Embed Size (px)
Citation preview

Fibrotic Myopathy of the Semitendinosus Muscle in Four Dogs
ROBERT W. MOORE, D.V.M.,' GLEN P. ROUSE, D.V.M., M.S.,' D. L. PIERMATTEI, D.V.M., PHD.,*$ AND H. RODNEY FERGUSON, D.V.M., M.S., ptiD.t$
Fibrosis of the semitendinosus muscle resulted in a characteristic gait abnormality in four male German shepherd dogs. Blood chemistry, electrophoresis, and electromyographic studies were performed. Surgery was undertaken in each case to relieve the restricting fibrous tissue. The lameness returned with reappear- ance of the fibrous band within six months. The etiology of fibrotic myopathy is unknown, but electromyographic studies and electrophoresis results suggest a myopathy due to chronic inflammation. Histopathologic exam reveals replacement of degenerating muscle fi- bers with connective tissue.
IBROTIC MYOPATHY has been described in the F h o r s e , I in and in the dog6-'0 in various muscles. Little is known concerning the etiology of this disease other than its general association with trauma (in the horse) or intramuscular injections (man). Fibrotic myopathy of the semitendinosus mus- cle previously has been reported in the horse and is also associated with fibrosis of the semimembranosus and biceps femoris muscles.' This article discusses four cases of fibrotic myopathy of the semitendinosus muscle in the dog. Blood chemistry, electromyo- graphic (EMG) studies, and histopathologic alterations are presented.
Anatomy
The semitendinosus muscle arises on the caudal and ventrolateral parts of the lateral angle of the ischiatic tuberosity between the biceps femoris and the semimembranosus muscles. I t passes deep to the aponeurosis of the gracilis muscle and attraches to the medial surface of the tibia cranial to the flexor muscles but distal to the primary insertions of the semi- membranosus and gracilis muscles. Separate strands from both the gracilis and semitendinosus extend cra- nially in the crural fascia to attach to the rough surface of the distal end of the tibial crest. From the caudal edge near its origin, a tendon originates and unites with a tendon of the gracilis muscle to insert on the tuber
$ Diplomate, American College of Veterinary Surgeons.
Colorado State University, Fort Collins, Colorado 80523. Reprint requests: R. W. Moore, Department of Clinical Sciences,
From the 'Department of Clinical Sciences, Colorado State University,
Fort Collins, Colorado, and the tDepartment of Small Animal Surgery,
Kansas State University, Manhattan, Kansas
calcis. The function of the semitendinosus is extension of the hip, stifle, and tarsus, and flexion of the stifle when in a non-weight-bearing position. It is innervated by muscular branches of the tibial nerve."
Case Reports
Case I A four-year-old intact German shepherd was admit-
ted to Colorado State University Veterinary Teaching Hospital (CSU-VTH) with a history of a gradual onset of lameness in the right rear limb of approximately two months' duration. There was no history of trauma or pain associated with the lameness. Temperature, pulse, and respiration were normal. No pain could be elicited upon manipulation of the limb, but a dense, taut band could be palpated on the caudomedial aspect of the upper limb in the region of the semitendinosus muscle (Fig. 1). Radiographs of the stifle showed no changes in the bone or soft tissue. However, multiple metallic fragments were visible in the soft tissues around the stifle. The dog had a peculiar gait (Figs. 2A-D). As the limb was advanced the hock rotated externally and the stifle rotated internally. Just before the end of the swing phase, the limb would pull back- ward several inches and then be placed down. A tentative diagnosis of f ibrotic myopathy of the semitendinosus muscle was made.
Surgical exploration of the semitendinosus muscle revealed a thick fibrous band within the muscle belly. A 3-inch myotenectomy of the semitendinosus muscle and fibrous band was performed (Fig. 3). The tissue was submitted for histopathologic evaluation. The dog's gait was improved immediately after surgery, but three months later the dog was readmitted for the same lameness which had gradually reappeared. It was
0161-3499/81/1000/0169/$00.80 @) American College of Veterinary Surgeons
169

170 VETERINARY SURGERY October-December 1981 Vol. 10
noted at physical exam that the taut band was present as before. The owner elected to have no further surgery and the dog was sent home. Five years later the dog was reexamined. The characteristic gait ab- normality was still present but not apparently worse. The dog was an acceptable pet and did not seem to have any pain except that associated with hip dysplasia in the opposite limb.
Cuse 2
A seven-year-old intact male German shepherd was presented to CSU-VTH with a history of lameness in the right rear limb of approximately one and a half months’ duration. For the past four years the owner had taken the dog jogging daily for a distance of four miles. For the past several weeks the dog seemed to pace sideways. No other lameness problems had been seen and there was no history of trauma. The dog was less lame when running than when walking but did not seem to work out of the lameness. Advancement of the limb resulted in external rotation of the hock, internal rotation of the stifle, and caudal displacement just prior to touching the limb to the floor. No pain could be elicited through a full range of motion of the hip and stifle joints. A taut fibrous band could be palpated on the caudomedial aspect of the limb. Complete blood count (CBC), blood chemistry, and two protein elec- trophoresis test results were normal. The creatinine phosphokinase (CPK) was 120 (normal, 0-SO) , with the CPK isoenzyme MM component at 54.5% (normal, 30-50%). The lactic dehydrogenase (LDH) was 97 (normal, 0-90) but no isoenzymes were ran. EMG studies of the sernitendinosus muscle showed an ab- sence of normal muscle and fibrillation potentials.
At surgery a 2-cm-wide x 1-cm-thick fibrous band could be visualized extending from the tuber ischii to the tibia within the belly of the semitendinosus muscle. The band was dissected and removed for his- topathologic evaluation. After surgery the gait re- turned to normal, and the dog remained normal for approximately three months, at which time the gait abnormality and fibrous band returned. The owners elected to have no further surgery. The dog was euthanized one year later for other causes. A necropsy was not permitted,
Clrse 3
A five-year-old intact male German shepherd was presented to CSU-VTH with a history of a right rear limb lameness. The lameness was first noted three to four months previously and had progressed to the point where the dog was non-weight bearing at times. Also noted in the history was an incident of the dog
Fig. 1. Note the taut fibrous band extending down the me- dial aspect of the femur,
running into a pole, with resulting trauma to the chest area which caused no long-term problems. No pain could be elicited with manipulation of the limb. As the dog ambulated, the stifle rotated internally and the hock externally. Thickening of the semitendinosus muscle was discovered on later physical examination. CBC and blood chemistry results were normal, includ- ing LDH and CPK enzymes. Radiographic examina- tion for hip dysplasia was negative. Radiographic in- spection of the lumbar spine showed early signs of spondylosis at L7-S1 but no other radiographic ab- normalities. Surgical exploration of the fibrotic area revealed fibrous adhesions within and between the muscle bellies of the semitendinosus and gracilis mus- cles. The two muscle bellies were isolated and re- moved. The dog’s gait appeared normal four days postoperatively, and he remained normal for six to eight months. Fourteen months after surgery the pa- patient became progressively lame on the right leg and was re-admitted to CSU-VTH for evaluation. A fibrotic

FIBROTIC MYOPATHY Moore, et al. 171 No. 4
A
Fig. 2A (top left). The characteristic gait is seen with a lengthened caudal phase and a shortened cranial phase. With the "goose-stepping" the dog overreaches by 3 to 4 inches and then places the leg back and down. B (top right), C (middle), D (bottom). As the limb is carried forward the hock rotates exter- nally and the stifle rotates internally. As the paw contacts the ground, the limb is no longer rotated.
tendinous structure could be palpated again in the area of the semitendinosus muscle. Radiographic findings of the stifle and pelvic areas were again normal. CBC and blood chemistries were within normal ranges, ex- cept for serum glutamic-oxaloacetic transaminase (SGOT), which was 65 (normal, 15-50) and the CPK, which was 80 with the MM isoenzyme being 91% (normal, 30-5096). The LDH was 90 with isoenzyme levels being normal. Serum electrophoresis showed an increase in beta-1 and gammaglobulin levels, sugges- tive of chronic inflammation or an autoimmune prob- lem. EMG studies along the fibrous band showed fib- rillations. The dog was sent home to be returned in one month for follow-up EMG studies. However, the dog began to have seizures one month later and died shortly after emergency presentation to the hospital. No specific cause of death could be determined at nec- ropsy. A 1-cm x 0.3-cm fibrous band was found to be
c
W r\

172 VETERINARY SURGERY October-December 1981 VOl. 10
stretching from the tuber ischii to the stifle along the entire length of the semimembranosus muscle. There was loss of muscle striations and some minor inflam- matory changes histologically.
Case 4
A two-year-old intact male German shepherd was presented to the University of Minnesota Veterinary Hospital with a history of a gait abnormality in the left rear limb, identical to that described in the three previ- ous cases. Four months previously the dog had fallen -
down some stairs and was found splay-legged. Since that time, gait abnormality had progressed. A fibrous band could be palpated on the caudomedial thigh that
Fig. 3. This thick fibrous band was found to run the entire of the semi~endinosus
prevented full extension of the limb. CBC results were normal. At surgery the semitendinosus muscle ap- peared as a yellowish-white band of connective tissue about 2 cm x 4 mm in size. A tenorrhaphy was per- formed to lengthen the band by 5 to 6 cm. No tissue was taken for histology. Following surgery the dog's gait was very close to normal, and full extension of the stifle was possible. Long-term follow-up on this case is not known, although there was still gait abnormality ten days postoperatively.
Histologic Evaluation
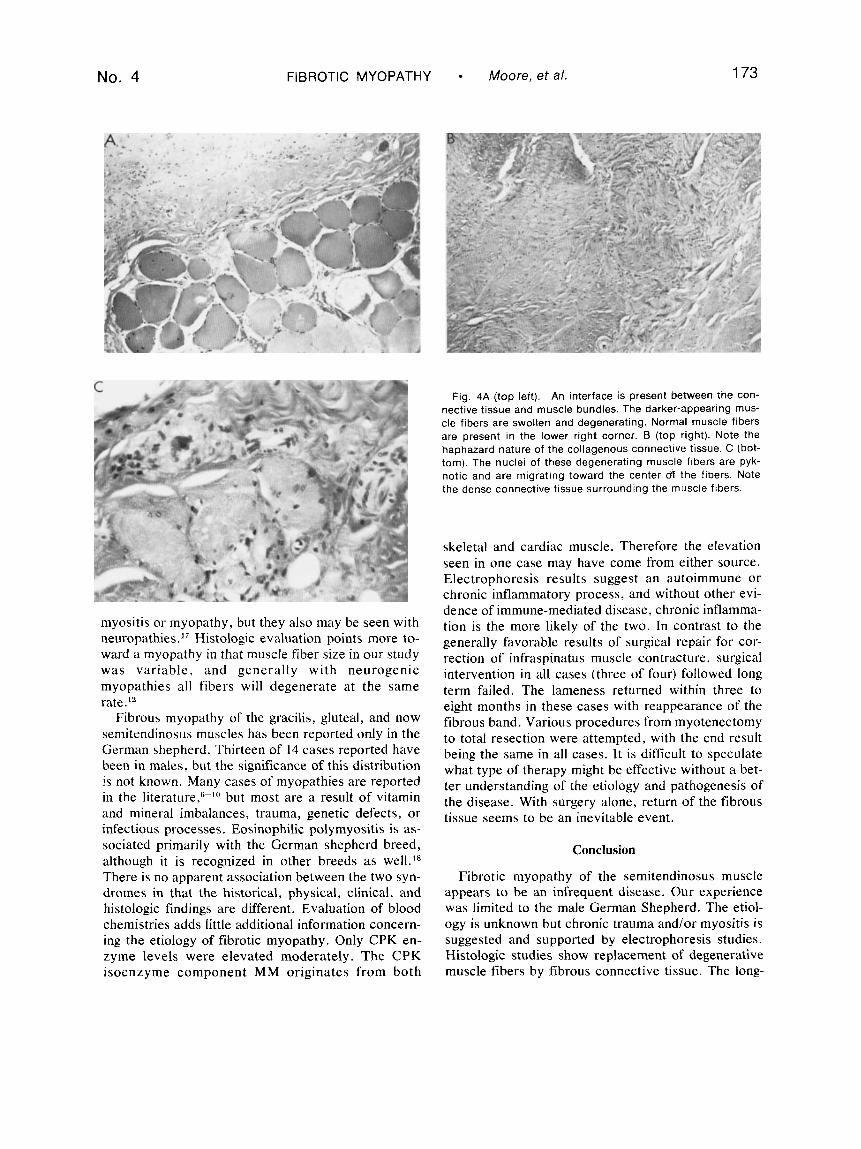
Tissue samples were submitted in three of four dogs. All samples had a similar appearance. An abundance of dense collagenous connective tissue was present in an extremely haphazard manner. Normal muscle fi- bers were visible, along with swollen degenerative fi- bers. Pyknotic nuclei were present, as well as nuclei migrating from the periphery of the muscle fiber and appearing in the center of the fiber (Figs. 4A-C). In most areas a very distinct interface was present be- tween connective tissue and muscle bundles. In other areas abundant connective tissue was present between muscle bundles and totally surrounded some smaller bundles. Only minimal inflammatory changes were present. The haphazard nature of the connective tissue is generally associated with an active replacement process. The presence of a degenerative myopathy is evidenced by abnormal nuclei, loss of sarcolemma, vacuolar degeneration, and variability in muscle fiber size.12 These changes are similar to those previously reported in contracture of the infraspinatus muscle.*
Discussion
Previous reports of fibrotic myopathy in the dog de- scribe involvement of the infraspinatu~,~-~O supra- sp ina tu~ ,~ gra~i l i s ,~ and quadriceps7 muscle groups. A
fibrosing and ossifying myositis has also been reported in the gluteal muscles in dogs.6 In man, muscle fibrosis is described in several muscle groups, the most com- mon of which are the q ~ a d r i c e p s , ~ gluteals2j" and del- t o i d ~ . ~ In the horse fibrosing myopathies are reported to occur in the semitendinosus, biceps, semimem- branosus,' and gracilis13 and are associated with os- sifying myopathy of the same muscles.
Attempts have been made to determine the etio- pathogenesis of fibrotic my~pathy.~-'O In our series, all dogs were intact male German shepherds with an age range from two to seven years. In three of four dogs the right rear limb was affected. All dogs were described by their owners as being very active, but none were used as working dogs and only one was exercised for any great distance on a daily basis. Ex- cessive exercise over a long period resulting in tearing or stretching of muscle fibers has been proposed as an agent responsible for fibrotic myopathy.'S7 Acute trauma has also been implicated in fibrotic myopathy.R Only one of the four dogs had a definitive history of acute trauma, and no definite association with trauma, either acute or chronic, could be concluded from this study. In man, fibrous myopathy is primarily as- sociated with long-term parenteral injections, with meperidine and pentazocine having accounted for many of the cases.I4 Drug addicts are known to de- velop chronic muscle fibrosis, and antibiotic and tetanus injections in children have also resulted in this d i s e a ~ e . ~ , ~ , ' ~ Antibiotic injections in dogs have also been shown to cause f i b r o s i ~ . ' ~ Repeated needle trauma itself mHy add to the process of fibrosis.I6
Fibrous myopathy could be the result of a primary neuropathy or primary myopathy . The total absence of muscle potentials in one dog indicates a complete lack of muscle fibers. Fibrillation or denervation potentials, as seen in another dog, are generally associated with
No. 4 FIBROTIC MYOPATHY Moore, et a/. 173
myositis or myopathy, but they also may be seen with neuropathies." Histologic evaluation points more to- ward a myopathy in that muscle fiber size in our study was variable, and generally with neurogenic myopathies all fibers will degenerate at the same rate.12
Fibrous myopathy of the gracilis, gluteal, and now semitendinosus muscles has been reported only in the German shepherd. Thirteen of 14 cases reported have been in males, but the significance of this distribution is not known. Many cases of myopathies are reported in the literature,fi-lu but most are a result of vitamin and mineral imbalances, trauma, genetic defects, or infectious processes. Eosinophilic polymyositis is as- sociated primarily with the German shepherd breed, although it is recognized in other breeds as well.'x There is no apparent association between the two syn- dromes in that the historical, physical, clinical, and histologic findings are different. Evaluation of blood chemistries adds little additional information concern- ing the etiology of fibrotic myopathy. Only CPK en- zyme levels were elevated moderately. The CPK isoenzyme component MM originates from both
Fig. 4A (top left). An interface is present between the con- nective tissue and muscle bundles. The darker-appearing mus- cle fibers are swollen and degenerating. Normal muscle fibers are present in the lower right corner. B (top right). Note the haphazard nature of the collagenous connective tissue. C (bot- tom). The nuclei of these degenerating muscle fibers are pyk- notic and are migrating toward the center fl the fibers. Note the dense connective tissue surrounding the muscle fibers.
skeletal and cardiac muscle. Therefore the elevation seen in one case may have come from either source. Electrophoresis results suggest an autoimmune or chronic inflammatory process, and without other evi- dence of immune-mediated disease, chronic inflamma- tion is the more likely of the two. In contrast to the generally favorable results of surgical repair for cor- rection of infraspinatus muscle contracture, surgical intervention in all cases (three of four) followed long term failed. The lameness returned within three to eight months in these cases with reappearance of the fibrous band. Various procedures from myotenectomy to total resection were attempted, with the end result being the same in all cases. It is difficult to speculate what type of therapy might be effective without a bet- ter understanding of the etiology and pathogenesis of the disease. With surgery alone, return of the fibrous tissue seems to be an inevitable event.
Conclusion
Fibrotic myopathy of the semitendinosus muscle appears to be an infrequent disease. Our experience was limited to the male German Shepherd. The etiol- ogy is unknown but chronic trauma and/or myositis is suggested and supported by electrophoresis studies. Histologic studies show replacement of degenerative muscle fibers by fibrous connective tissue. The long-

1 74 VETERINARY SURGERY
term prognosis has been poor following surgery, with the lameness returning to all dogs within three to eight months.
References
1. A d a m OR: Lameness in Horses. 3rd ed. Philadelphia, Lea & Febiger, 1974, pp 320-322.
2. Sacristan HD, Sanchez-Brba A, Stem LL, et al: Fibrosis of the gluteal muscle. J Bone Joint Surg 56: 1510, 1974.
3. Yadar SS: Extension contracture of the hip due to idiopathic fibrosis of the gluteus maximus. Int Surg 63: 27, 1978.
4. Mukhejee PK, Das AK: Injection fibrosis in the quadriceps femoris muscle in children. J Bone Joint Surg 62: 453, 1980.
5. Wolbink AJ, Hsu Z, Bianco AJ: Abduction contracture of the shoulders and hip secondary to fibrous bands: report of a case. J Bone Joint Surg 55: 844, 1973.
6. Lie SK, Dorfman HD: A condition resembling human localized myositis ossificans in two dogs. J Small Anim Pract 17: 371, 1976.
7. Vaughan LC: Muscle and tendon injuries in dogs. J Small Anim Pract 20: 711, 1979.
October-December 1981 VOl. 10
8. Pettit GD, Chatburn CC, Hegreberg GA, et al: Studies on the pathophysiology of infraspinatus muscle contracture in the dog. Vet Surg 1: 8, 1978.
9. Hufford TJ, Olmstead ML, Butler HC: Contracture of the in- fraspinatus muscle and surgical correction in two dogs. J Am Anim Hosp Assoc 11: 613, 1975.
10. Pettit GD, Slatter DH: Infraspinatus contracture associated with suprascapular paralysis in a dog. J Small Anim Pract 13: 699, 1972.
11. Miller ME, Christensen GC, Evans HE: Anatomy of the Dog. Philadelphia, WB Saunders, 1964, p 238.
12. Adams RD, Denny-Brown D, Pearson CM: Diseases of the Muscle. New York, Harper & Row, 1962.
13. Bishop R: Fibrotic myopathy in thegracilis muscle of a horse. Vet Med Small Anim Clin 67: 270, 1972.
14. Levin BE, Engel WK: Iatrogenic muscle fibrosis-arm levitation as an initial sign. J Am Med Assoc 10: 621, 1975.
IS. Gray JE: Local histologic changes following long term in- tramuscular injections. Arch Pathol 84: 522, 1967.
16. Engel WK: Focal myopathic changes produced by electromyo- graphic and hypodermic needles. Arch Neurol 16: 509, 1967.
17. Hoerlein BF: Canine Neurology. 2nd ed. Philadelphia, WB Saunders, 1971, pp 212-213.
18. Scott DW, deLahunta A: Eosinophilic polymyositis in a dog. Cornell Vet 64: 47. 1974.
J. B. L I P P I N C O l T COMPANY, EAST WASHINGTON SQUARE, P H I L A D E L P H I A , PA 19105 EOITOS w.n. ,"a C ~ m n Y . I.,*"SLdd~*l,
0. L. P I E R E I A I T E I . D W , 111 EAST DRAKE, SUITE 7 0 5 8 , FT. C O L L I N S , CO 8 0 5 2 3 MINIGINS E D l l O l p..". ."*COmp*(.L,,l"g .*#,",I
1 DiBORrui A . FINCH, EAST WASHINGTON SQUARE. PHILADELPHIA. PA 1 9 1 0 5





























