Embed Size (px)
Citation preview

University of Michigan Radiation Oncology Analysis of Treatment Process & Start Times
During Radiation Therapy Final Report
Prepared for:
Kathy Lash, Director of Operations, Radiation Oncology Scott Hadley, Physicist, Radiation Oncology
Sheri Curnes, Project Coordinator, Sr. Management Engineer
Prepared by: Student Lean Team
Nitin Gupta Emily Servinsky Kelly Wendling
Date of Submission: December 18, 2006

Table of Contents Executive Summary.......................................................................................................................3
Introduction....................................................................................................................................5
Background ....................................................................................................................................5
Key Issues .......................................................................................................................................6
Goals and Objectives .....................................................................................................................6
Project Scope ..................................................................................................................................6
Current Situation...........................................................................................................................7
Methodology ...................................................................................................................................8 Preliminary Observations.....................................................................................................8 Time Studies ........................................................................................................................8 Data Collection Logistics.........................................................................................8 Patient Representation .............................................................................................9 Surveys and Interviews ......................................................................................................11 Data Analysis .....................................................................................................................11
Findings.........................................................................................................................................11 Time Studies ......................................................................................................................11 Observations ..........................................................................................................12 Data Analysis .........................................................................................................12 Day One Treatment....................................................................................13 Day Two Treatment ...................................................................................14 Day Three Treatment .................................................................................16 Late Start Causes........................................................................................17 System Waste.............................................................................................18 Surveys and Interviews ......................................................................................................18
Conclusions...................................................................................................................................19
Alternatives Considered ..............................................................................................................19 Chart and Immobilization Equipment Storage ..................................................................19 Additional Machine ...........................................................................................................19 Additional Staffing.............................................................................................................20
Recommendations ........................................................................................................................20 Standardized Work.............................................................................................................20 Scheduling..........................................................................................................................21
Chart Completeness ...........................................................................................................22 Interruption Management...................................................................................................22 Scheduled Start Times .......................................................................................................22
Appendix A: Data Collection Sheets ............................................................................................24
Appendix B: Machine Representation Stratified By Day One, Two and Three Treatments........33
1

Table of Contents (Continued)
Appendix C: Weekday Representation Stratified By Day One, Two and Three Treatments ......34
Appendix D: Survey .....................................................................................................................35
Appendix E: Interview Questions.................................................................................................36
Appendix F: Day One Current State Value Stream Map .............................................................37
Appendix G: Day One First Time Quality Summary...................................................................38
Appendix H: Highlighted Waste on Day One Current State Value Stream Map.........................39
Appendix I: Day Two Current State Value Stream Map..............................................................40
Appendix J: Day Two First Time Quality Summary ...................................................................41
Appendix K: Highlighted Waste on Day Two Current State Value Stream Map........................42
Appendix L: Day Three Current State Value Stream Map ..........................................................43
Appendix M: Day Three First Time Quality Summary ...............................................................44
Appendix N: Highlighted Waste on Day Three Current State Value Stream Map ......................45
Appendix O: Summary of Survey Results ...................................................................................46
Appendix P: Standardized Work Template ..................................................................................47
2

Executive Summary The Lean Team has determined that one of the causes of long hours is variance among the time required to set up and administer a new patient’s first treatment. This process is known as the patient’s start time, and the variance in start times increase the treatment duration, which causes the department to fall behind schedule. As one treatment falls behind schedule, following treatments on a machine are continually pushed back. This snowball effect causes more treatments to run past their allotted times, which requires employees to stay long to finish treatments. The Radiation Oncology Department would like to determine why the department experiences longer working hours than in the past, and why start times tend to exceed or to fall below their allotted time of one hour. Additionally, the department has requested our assistance to determine why start times are necessary. The key issues driving this project are that patients often have a long wait before being taken back for treatment, treatments often go over their allotted time scheduled, and employees often work beyond their normal operating hours. To complete this request, the Student Lean Team observed treatments, carried out time studies on 20 in-scope patients, distributed surveys, and interviewed three radiation therapists. Our findings from each step led us to draw the following conclusions:
• There is no standard work for RTTs to follow during treatment • Removing scheduling from the control room would allow higher utilization of
treatment rooms • Scheduling would be less difficult if patients had consistent appointment times and
less appointment changes/cancellations • There is no standard on which to base length of appointment during scheduling • Incomplete charts/missing documentation sometimes not noticed until the scheduled
time of treatment • Chemo patients should not be schedule for morning starts/treatments • There is a lapse in communication between Chemotherapy and Radiation Oncology • There are many interruptions during the treatment process, however the frequency
and duration of these interruptions was not precisely recorded during data collection • Scheduled start times may not be optimal • It may be useful to have starts at different times on different machines
In order to eliminate and/or mitigate these problems, we recommend the following suggestions be implemented.
1. Standard Work - Develop standard work for when there are 1, 2, or 3 RTTs on a machine and train all RTTs on the new procedure
2. Scheduling - Create one station where all patients schedule their future appointments or change appointment times a. Enforce consistent appointment times and the definition of an emergency
appointment change more strictly b. Develop appointment length guidelines based on diagnosis and plan
3

c. Schedule all patients undergoing both chemotherapy and radiation for afternoon starts and treatments
d. Flag patients that are undergoing both chemotherapy and radiation treatment, make it a standard for Chemotherapy to notify Radiation Oncology if the patient does not show for their appointment
3. Chart Completeness - Develop check sheet to be used to verify chart completeness before and after day one treatment
4. Interruption Management - Carry out an interruption study to determine the frequency and duration of interruptions, and how identified interruptions can be eliminated/mitigated
5. Scheduled Start Times - Carry out further study/analysis to determine if there are better start times would be for each machine
4

Introduction Currently, the Radiation Oncology Department of the University of Michigan Hospital experiences long working hours. Treatments begin at 7 AM and often extend past 7 PM, with some treatments occurring up until 10PM at night. As a result, employees within the department work without knowing in advance exactly when their day will end. A lean team was organized to assess this problem; this team consists of employees with various roles in the Radiation Oncology Department. The Lean Team has determined that one of the causes of long hours is variance among the time required to set up and administer a new patient’s first treatment. This process is known as the patient’s start time, and the variance in start times increase the treatment duration, which causes the department to fall behind schedule. As one treatment falls behind schedule, following treatments on a machine are continually pushed back. This snowball effect causes more treatments to run past their allotted times, which requires employees to stay long to finish treatments. The Radiation Oncology Department would like to determine why the department experiences longer working hours than in the past, and why start times tend to exceed or to fall below their allotted time of one hour. Additionally, the department has requested our assistance to determine why start times are necessary. To identify a reason for start times, we collected data on 20 patients with the help of the Radiation Oncology’s Lean Team. We chose 20 patients because this number allowed data collection for the wide range of treatments carried out in the department. This collection spanned the first three days of a new patient’s radiation treatment to include a start time and following treatments where rework of a start time treatment might be required. Ideally, the third treatment simulates the rest of the patient’s treatments, thus the whole process is included to determine why treatments run late. The objective is to identify wasted work during the treatment process and to determine why the daily schedule of treatments often extends beyond the department’s normal operating hours. Based on the data we collected, we have recommended process modifications to reduce the time required to administer treatment to a patient, particularly during the treatment start time. Doing so will keep treatment duration to its allotted time, decrease the time a patient spends in the waiting room before treatment, and increase employee satisfaction. This report presents our methodology, findings, conclusions and recommendations. Background The Radiation Oncology Department at the University of Michigan Hospital is an extremely active unit open for treatment on Monday through Friday. Approximately 120 patients are treated per day with different types of treatment plans depending on the patient’s diagnosis. The department has four machines that deliver radiation therapy to patients. Patients may have their first treatment on any of the three EX machines at either 11AM or 2PM. Additionally, one machine performs first treatments at 12PM and 2PM. The department prefers to have the same patients on the same machine with the same therapists throughout treatment, but patients are
5

moved to similar machines if problems with a machine arise. These problems can be that a treatment takes longer than usual or that a machine is being repaired. In this case, the patient’s equipment is moved back to the scheduled machine room at the end of the treatment on a different machine. Therapists schedule one hour for the first treatment of a new patient due to patient set up, paperwork, questions, and general unfamiliarity with the treatment process. The therapists schedule all other treatments to run for an average of 20 minutes, although the exact schedule depends on the type of patient treatment. Extended work hours are required most of the time, and the work shifts fluctuate daily. Key Issues The following key issues created a need for this project.
• Patients often have a long stay in the waiting room before being taken back for treatment due to previous appointments that ran late.
• Treatments often go over the allotted time of one hour, which means that the machine and therapists cannot treat the next patient. This effect results in longer operating hours.
• Employees often work past the normal operating hours. Goals and Objectives The main goal of this project was to determine why the Radiation Oncology department has long treatment process times that contribute to long start times. The secondary objectives of this project were to:
• Reduce the patient wait time during treatment visits • Keep schedules to the treatment time allotted • Increase employee and patient satisfaction
Project Scope This project included an investigation of only the first to third treatments for radiation therapy patients. The treatment process begins half hour prior to the patient’s first treatment appointment and ends at the completion of the third treatment. Any process outside of these treatments was not considered. More specifically, this analysis did not include the planning process prior to the time of the first treatment or treatments beyond the third treatment. The intent was that the treatments beyond the first three treatments are similar to the second and third treatments so that the data collected after day three treatments is redundant. In addition, several procedures were considered out of the project scope due to their uncommon occurrences. However, after the project proposal was approved, simulation on set was considered within the project’s scope if the specific treatment followed a similar treatment flow as common treatments.
6

A summary of the out-of-scope procedures is: • Total Body Irradiation • Stereotactic Radiation Therapy • High-dose radiation • Charge Capture • PMI’s (preventative maintenance) • Boost fields
Current Situation We observed the current treatment process to determine the process that the radiation therapists follow and found the following. While administering day one radiation treatment, the process roughly follows these steps:
1. The patient arrives, checks in, changes into appropriate clothing for treatment, and waits in the waiting room.
2. Once the Radiation Treatment Therapists (RTT) finish their current treatment, they find the patient’s chart and review it, and locate required immobilization.
3. The patient is greeted by an RTT and taken into the treatment room. 4. The RTTs educate the patient about the treatment process and answer any patient
procedural questions. 5. The RTT helps the patient onto the treatment table, moves the patient precisely to the
correct position, and then exits the room. 6. From the control room, the RTTs film the orthogonal pairs and fields and makes moves if
necessary. 7. One RTT enters the treatment room and measures the SSDs, while the other RTT remains
in the control room and verifies these measurements. 8. The RTT in the treatment room prepares for treatment, then returns to the control room,
where the other RTT has prepared the control room for treatment. 9. From the control room, treatment is administered and the dose is recorded. 10. The RTTs document information for future treatment. 11. The RTTs enter the room, tattoo the patient, and take pictures of the patient . 12. One RTT removes the patient from the table and cleans the room. 13. One RTT fills out the forms and charts and schedules the patient for future treatments.
During treatment, the RTTs also are responsible for helping patients that call to change an appointment since scheduling can only be done in the patient’s scheduled control room. RTTs also answer waiting patient’s questions and respond to fellow RTTs’ needs. Additionally, RTTs do not have a scheduled time for lunches and breaks. Each RTT gets one thirty-minute lunch break and two fifteen-minute breaks they can take when they choose, although they first must ensure there are enough RTTs to cover treatment. Day two and three treatments follow a similar process, but are less complex since the patient has already had one treatment. Specifically, days two and three do not include filming treatment fields and iso-documentation (recording patient setup information).
7
Methodology The Student Lean Team examined all activities in the Radiation Oncology department. The primary parties that were involved in the process were the patients, the radiation therapy technologists, the physicians and therapists, the dosimetrists, and the Director of Operations of Radiation Oncology. To execute this project, we observed the treatment process, collected time study data, distributed surveys, interviewed radiation therapists, and developed recommendations. Preliminary Observations The Student Lean Team observed seven radiation treatments, focusing primarily on the duties the therapist performs during radiation treatment. The observations familiarized the team with the basic procedure to complete the treatment and allowed the team to determine logical tasks on which times should be recorded during the time studies. These tasks can be found in the data collection sheet in Appendix A. In the data collection sheets, the treatment process tasks were explicitly stated, and we defined the start and stop times for each step to keep consistency during the data collection. Time Studies The following section discusses the logistics of the data collection and the patient representation during the data collection. The data collection logistics includes when the data was collected, how the data was collected and who performed the data collection. The patient representation section includes a discussion of the representation with respect to patient diagnosis, treatment type, machine, and weekday. Data Collection Logistics The team then performed time studies for the treatment process, recording times on the tasks that were identified during the preliminary observations. The time study data collectors formed groups of two people from the Hospital Lean Team and the Student Lean Team. Since the treatment process usually involves two radiation therapists to treat a patient, each data collector ideally followed one radiation therapist. Sometimes, in treatment days two and three, only one person performed the time study because the process flow is easier to follow on those days. Specifically, data collectors recorded the start time and end time for each task during treatment. Additionally, collectors recorded whether rework was required for each task, any equipment faults that occurred, and any unusual occurrences. The data collection sheets and tasks used in the time studies can be seen in Appendix A. Data collection began October 9, 2006 and ended October 27, 2006. A total of 20 patients were studied that represented all in-scope treatments. Data collection began on the day one treatment and went through to the day three treatment. The frequency of a new patient followed on their first day of treatment is shown in Table 1 on the next page.
8

Table 1: Frequency of New Patient Followed During Day 1 Treatment Week of M Tu W Th F
8-Oct 2 2 2 2 1 15-Oct 2 2 2 2 1 22-Oct 2
Patient Representation Figure 1 shown below represents the diagnosis of patients tracked during the time studies. The diagnoses the most highly represented were Head & Neck with 28%, Pancreas with 18%, and Prostate with 12%. The remaining diagnoses each represented 6% of the data collection. This distribution is fairly representative of treatments observed, but with Head & Neck and Pancreas being slightly overrepresented. Additionally, prostate and breast cancer treatments are slightly underrepresented.
Abdomen 6%Pelvis 6% Anal 6% Whole Brain 6%
Breast 6% Femur 6%
Prostate 12%
Floor of Mouth 6% Pancreas 18%
Head & Neck 28%
Figure 1: Diagnosis Representation in Data Collection The following pie chart, Figure 2, shows the treatment type distribution. 70% of the treatments followed were 3D, 18% were IMRT, and 12% were AP/PA.
IMRT 18%
AP/PA 12% 3D 70%
Figure 2: Treatment Representation in Data Collection.
9

Figure 3, shown below, is a pie chart representing the machines used during the data collection. EX2 (41%) and EX1 (33%) were primarily used, while the 6/100 accounted for 15% and EX3 11%. This distribution is fairly representative. EX1 and EX2 account for most of the in-scope starts because EX3 and the 6/100 are often engaged for more intricate, out-of-scope treatments. Appendix B shows the machine representation stratified by first, second and third treatments.
6/100 15%
EX1 33% EX3 11%
EX2 41%
Figure 4 illustrates the distribution of the week day on which treatments were tracked and shows the highest representation occurred on Monday, Tuesday and Wednesday of 22%, 28% and 26%, respectively. Appendix C shows the weekday representation stratified by first, second and third treatments. Some physicians prefer for patients to receive treatment no more than a day after their first treatment. This preference means that first starts are less likely to occur on a Friday.
Figure 3: Machine Representation in Data Collection
Fri 9%
Thurs 15% Mon 22%
Tues 28% Wed 26%
Figure 4: Distribution of Weekday in Data Collection.
10

Surveys and Interviews The Student Lean Team distributed surveys to the radiation therapists and dosimetrists. The survey asked questions to determine what the employees believe causes the extended hours and what can be done to improve the process. Seventeen surveys were returned to the Lean Team and analyzed for the most significant reasons for delays in the process. The surveys were analyzed based on counting the frequency of each complaint. Furthermore, the numeric scale results provided for the causes of delays, a number from 3 to 5 was considered significant since it indicates a high delay. Otherwise, the number ranking was considered insignificant. All the results were compiled and the top five most common reasons for delays within the process were tabulated. The surveys provided a basis for alternatives and solutions to late start times in the project as well as assisted with developing interview questions for the radiation therapists. The copy of the survey can be seen in Appendix D. After the surveys were collected, three radiation therapists were interviewed. The interviews further helped clarify the main issues identified in the surveys, more specifically, the five most common reasons for delays in the process. Additionally, we asked questions to gauge radiation therapists’ perceptions of the potential solutions. The questions for the interview are shown in Appendix E. Data Analysis Based on the data collected, we used lean manufacturing techniques to formulate and recommend ways to improve the treatment process to optimize start times, reduce the patient wait times before treatment, and keep the observed treatment times to schedule. Recurring long process and wait times were identified and the team determined the tasks that can be performed in parallel, optimal techniques to schedule the treatments throughout the day, and determined if more machines and staffing are necessary. Findings This section discusses a detailed description of our findings for each step of our methodology. Specifically, we discuss observations, time study statistics, treatment process wastes, and late start causes. Time Studies We have separated the information derived from the time studies into two sections. The first section, Observations, summarizes comments made by the data collectors during the time studies. The second section, Data Analysis, is a statistical summary of the times observed during data collection.
11

Observations During the data collection, we observed the following causes of delay: Lack of Standardization
• Non-standard treatment process among control rooms • Non-standard treatment process among radiation therapists
Delay in Communication
• Patient did not arrive to chemotherapy in the morning and thus could not make the scheduled treatment time
• Multiple radiation therapists check the chart when a radiation therapist was replaced Underutilization and Variation of Appointment Times
• Scheduled appointment time changes • Patients have different scheduled appointment times for different days • Patients scheduled at 11AM when they had chemotherapy in the morning and thus
could not make the 11AM • Radiation therapists move between patient and computer screen to schedule • Patients arrive late • Patients sent to clinic upon arrival to treatment since radiation therapists realized that
the patient needed to go to the clinic first. Non-value Added Treatment Time
• Radiation therapists create rework by making multiple wasteful imager moves and couch moves when filming
Delays Due to Incomplete Charts and Treatment Planning
• Patient consent not signed in advance • Dosimetry still planning • Physician has not approved images • Incomplete chart (patient set up not recorded and physician on set not recorded on
day 1 for future use) Delays Due to Interruptions
• Phone calls • Radiation therapists from other control rooms looking for equipment • Radiation therapists from other control rooms looking for chart
Equipment Delays
• Machine down Data Analysis The following section details the data analysis for day one, day two, and day three treatments. Specifically, this section presents time study statistics, treatment process wastes, and late start causes.
12

Day One Treatment Table 2 shown on the next page is a summary of the observed day one statistics. Since the variation for each task time was large, we used the median values for the majority of the data analysis.
Table 2: Day One Statistics Summary
Statistic Process Time
Wait Time
Lead Time
Work Time
Fraction Value Add
Fraction Non-Value Add
First Time Quality
Median (x) 0:51 0:43 1:34 1:42 54% 46% Mean (µ) 1:09 0:51 2:00 2:18 58% 42%
2.4%
The median processing time for treatment was observed to be 51 minutes, while the overall wait time had a median of 43 minutes. Roughly 54% of the work observed was value added, while 46% was judged to be non-value added. The overall FTQ of day one treatment was calculated to be 2.4%. The updated day one current state map with the statistics for each step of the process is included in Appendix F. From this map, we observed that 11.5% of the treatment time is spent greeting the patient and checking the chart, 53% is spent setting up the patient and imaging, 11.5% is spent treating the patient, and 24% is spent on post treatment procedures. These percentages are shown in Table 3, along with median processing times for each category of treatment.
Table 3: Day 1 Treatment Time Distribution Category Median P/T (min) Percentage
Greet PT/Check Chart 6 11.5% Set Up PT/Imaging 27 53% Administer TX 6 11.5% Post TX 12 24%
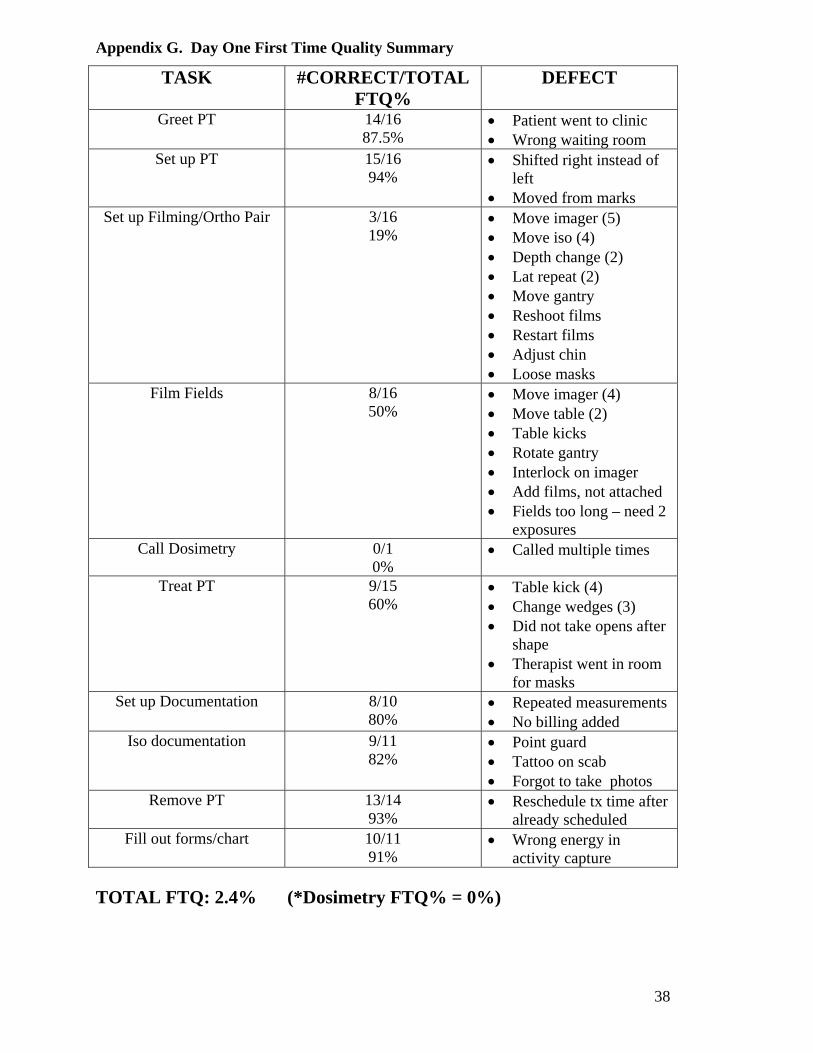
Additionally, we observed that there are long wait times before the patient is taken back for treatment (median 16 minutes), before the RTTs set up the treatment room (median 30 minutes), and between calling a physician or Dosimetry and their arrival (median 26 minutes). Tasks with long processing times include setup filming and ortho pairs (median 7 minutes), filming the treatment fields (median 10 minutes), preparing for treatment in the treatment and control rooms (median 1 minute), and filling out charts and forms (median 3 minutes). Several tasks in the day one treatment process have excessive rework due to low first time quality metrics. These tasks in include setup, filming, and orthogonal pairs (FTQ 19%), filming the treatment fields (FTQ 50%), calling a physician or Dosimetry (FTQ 0%), and treating the patient (FTQ 60%),. A summary of all the first time quality metrics and the reason for rework can be seen in Appendix G. The first time quality metrics and rework are detailed on a waste current state map, which also includes system wastes that are pointed out on the diagram. A marked up version of the day one current state map that highlights waste observations can be found in Appendix H. A discussion of the system wastes occurs in the following System Waste section.
13

Finally, there were several occasions where treatment was delayed due to either the patient arriving late or not arriving at all. As Figure 5 illustrates, 15% of the patients studied were late for their day one treatment, while 10% of patients did not inform the department of their cancellation.
Late 15% Cancellation with no call 15%
On time 75%
Figure 5: Day 1 Patient Lateness Day Two Treatment Table 4 shown below is a summary of the observed day one statistics. The median processing time for treatment was observed to be 15 minutes, while the overall wait time had a median of 4 minutes. Roughly 79% of the work observed was value added, while 21% was judged to be non-value added. The overall FTQ of day one treatment was calculated to be 39%.
Table 4: Day Two Statistics Summary
Statistic Process
Time Wait Time
Lead Time
Work Time
Fraction Value Add
Fraction Non-Value Add
First Time Quality
Median(x) 0:15 0:04 0:19 0:28 79% 21% Mean (µ) 0:19 0:07 0:26 0:36 73% 27%
39%
The updated day two current state map with the statistics for each step of the process is included in Appendix I. From this map, we observed that 13% of the treatment time is spent greeting the patient and checking the chart, 40% is spent setting up the patient, 40% is spent treating the patient, and 7% is spent on post treatment procedures. These percentages are shown in Table 5, along with median processing times for each category of treatment.
Table 5: Day 2 Treatment Time Distribution Category Median P/T (min) Percentage
Greet PT/Check Chart 2 13% Set Up PT/Imaging 6 40% Administer TX 6 40% Post TX 1 7%
On day two, we observed that there are again waits before the patient is taken back for treatment (median 2 minutes) and before the RTTs begin setting up the treatment room (median 2
14
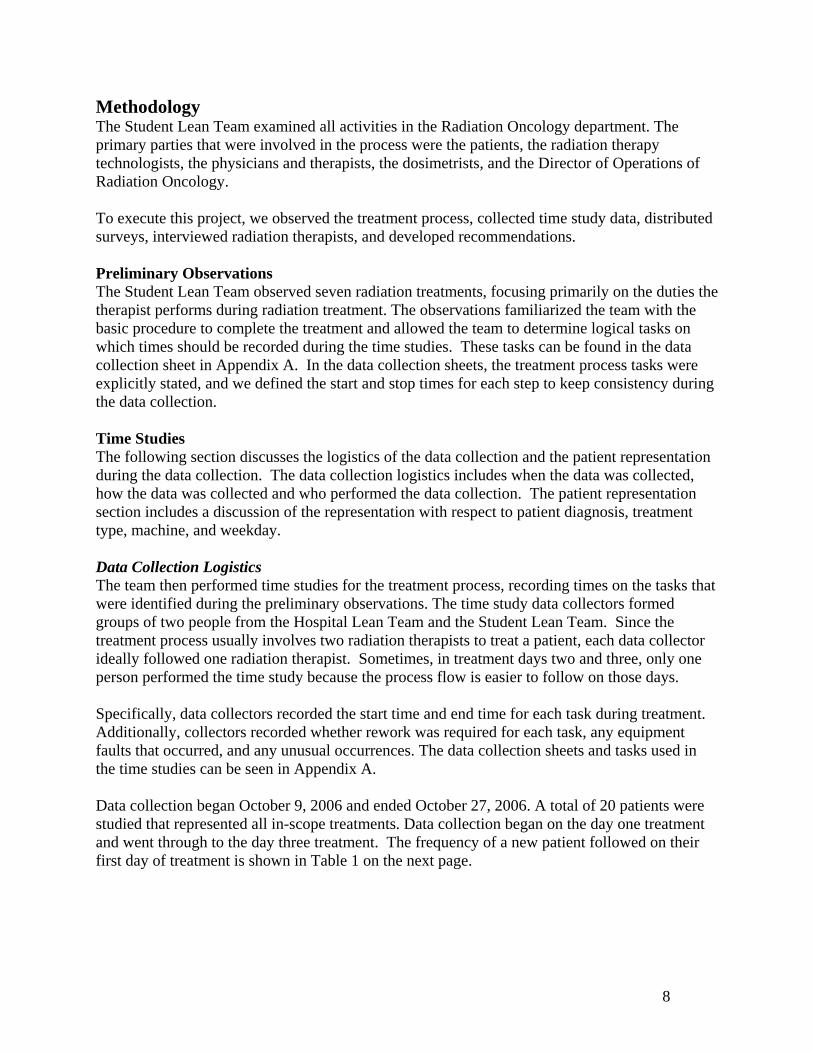
minutes). While these waits are significantly less than was observed during day one treatment, it would be optimal to eliminate the waits entirely. Also consistent with day one, rework is observed during setting up the treatment room (FTQ 92%), setting up the patient (FTQ 80%), setup filming and ortho pairs (FTQ 60%), and removing the patient and cleaning the treatment room (FTQ 94%). A summary of the first time quality metrics and the reason for rework can be seen in Appendix J. We observed that the tasks setup filming and ortho pairs and removing the patient and cleaning the treatment room have relatively long processing times. Median times of 4 minutes and 1 minute were observed, respectively. The first time quality metrics and rework are detailed on a waste current state map, which also includes system wastes that are pointed out on the diagram. A marked up version of the day two current state map that highlights waste observations can be found in Appendix K. A discussion of the system wastes occurs in the following System Waste section. On day two treatments, significantly fewer patients were late for their appointment. As Figure 6 shows,7.7% of the patients studied were late for their day two treatment, while no patients observed failed to show up for treatment.
Late 7.7%
On time 92.3%
Figure 6: Day 2 Patient Lateness
15

Day Three Treatment Table 6 shown below is a summary of the observed day one statistics. The median processing time for treatment was observed to be 17 minutes, while the overall wait time had a median of 1 minute. Roughly 94% of the work observed was value added, while 6% was judged to be non-value added. The overall FTQ of day one treatment was calculated to be 34%.
Table 6: Day Three Statistics Summary
Statistic Process
Time Wait Time
Lead Time
Work Time
Fraction Value Add
Fraction Non-Value Add
First Time Quality
Median(x) 0:17 0:01 0:18 0:34 94% 6% Mean (µ) 0:17 0:00 0:17 0:34 100% 0%
34%
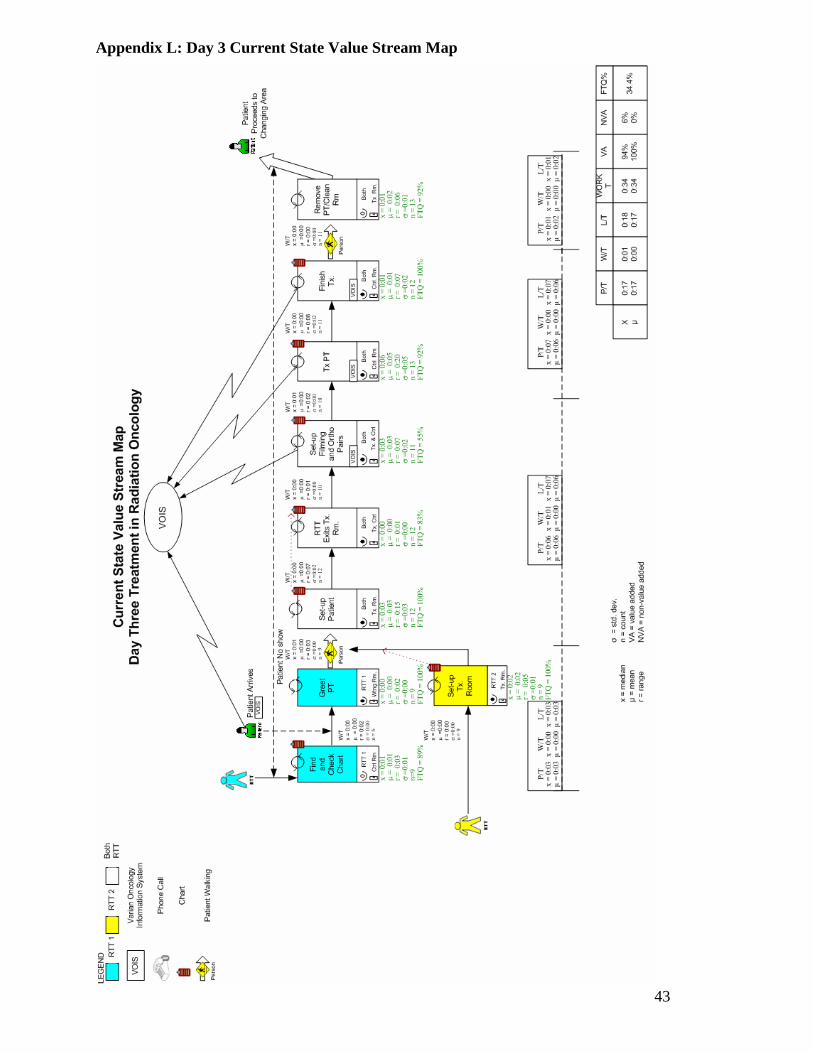
The updated day three current state map with the statistics for each step of the process is included in Appendix L. From this map, we observed that 18% of the treatment time is spent greeting the patient and checking the chart, 35% is spent setting up the patient, 41% is spent treating the patient, and 6% is spent on post treatment procedures. These percentages are shown in Table 7, along with median processing times for each category of treatment.
Table 7: Day 3 Treatment Time Distribution Category Median P/T (min) Percentage
Greet PT/Check Chart 3 18% Set Up PT/Imaging 6 35% Administer TX 7 41% Post TX 1 6%
Consistent with day one and two treatments, the patient often waits before being taken back for treatment, but the wait tends to be much less significant. Also consistent with days one and two treatments, rework is observed during the tasks of finding and checking the chart, setup filming and ortho pairs, and removing the patient and cleaning the treatment room. The FTQ values for these three tasks were observed to be 89%, 55%, and 92%, respectively. A summary of the first time quality metrics and the reason for rework can be seen in Appendix M. The first time quality metrics and rework are detailed on a waste current state map, which also includes system wastes that are pointed out on the diagram. A marked up version of the day three current state map that highlights waste observations can be found in Appendix N. A discussion of the system wastes occurs in the following System Waste section.
16

On their third day of treatment, all patients showed up on time for their treatment. Figure 7 below illustrates that patient lateness or absence did not cause delays on the third day of treatment.
On time 100%
Figure 7: Day 3 Patient Lateness Late Start Causes From the observations and data collection we brainstormed reasons and calculated the actual reasons for late starts on the first day of treatment. Seventy percent of first day treatments were late and the cause and effect diagram listed in Figure 8 below shows the distributed percentages for the treatments that started late in.
Figure 8: Cause and Effect Diagram of Delayed Start of a Patient’s First Treatment
17

System Waste The first time quality metrics and rework are detailed in the waste current state maps, which also include system wastes that are pointed out on the respective diagrams found in Appendix H, Appendix K, and Appendix N. We detailed excessive wait times on the map, which mostly occurred before the room was setup for the patient. Additionally, we noted the following wastes:
• Correction o Fixing an incomplete chart
• Overproduction o Setting up a treatment room when patient never arrives
• Motion o Searching for a missing chart or a chart outside of the specified control room o Walking to retrieve equipment from a different treatment room o Walking to the treatment room to make unnecessary movements
• Material Movement o Retrieving equipment from a different treatment room
• Waiting o Waiting in the waiting room for a delayed treatment (patient) o Waiting for the physician
• Processing o Making unnecessary movements in the treatment room o Scheduling a patient for their future appointments
• Mura (unevenness or lack of consistency) o Arrival of patient o Arrival of treatment plan
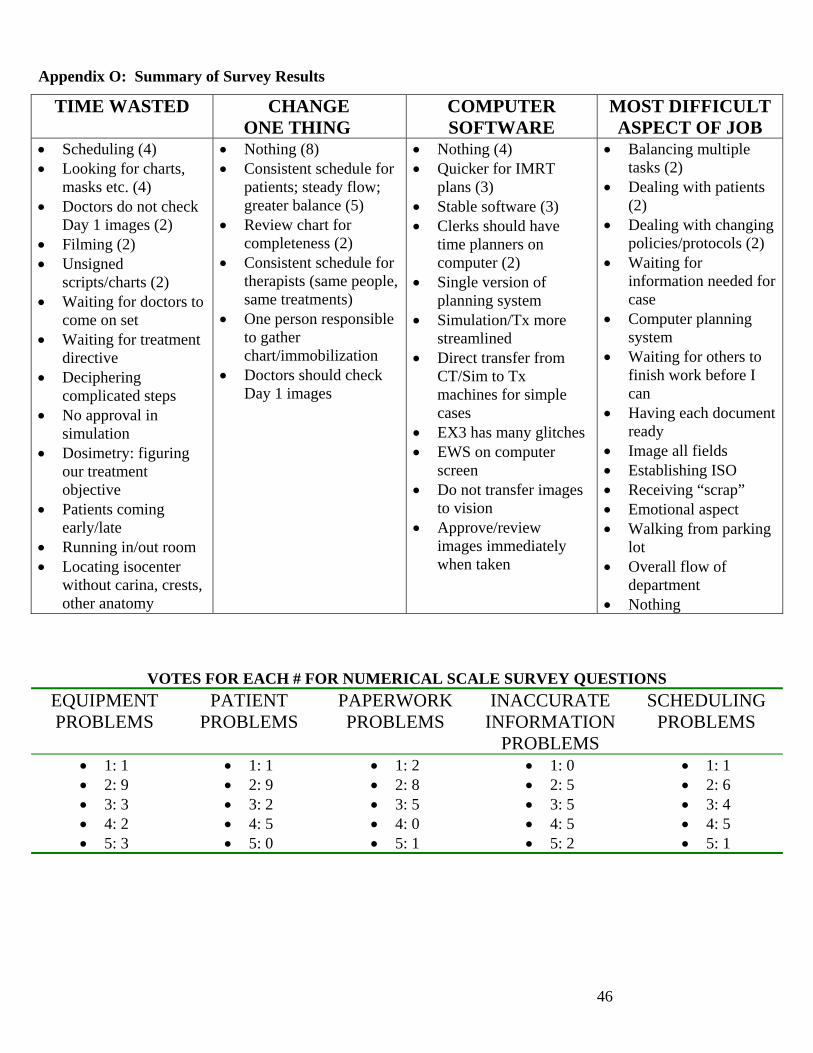
Surveys and Interviews Based on the surveys of the radiation therapists and dosimetrists, the top five most common reasons for delays in descending order are:
1. Patient scheduling (in regards to their flow during the day and order) 2. Inaccurate or missing information (wrong details in chart, consents not signed by doctors) 3. Equipment or paper search (looking for the charts and masks, etc.) 4. Unchecked day one images 5. Rotation of therapists (disruption of working with different radiation therapists)
Other findings from the surveys and interviews included:
1. Therapists schedule the amount of treatment differently and schedule a shorter time period for the treatment if that is what’s available.
2. Therapists generally liked the idea of standardized work and thought it would help the process.
3. Often too many therapists at one time in a control room. A summary the survey results can be seen in Appendix O.
18

Conclusions Based on our findings, we drew the following conclusions:
• There is no standard work for RTTs to follow during treatment • All patient scheduling should be moved out of the control room • Scheduling would be less difficult if patients had consistent appointment times and
less appointment changes/cancellations • Appointment lengths should be adjusted depending on diagnosis and plan • FTQ of completing charts should be improved • Chemo patients should not be schedule for morning starts/treatments • There is a lapse in communication between Chemotherapy and Radiation Oncology • There are many interruptions during the treatment process, however the frequency
and duration of these interruptions was not precisely recorded during data collection • Scheduled start times may not be optimal • It may be useful to have starts at different times on different machines
Alternatives Considered After analyzing the data from the time studies, surveys, and interviews, the Lean Team discussed several alternatives as solutions to lengthy start times and falling behind schedule within the department that ultimately were not recommended. These alternatives are listed below:
• Create a central location where all charts and immobilization are stored • Introduce additional machine • Hire additional radiation therapists
Chart and Immobilization Equipment Storage Since a majority of the interruptions observed during the treatment process were due to RTTs from other control rooms looking for charts and immobilization equipment, we discussed storing all charts and immobilization equipment in one central location. We felt that this change in storage would reduce the number of interruptions occurring throughout the treatment process. However, upon further consideration we decided that individually getting each patient’s chart and immobilization from the storage room would actually take more time than the delay caused by the interruptions themselves. Therefore, we chose not to recommend that the storage system be changed. Additional Machine Since the Radiation Oncology department consistently treats patients beyond normal operating hours, the intuitive conclusion is that patient volume is above the department’s capacity. For this reason, we initially considered recommending that an additional machine be installed. However, after observation and analysis, we determined that there is great potential to streamline the treatment process and move more patients through treatment each day. Also, the department is currently installing a fifth machine to administer treatment. For these two reasons, we decided not to recommend a sixth machine, and rather concentrate on improving the treatment process itself.
19

Additional Staffing Another intuitive response when volume is greater than the current capacity is to hire additional staffing. However, after observation we quickly realized that the number of RTTs administering treatment was not the constraint preventing faster treatment. When three RTTs were treating on a single machine rather than two, there was not a significant reduction in the treatment time observed. Therefore we decided that additional RTTs would not be beneficial, rather we should concentrate on how to streamline the current treatment process. Recommendations Based on our findings and conclusions, we have the following recommendations to optimize the radiation therapy treatment process:
1. Standard Work - Develop standard work for when there are 1, 2, or 3 RTTs on a machine and train all RTTs on the new procedure a. Therapist responsibilities detailed by team color assignment b. Proactive lunch scheduling
2. Scheduling - Create one station where all patients schedule their future appointments or change appointment times a. Enforce consistent appointment times and the definition of an emergency
appointment change more strictly b. Develop appointment length guidelines based on diagnosis and plan c. Schedule all patients undergoing both chemotherapy and radiation for afternoon
starts and treatments d. Flag patients that are undergoing both chemotherapy and radiation treatment,
make it a standard for Chemotherapy to notify Radiation Oncology if the patient does not show for their appointment
3. Chart Completeness - Develop check sheet to be used to verify chart completeness before and after day one treatment
4. Interruption Management - Carry out an interruption study to determine the frequency and duration of interruptions, and how identified interruptions can be eliminated/mitigated
5. Scheduled Start Times - Carry out further study/analysis to determine if there are better start times would be for each machine
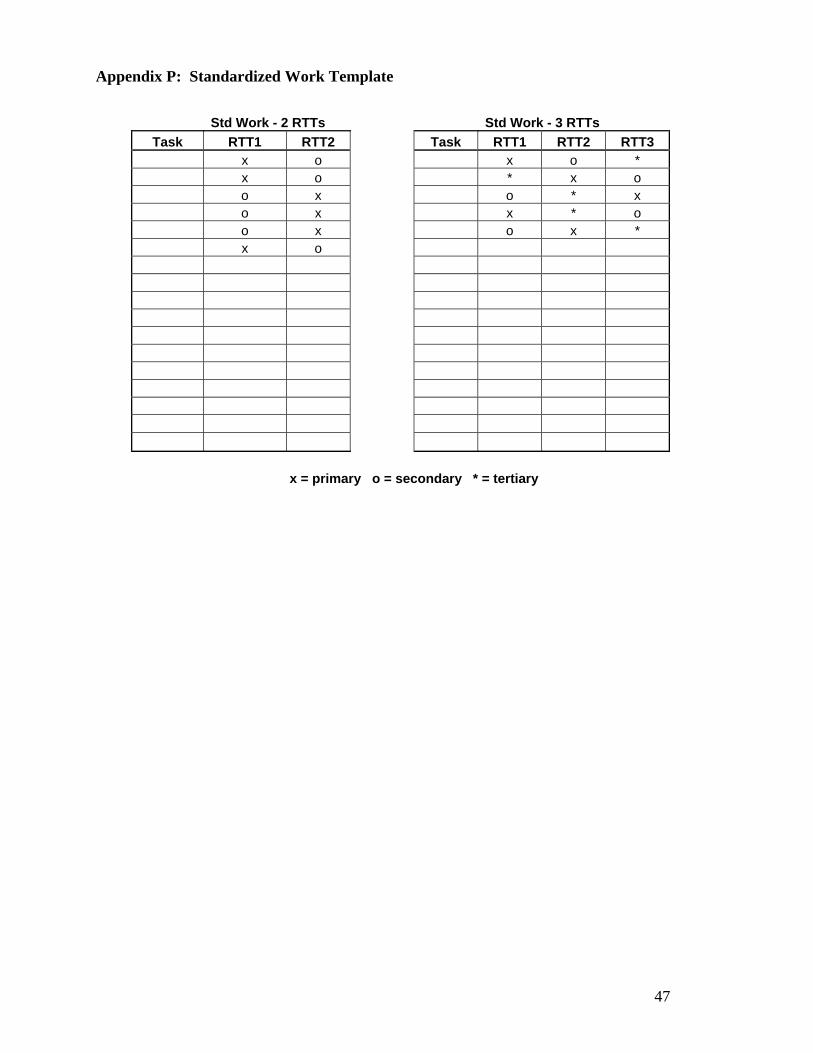
These recommendations are each discussed below in more detail. Standard Work The data indicates that the variation in task times ranges from 1 to 7 minutes. This variation makes it difficult to predict how long a treatment will require. The large variation also indicates that there is inconsistency in the procedure followed by RTTs during treatment. Therefore, we recommend minimizing the overall variation by developing standard work for RTTs to follow during treatment. RTTs would be assigned to a specific team each day, and wear a specific color shirt to identify which team they are on that particular day. For example, if there are two RTTs on a machine,
20

one would be on the maize team and the second on the blue team. Each color team should have a specific list of their primary and secondary responsibilities during the treatment process when there are one, two, or three RTTs administering treatment. Having standard work will ensure that each treatment follows the same procedure and that a specific person will be accountable for completing each step accurately. A template of a standard work representation can be found in Appendix P. Once the standard work is developed, we recommend training all RTTs extensively on the new process to administer treatment. These standards should also include when each RTT should take their lunch and breaks, depending on when their shift began. Employees would sign up for when they will take their lunch in advance. This proactive lunch scheduling will eliminate the need to check with other RTTs before taking lunch or break, and guarantee that there would always be enough RTTs staffing each machine. Standard work during treatment will also aid in the process of continuous improvement. Once all RTTs administer treatment identically, it will be much easier to identify areas of waste in the procedure, develop potential improvements, and determine whether trial improvements are effective. Scheduling To eliminate the time dedicated to scheduling in the control room, we recommend that one station be created to schedule future appointments for all patients, to handle all appointment time changes, and to handle all telephone calls that currently go to the control rooms. Patients would visit the scheduler in a central location after receiving their first treatment. Removing scheduling from the control room would allow higher utilization of the treatment rooms, since a greater percentage of the day would be dedicated to treatment. In other words, since scheduling requires at least 3 minutes per patient and an average of 120 treatments are administered in the department daily, removing this duty would eliminate 360 minutes, or 6 hours, of work time from the control rooms. The data collection also indicated that the time required for treatment varies significantly by diagnosis and treatment plan. We recommend that standard guidelines for treatment duration be developed for based on diagnosis and plan, and that these guidelines be used during scheduling. Doing so will allow the treatment schedule to more accurately represent the observed treatment times and reduce the time a patient spends in the waiting room before being taken back for treatment. We recommend imposing new standards for patients undergoing both chemotherapy and radiation therapy. Currently, these patients can have starts or appointments scheduled in the morning, however if they also have chemotherapy the same day, they are unable to make their radiation therapy appointments. For this reason, we recommend that patients receiving both chemotherapy and radiation therapy be scheduled for radiation only in the afternoon. Additionally, we observed a situation where one such patient did not arrive for their chemotherapy appointment in the morning and the Radiation Oncology department was not
21

notified. Radiation Oncology did not know the patient would not be receiving treatment until their scheduled appointment time; had they known earlier they could have moved appointment times ahead and completed the day’s treatments early. For this reason, we recommend that it becomes standard for Chemotherapy to notify Radiation Oncology if a mutual patient does not arrive for treatment. From the analysis on late treatment starts, we also found that 14.3% of the patients studied had to be seen in the clinic before their first treatment could begin. This clinic time cut into the patients’ appointment times, which caused both patients to go over their scheduled appointment times and delay the treatments of the following patients. Additionally, this clinic time required the radiation therapists and the machine to wait for the patient’s return to the treatment room. We recommend that patients should be seen in the clinic before their scheduled appointment time. Chart Completeness While it is not often that we observed incomplete charts, when it did occur it often led to a lengthy delay. We recommend the development of a check sheet as a relatively simple way to eliminate these delays. The check sheet would include a list of everything that must be completed prior to the first treatment. It could be used either while filling completing the chart, or during a quick chart completeness verification prior to a scheduled start. The same check sheet would be used after treatment is completed to verify all relevant information regarding setup is documented in the chart before the patient leaves the treatment room. After this step, the check sheet may be discarded. Interruption Management During the time studies, data collectors observed many interruptions during the treatment process. These interruptions consisted primarily of patients with scheduling questions, telephone calls, and fellow RTTs searching for charts and immobilization equipment. Not only do these interruptions cause delays, they also take the treating RTTs’ attention away from their primary objective, treating their patient. However, we determined that the data collection did not precisely capture the frequency or duration of these interruptions. For this reason, we recommend carrying out an additional study to determine interruption frequency and duration, as well as to identify ways in which interruptions may be eliminated or mitigated. Scheduled Start Times The time study results indicate that starts have the most variation and complexity. For this reason, it is difficult to determine how long starts will require, leading to appointments that often run over their allotted time. When this happens, subsequent appointments also fall behind schedule. Currently, starts are scheduled for 11AM and 2PM on three machines, and 12PM and 2PM on the fourth machine. Since starts have the most potential to run long, the question is raised whether these are optimal times for starts. Should a morning start run long, almost an entire day’s worth of appointments would be behind schedule. If starts were later in the afternoon, less subsequent appointments would be affected should they run long.
22

23
Additionally, all starts essentially occur at the same time on all machines. If the starts were staggered throughout the day, machines might be able to help one another get back on schedule should a start run long. We recommend that the Lean Team further investigate the optimal times for starts. Optimizing the scheduled times for starts would help to keep treatments to schedule.

24
Appendix A: Data Collection Sheets Data Collection for Treatment Days 1 - 3 Patient: PLACE STICKER HERE Patient Diagnosis: ____________________________ Type of Treatment: IMRT 3D Electron ABC Other: ____________ Immobilization: Alpha Cradle Belly Board Breast Board
H&N Board Knee cushions Masks Thorax Board None Other: _______________
Scheduled Appointment Date and Time: Treatment One: _______________________________ FILMS ONLY? Yes No
If yes, why only films?____________ Treatment Two: _______________________________ Treatment Three: _______________________________ Treatment Four: (Fill out only if treatment one was just filmed): ________________________ Please make sure that you:
- find someone to cover the patient’s 2nd and 3rd treatments - fill this coverage out on the massive schedule located by the data collection packets
Treatment One: Follower: _______________________________ Planned Machine: EX1 EX2 EX3 600 Actual Machine Used: EX1 EX2 EX3 600 Radiation Therapist(s) Followed: Greeter Non-greeter Extra therapist Treatment Two: Follower: _______________________________ Actual Appointment Date and Time: ___________________ Planned Machine: EX1 EX2 EX3 600 Actual Machine Used: EX1 EX2 EX3 600 Radiation Therapist(s) Followed: Greeter Non- greeter Extra therapist Treatment Three: Follower: _______________________________ Actual Appointment Date and Time: ___________________ Planned Machine: EX1 EX2 EX3 600 Actual Machine Used: EX1 EX2 EX3 600 Radiation Therapist Followed(s): Greeter Non- greeter Extra therapist
25
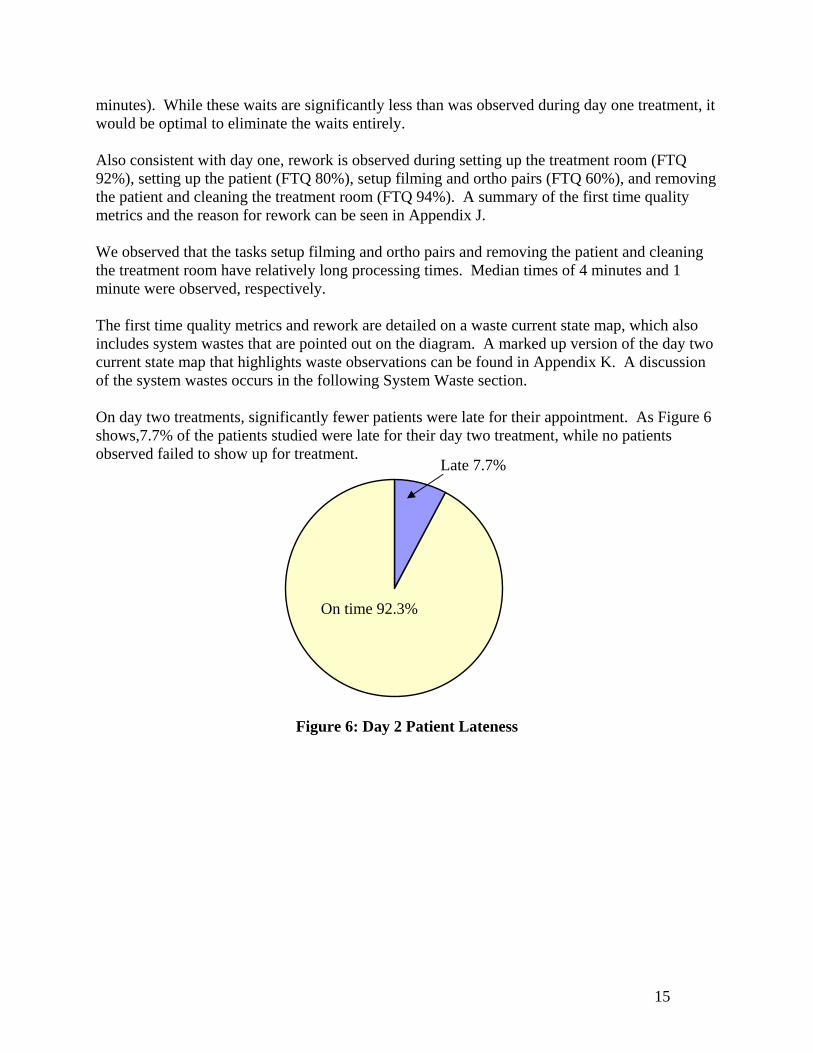
Instructions for Cover page:
• Patient: Patient identifier sticker will be placed here • Patient diagnosis: Example: Prostate • Type of Treatment: Example: IMRT • Immobilization: The checked boxes should be the devices used to immobilize that patient. • Scheduled Appointment Day & Time:
o 1st Treatment: The date and time of patient’s first appointment o 2nd & 3rd Treatments: These should be the appointments made on the 1st day of treatment for
treatments 2&3.
• Follower: The name of the recorder (you) following the specific therapist. • Planned Machine: Appointment the machine was originally made on. • Actual Machine Used: Machine used for that treatment day. • Actual Appointment Time: This is used for if the patient rescheduled his/her appointments. • Radiation Therapist Followed:
o This is based on who greets the therapist first. The other follower should be collecting data on the other radiation therapist.
o If more than two therapists are with a patient then each data collector should record times for tasks conducted by the designated person followed times for tasks conducted by the extra therapist
Instructions for Day One Treatment Part I of II:
Task Starts when RTT… Ends when RTT… 1. Find Chart Begins to search for the chart. Finds the chart. 2. Patient Arrives No need to fill this out
We will use Vision for this start.
There won’t be an end time to calculate from.
3. Chart Review Opens chart to check its readiness. Finishes making any changes to the chart.
3a. Set up Room Starts to set up equipment in room. Finishes setting up equipment in room.
4. Greet PT Brings the patient from the waiting room.
Finishes asking questions to identify patient and about chemo.
5. PT Education Starts to explain the initial process. Finishes explaining the initial process. 6. Set up PT Begins to put patient on table. Finishes adjusting the patient. 7. RTT Exits Rm Starts to leave the room. Sits in the control room. 8. Filming/Ortho Starts to acquire couch position. Ends filming. 9. Film fields Starts to film treatment fields. Finishes filming treatment fields.

DAY ONE TREATMENT Part I of II Task Start End Rework Required? Comments
1.Find Chart (Look at TX Unit)
Yes Reason:
2.Patient Arrives (Check in, Changes, WR)
Yes Reason:
3.Chart Review (Check in, Changes, WR)
Yes Reason:
3a.Set up Room (IMM, Extras, 4DTC, Verify)
Yes Reason:
4. Greet PT (Name, Photo, DOB, Chemo)
Yes Reason:
5. PT Education (Explain Rm/Proc, Instruc/Lim)
Yes Reason:
6. Set up PT (Lift, On table, Level, Marks with Lasers, SSD, Verify DRR, Imager Out dot in, Look at light field, more educ.)
Yes Reason:
7. RTT Exits Rm (Take chart, family out, LMO, Pull key, Close door)
Yes Reason:
8. Filming/Ortho (Acquire couch pos., Add image temp., Mode up, Take image, Determine error, Repeat (if nec.), Move couch)
Yes Reason:
9. Film fields (Mode up, take images, verify shape, repeat)
Yes Reason:
FAULTS Step Number Fault Identification Reason
26

27
Instructions for Day One Part II of II:
Task Starts when RTT… Ends when RTT… 10. Check SSDs Leaves control room to check
SSDs. Finishes checking SSDs
10a. Call dosim Places call to dosim. Finishes conversation with dosim. 10b. Call Dr. if nec. Places call to physician. Finishes conversation with doctor. 11. Mark PT Starts to mark with marker. Stops marking patient. 12. Prepare TX Starts to retract imager, etc. Leaves room to return to control room.12a. Prepare TX in Control Room
Prepares treatment by examining treatment fields, and reviewing dosage.
Finishes treatment preparation.
13. Tx Pt Starts the beam. Finishes giving radiation treatment. 14. Finish Tx Starts to record the dose given. Finishes billing (“charge capture”) 15. Set up docum. Starts to record information for
future treatments. Finishes with documentation of the patient.
16. Iso Documentation Starts to remask, give tattoos, take and print pictures, etc.
Finishes recording all patient set up.
17. Remove PT Starts to help patient off of the table.
Finishes cleaning the room.
18. Fill out forms/chart Starts to fill out forms, fills out the chart and schedules the patient.
Finishes all forms, the chart and scheduling tasks.

DAY ONE TREATMENT Part II of II Task Start End Rework Required? Comments
28
10. Check SSDs (During image or after, Record)
Yes Reason:
Yes 10a. Call dosim (If SSD>1cm, Discuss, Note in chart) Reason:
10b. Call Dr. if nec
Yes Reason:
11. Mark PT (Iso with sharpee, More educ.)
Yes Reason:
12. Prepare TX Yes (Retract imager, Remove Dot, Insert needed acc., Move mach and set up for field, check light field, more educ.)
Reason:
12a. Prepare TX in Control Room (Mode up TX field, Recheck script, Review TxD MU, Tun key/beam on)
Yes
Reason:
13. Tx Pt Yes (Beam on, Monitor pt, Turn Key Off, Log Tx in Chart, AGT or in room for next beam, Repeat)
Reason:
14. Finish Tx (Record Dose, Charge Capture)
Yes Reason:
15. Set up docum. Yes (Record MTH, Record DTH, Record Tatoo, Record Iso loc., Record board reg, add set up notes)
Reason:
16.Iso Documentation Yes (Remask/cradle, Give tattoos, Take set up notes, Take pic, Print photos)
Reason:
17. Remove PT Yes (Lift help, Gather personal stuff, Future tx time, Check chemo appt., Clean Room)
Reason:
18.Fill out forms/chart Yes Reason: (Auto Go To Sheet, Move Sheet,
Patient educ. Note, Place in color chart and ach. Sticker, Label with name/MD Day, Name alert, Check for chart tracker tag)
FAULTS Step Number Fault Identification Reason

29
Instructions for Day Two: Task Starts when RTT… Ends when RTT… 1. Find and Check Chart
Begins to search for the chart. Finishes reviewing chart.
2. Patient Arrives No need to fill this out
We will use Vision for this start.
There won’t be an end time to calculate from.
3. Greet PT Brings the patient from the waiting room.
Finishes asking questions to identify patient and about chemo.
3a. Set up room Starts to set up equipment in room. Finishes setting up equipment in room.
4. Set up PT Begins to put patient on table. Finishes adjusting the patient. 5. RTT Exits Rm Starts to leave the room. Sits in the control room. 6. Film/Ortho pair Starts to film. Ends filming. 7. Tx Pt Starts the beam. Finishes giving radiation treatment. 8.Finish Tx Starts to record the dose given. Finishes billing (“charge capture”) 9. Remove PT/Clean Rm
Starts to help patient off of the table.
Finishes cleaning the room.

DAY TWO TREATMENT Task Start End Rework Required? Comments
30
1.Find and check chart (Look at TX Unit)
Yes Reason:
2. PT Arrives (Checks in, Changes, Go to WR)
Yes Reason:
3.Greet PT Yes (Check set up pg, Consent, Check signed plan/RX, Check Move Sheet/DRRs, Check protocol, Check Chemo, MD Approval)
Reason:
3a. Set up room (Get IMM, Extras, 4DTC plan, Verify pt)
Yes Reason:
4. Set up PT
Yes Reason:
5. RTT Exits Rm
Yes Reason:
6. Film/Ortho pair
Yes Reason:
7. Tx Pt Yes (Beam on, Monitor pt, Turn key off, Log TX in chart, AGT or in room, Repeat)
Reason:
8.Finish Tx
Yes Reason:
9. Remove PT/Clean Rm
Yes Reason:
FAULTS Step Number Fault Identification Reason
31
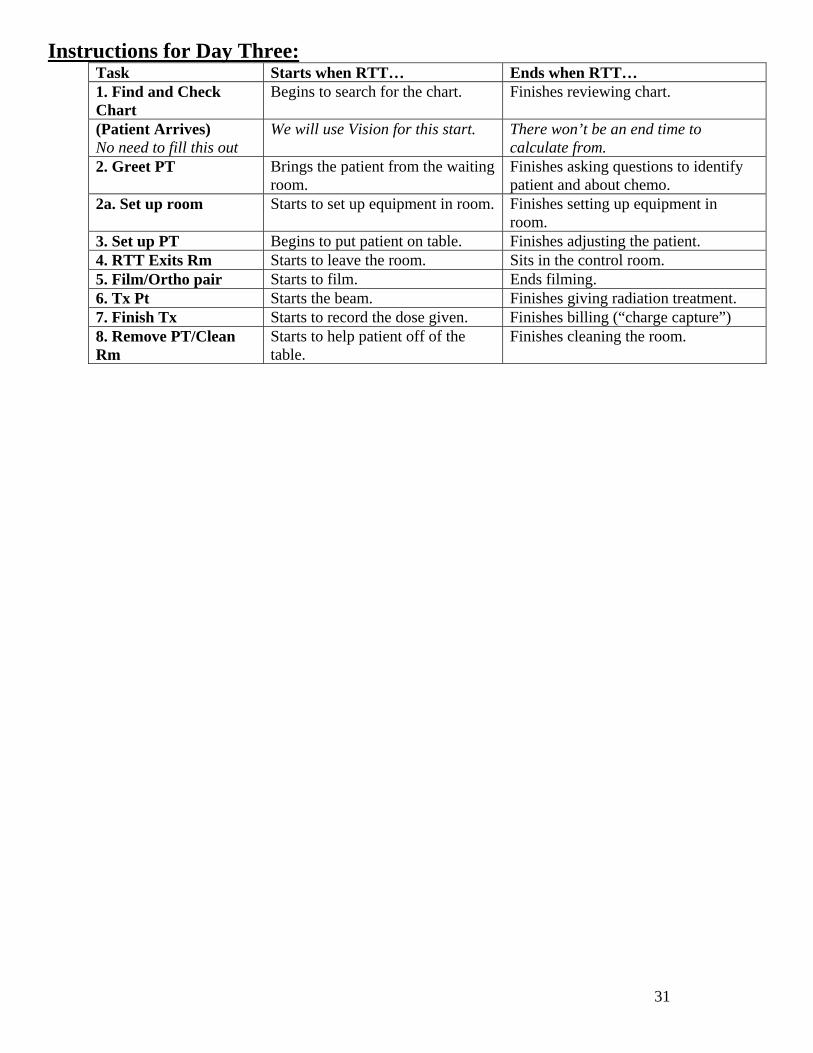
Instructions for Day Three: Task Starts when RTT… Ends when RTT… 1. Find and Check Chart
Begins to search for the chart. Finishes reviewing chart.
(Patient Arrives) No need to fill this out
We will use Vision for this start.
There won’t be an end time to calculate from.
2. Greet PT Brings the patient from the waiting room.
Finishes asking questions to identify patient and about chemo.
2a. Set up room Starts to set up equipment in room. Finishes setting up equipment in room.
3. Set up PT Begins to put patient on table. Finishes adjusting the patient. 4. RTT Exits Rm Starts to leave the room. Sits in the control room. 5. Film/Ortho pair Starts to film. Ends filming. 6. Tx Pt Starts the beam. Finishes giving radiation treatment. 7. Finish Tx Starts to record the dose given. Finishes billing (“charge capture”) 8. Remove PT/Clean Rm
Starts to help patient off of the table.
Finishes cleaning the room.

DAY THREE TREATMENT Task Start End Rework Required? Comments
32
1.Find and Check chart Yes (Look at TX Unit, Check SSDS complete, Check images checked by MD)
Reason:
2. Greet PT (Checks in, Changes, Go to WR)
Yes Reason:
2a. Set up room Yes (Get imm, Extras, 4DTC plan, Verify Patient)
Reason:
Yes 3. Set up PT (Check set up pg, Put on IMM dev., Level, Double check chart, Place acc., Place custom dev., Check light field)
Reason:
4. RTT Exits Rm (Get Key, LMO, Hit Door Butt.)
Yes Reason:
5. Film/Ortho pair
Yes Reason:
6. Tx Pt Yes (Beam on, Monitor Pt, Turn key off, Log TX in chart, AGT/In room, Repeat)
Reason:
7. Finish Tx
Yes Reason:
8. Remove PT/Clean Room
Yes Reason:
FAULTS Step Number Fault Identification Reason

Appendix B: Machine Representation Stratified By Day One, Two and Three Treatments
6/100 17.6% EX1 29.4%
EX3 11.8%
EX2 41.2%
Figure B1: Day 1 Machine Representation
6/100 18.75% EX1 31.25%
EX3 12.5%
EX2 37.5%
Figure B2: Day 2 Machine Representation
33
6/100 7.7%
EX3 7.7%
EX1 38.46%
EX2 46.15%
Figure B3: Day 3 Machine Representation

Appendix C: Weekday Representation Stratified By Day One, Two and Three Treatments Fri 5.9%
Thurs 11.8%
Mon 47.1% Wed 17.6%
Tues 17.6%
Figure C1: Day 1 Weekday Representation
Mon 12.5%
Thurs 18.75%
Wed 18.75%
Tues 50.0%
Figure C2: Day 2 Weekday Representation
Tues 15.38%
Fri 23.08%
Thurs 15.38% Wed 46.15%
Figure C3: Day 3 Weekday Representation
34
35
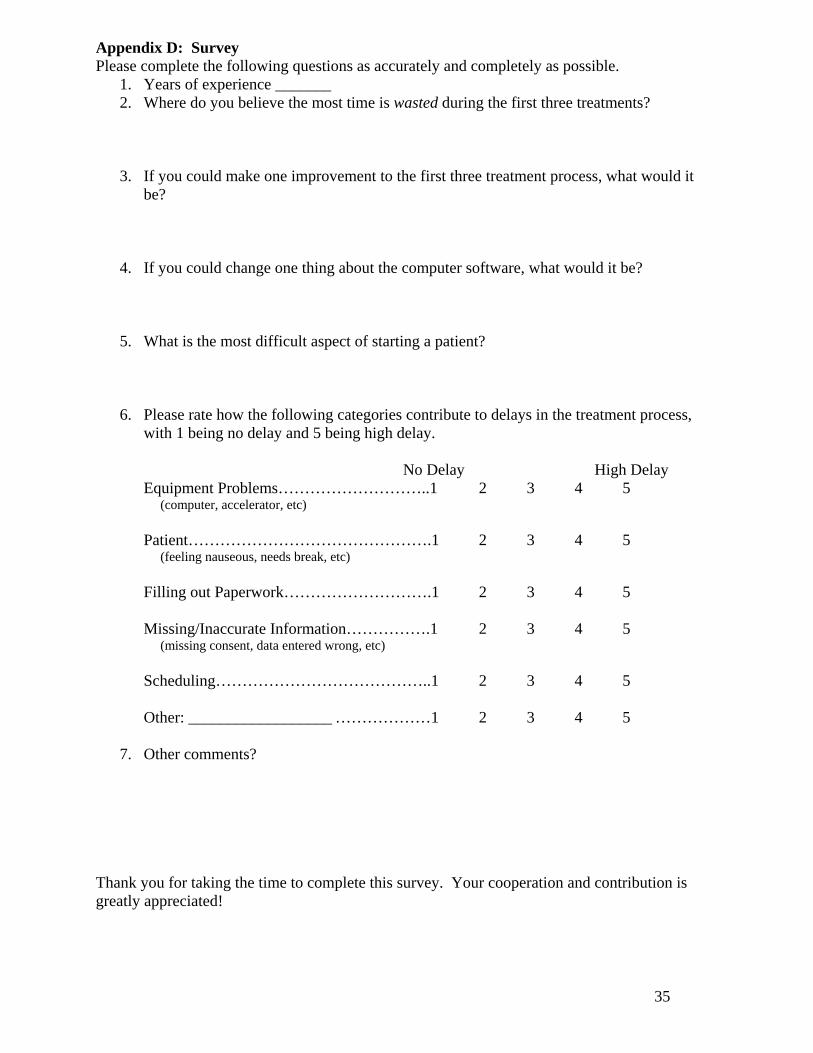
Appendix D: Survey Please complete the following questions as accurately and completely as possible.
1. Years of experience _______ 2. Where do you believe the most time is wasted during the first three treatments?
3. If you could make one improvement to the first three treatment process, what would it be?
4. If you could change one thing about the computer software, what would it be?
5. What is the most difficult aspect of starting a patient?
6. Please rate how the following categories contribute to delays in the treatment process, with 1 being no delay and 5 being high delay.
No Delay High Delay
Equipment Problems………………………..1 2 3 4 5 (computer, accelerator, etc) Patient……………………………………….1 2 3 4 5 (feeling nauseous, needs break, etc) Filling out Paperwork……………………….1 2 3 4 5 Missing/Inaccurate Information…………….1 2 3 4 5 (missing consent, data entered wrong, etc) Scheduling…………………………………..1 2 3 4 5 Other: __________________ ………………1 2 3 4 5
7. Other comments?
Thank you for taking the time to complete this survey. Your cooperation and contribution is greatly appreciated!
36
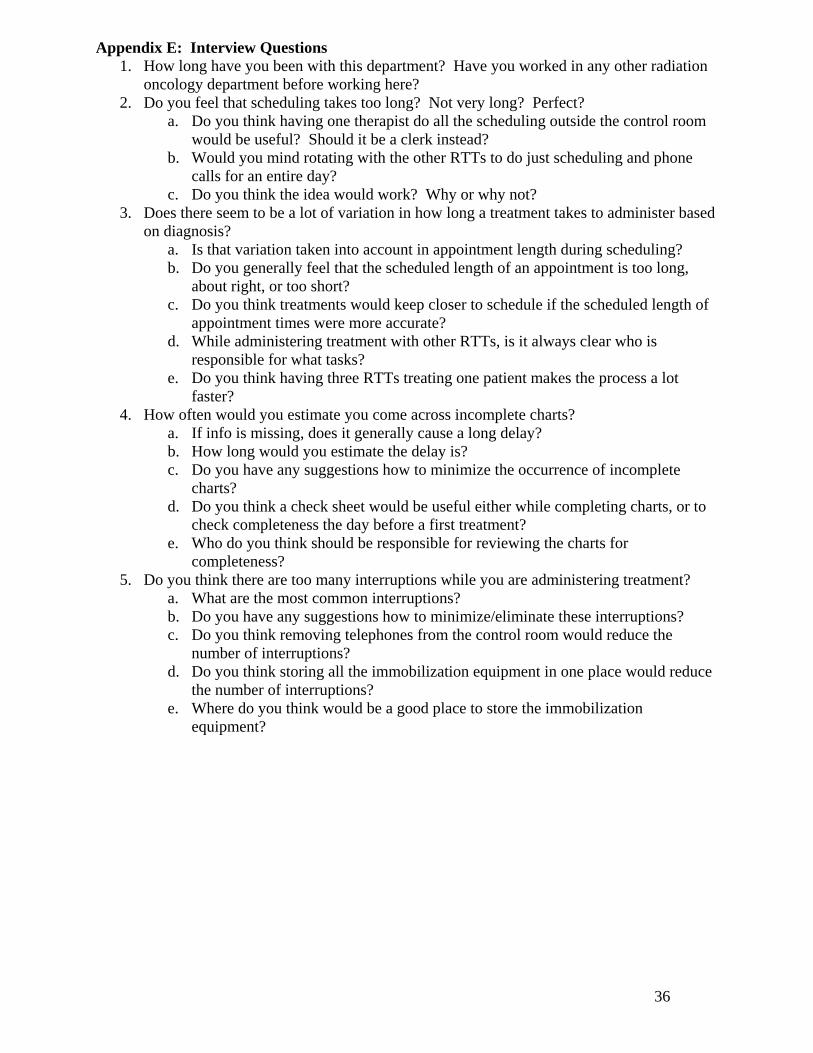
Appendix E: Interview Questions 1. How long have you been with this department? Have you worked in any other radiation
oncology department before working here? 2. Do you feel that scheduling takes too long? Not very long? Perfect?
a. Do you think having one therapist do all the scheduling outside the control room would be useful? Should it be a clerk instead?
b. Would you mind rotating with the other RTTs to do just scheduling and phone calls for an entire day?
c. Do you think the idea would work? Why or why not? 3. Does there seem to be a lot of variation in how long a treatment takes to administer based
on diagnosis? a. Is that variation taken into account in appointment length during scheduling? b. Do you generally feel that the scheduled length of an appointment is too long,
about right, or too short? c. Do you think treatments would keep closer to schedule if the scheduled length of
appointment times were more accurate? d. While administering treatment with other RTTs, is it always clear who is
responsible for what tasks? e. Do you think having three RTTs treating one patient makes the process a lot
faster? 4. How often would you estimate you come across incomplete charts?
a. If info is missing, does it generally cause a long delay? b. How long would you estimate the delay is? c. Do you have any suggestions how to minimize the occurrence of incomplete
charts? d. Do you think a check sheet would be useful either while completing charts, or to
check completeness the day before a first treatment? e. Who do you think should be responsible for reviewing the charts for
completeness? 5. Do you think there are too many interruptions while you are administering treatment?
a. What are the most common interruptions? b. Do you have any suggestions how to minimize/eliminate these interruptions? c. Do you think removing telephones from the control room would reduce the
number of interruptions? d. Do you think storing all the immobilization equipment in one place would reduce
the number of interruptions? e. Where do you think would be a good place to store the immobilization
equipment?
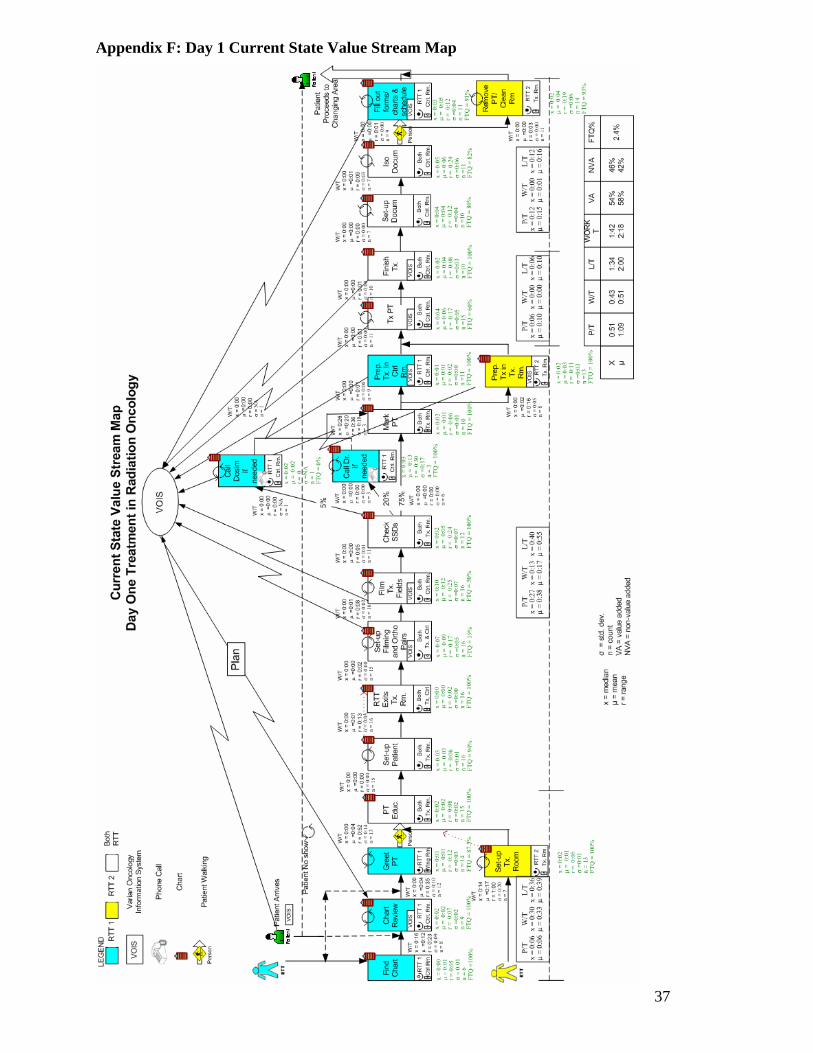
Appendix F: Day 1 Current State Value Stream Map
37
38
Appendix G. Day One First Time Quality Summary
TASK #CORRECT/TOTAL FTQ%
DEFECT
Greet PT 14/16 87.5%
• Patient went to clinic • Wrong waiting room
Set up PT 15/16 94%
• Shifted right instead of left
• Moved from marks Set up Filming/Ortho Pair 3/16
19% • Move imager (5) • Move iso (4) • Depth change (2) • Lat repeat (2) • Move gantry • Reshoot films • Restart films • Adjust chin • Loose masks
Film Fields 8/16 50%
• Move imager (4) • Move table (2) • Table kicks • Rotate gantry • Interlock on imager • Add films, not attached • Fields too long – need 2
exposures Call Dosimetry 0/1
0% • Called multiple times
Treat PT 9/15 60%
• Table kick (4) • Change wedges (3) • Did not take opens after
shape • Therapist went in room
for masks Set up Documentation 8/10
80% • Repeated measurements • No billing added
Iso documentation 9/11 82%
• Point guard • Tattoo on scab • Forgot to take photos
Remove PT 13/14 93%
• Reschedule tx time after already scheduled
Fill out forms/chart 10/11 91%
• Wrong energy in activity capture
TOTAL FTQ: 2.4% (*Dosimetry FTQ% = 0%)

Appendix H: Highlighted Waste on Day 1 Current State Value Stream Map
39

Appendix I: Day 2 Current State Value Stream Map
40

41
Appendix J: Day Two First Time Quality Summary
TASK #CORRECT/TOTAL FTQ% DEFECT
Greet PT 13/14 93%
• Dose not filled from day 1
Set Up TX Room 12/13 92%
• No set up notes • No MTH • No picture
Set Up PT 12/15 80%
• Multiple calls for films, not checked
• PT was not changed • Retrieve mask • Tboard not indexed
Set up Film/Ortho Pair 9/15 60%
• Move imager (2) • No photos of tattoo • Nose clip came off • Retract/remove dot • Day 1 films not checked • Move iso • Can’t see reshoot • Lateral table adjust • Move wrong way
Finish Treatment 15/16 94%
• MTH needed
TOTAL FTQ: 38.6%

Appendix K: Highlighted Waste on Day 2 Current State Value Stream Map
42
Appendix L: Day 3 Current State Value Stream Map
43

44
Appendix M: Day Three First Time Quality Summary
TASK #CORRECT/TOTAL FTQ% DEFECT
Find Chart 8/9 89%
• Chart in clinic
RTT Exits Room 10/12 83%
• Left key in room (2)
Set up Film/Ortho Pair 6/11 55%
• Retract imager (2) • Report due to physician
moves • Change mask marks • Mlc fault • Shoot 2nd film – outside
of tolerance Treat PT 12/13
92% • Crash KV tube into cart
Remove PT/Clean Room 12/13 92%
• Give tattoos – none given on 1st or 2nd day
TOTAL FTQ: 34.4%

Appendix N: Highlighted Waste on Day 3 Current State Value Stream Map
45
46
Appendix O: Summary of Survey Results
TIME WASTED CHANGE ONE THING
COMPUTER SOFTWARE
MOST DIFFICULT ASPECT OF JOB
• Scheduling (4) • Looking for charts,
masks etc. (4) • Doctors do not check
Day 1 images (2) • Filming (2) • Unsigned
scripts/charts (2) • Waiting for doctors to
come on set • Waiting for treatment
directive • Deciphering
complicated steps • No approval in
simulation • Dosimetry: figuring
our treatment objective
• Patients coming early/late
• Running in/out room • Locating isocenter
without carina, crests, other anatomy
• Nothing (8) • Consistent schedule for
patients; steady flow; greater balance (5)
• Review chart for completeness (2)
• Consistent schedule for therapists (same people, same treatments)
• One person responsible to gather chart/immobilization
• Doctors should check Day 1 images
• Nothing (4) • Quicker for IMRT
plans (3) • Stable software (3) • Clerks should have
time planners on computer (2)
• Single version of planning system
• Simulation/Tx more streamlined
• Direct transfer from CT/Sim to Tx machines for simple cases
• EX3 has many glitches • EWS on computer
screen • Do not transfer images
to vision • Approve/review
images immediately when taken
• Balancing multiple tasks (2)
• Dealing with patients (2)
• Dealing with changing policies/protocols (2)
• Waiting for information needed for case
• Computer planning system
• Waiting for others to finish work before I can
• Having each document ready
• Image all fields • Establishing ISO • Receiving “scrap” • Emotional aspect • Walking from parking
lot • Overall flow of
department • Nothing
VOTES FOR EACH # FOR NUMERICAL SCALE SURVEY QUESTIONS EQUIPMENT PROBLEMS
PATIENT PROBLEMS
PAPERWORK PROBLEMS
INACCURATE INFORMATION
PROBLEMS
SCHEDULING PROBLEMS
• 1: 1 • 2: 9 • 3: 3 • 4: 2 • 5: 3
• 1: 1 • 2: 9 • 3: 2 • 4: 5 • 5: 0
• 1: 2 • 2: 8 • 3: 5 • 4: 0 • 5: 1
• 1: 0 • 2: 5 • 3: 5 • 4: 5 • 5: 2
• 1: 1 • 2: 6 • 3: 4 • 4: 5 • 5: 1
47
Appendix P: Standardized Work Template
Std Work - 2 RTTs Std Work - 3 RTTs Task RTT1 RTT2 Task RTT1 RTT2 RTT3 x o x o * x o * x o o x o * x o x x * o o x o x * x o
x = primary o = secondary * = tertiary