Embed Size (px)
Citation preview

Focal epithelial hyperplasia Report of nine cases from Sweden and review of the literatufe
G&-an Pilgbrd, D.D.S., Linkiiping, Sweden
DEPARTMENT OF ORAL SURGERY, UNIVERSITY HOSPITAL
Nine cases of focal epithelial hyperplasia (FEH) from the northern part of Sweden are reported. Four of
these occurred within the same Caucasian family. In one case FEH was diagnosed in a Laplander,
ethnically related to Eskimos. The results of follow-up after surgical removal of the lesions are presented.
(ORAL SURG. 57540543, 1984.)
F ocal epithelial hyperplasia (FEH) or Heck’s dis- ease is an unusual lesion of the oral mucosa. The term focal epithelial hyperplasia was introduced in 1965,‘*2 although the condition had been described earlier under other names.3-5
Since 1965 FEH has been reported among Amer- ican Indians and Eskimos in Greenland and Alaska.6 Only a few cases have been reported from Sweden.‘** Prevalence studies of FEH indicate a prevalence of more than 3% and mostly above 10% in Eskimo populations (highest 35.8%)g and less than 3.5% among Indians9 (highest 33.75% in 4- to lZyear-old Indians).5
As very few cases have been reported in Cauca- sians, it seems reasonable to conclude that the disorder is very rare among members of this race.‘*” Lindeberg” has suggested, from a genetic stand- point, that the Laplanders from northern Scandina- via might exhibit FEH in a prevalence corresponding to that of the Eskimos.
Fig 1. Case 1. Focal epithelial hyperplasia, type 1, on the right buccal mucosa.
Both types show a partly irregular boundary between the affected and unaffected mucosae.‘* Their size ranges between 0.1 and 1 .O cm. When the mucosa is stretched, the lesions tend to disappear.8
ETIOLOGY
It has been postulated that FEH is a virus-induced benign hyperplasia of the oral mucosa.2~‘2
As most cases have been reported in Indians and Eskimos, and as there have sometimes been familial occurrences, a genetic factor may be involved.2 In some families FEH has been found in more than one member.13-”
Among American Indians, FEH is located most commonly on the lower lip. Among Eskimos more than 50% of the lesions have a lingual location.9
Most patients with FEH have had the lesions for a very long time, periods up to 20 years having been reported.”
HISTOPATHOLOGY
CLINICAL FEATURES
Clinically, FEH seems to be of two types: Type 1 consists of circumscribed, sessile, soft,
rounded, and nodular elevations with a color similar to that of the adjoining mucosa (Figs. 1 and 2).
Type 2 involves a well-demarcated, soft, slightly elevated papule with a flat, whitish surface or with a color similar to that of the adjoining mucosa (Fig. 3).
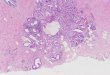
Histologically, FEH is characterized by a local- ized epithelial hyperplasia with acanthosis. Slight parakeratosis often occurs. There is elongation and anastomosis of rete ridges by horizontal outgrowth. One of the prominent features is the presence at various levels of the epithelium of ballooning cells that show mitosis-like aberrations, or so-called FEH cellsI (Fig. 4). Inclusion bodies ean be seen in the center of the nuclear areas of these cells. Intranu- clear papovavirus-like particles with a diameter of
540

Volume 57 Number 5
Focal epithelial h yperplasia 54 1
Fig 2. Case 1. Two lesions of focal epithelial hyperplasia, type 1, on the tongue.
Fig 3. Case 4. Multiple lesions of focal epithelial hyper- plasia, type 2, on the left side of the tongue.
Table I. The clinical appearance of FEH in the family discussed in Case 6.
Age/sex Duration of known
lesion (yr) Site of FEH Time of follow-up without recurrence
52/F (Case 6)
54/F 50/M 55/F
20 Lower lip, left buccal mucosa, tongue
14 Left buccal mucosa Unknown Lower lip
30 Tongue
9 mo
6 yr 9 mo -
400 to 600 A have been found in electron microscop ic studies.L2* 2o
There seems to be no hyperplasia of the connective tissue. A very mild chronic inflammation of the interstitial connective tissue may also be found.9
DIFFERENTIAL DIAGNOSIS
Buchner and Sandbank*’ have reported a lesion, called multiple fibroepithelial hyperplasia, which is clinically similar to FEH although somewhat differ- ent histologically.*’
TREATMENT AND COURSE
Spontaneous regression or disappearance of the lesion has been observed by several investigators.‘*’ Variable cure rates have been reported subsequent to surgical excision.“,**
CASEREPORTS
The present report describes nine cases of FEH, four of which were in one family. All cases were diagnosed in northern Sweden. The series was col- lected between 1976 and 1979.
CASE I
A 40-year-old woman had several lesions on the buccal mucosa and the lower lip. They had been present for as
long as she could remember and had not caused any discomfort. The patient recalled that her mother had similar lesions.
There were some lesions of type 1, approximately 3 mm in diameter, on the lower lip, on the right buccal mucosa at the level of the occlusal plane (Fig. l), and on the tongue (Fig. 2). Some lesions were excised, and histologic exami- nation showed them to be FEH. One year after the first examination and treatment, there were new lesions but in different locations from where the first biopsy specimen was taken. After 4 years there was a regression of the lesions without treatment, in contrast to the first occasion, and there was no recurrence at the biopsy sites.
CASE 2
An 80-year-old woman had a lesion of unknown dura- tion on the tip of the tongue. Symptoms included sharp pain in this area, especially when the patient took warm drinks.
There was a 5 by 4 mm lesion of type 1 on the tip of the tongue. The lesion was excised and a histologic diagnosis of FEH was made. After 3!4 years there was no recurrence or pain at the tip of the tongue.
CASE 3
A 6%year-old woman had noted a lesion on the lower lip for some years. This lesion was traumatized by a lower dental prosthesis. Two lesions of type 1 were found on the lower lip. One measured 15 by 7 mm, and the other was

542 Pilgirrd Oral Surg. May, 1984
Fig 4. The histologic appearance of FEH. The epitheli- urn is thickened with ballooning or so-called FEH cells showing a mitosis-like aberration.
considerably smaller. Both lesions were excised and the histologic diagnosis was FEH. There was no recurrence after 2 years.
CASE 4
A 39-year-old man with Crohn’s disease presented with lesions on the tongue, which had been present as long as he could remember. He thought that they were a result of chronic tongue biting.
There was a long string of lesions of type 2 on both sides of the tongue. There were ten such lesions on the left side (Fig. 3) and three on the right. One of these was excised and the histologic diagnosis was FEH.
On examination 2 years later, there was no recurrence at the site of the biopsy. There was no change in the remaining lesions.
CASE 5
A 65year-old Laplander had asymptomatic oral lesions for 2 years. The lips demonstrated many type 1 lesions, and similar lesions were seen on the tongue and on the buccal mucosa. These varied between 2 and 10 mm in diameter.
One of them was excised, and a histologic diagnosis of FEH was made.
At follow-up 3 years later, no changes were evident.
CASE 6
A 52-year-old woman presented for evaluation of lesions of the lower lip which had been present for more than 20 years but lately had been esthetically disturbing and had interfered with speech. A radical excision was performed and resulted in paresthesia of the lower lip. There was no recurrence at this site after 9 months.
Clinical examination revealed one lesion of type 2 on the left buccal mucosa and five on the right side of the tongue. The size of the lesions ranged from 2 to 5 mm. A re-examination of the biopsy specimen from the radical operation led to a diagnosis of FEH.
The patient disclosed that one brother and two sisters (Cases 7, 8, and 9) had similar lesions (Table I). These lesions were type 2 in nature.
DISCUSSION
Focal epithelial hyperplasia (FEH) is an unusual disease which often appears in members of the same family. Witkop and Niswander2 discussed a possible genetic factor in the etiology of this disorder, which Cases 6 to 9 may support. The same cases also suggest that FEH is a virus-induced lesion. Perhaps both of these factors, in a concurrent sense, are necessary for the disease to become evident.
The most common location of FEH in the present series was the tongue and its lateral border. This is in agreement with the findings of Ax& Hammar- striim, and Larsson.18 One explanation might be that the lateral border of the tongue is easily traumatized and thus susceptible to viral implantation.
In most cases the lesions had been present for a very long time, in Case 6 for 20 years and in Case 9 for 30 years. The lesions are hardly ever painful, and the patients often did not know of their presence until they became esthetically disturbing or were trauma- tized. Trauma and esthetic effects were considered indications for surgical removal. It has been observed that FEH lesions can disappear spontaneously.’ In Case 1 there were more lesions after 1 year, but after 4 years there were fewer than when the patient was first seen.
Published opinions concerning the effect of surgi- cal treatment and prolonged follow-up are divided. The observation time in the present study was between 9 months and 6 years. No recurrence at the site of the excised lesions was seen, although it appears that the entire lesion must be excised. Extensive surgical intervention, as in Case 6, is not indicated. Only local excision is recommended, and the diagnosis should be confirmed histologically.

Volume 57 Number 5
REFERENCES
1. Archard HO, Heck JW, Stanley HR: Focal epithelial hyper- plasia: An unusual oral mucosal lesion found in Indian children. ORAL SURG 20: 201-212, 1965.
2. Witkop CJ, P&wander JD: Focal epithelial hyperplasia in Central and South American Indians and Ladinos. ORAL
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
SURC 20: 213-217, 1965. March CJ: Multiple papillary tumors of the labial buccal and glossal mucous membrane. Dent Cosmos 23: 165, 188 1. Helms 0: Syfilis i Grdnland. Ugeskr Laeger 5 rk 1: 265-276, 1894. Soneira A, Fonseca N: Sobre una lesion de la mucosa oral en 10s Ninos Indios de la Mision Los Angeles de1 Tokuko. Venez Odontol 29: 109-l 19, 1964. Praetorius-Clausen F: Geographical aspects of oral focal epithelial hyperplasia. Pathol Microbial 39: 204-213, 1973. Bergenholtz A: Multiple polypous hyperplasias of the oral mucosa with regression after removal of amalgam fillings. Acta Odontol Stand 23: 111,.134, 1965. Pindborg JJ: Atlas of diseases of the oral mucosa, ed. 3, Copenhagen, 1980, E. Munksgaard, p. 186. Praetorius-Clausen F: Rare oral viral disorders (molluscum contagiosum, localized keratoacanthoma, verrucae, condylo- ma acuminatum, and focal epithelial hyperplasia). ORAL SURG 34: 604..618, 1972. Axe11 T: Prevalence study of oral mucosal lesions in an adult Swedish population. Odontol Revy Suppl. 36, 1976. Lindeberg, H: Fokal epitelial hyperplasi. Nor Tannlaegeforen Tid 86: 207-210, 1976. Praetorius-Clausen F, Willis JM: Papova virus-like particles in focal epithelial hyperplasia. Stand J Dent Res 79: 362-365, 1971.
Focal epithelial hyperplasia 543
13. Buchner A, Mass E: Focal epithelial hyperplasia in an Israeli family. ORAL SURG 36: 507-511, 1973.
14. Buchner A: Focal epithelial hyperplasia in Israeli families of Libyan origin. ORAL SURG 46: 64-69, 1978.
15. Gomez A, Calle C, Arcila G, Pindborg JJ: Focal epithelial hyperplasia in a half-breed family of Colombians. J Am Dent Assoc 79: 663-667, 1969.
16. Schock RK: Familial focal epithelial hyperplasia: Report of a case. ORAL SURG 28: 598-602, 1969.
17. Thomsson M, Hammarstrijm L: Fokal epitelial hyperplasi. Tandlakartidningen 70: 216-219, 1978.
18. Ax611 T, Hammarstrijm L, Larsson A: Focal epithelial hyper- plasia in Sweden. Acta Odontol Stand 39: 201-208, 1981.
19. Anderson DR: Focal epithelial hyperplasia: Report of a case in a South African Caucasoid. J Dent Assoc S Afr 26: 32-35, 1971.
20. Hollander CF, van Noord MJ: Focal epithelial hyperplasia: A virus-induced oral mucosal lesion in the chimpanzee. ORAL SURG 33: 220-226, 1972.
21. Buchner A, Sandbank M: Multiple fibroepithelial hyperpla- sias of the oral mucosa. ORAL SURG 46: 34-39, 1978.
22. El-Khashab MM, Abd-El-Azis AM: Focal epithelial hyper- plasia (Heck’s disease). ORAL SURC 31: 637-646, 1971.
Reprint requests to:
Dr. G&an Pilgard Department of Oral Surgery University Hospital S-581 85 LinkBping, Sweden


![Endometrium presentation - Dr Wright[1] · Endometrial Hyperplasia Simple hyperplasia Complex hyperplasia (adenomatous) Simple atypical hyperplasia ... Progression of Hyperplasia](https://img.dokumen.tips/doc/110x75/5b8a421e7f8b9a50388bc13d/endometrium-presentation-dr-wright1-endometrial-hyperplasia-simple-hyperplasia.jpg)



















![Hepatic angiosarcoma with an associated focal nodular ... · vascular channels [1,2]. Focal nodular hyperplasia (FNH), on the other hand, is a benign hepatic lesion displaying hepatocytic](https://img.dokumen.tips/doc/110x75/5f05ab797e708231d4141d25/hepatic-angiosarcoma-with-an-associated-focal-nodular-vascular-channels-12.jpg)




