-
8/11/2019 First-trimester markers of aneuploidy in women.pdf
1/5
First-trimester markers of aneuploidy in womenpositive for HIVMD
Savvidou,a I Samuel,b A Syngelaki,c M Poulton,b KH Nicolaidesc
a Department of Maternal Fetal Medicine, Imperial College School
of Medicine, Chelsea and Westminster Hospital b Department of
Sexual
Health and HIV c Harris Birthright Research Centre for Fetal
Medicine, Kings College Hospital, London, UK
Correspondence: MD Savvidou, Department of Maternal Fetal
Medicine, Imperial College School of Medicine, Chelsea and
Westminster
Hospital, 369 Fulham Road, London SW10 9NH, UK. Email
[email protected]
Accepted 17 September 2010. Published Online 10 November
2010.
Objective To investigate whether the sonographic and
maternal
serum biochemical markers used in first-trimester screening
for
chromosomal abnormalities are altered in pregnancies affected
by
maternal HIV infection.
DesignNested casecontrol study.
Setting Routine antenatal visit in a teaching hospital.
PopulationNinety HIV-positive and 450 HIV-negative pregnant
women.
MethodsFindings from first-trimester antenatal visit for
calculation of the risk for chromosomal abnormalities were
compared between HIV-positive (treated and untreated) and
HIV-negative women.
Main outcome measuresFirst-trimester maternal serum free b
human chorionic gonadotrophin (free b-hCG) pregnancy-
associated plasma protein-A (PAPP-A) and fetal nuchal
translucency thickness (NT), were compared.
ResultsThere were no statistically significant differences
between the HIV-positive and HIV-negative women in the
median maternal levels of free b-hCG, PAPP-A and fetal NT.
However, within the HIV-positive group those receiving
antiretroviral treatment (n = 41) had a significantly lower
median multiple of the median (MoM) for free b-hCG (0.74,
interquartile range [IQR] 0.451.32 MoM) than HIV-positive
women on no treatment (1.03, IQR 0.761.85 MoM; P= 0.006)
and HIV-negative women (1.0, IQR 0.681.47 MoM;
P = 0.003). There was no correlation between the level
of free b-hCG or PAPP-A and maternal viral load or CD4+
count.
Conclusions Maternal levels of free b-hCG in treated
HIV-positive
pregnant women were lower compared with those in non-treated
HIV-positive and HIV-negative women, whereas the PAPP-A
levels and fetal NT remained unaltered.
KeywordsChromosomal abnormalities, first trimester, free
b-human chorionic gonadotrophin, HIV, pregnancy,
pregnancy-associated plasma protein-A.
Please cite this paper as: Savvidou M, Samuel I, Syngelaki A,
Poulton M, Nicolaides K. First-trimester markers of aneuploidy in
women positive for HIV.
BJOG 2011;118:844848.
Introduction
In the past two decades, acquisition of human immunode-
ficiency virus (HIV) has reached epidemic levels globally,
as there are an estimated 33 million people living withHIV.
Women account for half of these people and the
majority of them are of reproductive age.1 In the UK, the
introduction of routine antenatal screening, with 95% of
pregnant women accepting antenatal HIV testing, has
enabled the identification of the vast majority of HIV-posi-
tive pregnant women.2 Additionally, the introduction of
highly active anti-retroviral treatment in pregnancy has
reduced the risk of mother-to-child transmission to around
1%, leading to a rising number of pregnancies in these
women.3 As a result of these changes, the prevalence of
HIV among women giving birth in the UK has increased
five-fold over the past decade.2
Effective screening for chromosomal abnormalities in thefirst
trimester of pregnancy is provided by assessment of a
combination of maternal age, measurement of fetal nuchal
translucency (NT), maternal serum free b-human chorionic
gonadotrophin (free b-hCG) and pregnancy-associated
plasma protein-A (PAPP-A).4 This method of screening,
which gives a detection rate for trisomy 21 of 90% for a
5% false-positive rate, is now recommended for all preg-
nant women in the UK.5 Free b-hCG and PAPP-A are
844 2010 The Authors Journal compilationRCOG 2010 BJOG An
International Journal of Obstetrics and Gynaecology
DOI: 10.1111/j.1471-0528.2010.02767.x
www.bjog.orgFetal medicine
-
8/11/2019 First-trimester markers of aneuploidy in women.pdf
2/5
known to be affected by maternal race, weight, smoking
status, gestational age, parity and method of conception.6,7
Conversely, little is known about the effect of the maternal
immune status, as regards HIV status, on their levels.812
The aim of the study was to assess whether the first-
trimester maternal serum levels of free b-hCG and PAPP-
A, used for the assessment of risk of chromosomal
abnormalities, are affected by the presence of maternal
HIV.
Methods
This was a casecontrol study from an ongoing prospective
study to identify potential biomarkers of pregnancy com-
plications in women attending for their routine first hospi-
tal visit in pregnancy at Kings College Hospital, UK. In
this visit, which is held at 11+013+6 weeks of gestation,
all
women have an ultrasound scan, first, to confirm
gestational age from the measurement of the fetal crown
rump length (CRL); second, to diagnose any major
fetalabnormalities; and third, to measure the fetal NT
thickness
as part of screening for chromosomal abnormalities. In
addition, the maternal serum free b-hCG and PAPP-A are
determined and the results are combined with maternal age
and fetal NT to calculate the patient-specific risk for tri-
somy 21 and trisomy 13/18. All blood samples were pro-
cessed immediately and an automated machine that
provides reproducible results within 30 minutes, was used
to measure free b-hCG and PAPP-A (Delfia Express Sys-
tem; Perkin Elmer, Waltham, MA, USA). Maternal demo-
graphic characteristics, ultrasonographic measurements and
biochemical results were recorded in a computer database
where details on pregnancy outcomes were added as soon
as they became available.
The casecontrol study population comprised 90 HIV-
positive women with singleton pregnancies and a live birth.
For each HIV-positive woman, five HIV-negative women
were selected, matched according to the date of scan and
consequently the date of the biochemical measurements.
The study period was from March 2006 to August 2009
and during this period we examined 35 964 singleton preg-
nancies. Among the 90 HIV-positive women, 41 (45.5%)
were on anti-retroviral treatment (median duration of
treatment: 20 months) including 17 women (41.5%) on
nucleoside reverse transcriptase inhibitor (NRTIs) and aprotease
inhibitor, 23 women (56%) on NRTIs and a non-
NRTI and one woman (2.5%) on monotherapy. Informa-
tion on the viral load and CD4+ count, at a date closest to
the scan date, was also obtained. Approval by the local
Research Ethics Committee was sought but was not
thought to be necessary under the terms of the Governance
Arrangements for Research Ethics Committees in the UK.
Furthermore, women in our centre routinely give written
informed consent for their data to be used for audit and
research purposes.
Statistical analysisIn the cases and controls the measured serum
PAPP-A and
free b-hCG were converted to multiples of the expected
normal median (MoM) corrected for fetal CRL, maternal
weight, smoking, parity, racial origin and method of con-
ception as previously described.6 The measured NT was
expressed as a difference from the expected normal mean
for gestation (delta value).13 Normality of the data
distribu-
tion was examined with the KolmogorovSmirnov test and
probability plots. Data were expressed as mean standard
deviation or as median and interquartile range (IQR) for
normally and non-normally distributed data, respectively.
Comparisons between groups were performed using
Students t test, MannWhitney U test or chi-square test
for numerical and categorical data, respectively. Power
calculation indicated that a sample of 90 HIV-positive and
450 HIV-negative women would have more than 80%power with an
alpha 0.05 (two-tails) for the detection of a
mean difference of 0.25 MoM in free b-hCG (1:5 matched
case controls). The effect size was estimated from previous
publications.12 The statistical analyses were performed
using
the SPSS (Version 12.0, SPSS Inc., Chicago, IL, USA).
Results
The maternal demographic and pregnancy characteristics
and outcomes of the 90 HIV positive and 450 HIV negative
women are given in Table 1. None of the neonates in this
study was affected by a chromosomal abnormality. The
HIV positive women, compared with the HIV-negative
group, were more likely to be black, heavier and non-
smokers and were more likely to deliver earlier and have
smaller neonates. There were no significant differences
between the HIV-positive and HIV-negative pregnancies in
fetal CRL and NT or in maternal adjusted levels of free
b-hCG and PAPP-A.
The maternal demographic and pregnancy characteristics
and outcome of the HIV-positive women depending on the
use of anti-retroviral treatment are also given in Table 1.
Women receiving anti-retroviral treatment (n = 41) were
more likely to be older and had a significantly lower med-
ian serum free b-hCG than HIV-positive women on notreatment and
HIV-negative women (0.74, IQR 0.451.32
MoM versus 1.0, IQR 0.681.47 MoM; P= 0.003). In the
HIV group on treatment, there was no significant statistical
correlation between maternal serum free b-hCG and dura-
tion of treatment (P = 0.081). Similarly, there was no sig-
nificant difference in maternal median serum free b-hCG
between those receiving NRTIs together with a protease
inhibitor and those on a combination of NRTIs and a non-
Maternal levels of free b-hCG and PAPP-A in HIV
2010 The Authors Journal compilation RCOG 2010 BJOG An
International Journal of Obstetrics and Gynaecology
845
-
8/11/2019 First-trimester markers of aneuploidy in women.pdf
3/5
NRTI (0.82, IQR 0.421.44 MoM versus 0.74 IQR 0.51
1.26 MoM; P= 0.80). There were no statistically significant
differences between the HIV-positive women on treatment
and those on no treatment in fetal CRL, NT and levels of
PAPP-A. There was no statistically significant correlation
between maternal free b-hCG and maternal viral load
(P= 0.59) or CD4+ count (P = 0.77) even if women with
more severe infection, with CD4+ cell count/mm3
-
8/11/2019 First-trimester markers of aneuploidy in women.pdf
4/5
especially considering the immunomodulatory properties of
b-hCG.15,16
From a clinical perspective, the differences that we
detected in free b-hCG levels are unlikely to be of clinical
significance but may have implications in the estimation of
individual risks of chromosomal abnormalities. In pregnan-
cies affected by trisomy 21, maternal serum free b-hCG isabout
twice as high and PAPP-A is reduced to about half
compared with values in chromosomally normal pregnan-
cies.4,6,17 Conversely, pregnancies affected by trisomy
13/18
demonstrate low levels of both maternal free b-hCG and
PAPP-A.17 Consequently, lower levels of free b-hCG in
treated HIV-positive pregnant women may underestimate
the risk for trisomy 21 or overestimate the risk for trisomy
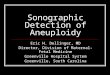
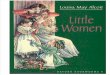
13/18. Nevertheless, this is a theoretical risk. A
hypothetical
35-year-old woman, who is HIV-positive on treatment,
with fetal CRL of 65 mm, NT of 1.8 mm, PAPP-A levels of
1 MoM (all mean values of our study population) and free
b-hCG of 0.7 MoM, instead of 1 MoM, will not have a
different risk for chromosomal abnormalities compared
with an untreated HIV-positive woman or even an HIV-
negative woman with similar characteristics (Figures 1 and
2). For the majority of women this will have little impact
but may be crucial in women with intermediate risk when
small deviations may shift the balance between further
investigations in terms of invasive testing or not. This is
certainly, a parameter of which clinicians should be aware
and it should be taken into account in the estimation of
patient-specific risks for aneuploidies especially in view
of
the theoretical increased risk of HIV vertical transmission
that is associated with early invasive diagnostic tech-
niques.18,19 Definitely, further larger studies will be
required
to confirm our findings. The study did not include any
cases of chromosomal abnormalities and therefore, it is not
possible to comment on the levels of the maternal freeb-hCG and
PAPP-A in these women.
Conclusion
In summary, we found that maternal levels of free b-hCG
in treated HIV-positive pregnant women are lower com-
pared with non-treated HIV-positive and HIV-negative
women, whereas the levels of PAPP-A are not significantly
altered.
Disclosure of interestsNone declared.
Contribution to authorshipMDS is the main corresponding author
and she conceived
and designed the study. IS, AS and MP contributed to the
design and conduction of the study and interpretation of the
results. KHN is the main supervisor. All the authors
partici-
pated in and contributed to the writing of the manuscript.
Details of ethics approvalApproval by the local Research Ethics
Committee was
sought but was not thought to be necessary under the
terms of the Governance Arrangements for Research Ethics
Committees in the UK.
FundingThe study was supported by The Fetal Medicine
Foundation
(UK Registered Charity number: 1037116).
AcknowledgementsThe study was supported by The Fetal Medicine
Founda-
tion (UK Registered Charity number: 1037116).j
Risko
ftrisomy21
1/10000
1/5000
1/3333
1/2500
1/2000
1/1666
1/1428
1/1250
1/1111
0 0.5 1 1.5 2
0
Free -human chorionic gonadotrophin (MoM)
Figure 1. Scatter plot of the risk of trisomy 21 in a
hypothetical
35-year-old pregnant woman, with fetal CRL 65 mm, NT 1.8 mm,
PAPP-A 1 MoM (all mean values of our study population),
depending
on the maternal levels of free b-hCG.
Riskoftrisomy13/18
0
1/10000
1/5000
1/3333
1/2500
1/2000
1/1666
1/1428
1/1250
0 0.5 1 1.5 2
Free -human chorionic gonadotrophin (MoM)
Figure 2. Scatter plot of the risk of trisomy 13/18 in a
hypothetical
35-year-old pregnant woman, with fetal CRL 65 mm, NT 1.8 mm,
PAPP-A 1 MoM (all mean values of our study population),
depending
on the maternal levels of free b-hCG.
Maternal levels of free b-hCG and PAPP-A in HIV
2010 The Authors Journal compilation RCOG 2010 BJOG An
International Journal of Obstetrics and Gynaecology
847
-
8/11/2019 First-trimester markers of aneuploidy in women.pdf
5/5
References
1 UNAIDS. 2008 Report on the global AIDS epidemic. Status of
the global HIV epidemic. [www.unaids.org/en/KnowledgeCentre/
HIVData].
2 Health Protection Agency. HIV in the United Kingdom. 2009
Report.
[www.hpa.org.uk/publications].
3 Townsend CL, Cortina-Borja M, Peckham CS, de Ruiter A, Lyall
H,
Tookey PA. Low rates of mother-to-child transmission of HIV
follow-ing effective pregnancy interventions in the United Kingdom
and
Ireland, 20002006.AIDS 2008;22:97381.
4 Nicolaides KH, Spencer K, Avgidou K, Faiola S, Falcon O.
Multicenter
study of first-trimester screening for trisomy 21 in 75 821
pregnan-
cies: results and estimation of the potential impact of
individual risk-
orientated two-stage first-trimester screening. Ultrasound
Obstet
Gynecol 2005;25:2216.
5 National Collaborating Centre for Womens and Childrens
Health.
Antenatal Care: Routine Care for the Healthy Pregnant Woman.
London: National Institute for Clinical Excellence, 2008.
6 Kagan KO, Wright D, Spencer K, Molina FS, Nicolaides KH.
First-
trimester screening for trisomy 21 by free beta-human
chorionic
gonadotropin and pregnancy-associated plasma protein-A: impact
of
maternal and pregnancy characteristics.Ultrasound Obstet
Gynecol
2008;31:493502.7 Spencer K, Bindra R, Nicolaides KH. Maternal
weight correction of
maternal serum PAPP-A and free beta-hCG MoM when screening
for trisomy 21 in the first trimester of pregnancy. Prenat
Diagn
2003;23:8515.
8 Yudin MH, Prosen TL, Landers DV. Multiple-marker screening
in
human immunodeficiency virus-positive pregnant women: screen
positivity rates with the triple and quad screens. Am J Obstet
Gyne-
col 2003;189:9736.
9 Einstein FH, Wright RL, Trentacoste S, Gross S, Merkatz IR,
Bernstein
PS. The impact of protease inhibitors on maternal serum
screening
analyte levels in pregnant women who are HIV positive. Am J
Obstet
Gynecol 2004;191:10048.
10 Gross S, Castillo W, Crane M, Espinosa B, Carter S, DeVeaux
R,
et al. Maternal serum alpha-fetoprotein and human chorionic
gona-
dotropin levels in women with human immunodeficiency virus. Am
J
Obstet Gynecol 2003;188:10526.
11 Le Meaux JP, Tsatsaris V, Schmitz T, Fulla Y, Launay O,
Goffinet F,
et al. Maternal biochemical serum screening for Down syndrome
in
pregnancy with human immunodeficiency virus infection.
Obstet
Gynecol 2008;112:22330.
12 Brossard P, Boulvain M, Coll O, Barlow P, Aebi-Popp K,
Bischof P,
et al. Swiss HIV Cohort Study. Swiss HIV Mother and Child
Cohort
Study; Is screening for fetal anomalies reliable in HIV-infected
preg-nant women? A multicentre study. AIDS 2008;22:20137.
13 Wright D, Kagan KO, Molina FS, Gazzoni A, Nicolaides KH. A
mix-
ture model of nuchal translucency thickness in screening for
chro-
mosomal defects. Ultrasound Obstet Gynecol 2008;31:37683.
14 Cruz J, Cruz G, Minekawa R, Maiz N, Nicolaides KH. Effect of
tem-
perature on the measurement of free b-hCG and PAPP-A
concentra-
tion. Ultrasound Obstet Gynecol 2010;36:1416.
15 Polliotti BM, Gnall-Sazenski S, Laughlin TS, Miller RK.
Inhibitory
effects of human chorionic gonadotropin (hCG) preparations on
HIV
infection of human placenta in vitro. Placenta
2002;23:S1026.
16 Lin J, Lojun S, Lei ZM, Wu WX, Peiner SC, Rao CV.
Lymphocytes
from pregnant women express human chorionic gonadotropin/
luteinizing hormone receptor gene. Mol Cell Endocrinol
1995;111:
R137.
17 Kagan KO, Wright D, Valencia C, Maiz N, Nicolaides KH.
Screeningfor trisomies 21, 18 and 13 by maternal age, fetal nuchal
translu-
cency, fetal heart rate, free beta-hCG and
pregnancy-associated
plasma protein-A.Hum Reprod 2008;23:196875.
18 Somigliana E, Bucceri AM, Tibaldi C, Alberico S, Ravizza M,
Savasi
V, et al. Italian Collaborative Study on HIV Infection in
Pregnancy;
Early invasive diagnostic techniques in pregnant women who
are
infected with the HIV: a multicenter case series. Am J Obstet
Gyne-
col 2005;193:43742.
19 Mandelbrot L, Jasseron C, Ekoukou D, Batallan A, Bongain A,
Pan-
nier E, et al. ANRS French Perinatal Cohort; Amniocentesis
and
mother-to-child human immunodeficiency virus transmission in
the
Agence Nationale de Recherches sur le SIDA et les Hepatites
Virales
French Perinatal Cohort. Am J Obstet Gynecol 2009;200:160.
Sawidou et al.
848 2010 The Authors Journal compilationRCOG 2010 BJOG An
International Journal of Obstetrics and Gynaecology