Embed Size (px)
Citation preview

1
Kilimanjaro Christian Medical Centre
FIVE YEAR ROLLING
STRATEGIC PLAN
2015 - 2020

2
FOREWORD
In the year 2013, Kilimanjaro Christian Medical Centre embarked in preparing Strategic Plan.
KCMC Management in this regard is grateful to the Board of Governors, Board of Trustees. the
Consultant and the entire KCMC staff for their constructive and fruitful contributions.
We pray to Almighty God, to continue giving KCMC staff good health, courage and love so that
they continue to serve with humility and dignity for the benefit of patients, students and visitors
who come to KCMC.
Prof. R. M. Olomi
ACTING: EXECUTIVE DIRECTOR, KCMC AND
EXECUTIVE SECRETARY, GSF

3
TABLE OF CONTENTS
CHAPTER ONE ..................................................................................................................................... 4
1.0 Introduction ................................................................................................................................... 5
1.1 Background Information ............................................................................................................... 5
1.2 Strategic Planning Process ............................................................................................................ 7
CHAPTER TWO .................................................................................................................................... 7
2.0 The Vision, Mission, Values and Functions of the Hospital ............................................................ 8
2.1 The Vision ..................................................................................................................................... 8
2.2 The Mission .................................................................................................................................. 8
2.3 Values ........................................................................................................................................... 8
2.4 The Functions ................................................................................................................................ 9
CHAPTER THREE .............................................................................................................................. 10
3.0 Environmental Scanning ................................................................................................................ 10
3.1 General environment ...................................................................................................................... 10
3.2 Global Environment ....................................................................................................................... 10
3.3 National environment ..................................................................................................................... 10
3.4 Institutional level Environment ...................................................................................................... 11
CHAPTER FOUR ................................................................................................................................ 15
4.0 Strengths, Weaknesses, Opportunities and Threats (SWOTs) analysis ......................................... 15
4.1 SWOTS Clinical Services .............................................................................................................. 15
4.2 SWOTs Leadership and management ......................................................................................... 16
4.3 SWOTs Human Resources.......................................................................................................... 17
4.4 SWOTs Financial Resource and sustainability ........................................................................... 18
4.5 SWOTS Infrastructure development ........................................................................................... 19
4.6 SWOTs Hospital equipment and Supplies .................................................................................. 20
4.7 SWOTs Health Management Information System ..................................................................... 21
CHAPTER FIVE .................................................................................................................................. 22
5.0 Strategic Objectives .................................................................................................................... 22
CHAPTER SIX .................................................................................................................................... 31
6.0 Operating plan and Budget ......................................................................................................... 31
6.1 Introduction ................................................................................................................................. 31
6.2 Budget Plan ................................................................................................................................ 31

4
6.3 Budget summary ......................................................................................................................... 31
6.4 Financing sources ........................................................................................................................ 37
ABBREVIATIONS
1. EDR – Executive Director
2. CCFCC – Child Centred Family Care Clinic
3. CPS – Clinical Pastoral Services
4. TATCOT – Tanzania Training Centre for Orthopaedic Technologists
5. CPEP – Continue Paediatric Education Pragramme
6. ENT – Ear, Nose and Throat (Otorhinolaryngology) Department
7. ICU – Intensive Care Unit
8. OPD – Out Patient Department
9. SOP – Standard Operating Procedures
10. CBM – Christoffel Blinden Mission
11. EGPAF – Elizabeth Glasier Paediatric AIDS Foundation
12. GSF – Good Samaritan Foundation
13. KCMU Co – Kilimanjaro Christian Medical University College

5
CHAPTER ONE
1.0 Introduction
1.1 Background Information Soon after Independence of Tanganyika from British rule, the Government called on the
protestant Churches in the Country to establish a referral and teaching hospital in the Northern
zone of the country. Under the leadership of the Right Reverend Stefano R. Moshi, Bishop of the
Evangelical Lutheran Church in Tanganyika, Good Samaritan Foundation (GSF) was established
as a corporate body and registered in Tanganyika in 1961, with Bishop Stefano Moshi as its first
Chairman.
GSF planned for the construction of the Kilimanjaro Christian Medical Centre (KCMC) and
raised large funds from overseas partners to build and equip the hospital.
Therefore, the idea to build Kilimanjaro Christian Medical Centre (KCMC) was born 1961, with
capital funds assured from Luther Hjalpen of Sweden , Central Agency and Bread for the World
of Germany, coupled with an anonymous Christian donation of USD $209,000.00 from Texas,
USA. Site work began in April 1965. The cornerstone for the hospital was laid by the first
President of Tanzania, Julius K. Nyerere, on 8th June 1965.
The project was an integral and essential part of the Tanzania Government's 5-Year Medical
Plan. The Government agreed to contribute annually towards its basic operating costs. In the
overall plan of 1965 there was provision for development, at a later stage of full Medical School.
Kilimanjaro Christian Medical Centre is one among the four Zonal Consultant hospitals in
Tanzania. It was formally established in 1971 as a Zonal Referral Consultant hospital owned by
the Evangelical Lutheran Church of Tanzania (ELCT) under the Good Samaritan Foundation
(GSF). The aim was to create an independent legal body which nevertheless is to be permanently
linked to the ELCT and Christian Council of Tanganyika. The immediate purpose of the
foundation was to be a body capable of establishing the Kilimanjaro Christian Medical Centre.
The referral hospital was established in order to serve the northern, eastern and central zone of
Tanzania. Its record in Medical Services, Research, and Education has significant influence in
East Africa and beyond.
In 2011, KCMC continued to carry out its services to people according to the mission statement,
“To render God’s healing services to set mankind free from the bondage of sickness, suffering
and sin”, “To reflect Christ’s character of love, mercy, compassion and faithfulness in the course
of fulfilling the call to care and heal the sick” and “To share God’s grace and love through the
power of the Holy Spirit in the course of treating and caring for the sick”. Since 1971 the
Hospital has continued to grow, serving the northern, eastern and central zones of Tanzania as a
world-class centre for patient care, teaching and research with leading clinical specialty areas and
an internationally renowned research institute. KCMC has ability to create a culture of
excellence and care and therefore this has made KCMC as an institution where patients want to

6
come for care and staff and trainees want to work. We remain inspired by the dedication of our
founders and we are committed to their vision of providing excellent care, now and in the future.

7
1.2 Strategic Planning Process
Through a participatory process the hospital developed the 2015-2020 Five Year Rolling
Strategic Plan. The development of the Strategic Plan started from the Hospital constituent
key units, which included all stakeholders with participation of the Hospital management
under the leadership of the Executive Director, setting the agenda for brainstorming. Key
result areas were identified and discussed.
This was a done through a series of Strategic Planning workshops.

8
CHAPTER TWO
2.0 The Vision, Mission, Values and Functions of the Hospital
2.1 The Vision
A referral hospital excelling in quality service, training and research
2.2 The Mission
To provide accessible, affordable and high quality health care services
2.3 Values
In order to realize the vision and its mission, KCMC shall be guided by the following values:
Excellence
Excellence and Innovation in Clinical Care, Teaching and Research
Pursue excellence in everything we do with continuous improvements in quality, service and
cost-effectiveness.
Patient-Centred Care
Prioritize safety, quality and the patient experience in everything we do.
KCMC will always regard the patient as the centre of its activities and maintain a patient -
centered hospital environment.
Teamwork
Embrace a collaborative and interdisciplinary approach to clinical care, teaching and research.
Collaboration
Establish internal and external partnerships to integrate and coordinate patient services
effectively.
Respect and Diversity
Value and respect the differences of the patients and families who seek our care as well as those
who provide that care.
Leadership
Promote the development and growth of leaders throughout the organization and continue to
allow our leading programs to export our knowledge nationally and internationally.
Accountability and Transparency
In making decisions and implementation of all activities, KCMC management will observe
openness, team-work, participation, liableness and answerability.

9
Moral Standard and Integrity
In all its undertakings, the KCMC community will uphold and observe accuracy, professional
ethics, honesty, corporate social responsibility and human respect.
Partnerships
KCMC will work very closely with its stakeholders who include staff, students, Government
institutions, NGOs, Civil Society groups, service providers, development partners and other health care
providing institutions, both within and outside the country
Equity
KCMC is an equity observing institution. Thus all sections of the society, especially the
disadvantaged groups and individuals, will be given opportunity to education, training,
recruitment, promotion, decision-making and treatment.
Innovation
In performing the activities related to its core functions, KCMC will attempt to be creative, up to
date and novel
2.4 The Functions The functions and activities of the hospital are guided by the following components of the Mission
1. To provide the public high quality of health care services
2. To provide to the public super-specialized health care services
3. To serve as a centre of excellence for certain specific diseases that can be utilized by local
stakeholders for the development, optimization or implementation of medical interventions and
health policies.
4. To conduct clinical research 5. To train different levels of health cadres

10
CHAPTER THREE
3.0 Environmental Scanning
3.1 General environment The environmental scanning for KCMC includes both external and internal environment. It covers health,
political, social, economic and technological developments and their challenges. In this chapter a number
of pertinent issues at different levels (Global, National and institutional) have been described. As a result
KCMC has an obligation to respond to the resulting dynamics, opportunities and challenges.
3.2 Global Environment Worldwide socio-cultural-economic relations have been intensified by globalization resulting into impact
on health development. Tanzania is faced with a challenge of integration in the competitive areas of
health care delivery on one hand, and international knowledge in scientific and technological
developments on the other hand. KCMC has a responsibility to contributing to the national development
in these areas.
Health delivery The Millennium Development Goals (MDGs) and related global initiatives have refocused global
attention on the challenges facing the world and Africa in particular. For instance the World Health
Organization (WHO) asserts that in order to achieve the MDGs a minimum density of 2.5 health workers
per 1,000 people is required. In Tanzania there is a severe shortage of health workers especially in the
high skilled cadre and the density is estimated to be 1.5. Therefore KCMC as one of the zonal referral and
teaching hospitals in the country has a responsibility to contribute to the national efforts in the attainment
of the health related MDGS.
3.3 National environment
3.3.1 National Economy The country’s economic performance is still poor and a good proportion of the Government budget is
dependent on donor support. As a result Government revenue that could be made available to the health
sector is insufficient compared to the actual demand. This requires new approaches of funding the health
sector. Under these circumstances KCMC community needs to acquire and develop entrepreneurship
skills so as to be able to mobilize resources to cover the budget deficit and meet its recurrent and capital
development budget
3.3.2 The national Health Policy The Tanzania Health Policy has adopted Primary Health care (PHC) as an approach to health
improvement in the country. This policy puts an emphasis on equity in health service, which is responsive
to the needs of the community, especially those who are most at risk. It is geared to address the MDGs
within the National Strategy for Growth and Poverty Reduction (NSGPR) and Vision 2025 which aim at

11
providing access to quality reproductive services, reduction in infant and maternal mortality, raise life
expectancy and reduction of malaria related morbidity and mortality.
NSGPR has identified key obstacles in the provision and access to health care services, which include
shortage of skilled health care providers and poor quality of care, accountability and governance. KCMC
intends to play a positive role in addressing these issues.
KCMC will endeavor to address the problem of poverty reduction impediments by offering high quality
service to the population and by increasing the number and diversity of highly trained health care
providers and managers of health care systems. KCMC will also continue to give high priority to research
activities that aim at improving care and reducing the burden of most prevalent diseases in Tanzania.
3.3.3 Political Environment The orientation of political environment in the country is towards effective and greater democratization
and pluralism. The Government agenda of ensuring good governance is applied in all institutions. KCMC,
though a faith based institution has an obligation to practice good governance just as it is done in the
public institutions.
3.4 Institutional level Environment
3.4.1 Institutional Governance
Based on the organizational structure of KCMC, the institution is headed by the Executive
Director who is answerable to the Good Samaritan Foundation (GSF) Board of Trustees. The
Executive Director serves also as the Executive Secretary of GSF. Under the Executive Director
are Directors of different units and under them are Heads of Departments.

12

13
3.4.2 Human resource Development and Management
Human resource is an important element for institutional development. The Directorate of
Human Resources is concerned with supervising and coordinating departmental heads of general
administration and personnel in Managerial matters. It also implements Personnel Development
Plan as well as recommending and advising management on training policy and available
training opportunities.
3.4.3 Financial Resources and Management
The source of funding of the hospital is mainly from the Government, Cost sharing, GSF and
donations.
KCMC has an established financial management structure. The Finance Directorate is
comprising of five departments namely Revenue, Salaries, Expenditure, Projects and Final
Accounts.
3.4.4 Training
Training is one of the core functions of KCMC. The hospital currently is hosting 16 Allied
Health Schools which are owned by the MoHSW. These Schools offer different
disciplines/specialties in both certificate and diploma levels. The KCMU Co uses KCMC as a
teaching hospital.
3.4.5 Research Development and Management
Research is one of the core functions of KCMC. Through the Kilimanjaro Clinical Research
Institute (KCRI) KCMC has managed to harmonize health services, health training and health
research. This unique practice of harmonizing patients’ care, training of health professionals and
conducting health research without jeopardizing patients’ health and well-being is well
structured through the establishment of well-defined functions of the KCMC hospital, the
University Medical College (KCMU – College).
3.4.6 Links and Networking
KCMC has always had links with various partners both locally and internationally.
Through these links it has been able to fulfill its mission.
3.4.7 Infrastructure Development and other Support facilities
The hospital started functioning in 1971 However, it has continued to expand for example
establishment of the Orthopaedic Rehabilitation Unit, Dermatology and Burns Unit, Child

14
Centred Family Care Clinic and Emergency Medicine. The other planned expansion areas
include establishment of the Orthopaedic Centre for Excellence and Cancer Unit.
3.4.8 Public Relations
In order to remain competitive KCMC has to device novel ways of conducting its business.
Through the Unit of Public Relations the hospital has continued to maintain its good relationship
with all key stakeholders/parties i.e. government, political leaders, donors, other hospitals and
the surrounding communities.
3.4.9 Gender issues
In order to address issues pertaining gender, the hospital has created a gender desk with a
coordinator and a counselor. Gender policy and guidelines for anti- sexual harassment and
discrimination are still in process of preparation. Nevertheless, the hospital needs to expand the
gender activities.

15
CHAPTER FOUR
4.0 Strengths, Weaknesses, Opportunities and Threats (SWOTs) analysis
4.1 SWOTs Clinical Services
4.1.1 Strengths 1. Unique Clinical Departments and Services (Dermatology, CCFCC, Orthopaedics,
Research laboratory, Endoscopy Services CT-Scan, Mammography)
2. Unique Clinical Services (Paediatric Urology, Clinical Pastoral services (CPS), Birth
registry, TATCOT
3. Training of Specialists
4. Networking with other hospitals e.g. Flying Doctors Services, CPEP
5. Community Ophthalmology
6. Indigenous Specialists who know the local conditions well
7. Existing Post Graduate Seminars twice a year
8. Existing of clinical conferences every Wednesday
9. Nurses continuous education weekly and annual conference

16
4.1.2 Weaknesses 1. Shortage of Staff (ENT, Anaesthesia, Radiology, Dermatology. And Nurses in all
Departments,)
2. Inadequate space in the patient wards e.g. Surgical, Clinics Casualty, Diabetic and
offices (Mainly a cross cutting issue )
3. Inadequate supplies
4. Shortage of specialists and super speciality e.g. –Cardiologist, Neurologists,
Haematologist, Pathologists, Endocrinologists, Nephrologists, Oncologists, ICU nurses
5. Poor Patient flow
6. Lack of 24 hours OPD Services
7. Shortage of Equipments e.g. Autoclaves, Ventilators, MRI,
8. Lack of SOPs and Protocols
9. Misallocation of staff e.g. Pathology
10. Lack of Disaster Emergency preparedness e.g. assembly hall
11. Ineffective Laboratory support services
12. Poor system of accessibility of staff for emergency on call rooms, transport, residence
house
13. 0vercrowding of students
14. Poor Referral System
15. Lack of effective Retention Program for staff
16. Shortage of Funds
17. Standards not validated
4.1.3 Opportunities 1. Well established services known inside and outside the country
2. Support from the Ministry
3. Existing collaborations e.g. Duke, CBM, EGPAF
4. Ongoing resource services support from ministry
5. International collaboration
4.1.4 Threats 1. Inadequate government funds
2. Donors dependency
3. Exodus of staff e.g. laboratory technicians, Nurses,
4. Inability to keep pace with modern equipment e.g. CBC
4. Unprepared for internal competition e.g. East African Community
4.2 SWOTs Leadership and management
4.2.1 Strengths 1. Existence of well structured organogram of leadership
(EDR, Directors, Heads of Departments)
2. Unification of directorates of College, Research and Clinical entities under the overall
leadership of EDR
3. Existence of top governing bodies i.e Board of Governors and Board of trustees

17
4. Good relationship between KCMC and government through Ministry of Health and
Social Welfare
5. Existence of hospital managerial committee
(Hospital Management Team/Committee)
6. Availability of several (27) operational committees
7. Availability of legitimate health workers, academic staff, and students’ welfare
committees
8. Existence of internal hospital policies e.g patient/client charter
9. Availability of job description of various cadres.
10. Availability of statutory laws and regulations for KCMC employees
11. Availability of job description of various cadres.
12. Existence of ALMANAC
4.2.2 Weaknesses 1. Lack of Planning Unit
2. Lack of Quality Assurance unit
3. Overlapping of functions in certain committees
4. Lack of other important Staff welfare Policies: e.g
Anti- sexual harassment, Gender policy, retirement policy, staff establishment policy
5. Lack of job description for doctors
6. Lack of induction/orientation course for newly employed staff
7. Reception of unskilled foreign staff
8. Reception of unwanted/worn out materials
9. Reception of unregistered/unrecognized foreign groups from their country of origin.
4.2.3 Opportunities 1. Representation of Ministry of Health and Social Welfare (MoHSW) in the Board of
Governors and Board of Trustees
2. Integration of Hospital with external faith based institutions.
4. Government support through remittance of funds (salaries), provision of drugs and
placement of health staff
5. Financial, human and material support from foreign collaborators/partners
4.2.4 Threats 1. Overdependence on MoHSW and donors’ support
2. Human right advocacy institutions
3. Certification by MoHSW regulatory bodies
4. Collaborators/partners dependence
5. Unemployment of indigenous staff
4.3 SWOTs Human Resources
4.3.1 Strengths 1. Existence of specialized health professionals
2. Existence of training institutions
3. Having local employees who are familiar with the working environment

18
4. Existence of a programme for recognition and rewarding employees at all levels for good
performance
5. Involvement of employees in various decision-making organs
6. Reliable source of staff salaries
7. Existence of super specialities (Urology, ENT)
8. Existence of unique specialties (TATCOT)
4.3.2 Weaknesses 1. Overdependence on staff from the Government through the Ministry of Health and Social
Welfare
2. Big proportion of aged staff
3. Non existence of succession plan
4.3.3 Opportunities 1. Availability of training institutions within the hospital.
2. Combination of patient care, training and research activities under one roof.
3. Training avenues.
4. Availability of enough land for expansion
5. Good – will by Government and other stakeholders
8. Society demand for specialized services in health.
12. Existence of International Collaboration programmes.
13. Big catchment area to offer referral services
4.3.4 Threats 1. Change of policy.
2. Donor/Government dependency
3. Society demand for specialized services in health.
4. Brain drain due to inadequate staff remuneration and retirement benefits
5. Upgrading of regional hospitals to become referral hospitals.
6. Establishment of private hospitals offering health services.
7. HIV/AIDS pandemic
4.4 SWOTs Financial Resource and sustainability
4.4.1 Strengths 1. Cost sharing as source of revenue
2. Government funding
3. Collaboration with Insurance companies (e.g. National Health Insurance)
4. Existence of some viable GSF projects
5. Existence of three pillars, patient care, training and research attracts more research
funding
6. Existence of research projects which remit to KCMC overhead funds
7. Funds from specialized and unique services
8. Introduction of accounting package WEBERP and Care2x
9. Existence of land which can be used as collateral for sourcing of investment funds

19
4.4.2 Weaknesses
1. Terms and conditions for insurance services not favorable to KCMC
2. Reliance on government funding
3. GFS projects operate on service oriented rather than commercial bases.
4. Uncompleted research registry
5. Specialized and unique services not fully utilized on commercial bases eg fast track
services.
6. Weak internal audit in terms of resources (staffing and qualified personnel)
7. Weak internal control systems (reconciliation, documentation, authorization, timely
preparation of books of accounts, revenue controls)
8. The current accounting system not able to capture all finance related data. It is manually
done
9. Failure to utilize current ICT development
10. Inadequate budget. Control mechanisms (Budgeted expenditure. Vs actual)
11. Non adherence to procurement plan
12. Failure to optimize and utilize land, including investment appraisal mechanism.
13. Low level cost containment awareness.
4.4.3 Opportunities
1. Provision of grants from government
3. Ready market for projects if operated on commercial basis
4. Reputation of KCMC to major funders such as EDTCP, EU
5. Existence of donor funded projects.
7. Existence of financial institutions to extend loans for investment
8. Exemption from tax being faith based institution, assist our cash flow.
4.4.4 Threats
1. Change in government policy/MoU
2. Disparity between requested budget vs approved budget (approximately 30%)
3. Untimely remittance of funds
4.5 SWOTS Infrastructure development
4.5.1 Strengths 1. Availability of adequate land with title deed
2. Availability of Structured hospital buildings.
- Wards
-Service laboraties
-Hostels.
-Residential houses.
-Offices.
-Lecture/ Seminar halls
3. Availability of adequate water supply
4. Possibility of sharing infrastructure

20
5. Availability of dedicated electric supply and backup system
6. Availability of ramp and elevators
7. Availability of functioning internal communication system
8. Availability of central sewage system.
4.5.2 Weaknesses 1. Land is not physically protected/fencing
2. Inadequate space;
-Wards.
-Emergency department.
-Offices.
-Stores.
-Car parking.
-Laboratory rooms.
3. Buildings have not been renovated for a long time
4. Reliance on a single source of water
5. Lack of infrastructure development plan and implementation
6. Unstable power supply -Standby generator does not cover the whole hospital
4.5.3 Opportunities 1. Government and donor support
2. Suitable geographical location
4.5.4 Threats
1. Over dependence and change of interest of donors /Government
2. Unstable national economy
4.6 SWOTs Hospital equipment and Supplies
4.6.1 Strengths 1. Availability of hospital formulary list
2. Availability of annual procurement Plan
3. The zonal medical store is within the catchment area
4. Existence and use of tendering system
5. Availability of hospital equipment donations
6. Support from Ministry of Health and Social Welfare
7. Availability of ICT equipment
8. Availability of orthopaedic workshop
9. Existence of local production of intravenous fluids and additives e.g spinal anaesthesia
and local anaesthetics
10. Existence of local production of extemporaneous preparations. e.g dermatological and
oral solutions for paediatric
11. Existence of categorized storage space
12. Existence of proper system of documentation
13. Availability of oxygen and Nitrogen Plants

21
4.6.2 Weaknesses
1. Irrational prescribing
2. Poor disposal of expired medicines, medical supplies and equipment
3. Lack of Hospital equipments planned preventive maintenance
5. Poor specification of equipments and supplies
6. Donation guideline not used
7. Inadequate equipments and supplies
8. Inconsistence allocation of funds for purchase of equipments and supplies
9. Inadequate ICT facilities
10. Low production rate of wheelchair and Prosthetic materials
11. The machine for local production of intravenous fluids and additives is very old
12. Unavailability of ingredients for Local production of extemporaneous preparations. e.g
dermatological and oral solutions for paediatric.
13. Dead stock generation eg. Vaccines, laboratory reagents and some equipment
14. Lack of reliable transport system
15. Loss/poor feedback on drugs, equipments and supplies.
4.6.3 Opportunities 1. Guaranteed support of funding from ministry of Health and Social welfare
2. Collaboration with various collaborators
3. High profile of KCMC as an Institution
4. Availability of funds from cost sharing, NHIF and Donors
5. Sharing of resources with other hospitals e.g. Sterilization of equipment
4.6.4 Threats 1. Lack of sustainable funding
2. Fluctuation of foreign currency
3. Over dependency on government funding
4. Change of Government policy
4.7 SWOTs Health Management Information System
4.7.1 Strengths 1. Existence of professionally designed filing system (6 digit coding system)
2. Functioning patient file location system
3. Existence of the only medical records training school in the country
4. Presence of physical space
5. Presence of trained indigenous personnel
6. Existence of medical archives
7. Possibility of access to patient data for research
8. Regular production of reports on regular basis
9. Data entry and analysis mechanisms in place
10. Dissemination mechanism in place
13. Existence of a solid and continuous patient folder reference mechanism

22
4.7.2 Weaknesses 1. Manual filling system which is labor intensive and needs a large physical space
2. Patient filling system is manual thus difficult to retrieve
3. Medical records training school is small with small intakes. It offers certificate training
only
-Outdated curriculum
-Being the only school in Tanzania, minimizes comparative competence
4. Space for medical records is small
5. Small number of Tanzanian students on training the rest being foreign
6. Inadequate archive management system
7. For medical records real time statistical analyses is not done
8. No emergency reporting mechanism
9. Absence of standardized data entry and analysis strategy
10. Unclear dissemination system
-data utilization not properly planned
11. Unguaranteed patient confidentiality
4.7.3 Threats 1. Rapid change in ICT technology
2. Similar Web based, distance learning programs by other institutions
3. Current archive is vulnerable to fire, rainfall etc
CHAPTER FIVE
5.0 Strategic Objectives The strategic objectives have been developed based on the environmental scanning and the
SWOT analysis which reflect the current status of the Hospital and the factors that would
positively or negatively influence its development.
The seven key result areas which have been considered are:
1. Clinical services
2. Leadership and management
3. Human Resources
4. Financial resources and sustainability
5. Infrastructure development
6. Hospital equipment and supplies
7. Health management information system
Strategic Objective No 1: Improved Quality of Clinical services
The competitive environment with which the Hospital operates demands quality performance in its core
function of patient care. In order to ensure quality delivery of services the hospital needs to improve its
specialist patient care. This strategic objective is geared towards achieving this goal.

23
Targets
1. Hospital social welfare services provided to all needy patients by June 2015
2. A continuous quality improvement program strengthened by June 2015
3. Compliance with national standards and guidelines improved by June 2015
4. An acceptable level of staff competences in providing quality services achieved by June
2016
5. Emergency preparedness ensured by December 2015
6. Rational prescribing of drugs ensured by July 2015
7. Timely availability of supplies ensured by July 2015
Strategies 1. Develop Hospital policy and guidelines for social welfare services
2. Adopt and implement the 5s-CQI-TQM in each clinical department
3. Update the hospital formulary annually and regularly and provide prescribers with information on
drugs available
4. Institute regular clinical audit
5. Put in place disaster preparedness plans
6. Conduct disaster preparedness exercises regularly
7. Train staff in disaster management
8. Run short courses for prescribing of drugs for doctors
9. Ensure the implementation of annual procurement plan
10. Strengthen procurement process
Performance indicators 1. Proportion of hospital days due to waiting for social services (repatriation, exemptions)
2. Proportion of referred upcountry patients exempted from paying fees
2. Proportion of staff trained in 5s-CQI-TQM in each department
3. Number of functioning Quality improvement teams in the hospital
4. Proportions of clinical departments attaining step 5 (sustain/self discipline)
5. Client/Patient satisfaction rates
6. 95% of prescriptions are appropriate
7. Proportion of meetings of Hospital Therapeutics Committee
8. List of drugs not available issued fortnightly
9. Client/patient satisfaction rates
10. Hospital mortality rates/case fatality rates reduced by 20%.
11. Average duration of hospital stay less than 8 days on average
12. Proportion of unnecessary and rejected requests for laboratory investigations reduced by 50%
13. Re-attendances as a proportion of all full consultancy episodes

24
14. Proportion of patient files with proper specialist documentation
15. Proportion of admissions seen by a specialist before discharge
16. Outpatient consultations of at least 6 new cases and at least 10 follow-up per specialist clinic
17. Referrals from wards as % of all outpatient visits
18. Laboratory tests per outpatient visits
19. Proportion of discharge forms fully and accurately completed in Jeeva System
20. Proportion of patients who receive medication on time
21. Patient re-operation rates
22. % of elective surgeries without postoperative infections and complications
23. Number of trained staff
Strategic Objective No 2: Enhanced Institutional Governance and
Management
KCMC has a well structured organogramme of leadership with relevant committees. There exist
also top governing bodies (Board of Governors and Board of Trustees). However, certain
important units and policies are lacking. These would greatly enhance the governance and
management of the hospital. This objective is designed to facilitate improvement in governance
and management.
Targets
1. Directorate of planning and Development Established by June 2015
2. Institutional management team trained on leadership and management skills by July 2015
3. External links unit established by June 2015
4. Institutional policies developed by December 2015
5. Board of Governors, Board of Trustees, Institutional Committees Strengthened
6. MoU between and GSF reviewed and updated
7. Number of HMI system personnel increased by 50% by December 2015
8. All of HMI system personnel on electronic HMI system trained by June 2015
9. HMI system physical infrastructure refurbished by June 2015
10. Electronic HMI system established by August 2015
11. Number of students in school of medical records increased by 100% by September 2015
12. Diploma course in Medical Records introduced by September 2015
Strategies
1. Prepare a write up of Establishment of Directorate of planning and development
2. Locate space for the directorate of Planning and Development
3. Employ staff for the Directorate of Planning and Development
4. Develop anti sexual harassment policy
5. Develop gender policy

25
6. Develop recruitment , retention and retirement policy
7. Develop staff establishment policy
8. Provide office for the links unit
9. Recruit links office staff
10. Develop data base for external links
11. Review tenure, roles and responsibilities, composition of staff
12. Increase number of personnel through employment of new graduates from the school of medical
records
13. Conduct training on advanced ICT utilization
14. Organize on-job training on use of electronic HMI system e.g. care 2X
15. Restructure and refurbish the current physical infrastructure to support both manual and
electronic HMI systems
16. Develop SOPs for HMI system (data entry, analysis, reporting and dissemination)
17. Establish quality assurance and control system
18. Acquire ICT facilities
19. Install appropriate HMI system software
20. Acquire modern learning aids (audio-visual systems, computers etc)
21. Advertise the school made widely
22. Develop curriculum for diploma programme in medical Records
23. Negotiate for the programme to be registered under the KCMC University College
Performance indicators 1. Directorate of planning and Development
2. Head personnel of the Directorate of Planning and Development
3. Anti sexual harassment Policy
4. Gender Policy
5. Staff establishment policy
6. Data base
7. Regular meetings
Strategic Objective No 3: Enhanced Human Resources Management
The hospital human resource consists of mostly staff seconded from the Government. The government
will second only staff requested by the hospital. Once staff is seconded to the hospital, it is its
responsibility to see to it that the staff are enabled to work properly and well motivated. Currently the
necessary tools to that end are lacking. Therefore KCMC needs to put in place the necessary mechanisms
for that. This strategic objective is designed to enhance recruitment, retention and motivation of staff at
the hospital.
Targets
1. Human resource development plan developed by December 2015

26
2. Job descriptions for all staff operationalized by December 2015
3. Performance management System established by January 2016
4. Staff retention improved by June 2015
5. Number of various specialists increased by June 2015
6. Human Resources policies operationalized by December 2015
7. Effective Human resource Information Health system developed by December 2016
8. An acceptable level of staff compliance with national guidelines and standards achieved
by June 2017
Strategies
1. Do Situational analysis of the existing staff
2. Apply job description
3. Review the current staff scheme of service and promotion guidelines
4. Operationalize the reviewed staff promotion guidelines
5. Improve the existing general working environment
6. Develop an attractive loan/credit scheme for staff
7. Involve staff in decision –making process
8. Improve the existing employees’ induction/ orientation process.
9. Review and update the existing Staff and training regulations.
10. Recruit various specialists to increase their number from 60 to 120
11. Train various specialists for deficient specialties
12. Establish recreational facilities for staff
13. Maintain an updated database of all staff
Performance indicators
1. Human resource needs identified
2. Recruitment plan prepared
3. Staff training and development plan in place
4. Job description
5. Linkage between staff annual review and staff promotion
6. Number of specialists
7. Worker’s participation in decision making
Strategic Objective No 4: Enhanced financial capability, efficiency and
sustainability
KCMC although a faith-based institution, largely depends on Government and Good Samaritan
Foundation (GSF) funding to carry out its core functions. However, these sources of funding are
also constrained. KCMC therefore needs to develop mechanisms that will ensure that the funds

27
are utilized in an efficient and sustainable way. The strategic objective is designed to ensure
rational utilization of available funds at the centre.
Targets
1. Internal audit department strengthened by Jan 2016
2. Accounting software (WebERP) operationalized fully by Dec 2016
3. Internally generated income improved by June 2015
4. Accounting and procurement manuals established by January 2017
5. Internal control systems improved by Dec 2016
6. Government funding level increased to 40% from current level (30%) by May 2016
7. Revenue unit strengthened by November 2016
8. Expenditure unit strengthened by November 2016
9. Budget unit established by November 2015
10. Procurement unit strengthened by November 2016
11. Inventory unit established by December 2016
Strategies
1. Recruit more professional and competent internal audit staff at least one Senior Internal Auditor
and three Assistant Senior internal Auditors
2. Provide capacity building (continuing education) to Auditors
3. Establish Audit Committee
4. Develop internal Audit Manuals
5. Purchase audit software and ICT equipment
6. Provide office space for internal audit unit
7. Encourage staff to use WebERP
8. Conduct cost benefit analysis for internally income generating projects
9. Draft accounting and procurement manuals
10. Review the current internal control systems
11. Negotiate with government to increase funding level
12. Head of the unit appointed
10. Qualified receiving and paying cashiers employed
11. Strong room built
12. Cash office grilled
13. Clearly defined authorization mechanism established
14. Provide office space for Budgeting unit
15. Recruit staff ( Management accountant)
15. Head of the inventory unit employed
16. Qualified staff employed for inventory unit

28
Performance indicators 1. Efficiency of audit unit
2. Audit committee
3. Internal Audit manuals
4. Amount of internally generated funds
5. Funding from Government
6. Funding from GSF
7. Expenditure
8. Budgeting
9. Procurement
10. Inventory of hospital property
Strategic Objective No 5: Developed and maintained Hospital infrastructure
Most of the infrastructure at the hospital dates back to 1971 when it was established. Since then some
buildings have been added and sporadic rehabilitation of some of the buildings has been done. However,
systematic care of the infrastructure has been lacking. This strategic objective therefore is designed to
ensure that proper units and systems are in place to oversee proper care of the hospital infrastructure.
Targets
1. Estate Department improved by July 2016
2. Existing Infrastructure rehabilitated by July 2018
3. Water supply system improved by December 2017
4. Power supply improved by June 2017
5. Maintenance systems strengthened by July 2016
6. Communication and information systems improved by December 2015
7. Administration block constructed by June 2019
8. Clinical wards expanded by December 2019
9. Hospital feeder roads improved by 2019
Strategies
1. Separate instrument repair laboratory from Estates Department
2. Repair all hospital buildings
3. Paint all hospital buildings
4. Put in place second source of water supply
5. Seek from TANESCO exemption from power rationing
6. Put in place mechanisms of reduction of power consumption
7. Rehabilitate internal telephone communication system
8. Prepare architectural drawings for the new administrative block
9. Solicit funds for Administrative block construction

29
10. Prepare architectural drawings for the new clinical wards
11. Solicit funds for clinical wards construction
12. Rehabilitate all the hospital feeder roads
Performance indicators
1. Well organized and efficient estates department
2. Condition of hospital buildings
3. Condition of hospital feeder roads
4. Availability of water supply
5. Availability of electrical power supply
6. Telephone internal communication system
7. Administration block
8. New clinical wards
Strategic Objective No 6: Ensured availability of Hospital equipment
KCMC is currently equipped with a mixture of equipment some being new while others are old. There is
no system of ensuring that there is adequate and updated equipment. This strategic objective is designed
to ensure adequacy of equipment at KCMC hospital.
Targets
1. Central workshop strengthened by July 2016
2. Planned Preventive Maintenance (PPM) for hospital equipment developed by July 2015
3. All old machines replaced with new ones by July 2019
4. Production of locally manufactured equipment and supplies increased by July 2019
Strategies
1. Procure equipment for the central workshop
2. Solicit funds for renovation of central workshop to carter for hospital equipment
maintenance
3. Employ and train technical staff
4. Prepare a write up for Planned Preventive Maintenance (PPM) for hospital equipment
5. Establish replacement policy of old machines/equipment
6. Acquire new and modern equipment
7. Optimize production skills for local products
8. Set production targets
9. Strengthen the local production of infusions
Performance indicators
1. New equipment

30
2. Renovated central workshop
3. Locally produced infusions
Strategic Objective No 7: Enhanced Response among staff towards HIV and
AIDS Prevention, Treatment and care
HIV and AIDS is a global health problem which has affected all sectors of service delivery. KCMC as
one of the health care delivery institutions has the responsibility to put in place mechanisms for
prevention and control of the pandemic at the work place.
Targets
1. HIV and AIDS control activities strengthened at KCMC by July 2015
2. HIV and AID research and consultancy strengthened by July 2015
Strategies
1. Strengthen the KCMC Technical AIDS subcommittee
2. Operationalize the KCMC HIV and AIDS Policy
3. Support the existing HIV and AIDS prevention and control activities
4. Support and participate in the National intervention for voluntary counseling and
testing
5. Establish KCMC HIV and AIDS situation at KCMC
6. Support research and consultancy on HIV and AIDS
Performance indicators
1. Technical AIDS subcommittee
2. Research and consultancy on AIDS
3. Situation analysis
4. Voluntary counseling and testing
5. Prevention and control

31
CHAPTER SIX
6.0 Operating plan and Budget
6.1 Introduction This strategic plan is based on the KCMC vision and mission. In order to achieve this, KCMC has
developed novel approaches in the implementation of its core functions. The strategic plan has taken into
account that service delivery to the public has to be improved in a sustainable way.
6.2 Budget Plan This budget focuses on the recurrent costs, capital and research development.
The operational plan and estimated budget has been prepared with the following assumptions:
1. The rate of inflation will remain constant and therefore for the whole period of the five-year plan
prices will remain reasonably stable
2. Availability of continued Government support and development partners
6.3 Budget summary The table below summarizes the targets of the main strategic objectives and the estimated budget for
implementation
Figures (x1000)
Strategic Objective No 1: Improved Quality of Clinical
services
2015/16 2016/17 2017/18 2018/19 2019/20
Target 1 Hospital social welfare services provided to all
needy patients by June 2015
50,000 0 0 0 0

32
Target 2 A continuous quality improvement program
strengthened by June 2015
20,000 0 0 0 0
Target 3 Compliance with national standards and
guidelines improved by June 2015
0 0 0 0 0
Target 4 Acceptable level of staff competences in providing
quality services achieved by June 2015 20,000 0 0 0 0
Target 5 Emergency preparedness ensured by December
2016
0 0 0 0 0
Target 6 Rational prescribing of drugs ensured by July 2016
0 0 0 0 0
Target 7 Timely availability of supplies ensured by July
2015
0 0 0 0 0
SUBTOTAL 90,000 0 0 0 0
Strategic Objective No. 2: Enhanced Institutional
Governance and Management
2015/16 2016/17 2017/18 2018/19 2019/20
Target No. 1 Directorate of planning and Development
Established by July 2015
20,000 0 0 0 0
Target No. 2 Institutional management team trained on
leadership and management skills by July 2015
20,000 0 0 0 0
Target No. 3 External links unit established by June 2015
0 0 0 0 0
Target No. 4 Institutional policies developed by December
2015
20,000 0 0 0 0

33
Target No.5 Board of Governors, Board of Trustees,
Institutional Committees Strengthened by June 2015
0 0 0 0 0
Target No. 6 MoU between KCMC and GSF reviewed and
updated by June 2015
0 0 0 0
Target No.7 Number of HMI system personnel increased by
50% by December 2015
20,000 0 0 0 0
Target No.8 All of HMI system personnel trained by June
2015
20,000 0 0 0 0
Target No.9 HMI system physical structure refurbished by
June 2015
20,000 0 0 0 0
Target No. 10 Electronic HMI system established by
August 2015
20,000 0 0 0 0
Target No. 11 Number of students in school of medical
records increased by 100% by September 2015
0 0 0 0 0
Target No. 12 Diploma course in Medical Records
introduced by 2015 0 0 0 0 0
SUBTOTAL
140,000 0 0 0 0
Strategic Objective No 3: Enhanced Human Resources
Management
2015/16 2016/17 2017/18 2018/19 2019/20
Target No.1 Human resource development plan developed
by December 2015
20,000 0 0 0 0
Target No.2: Job descriptions for all staff operationalized
by December 2015 0 0 0 0 0

34
Target No.3: Performance management System established
by January 2016
5,000 0 0 0
Target No.4: Staff retention improved by June 2015
0 0 0 0 0
Target No.5: Number of various specialists increased by
June 2015
50,000 0 0 0 0
Target No.6: Human Resources policies operationalized
by December 2015
0 0 0 0 0
Target No.7: Effective Human resource Information Health
system developed by December 2016
20,000 0 0 0 0
Target No.8: An acceptable level of staff compliance with
national guidelines and standards achieved by June 2017
5,000 5,000 0 0 0
SUBTOTAL 100,000 5,000 0 0 0
Strategic Objective No 4:Enhanced financial capability,
efficiency and sustainability
2015/16 2016/17 2017/18 2018/19 2019/20
Target No.1: Internal audit department strengthened by
Jan 2016
5,000 0 0 0 0
Target No.2: Accounting software (WebERP)
operationalized fully by December 2016
0 0 0 0 0
Target No. 3: Internally generated income improved by
December 2016 0 0 0 0 0

35
Target No.4: Accounting and procurement manuals
established by January 2017
5,000 0 0 0 0
Target No. 5 Internal control systems improved by
December 2016 0 0 0 0 0
Target No. 6 Government funding level increased to 40%
from current level (30%) by May 2015
0 0 0 0 0
Target No.7: Revenue unit strengthened by December 2016
5,000 0 0 0 0
Target No 8: Expenditure unit strengthened by November
2016
0 0 0 0
Target No.9: Budget unit established by November 2015
5,000 0 0 0 0
Target No10: Procurement unit strengthened by November
2016
5,000 0 0 0 0
Target No.11: Inventory unit established by December 2016
5,000 0 0 0 0
SUBTOTAL 30,000 0 0 0 0
Strategic Objective No 5: Developed and maintained
Hospital infrastructure
2015/16 2016/17 2017/18 2018/19 2019/20
Target No.1: Estate Department improved by July 2016 30,000 20,000 0 0 0
Target No.2: Existing Infrastructure rehabilitated by July
2018
500,000 300,000 200,000 100,000 0
Target No.3: Water supply system improved by December
2017 50,000 30,000 20,000 0 0

36
Target No.4: Power supply improved by June 2017
30,000 20,000 20,000 0 0
Target No.5: Maintenance systems strengthened by July
2016
20,000 20,000 0 0 0
Target No.6: Communication and information systems
improved by December 2015
50,000 0 0 0 0
Target No.7: Administration block constructed by June
2019
300,000 200,000 100,000 100,000 50,000
Target No.8: Clinical wards expanded by December 2019
300,000 50,000 20,000 20,000 20,000
Target No. 9: Hospital feeder roads improved by 2019
100,000 50,000 20,000 20,000 20,000
SUBTOTAL 1,360,000 690,000 380,000 240,000 90,000
Strategic Objective No 6:Ensured availability of
Hospital equipment
2015/16 2016/17 2017/18 2018/19 2019/20
Target No.1: Central workshop strengthened by July 2016
30,000 30,000 0 0 0
Target No.2: Planned Preventive Maintenance (PPM) for
hospital equipment developed by July 2015
30,000 0 0 0 0
Target No.3: All old machines replaced with new ones by
July 2019
500,000 0 0 0 0
Target No. 4: Production of locally manufactured
equipment and supplies increased by July 2019 20,000 0 0 0 0
SUBTOTAL 580,000 30,000 0 0 0

37
Strategic Objective No 7:Enhanced Response among
staff towards HIV and AIDS Prevention, Treatment and
care
2015/16 2016/17 2017/18 2018/19 2019/20
Target No.1: HIV and AIDS control activities strengthened
at KCMC by July 2015
5,000 0 0 0 0
Target No.2: HIV and AID research and consultancy
strengthened by July 2015
5,000 0 0 0 0
SUBTOTAL 10,000 0 0 0 0
GRAND TOTAL 2,310,000 725,000 380,000 240,000 90,000
GRAND TOTAL BUDGET FOR FIVE YEARS 3,745,000,000
6.4 Financing sources KCMC will depend on the Good Samaritan Foundation, Government, donor support and internally
generated funds to finance the Five year Rolling Strategic Plan

38
CHAPTER SEVEN
7.0 Implementation Framework, Monitoring and Evaluation
7.1 Introduction
Monitoring and Evaluation of the KCMC Five-Year Rolling and Strategic Plan is designed to
ensure effective and efficient implementation of the plan and sustainability of the intended
impacts. It is presented as a review mechanism to monitor the progress and appraise outcomes
compared to the original objectives, targets and expected results.
7.2 Implementation
The KCMC Management is responsible for the implementation of the Five-Year Rolling and
Strategic Plan. In order to increase efficiency and effectiveness, the Directorate of Planning shall
coordinate all the activities related to the implementation of the plan. The implementation shall
be realized through annual plans and budgets, where departments and Units will prepare their
plans and budgets in line with the KCMC-wide strategic plan.
The Directorate of Planning, on the basis of the individual Departments and Units Plans will
prepare a KCMC – level annual work plan (operational plan) to guide the implementation of the
Five-Year Rolling and Strategic Plan. This will show all the activities to be implemented by
KCMC and its units.
Each key officer responsible for the implementation of a specific activity will be expected to
observe the anticipated targets together with the time frame and resources required.
7.3 Monitoring
A monitoring and evaluation system is required to measure and evaluate the level of
implementation, performance, achievement and impact of the strategic plan.
Monitoring of the implementation will be the overall responsibility of the KCMC Management
through the Directorate of Planning.

39
KCMC shall organize bi-annual meetings to discuss the progress in implementing the KCMC-
wide and units’ plans.
The progress reports will be used to update and roll forward the Strategic Plan every year.
The following table is the format to be used for reporting the progress implementation of the
strategic plan
Table 1. Progress implementation report of the Five-Year Rolling and Strategic Plan.
Strategic
Objectives
Targets Strategies Planned
activities
Achievements Planned
Remedial
Action
Performed
activities
Targets
achieved
Reasons
for
deviation
7.4 Evaluation
Evaluation will focus of comparison between planned targets and actual performance. The
evaluation of KCMC strategic plan will have the following objectives:
i) Assessing the reasons for success or failure of specific aspects of the strategic plan
ii) Assessing whether the Strategic Plan is achieving its objectives
iii) Finding out whether the effects of the strategic Plan are contributing to a better
fulfillment of the Mission and Vision of KCMC

40
iv) Assessing the adequacy of resources being mobilized for implementation of the plan
v) Determining whether available resources are being utilized efficiently
vi) Determining whether the process of strategic planning and implementation is facing
any problems that need attention
Strategic Objective No. 1: Improved Quality of Clinical services
Targets Strategies Planned Activities Performance indicators
Number of various
specialists
increased by June
2018
Recruit various
specialists to increase
their number from 60
to 120
Request for recruitment
permission from GSF
Advertise required
positions
Request for secondment
form Government
Number of specialists
Train various
specialists for deficient
specialties
Seek for funds
Identify suitable
Undergraduate candidates
Identify suitable
registrars in various
departments
Quality social
welfare services
provided to all
patients by June
2015
Establish social
welfare department
Develop proposal for
establishment of social
welfare department
Identify office space
Equip the office
Employ/deploy staff
Proportion of hospital
days due to waiting for
social services
(repatriation, exemptions,
etc)
1. Develop standard
operating
procedures
Appoint committee
Process SOPs through
participatory organs
Operationarize the SOPs
Proportion of referred
upcountry patients
served with meals

41
Strategic Objective No. 1: Improved Quality of Clinical services
Targets Strategies Planned Activities Performance indicators
An acceptable
level of staff
competences in
providing quality
services achieved
by June 2017
Establish continuing
education office
Develop proposal for
establishment of the
office
Employ/deploy staff
Establish continuous
professional development
programs
Proposal in place and
office established
Required staff recruited
Professional development
programmes established
Staff to be compelled
to attend at least one
continued medical
education course per
year
Introduce attendance of
at least one continued
medical education course
per year as criteria for
promotion
Staff attend continued
medical education as one
of the promotion
criterion
Train staff in customer
care
Identify staff to be trained
in customer care
Solicit for funds
Identify
consultant/training
institution
Send them for training
Proportion of staff trained
in customer care
A continuous
quality
improvement
program
established by
June 2015
Establish service
targets for all
departments
Draw up a Standard
Operating Procedures
(SOPs) for service
delivery
Projections of services to
be provided available for
each department
Develop and
implement standards
of care for all major
causes of attendance
and admission
Implement the agreed
SOPs
Proportions of
patients/clients attended
according to set standards
Proportions of
patients/clients not
attended the same day
(includes postponed
clinics)
Copies of
Guidelines/protocols
present at places of work
Update the hospital
formulary annually
95% of prescriptions are
appropriate

42
Strategic Objective No. 1: Improved Quality of Clinical services
Targets Strategies Planned Activities Performance indicators
and regularly provide
prescribers with
information on drugs
available
Proportion of meetings of
Hospital Therapeutics
Committee held as
planned
List of drugs not
available issued
fortnightly
Institute clinical audit Client/Patient satisfaction
rates.
Proportions of hospital
information accurately
entered (completeness of
data records and entry)
Hospital mortality
rates/case fatality rates
reduced by 20%.
Average duration of
hospital stay less than 8
days.
Proportion of rejected
requests for laboratory
investigations reduced by
50%
Proportion of all basic
investigations results
received within 24 hrs of
admission.
Proportion of inter-
departmental
consultations attended
within 24 hours of
request
Proportion of days with
bed occupancy of less
than 100%
% of patient charts
completed as required
Average time from
admission to clerking by
admitting doctor
Proportion of days
without ward rounds

43
Strategic Objective No. 1: Improved Quality of Clinical services
Targets Strategies Planned Activities Performance indicators
Proportion of planned
mortality/morbidity
meetings attended by all
staff
Proportions of patients
examined in side rooms (
privacy observed during
patient examination)
Average number of
outpatients per doctor
Proportion of patients for
major surgery with pre-
operative evaluation by
an anaesthetist
Proportion of emergency
patients attended by a
medical officer within 15
minutes of arrival.
Proportions of patients
seen by a specialist
within 12 hours of
admission.
Waiting time for
appointment to outpatient
clinics and physiotherapy
less than 2 weeks.
Re-attendances as a
proportion of all full
consultancy episode
Re-admission as a
proportion of all
admissions.
Proportion of patient files
with proper specialist
documentation
Proportion of admissions
seen by a specialist
before discharge
An outpatient
consultations of at least 6
new cases and at least 10
follow-up per specialist
clinic

44
Strategic Objective No. 1: Improved Quality of Clinical services
Targets Strategies Planned Activities Performance indicators
Referrals from wards as
% of all outpatient visits
Laboratory tests per
outpatient visits
X-rays per outpatient
visits
Laboratory tests per
admission
Proportion of appropriate
X-rays requested among
admitted patients
Number of major
operations per doctor per
month
Number of caesarian
section operations per
doctor per month
Number of minor
operations per doctor per
month
% of major ward rounds
attended by all
consultants for the ward.
Proportion of
prescriptions in generic
drug names
Proportion of all
caesarian sections are
elective
Proportion of surgeries as
private among all
surgeries
Proportion of discharge
forms fully and
accurately completed in
Jeeva System
Proportion of patients
transferred into another
department following
wrong admissions.
Proportion of patients
discharged within a day
of admission

45
Strategic Objective No. 1: Improved Quality of Clinical services
Targets Strategies Planned Activities Performance indicators
Proportion of seriously ill
patients sent to the wards
before appropriate
resuscitation
Proportion of patients
HIV/AIDS tested among
all patients
Proportion of patient files
with proper nursing
documentation
Proportion of charts
appropriately filled
Proportion of patients
who received appropriate
medications on time
Proportion of patients
with nursing plans
Copies of guidelines/
protocols present and
followed
Caesarian sections as %
of all deliveries
% of babies with AGPAR
Score equal or less than 6
% Fresh stillbirth among
all deliveries
Fresh stillbirth rates
reduced by 50%
Patient re-operation rates.
Average time from
notifying theatre to start
of operation
Proportion of patients
operated within 2 hours
from notifying theatre
and starting the
operation.
% of elective surgeries
without post-operative
infections
% of elective surgeries
without any
complications

46
Strategic Objective No. 1: Improved Quality of Clinical services
Targets Strategies Planned Activities Performance indicators
Proportion of patients
waiting for less than 4
weeks for elective
surgery following the
decision to operate.
Average hospital stay
before operation
Proportion of patients
who stay for less than 48
hours before operation
Average hospital stay
after operation
Proportion of patients
who stay less than 4 days
post operatively
Postoperative sepsis rates
in elective surgery
Proportion of emergency
operations not done (or
done) within three hours
of admission
Proportion of emergency
results communicated
within 1hr of submission
of specimen
Proportion of all results
of basic investigations
available within 24 hrs of
specimens being taken.
Proportion of results of
cultures available within
the minimum standard
period of 72 hrs.
Proportion of biopsy
results available within 7
working days of the
biopsy.
Proportion of all
requested tests available.
Proportion of all
laboratory tests under a
quality assurance scheme.

47
Strategic Objective No. 1: Improved Quality of Clinical services
Targets Strategies Planned Activities Performance indicators
Waiting time for
dispensing drugs less
than 15 minutes
Proportion of blood
products requests
fulfilled within 24 hours
Proportion of emergency
requests for blood
fulfilled within 45
minutes of request
Waiting time at radiology
less than 30 minutes
Proportion of radiology
results reported within 24
hours
Proportion of days
without an efficient
communication system.
Proportion of patients
with temporary files
Proportion of patient files
available at the beginning
of a clinic
% of laboratory test
results available at the
next visit
Number of major
incidents simulations
performed
Disaster
preparedness
ensured by
December 2015
Put in place disaster
preparedness plans
Employ
consultant/identify a team
to develop disaster
preparedness plans
Plans available
Conduct disaster
preparedness exercises
regularly
Create a committee that
will be carrying out
disaster preparedness
regularly
Regular reports available

48
Strategic Objective No. 1: Improved Quality of Clinical services
Targets Strategies Planned Activities Performance indicators
Train staff in disaster
management
Identify staff to be trained
in disaster management
Solicit for funds
Identify
consultant/training
institution
Number of trained staff
Scope of tertiary
services provided
increased by
December 2015
Recruit and/or train
required staff
Develop manning levels
of the hospital
Identify staff to be trained
Recruit new staff
Number of new
specialists services
established
Procure required
equipment
Carry out needs
assessment of the
required equipment
Initiate tendering process
Procure equipment
Essential equipment
available for the new
services
Procure required space
and/or buildings
Identify Suitable
building/Areas
Space availability
Easy availability
of key clinical
staff on call
ensured by
December 2012
Provide mobile phones
to key staff
Identify staff to be
provided with mobile
phones
Procure and issue mobile
phones to the identified
staff
Proportion of key staff
with mobile phones
Build houses within or
near the hospital to
accommodate staff for
emergency services
Identify area for staff
construction
Solicit for funds to
construct staff houses
Identify consultant and
contractor
Proportion of key staff
accommodated within 5
km of the hospital

49
Strategic Objective No. 2: Enhanced Institutional Governance and Management
Targets Strategies Planned Activities Performance indicators
KCMC planning
unit established by
December 2014
Provide office space
for the planning unit
Solicit for Funds,
Renovate the acquired
office space
Procure office furniture
Availability of space
Recruit planning office
staff
Seek recruitment permit
Carry out recruitment
process
Availability of planning
officer and other staff
Institutional
quality assurance
unit established by
December 2015
Provide office space
for the quality
assurance unit
Solicit for Funds,
Renovate the acquired
office space
Procure office furniture
Availability of space
Recruit Quality
Assurance office staff
Seek recruitment permit
Carry out recruitment
process
Availability of quality
assurance staff
3. Institutional
policies
established by
April 2015
Develop staff welfare
policy
Solicit for funds
Identify consultant/team
to develop staff welfare
policy
Availability Staff
Welfare Policy made
available
Develop anti sexual
harassment policy
Solicit for funds
Identify consultant/team
to develop anti sexual
harassment policy
Availability antisexual
harassment
Policy made available
Develop gender policy
Solicit for funds
Identify consultant/team
to develop gender policy
Availability of Gender
Policy made
Develop recruitment ,
retention and
retirement policy
Identify a team to
develop recruitment ,
retention and retirement
policy
Availability of
recruitment , retention
and retirement policy

50
Strategic Objective No. 2: Enhanced Institutional Governance and Management
Targets Strategies Planned Activities Performance indicators
Develop institutional
staff
establishment/manning
levels
Solicit for funds
Identify consultant/team
to develop institutional
staff
establishment/manning
levels
Availability of
institutional staff
requirement
Institutional
management
team trained on
leadership and
management skills
by July 2015
Hold training
workshop
Identify sources and
solicit for funds
Required funds acquired
by December 2010
Identify facilitators and
conduct the training
Facilitators identified and
training programme
developed by October
2010
Job descriptions
for all staff
operationalized by
December 2015
Head of each unit to
ensure each staff has
job description
Develop job description
for each staff
Availability of Job
Description of each staff
Job description
External links unit
established by
December 2016
Provide office for the
links unit
Allocate and renovate
office for external links
Procure office furniture
Office space made
available
Recruit links office
staff
Advertise the identified
positions
Recruit suitable staff
Staff recruited
Develop data base for
external links
Develop database for
archiving links
information
Links data base
established and updated
Strategic Objective No. 3: Enhanced Human resources Management
Targets Strategies Planned Activities Performance indicators

51
Strategic Objective No. 3: Enhanced Human resources Management
Targets Strategies Planned Activities Performance indicators
Staff Recruitment
and development
master plan
developed and
operationalized by
December 2015
Do Situational analysis
of existing staff to
establish recruitment
needs.
Carry out needs
assessment using
available tools
Needs assessment carried
out by July 2014
Establish staff
recruitment needs.
Analyze data to establish
the needs
Recruitment and staff
development
requirements established
by July 2015
Establish staff training
and development
master plan.
Draw up and implement
the master plan
Staff recruitment and
development master plan
in place and
operationalized by July
2015
Shortage of staff
addressed staff by
2016.
Make use of the
permission given to the
institution to fill in
Specific approved
positions.
Advertise all positions
which have permission
Staff recruited by June
2015
Use contractual
employment as a
mechanism for
handling current
critical staff shortages.
Solicit funds to finance
salaries for contractual
employee
Availability of fund
Required staff requited
Introduce tenure of
employment for staff.
Put in place an
effective human
resource succession
plan
Develop staff succession
master plan
Succession master plan
made available
3. Staff promotion
guidelines
reviewed and
operationalized by
December 2015
Review the current
staff scheme of service
and promotion
guidelines
Review of scheme of
service and guidelines
for promotion
Revised scheme of
service and guidelines for
promotion in place by
December 2014
Operationalize the
reviewed staff
promotion guidelines.
Disseminate the
guidelines to stakeholders
and implement
Guidelines and
implemented by March
2015
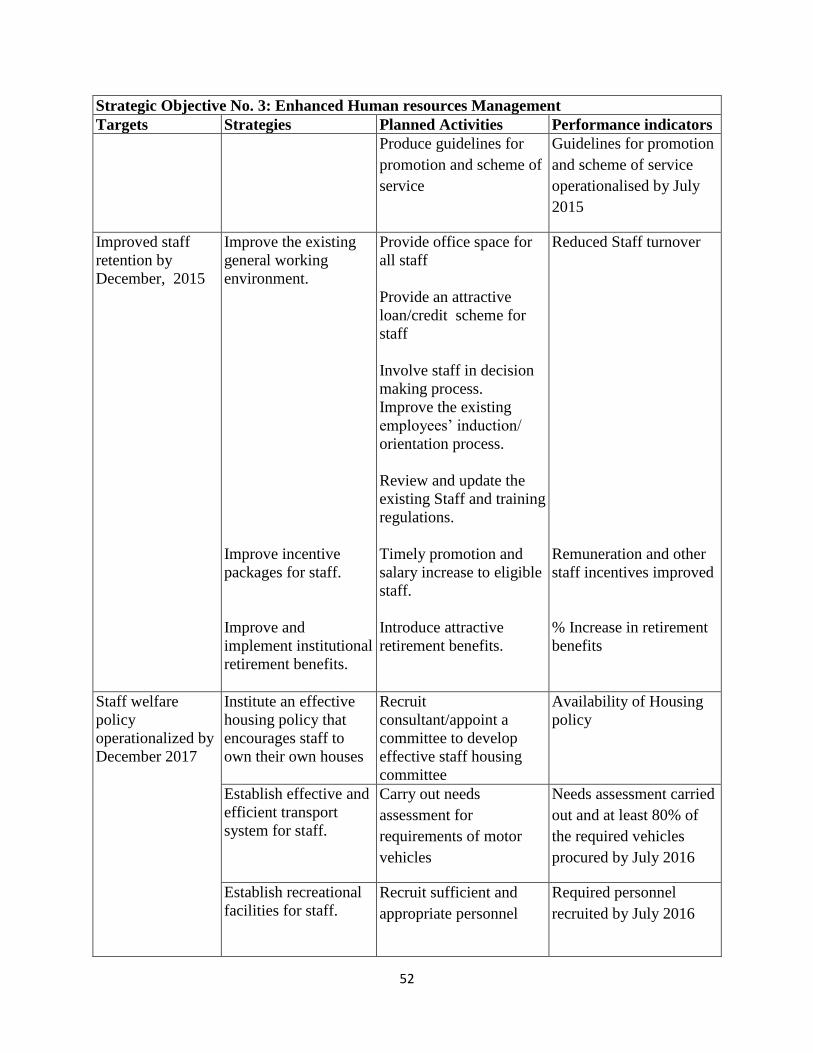
52
Strategic Objective No. 3: Enhanced Human resources Management
Targets Strategies Planned Activities Performance indicators
Produce guidelines for
promotion and scheme of
service
Guidelines for promotion
and scheme of service
operationalised by July
2015
Improved staff
retention by
December, 2015
Improve the existing
general working
environment.
Improve incentive
packages for staff.
Improve and
implement institutional
retirement benefits.
Provide office space for
all staff
Provide an attractive
loan/credit scheme for
staff
Involve staff in decision
making process.
Improve the existing
employees’ induction/
orientation process.
Review and update the
existing Staff and training
regulations.
Timely promotion and
salary increase to eligible
staff.
Introduce attractive
retirement benefits.
Reduced Staff turnover
Remuneration and other
staff incentives improved
% Increase in retirement
benefits
Staff welfare
policy
operationalized by
December 2017
Institute an effective
housing policy that
encourages staff to
own their own houses
Recruit
consultant/appoint a
committee to develop
effective staff housing
committee
Availability of Housing
policy
Establish effective and
efficient transport
system for staff.
Carry out needs
assessment for
requirements of motor
vehicles
Needs assessment carried
out and at least 80% of
the required vehicles
procured by July 2016
Establish recreational
facilities for staff.
Recruit sufficient and
appropriate personnel
Required personnel
recruited by July 2016

53
Strategic Objective No. 3: Enhanced Human resources Management
Targets Strategies Planned Activities Performance indicators
Effective Human
Resource
Information
Health system
developed by
December 2017.
Procure and Install
integrated software for
human resource and
health information
systems.
Identify suitable software
Procure and install IT
equipment
Provide training for ICT
staff and identified users.
Establish databases to
provide staff’s
particulars.
Ensure maintenance
schedules for the
equipment
Integrated software for
software for human
resource and health
information systems in
place
Strategic Objective No. 4: Enhanced financial capability, efficiency and sustainability
Targets Strategies Planned Activities Performance indicators
Internal audit
department
strengthened by
Jan 2018
Recruit more
professional and
competent internal
audit staff
Carry out needs
assessment
Recruit competent and
required number of
auditors
Competent and required
number of auditors
employed
Purchase audit
software and ICT
equipments
Identify Audit software ,
ICT equipment and
initiate tendering
processes
Required audit software,
ICT equipment Procured
Provide office space
for internal audit
Secure and allocate office
to internal audit unit
Internal audit office made
available
Accounting
software
(WebERP)
operationalized
fully by Dec 2015
Encourage staff to use
Web ERP
Train staff on Web ERP
software
All staff are conversant
with Web ERP software
Budgeting unit
established by
Dec. 2016
Provide office space
for Budgeting unit
Secure and allocate office
to budgeting unit
Internal audit office made
available
2. Recruit staff for
budget unit
Seek recruitment
permission from relevant
organ
Required staff employed

54
Strategic Objective No. 4: Enhanced financial capability, efficiency and sustainability
Targets Strategies Planned Activities Performance indicators
Internally
generated income
improved by June
2016
Conduct cost benefit
analysis for internally
income generating
projects.
Develop procedures for
cost containment
Procedures in place and
in use by July 2015
Sensitize KCMC
community to exercise
cost containment
measures
Cost contained by at least
20% by July 2015
Hire consultant/expert
for new
investments/Investment
plan
Identify
experts/consultants
Develop Investment
business plan for the next
five years
Consultant procured and
investment business plan
in place
Institutional
Financial
Regulation
Developed by Nov
2015
Hire consultant/expert
for development of
KCMC Financial
regulations
Identify
experts/consultants
Develop Investment
business plan for the next
five years
KCMC financial
regulation in place
Internal control
systems improved
by Dec 2015
.Strengthen the internal
control system
Review the current
internal control systems
Existence of better
control system
Government and
other good
Samaritan funding
level increased to
40% from current
level (30%) by
May 2018
Negotiate with
government and other
donors to increase
funding level
Draw up a fundable
proposal
Proposal developed and
submitted to relevant
funding agencies

55
Strategic Objective No. 5: Developed and maintained Hospital infrastructure
Targets Strategies Planned Activities Performance indicators
Directorate of
Planning and
Development
Established by
2016
Prepare a write up of
Establishment of
Directorate of planning
and development
Identify a team of experts
to develop a write up
Write up in place
Establish Directorate of
Planning and
Development
Directorate of planning
and Development
Established
Locate space for the
Directorate of
Planning and
Development
Renovate and procure
furniture for the
directorate
Office allocated
Employ staff for the
Directorate of
Planning and
Development
Advertise and recruit
staff for the Directorate
Staff recruited
Estate Department
Improved by 201
Streamline function of
estate department
Separate instrument
repair laboratory from
Estates Department
Laboratory repair
instrument are not kept in
the estate department
Existing
Infrastructure
rehabilitated by
July 2014
Repair all hospital
buildings
Solicit for funds Availability of funds
Identify contractor
through tendering system
Contractor identified
Paint all hospital
buildings
Solicit for funds Availability of funds
Identify contractor
through tendering system
Contractor identified
Repair all hospital
feeder roads
Solicit for funds
Availability of funds
Identify contractor
through tendering system
Contractor identified
Water supply
system improved
by December 2015
Put in place second
source of
Water supply
Drill water bore halls Availability of water
from bore halls
Power supply
improved by July
2014
Seek from TANESCO
exemption from power
rationing
Send a request and make
follow up with
TANESCO
No Power rationing
Put in place
mechanisms of
reduction of power
consumption
Sensitize KCMC staff to
switch off power when is
not in use
Mater separation
Electricity bill reduced
Communication
improved by July
2015
Rehabilitate internal
telephone
communication system
Solicit for funds Better performance of
internal telephone
communication system Initiate procurement of
contractor

56
Strategic Objective No. 5: Developed and maintained Hospital infrastructure
Targets Strategies Planned Activities Performance indicators
Rehabilitate the telephone
system
Administrative
block constructed
by 2015
Prepare architectural
drawings for the new
administrative block
Solicit funds for
Administrative block
construction
Funding status
established by July 2014
Procure consultant Architectural drawings
for the new
administrative block in
place
Prepare Architectural
drawings
Procure contractor and
initiate construction
Administrative block
constructed by 2015
Clinical wards
expanded by 2016
Prepare architectural
drawings for the new
clinical wards
Solicit funds for Clinical
wards construction
Funding status
established by July 2015
Procure consultant Architectural drawings
for the new Clinical
wards in place July 2015 Prepare Architectural
drawings
Procure contractor and
initiate construction
New clinical wards
constructed by 2016
Strategic Objective No. 6: Ensured availability of Hospital equipment and supplies
Targets Strategies Planned Activities Performance indicators
Central workshop
established by July
2018
Prepare architectural
drawings for the new
central workshop
Solicit funds for Central
workshop construction
Funding status
established by July 2015
Procure consultant Architectural drawings
for the new Central
workshop in place July
2015
Prepare Architectural
drawings
Availability of
architectural drawings
July 2015
Procure contractor and
initiate construction
New Central workshop
constructed by 2018

57
Strategic Objective No. 6: Ensured availability of Hospital equipment and supplies
Targets Strategies Planned Activities Performance indicators
Employ and train
technical staff for the
new central workshop
Recruit required and
competent staff
Staff in employed by
June 2017
Conduct training needs
assessment
Report on training needs
assessment in place June
2017
Identify facilitator and
conduct training
Facilitator identified and
training conducted June
2017
Planned
Preventive
Maintenance
(PPM) for hospital
equipment
developed by July
2015.
Prepare a write up for
Planned Preventive
Maintenance (PPM)
for hospital equipment
Identify
consultant/experts
Preventive and
Maintenance programe in
place and full operational
June 2015 Develop KCMC
Preventive and
Maintenance programme
All old machines
replaced with new
ones by July 2016.
Establish replacement
policy of old
machines/equipment
Draw up KCMC disposal
and replacement policy
Availability of disposal
and replacement policy
by June 2015
Dispose obsolete
equipment
All obsolete equipment
disposed September 2015
Acquire modern
equipment
Solicit for fund Modern equipment
acquired by June 2016 Procure modern and
required equipment
Production of local
manufactured
equipment
increased by July
2015.
Optimize production
skills for local
products.
Identify and train staff Local manufactured
equipment increased by
30% by July 2015.
Set production targets establish production
target
Rational
prescribing of
drugs ensured by
July 2015.
Run short courses for
prescribing of drugs
for doctors
Develop training needs
assessment and identify
staff to be trained
Better prescription of
drugs July 2015
Indentify facilitators and
train staff
Timely availability
of supplies
ensured by July
2016
Ensure the
implementation of
annual procurement
plan
Solicit for funds Planned Goods and
services procured as
planned July 2015 Timely preparation of
annual procurement plan
Strengthen
procurement process.
Recruit requirement
number of staff
Timely acquisition of
goods and services July

58
Strategic Objective No. 6: Ensured availability of Hospital equipment and supplies
Targets Strategies Planned Activities Performance indicators
Improve system of
procurement process
2015
Strategic Objective No. 7: Improved Health Management Information system
Targets Strategies Planned Activities Performance indicators
Number of HMI
system personnel
increased by 50%
by December 2015
Increase number of
personnel through
employment of new
graduates from the
school of medical
records
Develop staff
establishment
Recruit required number
of HMI staff
Number of employed
HMI personnel by
December 2015
All of HMI system
personnel on
electronic HMI
system trained by
February 2016
Conduct training on
advanced ICT
utilization
Solicit for funds
Identify facilitator and
conduct training
Staff trained in advanced
ICT utilization by
January 2016
Organize on-job
training on use of
electronic HMI system
e.g. care2X
Solicit for funds
Identify facilitator and
conduct training
Staff trained in electronic
HMI February 2016
HMI system
physical
infrastructure
refurbished by
June 2015
Restructure and
refurbish the current
physical infrastructure
to support both
manual and electronic
HMI systems
Identify consultant to
develop architectural
design
Rehabilitate the identifies
facility to suit the
requirement
physical infrastructure
refurbished to support
both manual and
electronic HMI systems
June 2015
Electronic HMI
system established
by August 2016
Develop SOPs for
HMI system (data
entry, analysis,
reporting and
dissemination)
Identify a team of expert
to develop SOPs
Submit to the relevant
organs for approval
SOPs developed and in
use by June 2016
Establish quality
assurance and control
system
Establish directorate of
quality control
Develop KCMC quality
control policy
Directorate of quality
control established
Quality control document
made available

59
Strategic Objective No. 7: Improved Health Management Information system
Targets Strategies Planned Activities Performance indicators
Acquire ICT facilities
Solicit for funds
Procure required ICT
equipment
ICT equipment procured
Establish reliable
back-up system
Procure servers and
heavy duty UPS
Availability of savers and
UPS
Number of
students in school
of medical records
increased by 100%
by September
2018
Request from
Government to
increase by two-fold
the current enrollment
of students
Prepare a proposal and
submit to Government
that justify two fold
increase of students
Permission granted by
June 2015
Recruit new teaching
staff
Seek recruitment
permission
Advertise the position
and recruit required
number of staff
Number of staff recruited
June 2015
Acquire modern
learning aids (audio-
visual systems,
computers etc)
Solicit for funds
Procure required quantity
of learning aids
Availability of Learning
Aids June 2015
Advertisements of the
school made widely
Develop marketing tools
Upload course provided
in the website
Increase number of
registered students June
2015
Diploma course in
Medical Records
introduced by
September 2015
Develop curriculum
for diploma program in
medical records
Identify a team of expert
to develop curriculum for
diploma program in
medical records
Submit to the relevant
organs for approval
Curriculum for diploma
program in medical
records
developed and
operationarised by June
2016

60





























