Embed Size (px)
Citation preview

Fetal Chest and Heart

Normal Imaging of the Chest
• Heart:– ¼ to 1/3 of thoracic cavity– Apex to left– Cardiac axis approximately 45°
• Lungs– Homogenous, intermediate echogenicity– Echogenicity increases with age– Volume of right greater than left, lobar anatomy not appreciable
• Diaphragm– Continuous hypoechoic band between pleural and peritoneal
cavities

Fetal Heart

Normal Lungs and Diaphragm



CONGENITAL DIAPHRAGM HERNIA• Bochdalek - 90% on left; most unilat• All should have amniocentesis and
dedicated echo• Secondary pulmonary hypoplasia is
major cause of mortality• Findings
– Polyhydramnios– Stomach/bowel/liver adjacent to heart
• Absent stomach bubble in normal spot
– Peristalsis in chest– Mediastinal shift– Absent gastric bubble– Reduced abdominal circumference
compared to rest of fetal biometry

• Associated anomalies– Aneuploidy (T18, T21); NTD; CHD; malrotation, omphalocele
• DDX– CCAM– Other cystic masses such as foregut duplication cysts are
rare


CCAM• Most common fetal lung mass (75%)• Types I-III
– Types I and II macroscopic cysts >5mm with good prognosis and hydrops is rare
• Small risk of malignant degeneration (rhabdomyosarcoma)• Imaging
– Macroscopic types appear cystic– Microscopic types appear solid (echogenic)
• Pulmonary hypoplasia of normal lung - degree determines prognosis• Mediastinal shift - cardiac compromise causes polyhydramnios (impaired
swallowing) and hydrops• Associations (type II)
– Cardiac anomalies– Pulmonary sequestration– Pectus excavatum– Jejunal atresia– Renal agenesis, prune-belly syndrome
• Pathology– Hamartomatous proliferation of terminal bronchioles– Cysts lined by respiratory epithelium and communicate with airways at birth– Vasc supply from pulmonary artery

CCAM


EXTRALOBAR SEQUESTRATION• More common in males (4:1)• 90% LLL or below diaphragm• Always airless as it has its own pleural envelope and no
communication with bronchial tree• Systemic arterial supply - Aorta 80%• Systemic venous drainage - IVC, azygos, portal v • Imaging Findings
– Solid hyperechogenic mass– Look for systemic arterial supply on Doppler– Polyhydramnios– Hydrops
• Associations 65%– CDH– Cardiac– GI, Renal, Vertebral anomalies
• Often regress in utero• DDX
– CCAM– Congential lobar emphysema (initially filled with fetal fluid)– Neuroblastoma

Bronchopulmonary Sequestration

Teratoma
• Neoplasm composed of all three germ cell layers• In the thorax, most originate from the mediastinum or
pericardium, primary lung teratomas are rare• Variable size but typically large, may grow rapidly• Appears as heterogenous mass with solid and cystic
components, calcification is the most specific feature but is not always present, no feeder vessel
• Mediastinal– Typically occur anteriorly and may cross midline– Difficult to distinguish from lung mass
• Pericardial– May be intra or extra pericardial. Intracardiac nearly always have a
pericardial effusion and are at risk of tamponade

Pericardial Mass

PULMONARY HYPOPLASIA• Agenesis – complete absence of one or both lungs
(airways, alveoli, and vessels)• Aplasia – absence of lung except for a rudimentary
bronchus that ends in a blind pouch• Hypoplasia – decrease in number and size of
airways and alveoli– Primary– Secondary
• Bilateral - Oligohydramnios (Potter’s sequence); Skeletal dysplasia
• Unilateral - CCAM; Sequestration; CDH; Hydrothorax
• Imaging– Reduced thoracic circumference (<2SD) is suggestive– Fetal lung maturity best sssessed with
lecithin:sphingomyelin ratio in amniotic fluid– Echogenic pattern unreliable marker for maturity

Pulmonary Hypoplasia
– Oligohydramnios• Renal conditions (agenesis, obstruction, polycystic disease)• PROM• IUGR (placental insufficiency, aneuploidy)
– Cardiac Malformations• Right sided obstruction decreasing pulmonary blood flow• Pulmonary atresia or stenosis• Hypoplastic right heart
– Neuromuscular Abnormalities• Decreased fetal breathing and poor lung development
– Thoracic cavity mechanical problems• Small or deformed thoracic cavity – osteogenesis imperfecta,
achondrogenesis, asphyxiating thoracic dystrophy etc.

Pulmonary Hypoplasia
• Imaging– No universally accepted diagnostic criteria– Many measurements and ratios
• Thoracic circumference – correlate with GA or as ratio with another growth parameter, particularly AC. TC/AC ratio > 0.80
• Lung head ratio – mainly in CDH – measure contralateral lung volume and divide by HC to give LHR - <1.0 poor, >1.4 good
• Peripheral pulmonary artery resistance (Doppler) – increased in hypoplasia but non specific
• Pulmonary artery Doppler of acceleration time/ejection time (AT/ET).
– Normal ‘spike and dome’ pattern with reversal of flow at diastole due to closure of pulmonary valve
– Normal ratios are 0.17 on right, 0.15 left, low ratio suggestive of hypoplasia

Normal Pulmonary Artery

Fetal Heart Normal View
• 4 chamber view– Atrial and ventricular septa, mitral and tricuspid valves– Axis 45°-50°– Foramen ovale interrupts atrial septum, with the flap of
the foramen opening towards the left atrium– Ventricles are approximately same size– Right ventricle characterised by moderator band, and
lower septal attachments of tricuspid valve
• Base of heart• Left and Right ventricular outflow tracts• Aortic ‘candy cane’

FETAL HEARTTechnique• Abdominal situs view
– 4-chamber view– LVOT
• Posterior/central to RVOT• Runs left to right
– RVOT• Anterior to LVOT• Runs right to left• Bifurcates early: DA and RPA• Check for antegrade flow in DA• Anatomical trifurcation: DA, RPA, LPA
– 3-vessel view
• amniocentesis indicated in all abnormal: 15-40% will have chromosomal anomalies
• ventricles/atria are of roughly same size as other ventricle/atria• 3 in 1 rule: heart fills 1/3 of axial chest• Cardiac circumference 1/2 chest circumference• Length atrial septum: ventricular septum 1:2• Normal HR: 120-160bpm, SR

• Best seen on Four-Chamber View– Septal defect– Endocardial cushion defect (AVSD)– Hypoplastic left heart– Ebstein’s anomaly– Critical AS– Coarctation

4 chamber view

3-VESSEL VIEW
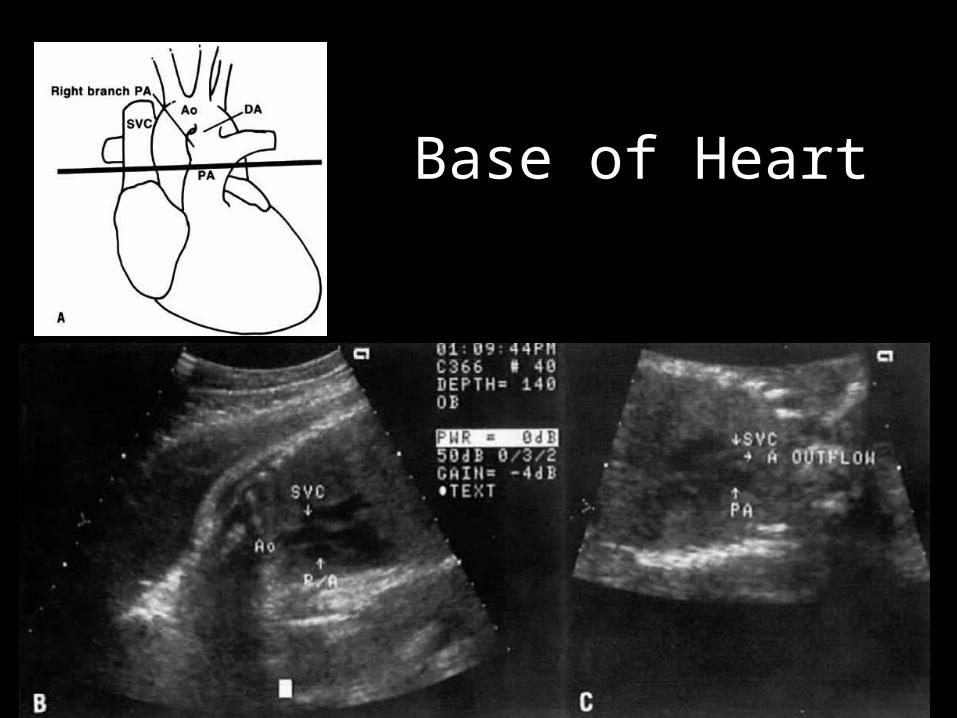
Base of Heart

VOT

Aorta – candy cane


Pericardial Effusion
• Pericardial fluid >2mm in depth is abnormal• Multiple causes:
– Cardiac abnormality • Structural• CMO• Arrhythmia
– As a feature of hydrops– Congenital infection – TORCH– High output state
• tumour • AVM• anaemia• TTTS

VSD
• Most common cardiac anomaly (20-40%) congenital heart defect, and 50% are associated with another anomaly
• Location– Membranous 80% - associated with tetralogy, truncus
– Muscular 10%
– Outlet 5% - often associated with aortic insufficiency
– Inlet 5% - component of AVSD or endocardial cushion defect
• Karyotype if associated extra-cardiac anomaly (trisomy, Holt Oram)
• Monitor growth• Many are undetected, and only appreciable at birth or
beyond• 50% close spontaneously, may need surgical closure
especially if large with shunting

Title

VSD
• Imaging findings:– May see defect in b mode – echogenic edge– Needs to be seen in 2 planes– Doppler – may be only clue
• Bi directional shunt as right and left ventricular pressures similar in fetus
• If unidirectional, look for other cardiac anomaly altering ventricular pressures

VSD

VSD

AVSD/Endocardial Cushion Defect
• EC forms lower atrial septum, superior ventricular septum, anterior MV leaflet and septal TV leaflet
• Central heart defect involving – Atrial septum– Ventricular septum– Atrioventricular valves– Conducting system
• Spectrum – partial more common than complete in newborns
• 2-7% of congenital heart defects• High association with aneuploidy
– 40% have trisomy 21

AVSD
• Imaging findings– Single AV valve makes solid line across heart in systole
(normally there is an offset of 2mm between valves)– Atrial and ventricular septal defect – b mode and
Doppler– Arrhythmia – especially CHB– Additional cardiac malformations are common
• Tetralogy of fallot• Pulmonary stenosis• Left heart/LVOT obstruction• AV regurgitation
– Fetal heart failure and hydrops (poor prognosis)

AVSD/Endocardial Cushion Defect

Ebstein’s Anomaly• Septal and posterior leaflets of tricuspid valve
prolapse and are integrated into RV wall• Atrialisation of RV• Large RA due to massive regurg• Maternal lithium is a risk factor

Hypoplastic Left Heart Syndrome
• Small/hypoplastic left ventricle, associated with– Aortic atresia/stenosis– Mitral atresia/stenosis– Hypoplastic ascending aorta
• 9% of congenital heart defects• Associated with chromosomal abnormalities in 2-10%,
particularly Turner’s, karyotype should be considered• Prognosis: 20% fetal demise, long term survival 30years
with surgical treatment, otherwise rapidly (weeks) fatal• Imaging:
– Small left ventricle with poor contraction (4 chamber)– Normal right ventricle– Bowing of atrial septa to right, minimal flow across mitral valve– Small ascending aorta with minimal flow across aortic valve

LVOTO
• Obstruction to flow across the aortic valve– Valvular– Subvalvular– Supravalvular
• 2-3% of congenital heart defects• Associated with chromosomal abnormalities, particularly
supravalvular (Turner’s, William’s syndrome)• Prognosis depends on severity and surgical intervention, in
extreme cases may consider fetal balloon valvuloplasty

LVOTO
• Imaging features– Variable size of left ventricle, usually with reduced function– May see RV hypertrophy to compensate– Turbulent Doppler flow across LVOT– MR from increased LV pressure– Left to right flow (shunting) across foramen ovale
– Subvalvular• Muscular: asymmetrical septal hypertrophy
• Membranous: membrane from septum to mitral valve
– Valvular• Thickened valve leaflets (often bicuspid)
– Supravalvular• Narrow/stenosis in proximal ascending aorta

Pulmonary Atresia• Hypoplastic RA and RV• Pulmonary artery calibre may be
normal• Reversed flow in DA

Persistent Truncus Arteriosus
• Single vessel overriding outflow valves and feeding aorta and pulmonary artery
• 1% of congenital heart defects• Almost always associated with a VSD, right sided arch in
30% of cases• Needs early surgical correction to avoid pulmonary HTN,
excellent prognosis with surgery• High association with 22q11 deletion – karyotype for
recurrence risk• Association with maternal diabetes• Imaging
– Failure of normal crossing of great vessels– Single truncus vessel dividing into aorta and pulmonary artery

Transposition of Great Vessels
• 5 % of congenital heart defects• Rare association with aneuploidy• There is an association with maternal diabetes• Excellent prognosis
• Imaging– Careful orientation required– Failure of vessels to cross– Vessels arising from either side of the septum

Transposition of Great Vessels• Aorta arises from RV and pulmonary trunk
from LV• Aorta and pulmonary artery are parallel
instead of perpendicular to each other

Tetralogy of Fallot
• 3-7% of congenital heart defects• 4 components
– Right ventricular outflow tract obstruction– VSD– Overriding aorta– Right ventricular hypertrophy
• Associated with chromosomal abnormalities in 45% cases, and fetal cases should be karyotyped– Trisomy 21– Trisomy 18 and 13– PKU
• Excellent prognosis in the absence of chromosomal abnormality

Tetralogy of Fallot
• Imaging:– 4 chamber view normal in most cases– Large aortic outflow (due to VSD and RVOT obstruction)– Aortic root overriding VSD– RVOT obstruction
• Abnormal pulmonary valve• Small pulmonary annulus• Turbulent flow in RVOT
– Abnormal ductus arteriosis – small or absent
– Heart failure and hydrops

Double Outlet Right Ventricle
• Both great arteries arise partially or completely from right ventricle
• 1-2% of congenital hear defects• Nearly always associated with a VSD• High association with chromosomal abnormalities (18&13) • Good prognosis with surgery in the absence of
chromosomal abnormalities• Imaging
– Usually not evident on 4 chamber view– Great vessels are parallel (do not cross)– Both aorta and PA arise from right ventricle– Need to show both on one side of septum to differentiate between
transposition

Endocardial Fibroelastosis• Increased echogenicity of
endocardium• Ventricular dilatation and poor
contractility
Ectopia Cordis

Rhabdomyoma• Hamartoma of myocytes• Strong association with Tuberous Sclerosis
– 50-85% of fetuses with it have TS– 50% of TS have it
• Echogenic mass, usually intraventricular, can arise from IV septum

Arrhythmia
• 1-2% pregnancies, <10% are significant
• Premature atria or ventricular contraction – – transient and benign, – account for over 90% or arrhythmias– Need no treatment, but advise to reduce caffeine, nicotine– Monitor weekly for SVT
• SVT: 1 to 1 AV relationship– Most common tachyarrhythmia– Typical rate of 230-280– Treatment recommended to prevent hydrops– Digoxin 1st line (Flecanide, amiodarone, sotalol)
• Atrial Flutter– Typical rate of 300-500– Variable AV block– Treat as for SVT

Arrhythmia• Second degree heart block
– Type 1 (Wencheback) – usually benign and does not progress to complete heart block
– Type 2 (constant prolonged AV conduction time with dropped beats) – may progress to CHB
– Monitor for CHB – no pharmacological therapy
• Complete Heart Block
– Association with maternal autoimmune diseases, and structural heart conditions
– High mortality (20%)
– Survivors nearly always need pacemaker
– Pharmacological therapy in utero is limited and unproven
• Fetal bradycardia (HR <100 for >10sec)– If persistent - consider structural cardiac defects or maternal CVD



































