Embed Size (px)
Citation preview
University of Michigan Health SystemProgram and Operations Analysis
Standardization of Resident Patient HandoffFinal Report
To:Christopher Scally, Department of Surgery Resident, University of Michigan Hospital
Mary Duck, Industrial Engineer Expert, Program and Operations AnalysisMatthew Shirer, Industrial Engineer Fellow, Program and Operations Analysis
Mark Van Oyen, Associate Professor, IOE Department, University of Michigan
From:IOE 481 Project Team 5
Melinda Alberty, Student, IOE Department, University of MichiganKevin Michaud, Student, IOE Department, University of Michigan
Matthew Rouhana, Student, IOE Department, University of MichiganNicolaas van Dijk, Student, IOE Department, University of Michigan
Date: April 22, 2014
Table of ContentsExecutive Summary.........................................................................................................................1
Introduction..................................................................................................................................1
Methods........................................................................................................................................1
Findings and Conclusions............................................................................................................1
Recommendations: Pre-Pilot Study.............................................................................................2
Pilot Study....................................................................................................................................3
Future Work.................................................................................................................................3
Introduction......................................................................................................................................4
Background......................................................................................................................................4
Key Issues....................................................................................................................................5
Goals and Objectives...................................................................................................................6
Project Scope................................................................................................................................6
Methods...........................................................................................................................................6
Literature Search..........................................................................................................................6
Observations and Time Studies....................................................................................................7
Interviews.....................................................................................................................................7
Surveys.........................................................................................................................................7
Tally Sheets..................................................................................................................................8
Pilot Study....................................................................................................................................8
Findings and Conclusions................................................................................................................8
Mnemonic Device........................................................................................................................8
Quiet Location..............................................................................................................................9
Training Program.........................................................................................................................9
In-Person Morning Handoff.......................................................................................................10
Recommendations: Pre-Pilot Study...............................................................................................10
Implement Mnemonic Device....................................................................................................11
Require Quiet Location..............................................................................................................11
Develop Training Program.........................................................................................................11
Convert Morning Handoff to In-Person.....................................................................................11
ii

Pilot Study.....................................................................................................................................12
Pilot Study Methods...................................................................................................................12
Pilot Study Validation................................................................................................................12
Pilot Study Results.....................................................................................................................12
Final Recommendations................................................................................................................13
Expected Impact............................................................................................................................14
Future Work...................................................................................................................................14
Works Cited...................................................................................................................................16
Additional References...................................................................................................................16
Appendices....................................................................................................................................17
Appendix A: Preliminary Interview Questions..........................................................................18
Appendix B: Preliminary Survey Questions..............................................................................19
Appendix C: Preliminary Survey Results..................................................................................20
Appendix D: Tally Card Sample................................................................................................26
Appendix E: Pilot Interview Questions.....................................................................................27
Appendix F: Pilot Survey Questions..........................................................................................28
Appendix G: Pilot Survey Results.............................................................................................29
iii
List of Figures and Tables
Figure 1: Current Patient Handoff Process………………………………………………………. 5Figure 2: Survey Response Data Regarding Desired Handoff Categories………………………. 9Figure 3: Standardized Template for Email Handoff…………………………………………... 12Figure 4: Comparison of Handoff Times……………………………………………………….. 13
iv

Executive Summary
IntroductionResidents must transfer the responsibility of patient care between each other more often due to a decrease in the number of hours per week they can work. This transfer of patient information is called a handoff. Handoffs involve transferring a variety of patient information such as medical history, diet, medications, allergies, and potential issues. The current handoff process is unstructured and prone to communication errors. The Department of Surgery at the University of Michigan wishes to standardize their morning and evening handoffs between residents for the elective surgery service. The team believes the project will improve overall communication, reduce communication errors, and improve process efficiency.
MethodsThe team used seven different methods in order to develop the best approach for standardizing resident patient handoffs:
Selected eight technical papers. The team performed a literature search on other projects related to patient handoffs in order to find techniques that have been successful for similar professional projects.
Observed and timed five in-person handoffs. In order to determine a baseline scenario, the team observed and timed in-person handoffs.
Observed 24 email handoffs. The team examined email handoffs to determine if they are necessary for the morning handoff, and if so, to standardize them.
Performed seven interviews. To gain input from the residents who have first-hand experience with the handoff process, the team interviewed residents to find what works well and what does not work well from the resident point of view.
Received 24 resident survey results. The team surveyed residents to gain input about the handoff process with the additional goal of receiving numerical data to better justify the team’s recommendations.
Developed tally cards to mark errors. The goal of the tally card was to quantify errors seen by on-shift residents related to missing/incorrect handoff information. Due to low response rates, the tally cards were discontinued.
Findings and ConclusionsThe team used findings from the aforementioned methods to make the following conclusions:
The team concluded that a tailored mnemonic device will standardize the handoff process while including necessary patient information to reduce errors and missing information.
o Literature search – hospitals around the United States use mnemonics for the handoff process
1

o Observations – each resident conducts handoffs differently, there is even variation within a single resident’s handoffs
o Survey – residents marked categories of patient information they wanted to see in the handoff
The team concluded that the handoff should occur in a quiet location with computer access.
o Observations – locations can be noisy and distracting (House Officer’s Lounge, ward conference rooms, Surgical ICU)
o Survey – residents think a quiet location would be beneficial
The team concluded that the handoff process requires a training program incorporated into the resident orientation and supervision for new residents.
o Literature search – literature recommends a training program for the handoff process
o Survey – residents asked for the opportunity to learn the handoff process more thoroughly and practice it during orientation
o Client discussion – residency programs have requirements for the number of hours interns must be supervised
The team concluded that an in-person handoff is preferable to an email handoff as it allows for better communication, the ability to ask questions, and a more thorough understanding of each patient’s medical situation.
o Observations – residents use time during in-person handoffs to ask questionso Interviews – mixed opinions regarding the email handoffo Survey – according to a Department of Surgery resident, a previous survey
conducted by the Department of Surgery showed that in-person handoffs take less time than the current email handoff process
Recommendations: Pre-Pilot StudyThe team developed the following recommendations to standardize the handoff process:
Implement the mnemonic device InterSECT for residents to use during the handoff.1. Inter – Introduction (Name, Operation, Post-Op Day)2. S - Stability3. E - Events4. C - Changes5. T - To-do (Action Items)
Require that all handoffs occur in a quiet environment, away from distractions.By encouraging greater focus on the handoff itself, and preventing the residents from being interrupted by others, this will facilitate better communication and reduce the likelihood of error. The team recommends that access to a computer is maintained.
Develop a training program to teach proper handoff procedure to new residents.
2
All new residents would go through this program during resident orientation, to learn and practice the procedure correctly. The team also recommends that new residents be observed giving handoff by a senior resident 2-3 times during their first month of residency.
Convert the morning email handoff to an in-person handoff.The in-person handoff would take less time, improve communication, and provide an opportunity for questions. The transition should be made in July 2014, when the new residents begin work. For the interim period, the team has developed a standardized email template based on the InterSECT mnemonic device.
Pilot StudyThe team implemented a pilot study of the InterSECT mnemonic with select residents. The residents used the mnemonic during handoff while the team observed and collected feedback. Overall, the residents thought the mnemonic was an improvement to the current handoff method. Also, the mnemonic does not add a significant amount of extra time to current handoff method. However, the residents offered feedback on how to improve the mnemonic and the team adjusted it accordingly. First, the introduction section can be limited for known patients. Second, Concerns replaces Changes so that the sections are more clearly defined and information does not overlap. Finally, the team recommends that the process be interactive and that residents ask questions throughout, to minimize the risk of miscommunication.
Future WorkIn addition to the team’s recommendations, there are several other areas the Department of Surgery may consider improving in the future:
The mnemonic device should be integrated with the rounding sheets from the new electronic medical records system.
The morning email handoff should be done in person to facilitate better communication. The incoming residents should receive formal training on how to perform handoffs. This
training can be implemented starting in July 2014 with the incoming residents. Handoffs should be performed in the new Department of Surgery resident room once its
construction is completed. The physician assistants’ handoffs to the residents in the afternoon should be addressed.
3

Introduction
Due to recent Accreditation Council for Graduate Medical Education (ACGME) regulation changes, surgical residents’ work hours have been drastically reduced leading to shorter shifts. Surgical patients are primarily under the care of residents. Therefore, residents transfer the responsibility of caring for patients more often, through handoffs at the ends of their shifts. End-of-shift handoffs may be unstructured and prone to communication errors, which may impact patients’ care and lead to delays and adverse events.
Thus, a fourth-year resident from the Department of Surgery at the University of Michigan asked an Industrial and Operations Engineering (IOE) 481 student team from the University of Michigan to standardize the handoff process. The team performed a literature search, observed and time studied the current process, interviewed resident and attending surgeons about the handoff process, developed and conducted resident surveys, distributed tally cards, and reviewed emails. Based on this information, the team developed recommendations to standardize the patient handoff process and reduce communication errors. This report presents the team’s findings, conclusions, and recommendations to standardize the handoff process.
Background
Federal legislation has restricted residents to 80-hour work weeks in order to reduce their fatigue. This change has increased the number of handoffs between residents. Patient handoffs (sometimes referred to as signouts) are a transfer of patient information between care providers, which may include a patient summary, lab results, allergies, a care plan, diet, vitals, and other relevant information about the patient. Due to this increased number of handoffs and variety of information in a handoff, there are many opportunities for miscommunication. Thus, hospitals around the country have standardized handoff processes in place.
The Department of Surgery at the University of Michigan performs two inpatient general surgery services: elective surgeries and emergent surgeries. These services include surgery and post-operative care. The care team for each patient consists of an attending surgeon, chief resident, mid-level residents, junior residents, and physician assistants.
For the elective surgeries, the daily workflow in the Department of Surgery is as follows (times are approximate):
1. 6AM: The overnight junior resident emails the daytime care team regarding overnight events.
2. Between 6AM and 8AM: The care team performs rounds, visiting their patients and discussing a plan for care with the attending surgeon.
3. After rounds: Mid-level residents perform elective surgeries while physician assistants and junior residents provide care to postoperative patients.
4. 3PM: The physician assistants email patient status, progress, and discharge along with “to-do” list to the remainder of the daytime care team.
4

5. 5PM: The chief resident and a daytime junior resident perform evening rounds to further discuss plans of care for each patient.
6. 6PM: The daytime junior residents hand off patients to the overnight junior resident.
Figure 1. Current Patient Handoff Process (Department of Surgery Resident)
The Department of Surgery relies heavily on handoffs between residents; however, the department does not have a seamless or standardized process for handing off patients. Thus, handoffs may be susceptible to miscommunication, which can lead to adverse events. Therefore, the IOE 481 team investigated how handoffs occur and developed best practices for how to hand off patients.
Key IssuesA standard process for patient handoffs is necessary for the following reasons:
Handoffs are not standardized Handoffs have been identified as a potential source of error and unnecessary delays Handoffs may contain inefficiencies
By standardizing the handoff process, the team hopes to address the above issues. This will lead to reduced communication errors and increased efficiency. Furthermore, changing the handoff process is expected to increase the quality of patient care.
5

Goals and ObjectivesTo determine areas of potential miscommunication during resident handoffs, the team completed the following tasks:
● Conducted a literature search● Observed the current handoff process● Interviewed residents about the handoff process● Performed time studies● Administered surveys● Performed a pilot study
With this information, the team:
● Standardized the handoff process● Reduced communication errors during resident handoffs● Reduced process inefficiencies
The results of this project are also expected to improve the quality of patient care.
Project ScopeCurrently handoffs occur at the end of each shift: at 6 AM, when the overnight intern emails the daytime team; at 3 PM, when the physician assistants email the remaining daytime team; and at 6 PM, when the daytime team verbally hands off to the overnight resident. This project focused on the 6 AM and 6 PM handoffs for the elective surgery service.
This project did not include hospital operations outside of patient handoffs. The team will not analyze surgery processes or the care of patients in the surgery department or any other department related to patient handoffs. Handoffs related to other departments, emergent surgery, or the nursing staff will not be considered. However, the team hopes that the University of Michigan Hospital can use the developed system as an example for other departments having similar issues.
Methods
The team used seven different methods to understand and standardize the Department of Surgery handoff process: literature search, observations, time studies, interviews, surveys, tally cards, and a pilot study.
Literature SearchThe team performed a literature search and compiled eight research papers to gather information on standardized handoffs at other institutions. From the information, the team determined best practices, such as specific areas of patient care to include in the patient handoff. These best practices were incorporated into the recommendations to the Department of Surgery.
6

Observations and Time StudiesThe team observed the Department of Surgery’s current handoff process between the day and night shift residents. The team used observations in conjunction with other forms of data collection to propose changes to the current process. Furthermore, the information collected in the time studies was used to ensure that the new process is not significantly longer than the current process.
Five pre-pilot observations were completed and four post-pilot observations were performed to assess the effectiveness of the changes. To perform observations, the team received resident contact information from the client and contacted the resident on call upon arrival at the hospital.
During observations, the team members performing the observations also performed simple time studies. The team recorded the amount of time the handoff process took and the number of patients that were discussed. The team used this information to determine the average time spent discussing one patient during a handoff.
InterviewsThe team conducted preliminary interviews with six resident surgeons and one attending surgeon. Three of the residents were in their third year of residency, two were in their fourth year, and one was a chief (seventh year) resident. The interviews were conducted to better understand the goals of residents during the handoff process and to gather recommendations to improve that process.
The preliminary interviews were conducted individually, with each team member interviewing only one resident at a time. The questions that were discussed in this interview can be found in Appendix A. Team members audio recorded each interview and listened to the recordings later, taking detailed notes. Along with the free response sections of the survey, the interview data was used to better understand concerns of the residents and gather subjective recommendations.
After implementation of the pilot, the team performed four more pilot interviews to receive feedback on the proposed method. The questions asked in the pilot interview can be seen in Appendix E. More detail on the pilot interviews will be covered in the pilot section of this report.
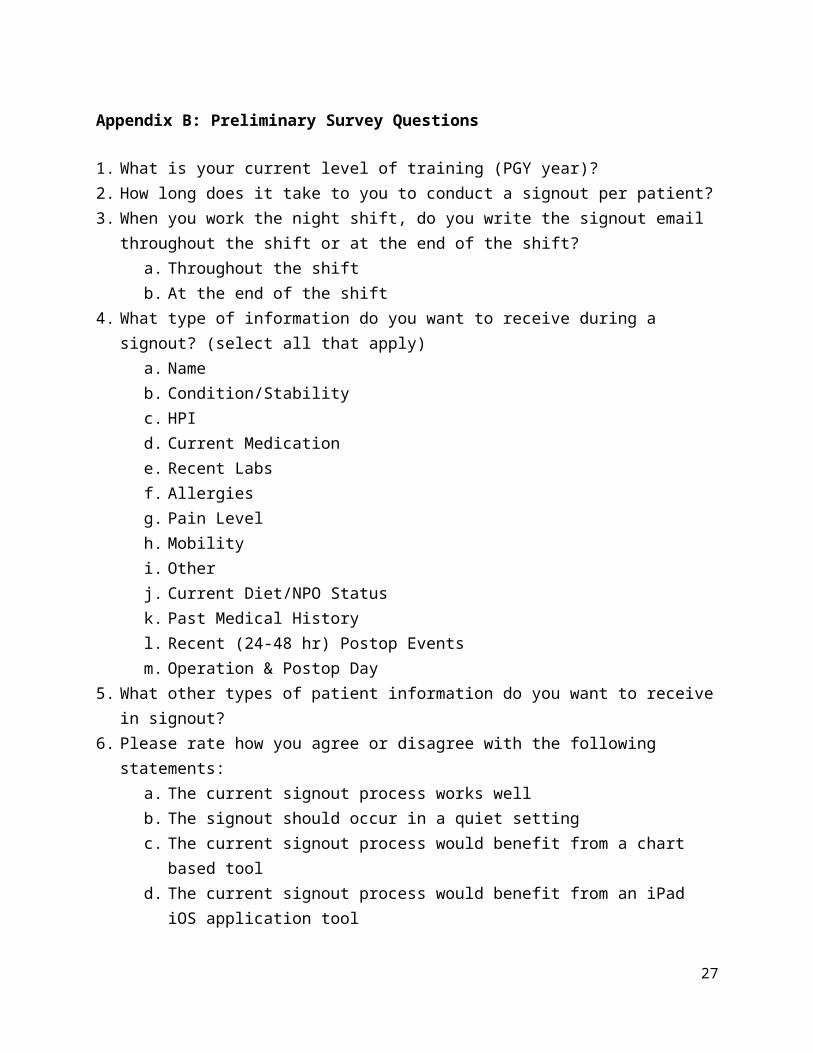
SurveysThe team created a preliminary survey for the residents to quantify their concerns related to the handoff process. The surgery resident and POA coordinators reviewed the preliminary survey questions and the team revised them accordingly. Once revised, this survey was sent via Qualtrics for the residents to complete on February 28th, 2014. Preliminary survey questions can be found in Appendix B and the respective results can found in Appendix C. The team received 24 responses from the 42 residents and analyzed the results. The findings from this analysis were used in developing the recommendations.
A pilot survey was also developed by the team and was used to gain further information on the proposed method. Pilot survey questions and results can be viewed in Appendix F and Appendix G respectively. One response was given and will be covered in more detail in the pilot section of this report.
7

Tally SheetsThe team also developed a tally system to determine whether or not residents find inefficiencies during their shift due to missing information from the previous handoff. The night-shift resident would record the number of times information was not included in a handoff by placing a tally into one of six categories. The categories on the tally card were developed by the team and approved by the surgery resident. Appendix D shows a sample of the tally card, front and back. The tally cards were sent out to the residents to fill out on February 28th, 2014. The team collected 2 tally cards; however the information on the cards was incomplete and could not be used in developing recommendations.
Pilot StudyAfter the team completed its analysis of the data and interviews, a pilot of the developed standardized handoff process was implemented. The purpose of the pilot study was to test the team’s revisions of the handoff process prior to full implementation. In this way, the team made minor changes based on suggestions given by the residents participating in the pilot. The team performed the pilot with four different combinations of residents conducting a handoff.
Findings and Conclusions
Based on the methods previously discussed, the team has compiled findings and made the following conclusions.
Mnemonic DeviceThe literature search focused on the best practices of various hospitals around the United States. The hospitals discussed in the articles reviewed used a standard mnemonic for the handoff process. The mnemonic provides a template for residents to ensure they discuss the important areas of patient care as decided by the individual hospital. Additionally, each hospital used a mnemonic that was short and easy to remember.
The observations revealed that the handoffs were different during each observation and varied significantly between residents.
The preliminary survey revealed the categories of information residents want in a handoff. Figure 2 shows the percent of respondents who wanted each category of patient information in the handoff. There is a wide variety of categories that residents felt were important to the handoff, but some categories were very common. The team was able to incorporate the top five responses into the recommended mnemonic.
8

Figure 2. Survey Response Data Regarding Desired Handoff Categories (preliminary survey, n = 24, February 27, 2014 – March 12, 2014)
From these findings, the team developed three conclusions1. Mnemonics are an easy-to-remember and tailored way to standardize the handoff process.2. A standard format will help to ensure that all desired patient information will be handed
off accurately and thoroughly. 3. A standard format will reduce the number of errors or missing information that may
result from a handoff.
Quiet LocationThe team observed handoffs in various locations including the House Officer’s Lounge, conference rooms in the wards, and the Surgical Intensive Care Unit (SICU). Observations revealed that these locations present various distractions to the residents such as television and other in-person or phone conversations, which can make them noisy. Furthermore, observations showed that residents often use the computers during the handoff to look up patient information.
The preliminary survey responses showed that 79% of residents felt a quiet handoff location would be beneficial. Therefore, the team concluded that the handoff should occur in a quiet location with computer access.
Training ProgramAccording to the team’s literature search, 75% of papers reviewed recommend an educational program in addition to a standardized handoff process.
9

In the free response section of the preliminary survey, two residents expressed interest in having the opportunity to learn the expectations and be given the chance to practice the handoff process during orientation.
Through discussions with the client, the team learned about the residency program’s requirements for interns to be supervised by senior residents.
The team concluded that the handoff process requires a robust training program for incoming residents in addition to supervision for new residents. This training will allow new residents to perform accurate and thorough handoffs. Furthermore, the team incorporated oversight by senior residents for interns into the recommendations.
In-Person Morning HandoffAccording to one article, “face-to-face handoffs are preferable” because “written and verbal communication occur together”, which “provides multiple channels for the information to be explained” [1].
During observations, the team found that residents take time during the in-person handoff to clarify points and ask questions. The interviews revealed that an email handoff does not allow for this kind of interactive exchange of information.
The team found mixed opinions about the morning handoff email. An interview with a chief resident showed that they prefer an email handoff from the overnight resident. According to the attending surgeon interview and resident interviews, they believe the email adds extra work and that the in-person handoff is preferable.
Additionally, according to a Department of Surgery resident, a survey conducted by the Department of Surgery previously showed that an in-person handoff takes less time than an email handoff.
The team concluded that an in-person handoff is preferable to an email handoff as it allows for better communication, the ability to ask questions, and a more thorough understanding of each patient’s medical situation.
Recommendations: Pre-Pilot Study
Using the findings and conclusions, the team developed the following recommendations for the Department of Surgery. These recommendations focus primarily on standardizing the process, with the expectation that the department will look for ways to continuously improve the process in the future. The team’s recommendations are: using a mnemonic device to standardize the handoff process, requiring that handoffs occur in a quiet location that is isolated from distractions, developing an educational training program to teach residents the handoff process, and switching the morning handoff email to an in-person handoff.
10

Implement Mnemonic DeviceThe team developed the mnemonic device InterSECT for the residents to use during the handoff. The mnemonic can be broken down as follows:
1. Inter - Introduction* : The introduction should contain basic patient identifying information. This includes name, age, procedure, post-op day, and a brief case history.
2. S - Stability : This section details the stability of the patient (critical, healthy, etc.).3. E - Events : This includes all major events that have occurred in the last 24 hours, as well
as any other events in the patient’s care history that the outgoing resident feels are worth noting.
4. C - Changes* : The changes section contains any pertinent changes to the patient care plan or changes in patient health trends. Examples include diet, medication, pain, mobility, vitals trends, etc.
5. T - To-do : This is a list of action items for the patient that should be completed in the upcoming shift.
*These sections were amended upon receiving resident feedback during the pilot study. These amendments will be addressed later in the paper.
The team recommends this mnemonic device as the primary means of standardizing the handoff procedure itself. It is short, easy to remember, and contains all pertinent handoff information.
Require Quiet LocationDue to distractions and noise in the current handoff locations, the team recommends that all handoffs occur in an isolated, quiet location set aside for handoffs. This will minimize distractions present, prevent the residents from being disturbed by others, and allow them to focus solely on the handoff. This will thus contribute to a higher quality of communication between the two residents, reducing the chances for communication error.
Additionally, the team recommends that access to a computer connected to the electronic medical records be maintained, as the residents often use a computer to access lab and imaging results, as well as other patient data.
Develop Training ProgramFrom findings in the literature search and survey, the team recommends that a formal handoff training program be developed to teach proper handoff procedure to new residents. The goal of establishing this program is to ensure that handoff standardization is consistent. All residents would go through this training program during resident orientation. This will allow them to learn the handoff process and give them an opportunity to practice it with their peers before they begin their residency. Along with the training program, the team recommends that PGY-1 residents are observed giving handoff by a senior resident 2-3 times during their first month of residency. This will allow new residents to get further instruction and feedback.
Convert Morning Handoff to In-PersonFinally, the team recommends that the email handoff used by the night resident be retired from use, and that it be converted to an in-person handoff. This will save the residents time, improve the quality of communication, and give the day team a chance to ask questions.
11

Due to the number of people that would be affected by this transition, the team recommends that the change be made when the new group of residents begins their residency in July 2014. For the interim period, the team has developed a standardized email template based on the InterSECT mnemonic device. The team recommends that this be implemented as soon as possible and that it be used until the transition to in-person handoffs has been made. The template is shown in Figure 3 below.
Figure 3: Standardized Template for Email Handoff
Pilot Study
After the data analysis was complete, the team implemented a pilot study of the mnemonic device with the residents. The residents were asked to use the InterSECT mnemonic when handing off patients while the team observed and took notes.
Pilot Study MethodsOn four different occasions, the team met with residents to conduct the pilot study. The outgoing resident was given a reference card which detailed each letter of InterSECT. The resident was then asked to tailor his or her handoff to the mnemonic. Two members of the IOE 481 team observed and timed each of the handoffs. Once the handoff was complete, the team interviewed both of the residents about what they liked and what they would improve. The night resident was also sent a survey with 5 questions to quantify the preferences of the residents.
Pilot Study ValidationThe team decided that InterSECT could be validated in two different ways. The first looked to see if the residents thought the mnemonic was an improvement on the current handoff process. The second was to see that the mnemonic would not increase the baseline time per patient of 56 seconds.
Pilot Study Results87% of the residents who participated in the pilot study believed the mnemonic was an improvement over the current method. Figure 4 shows that while the time per patient was greater
12
for the pilot than the current state, the time per patient decreased between the perceived survey data and the pilot study.
Figure 4. Comparison of Handoff Times (time studies, preliminary survey, time studies; n = 5, n = 24, n = 4; February 3, 2014 – March 24, 2014, February 27, 2014 – March 12, 2014; April 3,
2014 – April 11, 2014)
The mnemonic increased the time per patient from the baseline by 27 seconds. However, this increase can be attributed to the residents being unaccustomed to the new method. Furthermore, the team made adjustments to the recommendations based on resident feedback which will decrease the handoff time.
The residents offered three main points of feedback. 1. Residents believed that the “Introduction” section of the mnemonic was unnecessary for
patients with which the incoming resident was familiar. 2. Residents believed that the Events and Changes sections of the mnemonic were
redundant and felt that the information could be grouped into either of these categories.3. Residents wanted a section for asking questions.
Final Recommendations
Following the completion of the pilot study, the team suggests three improvements to the mnemonic in addition to the previous recommendations.
1. When both residents know the patient, they should limit the “Introduction” section to consist of only the patient’s name.
13

2. Replace the “Changes” section with a “Concerns” section so that patient information fits better in the categories of the mnemonic. “Concerns” includes information about potential problems the patient might face and anything the residents are worried about in the immediate future.
3. The residents should be encouraged to ask questions throughout the mnemonic to facilitate an interactive process.
Expected Impact
The team used a combination of observations, interviews with surgery residents, time studies of the current state, surveys of surgery residents, and a pilot study to develop and recommend a standard handoff process for use in the Department of Surgery. This recommendation will improve efficiency and quality in the handoff process. Specifically, the following outcomes can be expected:
Improved overall communication Reduced communications errors Increased process efficiency
These changes are further expected to increase the quality of patient care.
Future Work
The team has identified five areas where the department of surgery can further improve the handoff process in the future.
1. The team recommends that the rounding sheets be revised after the department switches to the electronic medical record system. Specifically, the mnemonic device should be integrated into the structure of the rounding sheet, to allow for ease of use and compatibility with recommended handoff procedure.
2. The team suggests that the morning email handoff be changed to an in-person handoff, similar to the process that takes place at night. Using the mnemonic in the morning handoff will help to alleviate the difficulties seen in the typical email handoff. By allowing the receiving resident to ask clarifying questions, communication errors can be avoided. These questions are nearly impossible to ask in an email handoff. Furthermore the team found that in-person handoffs require less time on average than a typical email handoff.
3. The team recommends that the Department of Surgery develops a formal handoff curriculum for resident orientation. This curriculum should be implemented for the next group of residents entering this program in July 2014. A formal handoff curriculum will allow the new residents to practice the recommended mnemonic and fine tune the information that needs to be addressed in a typical handoff.
4. Pending the completion of the new resident room, the team suggests that handoffs take place in this location. According to the client, this new room will provide residents with the quiet environment needed to perform a successful patient handoff.
14

5. Finally the team recommends that the PA handoff that takes place in the middle of the day be further examined. Since this specific handoff was not in scope for this project, the team recommends that the surgery department looks for ways to improve this handoff by drawing from the recommendations section of this report.
15

Works Cited
[1] D. J. Solet, J. M. Norvell, G. H. Rutan, and R M. Frankel. "Lost In Translation: Challenges And Opportunities In Physician-to-Physician Communication During Patient Handoffs." Academic Medicine, vol. 80, no. 12, pp. 1094 – 1099, Dec. 2005.
Additional References
[2] A. J. Starmer, N. D. Spector, R. Srivastava, A. D. Allen, C. P. Landrigan, and T. C. Sectish, “I-pass, a mnemonic to standardize verbal handoffs.,” Pediatrics, vol. 129, no. 2, pp. 201–4, Feb. 2012.
[3] D. S. Cheung, J. J. Kelly, C. Beach, R. P. Berkeley, R. a Bitterman, R. I. Broida, W. C. Dalsey, H. L. Farley, D. C. Fuller, D. J. Garvey, K. M. Klauer, L. B. McCullough, E. S. Patterson, J. C. Pham, M. P. Phelan, J. M. Pines, S. M. Schenkel, A. Tomolo, T. W. Turbiak, J. a Vozenilek, R. L. Wears, and M. L. White, “Improving handoffs in the emergency department.,” Ann. Emerg. Med., vol. 55, no. 2, pp. 171–80, Feb. 2010.
[4] E. S. Patterson, and R. L. Wears. "Patient Handoffs: Standardized and Reliable Measurement Tools Remain Elusive." Joint Commission Journal on Quality and Patient Safety, vol. 36, no. 2, pp. 52-61, Feb. 2010.
[5] M. E. Flanagan, E. S. Patterson, R. M. Frankel, and B. N. Doebbeling. "Evaluation of a Physician Informatics Tool to Improve Patient Handoffs." Journal of the American Medical Informatics Association, vol. 16, no. 4, pp. 509-515, Jul – Aug. 2009.
[6] V. M. Arora, E. Manjarrez, D. D. Dressler, P. Basaviah, L. Halasyamani, and S. Kripalani, “Hospitalist handoffs: a systematic review and task force recommendations.,” J. Hosp. Med., vol. 4, no. 7, pp. 433–40, Sep. 2009.
16

Appendices
A. Preliminary Interview QuestionsB. Preliminary Survey QuestionsC. Preliminary Survey ResultsD. Tally Card SampleE. Pilot Interview QuestionsF. Pilot Survey QuestionsG. Pilot Survey Results
17

Appendix A: Preliminary Interview Questions1. What do you do to prepare for a handoff?2. What is the most important information you want to get from a handoff?3. What online/computer programs do you use during a handoff?4. What paperwork do you use for reference during a handoff?5. What makes some handoffs longer than others?6. How long does the day resident normally stay after the handoff? What do they do?7. Who updates the handoff material before the handoff occurs?
8. Do you have any suggestions for improvements to the current handoff process?9. What would you find most useful for standardizing handoffs?10. What are the perceived barriers?11. What problems have risen that could have been solved by a better handoff?12. What critical information has not been shared during handoffs?13. How long should a handoff take? (stable vs ill) (known patient vs unknown patient)
18

Appendix B: Preliminary Survey Questions
1. What is your current level of training (PGY year)?2. How long does it take to you to conduct a signout per patient?3. When you work the night shift, do you write the signout email throughout the shift or at the
end of the shift?a. Throughout the shiftb. At the end of the shift
4. What type of information do you want to receive during a signout? (select all that apply)a. Nameb. Condition/Stabilityc. HPId. Current Medicatione. Recent Labsf. Allergiesg. Pain Levelh. Mobilityi. Otherj. Current Diet/NPO Statusk. Past Medical Historyl. Recent (24-48 hr) Postop Eventsm. Operation & Postop Day
5. What other types of patient information do you want to receive in signout?6. Please rate how you agree or disagree with the following statements:
a. The current signout process works wellb. The signout should occur in a quiet settingc. The current signout process would benefit from a chart based toold. The current signout process would benefit from an iPad iOS application tool
7. On average how often do the following events occur as a result of signout event?a. Missing patient informationb. Miscommunication about patient informationc. Delay in patient cared. Adverse health event for patient
8. Do you have any suggestions for improvements to the signout process?9. What would you find most useful for standardizing the handoff process?
10.
19

Appendix C: Preliminary Survey Results
1. What is your current level of training (PGY year)# Answer Response %1 1 7 29%2 2 5 21%3 3 2 8%4 4 1 4%5 5 3 13%6 6 3 13%7 7 3 13%
Total 24 100%
Statistic ValueMin Value 1Max Value 7Mean 3.38Variance 5.11Standard Deviation 2.26Total Responses 24
2. How long does it take you to conduct a signout per patient?# Answer Response %
1 Under 1 minute 4 17%
2 1 minute 8 33%3 2 minutes 9 38%4 3 minutes 3 13%5 4 minutes 0 0%
6 5 or more minutes 0 0%
Total 24 100%
Statistic ValueMin Value 1Max Value 4Mean 2.46Variance 0.87Standard Deviation 0.93Total Responses 24
20
3. When you work the night shift, do you write the signout email throughout the shift or at the end of the shift?
# Answer Response %
1 Throughout the night 15 75%
2 End of Shift 5 25%Total 20 100%
Statistic ValueMin Value 1Max Value 2Mean 1.25Variance 0.20Standard Deviation 0.44Total Responses 20
4. What type of information do you want to receive during a signout? (select all that apply)
# Answer Response %1 Name 23 96%
2 Condition/Stability 23 96%
3 HPI 4 17%
4 Current Medications 4 17%
5 Recent Labs 5 21%6 Allergies 0 0%8 Pain Level 3 13%9 Mobility 0 0%
10 Other 5 21%
11 Current Diet/NPO status 19 79%
12 Past Medical History 12 50%
13 Recent (24-48 hr) postop events 22 92%
14 Operation & Postop day 21 88%
Statistic ValueMin Value 1Max Value 14Total Responses 24
21

5. What other types of patient information do you want to receive in a signout?Text ResponseAnticipated issues and management strategy, action items (to dos)What is actually going on.tasks for the night.Depends on if it is the first signout or if it is an established patient - less info needed for established patients. Would want to know anticipated issues and plan for subsequent care over the next 24 hours, code status and attending of record.
Statistic ValueTotal Responses 4
6. Please rate how you agree or disagree with the following statements:
# Question DisagreeNeither
Agree nor Disagree
Agree Total Responses Mean
1The current signout process works well.
8 6 10 24 2.08
2The signout should occur in a quiet setting.
0 5 19 24 2.79
3
The current signout process would benefit from a chart based tool.
3 10 11 24 2.33
4
The current signout process would benefit from an iPad iOS application tool.
5 11 8 24 2.13
StatisticThe current
signout process works well.
The signout should occur in a
quiet setting.
The current signout process would benefit
from a chart based tool.
The current signout process would benefit
from an iPad iOS application tool.
Min Value 1 2 1 1Max Value 3 3 3 3Mean 2.08 2.79 2.33 2.13Variance 0.78 0.17 0.49 0.55Standard Deviation 0.88 0.41 0.70 0.74
Total Responses 24 24 24 24
22

7. On average, how often do the following events occur as a result of signout events?
# Question Rarely Occasionally1-3
times per shift
4 or more times
per shift
Total Responses Mean
1 Missing patient information 0 15 9 0 24 2.38
2Miscommunication about patient information
2 15 7 0 24 2.21
3 Delay in patient care 3 17 4 0 24 2.04
4 Adverse health event for patient 17 7 0 0 24 1.29
Statistic Missing patient information
Miscommunication about patient
information
Delay in patient care
Adverse health event for patient
Min Value 2 1 1 1Max Value 3 3 3 2Mean 2.38 2.21 2.04 1.29Variance 0.24 0.35 0.30 0.22Standard Deviation 0.49 0.59 0.55 0.46
Total Responses 24 24 24 24
23

8. Do you have any suggestions for improvements to the current signout process?Text ResponseGo over the expectations, give an example, and practice in orientation. A lot of this is learned over experience.I think a lot of the residents are getting too laid back about sign out as the year has gone on which is frustrating. The PM sign out is more frustrating when residents have been in the OR all day and don't take the time to see patients they are concerned about before signing it out to the night intern.Reduce the number of sign outs from PA to day resident to night resident. I count two distinct times when I just went by the email sign out because the day resident had no idea what was going on. The other difficult thing is the list. I have come on as the night resident and not had the list updated on many of the people. I get to know the people because I'm working on updating the list throughout the night but if something acutely were to happen I would be on the computer sifting through information because i do not know the hpi, PMH, psh, meds ...etc.Interns need to learn their patients.Good and relevant signout requires some practice. Maybe more time/training could be dedicated to this during orientation to help smooth the transition into intern year.Attitude shift about signout is needed - signout is not a passive process where the outgoing team spoon-feeds everything to the cross-cover team, but there needs to be a certain degree of ownership by the cross-cover team to have a clue about the patients before coming on-board for the night/shift.Email works pretty well but nothing is a substitute for having the post call guy round with the team.Sign-out from Junior-to-Junior should be protected time from attendings and chiefs. Frequently, attendings and chief residents would like to round, complete clinic, etc with the juniors when it is the designated sign out time - this leads to a rushed sign-out or delayed sign-out when things can be missed or overlooked. It will not take long - designate 30 minutes from 6-630pm where noone can bother the juniors, so they can get a complete sign-out - including all pertinent information and "trivial" information that the attendings/chiefs do not care to hear about.
Statistic ValueTotal Responses 8
24

9. What would you find most useful for standardizing signout?Text ResponseI preset expectation that we are taught to follow.an app would be awesome--include diet, things to follow up--with whether or not the chief wants to know about it, how to contact the chief and then the app could create the sign out emailI think the PAs should have a standard sign out email format. It can be incredibly helpful or terrible day to day and reducing that variability would be great.customizable service-specific tools in the EMR that could be updated continuously, synced across devices, and printed out for different residents' prreferred stylesA tool that efficiently updates recent clinical events, labs, and the plan.If you make a tool, keep it simple and something that doesn't require people to update because that doesn't workA hand-off worksheet might be helpful for some, though I don't think it would be necessary.A patient info sheet with a check list will likely be most useful.I dont think it needs to be standardized, it just needs to be done well. Oftentimes a conversation is much more helpful than a long email. I would just encourage that the post call guy talk to the oncoming guy person to person if possible either via phone or in OR if face to face conversation is not possible.Name - presenting complaint - procedure - post-op day - course thus far - pertinent PMH - anything to do overnight? Frequently most of this is not discussed, but this is what I like to hear.
Statistic ValueTotal Responses 10
** Survey response removed for confidentiality purposes
25

Appendix D: Tally Card Sample
Figure 1. Tally Card Sample (Left: front, Right: back)
26

Appendix E: Pilot Interview Questions
1. How did the signout go? Are there specific things that were good or bad?2. Do you think this signout method is an improvement over the current method?3. Did you add any information to the signout? If so, what information?4. Are there any parts of the signout that you feel were unnecessary?5. Do you think this signout took a reasonable amount of time?6. Is the mnemonic easy to remember?7. In the long term, do you think this method will be useful to you personally?8. Will this signout method be sustainable for all residents?9. Do you have any other comments or questions?
27
Appendix F: Pilot Survey Questions
1. Please rate how you would agree with the following statements about the proposed signout process.
a. The proposed signout process is an improvement over the current signout processb. The proposed signout process takes a reasonable amount of timec. I would feel comfortable using the proposed signout method for future signouts
2. How often did the following events occur as a result of the proposed signout method?a. Missing patient informationb. Miscommunication about patient informationc. Delay in patient cared. Adverse health event for patient
3. Please rate how you would agree with the following statements about the InterSECT mnemonic device.
a. The mnemonic is easy to rememberb. The mnemonic contains all patient information that I want to receive during signoutc. The mnemonic contains unnecessary or redundant patient information
4. What are your thoughts regarding the proposed signout process?5. Do you have any suggestions for improvements to the proposed signout process?
28

Appendix G: Pilot Survey Results
1. Please rate how you would agree with the following statements about the proposed signout process.
# Question Strongly Agree Agree
Neither Agree
nor Disagree
Disagree Strongly Disagree
Total Response
sMean
1
The proposed signout process is an improvement over the current signout process.
0 0 0 1 0 1 4.00
2
The proposed signout process takes a reasonable amount of time.
0 1 0 0 0 1 2.00
3
I would feel comfortable using the proposed signout method for future signouts.
0 1 0 0 0 1 2.00
Statistic
The proposed signout process is an
improvement over the current signout process.
The proposed signout process takes a
reasonable amount of time.
I would feel comfortable using the
proposed signout method for future
signouts.Min Value 4 2 2Max Value 4 2 2Mean 4.00 2.00 2.00Variance 0.00 0.00 0.00Standard Deviation 0.00 0.00 0.00Total Responses 1 1 1
29

2. How often did the following events occur as a result of the proposed signout method?
# Question Rarely Occasionally 1-3 time per shift
4 or more times
per shift
Total Responses Mean
1 Missing patient information 0 1 0 0 1 2.00
2Miscommunication about patient information
1 0 0 0 1 1.00
3 Delay in patient care 1 0 0 0 1 1.00
4 Adverse health event for patient 1 0 0 0 1 1.00
Statistic Missing patient information
Miscommunication about patient
information
Delay in patient care
Adverse health event for patient
Min Value 2 1 1 1Max Value 2 1 1 1Mean 2.00 1.00 1.00 1.00Variance 0.00 0.00 0.00 0.00Standard Deviation 0.00 0.00 0.00 0.00
Total Responses 1 1 1 1
30

3. Please rate how you would agree with the following statements about the InterSECT mnemonic device.
# Question Strongly Agree Agree
Neither Agree
nor Disagree
Disagree Strongly Disagree
Total Responses Mean
1
The mnemonic is easy to remember.
0 0 0 1 0 1 4.00
2
The mnemonic contains all patient information that I want to receive during signout.
0 1 0 0 0 1 2.00
3
The mnemonic contains unnecessary or redundant patient information.
0 0 0 1 0 1 4.00
Statistic The mnemonic is easy to remember.
The mnemonic contains all patient information that I want to receive
during signout.
The mnemonic contains unnecessary or
redundant patient information.
Min Value 4 2 4Max Value 4 2 4Mean 4.00 2.00 4.00Variance 0.00 0.00 0.00Standard Deviation 0.00 0.00 0.00Total Responses 1 1 1
4. What are your thoughts regarding the proposed signout process?Text ResponseDuring the pilot I felt like we weren't doing things that differently from usual. Maybe I have too rosy a view of the status quo, or maybe the new process jet doesn't add much?
Statistic ValueTotal Responses 1
31

5. Do you have any suggestions for improvements to the proposed signout process?Text Response
Statistic ValueTotal Responses 0
** Survey response removed for confidentiality purposes
32





























