-
7/30/2019 First (Thumb) Metacarpal Fractures
1/10
Official reprint from UpToDatewww.uptodate.com
2013 UpToDate
Author
Josh Bloom, MD, MPH
Section Editor
Patrice Eiff, MD
Deputy Editor
Jonathan Grayzel, MD, FAAEM
First (thumb) metacarpal fractures
Disclosures
All topics are updated as new evidence becomes available and
ourpeer review process is complete.
Literature review current through: Mar 2013. | This topic last
updated: nov 14, 2012.
INTRODUCTION Metacarpal fractures are common [1]. They account
for 30 to 40 percent of all hand fractures.
First metacarpal (thumb) fractures make up almost 25 percent of
all metacarpal fractures, placing them second
only to fifth metacarpal fractures in terms of frequency. Of
these fractures, over 80 percent involve the base of the
metacarpal. Thumb fractures occur most often in children (0 to
16 years) and in older patients (>65 years). The
thumb provides approximately 40 percent of hand function so
metacarpal fractures can have grave consequences
[2].
This topic will review issues related to fractures of the first
(thumb) metacarpal. A general overview of metacarpal
fractures is presented separately. (See "Overview of metacarpal
fractures".)
PERTINENT ANATOMY AND CLASSIFICATION The thumb is distinct from
the other fingers anatomically and
biomechanically. Accordingly, fractures to the thumb are
considered separately from other metacarpal fractures.
Thumb anatomy is discussed in greater detail separately. (See
"Finger and thumb anatomy".)
The majority of thumb metacarpal fractures occur at the base.
Fractures of the thumb metacarpal are classified into
four patterns (figure 1). Types I and II are intraarticular
fractures and Types III and IV are extraarticular. Discerning
whether the articular surface is involved in the fracture is
critical as this dictates management.
Type I injury ("Bennett's fracture") is a fracture-dislocation
of the base of the metacarpal ( image 2C). In this
injury, a proximal metacarpal fragment maintains its ulnar
aspect attachment to the trapezium via the volar
ligament. The distal aspect of the metacarpal is supinated and
dislocated radially by the adductor pollicis.
The proximal aspect of this fragment is pulled proximally by the
abductor pollicis brevis and abductor pollicis
longus [3].
Type II injuries ("Rolando's fracture") can be thought of as a
comminuted version of a Bennett's fracture, in
which the fragments may form a T or Y pattern at the base of the
MC (image 1). Severe comminution may
occur and, in these cases, the classic Y or T pattern is not
present. Type II fractures are quite difficult to
treat, but fortunately, are a rare type of first metacarpal
fracture.
Type III fractures are the most common thumb fractures and are
extraarticular ( image 2A-B), eithertransverse or, less commonly,
oblique.
Type IV fractures are extraarticular pediatric injuries
involving the proximal physis and are not addressed in
this review.
MECHANISM OF INJURY First metacarpal fractures typically occur
with an axial load to a partially flexed
thumb. Fistfights are a frequent culprit in these fractures.
First metacarpal fractures can also be seen with
hyperabduction and/or hyperflexion occurring with a fall. If a
torsional force is included in the mechanism, the
fracture will often be oblique. Intraarticular and
extraarticular fractures occur from similar mechanisms.
http://www.uptodate.com.biblioprueba.udp.cl/contents/first-thumb-metacarpal-fractures/abstract/3http://www.uptodate.com.biblioprueba.udp.cl/contents/image?imageKey=EM%2F57258&topicKey=EM%2F193&rank=41%7E150&source=see_linkhttp://www.uptodate.com.biblioprueba.udp.cl/contents/finger-and-thumb-anatomy?source=see_linkhttp://www.uptodate.com.biblioprueba.udp.cl/contents/first-thumb-metacarpal-fractures/abstract/2http://www.uptodate.com.biblioprueba.udp.cl/contents/first-thumb-metacarpal-fractures/abstract/1http://www.uptodate.com.biblioprueba.udp.cl/home/editorial-policyhttp://www.uptodate.com.biblioprueba.udp.cl/contents/first-thumb-metacarpal-fractures/contributor-disclosurehttp://www.uptodate.com.biblioprueba.udp.cl/contents/first-thumb-metacarpal-fractures/contributorshttp://www.uptodate.com.biblioprueba.udp.cl/contents/first-thumb-metacarpal-fractures/contributorshttp://www.uptodate.com.biblioprueba.udp.cl/contents/first-thumb-metacarpal-fractures/contributorshttp://www.uptodate.com.biblioprueba.udp.cl/contents/first-thumb-metacarpal-fractures/contributorshttp://www.uptodate.com.biblioprueba.udp.cl/contents/first-thumb-metacarpal-fractures/contributorshttp://www.uptodate.com.biblioprueba.udp.cl/contents/first-thumb-metacarpal-fractures/contributorshttp://www.uptodate.com.biblioprueba.udp.cl/contents/first-thumb-metacarpal-fractures/contributorshttp://www.uptodate.com.biblioprueba.udp.cl/contents/image?imageKey=EM%2F50297%7EEM%2F63101&topicKey=EM%2F193&rank=41%7E150&source=see_linkhttp://www.uptodate.com.biblioprueba.udp.cl/contents/image?imageKey=EM%2F67033&topicKey=EM%2F193&rank=41%7E150&source=see_linkhttp://www.uptodate.com.biblioprueba.udp.cl/contents/first-thumb-metacarpal-fractures/abstract/3http://www.uptodate.com.biblioprueba.udp.cl/contents/image?imageKey=EM%2F72289&topicKey=EM%2F193&rank=41%7E150&source=see_linkhttp://www.uptodate.com.biblioprueba.udp.cl/contents/image?imageKey=EM%2F57258&topicKey=EM%2F193&rank=41%7E150&source=see_linkhttp://www.uptodate.com.biblioprueba.udp.cl/contents/finger-and-thumb-anatomy?source=see_linkhttp://www.uptodate.com.biblioprueba.udp.cl/contents/overview-of-metacarpal-fractures?source=see_linkhttp://www.uptodate.com.biblioprueba.udp.cl/contents/first-thumb-metacarpal-fractures/abstract/2http://www.uptodate.com.biblioprueba.udp.cl/contents/first-thumb-metacarpal-fractures/abstract/1http://www.uptodate.com.biblioprueba.udp.cl/home/editorial-policyhttp://www.uptodate.com.biblioprueba.udp.cl/contents/first-thumb-metacarpal-fractures/contributor-disclosurehttp://www.uptodate.com.biblioprueba.udp.cl/contents/first-thumb-metacarpal-fractures/contributorshttp://www.uptodate.com.biblioprueba.udp.cl/contents/first-thumb-metacarpal-fractures/contributorshttp://www.uptodate.com.biblioprueba.udp.cl/contents/first-thumb-metacarpal-fractures/contributorshttp://www.uptodate.com.biblioprueba.udp.cl/contents/first-thumb-metacarpal-fractures/contributorshttp://www.uptodate.com.biblioprueba.udp.cl/contents/first-thumb-metacarpal-fractures/contributorshttp://www.uptodate.com.biblioprueba.udp.cl/contents/first-thumb-metacarpal-fractures/contributorshttp://www.uptodate.com.biblioprueba.udp.cl/
-
7/30/2019 First (Thumb) Metacarpal Fractures
2/10
SYMPTOMS AND EXAM FINDINGS Patients with first metacarpal
fractures present with pain, dorsal swelling
over the base of the metacarpal and difficulty with range of
motion (ROM) at the metacarpophalangeal (MCP) and
carpometacarpal (CMC) joints. It is important to distinguish
tenderness at the base of the first metacarpal from
injury to the scaphoid, trapezium, or distal radius. In
addition, if pain, swelling, or ecchymosis occurs more distally
at the MCP joint (particularly on the ulnar side), care should
be taken to look for a potential injury to the ulnar
collateral ligament ("Game Keeper's Thumb"). (See "Ulnar
collateral ligament injury (gamekeeper's or skier's
thumb)".)
RADIOGRAPHIC FINDINGS Three views of the thumb are indicated to
assess potential fractures of the thumb
metacarpal. In addition to lateral and oblique views, a true AP
(Robert's view) should be taken. This view, taken in
maximum pronation, provides good visualization of the CMC joint.
A true lateral (Betts view) of a Bennetts fracture
dislocation can be obtained with the palm on the cassette, and
the hand then pronated 15 to 20 degrees and the
tube angled proximally 15 degrees [3]. Close inspection of an
apparent extraarticular fracture is required to ensure
that no portion of the fracture line involves the joint surface
(image 2A-C). An oblique extraarticular injury can be
confused with a Bennett's fracture. CT scanning is helpful at
times, particularly with regard to potential impaction
injury and to define the CMC joint and fracture fragment
position in intraarticular injuries.
INDICATIONS FOR REFERRAL All intraarticular first metacarpal
fractures warrant referral. Because the integrity
of the CMC joint is crucial to hand function, meticulous
maintenance of the joint surface is required and most
intraarticular fractures require surgical fixation. Less than 1
mm of displacement is desired for optimal outcome [4].
Extraarticular fractures, on the other hand, are usually managed
without surgical intervention. However, if adequate
reduction either cannot be attained by closed manipulation or
maintained, referral is indicated. This is particularly
important in transverse extraarticular fractures, which often
have apex radial angulation. Due to the relatively
unstable nature of oblique fractures, patients should be
informed about the risk of displacement of these fractures,
particularly in those requiring reduction.
INITIAL TREATMENT Splinting is used in the initial
immobilization of metacarpal fractures [1,5]. A detailed
description of the techniques for applying splints is presented
separately. (See "Splinting of musculoskeletal
injuries" and "Patient information: Cast and splint care (Beyond
the Basics)".)
Intraarticular fractures Intraarticular fractures of the first
metacarpal (ie, Type I - Bennett's fracture dislocation
and Type II - Rolando's fracture) should be managed initially
using a thumb-spica splint (picture 1) with theinterphalangeal (IP)
joint free and the wrist in 30 degrees of extension prior to being
referred to orthopedics within
two to three days. These patients should aggressively ice and
elevate the hand and will need adequate analgesia.
Extraarticular fractures Non-displaced extraarticular fractures
of the first metacarpal should be placed in a
short arm thumb-spica splint with the wrist in 30 degrees of
extension and the splint extending to the IP joint and
followed up in one week (picture 1). (See "Splinting of
musculoskeletal injuries".)
If the fracture is oblique or alignment is questionable, the
patient should be seen back within three to five days. Up
to 30 degrees of residual angularity is tolerated without
functional impairment due to the inherent mobility of the
thumb. Extraarticular fractures with >30 degrees of
angulation require reduction (see 'Closed reduction' below).
Definitive treatment for extraarticular fractures is thumb spica
cast (with IP joint free) for four to six weeks.
Patients should be made aware that significant swelling or
overly aggressive icing to this radial side of the thumb
can cause a temporary palsy to the superficial radial nerve
resulting in numbness over the dorsum of the thumb.
Closed reduction For angulated extraarticular fractures of the
first metacarpal, closed reduction is appropriate
prior to splinting. Reduction is typically performed by an
orthopedic surgeon for thumb metacarpal fractures,
however, if reduction is indicated and the treating clinician is
comfortable with the procedure, or if there is no referral
option available, reduction of extraarticular first metacarpal
fractures can be achieved in the following manner:
Anesthesia is generally readily achieved via hematoma block.
Placement of a hematoma block for
metacarpal fractures is described separately. (See "Metacarpal
shaft fractures", section on 'Anesthesia'.)
http://www.uptodate.com.biblioprueba.udp.cl/contents/metacarpal-shaft-fractures?source=see_link&anchor=H13#H13http://www.uptodate.com.biblioprueba.udp.cl/contents/first-thumb-metacarpal-fractures?topicKey=EM%2F193&elapsedTimeMs=0&source=search_result&searchTerm=fracture&selectedTitle=41%7E150&view=print&displayedView=full#H10http://www.uptodate.com.biblioprueba.udp.cl/contents/splinting-of-musculoskeletal-injuries?source=see_linkhttp://www.uptodate.com.biblioprueba.udp.cl/contents/image?imageKey=EM%2F81987&topicKey=EM%2F193&rank=41%7E150&source=see_linkhttp://www.uptodate.com.biblioprueba.udp.cl/contents/image?imageKey=EM%2F81987&topicKey=EM%2F193&rank=41%7E150&source=see_linkhttp://www.uptodate.com.biblioprueba.udp.cl/contents/cast-and-splint-care-beyond-the-basics?source=see_linkhttp://www.uptodate.com.biblioprueba.udp.cl/contents/splinting-of-musculoskeletal-injuries?source=see_linkhttp://www.uptodate.com.biblioprueba.udp.cl/contents/first-thumb-metacarpal-fractures/abstract/1,5http://www.uptodate.com.biblioprueba.udp.cl/contents/first-thumb-metacarpal-fractures/abstract/4http://www.uptodate.com.biblioprueba.udp.cl/contents/image?imageKey=EM%2F72289%7EEM%2F50297%7EEM%2F63101&topicKey=EM%2F193&rank=41%7E150&source=see_linkhttp://www.uptodate.com.biblioprueba.udp.cl/contents/first-thumb-metacarpal-fractures/abstract/3http://www.uptodate.com.biblioprueba.udp.cl/contents/ulnar-collateral-ligament-injury-gamekeepers-or-skiers-thumb?source=see_link
-
7/30/2019 First (Thumb) Metacarpal Fractures
3/10
Once adequate anesthesia is confirmed, apply gentle longitudinal
traction to the distal fragment while
applying pressure over the apex of the fracture and extending
the IP joint. Mild pronation of the distal
fragment may also help to achieve anatomic alignment. The
fracture should then be immobilized with a
thumb spica cast and post-reduction x-rays should be obtained to
confirm alignment.
FOLLOW-UP CARE Non-displaced fractures and those fractures with
good initial reduction should be seen and
reimaged in 7 to 10 days. Patients with oblique fractures or
questionable reduction require imaging within three to
five days. If follow-up films reveal angulation greater than 30
degrees, repeat reduction or referral is indicated.
Fractures with stable position should be placed in a short arm
thumb spica cast with the wrist in 30 degrees of
extension and the IP joint free. Radiographs should be repeated
at two-week intervals and immobilization should be
continued for a total of four weeks.
Following immobilization, act ive ROM exercise is initiated.
Total healing time is six to eight weeks.
RECOMMENDATIONS FOR RETURN TO WORK OR SPORT Patients requiring
repetitive gripping at work can
expect return to regular duty after they are pain free, the
fracture site is nontender, and functional range of motion
has been reestablished. If the patient desires return to contact
sport, the thumb should be protected in a club-type
pad or a firm thumb-spica orthosis for an additional six to
eight weeks.
SUMMARY AND RECOMMENDATIONS
First (thumb) metacarpal fractures are common and generally
involve the base of the metacarpal.
The thumb is integral to normal function of the hand. Due to the
unique anatomy and biomechanics of the
thumb, first metacarpal fractures are described and managed
differently than other metacarpal fractures.
(See 'Pertinent anatomy and classification' above and 'Mechanism
of injury' above.)
Thumb metacarpal fractures are divided into two large groups:
intraarticular and extraarticular. (See
'Radiographic findings' above.)
Intraarticular fractures require orthopedic referral and
generally need surgical fixation. (See 'Indications for
referral' above.)
Extraarticular fractures are typically managed in a closed
fashion with thumb-spica immobilization and rarely
require surgery. Extraarticular fractures do not require perfect
anatomic reduction and can tolerate up to 30
degrees of angulation. (See 'Initial treatment' above.)
Oblique extraarticular fractures should be carefully
differentiated from Bennett's fractures, are prone to
displacement, and need to be observed closely (particularly
during the initial two weeks).
ACKNOWLEDGMENTS We are saddened by the untimely death of John
Marx, MD, who passed away in July
2012. We wish to acknowledge Dr. Marx's dedication and his many
contributions to UpToDate, in particular, his
work as editor-in-chief for Emergency Medicine and as a section
editor and author for Adult Trauma.
The author and editors would also like to acknowledge Kevin E
Burroughs, MD, who contributed to earlier versions
of this topic review.
Use of UpToDate is subject to the Subscription and License
Agreement.
Topic 193 Version 7.0
http://www.uptodate.com.biblioprueba.udp.cl/contents/licensehttp://www.uptodate.com.biblioprueba.udp.cl/contents/first-thumb-metacarpal-fractures?topicKey=EM%2F193&elapsedTimeMs=0&source=search_result&searchTerm=fracture&selectedTitle=41%7E150&view=print&displayedView=full#H7http://www.uptodate.com.biblioprueba.udp.cl/contents/first-thumb-metacarpal-fractures?topicKey=EM%2F193&elapsedTimeMs=0&source=search_result&searchTerm=fracture&selectedTitle=41%7E150&view=print&displayedView=full#H6http://www.uptodate.com.biblioprueba.udp.cl/contents/first-thumb-metacarpal-fractures?topicKey=EM%2F193&elapsedTimeMs=0&source=search_result&searchTerm=fracture&selectedTitle=41%7E150&view=print&displayedView=full#H5http://www.uptodate.com.biblioprueba.udp.cl/contents/first-thumb-metacarpal-fractures?topicKey=EM%2F193&elapsedTimeMs=0&source=search_result&searchTerm=fracture&selectedTitle=41%7E150&view=print&displayedView=full#H3http://www.uptodate.com.biblioprueba.udp.cl/contents/first-thumb-metacarpal-fractures?topicKey=EM%2F193&elapsedTimeMs=0&source=search_result&searchTerm=fracture&selectedTitle=41%7E150&view=print&displayedView=full#H2
-
7/30/2019 First (Thumb) Metacarpal Fractures
4/10
GRAPHICS
Base of the first metacarpal fracture types
Type I (Bennet's fracture-dislocation) and type II
(Rolando's
fracture) are intraarticular. Type III fractures are
extraarticular,either transverse (IIIA) or oblique (IIIB). Type IV
fractures areseen only in children and involve the proximal
epiphysis.Reproduced with permiss ion from: Eiff MP, Hatch RL,
Calmbach WL. FractureManagement for Primary Care, 2nd ed., W.B.
Saunders 2002. Copyright 2002 Elsevier.
-
7/30/2019 First (Thumb) Metacarpal Fractures
5/10
Fracture of thumb metacarpal base: Type I (Bennett's)
Each of these anteroposterior radiographs shows an
intra-articular fracture of the thumb metacarpal. The Type I
or"Bennett's" fracture of the proximal 1st metacarpal
illustratedhere is characterized by its articular involvement and
thepersistent attachment of the volar fragment to the
trapezium.Courtesy of Kevin Burroughs, MD.
-
7/30/2019 First (Thumb) Metacarpal Fractures
6/10
Fracture of the 1st metacarpal base: Type II (Rolando)
This plain radiograph shows a comminuted, intraarticular
fractureof the thumb metacarpal. The eponym for this injury
isRolando's fracture.Courtesy of Kevin E. Burroughs, MD.
-
7/30/2019 First (Thumb) Metacarpal Fractures
7/10
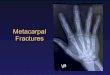
Extraarticular fracture of the first metacarpal
This anteroposterior radiograph shows a type III fracture of
theproximal 1st metacarpal with characteristic sparing of
thearticular surface. Significant shortening of the metacarpal is
alsoapparent in this view.Courtesy of Kevin Burroughs, MD.
-
7/30/2019 First (Thumb) Metacarpal Fractures
8/10
Nondisplaced thumb metacarpal fracture
In this radiograph a nondisplaced fracture of the
thumbmetacarpal distal to the carpal metacarpal joint is seen. This
is anondisplaced type III fracture of the first metacarpal.Courtesy
of Kevin Burroughs, MD.
-
7/30/2019 First (Thumb) Metacarpal Fractures
9/10
Thumb spica splint
The thumb spica splint provides excellent immobilization for
thethumb. It is often used for carpometacarpal osteoarthritis,
deQuervain's tenosynovitis, ulnar collateral ligament
injury(gamekeeper's or skier's thumb), and fractures of the
scaphoid,trapezium, and first metacarpal.Courtesy of Bruce C
Anderson, MD.
-
7/30/2019 First (Thumb) Metacarpal Fractures
10/10
2013 UpToDate, Inc. All rights reserved. | Subscr iption and
License Agreement | Release: 21.3 - C21.33
Licensed to: Universidad Diego Portales | Support Tag:
[1103-200.14.85.85-BF9EDC724C-I297751.14]
http://www.uptodate.com.biblioprueba.udp.cl/contents/license