Embed Size (px)
Citation preview

Focus on Focus on Fluid and ElectrolytesFluid and Electrolytes
(Relates to Chapter 17, (Relates to Chapter 17, “Fluid, Electrolyte, and Acid-Base “Fluid, Electrolyte, and Acid-Base
Imbalances,” Imbalances,” in the textbook)in the textbook)
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

2
Homeostasis Homeostasis
•State of equilibrium in body State of equilibrium in body •Naturally maintained by Naturally maintained by
adaptive responses adaptive responses •Body fluids and electrolytes Body fluids and electrolytes
are maintained within are maintained within narrow limits.narrow limits.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

3
Water Content of the Water Content of the BodyBody
• 50% to 60% of body weight 50% to 60% of body weight in adultin adult
• 45% to 55% in older adults45% to 55% in older adults• 70% to 80% in infants70% to 80% in infants•Varies with gender, body Varies with gender, body
mass, and agemass, and age
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

4
Changes in Water ContentChanges in Water Content
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Fig. 17-1. Changes in body water content with age and gender.

5
CompartmentsCompartments
• Intracellular fluid (ICF)Intracellular fluid (ICF)• Extracellular fluid (ECF)Extracellular fluid (ECF)• Intravascular (plasma)Intravascular (plasma)• InterstitialInterstitial•TranscellularTranscellular
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

6
Fluid Compartments of Fluid Compartments of the Bodythe Body
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Fig. 17-2. Relative volumes of three body fluids. Values represent fluid distribution in a young male adult.

7
ElectrolytesElectrolytes
•Substances whose Substances whose molecules dissociate into molecules dissociate into ions (charged particles) ions (charged particles) when placed into waterwhen placed into water•Cations: positively chargedCations: positively charged•Anions: negatively chargedAnions: negatively charged
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

8
Measurement of Measurement of ElectrolytesElectrolytes
• International standard is International standard is millimoles per liter millimoles per liter (mmol/L).(mmol/L).
•U.S. uses milliequivalent U.S. uses milliequivalent (mEq).(mEq).• Ions combine mEq for mEq.Ions combine mEq for mEq.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

9
Electrolyte CompositionElectrolyte Composition
• ICFICF•Prevalent cation is KPrevalent cation is K++..•Prevalent anion is POPrevalent anion is PO44
33• ECFECF•Prevalent cation is NaPrevalent cation is Na++..•Prevalent anion is ClPrevalent anion is Cl
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

10
Mechanisms Controlling Mechanisms Controlling Fluid and Electrolyte Fluid and Electrolyte
MovementMovement•DiffusionDiffusion• Facilitated diffusionFacilitated diffusion•Active transportActive transport•OsmosisOsmosis•Hydrostatic pressureHydrostatic pressure•Oncotic pressureOncotic pressure
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

11
DiffusionDiffusion
•Movement of molecules from Movement of molecules from high to low concentration high to low concentration •Occurs in liquids, solids, and Occurs in liquids, solids, and
gasesgases•Membrane separating two Membrane separating two
areas must be permeable to areas must be permeable to diffusing substance.diffusing substance.
•Requires no energyRequires no energy
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

12
DiffusionDiffusion
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Fig. 17-4. Diffusion is the movement of molecules from an area of high concentration to an area of lowconcentration. Eventually the sugar molecules are evenly distributed.

13
Facilitated DiffusionFacilitated Diffusion
•Movement of molecules Movement of molecules from high to low from high to low concentration without concentration without energyenergy
•Uses specific carrier Uses specific carrier molecules to accelerate molecules to accelerate diffusiondiffusion
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

14
Active TransportActive Transport
•Process in which molecules Process in which molecules move against concentration move against concentration gradientgradient•Example: sodium–potassium Example: sodium–potassium
pumppump• External energy requiredExternal energy required
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

15
Sodium-Potassium PumpSodium-Potassium Pump
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Fig. 17-5. Sodium-potassium pump. As sodium (Na+) diffuses into the cell and potassium (K+) diffuses out of thecell, an active transport system supplied with energy delivers Na+ back to the extracellular compartment and K+ tothe intracellular compartment. ATP, Adenosine triphosphate.

16
OsmosisOsmosis
•Movement of water Movement of water between two compartments between two compartments by a membrane permeable by a membrane permeable to water but not to soluteto water but not to solute
•Moves from low solute to Moves from low solute to high solute concentrationhigh solute concentration
•Requires no energyRequires no energy
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

17
OsmosisOsmosis
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Fig. 17-6. Osmosis is the process of water movement through a semipermeable membrane from an area of lowsolute concentration to an area of high solute concentration.

18
Osmotic PressureOsmotic Pressure
•Amount of pressure Amount of pressure required to stop osmotic required to stop osmotic flow of waterflow of water•Determined by concentration Determined by concentration
of solutes in solutionof solutes in solution
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

19
Effects of Water Status on Effects of Water Status on RBCRBC
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Fig. 17-7. Effects of water status on red blood cells. A, Hypotonic solution (H2O excess) results in cellularswelling. B, Isotonic solution (normal H2O balance) results in no change. C, Hypertonic solution (H2O deficit)results in cellular shrinking.

20
Hydrostatic PressureHydrostatic Pressure
• Force within a fluid Force within a fluid compartment compartment
•Major force that pushes Major force that pushes water out of vascular water out of vascular system at capillary levelsystem at capillary level
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

21
Oncotic PressureOncotic Pressure
•Osmotic pressure exerted Osmotic pressure exerted by colloids in solutionby colloids in solution•Protein is a major colloid.Protein is a major colloid.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

22
Fluid Movement in Fluid Movement in CapillariesCapillaries
•Amount and direction of Amount and direction of movement determined bymovement determined by•Capillary hydrostatic Capillary hydrostatic
pressurepressure•Plasma oncotic pressurePlasma oncotic pressure• Interstitial hydrostatic Interstitial hydrostatic
pressurepressure• Interstitial oncotic pressureInterstitial oncotic pressure
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

23
Fluid Exchange Between Fluid Exchange Between Capillary and TissueCapillary and Tissue
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Fig. 17-8. Dynamics of fluid exchange between a capillary and tissue. An equilibrium exists between forces filteringfluid out of the capillary and forces absorbing fluid back into the capillary. Note that the hydrostatic pressure isgreater at the arterial end of the capillary than at the venous end. The net effect of pressures at the arterial end ofthe capillary causes a movement of fluid into the tissue. At the venous end of the capillary, there is net movementof fluid back into the capillary.

24
Fluid ShiftsFluid Shifts
•Plasma-to-interstitial fluid Plasma-to-interstitial fluid shift results in edema.shift results in edema.•Elevation of hydrostatic Elevation of hydrostatic
pressurepressure•Decrease in plasma oncotic Decrease in plasma oncotic
pressurepressure•Elevation of interstitial Elevation of interstitial
oncotic pressureoncotic pressure
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

25
Fluid ShiftsFluid Shifts
• Interstitial fluid to plasmaInterstitial fluid to plasma•Fluid drawn into plasma Fluid drawn into plasma
space with increase in space with increase in plasma osmotic or oncotic plasma osmotic or oncotic pressurepressure
•Compression stockings Compression stockings decrease peripheral edema. decrease peripheral edema.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

26
Fluid Movement Between Fluid Movement Between ECF and ICFECF and ICF
•Water deficit (increased Water deficit (increased ECF) ECF) •Associated with symptoms Associated with symptoms
that result from cell that result from cell shrinkage as water is pulled shrinkage as water is pulled into vascular systeminto vascular system
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

27
Fluid Movement Between Fluid Movement Between ECF and ICFECF and ICF
•Water excess (decreased Water excess (decreased ECF)ECF)•Develops from gain or Develops from gain or
retention of excess waterretention of excess water
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

28
Fluid SpacingFluid Spacing
• First spacingFirst spacing•Normal distribution of fluid in Normal distribution of fluid in
ICF and ECFICF and ECF•Second spacingSecond spacing•Abnormal accumulation of Abnormal accumulation of
interstitial fluid (edema)interstitial fluid (edema)
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

29
Fluid SpacingFluid Spacing
• Third spacingThird spacing•Fluid accumulation in part of Fluid accumulation in part of
body where it is not easily body where it is not easily exchanged with ECFexchanged with ECF
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

30
Regulation of Water Regulation of Water BalanceBalance
•Hypothalamic regulationHypothalamic regulation•Pituitary regulationPituitary regulation•Adrenal cortical regulationAdrenal cortical regulation•Renal regulationRenal regulation
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

31
Regulation of Water Regulation of Water BalanceBalance
•Cardiac regulationCardiac regulation•Gastrointestinal regulationGastrointestinal regulation• Insensible water lossInsensible water loss
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

32
Hypothalamic RegulationHypothalamic Regulation
•Osmoreceptors in Osmoreceptors in hypothalamus sense fluid hypothalamus sense fluid deficit or increase.deficit or increase.•Stimulates thirst and Stimulates thirst and
antidiuretic hormone (ADH) antidiuretic hormone (ADH) releaserelease
•Result in increased free water Result in increased free water and decreased plasma and decreased plasma osmolarityosmolarity
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

33
Pituitary RegulationPituitary Regulation
•Under control of Under control of hypothalamus, posterior hypothalamus, posterior pituitary releases ADH.pituitary releases ADH.
•Stress, nausea, nicotine, Stress, nausea, nicotine, and morphine also and morphine also stimulate ADH release.stimulate ADH release.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

34
Adrenal Cortical Adrenal Cortical RegulationRegulation
•Releases hormones to Releases hormones to regulate water and regulate water and electrolyteselectrolytes•GlucocorticoidsGlucocorticoids
•CortisolCortisol•MineralocorticoidsMineralocorticoids
•AldosteroneAldosterone
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

35
Factors Affecting Factors Affecting Aldosterone Aldosterone SecretionSecretion
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Fig. 17-9. Factors affecting aldosterone secretion. ACTH, Adrenocorticotropic hormone.

36
Effects of Stress on Effects of Stress on Fluid and Electrolyte Fluid and Electrolyte
BalanceBalance
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Fig. 17-10. Effects of stress on fluid and electrolyte balance. ACTH, Adrenocorticotropic hormone; ADH,antidiuretic hormone; CRH, corticotropin-releasing hormone.

37
Renal RegulationRenal Regulation
•Primary organs for Primary organs for regulating fluid and regulating fluid and electrolyte balanceelectrolyte balance•Adjusting urine volumeAdjusting urine volume
•Selective reabsorption of water Selective reabsorption of water and electrolytesand electrolytes
•Renal tubules are sites of Renal tubules are sites of action of ADH and aldosterone. action of ADH and aldosterone.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

38
Cardiac RegulationCardiac Regulation
•Natriuretic peptides are Natriuretic peptides are antagonists to the RAAS.antagonists to the RAAS.•Produced by cardiomyocytes in Produced by cardiomyocytes in
response to increased atrial response to increased atrial pressurepressure
•Suppress secretion of Suppress secretion of aldosterone, renin, and ADH to aldosterone, renin, and ADH to decrease blood volume and decrease blood volume and pressurepressure
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

39
Gastrointestinal Gastrointestinal Regulation Regulation
•Oral intake accounts for most Oral intake accounts for most water.water.
•Small amounts of water are Small amounts of water are eliminated by gastrointestinal eliminated by gastrointestinal tract in feces.tract in feces.
•Diarrhea and vomiting can Diarrhea and vomiting can lead to significant fluid and lead to significant fluid and electrolyte loss.electrolyte loss.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

40
Insensible Water LossInsensible Water Loss
• Invisible vaporization from Invisible vaporization from lungs and skin to regulate lungs and skin to regulate body temperaturebody temperature•Approximately 600 to 900 Approximately 600 to 900
mL/day mL/day is lost. is lost.
•No electrolytes are lost. No electrolytes are lost.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

41
Gerontologic Gerontologic ConsiderationsConsiderations
•Structural changes in kidneys Structural changes in kidneys decrease ability to conserve decrease ability to conserve water.water.
•Hormonal changes lead to Hormonal changes lead to decrease in ADH and ANP.decrease in ADH and ANP.
• Loss of subcutaneous tissue Loss of subcutaneous tissue leads to increased loss of leads to increased loss of moisture.moisture.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

42
Gerontologic Gerontologic Considerations Considerations
•Reduced thirst mechanism Reduced thirst mechanism results in decreased fluid results in decreased fluid intake.intake.
•Nurse must assess for Nurse must assess for these changes and these changes and implement treatment implement treatment accordingly.accordingly.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

43
Fluid and Electrolyte Fluid and Electrolyte ImbalancesImbalances
•Common in most patients Common in most patients with major illness or injurywith major illness or injury•Directly caused by illness or Directly caused by illness or
disease (burns or heart failure)disease (burns or heart failure)•Result of therapeutic measures Result of therapeutic measures
(IV fluid replacement or (IV fluid replacement or diuretics)diuretics)
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

44
Extracellular Fluid Volume Extracellular Fluid Volume ImbalancesImbalances
• ECF volume deficit ECF volume deficit (hypovolemia)(hypovolemia)•Abnormal loss of normal body Abnormal loss of normal body
fluids (diarrhea, fistula drainage, fluids (diarrhea, fistula drainage, hemorrhage), inadequate intake, hemorrhage), inadequate intake, or plasma-to-interstitial fluid shiftor plasma-to-interstitial fluid shift
•Treatment: Replace water and Treatment: Replace water and electrolytes with balanced IV electrolytes with balanced IV solutionssolutions
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

45
Extracellular Fluid Volume Extracellular Fluid Volume Imbalances Imbalances
• Fluid volume excess Fluid volume excess (hypervolemia)(hypervolemia)•Excessive intake of fluids, Excessive intake of fluids,
abnormal retention of fluids abnormal retention of fluids (HF), or interstitial-to-plasma (HF), or interstitial-to-plasma fluid shiftfluid shift
•Treatment: Remove fluid without Treatment: Remove fluid without changing electrolyte composition changing electrolyte composition or osmolality of ECFor osmolality of ECF
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

46
Nursing ManagementNursing ManagementNursing DiagnosesNursing Diagnoses
•HypovolemiaHypovolemia•Deficient fluid volumeDeficient fluid volume•Decreased cardiac outputDecreased cardiac output•Risk for deficient fluid Risk for deficient fluid
volumevolume•Potential complication: Potential complication:
Hypovolemic shockHypovolemic shock
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

47
Nursing ManagementNursing ManagementNursing DiagnosesNursing Diagnoses
•HypervolemiaHypervolemia•Excess fluid volumeExcess fluid volume•Risk for imbalanced fluid Risk for imbalanced fluid
volumevolume• Ineffective airway clearanceIneffective airway clearance•Risk for impaired skin integrityRisk for impaired skin integrity•Disturbed body imageDisturbed body image•Potential complications: Potential complications:
Pulmonary edema, ascitesPulmonary edema, ascitesCopyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

48
Nursing ManagementNursing ManagementNursing ImplementationNursing Implementation
• I & OI & O•Monitor cardiovascular Monitor cardiovascular
changes.changes.•Assess respiratory Assess respiratory
changes.changes.•Daily weightsDaily weights•Skin assessmentSkin assessment
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

49
Assessment of Skin Assessment of Skin TurgorTurgor
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Fig. 17-11. Assessment of skin turgor. A and B, When normal skin is pinched, it resumes shape in seconds.C, If the skin remains wrinkled for 20 to 30 seconds, the patient has poor skin turgor.

50
Nursing ManagementNursing ManagementNursing ImplementationNursing Implementation
•Neurologic functionNeurologic function•LOCLOC•PERLAPERLA•Voluntary movement of Voluntary movement of
extremitiesextremities•Muscle strengthMuscle strength•ReflexesReflexes
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

51
Electrolyte DisordersElectrolyte DisordersSigns and SymptomsSigns and Symptoms
Electrolyte Electrolyte ExcessExcess DeficitDeficit
Sodium (Na)Sodium (Na) HypernatremiaHypernatremia
ThirstThirst
CNS deteriorationCNS deterioration
Increased interstitial fluidIncreased interstitial fluid
HyponatremiaHyponatremia
CNS deteriorationCNS deterioration
Potassium (K)Potassium (K) HyperkalemiaHyperkalemia
Ventricular fibrillationVentricular fibrillation
ECG changesECG changes
CNS changesCNS changes
Hypokalemia Hypokalemia
BradycardiaBradycardia
ECG changes ECG changes
CNS changesCNS changes
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

52
Electrolyte DisordersElectrolyte DisordersSigns and SymptomsSigns and Symptoms
Electrolyte Electrolyte ExcessExcess DeficitDeficit
Calcium (Ca)Calcium (Ca) HypercalcemiaHypercalcemia
ThirstThirst
CNS deteriorationCNS deterioration
Increased interstitial fluidIncreased interstitial fluid
HypocalcemiaHypocalcemia
TetanyTetany
Chvostek’s, Trousseau’s signs Chvostek’s, Trousseau’s signs
Muscle twitchingMuscle twitching
CNS changesCNS changes
ECG changesECG changes
Magnesium Magnesium (Mg)(Mg)
Hypermagnesemia Hypermagnesemia
Loss of deep tendon reflexes Loss of deep tendon reflexes (DTRs)(DTRs)
Depression of CNSDepression of CNS
Depression of neuromuscular Depression of neuromuscular functionfunction
Hypomagnesemia Hypomagnesemia
Hyperactive DTRsHyperactive DTRs
CNS changesCNS changes
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

53
SodiumSodium
• Imbalances typically Imbalances typically associated with parallel associated with parallel changes in osmolality changes in osmolality
• Plays a major role inPlays a major role in• ECF volume and concentrationECF volume and concentration• Generation and transmission Generation and transmission
of nerve impulsesof nerve impulses• Acid-base balanceAcid-base balance
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

54
HypernatremiaHypernatremia
• Elevated serum sodium Elevated serum sodium occurring with water loss or occurring with water loss or sodium gainsodium gain
•Causes hyperosmolality Causes hyperosmolality leading to cellular leading to cellular dehydration dehydration
•Primary protection is thirst Primary protection is thirst from hypothalamus. from hypothalamus.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

55
Differential Assessment of Differential Assessment of
ECF VolumeECF Volume
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Fig. 17-12. Differential assessment of extracellular fluid (ECF) volume.

56
Imbalances in ECF VolumeImbalances in ECF Volume
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Fig. 17-13. Isotonic gains and losses affect mainly the extracellular fluid (ECF) compartment with little or nowater movement into the cells. Hypertonic imbalances cause water to move from inside the cell into the ECF todilute the concentrated sodium, causing cell shrinkage. Hypotonic imbalances cause water to move into thecell, causing cell swelling.

57
HypernatremiaHypernatremia
•ManifestationsManifestations•Thirst, lethargy, agitation, Thirst, lethargy, agitation,
seizures, and comaseizures, and coma• Impaired LOCImpaired LOC•Produced by clinical states Produced by clinical states •Central or nephrogenic Central or nephrogenic
diabetes insipidusdiabetes insipidus
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

58
Nursing ManagementNursing ManagementNursing DiagnosesNursing Diagnoses
•Risk for injuryRisk for injury•Risk for electrolyte Risk for electrolyte
imbalanceimbalance•Potential complication: Potential complication:
Seizures and coma leading Seizures and coma leading to irreversible brain to irreversible brain damagedamage
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

59
Nursing ManagementNursing ManagementNursing ImplementationNursing Implementation
• Treat underlying cause.Treat underlying cause.• If oral fluids cannot be If oral fluids cannot be
ingested, IV solution of 5% ingested, IV solution of 5% dextrose in water or dextrose in water or hypotonic salinehypotonic saline
•DiureticsDiuretics
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

60
HyponatremiaHyponatremia
•Results from loss of Results from loss of sodium-containing fluids or sodium-containing fluids or from water excess.from water excess.
•ManifestationsManifestations•Confusion, nausea, vomiting, Confusion, nausea, vomiting,
seizures, and comaseizures, and coma
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

61
Nursing ManagementNursing ManagementNursing DiagnosesNursing Diagnoses
•Risk for injuryRisk for injury•Risk for electrolyte Risk for electrolyte
imbalanceimbalance•Potential complication: Potential complication:
Severe neurologic changesSevere neurologic changes
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

62
Nursing ManagementNursing ManagementNursing ImplementationNursing Implementation
•Caused by water excessCaused by water excess•Fluid restriction is needed.Fluid restriction is needed.
•Severe symptoms Severe symptoms (seizures)(seizures)•Give small amount of IV Give small amount of IV
hypertonic saline solution hypertonic saline solution (3% NaCl).(3% NaCl).
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

63
Nursing ManagementNursing ManagementNursing ImplementationNursing Implementation
•Abnormal fluid lossAbnormal fluid loss•Fluid replacement with Fluid replacement with
sodium-containing solutionsodium-containing solution•VasopressinsVasopressins
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

64
PotassiumPotassium
•Major ICF cationMajor ICF cation•Necessary forNecessary for•Transmission and conduction Transmission and conduction
of nerve and muscle impulses of nerve and muscle impulses •Cellular growthCellular growth•Maintenance of cardiac Maintenance of cardiac
rhythmsrhythms•Acid-base balanceAcid-base balance
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

65
PotassiumPotassium
•Sources Sources •Fruits and vegetables Fruits and vegetables
(bananas and oranges)(bananas and oranges)•Salt substitutes Salt substitutes •Potassium medications (PO, Potassium medications (PO,
IV)IV)•Stored bloodStored blood
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

66
HyperkalemiaHyperkalemia
•High serum potassium High serum potassium caused bycaused by•Massive intakeMassive intake• Impaired renal excretionImpaired renal excretion•Shift from ICF to ECFShift from ICF to ECF
•Most common in renal Most common in renal failurefailure
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

67
HyperkalemiaHyperkalemia
•ManifestationsManifestations•Cramping leg painCramping leg pain•Weak or paralyzed skeletal Weak or paralyzed skeletal
musclesmuscles•Ventricular fibrillation or Ventricular fibrillation or
cardiac standstill cardiac standstill •Abdominal cramping or Abdominal cramping or
diarrheadiarrhea
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

68
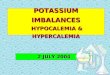
ECG Effects of ECG Effects of HyperkalemiaHyperkalemia
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Fig. 17-14. Electrocardiographic changes associated with alterations in potassium status.

69
Nursing ManagementNursing ManagementNursing DiagnosesNursing Diagnoses
•Risk for electrolyte Risk for electrolyte imbalanceimbalance
•Risk for injuryRisk for injury•Potential complication: Potential complication:
DysrhythmiasDysrhythmias
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

70
Nursing ManagementNursing ManagementNursing ImplementationNursing Implementation
• Eliminate oral and Eliminate oral and parenteral K intake.parenteral K intake.
• Increase elimination of K Increase elimination of K (diuretics, dialysis, (diuretics, dialysis, Kayexalate).Kayexalate).
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

71
Nursing ManagementNursing ManagementNursing ImplementationNursing Implementation
• Force K from ECF to ICF by Force K from ECF to ICF by IV insulin or sodium IV insulin or sodium bicarbonate.bicarbonate.
•Reverse membrane effects Reverse membrane effects of elevated ECF potassium of elevated ECF potassium by administering calcium by administering calcium gluconate IV.gluconate IV.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

72
HypokalemiaHypokalemia
• Low serum potassium Low serum potassium caused bycaused by•Abnormal losses of KAbnormal losses of K++ via the via the
kidneys or gastrointestinal kidneys or gastrointestinal tracttract
•Magnesium deficiencyMagnesium deficiency•Metabolic alkalosisMetabolic alkalosis
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

73
HypokalemiaHypokalemia
•ManifestationsManifestations•Most serious are cardiac.Most serious are cardiac.•Skeletal muscle weakness (legs)Skeletal muscle weakness (legs)•Weakness of respiratory musclesWeakness of respiratory muscles•Decreased gastrointestinal Decreased gastrointestinal
motilitymotility• Impaired regulation of arteriolar Impaired regulation of arteriolar
blood flowblood flow
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

74
Nursing ManagementNursing ManagementNursing DiagnosesNursing Diagnoses
•Risk for electrolyte Risk for electrolyte imbalanceimbalance
•Risk for injuryRisk for injury•Potential complication: Potential complication:
DysrhythmiasDysrhythmias
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

75
Nursing ManagementNursing ManagementNursing ImplementationNursing Implementation
•KCl supplements orally or KCl supplements orally or IVIV
•Should not exceed 10 to 20 Should not exceed 10 to 20 mEq/hr mEq/hr •To prevent hyperkalemia and To prevent hyperkalemia and
cardiac arrestcardiac arrest
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

76
CalciumCalcium
•Obtained from ingested Obtained from ingested foodsfoods
•More than 99% combined More than 99% combined with phosphorus and with phosphorus and concentrated in skeletal concentrated in skeletal systemsystem
• Inverse relationship with Inverse relationship with phosphorusphosphorus
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

77
CalciumCalcium
•Bones are readily available Bones are readily available store.store.
•Blocks sodium transport Blocks sodium transport and stabilizes cell and stabilizes cell membranemembrane
• Ionized form is biologically Ionized form is biologically active.active.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

78
CalciumCalcium
• Functions Functions •Transmission of nerve Transmission of nerve
impulsesimpulses•Myocardial contractionsMyocardial contractions•Blood clottingBlood clotting•Formation of teeth and boneFormation of teeth and bone•Muscle contractionsMuscle contractions
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

79
CalciumCalcium
•Balance controlled byBalance controlled by•Parathyroid hormoneParathyroid hormone•CalcitoninCalcitonin•Vitamin DVitamin D
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

80
HypercalcemiaHypercalcemia
•High serum calcium levels High serum calcium levels caused bycaused by•Hyperparathyroidism (two Hyperparathyroidism (two
thirds of cases)thirds of cases)•Malignancy Malignancy •Vitamin D overdoseVitamin D overdose•Prolonged immobilizationProlonged immobilization
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

81
HypercalcemiaHypercalcemia
•ManifestationsManifestations•Decreased memoryDecreased memory•ConfusionConfusion•DisorientationDisorientation•FatigueFatigue•Constipation Constipation
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

82
Nursing ManagementNursing ManagementNursing DiagnosesNursing Diagnoses
•Risk for electrolyte Risk for electrolyte imbalanceimbalance
•Risk for injuryRisk for injury•Potential complication: Potential complication:
DysrhythmiasDysrhythmias
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

83
Nursing ManagementNursing ManagementNursing ImplementationNursing Implementation
• Excretion of Ca with loop Excretion of Ca with loop diureticdiuretic
•Hydration with isotonic Hydration with isotonic saline infusionsaline infusion
•Synthetic calcitoninSynthetic calcitonin•MobilizationMobilization
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

84
HypocalcemiaHypocalcemia
• Low serum Ca levels caused Low serum Ca levels caused byby•Decreased production of PTHDecreased production of PTH•Acute pancreatitis Acute pancreatitis •Multiple blood transfusions Multiple blood transfusions •AlkalosisAlkalosis•Decreased intakeDecreased intake
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

85
HypocalcemiaHypocalcemia
•ManifestationsManifestations•Positive Trousseau’s or Positive Trousseau’s or
Chvostek’s signChvostek’s sign•Laryngeal stridorLaryngeal stridor•DysphagiaDysphagia•Tingling around the mouth or Tingling around the mouth or
in the extremities in the extremities
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

86
Tests for HypocalcemiaTests for Hypocalcemia
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Fig. 17-15. Tests for hypocalcemia. A, Chvostek’s sign is contraction of facial muscles in response to a light tapover the facial nerve in front of the ear. B, Trousseau’s sign is a carpal spasm induced by C, inflating a bloodpressure cuff above the systolic pressure for a few minutes.

87
Nursing ManagementNursing ManagementNursing DiagnosesNursing Diagnoses
•Risk for electrolyte Risk for electrolyte imbalanceimbalance
•Risk for injuryRisk for injury•Potential complication: Potential complication:
Fracture or respiratory Fracture or respiratory arrestarrest
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

88
Nursing ManagementNursing ManagementNursing ImplementationNursing Implementation
• Treat cause.Treat cause.•Oral or IV calcium Oral or IV calcium
supplementssupplements•Not IM to avoid local reactionsNot IM to avoid local reactions
• Treat pain and anxiety to Treat pain and anxiety to prevent hyperventilation-prevent hyperventilation-induced respiratory alkalosis.induced respiratory alkalosis.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

89
PhosphatePhosphate
•Primary anion in ICFPrimary anion in ICF• Essential to function of Essential to function of
muscle, red blood cells, and muscle, red blood cells, and nervous systemnervous system
•Deposited with calcium for Deposited with calcium for bone and tooth structurebone and tooth structure
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

90
PhosphatePhosphate
• Involved in acid-base Involved in acid-base buffering system, ATP buffering system, ATP production, and cellular production, and cellular uptake of glucoseuptake of glucose
•Maintenance requires Maintenance requires adequate renal functioning.adequate renal functioning.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

91
HyperphosphatemiaHyperphosphatemia
•High serum POHigh serum PO4433 caused by caused by
•Acute or chronic renal failureAcute or chronic renal failure•ChemotherapyChemotherapy•Excessive ingestion of Excessive ingestion of
phosphate or vitamin Dphosphate or vitamin D
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

92
HyperphosphatemiaHyperphosphatemia
•Manifestations Manifestations •Calcified deposition in soft Calcified deposition in soft
tissue such as joints, tissue such as joints, arteries, skin, kidneys, and arteries, skin, kidneys, and corneascorneas
•Neuromuscular irritability Neuromuscular irritability and tetanyand tetany
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

93
HyperphosphatemiaHyperphosphatemia
•ManagementManagement• Identify and treat underlying Identify and treat underlying
cause.cause.•Restrict foods and fluids Restrict foods and fluids
containing phosphorus.containing phosphorus.•Adequate hydration and Adequate hydration and
correction of hypocalcemic correction of hypocalcemic conditionsconditions
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

94
HypophosphatemiaHypophosphatemia
• Low serum POLow serum PO4433 caused by caused by
•Malnourishment/Malnourishment/malabsorptionmalabsorption
•Alcohol withdrawalAlcohol withdrawal•Use of phosphate-binding Use of phosphate-binding
antacidsantacids•During parenteral nutrition During parenteral nutrition
with inadequate replacementwith inadequate replacementCopyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

95
HypophosphatemiaHypophosphatemia
•ManifestationsManifestations•CNS depressionCNS depression•Confusion Confusion •Muscle weakness and painMuscle weakness and pain•Dysrhythmias Dysrhythmias •Cardiomyopathy Cardiomyopathy
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

96
HypophosphatemiaHypophosphatemia
•ManagementManagement•Oral supplementationOral supplementation• Ingestion of foods high in Ingestion of foods high in
phosphorusphosphorus• IV administration of sodium IV administration of sodium
or potassium phosphate or potassium phosphate
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

97
MagnesiumMagnesium
• 50% to 60% contained in 50% to 60% contained in bone.bone.
•Coenzyme in metabolism of Coenzyme in metabolism of protein and carbohydrates protein and carbohydrates
• Factors that regulate calcium Factors that regulate calcium balance appear to influence balance appear to influence magnesium balance.magnesium balance.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

98
MagnesiumMagnesium
•Acts directly on myoneural Acts directly on myoneural junction junction
• Important for normal Important for normal cardiac functioncardiac function
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

99
HypermagnesemiaHypermagnesemia
•High serum Mg caused byHigh serum Mg caused by• Increased intake or ingestion Increased intake or ingestion
of products containing of products containing magnesium when renal magnesium when renal insufficiency or failure is insufficiency or failure is present present
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

100
HypermagnesemiaHypermagnesemia
•ManifestationsManifestations•Lethargy or drowsinessLethargy or drowsiness•Nausea/vomitingNausea/vomiting• Impaired reflexesImpaired reflexes•Somnolence Somnolence •Respiratory and cardiac Respiratory and cardiac
arrestarrest
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

101
HypermagnesemiaHypermagnesemia
•ManagementManagement•PreventionPrevention•Emergency treatmentEmergency treatment
•IV CaCl or calcium gluconateIV CaCl or calcium gluconate•Fluids to promote urinary Fluids to promote urinary
excretionexcretion
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

102
HypomagnesemiaHypomagnesemia
• Low serum Mg caused byLow serum Mg caused by•Prolonged fasting or starvationProlonged fasting or starvation•Chronic alcoholismChronic alcoholism•Fluid loss from gastrointestinal Fluid loss from gastrointestinal
tracttract•Prolonged parenteral nutrition Prolonged parenteral nutrition
without supplementationwithout supplementation•DiureticsDiuretics
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

103
HypomagnesemiaHypomagnesemia
•ManifestationsManifestations•ConfusionConfusion•Hyperactive deep tendon Hyperactive deep tendon
reflexesreflexes•TremorsTremors•Seizures Seizures •Cardiac dysrhythmias Cardiac dysrhythmias
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

104
HypomagnesemiaHypomagnesemia
•ManagementManagement•Oral supplementsOral supplements• Increase dietary intake.Increase dietary intake.•Parenteral IV or IM Parenteral IV or IM
magnesium when severemagnesium when severe
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

105
IV FluidsIV Fluids
• PurposesPurposes1.1. MaintenanceMaintenance
• When oral intake is not When oral intake is not adequateadequate
2.2. ReplacementReplacement• When losses have occurred When losses have occurred
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

106
IV FluidsIV Fluids
•HypotonicHypotonic•More water than electrolytesMore water than electrolytes
•Pure water lyses RBCs.Pure water lyses RBCs.•Water moves from ECF to ICF Water moves from ECF to ICF
by osmosis.by osmosis.•Usually maintenance fluidsUsually maintenance fluids
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

107
IV FluidsIV Fluids
• IsotonicIsotonic•Expands only ECFExpands only ECF•No net loss or gain from ICFNo net loss or gain from ICF
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

108
IV FluidsIV Fluids
•HypertonicHypertonic• Initially expands and raises Initially expands and raises
the osmolality of ECFthe osmolality of ECF•Require frequent monitoring Require frequent monitoring
ofof•Blood pressureBlood pressure•Lung soundsLung sounds•Serum sodium levelsSerum sodium levels
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

109
D5WD5W
• IsotonicIsotonic•Provides 170 cal/LProvides 170 cal/L• Free waterFree water•Moves into ICFMoves into ICF• Increases renal solute Increases renal solute
excretion excretion
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

110
D5WD5W
•Used to replace water Used to replace water losses and treat losses and treat hyponatremiahyponatremia
•Does not provide Does not provide electrolyteselectrolytes
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

111
Normal Saline (NS)Normal Saline (NS)
• Isotonic Isotonic •No caloriesNo calories•More NaCl than ECFMore NaCl than ECF• 30% stays in IV (most)30% stays in IV (most)•70% moves out of IV70% moves out of IV
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

112
Normal Saline (NS)Normal Saline (NS)
• Expands IV volumeExpands IV volume•Preferred fluid for immediate Preferred fluid for immediate
responseresponse•Risk for fluid overload higherRisk for fluid overload higher
•Does not change ICF volumeDoes not change ICF volume•Blood productsBlood products•Compatible with most Compatible with most
medicationsmedicationsCopyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

113
{Insert Archie animation {Insert Archie animation #490}#490}
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

114
Lactated Ringer’sLactated Ringer’s
• IsotonicIsotonic•More similar to plasma More similar to plasma
than NSthan NS•Has less NaClHas less NaCl•Has K, Ca, POHas K, Ca, PO44
33, lactate , lactate (metabolized to HCO(metabolized to HCO33))
• Expands ECFExpands ECF
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

115
D5 ½ NSD5 ½ NS
•HypertonicHypertonic•Common maintenance fluidCommon maintenance fluid•KCl added for maintenance KCl added for maintenance
or replacement or replacement
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

116
D10WD10W
•HypertonicHypertonic•Provides 340 kcal/LProvides 340 kcal/L• Free waterFree water• Limit of dextrose Limit of dextrose
concentration may be concentration may be infused peripherally.infused peripherally.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

117
•Stay in vascular space and Stay in vascular space and increase osmotic pressure. increase osmotic pressure.
•Colloids (protein solutions)Colloids (protein solutions)•AlbuminAlbumin•PlasmaPlasma•Commercial plasmasCommercial plasmas•Packed RBCsPacked RBCs
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Fig. 17-12. Differential assessment of extracellular fluid (ECF) volume.

In a patient with prolonged vomiting, the nurse In a patient with prolonged vomiting, the nurse monitors for fluid volume deficit because monitors for fluid volume deficit because vomiting results in:vomiting results in:
1. Fluid movement from the cells into the 1. Fluid movement from the cells into the interstitial space and the blood vessels.interstitial space and the blood vessels.
2. Excretion of large amounts of interstitial fluid 2. Excretion of large amounts of interstitial fluid with depletion of extracellular fluids. with depletion of extracellular fluids.
3. An overload of extracellular fluid with a 3. An overload of extracellular fluid with a significant increase in intracellular fluid volume. significant increase in intracellular fluid volume.
4. Fluid movement from the vascular system into 4. Fluid movement from the vascular system into the cells, causing cellular swelling and rupture.the cells, causing cellular swelling and rupture.
Audience Response Question
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 118

Case StudyCase Study
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 119

120
Case StudyCase Study
• 76-year-old man is brought 76-year-old man is brought to emergency department to emergency department with confusion and lethargy.with confusion and lethargy.
•He has a history of chronic He has a history of chronic heart failure, type 2 heart failure, type 2 diabetes, and hypertension. diabetes, and hypertension.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

121
Case StudyCase Study
• Lab values reveal low Lab values reveal low potassium levels and Hct potassium levels and Hct 56%.56%.
•Poor skin turgorPoor skin turgor
•BP 110/58 BP 110/58
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

122
Case StudyCase Study
•Heart rate 135 Heart rate 135
•Respiratory rate 26 Respiratory rate 26
• Temperature 99Temperature 99
•Recent fluRecent flu
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

123
Case StudyCase Study
•Patient forgot he took Patient forgot he took furosemide (Lasix) and furosemide (Lasix) and doubled dose twice in 1 doubled dose twice in 1 week.week.
•Started on .45 NaCl and IV Started on .45 NaCl and IV potassium chloridepotassium chloride
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

124
Discussion QuestionsDiscussion Questions
1.1. What important teaching What important teaching should be done with him?should be done with him?
2.2. What resources are What resources are available to help him available to help him manage his medications?manage his medications?
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.