Embed Size (px)
Citation preview

Dr Ralph Diedericks
Emergency Paediatrics
Red Cross Hospital
FLUID THERAPY IN THE
EMERGENCY UNIT
Management of Septic Shock in the
Emergency Unit
Recognition
Initial management
Pathophysiology
Clinical
Goal Orientated Approach
Recent controversy
Resolution


Presentation to Emergency Unit
Severe dehydration with/- hypovolaemic shock
Septic shock
Seizures
Acute Encephalopahty
Acute Severe Respiratory Infection
Metabolic Disease

Initial assessment
TRIAGE
A – AIRWAY
B – BREATHING SATs
C – CIRCULATION
VENOUS ACCESS - RAPID!!
LABS – ABGs, Blood cultures, Elecs , LACTATE etc

Intra osseous Lines
Rapid
Access

Initial assessment
Fluid Balance
Shock/ no shock
Which Fluid?
Circulatory Shock is defined as a failure of the
cardiovascular system to maintain effective tissue
perfusion causing cellular dysfunction and acute
organ system failure if not promptly restored [ Crit
Care Med 2011 Vol 39 ]

Clinical manifestations of Shock Early recognition is essential
Signs of poor tissue perfusion
Prolonged CRT > 2 sec
Low pulse volume, tachycardia
Cool peripheries. Increased toe-core gap
Mottled extremities
Tachypnoea
Measure UO 1-2ml/kg/hr
Impaired LOC – altered mental state
Normal BP ( compensated), hypotension ( uncompensated)

Types of Shock
Hypovolaemic – GIT, burns, trauma
Distributive – sepsis, anaphylaxis
Cardiogenic – pump failure
Obstructive – obstruction to blood flow
Dissociative – inadequate O2 releasing capacity
Clinical features of shock common to all groups

Evaluating haemodynamics
FLOW = perfusion pressure / Resistance
Cardiac Output ≈ SV X Heart rate
CO ≈ MAP – Central venous press/ systemic vasc
resistance
Renal BF = Mean renal art pressure – mean renal
venous press

Effect on Micro circulation
Micro circulation is where oxygen release to tissues
takes place.
Arterioles,venules and capillaries < 100µm diam.
Flow
Blood Flow – determined by cap. Patency, driving
pressure, arteriolar tone
OOO
Oxygen
extraction

Micro circulatory Failure Regulation of micro vasculature – neuro endocrine,
paracrine, mechano sensory pathways.
Can be compromised by:
RBC morpholgy, viscosity
Products of inflammatory response
Coagulation cascade
Neutrophil response
Ince 2011

Effect of Micro circulatory Failure
Carcillo , Clin Ped Emerg Med:
“Shock is a state of acute energy
failure in which there is not enough
ATP production to support systemic
cellular function”
ATP
Failure of Oxygen Delivery
Mitochondrial dysfunction

Acid base status and Lactate
levels
Metabolic acidosis reflects poor tissue perfusion
Lactate levels ( anaerobic metabolism)
- Levels above 2,5 mmol/L associated with
increased mortality
- level of 4,0 mmol/L associated with 27% mortality
rate in septic shock ( cf 2.5%)

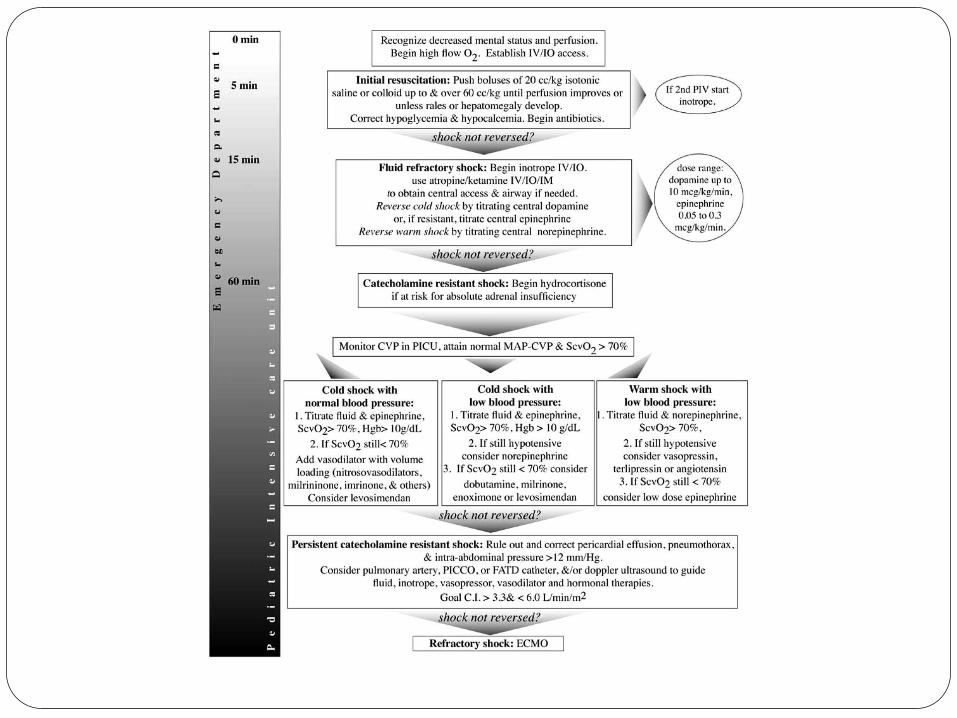
Goal Directed management of Shock
Early recognition and treatment saves lives
Fluid resuscitation
Step wise management in first hour
Han ,Pediatrics 2003,112
Carcillo, Clin Ped Emerg Med 2007
ACCM, Crit Care Med 2009
ETAT


Initial resuscitation
Push boluses of 20ml/kg of isotonic fluid
Up to and exceeding 60ml/kg until perfusion
improves
Watch the liver edge
[ correct hypoglycaemia, commence antibiotics ]
Evidence supports safety and improvements in
outcomes for shock : Septic, hypovolaemic,
Dengue

Which fluid?
Isotonic Crystalloid fluids:
Ringers lactate
Normal saline
Colloid:
SAFE study 2004 – adults
Cochrane 1998

Composition of IV Fluids Fluid Na
Mmo
l/l
Cl K Ca mOsmo
l/l
Glu lactate
N. Saline 154 154 308
Ringers Lactate 131 112 5 1.8 279
Half Dextrose-
Darrows
61 52 17 434 55 27
PMS 35 47 12 372 55
Rehydration Fluid 77 77 432 55
Neonatal Maint 33 33 5 627 110

Chasing the Base deficit? Monitor response to fluid boluses clinically
- CRT
- Pulse vol and rate
- Peripheries ? Warm/cool
- SATs ( continuous measurement)
- BP stable
- Urine output
- LOC , more alert
Avoid treating Blood gas result


Fluid refractory Shock
Begin INOTROPE:
Start Dopamine ( 5-9µg/kg/min) Low dose not effective
Dobutamine ( BP maintained )
Nor Adrenaline ( .05-1 µg/kg/min)
Must have adequate ventricular filling
Dedicated IV line
Continuous monitoring in place, experienced staff
Monitor effects

Intra vascular Volume and Cardiac
Output
0 5 10 15
Ventricle end-diastolic volume
A
B
C
D
Stroke
volume
CO= SV X HR Increase SV:
Inotropes
Vasoactive
drugs
Decrease SV:
Hypoxia, acidosis,
Endotoxin, metabolic


Rescuing the Microcirculation Microcirculatory and Mitochondrial distress
syndrome(MMS)
Monitoring the Microcirculation
- NIRS
- OPS ( Orthogonal polarization Spectral) imaging
Volume
iNOS inhibitors and Steroids
Vaso active and Inotropic support
APC

But what about FEAST?
NEJM 364,26 June 30 2011 FEAST Trial
Designed to investigate the practice of early resuscitation with saline or albumin bolus vs no bolus and
With albumin bolus vs saline bolus
Multi centre – Kenya, Uganda, Tanzania
Enrolled children with febrile illness with red. LOC, respiratory distress with impaired tissue perfusion

FEAST TRIAL
HYPOTENSION – Albumin/saline bolus 40ml/kg.
add 20ml/kg if impaired perfusion at 1 hr
NO HYPOTENSION – Albumin/saline bolus
20ml/kg /no bolus
Add 20ml/kg at 1 hr if still poor perfusion
If hypotension then given 40ml/kg
3170 enrolled, 29 hypotensive , 3141 randomised

FEAST TRIAL
OUTCOME
Mortality at 48 hrs
- 10,6% in albumin bolus
- 10,5 % in saline bolus
- 7,3% in control
NO EVIDENCE SUPPORTING BOLUS FLUID
INFUSION IN ANY SUBGROUP

PROBLEMS WITH FEAST
All children admitted and treated in general paed
ward
No High Care
No PICU
No ventilation
39 % lactate > 5
57% malaria
Excluded gastro enteritis, trauma, burns. All septic
shock
? Micro circulatory failure

Where do we go from here?
FEAST has challenged conventional established
treatment.
Raises issues about safety/ethics
Unexpected outcome, reasons not clear
Need for ongoing research

Concluding comments
Shock needs to be diagnosed and treated early and aggressively
ABC Oxygen is good stuff!
Rapid IV access
Isotonic Crystalloid volume expansion
Use inotropes and vaso active drugs
Think about the Microcirculation
DEFG Rx HYPOGLYCAEMIA!
Antibiotics in first hour

Caution
Watch out for malnutrition
Spare a thought for the Brain CPP= BP – ICP ?
Brain oxygenation better monitoring tool.

Nice to have ?

Essenti
al



Thank You

























