
follow-up of mood status by nurses in the next MCHC visit (Department of Health,
2013). In the target MCHC, 3,362 mothers have completed PND screening, either by
EPDS or clinical interview in 2013, in which 550 (16.4%) were identified as mothers
at risk with suspected PND (Department of Health, 2013). From the statistic report of
the target MCHC in 2013, 437 mothers (about 36 mothers being identified in each
month) with EPDS >9 were identified as clinically mood stable after assessments
done by nurses (Department of Health, 2013). Their mood condition would be
reassessed again by brief follow-up during their next MCHC visit. According to
literatures, the PND prevalence rate was estimated to increase in the future. Therefore,
it is estimated that more than 400 suspected PND mothers will be benefited from our
target setting annually when the innovation is put into real implementation. When it is
applied in all MCHCs, it is estimated that more than 5,000 suspected PND postnatal
mothers in Hong Kong will be benefited in the future every year.
Implementation plan and evaluation time

36
The implementation period of the whole program will take about 31 months and
will be divided into 3 phases: preparatory phase, implementation phase and evaluation
phase.
It starts with preparatory phase which takes about 2 months. Proposal and budget
plan will be sent to the Director of Health of the FHS at the monthly meeting for
approval. An organizing committee will be formed, and briefing and training of clinic
staff will be carried out accordingly.
Then implementation phase will start with a pilot study and will take about 9
months. Recruitment of suspected PND participants and volunteered peer supporters
will be carried out, peer supporters will be trained and allocation of recruited
participants and peer supporters will be done by nurses accordingly in the first month.
Once the peer supporters are being informed of their corresponding participants, the
support intervention, mainly conducted by phone, will be carried out for 6 months.
Evaluation of the pilot test will be carried out immediately after the pilot test.
Participants’ depression levels and perception of the innovation program from
participants, peer supporters and staff will be evaluated by distribution of satisfaction
surveys.
After the pilot test, a full-scale of the program will start and will take another 18
months. Recruitment and training will be continuously carried out from the 12th

37
month to the 23rd
month, while peer support intervention will be provided to
participants by peer supporters through phone intervention from the 13th
month to the
29th
month accordingly.
Lastly, the evaluation of the whole implementation program will be carried out
from the 19th
to the 31st month, which the whole period takes 13 months.
Post-intervention EPDS questionnaires and surveys will be distributed to participants,
peer supporters and staff.
An estimated schedule for the preparation, implementation and evaluation plan
of the pilot test and full-scale program is shown in a Gantt chart in Appendix E.
Feasibility
The feasibility of carrying out the innovation is assessed by freedom in carrying
out the innovation, organization atmosphere, administrative support, interference with
staff workload, consensus among staff and evaluation tools.
Freedom in carrying out the innovation
As mentioned before, promoting holistic health to women, including postnatal
mothers, through providing evidence-based program is the major mission of the FHS
of DH. Clinical meetings are carried out regularly at least once a month in the target
38
MCHC to discuss the most up-to-date nursing and medical practices. In the past 2
years, experiences in applying new evidence-based practice have been also taken
place, for example, the practice of skin-to-skin care has been introduced to improve
breastfeeding outcomes. It is shown that, with enough evidences supported, nursing or
medical staff have the freedom to propose, to modify current practices and to carry
out any updated guidelines which benefits patients.
Moreover, Director of Health, Principal Nursing Officer and Senior Nursing
Officers in the service are supportive to new evidence-based practices which can
benefit clients and they also give autonomy to nurses in the target MCHC to
implement, as well as to determinate a new intervention if any new and updated
evidence-based practices were published in the journals. As a result, it is estimated
that the implementation of the proposed program will be feasible in the target MCHC.
Organization atmosphere and administrative supports
The organization atmosphere also supports evidence-based practices in the
department. A majority of the currently available nursing protocols and practices are
evidence-based. Doctors and nursing staffs are always given opportunity to propose
and discuss the most up-to-date practices in clinical meetings. Since the proposed
program of peer support intervention is an evidence-based strategy that has been

39
supported by qualified studies in effectively minimizing postnatal depression
symptoms in postnatal women, it is no doubt that the higher administration and
management level, as well as the front line staffs, will positively support the proposed
program.
Interference with staff workload
At the moment, all nurses in the target MCHC are trained in assessing and
managing postnatal depression women. Therefore, it is estimated that the proposed
program will not put much burden to nurses’ daily workload as all nurses have
experience in handling and managing suspected PND mothers. Moreover, as the chief
manipulators of the proposed innovation are peer supporters recruited in the
community, nurses only carry out the role of monitoring and supporting, which do not
disturb their routine practices much. Therefore, nurses are positive about accepting the
new program.
However, extra time may be needed during nurse interview for recruiting
suitable participants and peer supporters in the community and in getting consents
from participants and peer supporters. Also, extra workload may be added to the
designated nurses in running the program, for example, in pairing up supporters and
participants.
40
Consensus among the Staff
Whenever a new innovation is to be proposed and implemented, there must be
somebody that has diverse opinions and viewpoints towards the change. Therefore, to
get consensus among all staff is important. Before the launch of the program, an
enquiry period that will last for one month will be given to staff to give comments and
to suggest modifications about the innovation. The proposal will also be distributed to
staff to read and familiarize with during the period. The organizing committee will be
responsible for collecting the comments and suggestions and will explain the details
and benefits of the program to postnatal mothers in the clinic. Moreover, a pilot test
will be worked out in order to test the feasibility of the program.
Cost-benefit ratio of the innovation
In order to assess the worthiness of the program, the cost and benefit of the
whole program will be assessed.
Potential risks
The current practice of handling PND is focused on the group of mothers whose
EDPS score >13 and with significant depressive mood symptoms, they will be

41
referred to doctors or psychiatric nurses assessment for further managing their mood.
However, there is no active intervention currently available for the group of mothers
whose EDPS score >9 and with comparatively stable moods after nurses’ assessments.
In addition, this group of postnatal mothers may develop PND if they are not being
supported and not given prompt intervention in minimizing their depressive
symptoms. Therefore, if the proposed peer support intervention is not implemented,
the psychological, mental and social health of this group of high-risk mothers may
deteriorate due to the lack of social supports and peer counseling.
Potential benefits
As mentioned in the previous chapter, peer support intervention is effective in
minimizing postnatal depression symptoms in postnatal women (Chen et al., 2000;
Dennis, 2003; Dennis et al., 2009; Gjerdingen et al., 2013; Letourneau et al.,
2011;Taft et al., 2011; Wiggins et al., 2005). Their EPDS scores significantly
decreased after receiving the intervention (Dennis, 2003; Dennis et al., 2009;
Letourneau et al., 2011). Therefore, high-risk postnatal women in developing PND
(EPDS scores >9) will be benenfited if the intervention is put into real practices. At
the same time, the psychological well-being and social networking of these suspected

42
PND postnatal women will be improved and broadened respectively under this
program.
Material and non-material cost
The cost of setting up and maintaining the intervention program is categorized
into material and non-material cost.
In the pilot test, it is estimated that 36 suspected PND mothers, 18 peer
supporters and around 22 nurses in the target MCHC will be involved. As for the full
scale of the program, it is estimated that around 460 participants and 230 peer
supporters will be involved. The required materials and calculation for the costs are
shown below.
Materials needed are: (a) a function room equipped with computer and overhead
projector: for providing staff briefing and a half-day training workshop for the
recruited peer supporters; (b) four EBP protocols: for nurses to read and take as
reference during the pilot test; (c) 18 ten-page training booklets with contents
regarding the provision of peer supporting intervention: to be distributed to each peer
supporters during the half-day training workshop; (d) 76 one-page questionnaires: for
collecting comments and feedbacks from peer supporters, participants and staff.

43
Material cost is the money spent on facilities and equipments needed,
photocopying the guidelines, booklets and questionnaires, while the non-material cost
is the labor cost. As the function room, overhead projector and computer are already
available in the target MCHC, the money is mainly spent on photocopying. It is
estimated that $54.4 will be spent on photocopying the protocols, booklets and
questionnaires (unit price for 1 page: $0.2).
The non-material cost is manpower cost. In the target MCHC, there are 22
registered nurses. Each nurse will be provided with a one-hour briefing on the
proposed program during the preparation stage, in which, the cost is $3,984. At the
same time, two identical four-hour peer supporter training workshops (each with
about 10 peer supporters) will be organized by two nurses on two separate dates (one
nurse is responsible for one workshop) to ensure all peer supporters are trained before
they provide support intervention, in which, the training costs $1,416. It is estimated
that $5,310 is needed as the manpower cost.
The details of the estimated expenditure in running the pilot program (both
material and non-material costs) are shown in Appendix F. It is estimated that a total
of $5,364.4 is required for the pilot test and a total of $17,590 to run the proposed
full-scale program.

44
Chapter 4: Evidence-based practice (EBP) guideline
After assessing the implementation potential, it is considered the proposed
intervention is transferable, feasible and beneficial when being applied in local setting.
In this chapter, a clear and user-friendly EBP guideline will be developed to guide the
use of this proposed intervention.
Title
Evidence-based practice guideline of peer support intervention in minimizing
depressive symptoms of postnatal women in MCHCs.
Purpose of the guideline
To guide MCHC nurses in providing and monitoring peer support intervention
based on the best available evidences;
To standardize the information on training peer supporters to provide peer
supports;
To guide peer supporters in delivering peer support intervention to postnatal
women
Target group
45
Postnatal women who are (a) with EPDS scores >9 after mood assessment and
professional judgment of nurses; (b) within 3 months of post delivery; and (c) aged
≧18. Exclusion criteria: women who (a) have history of or are currently diagnosed
with major psychiatric or mental disorders; (b) are taking antidepressants or
antipsychotic medications; or (c) have history of receiving psychotherapy in the past 1
year.
Recommendations
The grades of recommendations and levels of evidence are assessed by the
application of the Scottish Intercollegiate Guidelines Network (2012). The criteria of
recommendations are attached in Appendix H.
Recommendation 1 – Characteristics of participants
1.1 Participants being recruited should age at least 18 years.
(Grade of recommendation: A)
Evidences:
The participants recruited are at least 18 years old in a majority of the studies
and peer support intervention has shown to be effective in minimizing
postnatal depressive symptoms in these subjects (Chen et al., 2000; Dennis,
2003; Dennis et al., 2009; Letourneau et al., 2011; Wiggins et al., 2005).
46
1.2 Participants should have delivery within 3 months.
(Grade of recommendation: A)
Evidences:
Mothers who delivered healthy live babies within three months after delivery
are recruited in a majority of the studies (Chen et al., 2000; Dennis, 2003;
Dennis et al., 2009; Gjerdingen et al., 2013; Wiggins et al., 2005).
Most women develop PND in the first 12 weeks after delivery (Dennis, 2003;
Dennis et al., 2009).
1.3 Participants should have no previous and current psychiatric medical history.
(Grade of recommendation: A)
Evidences:
Women who have history of or currently diagnosed with major psychiatric or
mental disorders and are taking antidepressants or antipsychotic medications
are excluded in most studies (Dennis, 2003; Dennis et al., 2009; Letourneau
et al., 2011; Taft et al., 2011).
Recommendation 2 – Pre-assessment screening
2.1 Pre-assessment screening should be done with EPDS assessment tool.
(Grade of recommendation: A)

47
Evidences:
Most of the studies had pre-assessment screening before 3 months of
post-delivery: 2-3 days (Chen et al., 2000); 8 weeks (Denns 2003); 2 weeks
(Dennis et al., 2009); 2 months (Wiggins et al., 2005); 24 hours (Gjerdingen
et al., 2013).
EPDS is a well-established depression scale and is the most frequently used
instrument in assessing PND symptoms (Letourneau et al., 2011).
2.2 Participants should have EPDS score >9 and stable mood after professional
judgment by nurses.
(Grade of recommendation: A)
Evidences:
Five studies used EPDS cut off score >9 in pre-assessment screening (Dennis,
2003; Dennis et al., 2009; Letourneau et al., 2011; Taft et al., 2011; Wiggins
et al., 2005).
Recommendation 3 – Assignment of peer supporters to participants
3. Assignment of peer supporters to participants should base on geographic
residency and availability.
(Grade of recommendation: A)
Evidences:
48
Dennis (2003), Dennis et al. (2009) and Letourneau et al. (2011) matched the
peer supporters or volunteers to the recruited postnatal mothers according to
their region of resident and time of availability.
Recommendation 4 – Advice and monitor the peer supporters
4.1 The peer supporters should contact the participants by phone once a month.
(Grade of recommendation: A)
Evidences:
Telephone supports provide more privacy and flexibility, but less
stigmatization than clinical visits (Letourneau et al., 2011).
Using telephone in providing various kinds of supports, for example
emotional, informational supports, counseling and referral, was used in most
of the studies (Dennis, 2003; Dennis et al., 2009; Gjerdingen et al., 2013;
Letourneau et al., 2011; Wiggins et al., 2005).
Phone contacts were launched by peer supporters at almost once a month in
most of the studies (Dennis, 2003; Dennis et al., 2009; Gjerdingen et al.,
2013; Letourneau et al., 2011).
4.2 The length of telephone conversation should last more than 15 minutes.
(Grade of recommendation: A)

49
Evidences:
Challenges were reported by peer supporters in establishing rapport with
some mothers over the phone if conversation time was limited (Gjerdingen et
al., 2013).
The average length of each phone conversation launched by peer supporters
was longer than 15 minutes in studies with significant results (Dennis, 2003;
Dennis et al., 2009; Letourneau et al., 2011).
4.3 The duration of the phone intervention should last for six months.
(Grade of recommendation: A)
Evidences:
Significant intervention effect was seen in studies with intervention period
less than six months (Chen et al., 2000; Dennis, 2003; Dennis et al., 2009;
Letourneau et al., 2011).
Recommendation 5 - Post-assessment screening
5. Post-assessment should be done using EPDS assessment tool after the
intervention.
(Grade of recommendation: A)
Evidences:

50
Post-intervention assessments were being done after the intervention in all
studies (Chen et al., 2000; Dennis, 2003; Dennis et al., 2009; Letourneau et
al., 2011; Gjerdingen et al., 2013).
51
Chapter 5: Implementation Plan
After developing the evidence-based practice guideline for minimizing postnatal
depressive symptoms in suspected PND women, the next crucial step is to build up a
systemic communication plan before the real implementation in the selected local
setting taken place. In this chapter, the plan of communication process with potential
stakeholders and the conduction of a pilot study test will be discussed.
Identification of stakeholders
Establishing an effective communication with the stakeholders can build up a
cooperative relationship and gain their support throughout the whole implementation
of a new innovation (Ingersoll, 2005). Therefore, the first step is to identify all the
stakeholders, who are important persons to decide if an innovation can be successfully
carried out (Melnyk & Fineout-Overholt, 2011), then to develop a communication
plan with all of them. Three levels of stakeholders are involved: administrative and
management level, clinical level and client level.
Administrative and management level includes Director of Health, Principal
Nursing Officer (PNO) and Senior Nursing Officers (SNOs) in the FHS under DH.
They are in the administrative hierarchy who are responsible for making adoption of
proposals and implementing decisions, as well as allocating resources and manpower.

52
SNOs in the service also function as a bridge for communication and liaison with
higher level of administrators. Hence, approval should be obtained from this level.
The clinical level includes all staff working in the clinic. Frontline staff involves
of the Medical Officers (MOs), Nursing Officers (NOs) and Registered Nurses (RNs).
Nursing Officers (NOs) are important personnel to approve and to lead the whole
team in the implementation of the proposed program in the clinic. Hence, an effective
communication and detailed explanation of the guideline with RNs can necessarily
facilitate and sustain the program. Although MOs are not actually involved in carrying
out the program, their understanding and support is essential in monitoring and
sustaining the process.
The client level includes postnatal women (with EPDS scores >9 and mood
stable after professional judgments by nurses) and volunteered peer supporters.
Postnatal women with EPDS scores >9 with stable moods after nurse’s professional
judgment are the recipients, while volunteered peer supporters are responsible for
delivering phone counseling and supports to postnatal women.
Communication plan with potential users
A systemic communication plan facilitates better collaboration between
proposers and stakeholders to execute and implement a new program smoother and

53
easier. To make the communication effective, the whole communication process is
divided into three phases: preparatory, implementation and evaluation phases.
Preparatory phase (2 months)
The aim of the preparatory phase is to obtain the approval from higher
administrative, to develop a working committee, to explain and collect concerns and
feedbacks of staffs about the new peer support intervention.
In this phase, the proposal and budget plan will be sent to higher administrative
hierarchy for adoption and approval in one of the monthly departmental meetings
which is held by Director of Health, PNO, SNOs and regional NO and MO in-charges.
They are welcomed to give feedbacks and comments about the details of the program,
therefore, one can understand more about the interests of these senior administrators.
At the same time, an organizing committee comprises clinic NO in-charge, one
NO and two RNs will be formed to organize the planning and evaluation of the
process. Clinic NO in-charge takes the role of a leader in promoting the new program
and helps in liaison and communication with higher administrative and management
level. NO acts as a supervisor and a director in execution of the program, while the
two RNs take the role of instructor and trainer in providing training to other nurses
and peer supporters.
54
Once the proposal and budget are approved from administrators, the proposal
and guideline will be presented with PowerPoint presentation in one of the monthly
clinic staff meetings. The organizing committee will seek support from nursing staffs
by presenting the needs and significance of the current PND problem and the gap in
providing nursing intervention in minimizing PND symptoms among women at risk
in the current setting. Then the proposed program flow chart (Appendix H), budget
plan will be explained and benefits of the new program will be emphasized to further
convince all staffs. An enquiry period lasts for one month, which allows nurses
enough time to express concerns and comments on the proposed program. Refinement
of the proposed program may be required after addressing all concerns and
suggestions raised by staffs. It is estimated to take two months for this phase.
Implementation Phase (27 months)
In this phase, an implementation of a pilot study plan will be carried out in one
of the local MCHCs to assess the program logistics, participants, peer supporters and
nurses’ acceptances and satisfactions about the proposed guideline, and to monitor
patients’ and healthcare providers’ outcomes. After that, a full-scale implementation
will be carried out.
55
Pilot Testing (9 months)
A pilot test allows feasibility checking of the guideline, feedback collection and
identification of unanticipated barriers before the full-scale implementation of a new
innovation (Melnyk & Fineout-Overholt, 2011). It provides opportunities to refine
and finalize the EBP guideline before the real implementation and future
dissemination of the proposed guideline in other clinical units. Details of the pilot test
are discussed below.
Pilot Study Plan
Aim: to test the feasibility, evaluation, refinements and finalization of the new
proposed peer support intervention.
Objectives: . to review program logistics
. to evaluate staff acceptability, satisfaction and workload
. to evaluate postnatal women’s acceptability & satisfaction
. to evaluate peer supporters compliance, acceptability & satisfaction
. to fix potential pitfalls
Participants:
The target participants in the pilot test will be postnatal women who are (i) with
EPDS scores >9 with mood stable after professional judgments by nurses; (ii) within
3 months of post delivery; and (iii) aged ≧18. They should not have history of or are
currently diagnosed with major psychiatric or mental disorders, not taking

56
antidepressants or antipsychotic medications, or have history of receiving
psychotherapy in the past year.
Procedure:
The pilot test will be carried out in three stages: recruitment and training (1
month), and implementation of the peer support intervention (6 months), and
evaluation (2 months).
In the recruitment and training stage, all nurses will help to recruit participants
and peer supporters. Posters will be posted in the target MCHC in recruiting potential
peer supporters. Women who fulfill the recruitment criteria will have mood
assessment done for eligibility screening by nurses based on their professional
judgments. High-risk suspected PND women (e.g. with significant mood and mental
disturbances or harm thoughts) will be referred to specialists or doctors for immediate
treatments. Eligible women (EPDS >9 and mood stable after professional judgment
by nurses) will be given consent forms to enroll into the program (Appendix J). At the
same time, recruitment of peer supporters will be done by putting up posters in the
clinic and by nurses. According to statistical data from the target MCHC, there were
550 postnatal mothers recorded with EPDS >9 last year, approximately with about 45
suspected PND mothers identified in each month. With about 80% of agreement in
57
participation into the pilot study, it is expected to recruit 36 postnatal women and 18
peer supporters within the period.
Two identical four-hour training workshops will be organized for peer supporters
by two nurses to ensure all peer supporters will be trained before they provide
supports. Detailed training content for the peer supporters is illustrated in Appendix K.
It is estimated to take 1 month for the whole recruitment and training process.
After the recruitment, the 6-month implementation phase will start immediately.
The organizing committee will allocate the recruited 36 participants to the 18 peer
supporters (classified as one group, for nurses to monitor the progress) according to
their basic socio-demographics and geographic residency, in which, two participants
will be allocated to one peer supporter. Hence, there will be 18 pairs in one group and
their condition will be monitored by nurses at 1 week, 3 months and 6 months after
the start of the program using the intervention progress sheet (Appendix I). Nurses
will phone the peer supporters and will record their availability of contact of the
allocated postnatal woman, the number of contacts being made during the period and
the details of supporting services being given. Lastly, nurses will check with peer
supporters if any problems are encountered so that they can offer help if necessary.
Details of the intervention progress sheet are shown in Appendix I.
58
Evaluation of the pilot study will start immediately after the 6-month
intervention and will last 2 months. Women’s depression levels and perceptions of the
program will be evaluated by distributing EPDS questionnaires and satisfaction
surveys. At the same time, surveys will also be distributed to peer supporters and
nursing staff to evaluate their acceptability and satisfaction about the program. A
focus group meeting will be organized by the organizing committee to further discuss
and collect feedback from the nurses in the target setting. Data and comments will be
analyzed by the organizing committee for further refinement of the final guideline to
prepare for full-implementation in future.
Formats of the surveys for participants, peer supporters and staff are shown in
Appendix L, M and N.
Full-scale program implementation (18 months)
After the implementation of the pilot test, a full-scale program of peer support
intervention will start and last for 18 months. Recruitment and training will be
continuously carried out from the 12th
month to the 23rd
month, while the peer support
intervention will be provided to participants by peer supporters through phone
intervention from the 13th
month to the 29th
month accordingly.
Evaluation phase (13 months)

59
Lastly, evaluation of the whole implementation program will be carried out from
the 19th
to the 31st month, which the whole period takes 13 months. Post-intervention
EPDS questionnaires and surveys will be distributed to participants, peer supporters
and staff respectively after the intervention period.
An estimated schedule for the preparation, implementation and evaluation plan
of the pilot test and the full-scale program is shown in a Gantt chart in Appendix E.

60
Chapter 6: Evaluation Plan
Evaluation is the final part of a program to determine if the objectives are
achieved. Information in the evaluation is also crucial in refining and finalizing the
EBP guideline. In the evaluation plan, the identification of outcome measures, time
and frequency of measurements, nature and numbers of clients involved, and method
of data analysis will be discussed.
Identification of outcome measures
In this EBP guideline of minimizing postnatal depressive symptoms in postnatal
women at risk by peer supporters, patients’ outcomes and health care providers’
outcomes are measured.
Patients’ outcomes
Primary outcomes
As mentioned earlier in the chapter of affirming the need of the intervention,
there is a time lag in providing nursing intervention to minimize postnatal depressive
symptoms in suspected PND women in the local setting. The proposed program fills
this gap by providing peer support intervention for suspected PND women to manage
their depressive moods. Therefore, the primary outcome of this program is to prevent

61
and decrease the chance of deterioration of their mood by minimizing the postnatal
depressive symptoms in postnatal women using EPDS assessment tool.
EPDS is a 10-question self-rating scale in measuring the level of depression of
perinatal women by calculating the total score of the 10 items (Cox, Holden, &
Sagovsky, 1987). The Chinese version of EPDS has been validated by Lee & his team
since 1998 and has been used in all MCHCs to screen suspected PND women during
their routine visits at 2-3 months of post delivery since 1998 (Lee et al., 1998).
Secondary outcomes
The secondary patients’ outcome is to evaluate the satisfaction and acceptance
of peer support intervention in target women and peer supporters. Satisfaction survey
with a report scale between 1 (totally disagree) to 5 (totally agree) will be distributed
after the completion of the program. The questionnaire can be returned either by mail
or in person. In the questionnaire, an open-ended question is set and it helps to gather
any comments and suggestions for the program. Sample of surveys are illustrated in
Appendix M and N.
Health care providers’ outcomes
In addition to patient outcomes, healthcare providers’ outcomes are also

62
important for the successfulness of the program implementation. To evaluate nurses’
perception of the innovation, questions are asked towards acceptability, satisfaction
and competence of the healthcare providers in carrying out the intervention. A report
scale between 1 (totally disagree) to 5 (totally agree) will be used to measure the
results. An open-ended question is included in the questionnaire for nurses to
comment on the program. Moreover, a focus group meeting will be held after the
program by the organizing committee. All nurses are welcomed to provide any
feedback and suggestions regarding the whole process of the implementation in the
meeting. Sample of the questionnaire is shown in Appendix L.
Time and frequency of measurements
The full-scale implementation of the guideline takes 31 months. For eligible
postnatal women, pre- and post-EPDS questionnaires will be distributed at 2-3 months
post delivery and after the 6-month intervention period respectively. In addition,
satisfaction survey will be distributed and collected from participants and peer
supporters at the end of the program. During the 6-month intervention period, nurses
are required to monitor the progress of the intervention by phone contacting the peer
supporters regularly at 1st week, 3
rd month and 6
th month after the intervention starts.
An Intervention Progress Sheet (Appendix I) will help the nurses in monitoring the

63
progress of support provided by peer supporters to participants. Finally, satisfaction
survey will be distributed and focus group meetings will be held by the organizing
committee for the nurses after the program.
Nature and Number of Clients Involved
Nature of Clients
The clients to be involved in the evaluation plan are the target population. They
are postnatal women who are (a) with EPDS scores >9 and mood stable after
professional judgment by nurses; (b) within 3 months of post delivery; and (c) aged
≧18. Women who (i) have history of or are currently diagnosed with major
psychiatric or mental disorders; (ii) are taking antidepressants or antipsychotic
medications; or (iii) have history of receiving psychotherapy in the past one year are
excluded.
Number of Clients Involved
The sample size will be calculated by the online sample size calculator by Lenth
(2011) using one sample t-test. Since the EPDS scores measured are from the same
postnatal women and their corresponding mean pre- and post-intervention EPDS
scores are compared, one sample t-test is used.

64
Based on the literature, an effect size of 0.4 is taken from Dennis (2003)’s study,
as the study design most resembles the proposed program and it has the highest level
of evidence. Therefore, by taking significance level of 0.05 and a power of 80%, a
minimal sample size of 397 is needed. Since the dropout rate reported in the literature
ranged from 0% to 23.8% (the longer the intervention period, the higher the reported
rate), the highest rate recorded in the literature with an intervention period less than 6
months is chosen. That is, a dropout rate of 14.8% from Letourneau et al. (2011)’s
study is taken for calculation. As a result, a total sample of 460 women is required.
Data Analysis
The collected data, including the socio-demographic data of the participants and
peer supporters, the pre- and post-intervention EPDS scores and the satisfaction level
of participants, peer supporters and nurses will be entered into Statistical Package for
Social Science (SPSS) version 21 and analyzed statistically. Chi-square test will be
used in analyzing the socio-demographic data collected which includes age of
participants and their infants, geographic residency, education level, occupation,
status of marriage, household income, delivery type and breastfeeding status, while
one sample t-test will be used in measuring the mean score of EPDS rated by
participated postnatal women pre- and post-intervention. Satisfaction level of the

65
participants, peer supporters and staff will also be analyzed by calculating the
percentage of satisfaction of each item in the questionnaire. Qualitative data reported
by nurses in the focus group meeting will be analyzed with identification of categories,
key themes and patterns.
Criteria for Effectiveness
The guideline is considered effective when the depressive symptoms of
postnatal women are minimized by recording a lower EPDS score after six months of
peer support intervention. A reduction of 3 marks in EPDS score in Dennis (2003) is
taken into consideration to evaluate the effectiveness of the program since the study
has the highest level of evidence. Therefore, by using a mean reduction of 3 marks in
EPDS score, the program will be considered effective in minimizing depressive
symptoms in suspected PND women if the post-intervention EPDS score is reduced
by 3 marks or more.
On evaluating the satisfaction level of participants, peer supporters and nurses, a
10-item satisfaction survey using the five-point Likert-type scale is designed for
grading respondents’ satisfaction level. The program is considered effective if the total
score from the survey is being graded over 70% or an individual item in the survey
being graded equals to or greater than 4 marks.

66
Regarding the focus group meeting conducted by the organizing committee with
the nurses, the program is considered effective if positive comments were received
regarding the program implementation.

67
Chapter 7: Conclusion
Postnatal depression affects postnatal women’s physical and psychological
well-beings, and brings detrimental effects to their children and their family. In view
of the high and increasing prevalence of postnatal depression (PND) in Hong Kong, a
new approach should be taken to prevention the disease.
As many of the researchers have consistently concluded the importance of
psychosocial variables in managing and preventing PND, the seven selected studies
provided evidences for the provision of a new psychosocial intervention: peer support
intervention, which is feasible, possible and worthy to be carried out in MCHCs to
postnatal women in minimizing their PND symptoms.
The evidence-based guidelines for nurses and peer supporters are developed
respectively in this proposal and its transferability, feasibility, the cost of the
implementation, a detailed communication plan, pilot study plan and evaluation plan
were reviewed and examined to ensure its smooth application to the real setting. It is
believed that more PND women at risk can be benefited from the program by
minimizing their postnatal depressive symptoms.

68
Appendix A: Postnatal depression Report of Department of Health, 2013

69
Appendix A (continued):
Postnatal depression Report of Department of Health, 2013
RPT001A – Workload statistics on Child Health Service
Total no. (New registration, aged <1yr incl. local and non-local born): 54,656
RPT305 – Identification and management of mothers with postnatal depression
EPDS coverage n %
No. of mothers completing EPDS forms 38,113 -
Total score ≦9 and Q10 score = 0 32,632 85.6
Total score ≧10 or Q10 score > 0 5,481 14.4
EPDS coverage - 91.6
Suspected PND identified 6,734 14.6
By EPDS 5,335 79.2
By clinical interview 1,399 20.8
With psychosocial risk categories 1,171 17.4
Recommended HA service(s) n %
HA service indicated 4,479 66.5
Psychiatric nurse in MCHC 4,192 62.3
Psychiatric doctor in MCHC 4 0.1
HA psychiatric department 19 0.3
A & E 42 0.6
Community Paediatrician 406 6
Receiving appropriate services 166 2.5
Recommended MCHC service n %
Brief FU for progress 5,311 78.9
Phone FU session 1,126 16.7
MO assessment/counseling 1,113 16.5
Social Service needs n %
Social service indicated 2,579 38.3
Referral to IFSC 2,097 81.3
Client is receiving appropriate services 434 16.8
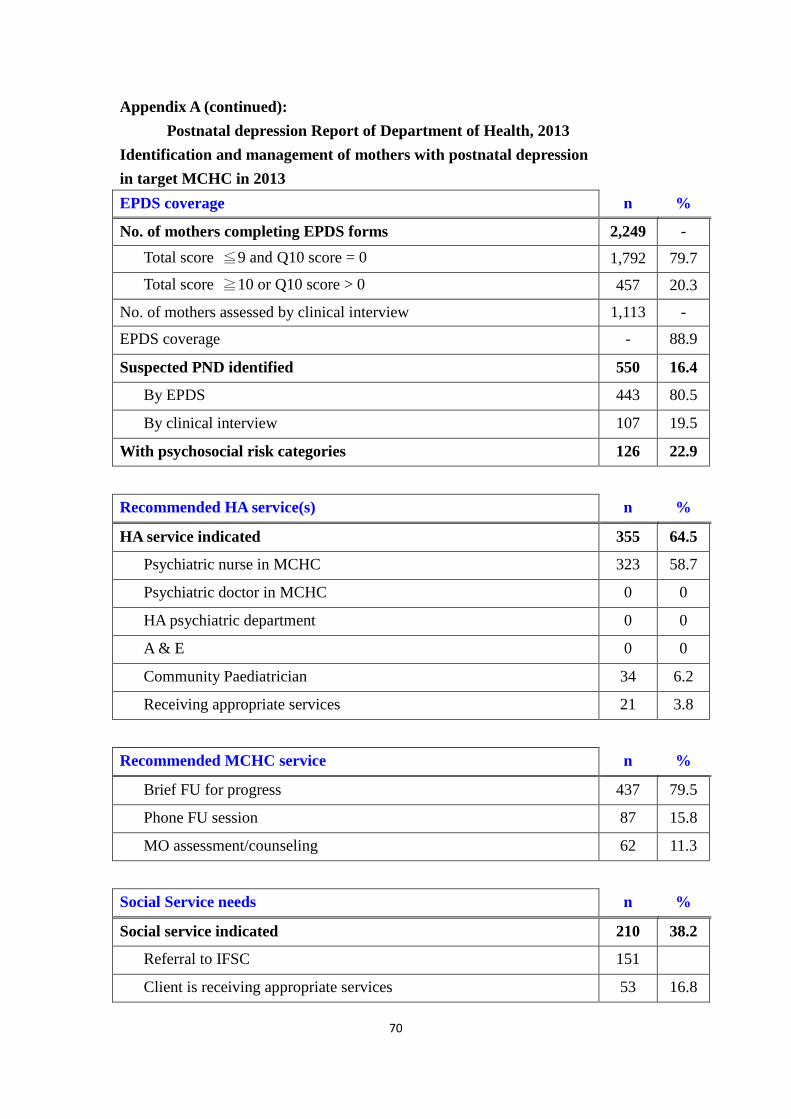
70
Appendix A (continued):
Postnatal depression Report of Department of Health, 2013
Identification and management of mothers with postnatal depression
in target MCHC in 2013
EPDS coverage n %
No. of mothers completing EPDS forms 2,249 -
Total score ≦9 and Q10 score = 0 1,792 79.7
Total score ≧10 or Q10 score > 0 457 20.3
No. of mothers assessed by clinical interview 1,113 -
EPDS coverage - 88.9
Suspected PND identified 550 16.4
By EPDS 443 80.5
By clinical interview 107 19.5
With psychosocial risk categories 126 22.9
Recommended HA service(s) n %
HA service indicated 355 64.5
Psychiatric nurse in MCHC 323 58.7
Psychiatric doctor in MCHC 0 0
HA psychiatric department 0 0
A & E 0 0
Community Paediatrician 34 6.2
Receiving appropriate services 21 3.8
Recommended MCHC service n %
Brief FU for progress 437 79.5
Phone FU session 87 15.8
MO assessment/counseling 62 11.3
Social Service needs n %
Social service indicated 210 38.2
Referral to IFSC 151
Client is receiving appropriate services 53 16.8
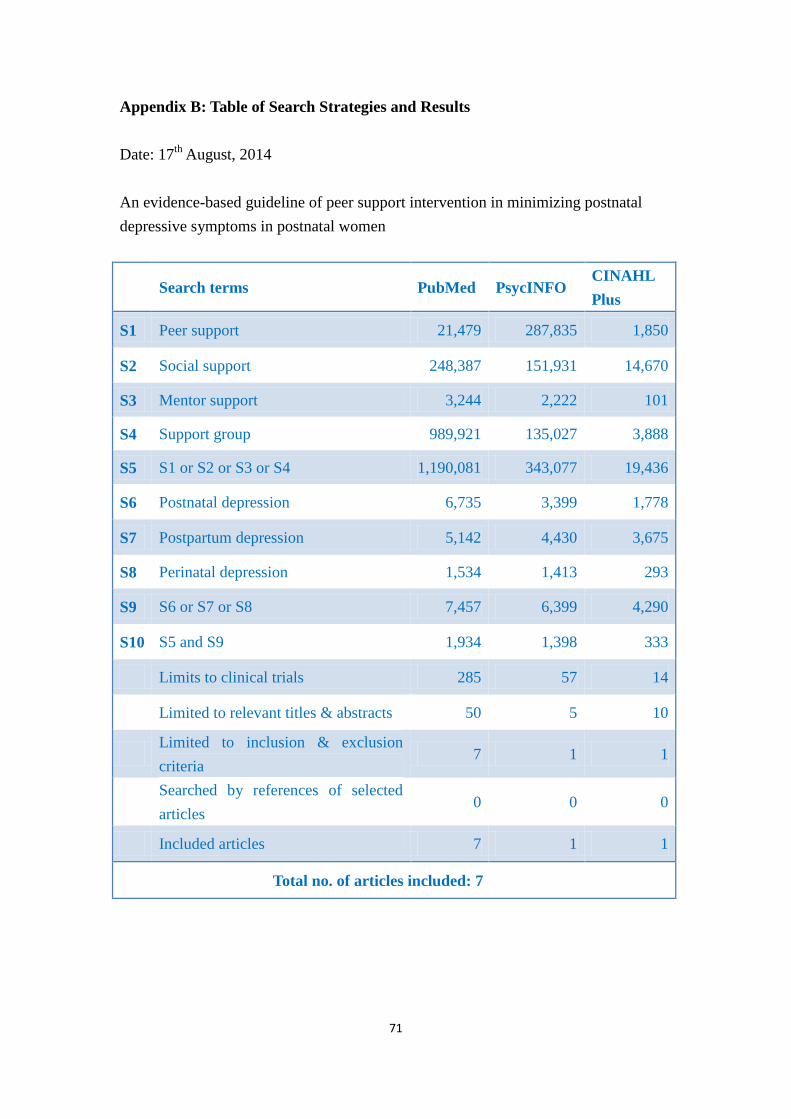
71
Appendix B: Table of Search Strategies and Results
Date: 17th
August, 2014
An evidence-based guideline of peer support intervention in minimizing postnatal
depressive symptoms in postnatal women
Search terms PubMed PsycINFO CINAHL
Plus
S1 Peer support 21,479 287,835 1,850
S2 Social support 248,387 151,931 14,670
S3 Mentor support 3,244 2,222 101
S4 Support group 989,921 135,027 3,888
S5 S1 or S2 or S3 or S4 1,190,081 343,077 19,436
S6 Postnatal depression 6,735 3,399 1,778
S7 Postpartum depression 5,142 4,430 3,675
S8 Perinatal depression 1,534 1,413 293
S9 S6 or S7 or S8 7,457 6,399 4,290
S10 S5 and S9 1,934 1,398 333
Limits to clinical trials 285 57 14
Limited to relevant titles & abstracts 50 5 10
Limited to inclusion & exclusion
criteria 7 1 1
Searched by references of selected
articles 0 0 0
Included articles 7 1 1
Total no. of articles included: 7

72
Appendix B (continued): PRISMA Flow Diagram of literatures searching
Studies identified through electronic database searching
(n = 2,665)
Scre
enin
g In
clu
ded
El
igib
ility
Id
enti
fica
tio
n
Studies after limited to clinical trials
(n = 356)
Studies screened
(n = 65)
Studies excluded
(Not fulfilling inclusion and
exclusion criteria)
(n = 56 )
Full text articles included
(n = 9)
Studies included in final appraisal
(n = 7)
Studies identified in
PubMed
(n = 1,934)
Studies identified in
PsycINFO
(n = 1,398)
Studies identified in
CINAHL Plus
(n = 333)
Studies excluded
(Irrelevant titles and abstracts)
(n = 291)
Studies excluded
(Duplicated copies)
(n = 2)
No extra studies yielded after
searching references
(n = 2)
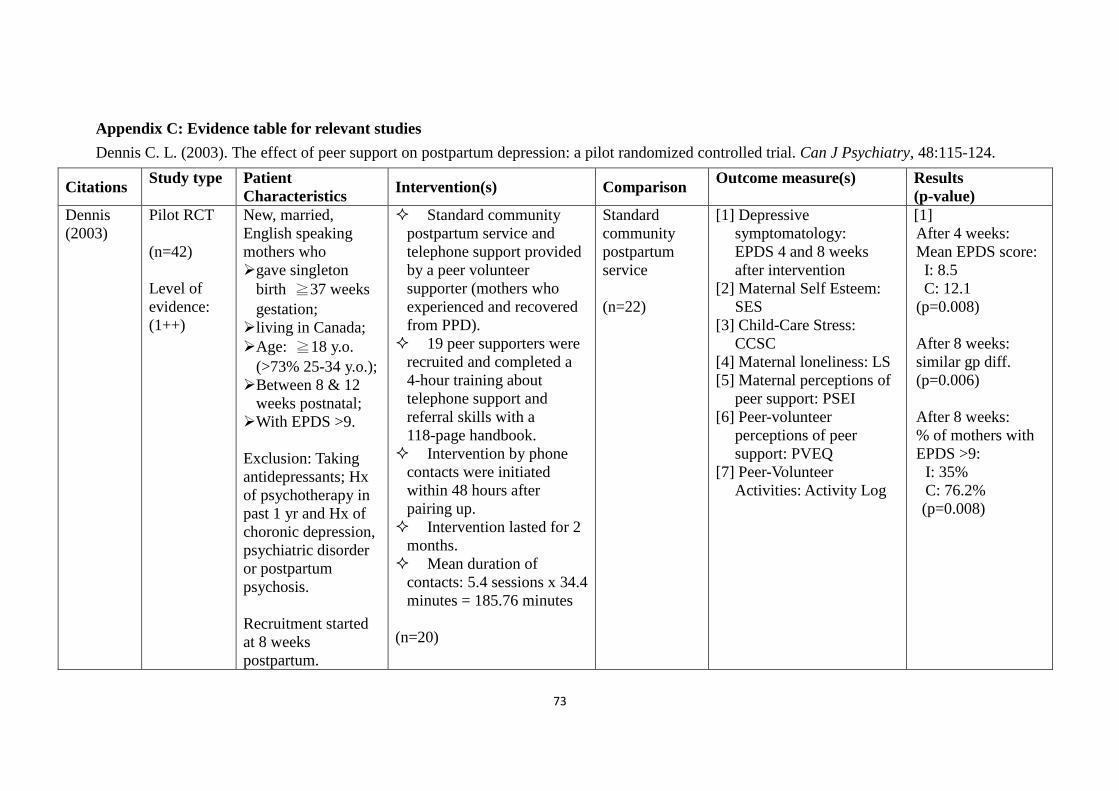
73
Appendix C: Evidence table for relevant studies
Dennis C. L. (2003). The effect of peer support on postpartum depression: a pilot randomized controlled trial. Can J Psychiatry, 48:115-124.
Citations Study type
Patient
Characteristics Intervention(s) Comparison
Outcome measure(s)
Results
(p-value)
Dennis
(2003)
Pilot RCT
(n=42)
Level of
evidence:
(1++)
New, married,
English speaking
mothers who
gave singleton
birth ≧37 weeks
gestation;
living in Canada;
Age: ≧18 y.o.
(>73% 25-34 y.o.);
Between 8 & 12
weeks postnatal;
With EPDS >9.
Exclusion: Taking
antidepressants; Hx
of psychotherapy in
past 1 yr and Hx of
choronic depression,
psychiatric disorder
or postpartum
psychosis.
Recruitment started
at 8 weeks
postpartum.
Standard community
postpartum service and
telephone support provided
by a peer volunteer
supporter (mothers who
experienced and recovered
from PPD).
19 peer supporters were
recruited and completed a
4-hour training about
telephone support and
referral skills with a
118-page handbook.
Intervention by phone
contacts were initiated
within 48 hours after
pairing up.
Intervention lasted for 2
months.
Mean duration of
contacts: 5.4 sessions x 34.4
minutes = 185.76 minutes
(n=20)
Standard
community
postpartum
service
(n=22)
[1] Depressive
symptomatology:
EPDS 4 and 8 weeks
after intervention
[2] Maternal Self Esteem:
SES
[3] Child-Care Stress:
CCSC
[4] Maternal loneliness: LS
[5] Maternal perceptions of
peer support: PSEI
[6] Peer-volunteer
perceptions of peer
support: PVEQ
[7] Peer-Volunteer
Activities: Activity Log
[1]
After 4 weeks:
Mean EPDS score:
I: 8.5
C: 12.1
(p=0.008)
After 8 weeks:
similar gp diff.
(p=0.006)
After 8 weeks:
% of mothers with
EPDS >9:
I: 35%
C: 76.2%
(p=0.008)

74
Appendix C (continued): Evidence table for relevant studies
Dennis, C. L., Hodnett, E., Kenton, L., Weston, J., Zupancic, J., Stewart, D. E., & Kiss, A. (2009). Effect of peer support on prevention of
postnatal depression among high risk women: multisite randomised controlled trial. BMJ, 338, a3064.
Citations Study type
Patient
Characteristics
Intervention(s) Comparison Outcome measure(s)
(Tool)
Results
(p-value)
Dennis et
al., (2009)
Multisite
RCT
(n=701)
Level of
evidence:
(1++)
New English
speaking mothers:
gave a live birth
baby and
discharged home
with baby;
lives in Canada
≦2 weeks
postpartum;
Age: ≧18 y.o.
(78% 20-34 y.o.);
>92% married;
EPDS score >9
(baseline EPDS:
I:12.5 & C:12.6).
Exclusion: taking
antidepressants or
antipsychotic drugs.
Recruitment started
within 24-48 hours
postpartum.
Standard postpartum
care and telephone support
provided by a peer
volunteer.
204 supporters were
training 4 hours with skills
in providing effective
telephone based support and
making hospital referrals
with a 121 page training
manual given.
Telephone supports
were initiated within 72
hours after peer allocation.
Intervention lasted for
24 weeks.
A minimum of 4
contacts should be taken by
each peer volunteer.
Mean duration of
contacts: 8.8 sessions x
14.1minutes = 124.08
minutes
(n=349)
Standard
postpartum
care
(n=352)
[1] Postnatal depression
After 12 & 24 weeks:
EPDS score;
[2] Anxiety: State-trait
anxiety inventory;
[3] Loneliness: UCLA
loneliness scale;
[4] Use of health service:
[1] EPDS score
after 12 weeks:
I: 7.93
C: 8.89
(p=0.02)
EPDS score after
24 weeks:
I: 7.00
C: 7.61
(p=0.10)
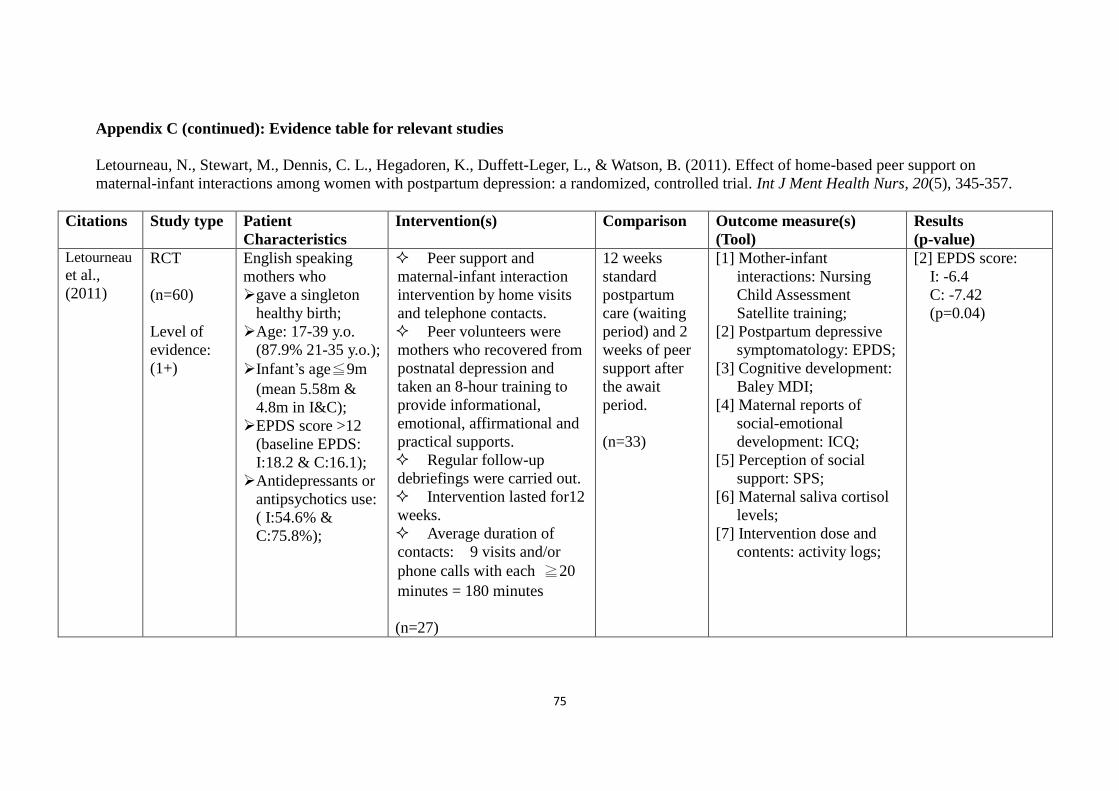
75
Appendix C (continued): Evidence table for relevant studies
Letourneau, N., Stewart, M., Dennis, C. L., Hegadoren, K., Duffett-Leger, L., & Watson, B. (2011). Effect of home-based peer support on
maternal-infant interactions among women with postpartum depression: a randomized, controlled trial. Int J Ment Health Nurs, 20(5), 345-357.
Citations Study type
Patient
Characteristics
Intervention(s) Comparison Outcome measure(s)
(Tool)
Results
(p-value) Letourneau et al.,
(2011)
RCT
(n=60)
Level of
evidence:
(1+)
English speaking
mothers who
gave a singleton
healthy birth;
Age: 17-39 y.o.
(87.9% 21-35 y.o.);
Infant’s age≦9m
(mean 5.58m &
4.8m in I&C);
EPDS score >12
(baseline EPDS:
I:18.2 & C:16.1);
Antidepressants or
antipsychotics use:
( I:54.6% &
C:75.8%);
Peer support and
maternal-infant interaction
intervention by home visits
and telephone contacts.
Peer volunteers were
mothers who recovered from
postnatal depression and
taken an 8-hour training to
provide informational,
emotional, affirmational and
practical supports.
Regular follow-up
debriefings were carried out.
Intervention lasted for12
weeks.
Average duration of
contacts: 9 visits and/or
phone calls with each ≧20
minutes = 180 minutes
(n=27)
12 weeks
standard
postpartum
care (waiting
period) and 2
weeks of peer
support after
the await
period.
(n=33)
[1] Mother-infant
interactions: Nursing
Child Assessment
Satellite training;
[2] Postpartum depressive
symptomatology: EPDS;
[3] Cognitive development:
Baley MDI;
[4] Maternal reports of
social-emotional
development: ICQ;
[5] Perception of social
support: SPS;
[6] Maternal saliva cortisol
levels;
[7] Intervention dose and
contents: activity logs;
[2] EPDS score:
I: -6.4
C: -7.42
(p=0.04)

76
Appendix C (continued): Evidence table for relevant studies
Taft, A. J., Small, R., Hegarty, K. L., Watson, L. F., Gold, L., & Lumley, J. A. (2011). Mothers' AdvocateS In the Community (MOSAIC) --
non-professional mentor support to reduce intimate partner violence and depression in mothers: a cluster randomised trial in primary care. BMC
Public Health, 11, 178.
Citations Study type
Patient
Characteristics
Intervention(s) Comparison Outcome measure(s)
(Tool)
Results
(p-value)
Taft et al.,
(2011)
Cluster
RCT
(n=174)
Level of
evidence:
(1+)
English speaking,
disclosed IPV or
psychosocially
distressed women:
Aged >= 16 y.o.
(mean: ~32 y.o.);
Pregnant or had
child(ren) <5 y.o.;
Depression status:
(EPDS score≧13:
I:70% & C:58%);
Exclusion: serious
mental illness and
level of English
inadequate for
informed consent.
MOSAIC’s mentoring
provided by 32 mentors
recruited in the community.
Mentoring was provided
by weekly home visiting.
Mentors were mothers
and were trained for five
days that included
befriending, domestic
violence advocacy, working
with depression, parenting
support, safety and self care
skills.
Intervention lasted for
12 months and regular
meetings (1, 4, 8, 12m) were
provided for mentors for
further training and support.
Intensity of intervention:
58% of participants reported
weekly meetings with
mentors.
(n=113)
6 hours IPV
training for
clinician only.
(n=61)
Primary outcomes:
[1] Partner abuse: CAS
[2] Depressive symptoms:
EPDS
Secondary outcomes:
[3] Mental and physical
health well-being: SF-36;
[4] Parenting stress: PSIS
[5] Social support: MOS SF
[2] EPDS score:
I: -6.1
C: -3
(p=0.09)
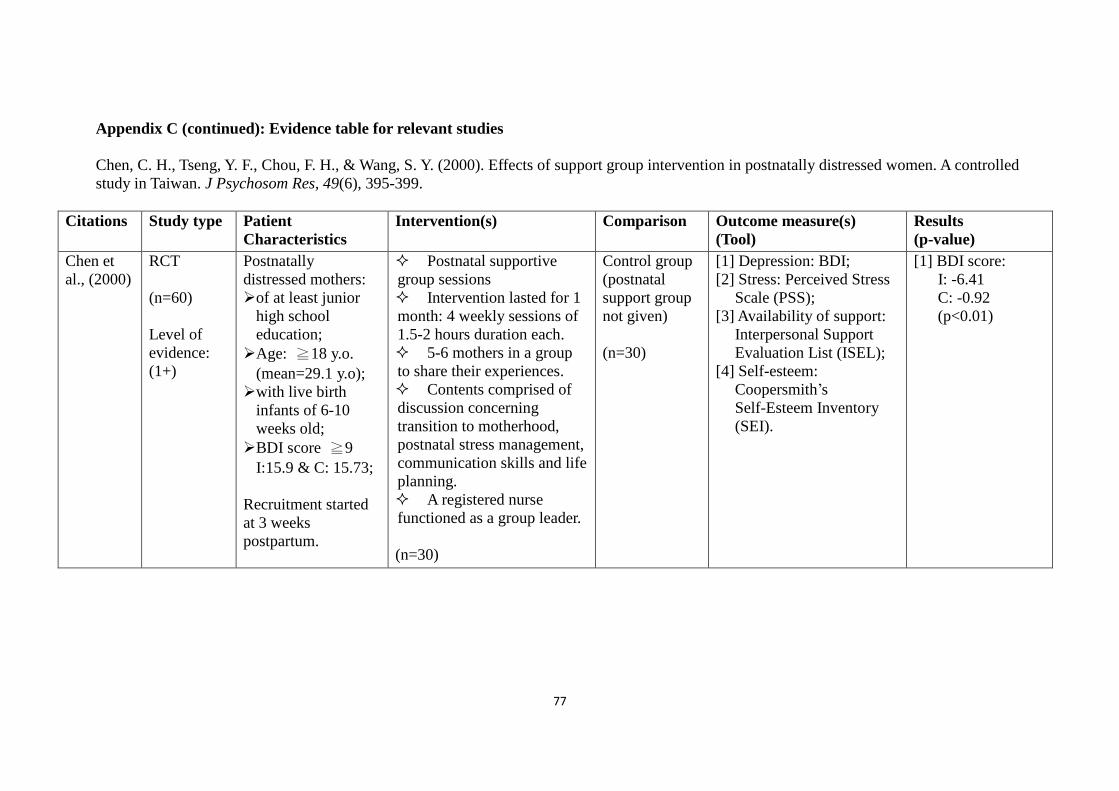
77
Appendix C (continued): Evidence table for relevant studies
Chen, C. H., Tseng, Y. F., Chou, F. H., & Wang, S. Y. (2000). Effects of support group intervention in postnatally distressed women. A controlled
study in Taiwan. J Psychosom Res, 49(6), 395-399.
Citations Study type
Patient
Characteristics
Intervention(s) Comparison Outcome measure(s)
(Tool)
Results
(p-value)
Chen et
al., (2000)
RCT
(n=60)
Level of
evidence:
(1+)
Postnatally
distressed mothers:
of at least junior
high school
education;
Age: ≧18 y.o.
(mean=29.1 y.o);
with live birth
infants of 6-10
weeks old;
BDI score ≧9
I:15.9 & C: 15.73;
Recruitment started
at 3 weeks
postpartum.
Postnatal supportive
group sessions
Intervention lasted for 1
month: 4 weekly sessions of
1.5-2 hours duration each.
5-6 mothers in a group
to share their experiences.
Contents comprised of
discussion concerning
transition to motherhood,
postnatal stress management,
communication skills and life
planning.
A registered nurse
functioned as a group leader.
(n=30)
Control group
(postnatal
support group
not given)
(n=30)
[1] Depression: BDI;
[2] Stress: Perceived Stress
Scale (PSS);
[3] Availability of support:
Interpersonal Support
Evaluation List (ISEL);
[4] Self-esteem:
Coopersmith’s
Self-Esteem Inventory
(SEI).
[1] BDI score:
I: -6.41
C: -0.92
(p<0.01)
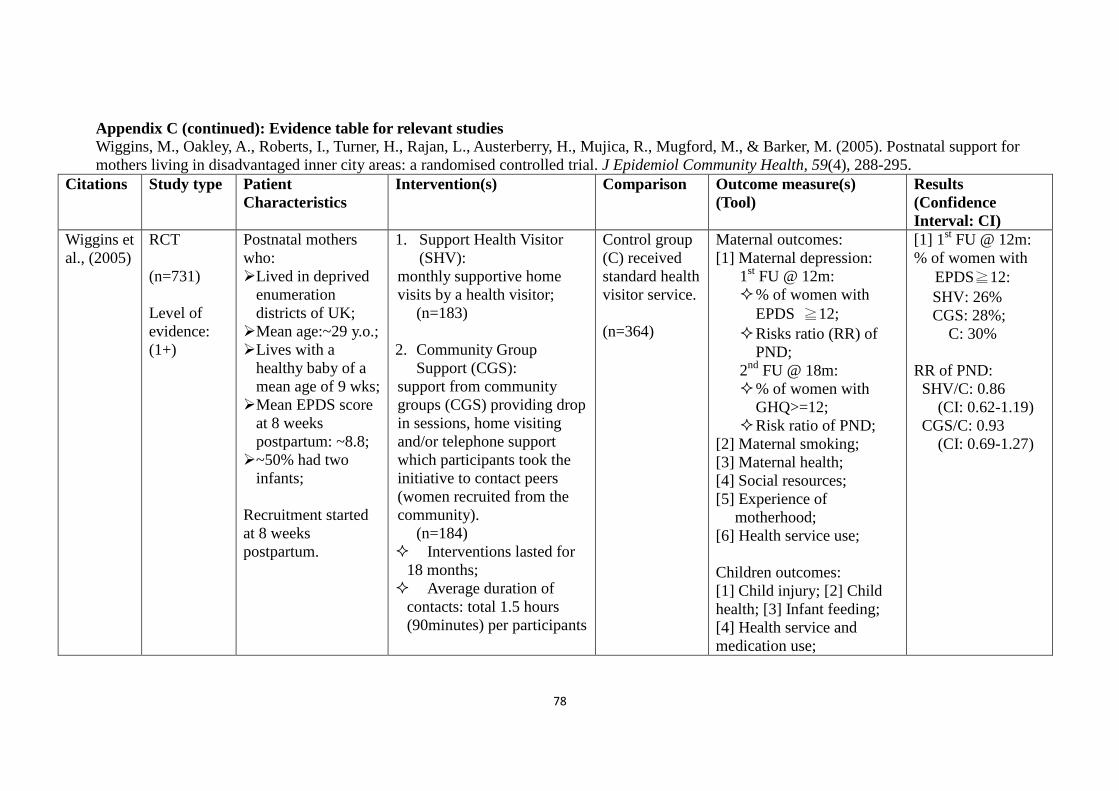
78
Appendix C (continued): Evidence table for relevant studies
Wiggins, M., Oakley, A., Roberts, I., Turner, H., Rajan, L., Austerberry, H., Mujica, R., Mugford, M., & Barker, M. (2005). Postnatal support for
mothers living in disadvantaged inner city areas: a randomised controlled trial. J Epidemiol Community Health, 59(4), 288-295.
Citations Study type
Patient
Characteristics
Intervention(s) Comparison Outcome measure(s)
(Tool)
Results
(Confidence
Interval: CI)
Wiggins et
al., (2005)
RCT
(n=731)
Level of
evidence:
(1+)
Postnatal mothers
who:
Lived in deprived
enumeration
districts of UK;
Mean age:~29 y.o.;
Lives with a
healthy baby of a
mean age of 9 wks;
Mean EPDS score
at 8 weeks
postpartum: ~8.8;
~50% had two
infants;
Recruitment started
at 8 weeks
postpartum.
1. Support Health Visitor
(SHV):
monthly supportive home
visits by a health visitor;
(n=183)
2. Community Group
Support (CGS):
support from community
groups (CGS) providing drop
in sessions, home visiting
and/or telephone support
which participants took the
initiative to contact peers
(women recruited from the
community).
(n=184)
Interventions lasted for
18 months;
Average duration of
contacts: total 1.5 hours
(90minutes) per participants
Control group
(C) received
standard health
visitor service.
(n=364)
Maternal outcomes:
[1] Maternal depression:
1st FU @ 12m:
% of women with
EPDS ≧12;
Risks ratio (RR) of
PND;
2nd
FU @ 18m:
% of women with
GHQ>=12;
Risk ratio of PND;
[2] Maternal smoking;
[3] Maternal health;
[4] Social resources;
[5] Experience of
motherhood;
[6] Health service use;
Children outcomes:
[1] Child injury; [2] Child
health; [3] Infant feeding;
[4] Health service and
medication use;
[1] 1st FU @ 12m:
% of women with
EPDS≧12:
SHV: 26%
CGS: 28%;
C: 30%
RR of PND:
SHV/C: 0.86
(CI: 0.62-1.19)
CGS/C: 0.93
(CI: 0.69-1.27)

79
Appendix C (continued): Evidence table for relevant studies
Gjerdingen, D. K., McGovern, P., Pratt, R., Johnson, L., & Crow, S. (2013). Postpartum doula and peer telephone support for postpartum
depression: a pilot randomized controlled trial. J Prim Care Community Health, 4(1), 36-43.
Citations Study type
Patient
Characteristics
Intervention(s) Comparison Outcome measure(s)
(Tool)
Results
(p-value)
Gjerdinge
n et al.,
(2013)
RCT
(n=39)
Level of
evidence:
(1+)
English speaking
mothers:
living in
Minneapolis/St.
Paul metropolitan
area of the US;
Age ≧16 y.o.
(mean=29.7 y.o.) ;
Infant age: 0-6
months old;
PHQ-9 score≧10;
Baseline mean
CES-D scores:
PD: 33.7
PTS: 32.5
C: 28.1;
1. 6 Postpartum doulas (PD):
Home visits
Average ~6.9 home
visits and 23.4 hours
contacts with each
assigned mothers;
Services included
education regarding infant
care and feeding, practical
and emotional support.
(n=12)
2. 6 Peer telephone
supporters (PTS):
Telephone supports on
educational, emotional
and comparison support.
Total duration of
contacts: ~5.6 calls (63.6
minutes) in telephone
conversation with each
participant.
Intervention lasted for 6
months.
(n=13)
Control group
(C)
(n=14)
[1] General health
[2] Mental & physical
health: Center for
Epidemiological
Studies-Depression
Scale: CES-D score;
[3] Social support
[2] CES-D score @
6 months:
PD: 16.9 (-16.3)
PTS: 17.8 (-14.5)
C: 17.9 (-10.1)
(p=0.397)

80
Appendix D: Quality Assessment of selected studies.
S I G N
Methodology Checklist 2: Controlled Trials
Dennis C. L. (2003). The effect of peer support on postpartum depression: a pilot randomized
controlled trial. Can J Psychiatry, 48:115-124.
Guideline topic:
An evidence-based guideline of peer support intervention in
minimizing postnatal depressive symptoms in postnatal
women
Key Question No: Reviewer:
Section 1: Internal validity
In a well conducted RCT study… Does this study do it?
1.1 The study addresses an appropriate and clearly focused question. Yes
1.2 The assignment of subjects to treatment groups is randomised. Yes Randomization was
achieved by using
consecutively
numbered, sealed,
opaque envelopes
containing randomly
generated numbers.
1.3 An adequate concealment method is used. Yes
1.4 Subjects and investigators are kept ‘blind’ about treatment
allocation.1
Yes Only research
assistants are blinded
to the group
allocation. Trial
participants and peer
supporters cannot be
blinded.

81
1.5 The treatment and control groups are similar at the start of the trial. Yes No significant
differences in age,
education, income,
and EPDS score were
found. There were no
statistically
significant differences
between the 2 groups.
1.6 The only difference between groups is the treatment under
investigation.
Yes
1.7 All relevant outcomes are measured in a standard, valid and reliable
way.
Yes
1.8 What percentage of the individuals or clusters recruited into each
treatment arm of the study dropped out before the study was
completed?
No drop out in the
experimental group. Only 1
mother (out of 22) dropped out
in the control group who did
not complete the 8-week
assessment.
1/42 = 2.38%
1.9 All the subjects are analysed in the groups to which they were
randomly allocated (often referred to as intention to treat analysis).
Yes Discontinuation of the
intervention did not
entail the participant’s
exclusion from the
study, and an
intention to treat
approach was used to
analyze these data.
1.10 Where the study is carried out at more than one site, results are
comparable for all sites.
Does not apply
Section 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise bias?
Code as follows:
High quality (++)
2.2 Taking into account clinical considerations, your
evaluation of the methodology used, and the
statistical power of the study, are you certain that
the overall effect is due to the study
intervention?
In this pilot randomized controlled trial, the
methodology used and the statistical power
presented are of good quality in evaluating the
effect of telephone peer support
(mother-to-mother) on depressive
symptomatology among mothers identified as
82
high-risk of postpartum depression (PPD). The
overall effect is due to the study intervention.
2.3 Are the results of this study directly applicable
to the patient group targeted by this guideline?
Yes
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment of the study,
and the extent to which it answers your question and mention any areas of uncertainty raised above.
Author’s conclusion: This pilot RCT effectively evaluated the effect of peer support telephone
intervention in decreasing the risk of PPD among high risk mothers.
Own comments: Recruitment of participants and volunteered peer supporters are well described.
Training contents of the peer supporters are also well illustrated. In reporting the intervention results,
only percentage of mothers who had EPDS scores >9 and >12 are presented instead of the actual
scores. Through p-values are stated, the actual effect of how much the intervention in decreasing the
EPDS score were not reported in the paper. Another limitation is the small sample size which
comprised of total 42 participants.
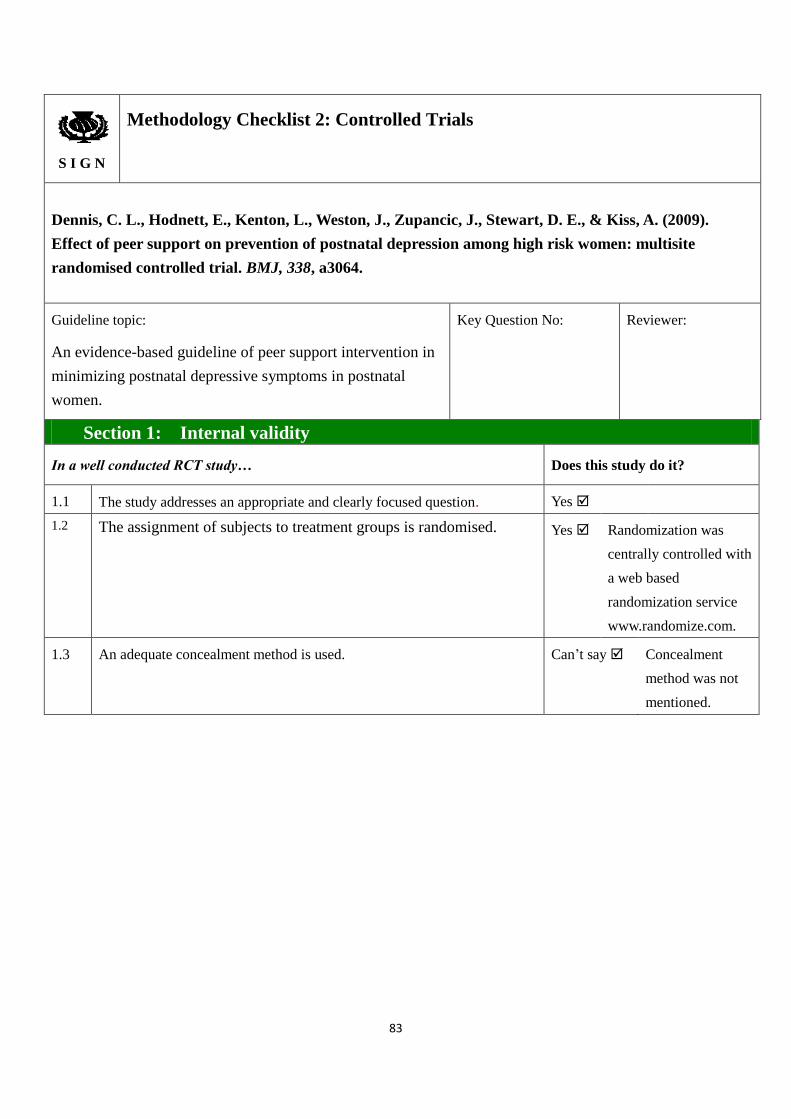
83
S I G N
Methodology Checklist 2: Controlled Trials
Dennis, C. L., Hodnett, E., Kenton, L., Weston, J., Zupancic, J., Stewart, D. E., & Kiss, A. (2009).
Effect of peer support on prevention of postnatal depression among high risk women: multisite
randomised controlled trial. BMJ, 338, a3064.
Guideline topic:
An evidence-based guideline of peer support intervention in
minimizing postnatal depressive symptoms in postnatal
women.
Key Question No: Reviewer:
Section 1: Internal validity
In a well conducted RCT study… Does this study do it?
1.1 The study addresses an appropriate and clearly focused question. Yes
1.2 The assignment of subjects to treatment groups is randomised.
Yes Randomization was
centrally controlled with
a web based
randomization service
www.randomize.com.
1.3 An adequate concealment method is used.
Can’t say Concealment
method was not
mentioned.

84
1.4 Subjects and investigators are kept ‘blind’ about treatment allocation. Yes Single blind (assessors
blinded). The research
nurses were blinded to
the group allocation and
were responsible to
assess trial outcomes.
Trial participants and
peer supporters could
not be blinded to group
allocation, health
professionals and
service providers of
standard community
postpartum care were
not informed of any
mother’s participation
in the trial or group
allocation. .
1.5 The treatment and control groups are similar at the start of the trial. Yes There were no clinically
important differences
between the two groups.
The mean scores of
EPDS were similar in
the 2 groups.
1.6 The only difference between groups is the treatment under investigation. Yes
1.7 All relevant outcomes are measured in a standard, valid and reliable way. Yes
1.8 What percentage of the individuals or clusters recruited into each
treatment arm of the study dropped out before the study was completed?
At 12 weeks postpartum,
87.4% participants completed
the FU telephone interview,
decreasingly slightly to 85.6%
participants at 24 weeks.
Dropout rate was 12.6% and
14.4% at 12 & 24 weeks FU
respectively.
1.9 All the subjects are analysed in the groups to which they were randomly
allocated (often referred to as intention to treat analysis).
Yes Data were analyzed
with SAS version 9.1
and an intention to treat
approach.

85
1.10 Where the study is carried out at more than one site, results are
comparable for all sites.
No Results were not
presented separately
from the7 large health
regions in Canada.
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise bias?
Code as follows:
High quality (++)
2.2 Taking into account clinical considerations, your
evaluation of the methodology used, and the
statistical power of the study, are you certain that the
overall effect is due to the study intervention?
Taking into account the clinical methodology used and
statistical power of the study, the overall effect is due
to the study intervention of peer telephone support
intervention.
2.3 Are the results of this study directly applicable to the
patient group targeted by this guideline?
Yes
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment of the study, and the
extent to which it answers your question and mention any areas of uncertainty raised above.
Author’s conclusion: Telephone based peer support might be effective in preventing PPD among high risk
postpartum mothers immediately after delivery. It is feasible to recruit lay people who have experienced a
similar health problem or stressor (e.g. PND) and they can have a positive effect on potential sufferers’
psychological wellbeing. Women in the study were satisfied and receptive in receiving telephone support and
such experience.
Own comments: In this study, the methodology used was RCT; statistical power was >80%; a significant
reduction of PPD risk (women received peer support through telephone were at 1/2 of the risk in developing
PPD at 12 weeks postpartum); lost to follow-up was <15% and >80% of participants were satisfied with the
intervention. The overall effect of the study was successful. Telephone based peer support could help to
prevent postnatal depression in mothers who have recently given birth.
The only limitation of the study was that the clinical diagnostic data for PND might be questionable because
the study only identified 7% of high risk PPD mothers in which the prevalence was lower than the current PND
prevalence of ~13% in recent meta-analysis. This was possibly due to the fact that data collection process was
carried out by generalized nurses who may be undertrained. In future, structured clinical interview could be
administered face-to-face by a mental health specialist as suggested by the author.
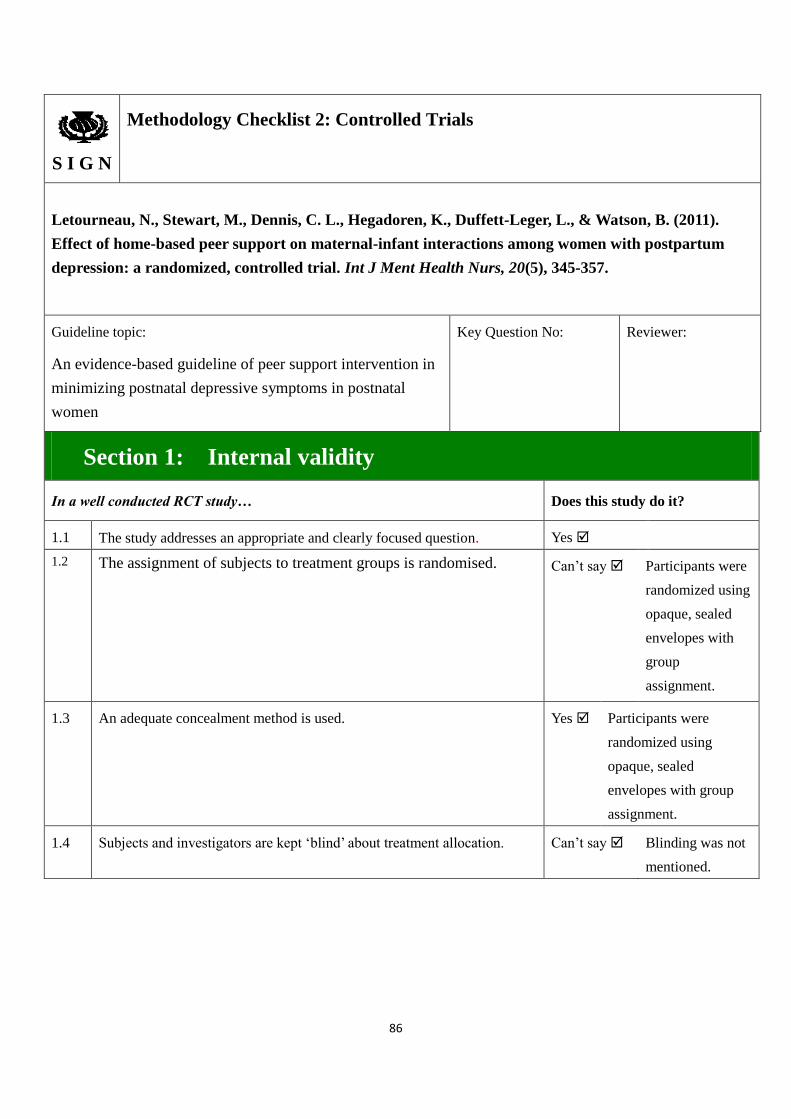
86
S I G N
Methodology Checklist 2: Controlled Trials
Letourneau, N., Stewart, M., Dennis, C. L., Hegadoren, K., Duffett-Leger, L., & Watson, B. (2011).
Effect of home-based peer support on maternal-infant interactions among women with postpartum
depression: a randomized, controlled trial. Int J Ment Health Nurs, 20(5), 345-357.
Guideline topic:
An evidence-based guideline of peer support intervention in
minimizing postnatal depressive symptoms in postnatal
women
Key Question No: Reviewer:
Section 1: Internal validity
In a well conducted RCT study… Does this study do it?
1.1 The study addresses an appropriate and clearly focused question. Yes
1.2 The assignment of subjects to treatment groups is randomised. Can’t say Participants were
randomized using
opaque, sealed
envelopes with
group
assignment.
1.3 An adequate concealment method is used. Yes Participants were
randomized using
opaque, sealed
envelopes with group
assignment.
1.4 Subjects and investigators are kept ‘blind’ about treatment allocation. Can’t say Blinding was not
mentioned.

87
1.5 The treatment and control groups are similar at the start of the trial. Yes No statistical
differences were
observed between the
groups on any
demographic or
descriptive variables,
except for medication
use and infant sex.
1.6 The only difference between groups is the treatment under investigation. Can’t say After the 12
weeks of await
period, the
participants
would receive 2
weeks of peer
supports.
1.7 All relevant outcomes are measured in a standard, valid and reliable way. Yes
1.8 What percentage of the individuals or clusters recruited into each
treatment arm of the study dropped out before the study was completed?
Dropout rate was 14.8% and
15.2 % in treatment and
control group respectively.
1.9 All the subjects are analysed in the groups to which they were randomly
allocated (often referred to as intention to treat analysis).
Yes Outliners were not
removed, and covariates
were not included in the
final analysis.
1.10 Where the study is carried out at more than one site, results are
comparable for all sites.
Does not apply
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise bias?
Code as follows:
Acceptable (+)
2.2 Taking into account clinical considerations, your
evaluation of the methodology used, and the
statistical power of the study, are you certain that the
overall effect is due to the study intervention?
After taking into account clinical considerations, it is
not certain that the overall effect of the study is due to
the intervention.
2.3 Are the results of this study directly applicable to the
patient group targeted by this guideline?
Part of the results (e.g. intervention effect in
minimizing postnatal depression level) was applicable
to the targeted patient group.

88
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment of the study, and the
extent to which it answers your question and mention any areas of uncertainty raised above.
Author’s conclusions: Though significant results were observed in the intervention group, the effect was
larger in the control group (control group had a greater reduction in the EPDS score for measures of symptoms
of postpartum depression and perceived social support.
Reasons: significant higher depressive symptoms experienced by the treatment group over the 12 weeks
intervention period might have impaired mothers’ ability to interact with their infants and participants in the
treatment group presented and persisted in having more sever depressive symptoms may have confounded the
findings. Training, follow-up and debriefing provided to peers might have been insufficient. Moreover, mothers
with PND are uncomfortable in receiving advices and would perceive it as judgment of their parenting
abilities.
Own comments: The primary outcome measure of this study is maternal-infant interactions via observational
nursing child assessment satellite training (NCAST) programme feeding and teaching scales through direct
home visits and/or telephone supports, while postpartum depressive symptomatology by EPDS is only one of
the secondary outcome measures. Therefore, supports provided by peer supporters might favors skills in
modifying feeding and parenting needs of the participants instead of providing supports on mental needs of
mothers. Also, the participants in the study were mothers having high scores (EPDS>12) and some were even
already taking depressive medications. These may confound the study outcome and the effectiveness of the
intervention.
Taking into account the significance of the study result in reducing maternal depressive symptoms, peer
telephone support with home visit intervention was effective in reducing postpartum depression symptoms in
mothers.

89
S I G N
Methodology Checklist 2: Controlled Trials
Taft, A. J., Small, R., Hegarty, K. L., Watson, L. F., Gold, L., & Lumley, J. A. (2011). Mothers'
AdvocateS In the Community (MOSAIC) -- non-professional mentor support to reduce intimate
partner violence and depression in mothers: a cluster randomised trial in primary care. BMC Public
Health, 11, 178.
Guideline topic:
An evidence-based guideline of peer support intervention in
minimizing postnatal depressive symptoms in postnatal
women
Key Question No: Reviewer:
Section 1: Internal validity
In a well conducted RCT study… Does this study do it?
1.1 The study addresses an appropriate and clearly focused question. Yes
1.2 The assignment of subjects to treatment groups is randomised. Yes
GP practices and
MCHN teams were
randomized at separate
public meetings for the
recruitment. For GPs,
names (stratified by
practice size – one GP
or more than one GP
participating)… the
selection made by an
invited guest from
outside the project or
research team.

90
1.3 An adequate concealment method is used. Yes Randomization were
concealed in opaque
envelopes and randomly
selected by someone
outside the study.
Similarly names of the
MCHN teams were
concealed in opaque
envelopes, with teams
stratified by the number of
births in the local
government area and GPs
and MCH nurse Team
Leaders were present to
ensure the fairness of the
process and to check the
contents of the envelopes
prior to their being sealed.
1.4 Subjects and investigators are kept ‘blind’ about treatment allocation. No MOSAIC is a
pragmatic
intervention study.
Due to cluster
randomization, it was
not possible to blind
the health care
providers… research
staff were not blind to
participant status.

91
1.5 The treatment and control groups are similar at the start of the trial. No At baseline, there
were few differences
in the
socio-demographic
profiles of
participants retained
in the study.
The intervention
group displayed
higher levels of
probable depression
and parenting stress
and significantly
lower social support.
Women lost to the
study were more
likely to be more
severely abused.
1.6 The only difference between groups is the treatment under investigation. No Baseline
socio-demographic,
depression and
parenting stress level
were different.
1.7 All relevant outcomes are measured in a standard, valid and reliable way. Yes
1.8 What percentage of the individuals or clusters recruited into each
treatment arm of the study dropped out before the study was completed?
133 (76.4%) women
completed follow-up at 12
months.
Dropout rate is 23.6%.
1.9 All the subjects are analysed in the groups to which they were randomly
allocated (often referred to as intention to treat analysis).
Yes
1.10 Where the study is carried out at more than one site, results are
comparable for all sites.
No This is a cluster RCT
which participating
clinicians and GPs were
stratified and
randomized at the time
of participation.
SECTION 2: OVERALL ASSESSMENT OF THE STUDY

92
2.1 How well was the study done to minimise bias?
Code as follows:
Acceptable (+)
2.2 Taking into account clinical considerations, your
evaluation of the methodology used, and the
statistical power of the study, are you certain that the
overall effect is due to the study intervention?
Taking into account clinical considerations, evaluation
of the methodology used and the statistical power of
the study, it was certain that the overall effect was due
to the study intervention.
2.3 Are the results of this study directly applicable to the
patient group targeted by this guideline?
Yes
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment of the study, and the
extent to which it answers your question and mention any areas of uncertainty raised above.
Author’s conclusion: The evidence for effective interventions to reduce IPV and improve abused women’s
wellbeing is very limited. In this first primary care randomized trial of non-professional mentor support for
women abused by intimate partners, there was evidence of a true difference of reduced partner violence
between mentored women referred from primary care populations compared with those not mentored. There
was weak evidence for other findings suggestive of mentor benefit in reducing depression and improving
physical and mental wellbeing.
Own comments: The weak intervention effect on both to reduce intimate partner violence and depression in
mothers might be due to potential bias in participant selection without blinding of clinicians during the
recruitment process and the small sample size being recruited (smaller number of participants being recruited
than anticipated). However, the intervention of providing home visits to mothers did show a clinical significant
result, and therefore, innovation was still useful and effective.

93
S I G N
Methodology Checklist 2: Controlled Trials
Chen, C. H., Tseng, Y. F., Chou, F. H., & Wang, S. Y. (2000). Effects of support group intervention in
postnatally distressed women. A controlled study in Taiwan. J Psychosom Res, 49(6), 395-399.
Guideline topic:
An evidence-based guideline of peer support intervention in
minimizing postnatal depressive symptoms in postnatal
women.
Key Question No: Reviewer:
Section 1: Internal validity
In a well conducted RCT study… Does this study do it?
1.1 The study addresses an appropriate and clearly focused question. Yes
1.2 The assignment of subjects to treatment groups is randomised. Can’t say Women who met
the inclusion
criteria were
randomly
assigned to either
the support or
control groups.
1.3 An adequate concealment method is used. Can’t say Concealment
method was not
mentioned
1.4 Subjects and investigators are kept ‘blind’ about treatment allocation. Can’t say

94
1.5 The treatment and control groups are similar at the start of the trial. Yes There were no
significant differences
in the demographic
characteristics of the
experimental and
control groups. The
psychosocial
parameters of these
two groups before the
group meetings were
also similar.
1.6 The only difference between groups is the treatment under investigation. Yes
1.7 All relevant outcomes are measured in a standard, valid and reliable way. Yes
1.8 What percentage of the individuals or clusters recruited into each
treatment arm of the study dropped out before the study was completed?
Although 34 of the distressed
women who were assigned to the
experimental group consented to
attend the support group sessions,
4 of them declined participation.
30 women received intervention
and all completed the study.
Drop out = 0%
1.9 All the subjects are analysed in the groups to which they were randomly
allocated (often referred to as intention to treat analysis).
Yes
1.10 Where the study is carried out at more than one site, results are
comparable for all sites.
Does not apply
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise bias?
Code as follows:
Acceptable (+)
2.2 Taking into account clinical considerations, your
evaluation of the methodology used, and the
statistical power of the study, are you certain that the
overall effect is due to the study intervention?
Taking into account clinical considerations, evaluation
of the methodology used and the statistical power of
the study, it was certain that the overall effect is due to
the study intervention.
2.3 Are the results of this study directly applicable to the
patient group targeted by this guideline?
Yes
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment of the study, and the

95
extent to which it answers your question and mention any areas of uncertainty raised above.
Author’s conclusion: A significant decrease from the baseline in the BDI scores was found in those
subjects who attended the support meetings. There was a significant decrease in the % of women with
BDI scored greater 9 (experimental group to 33% while the control group 60%) during their follow
up at the end of the four group sessions. The results demonstrated that participation in the support
group resulted in significant psychosocial benefits for postnatally distressed women.
Own comments: Participants in this RCT were Asians while subjects in other papers were
Westerners. The different in cultures and ethnicity may have confounders in future application of
innovation. This study adds evidence that the innovation of peer support also applies in Asian
cultures.
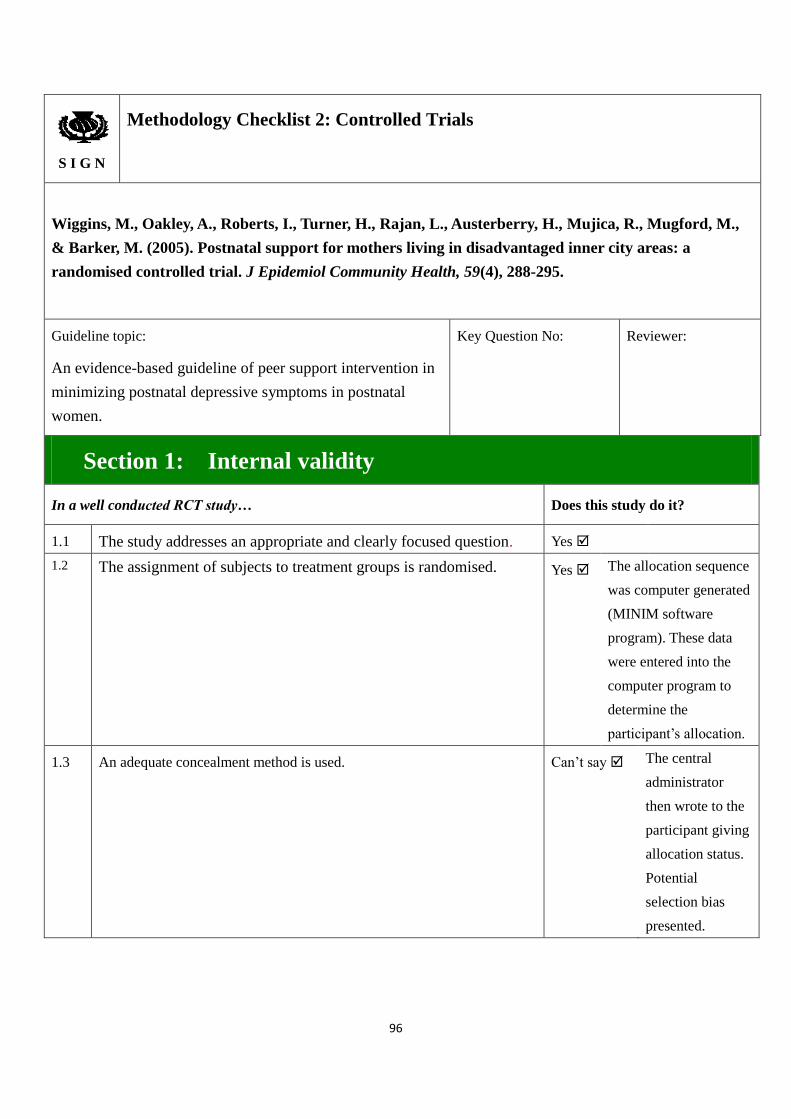
96
S I G N
Methodology Checklist 2: Controlled Trials
Wiggins, M., Oakley, A., Roberts, I., Turner, H., Rajan, L., Austerberry, H., Mujica, R., Mugford, M.,
& Barker, M. (2005). Postnatal support for mothers living in disadvantaged inner city areas: a
randomised controlled trial. J Epidemiol Community Health, 59(4), 288-295.
Guideline topic:
An evidence-based guideline of peer support intervention in
minimizing postnatal depressive symptoms in postnatal
women.
Key Question No: Reviewer:
Section 1: Internal validity
In a well conducted RCT study… Does this study do it?
1.1 The study addresses an appropriate and clearly focused question. Yes
1.2 The assignment of subjects to treatment groups is randomised. Yes The allocation sequence
was computer generated
(MINIM software
program). These data
were entered into the
computer program to
determine the
participant’s allocation.
1.3 An adequate concealment method is used.
Can’t say The central
administrator
then wrote to the
participant giving
allocation status.
Potential
selection bias
presented.

97
1.4 Subjects and investigators are kept ‘blind’ about treatment allocation. Yes Because of the nature of
the interventions, it was
not possible for either
the trial participants or
the researchers to be
blinded to group
allocation. Data entry
staff were blind to
allocation at the second
follow up.
1.5 The treatment and control groups are similar at the start of the trial. Yes Baseline characteristics
of participants are
similar.
1.6 The only difference between groups is the treatment under investigation. Yes
1.7 All relevant outcomes are measured in a standard, valid and reliable way. Yes
1.8 What percentage of the individuals or clusters recruited into each
treatment arm of the study dropped out before the study was completed?
At 1st FU (12 months):
Dropout rate:
SHV: 10%
CGS: 11%
Control: 10%
At 2nd
FU (18 months):
Dropout rate:
SHV: 18%
CGS: 15%
Control: 20%
1.9 All the subjects are analysed in the groups to which they were randomly
allocated (often referred to as intention to treat analysis).
Yes Analysis was carried
out on an intention to
treat basis.
1.10 Where the study is carried out at more than one site, results are
comparable for all sites.
Does not apply
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise bias?
Code as follows:
Acceptable (+)
2.2 Taking into account clinical considerations, your
evaluation of the methodology used, and the
Taking into account the clinical methodology used and
statistical power of the study, the overall effect is due

98
statistical power of the study, are you certain that the
overall effect is due to the study intervention?
to the study intervention.
2.3 Are the results of this study directly applicable to the
patient group targeted by this guideline?
Yes
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment of the study, and the
extent to which it answers your question and mention any areas of uncertainty raised above.
Author’s conclusions: Strengths of this trial included that allocation was well concealed, potential
confounders were balanced in randomization, an intention to treat analysis was carried out, and
outcome data were collected for 90% of the randomized participants.
At 12 and 18 months, there was little impact for either intervention on maternal depression (SHV:
0.86; 0.62 to1.19, CGS: 0.93; 0.69 to 1.27). Uptake of CGS intervention was low (only only 35
participants out of 184 received supports offered) due to the possibility of that such intervention was
inappropriate for mothers living in disadvantaged inner city areas who percept the service offered as
personally or culturally inappropriate or unnecessary.
Own comment: The CGS intervention mainly provides supports to mothers in different forms (e.g.
home visiting and/or telephone support) while the SHV intervention provides home supports given by
health professionals. The non-significant result might be affected due to long intervention period (18
months) and high dropout of participants. However, the intervention of Community Group Support
provided by community supporters did show an effect in reducing depression in mothers, and
therefore, it was still considered clinically significant.
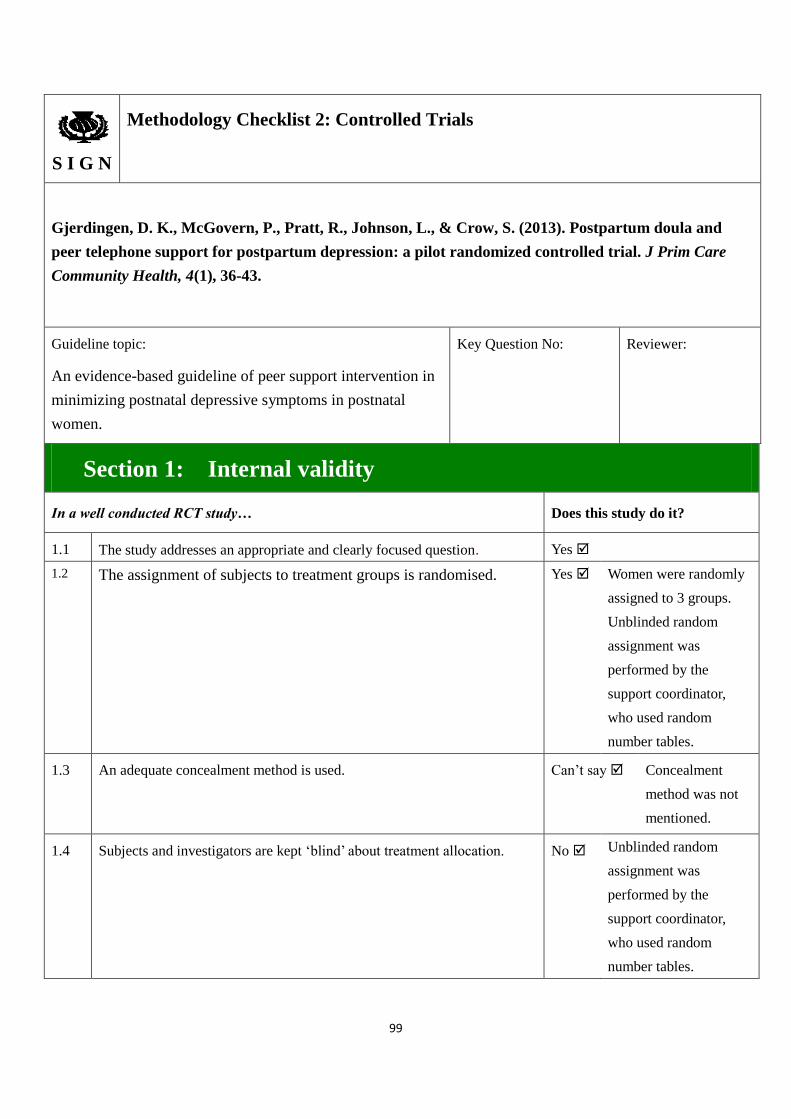
99
S I G N
Methodology Checklist 2: Controlled Trials
Gjerdingen, D. K., McGovern, P., Pratt, R., Johnson, L., & Crow, S. (2013). Postpartum doula and
peer telephone support for postpartum depression: a pilot randomized controlled trial. J Prim Care
Community Health, 4(1), 36-43.
Guideline topic:
An evidence-based guideline of peer support intervention in
minimizing postnatal depressive symptoms in postnatal
women.
Key Question No: Reviewer:
Section 1: Internal validity
In a well conducted RCT study… Does this study do it?
1.1 The study addresses an appropriate and clearly focused question. Yes
1.2 The assignment of subjects to treatment groups is randomised.
Yes Women were randomly
assigned to 3 groups.
Unblinded random
assignment was
performed by the
support coordinator,
who used random
number tables.
1.3 An adequate concealment method is used. Can’t say Concealment
method was not
mentioned.
1.4 Subjects and investigators are kept ‘blind’ about treatment allocation. No Unblinded random
assignment was
performed by the
support coordinator,
who used random
number tables.

100
1.5 The treatment and control groups are similar at the start of the trial. No Baseline demographic
and selected health
characteristics
categorized by group
assignment reveal that a
higher percentage of
women in the
postpartum doula group
had a previous history
of depression. There
were also trends for
more current depression
and a lower health state
among women in the
postpartum doula group,
and a higher level of
education among
controls.
1.6 The only difference between groups is the treatment under investigation. No Baseline demographics
and depression rates are
different.
1.7 All relevant outcomes are measured in a standard, valid and reliable way. Yes
1.8 What percentage of the individuals or clusters recruited into each
treatment arm of the study dropped out before the study was completed?
Of the 39 enrolled mothers, 2
dropped out after the initial
survey, 1 (8.3%) from the
postpartum doula group and 1
(7.7%) from the peer telephone
support group.
1.9 All the subjects are analysed in the groups to which they were randomly
allocated (often referred to as intention to treat analysis).
Yes Results are analyzed
using intent-to-treat
analysis.
1.10 Where the study is carried out at more than one site, results are
comparable for all sites.
Does not apply
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise bias?
Code as follows:1
Acceptable (+)

101
2.2 Taking into account clinical considerations, your
evaluation of the methodology used, and the
statistical power of the study, are you certain that the
overall effect is due to the study intervention?
Taking into account clinical considerations, evaluation
of the methodology used and the statistical power of
the study, the overall effect was due to the study
intervention.
2.3 Are the results of this study directly applicable to the
patient group targeted by this guideline?
Yes
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment of the study, and the
extent to which it answers your question and mention any areas of uncertainty raised above.
Author’s conclusion: At 6 months, the postpartum doula group had a higher proportion of women
who were currently depressed (82% vs 21% to 64%; P = .008) and currently receiving depression
treatment (100% vs 25% to 50%; P = .019); in addition, their duration of depression treatment was
longer (24 weeks vs 9-12 weeks, P = .003). There were no significant group differences in CES-D
scores, general health, or social support at 6 months. The changes in CES-D depression scores for
doula, telephone support, and control groups at 6 month follow-up are −16.3, −14.5, and −10.1
respectively. (P = .397).
It is feasible to recruit postpartum doulas, peer telephone supporters, and mothers with depressive
symptoms for a peer support intervention though recruitment efforts for this particular study required
a broad, multifaceted approach.
Own comments: Due to the differences in baseline characteristics of mothers of in the Doulas Group
who had a larger percentage of depression history, presence of allocation bias and small sample size,
a non-significant result was obtained in the study. However, when comparing the CES-D depression
scores of the 3 study groups, there was consistently a reduction in the total scores of the 3 groups,
including the peer telephone support group. Its clinical significance for peer telephone support in
reducing depression score in postnatal women was still considered effective.
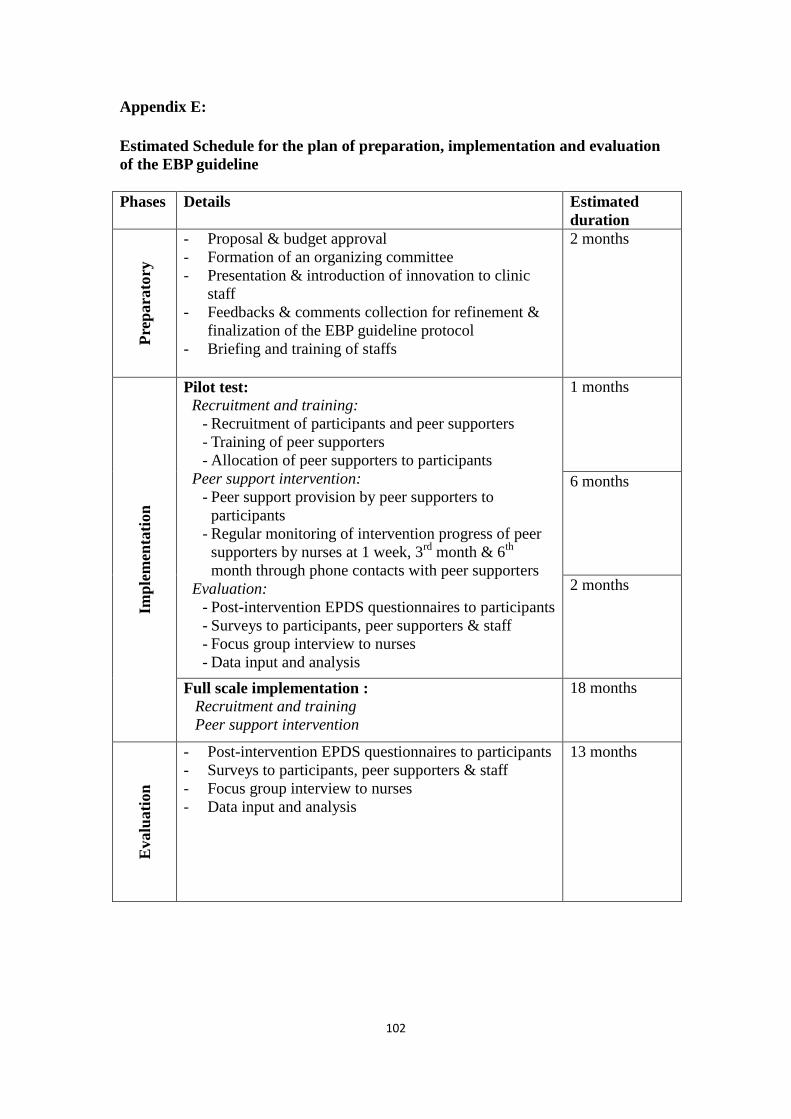
102
Appendix E:
Estimated Schedule for the plan of preparation, implementation and evaluation
of the EBP guideline
Phases Details Estimated
duration
Pre
para
tory
- Proposal & budget approval
- Formation of an organizing committee
- Presentation & introduction of innovation to clinic
staff
- Feedbacks & comments collection for refinement &
finalization of the EBP guideline protocol
- Briefing and training of staffs
2 months
Imp
lem
enta
tion
Pilot test:
Recruitment and training:
- Recruitment of participants and peer supporters
- Training of peer supporters
- Allocation of peer supporters to participants
Peer support intervention:
- Peer support provision by peer supporters to
participants
- Regular monitoring of intervention progress of peer
supporters by nurses at 1 week, 3rd
month & 6th
month through phone contacts with peer supporters
Evaluation:
- Post-intervention EPDS questionnaires to participants
- Surveys to participants, peer supporters & staff
- Focus group interview to nurses
- Data input and analysis
1 months
6 months
2 months
Full scale implementation :
Recruitment and training
Peer support intervention
18 months
Evalu
ati
on
- Post-intervention EPDS questionnaires to participants
- Surveys to participants, peer supporters & staff
- Focus group interview to nurses
- Data input and analysis
13 months

103
Appendix E (continued):
Gantt chart for the plan of preparation, implementation and evaluation of the Guideline
Phase Month
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31
Pre
para
tory
Proposal & budget approval
Formation of an organizing committee
Feedbacks & comments collection
Briefing and training of staffs
Imp
lem
enta
tion
Pil
ot
test
Sta
ges
1st: Recruitment & training
2nd
: Peer support intervention 6 months
3rd
: Evaluation 2
months
Fu
ll s
cale
imp
lem
enta
tion
Recruitment & training of
participants and peer
supporters
12 months
Peer support intervention 17 months
Evalu
ati
on
Post EPDS questionnaires
Surveys to participants, peer supporters
& staff
Focus group interview
Data input and analysis
13 months
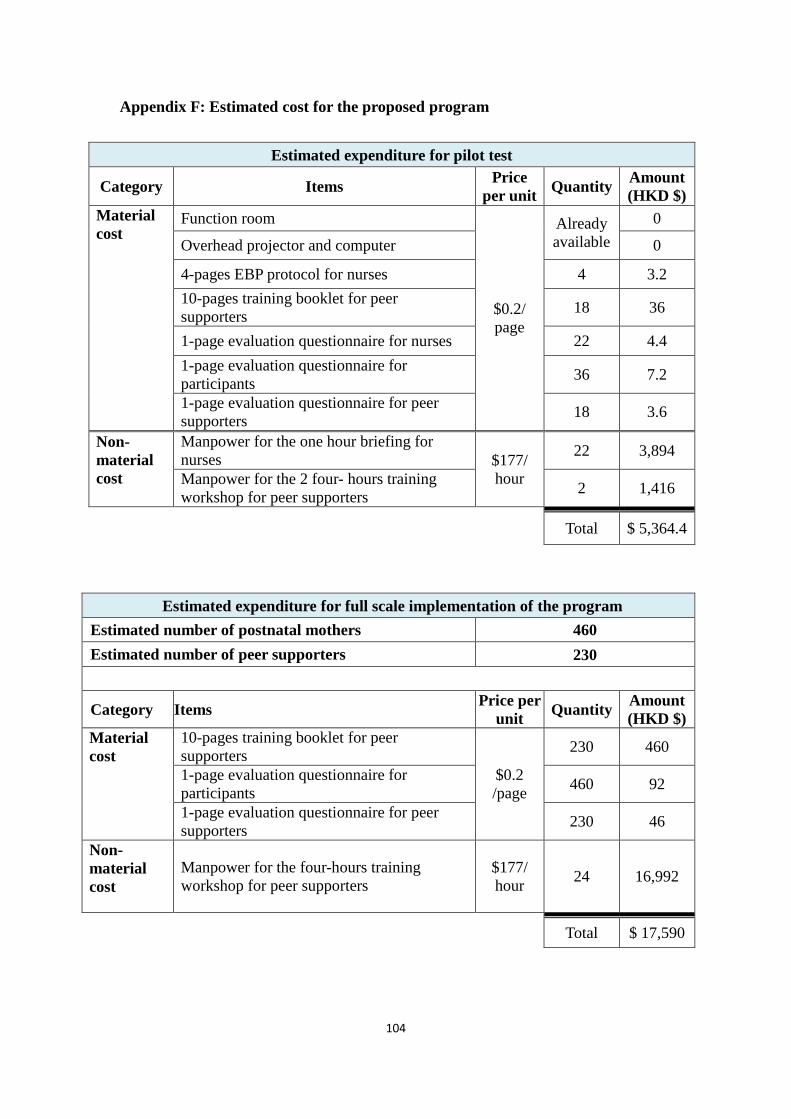
104
Appendix F: Estimated cost for the proposed program
Estimated expenditure for pilot test
Category Items Price
per unit Quantity
Amount
(HKD $)
Material
cost Function room
$0.2/
page
Already
available
0
Overhead projector and computer 0
4-pages EBP protocol for nurses 4 3.2
10-pages training booklet for peer
supporters 18 36
1-page evaluation questionnaire for nurses 22 4.4
1-page evaluation questionnaire for
participants 36 7.2
1-page evaluation questionnaire for peer
supporters 18 3.6
Non-
material
cost
Manpower for the one hour briefing for
nurses $177/
hour
22 3,894
Manpower for the 2 four- hours training
workshop for peer supporters 2 1,416
Total $ 5,364.4
Estimated expenditure for full scale implementation of the program
Estimated number of postnatal mothers 460
Estimated number of peer supporters 230
Category Items Price per
unit Quantity
Amount
(HKD $)
Material
cost
10-pages training booklet for peer
supporters
$0.2
/page
230 460
1-page evaluation questionnaire for
participants 460 92
1-page evaluation questionnaire for peer
supporters 230 46
Non-
material
cost
Manpower for the four-hours training
workshop for peer supporters
$177/
hour 24 16,992
Total $ 17,590
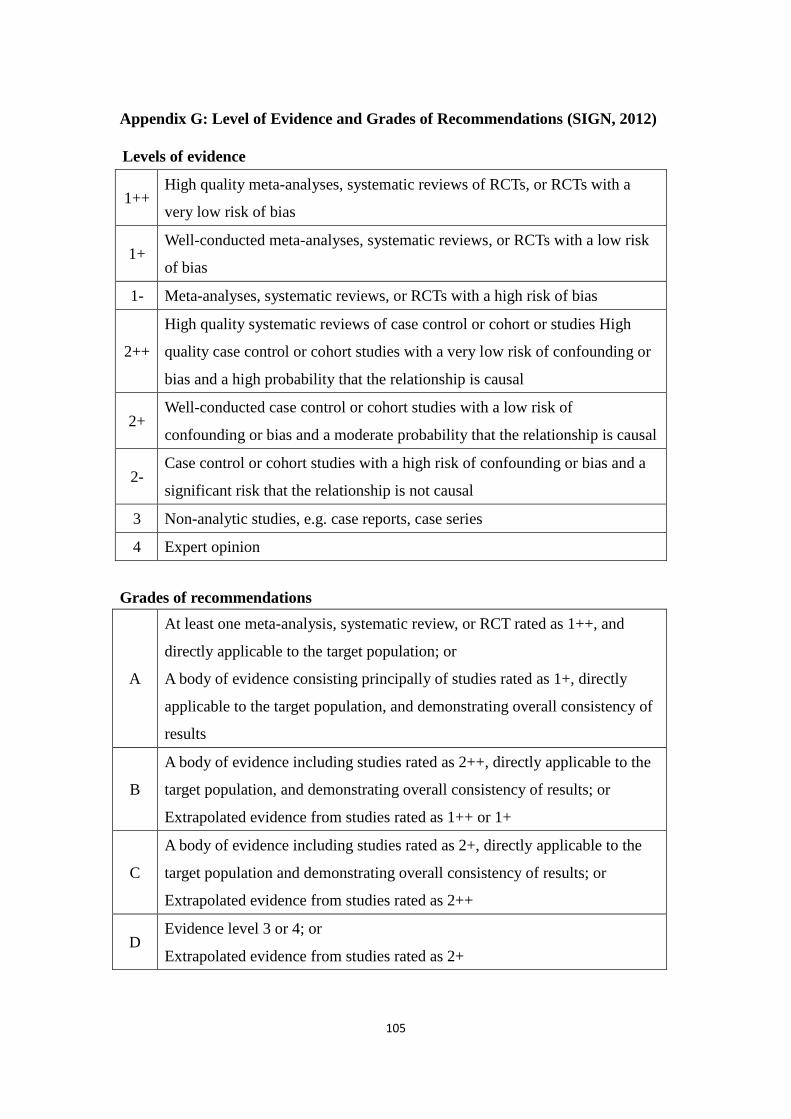
105
Appendix G: Level of Evidence and Grades of Recommendations (SIGN, 2012)
Levels of evidence
1++ High quality meta-analyses, systematic reviews of RCTs, or RCTs with a
very low risk of bias
1+ Well-conducted meta-analyses, systematic reviews, or RCTs with a low risk
of bias
1- Meta-analyses, systematic reviews, or RCTs with a high risk of bias
2++
High quality systematic reviews of case control or cohort or studies High
quality case control or cohort studies with a very low risk of confounding or
bias and a high probability that the relationship is causal
2+ Well-conducted case control or cohort studies with a low risk of
confounding or bias and a moderate probability that the relationship is causal
2- Case control or cohort studies with a high risk of confounding or bias and a
significant risk that the relationship is not causal
3 Non-analytic studies, e.g. case reports, case series
4 Expert opinion
Grades of recommendations
A
At least one meta-analysis, systematic review, or RCT rated as 1++, and
directly applicable to the target population; or
A body of evidence consisting principally of studies rated as 1+, directly
applicable to the target population, and demonstrating overall consistency of
results
B
A body of evidence including studies rated as 2++, directly applicable to the
target population, and demonstrating overall consistency of results; or
Extrapolated evidence from studies rated as 1++ or 1+
C
A body of evidence including studies rated as 2+, directly applicable to the
target population and demonstrating overall consistency of results; or
Extrapolated evidence from studies rated as 2++
D Evidence level 3 or 4; or
Extrapolated evidence from studies rated as 2+
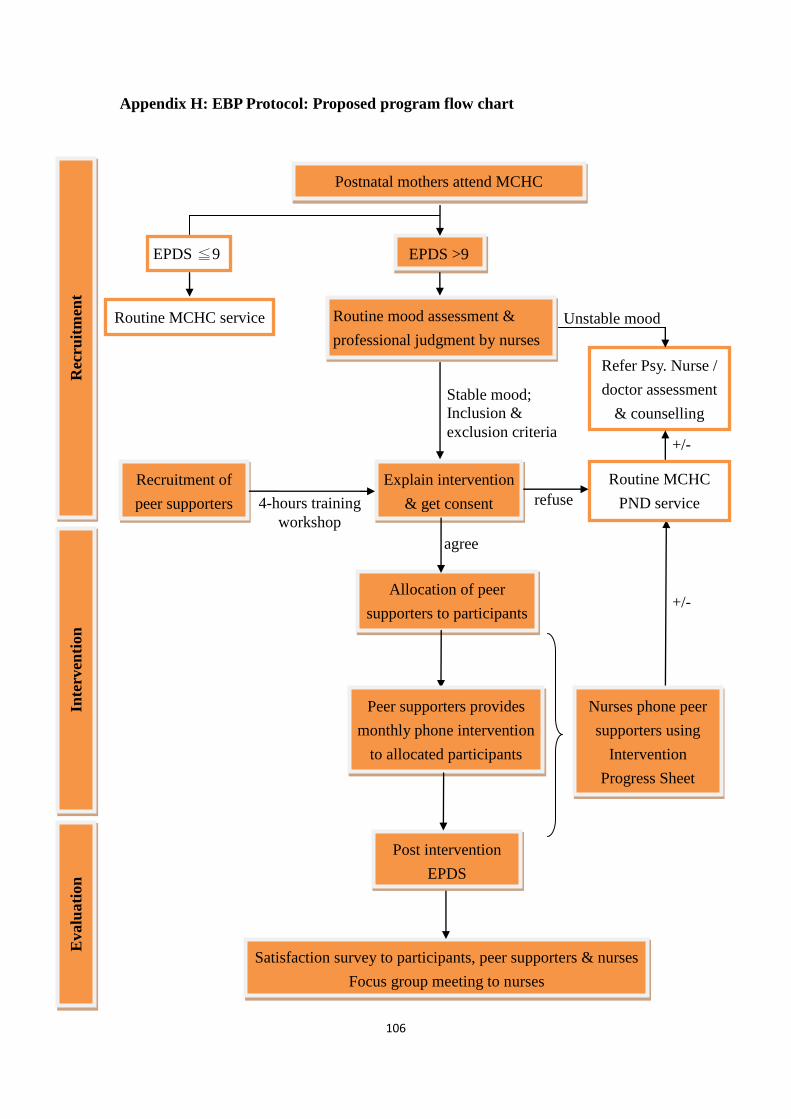
106
Appendix H: EBP Protocol: Proposed program flow chart
refuse
Rec
ruit
men
t In
terv
enti
on
E
valu
ati
on
+/
Postnatal mothers attend MCHC
EPDS ≦9 EPDS >9
Explain intervention
& get consent
Stable mood;
Inclusion &
exclusion criteria
Routine MCHC
PND service
Refer Psy. Nurse /
doctor assessment
& counselling
agree
Allocation of peer
supporters to participants
Recruitment of
peer supporters
Routine MCHC service
4-hours training
workshop
Nurses phone peer
supporters using
Intervention
Progress Sheet
Post intervention
EPDS
Satisfaction survey to participants, peer supporters & nurses
Focus group meeting to nurses
Routine mood assessment &
professional judgment by nurses
Unstable mood
+/
Peer supporters provides
monthly phone intervention
to allocated participants

107
Appendix I: Intervention Progress Sheet for nurses to monitor progress of telephone contacts by peer supporters to postnatal mothers
Pair Subject Names Intervention details
Regular phone contacts by nurses
1st FU
(1 week)
2nd
FU
(3rd
month)
3rd
FU
(6th
month) prn FU
1 Peer supporter:
______________
Contact no.:
______________
Participant:
______________
Are you able to contact the allocated participant?
How many contacts been made till the moment?
Details of supporting services being given:
Any problems encountered?
2 Peer supporter:
______________
Contact no.:
______________
Participant:
______________
Are you able to contact the allocated participant?
How many contacts been made till the moment?
Details of supporting services being given:
Any problems encountered?
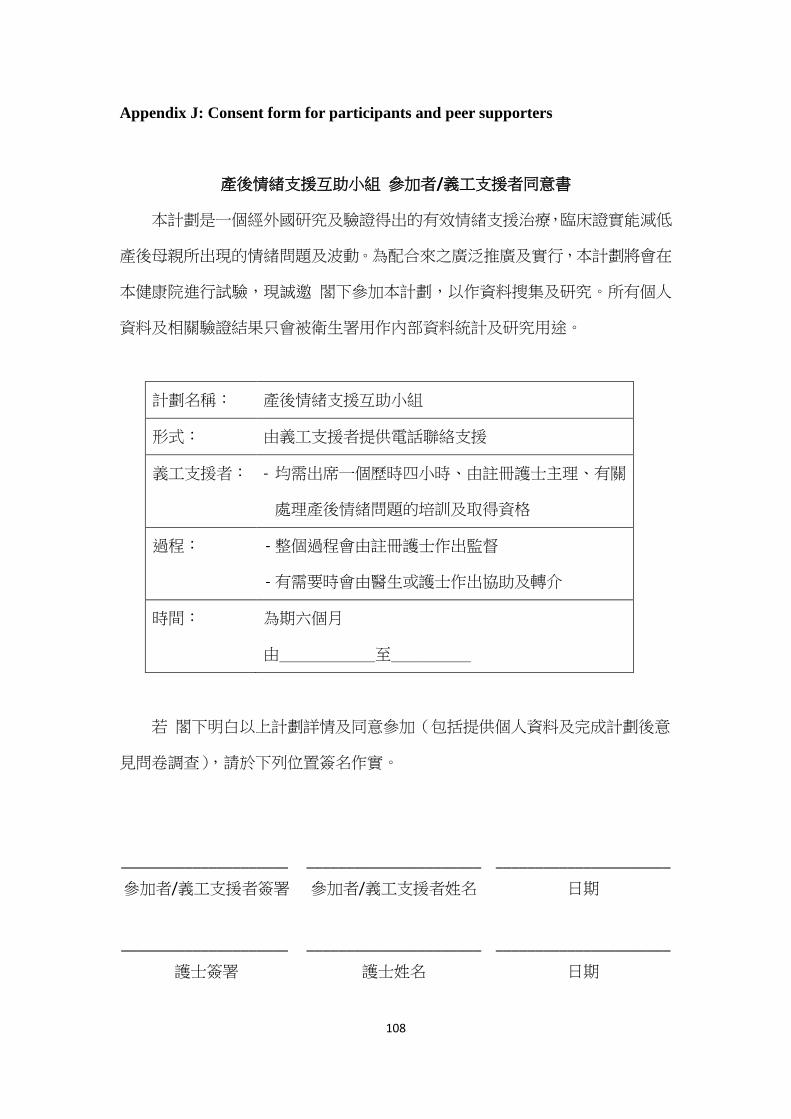
108
Appendix J: Consent form for participants and peer supporters
產後情緒支援互助小組 參加者/義工支援者同意書
本計劃是一個經外國研究及驗證得出的有效情緒支援治療,臨床證實能減低
產後母親所出現的情緒問題及波動。為配合來之廣泛推廣及實行,本計劃將會在
本健康院進行試驗,現誠邀 閣下參加本計劃,以作資料搜集及研究。所有個人
資料及相關驗證結果只會被衛生署用作內部資料統計及研究用途。
計劃名稱: 產後情緒支援互助小組
形式: 由義工支援者提供電話聯絡支援
義工支援者: - 均需出席一個歷時四小時、由註冊護士主理、有關
處理產後情緒問題的培訓及取得資格
過程: - 整個過程會由註冊護士作出監督
- 有需要時會由醫生或護士作出協助及轉介
時間: 為期六個月
由______至_____
若 閣下明白以上計劃詳情及同意參加(包括提供個人資料及完成計劃後意
見問卷調查),請於下列位置簽名作實。
_____________________ ______________________ ______________________
參加者/義工支援者簽署 參加者/義工支援者姓名 日期
_____________________ ______________________ ______________________
護士簽署 護士姓名 日期
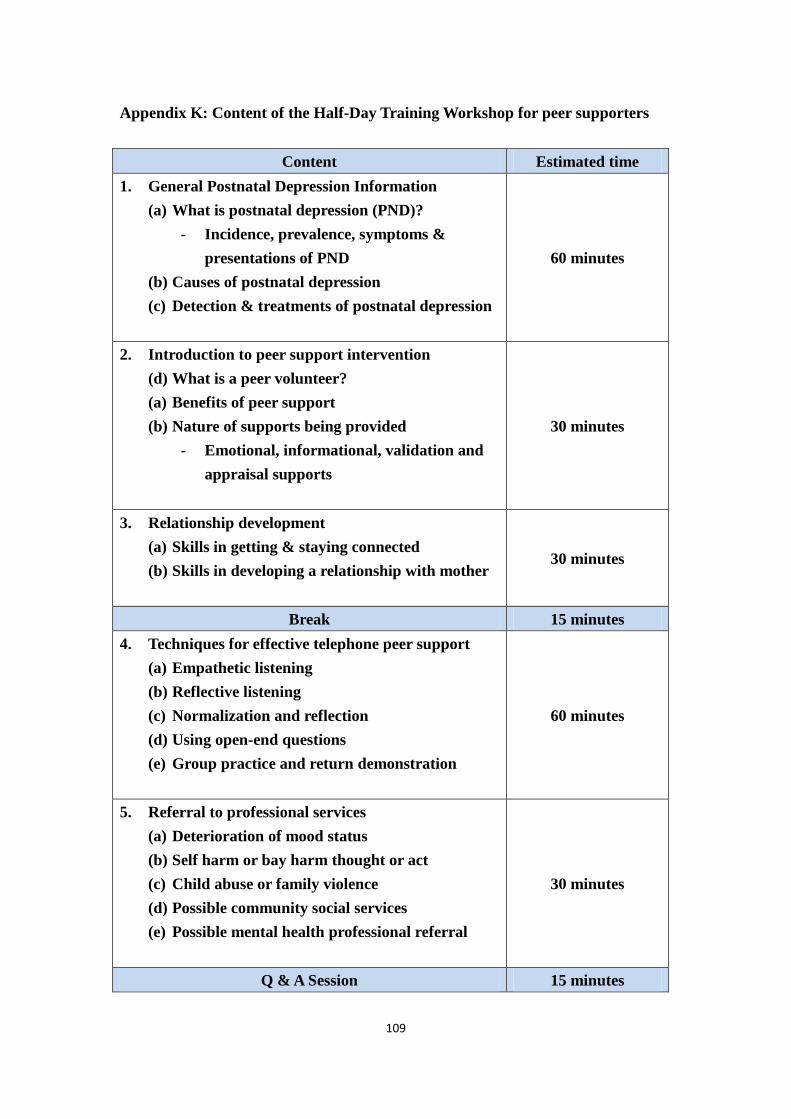
109
Appendix K: Content of the Half-Day Training Workshop for peer supporters
Content Estimated time
1. General Postnatal Depression Information
(a) What is postnatal depression (PND)?
- Incidence, prevalence, symptoms &
presentations of PND
(b) Causes of postnatal depression
(c) Detection & treatments of postnatal depression
60 minutes
2. Introduction to peer support intervention
(d) What is a peer volunteer?
(a) Benefits of peer support
(b) Nature of supports being provided
- Emotional, informational, validation and
appraisal supports
30 minutes
3. Relationship development
(a) Skills in getting & staying connected
(b) Skills in developing a relationship with mother
30 minutes
Break 15 minutes
4. Techniques for effective telephone peer support
(a) Empathetic listening
(b) Reflective listening
(c) Normalization and reflection
(d) Using open-end questions
(e) Group practice and return demonstration
60 minutes
5. Referral to professional services
(a) Deterioration of mood status
(b) Self harm or bay harm thought or act
(c) Child abuse or family violence
(d) Possible community social services
(e) Possible mental health professional referral
30 minutes
Q & A Session 15 minutes
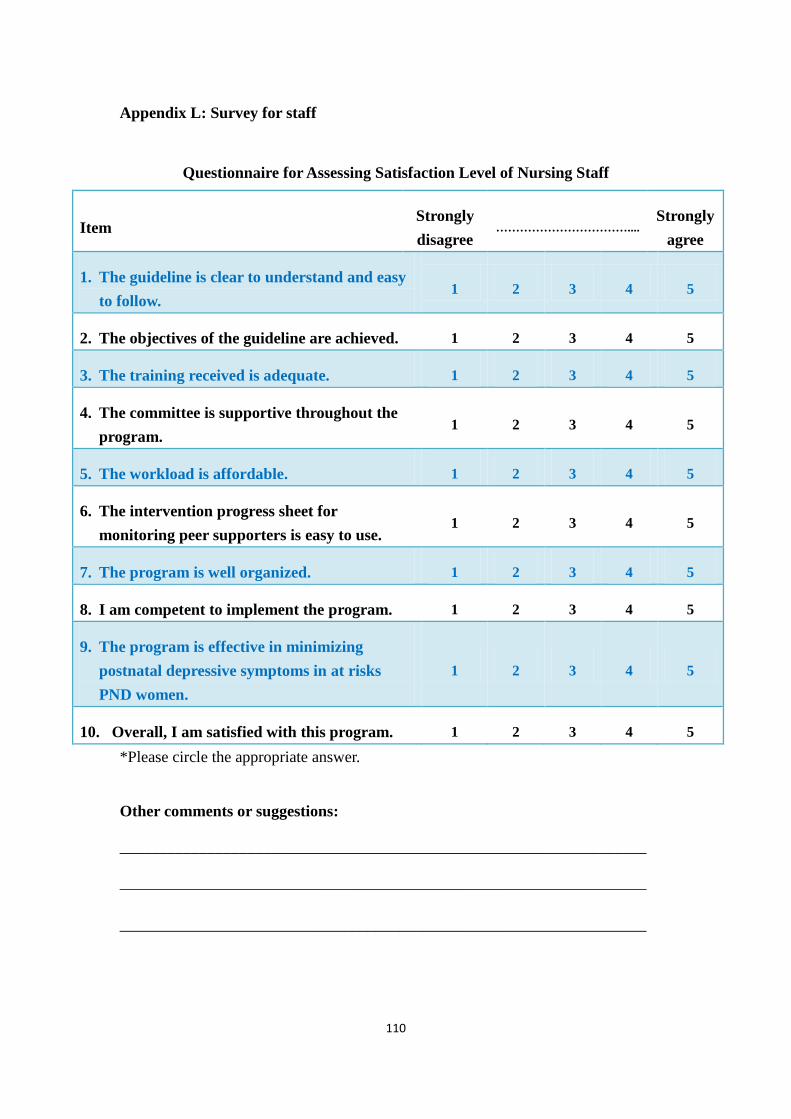
110
Appendix L: Survey for staff
Questionnaire for Assessing Satisfaction Level of Nursing Staff
Item Strongly
disagree ……………………………....
Strongly
agree
1. The guideline is clear to understand and easy
to follow. 1 2 3 4 5
2. The objectives of the guideline are achieved. 1 2 3 4 5
3. The training received is adequate. 1 2 3 4 5
4. The committee is supportive throughout the
program. 1 2 3 4 5
5. The workload is affordable. 1 2 3 4 5
6. The intervention progress sheet for
monitoring peer supporters is easy to use. 1 2 3 4 5
7. The program is well organized. 1 2 3 4 5
8. I am competent to implement the program. 1 2 3 4 5
9. The program is effective in minimizing
postnatal depressive symptoms in at risks
PND women.
1 2 3 4 5
10. Overall, I am satisfied with this program. 1 2 3 4 5
*Please circle the appropriate answer.
Other comments or suggestions:
__________________________________________________________________
__________________________________________________________________
__________________________________________________________________

111
Appendix M: Survey for participants
Questionnaire for Assessing Satisfaction Level of Participants
母嬰健康院 – 產後情緒支援互助小組計劃 參加者滿意度問卷調查
項目
關於計劃內容 非常不同意 ………………………………… 非常同意
1. 計劃前護士講解清晰詳盡。 1 2 3 4 5
2. 計劃流程安排暢順明確。 1 2 3 4 5
3. 電話支援互助形式方便有效。 1 2 3 4 5
4. 計劃能幫助我處理或減輕產後情緒問題。 1 2 3 4 5
關於義工支援者 非常不同意 ………………………………… 非常同意
5. 我能夠方便地聯絡到我的義工支援者。 1 2 3 4 5
6. 義工支援者能提供足夠次數的電話聯絡。 1 2 3 4 5
7. 義工支援者所提供的支援切合我的需要。 1 2 3 4 5
8. 我對我的義工支援者感到滿意。 1 2 3 4 5
整體 非常不同意 ………………………………… 非常同意
9. 我對產後情緒支援互助小組計劃感到滿意。 1 2 3 4 5
10. 我會將此計劃推薦給其他產後母親。 1 2 3 4 5
*請圈上適當答案
其它意見:
__________________________________________________________________
__________________________________________________________________
__________________________________________________________________

112
Appendix N: Survey for peer supporters
Questionnaire for Assessing Satisfaction Level of Participants
母嬰健康院 – 產後情緒支援互助小組計劃 義工支援者滿意度問卷調查
項目
關於計劃內容 非常不同意 ……………………………… 非常同意
1. 計劃前護士講解清晰詳盡。 1 2 3 4 5
2. 計劃流程安排暢順明確。 1 2 3 4 5
3. 計劃前培訓內容足夠清晰。 1 2 3 4 5
4. 計劃其間護士能提供適當支持。 1 2 3 4 5
5. 電話支援互助形式方便有效。 1 2 3 4 5
6. 計劃能處理或減輕參加者的產後情緒問題。 1 2 3 4 5
關於參加者 非常不同意 ……………………………… 非常同意
7. 我能夠方便地聯絡到我的產後母親。 1 2 3 4 5
8. 我能夠提供參加者所需的支援。 1 2 3 4 5
整體 非常不同意 ……………………………… 非常同意
9. 我對產後情緒支援互助小組計劃感到滿意。 1 2 3 4 5
10. 我會將此計劃推薦給其他產後母親。 1 2 3 4 5
*請圈上適當答案
其它意見:
__________________________________________________________________
__________________________________________________________________
__________________________________________________________________

113
References
Almond, P. (2009). Postnatal depression: a global public health perspective. Perspect
Public Health, 129(5), 221-227.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental
disorders, 5th
edition. Washington, DC: Author.
Campbell, R., Starkey, F., Holliday, J., Audrey, S., Bloor, M., Parry-Langdon, N.,
Hughes, R., & Moore, L. (2008). An informal school-based peer-led
intervention for smoking prevention in adolescence (ASSIST): a cluster
randomised trial. Lancet, 371(9624), 1595-1602. doi:
10.1016/s0140-6736(08)60692-3
Chan, J. C., Sui, Y., Oldenburg, B., Zhang, Y., Chung, H. H., Goggins, W., Au, S.,
Brown, N., Ozaki, R., Wong, R. Y., Ko, G. T., & Fisher, E. (2014). Effects of
telephone-based peer support in patients with type 2 diabetes mellitus
receiving integrated care: a randomized clinical trial. The Journal of American
Medical Association Internal Medicine, 174(6), 972-981. doi:
10.1001/jamainternmed.2014.655
Chen, C. H., Tseng, Y. F., Chou, F. H., & Wang, S. Y. (2000). Effects of support group
intervention in postnatally distressed women. A controlled study in Taiwan.
Journal of Psychosomatic Research, 49(6), 395-399.
Chen, C. M., Kuo, S. F., Chou, Y. H., & Chen, H. C. (2007). Postpartum Taiwanese
women: their postpartum depression, social support and health-promoting
lifestyle profiles. Journal of Clinical Nursing, 16(8), 1550-1560. doi:
10.1111/j.1365-2702.2006.01837.x
Chen, H., Bautista, D., Ch'ng, Y. C., Li, W., Chan, E., & Rush, A. J. (2013). Screening
for postnatal depression in Chinese-speaking women using the Hong Kong
translated version of the Edinburgh Postnatal Depression Scale. Asia Pacific
Psychiatry, 5(2), E64-72. doi: 10.1111/appy.12080
Civic, D., & Holt, V. L. (2000). Maternal depressive symptoms and child behavior
problems in a nationally representative normal birthweight sample. Maternal
and Child Health Journal, 4(4), 215-221.

114
Cox, J.L., Holden, J.M., & Sagovsky, R. (1987) Detection of postnatal depression:
development of the 10-item Edinburgh Postnatal Depression Scale. British
Journal of Psychiatry, 150, 782-786.
Dagher, R. K., McGovern, P. M., Dowd, B. E., & Gjerdingen, D. K. (2012).
Postpartum depression and health services expenditures among employed
women. Journal of Occupational and Environmental Medicine, 54(2),
210-215. doi: 10.1097/JOM.0b013e31823fdf85
DeAndrea, D. C., & Anthony, J. C. (2013). Online peer support for mental health
problems in the United States: 2004-2010. Psychological Medicine, 43(11),
2277-2288. doi: 10.1017/s0033291713000172
Department of Health, Family Health Service. (2012). Evaluation Report of
Comprehensive Child Development Service (CCDS). Retrieved August 30,
2014 from http://www.fhs.gov.hk/english/reports/files/ccds_exsummary.pdf
Department of Health. (2013). Postnatal Depression Report. Disclose approval letter
in Appendix A.
Department of Health, Family Health Service. (2014). Health Information – Child
Health. Retrieved August 30, 2014 from
http://www.fhs.gov.hk/english/health_info/class_life/child/child_tsy_child_d1
0.html
Dennis, C. L. (2003). The effect of peer support on postpartum depression: a pilot
randomized controlled trial. Canadian Journal of Psychiatry, 48(2), 115-124.
Dennis, C. L. (2014). Psychosocial interventions for the treatment of perinatal
depression. Best Practice & Research Clinical Obstetric & Gynaecology,
28(1), 97-111. doi: 10.1016/j.bpobgyn.2013.08.008
Dennis, C. L., & Dowswell, T. (2013). Psychosocial and psychological interventions
for preventing postpartum depression. Cochrane Database Systematic Reviews,
2, Cd001134. doi: 10.1002/14651858.CD001134.pub3
Dennis, C. L., Hodnett, E., Kenton, L., Weston, J., Zupancic, J., Stewart, D. E., &
Kiss, A. (2009). Effect of peer support on prevention of postnatal depression
115
among high risk women: multisite randomised controlled trial. British Medical
Journal, 338, a3064. doi: 10.1136/bmj.a3064
Dukhovny, D., Dennis, C. L., Hodnett, E., Weston, J., Stewart, D. E., Mao, W., &
Zupancic, J. A. (2013). Prospective economic evaluation of a peer support
intervention for prevention of postpartum depression among high-risk women
in Ontario, Canada. American Journal of Perinatology, 30(8), 631-642. doi:
10.1055/s-0032-1331029
Durukan, E., Ilhan, M. N., Bumin, M. A., & Aycan, S. (2011). Postpartum Depression
Frequency and Quality of Life Among a Group of Mothers Having a Child
Aged 2 Weeks-18 Months. Balkan Medical Journal, 28: 385-393.doi:
10.5174/tutfd.2010.04117.3
Family Health Service, Department of Health. (2014). Vision, Mission and Values.
Retrieved November 25, 2014, from
http://www.fhs.gov.hk/english/about_us/vision/vision.html
Field, T. (2010). Postpartum depression effects on early interactions, parenting, and
safety practices: a review. Infant Behaviour and Development, 33(1), 1-6. doi:
10.1016/j.infbeh.2009.10.005
Fisher, J., Cabral de Mello, M., Patel, V., Rahman, A., Tran, T., Holton, S., & Holmes,
W. (2012). Prevalence and determinants of common perinatal mental disorders
in women in low- and lower-middle-income countries: a systematic review.
Bull World Health Organization, 90(2), 139g-149g. doi:
10.2471/blt.11.091850
Gavin, N. I., Gaynes, B. N., Lohr, K. N., Meltzer-Brody, S., Gartlehner, G., &
Swinson, T. (2005). Perinatal depression: a systematic review of prevalence
and incidence. Obstetric Gynecology, 106(5 Pt 1), 1071-1083. doi:
10.1097/01.AOG.0000183597.31630.db
Gawlik, S., Muller, M., Hoffmann, L., Dienes, A., Wallwiener, M., Sohn, C., Schlehe,
B., & Reck, C. (2014). Prevalence of paternal perinatal depressiveness and its
link to partnership satisfaction and birth concerns. Archieves of Women’s
Mental Health, 17(1), 49-56. doi: 10.1007/s00737-013-0377-4

116
Gjerdingen, D. K., McGovern, P., Pratt, R., Johnson, L., & Crow, S. (2013).
Postpartum doula and peer telephone support for postpartum depression: a
pilot randomized controlled trial. Journal of Primary Care Community Health,
4(1), 36-43. doi: 10.1177/2150131912451598
Glavin, K., & Leahy-Warren, P. (2013). Postnatal depression is a public health nursing
issue: perspectives from norway and ireland. Nursing Research & Practice,
2013, 813409. doi: 10.1155/2013/813409
Goodman, J. H. (2004). Paternal postpartum depression, its relationship to maternal
postpartum depression, and implications for family health. Journal of
Advanced Nursing, 45(1), 26-35.
Goodman, S. H., Rouse, M. H., Connell, A. M., Broth, M. R., Hall, C. M., &
Heyward, D. (2011). Maternal depression and child psychopathology: a
meta-analytic review. Clinical Child & Family Psychology Review, 14(1), 1-27.
doi: 10.1007/s10567-010-0080-1
Gress-Smith, J. L., Luecken, L. J., Lemery-Chalfant, K., & Howe, R. (2012).
Postpartum depression prevalence and impact on infant health, weight, and
sleep in low-income and ethnic minority women and infants. Maternal &
Child Health Journal, 16(4), 887-893. doi: 10.1007/s10995-011-0812-y
Grigoriadis, S., VonderPorten, E. H., Mamisashvili, L., Tomlinson, G., Dennis, C. L.,
Koren, G., Steiner, M., Mousmanis, P., Cheung, A., Radford, K., Martinovic,
J., & Ross, L. E. (2013). The impact of maternal depression during pregnancy
on perinatal outcomes: a systematic review and meta-analysis. Journal of
Clinical Psychiatry, 74(4), e321-341. doi: 10.4088/JCP.12r07968
Hickey, D., Carr, A., Dooley, B., Guerin, S., Butler, E., & Fitzpatrick, L. (2005).
Family and marital profiles of couples in which one partner has depression or
anxiety. Journal of Marital & Family Therapy, 31(2), 171-182.
Ingersoll. G.L. (2005). Generating evidence through outcomes management. In
Melnyk, B., & Fineout-Overholt, E. (Eds). Evidence-based practice practice
in nursing & healthcare: a guide to best practice (pp. 299-332). Philadelphia:
Lippincott Williams & Wilkins.

117
Kaunonen, M., Hannula, L., & Tarkka, M. T. (2012). A systematic review of peer
support interventions for breastfeeding. Journal of Clinical Nursing, 21(13-14),
1943-1954. doi: 10.1111/j.1365-2702.2012.04071.x
Kerstis, B., Engstrom, G., Edlund, B., & Aarts, C. (2013). Association between
mothers' and fathers' depressive symptoms, sense of coherence and perception
of their child's temperament in early parenthood in Sweden. Scandinavian
Journal of Public Health, 41(3), 233-239. doi: 10.1177/1403494812472006
Lau, Y., & Wong, D. F. (2008). The role of social support in helping Chinese women
with perinatal depressive symptoms cope with family conflict. Journal of
Obstetric, Gynecologic & Neonatal Nursing, 37(5), 556-571. doi:
10.1111/j.1552-6909.2008.00273.x
Leahy-Warren, P., McCarthy, G., & Corcoran, P. (2011). Postnatal depression in
first-time mothers: prevalence and relationships between functional and
structural social support at 6 and 12 weeks postpartum. Archives of Psychiatric
Nursing, 25(3), 174-184. doi: 10.1016/j.apnu.2010.08.005
Lee, D. T., Chan, S. S., Sahota, D. S., Yip, A. S., Tsui, M., & Chung, T. K. (2004). A
prevalence study of antenatal depression among Chinese women. Journal of
Affective Disorders, 82(1), 93-99. doi: 10.1016/j.jad.2003.10.003
Lee, D. T., Yip, S. K., Chiu, H. F., Leung, T. Y., Chan, K. P., Chau, I. O., Leung, H. C.,
& Chung, T. K. (1998). Detecting postnatal depression in Chinese women.
Validation of the Chinese version of the Edinburgh Postnatal Depression Scale.
British Journal of Psychiatry, 172, 433-437.
Lee, S. J., Taylor, C. A., & Bellamy, J. L. (2012). Paternal depression and risk for
child neglect in father-involved families of young children. Child Abuse &
Neglect, 36(5), 461-469. doi: 10.1016/j.chiabu.2012.04.002
Letourneau, N., Stewart, M., Dennis, C. L., Hegadoren, K., Duffett-Leger, L., &
Watson, B. (2011). Effect of home-based peer support on maternal-infant
interactions among women with postpartum depression: a randomized,
controlled trial. International Journal of Mental Health Nursing, 20(5),
345-357. doi: 10.1111/j.1447-0349.2010.00736.x
118
Leung, B. M., & Kaplan, B. J. (2009). Perinatal depression: prevalence, risks, and the
nutrition link--a review of the literature. Journal of American Dietetic
Association, 109(9), 1566-1575. doi: 10.1016/j.jada.2009.06.368
Leung, S. S., Leung, C., Lam, T. H., Hung, S. F., Chan, R., Yeung, T., Miao, M.,
Cheng, S., Leung, S. H., Lau, A. & Lee, D. T. (2011). Outcome of a postnatal
depression screening programme using the Edinburgh Postnatal Depression
Scale: a randomized controlled trial. Journal of Public Health (Oxford), 33(2),
292-301. doi: 10.1093/pubmed/fdq075
Leung, S. S., Martinson, I. M., & Arthur, D. (2005). Postpartum depression and
related psychosocial variables in Hong Kong Chinese women: findings from a
prospective study. Research in Nursing & Health, 28(1), 27-38. doi:
10.1002/nur.20053
Lindahl, V., Pearson, J. L., & Colpe, L. (2005). Prevalence of suicidality during
pregnancy and the postpartum. Archives for Women’s Mental Health, 8(2),
77-87. doi: 10.1007/s00737-005-0080-1
Lumley, J., Austin, M. P., & Mitchell, C. (2004). Intervening to reduce depression
after birth: a systematic review of the randomized trials. International Journal
of Technological Assessment in Health Care, 20(2), 128-144.
Mallikarjun, P. K., & Oyebode, F. (2005). Prevention of postnatal depression. Journal
of Royal Society for the Promotion of Health, 125(5), 221-226.
Mao, H. J., Li, H. J., Chiu, H., Chan, W. C., & Chen, S. L. (2012). Effectiveness of
antenatal emotional self-management training program in prevention of
postnatal depression in Chinese women. Perspectives in Psychiatric Care,
48(4), 218-224. doi: 10.1111/j.1744-6163.2012.00331.x
Mao, Q., Zhu, L. X., & Su, X. Y. (2011). A comparison of postnatal depression and
related factors between Chinese new mothers and fathers. Journal of Clinical
Nursing, 20(5-6), 645-652. doi: 10.1111/j.1365-2702.2010.03542.x
Melnyk, B.M. & Fineout-Overholt, E. (2011). Evidence-based Practice in Nursing
and Healthcare, a guide to best practice. 2nd. ed. Lippincott Williams &
Wilkins.

119
Milgrom, J., Schembri, C., Ericksen, J., Ross, J., & Gemmill, A. W. (2011). Towards
parenthood: an antenatal intervention to reduce depression, anxiety and
parenting difficulties. Journal of Affective Disorders, 130(3), 385-394. doi:
10.1016/j.jad.2010.10.045
Murray, L., Cooper, P. J., Wilson, A., & Romaniuk, H. (2003). Controlled trial of the
short- and long-term effect of psychological treatment of post-partum
depression: 2. Impact on the mother-child relationship and child outcome.
British Journal of Psychiatry, 182, 420-427.
O'Hara, M. W., & McCabe, J. E. (2013). Postpartum depression: current status and
future directions. Annual Review of Clinical Psychology, 9, 379-407. doi:
10.1146/annurev-clinpsy-050212-185612
Patel, M., Bailey, R. K., Jabeen, S., Ali, S., Barker, N. C., & Osiezagha, K. (2012).
Postpartum depression: a review. Journal of Health Care for the Poor &
Underserved, 23(2), 534-542. doi: 10.1353/hpu.2012.0037
Patel, V., DeSouza, N., & Rodrigues, M. (2003). Postnatal depression and infant
growth and development in low income countries: a cohort study from Goa,
India. Archives of Diseases in Childhood, 88(1), 34-37.
Paulson, J. F., & Bazemore, S. D. (2010). Prenatal and postpartum depression in
fathers and its association with maternal depression: a meta-analysis. Journal
of American Medical Association, 303(19), 1961-1969. doi:
10.1001/jama.2010.605
Paulson, J. F., Dauber, S., & Leiferman, J. A. (2006). Individual and combined effects
of postpartum depression in mothers and fathers on parenting behavior.
Pediatrics, 118(2), 659-668. doi: 10.1542/peds.2005-2948
Pawlby, S., Sharp, D., Hay, D., & O'Keane, V. (2008). Postnatal depression and child
outcome at 11 years: the importance of accurate diagnosis. Journal of Affective
Disorders, 107(1-3), 241-245. doi: 10.1016/j.jad.2007.08.002
Prince, M., Patel, V., Saxena, S., Maj, M., Maselko, J., Phillips, M. R., & Rahman, A.
(2007). No health without mental health. Lancet, 370(9590), 859-877. doi:

120
10.1016/s0140-6736(07)61238-0
Rahman, A., Fisher, J., Bower, P., Luchters, S., Tran, T., Yasamy, M. T., Sasena, S., &
Waheed, W. (2013). Interventions for common perinatal mental disorders in
women in low- and middle-income countries: a systematic review and
meta-analysis. Bull World Health Organ, 91(8), 593-601i. doi:
10.2471/blt.12.109819
Rahman, A., Iqbal, Z., Bunn, J., Lovel, H., & Harrington, R. (2004). Impact of
maternal depression on infant nutritional status and illness: a cohort study.
Archives of General Psychiatry, 61(9), 946-952. doi:
10.1001/archpsyc.61.9.946
Ramchandani, P. G., Psychogiou, L., Vlachos, H., Iles, J., Sethna, V., Netsi, E., &
Lodder, A. (2011). Paternal depression: an examination of its links with father,
child and family functioning in the postnatal period. Depression & Anxiety,
28(6), 471-477. doi: 10.1002/da.20814
Sadat, Z., Abedzadeh-Kalahroudi, M., Kafaei Atrian, M., Karimian, Z., & Sooki, Z.
(2014). The Impact of Postpartum Depression on Quality of Life in Women
After Child's Birth. Iranian Red Crescent Medical Journal, 16(2), e14995. doi:
10.5812/ircmj.14995
Scottish Intercollegiate Guidelines Network (SIGN). (2008). Critical appraisal of
notes and methodology checklist. Retrieved August 30, 2014 from
http://www.sign.ac.uk/methodology/checklists.html
Scottish Intercollegiate Guidelines Network. (2012). A guideline developer’s
handbook. Retrieved November 25, 2014 from
http://www.sign.ac.uk/guidelines/fulltext/50/index.html
Simoni, J. M., Franks, J. C., Lehavot, K., & Yard, S. S. (2011). Peer interventions to
promote health: conceptual considerations. American Journal of
Orthopsychiatry, 81(3), 351-359. doi: 10.1111/j.1939-0025.2011.01103.x
Sockol, L. E., Epperson, C. N., & Barber, J. P. (2013). Preventing postpartum
depression: a meta-analytic review. Clinical Psychology Review, 33(8),
1205-1217. doi: 10.1016/j.cpr.2013.10.004

121
Taft, A. J., Small, R., Hegarty, K. L., Watson, L. F., Gold, L., & Lumley, J. A. (2011).
Mothers' AdvocateS In the Community (MOSAIC)--non-professional mentor
support to reduce intimate partner violence and depression in mothers: a
cluster randomised trial in primary care. Bio Medical Central Public Health,
11, 178. doi: 10.1186/1471-2458-11-178
Thombs, B. D., Arthurs, E., Coronado-Montoya, S., Roseman, M., Delisle, V. C.,
Leavens, A., Levis, B., Azoulay, L., Smith, C., Ciofani, L., Coyne, J. C.,
Feeley, N., Gilbody, S., Schinazi, J., Stewart, D. E. & Zelkowitz, P. (2014).
Depression screening and patient outcomes in pregnancy or postpartum: a
systematic review. Journal of Psychosomatic Research, 76(6), 433-446. doi:
10.1016/j.jpsychores.2014.01.006
United Nations Populations Fund (UNFPA). (2013). The Millennium Development
Goals Report 2012. Retrieved August 30, 2014 from
http://www.unfpa.org/public/publications/pid/6090.
Weissman, M. M., Pilowsky, D. J., Wickramaratne, P. J., Talati, A., Wisniewski, S. R.,
Fava, M., Hughes, C. W., Garber, J., Malloy, E., King, C. A., Cerda, G., Sood,
A. B., Alpert, J. E., Trivedi, M. H., & Rush, A. J. (2006). Remissions in
maternal depression and child psychopathology: a STAR*D-child report.
Journal of American Medical Association, 295(12), 1389-1398. doi:
10.1001/jama.295.12.1389
Wiggins, M., Oakley, A., Roberts, I., Turner, H., Rajan, L., Austerberry, H., Mujica, R.,
Mugford, M., & Barker, M. (2005). Postnatal support for mothers living in
disadvantaged inner city areas: a randomised controlled trial. Journal of
Epidemiology & Community Health, 59(4), 288-295. doi:
10.1136/jech.2004.021808
Wilson, S., & Durbin, C. E. (2010). Effects of paternal depression on fathers'
parenting behaviors: a meta-analytic review. Clinical Psychology Review,
30(2), 167-180. doi: 10.1016/j.cpr.2009.10.007
World Health Organization (WHO). (2003). Managing complications in pregnancy
and childbirth: A guide for midwives and doctors. The Department of
Reproductive Health and Research, World Health Organization. Retrieved

122
August 30, 2014 from
http://www.who.int/reproductive-health/impac/Clinical_Priciples/Emotional_s
upport_C7_C14.htm.
World Health Organization (WHO). (2008). Millennium Development Goal 5 –
improving maternal health. Retrieved August 30, 2014 from
http://www.who.int/mental_health/prevention/suicide/Perinatal_depression_m
mh_final.pdf?ua=1
Zhang, Y., & Jin, S. (2014). The impact of social support on postpartum depression:
The mediator role of self-efficacy. Journal of Health Psychology. doi:
10.1177/1359105314536454