Embed Size (px)
Citation preview

Short Communication
Focal nodular hyperplasia-like lesion of the liver in a childpreviously treated for nephroblastoma
Junji Takeyama,1 Ryo Ando,2 Tomoyuki Sato,2 Masaki Nio,2 Yoshihisa Shimanuki,3 Atsushi Sato4 andMasue Imaizumi4
Departments of 1Pathology, 2Surgery, 3Radiology and 4Hematology and Oncology, Miyagi Children’s Hospital,Sendai, Japan
Described herein is the case of an 8-year-old boy who devel-oped a hepatic nodular lesion after having receivedanti-neoplastic therapy for nephroblastoma. Histologicalexamination of the excised specimen indicated a disorderedarrangement of hepatic components with hemangioma-likefeatures. This case was diagnosed as a variant of focalnodular hyperplasia. It is speculated that this hepatic lesionis a late complication of treatment for nephroblastoma andmight develop from congenital malformative area of theliver.
Key words: focal nodular hyperplasia, hamartoma, hepaticnodule, nephroblastoma, veno-occlusive disease
Focal nodular hyperplasia (FNH) represents a localized livercell hyperplasia containing central and/or stellate fibrousscar. It is commonly assumed that FNH is a reactive disorderrelated to localized vascular abnormalities and circulatorydisturbances.1 Recently, FNH has been reported as a latecomplication in patients who have received anti-neoplastictreatments for malignancy.2–5 In this paper, we report a caseof FNH-like hepatic nodule that presented after completion oftherapy for nephroblastoma.
CLINICAL SUMMARY
A 6-month-old boy was diagnosed with stage II nephroblas-toma in the left kidney. He underwent left nephrectomy andsubsequently received chemotherapy using vincristine andactinomycin D. There was an episode of veno-occlusive
disease (VOD) during the therapy. At 11⁄2 years of age hedeveloped multiple foci of recurrences in the peritoneum.Surgical resection and high-dose chemotherapy with autolo-gous peripheral blood stem cell transplantation were per-formed. At 6 years of age a small focus of hepatic nodule wasdetected by contrast-enhanced CT. It gradually grew andbecame 2 cm in diameter at 8 years of age. On magneticresonance imaging (MRI) it had low signal intensityon T1-weighted imaging and high signal intensity onT2-weighted imaging. On dynamic MRI it was homogenouslyenhanced during the arterial phase, and was isointenseduring the delayed phase (Fig. 1). On superparamagneticiron oxide-enhanced MRI the lesion had lower intensity onT2-weighted imaging than on unenhanced MRI, which wasnot indicative of a metastatic tumor.6 Although the preopera-tive evaluation was suggestive of FNH, the hepatic nodulewas surgically resected due to its tendency to enlarge. Thepostoperative course was uneventful.
PATHOLOGICAL FINDINGS
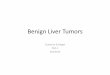
On gross examination the resected lesion was a well-circumscribed nodule without capsule. Central scar was notevident (Fig. 2). Microscopically, it was composed of a disor-dered proliferation of hepatic components: there were irregu-lar hepatic plates and interlacing fibrous bands containingnumerous capillary vessels and bile ducts (Fig. 3a–d). Thehepatocytes were hyperplastic and devoid of cytologicalatypia (Fig. 3e). No normal portal areas were detected. His-tological diagnosis was hamartoma or possibly a variant ofFNH (FNH-like lesion).
DISCUSSION
Although the radiological findings of the hepatic mass in thepresent case were compatible with FNH, the pathological
Correspondence: Junji Takeyama, MD, Department of Pathology,Miyagi Children’s Hospital, 4-3-17 Ochiai, Aoba-ku, Sendai 989-3126, Japan. Email: [email protected]
Received 20 February 2008. Accepted for publication 11 May2008.© 2008 The AuthorsJournal compilation © 2008 Japanese Society of Pathology
Pathology International 2008; 58: 606–608 doi:10.1111/j.1440-1827.2008.02277.x

features were unusual for FNH. Central and/or stellate scartypically seen in FNH was not observed. In addition, numer-ous capillary vessels proliferated in the interlacing fibrousbands, which looked like capillary hemangioma. FNH andhemangioma occasionally coexist in the same liver,7 andFNH rarely contains hemangioma in the same nodule.8,9
Ndimbie et al. and Saito et al. reported cases of FNH withhemangioma in the center of the lesion and hypothesizedthat the central scar is probably the end-stage of progressivesclerosis or thrombosis of vascular malformation.8,9 If thishypothesis is correct, the present case might be the earlystage of FNH and the fibrous bands with hemangioma-likefeatures might possibly become a typical scar at the laterstage. The histological features of this case may be helpful inilluminating the pathogenesis of FNH.
We suggest that this hepatic nodule is a malformativelesion. On histology it was composed of a disorderedarrangement of normal elements of the liver, which was
compatible with hamartoma. Hamartoma is generally a con-genital lesion resulting from faulty embryonal development.It is speculated that an abnormal interaction between theendoderm- and the mesoderm-derived tissues might leadto formation of the tumorous lesion that consisted of anirregular admixture of hepatic plates, bile ducts and con-nective tissue components. FNH is not a neoplasm but alocalized liver cell hyperplasia caused by vascular malfor-mation, which may be in the category of hamartoma. There-fore, this case was histologically diagnosed as a variant ofFNH.
It has been reported that FNH rarely presents as a latecomplication of treatment for malignancy.2–5 In such cases,vascular injuries caused by the anti-neoplastic therapies andsubsequent localized circulatory disturbances might result inthe development of FNH. This is supported by the fact thatthe patients who had VOD during treatment were at higherrisk of developing FNH.2,3 We doubt, however, that circulatorydisturbances alone can fully explain the pathogenesis of thepresent case. It is curious that such a solitary and well-circumscribed lesion developed after the toxicity of anti-neoplastic therapy had diffused through the whole liver. Wespeculate that the hepatic lesion developed from a focus ofpre-existing malformation that might be more resistant todamage than the surrounding normal tissue. This area waswell perfused by the malformative vessels, which resulted insecondary hyperplasia of the liver cells. The therapy fornephroblastoma might damage the extra-nodular area moreseverely than the nodular area, which made clear contrastbetween them. Although there are few possibilities of recur-rence or malignant transformation of hamartoma, the presentpatient requires long-term follow-up. Considering the patho-genesis of this lesion, another nodule may occur somewherein the liver.
a
b
Figure 1 Dynamic magnetic resonance imaging. The hepaticnodule (arrow) is (a) enhanced during the arterial phase and (b) isisointense to surrounding liver parenchyma during the delayedphase.
Figure 2 Cut surface of the hepatic nodule. Central scar is notapparent.
FNH-like lesion 607
© 2008 The AuthorsJournal compilation © 2008 Japanese Society of Pathology
REFERENCES
1 Kondo F. Benign nodular hepatocellular lesions caused by abnor-mal hepatic circulation: Etiological analysis and introduction of anew concept. J Gastroenterol Hepatol 2001; 16: 1319–28.
2 Bouyn CI, Leclere J, Raimondo G et al. Hepatic focal nodularhyperplasia in children previously treated for a solid tumor. Inci-dence, risk factors, and outcome. Cancer 2003; 97: 3107–13.
3 Brisse H, Servois V, Bouche B et al. Hepatic regeneratingnodules: A mimic of recurrent cancer in children. Pediatr Radiol2000; 30: 386–93.
4 Kumagai H, Masuda T, Oikawa H, Endo K, Endo M, Takano T.Focal nodular hyperplasia of the liver: Direct evidence of circu-latory disturbances. J Gastroenterol Hepatol 2000; 15: 1344–7.
5 Joyner BL Jr, Goyal RK, Newman B, Levin TL. Focal nodularhyperplasia of the liver: A sequela of tumor therapy. PediatrRadiol 2005; 35: 1234–9.
6 Okada T, Sasaki F, Kamiyama T et al. Focal nodular hyperplasiaof the liver: Usefulness of superparamagnetic iron oxide-enhanced magnetic resonance imaging. J Pediatr Surg 2005; 40:E21–5.
7 Vilgrain V, Uzan F, Brancatelli G, Federle MP, Zappa M, Menu Y.Prevalence of hepatic hemangioma in patients with focal nodularhyperplasia: MR imaging analysis. Radiology 2003; 229: 75–9.
8 Ndimbie OK, Goodman ZD, Chase RL, Ma CK, Lee MW. Heman-giomas with localized nodular proliferation of the liver. A sugges-tion on the pathogenesis of focal nodular hyperplasia. Am J SurgPathol 1990; 14: 142–50.
9 Saito M, Nagashima K, Horita S. Focal nodular hyperplasia of theliver with angioma-like features in the center. Intern Med 2005;44: 503–4.
Figure 3 Histological findings. (a)Low magnification demonstrates thatthere are interlacing fibrous bands inthe hepatic nodule. Central scar is notapparent (Azan). (b) In boxed area in(a), hepatic plates, bile ducts and bloodvessels are arranged haphazardly(HE). (c,d) High magnification of theboxed areas in (a) shows (c) numerouscapillary vessels, (d) ductular prolifera-tion and (e) hepatocellular hyperplasiawithout cellular atypia (HE).
a b
c d
e
608 J. Takeyama et al.
© 2008 The AuthorsJournal compilation © 2008 Japanese Society of Pathology