Embed Size (px)
Citation preview

������������������� ���������� �
����
���������� �������������� ������������������� ������� ����������������������������
������� �����
�� ���������������������������� �������� �����������������������������������
���������
���������������������������������� !�"�#�"��" "$�%��������
����������������������� ������� ��������������������������������������������������������������������������������� ����������������������� !�!����!"#�$�%���&����'����%�����%�(&����&��)��������%��������*+�,&�����������-�����������������.-����&+
��������
/�����0+� !�!+�������/������+�.�����������������'�����/��������%� ������������'������������1��'�'+�/���� ������������ ���������+����������� ������������� ������������������� �������� �������������������������$2$+�32���+� ������+�1.45"�67"�7$$27��387"+
,&�������-������������'�����&�����������%���������������'����%������������%������������-��&� �������� %����� %������������� %���'�� )1*�� �� ��������� �&�� ���������������%� ��������������%�������1�����'�������'�����)117111*����������������&�����������������&�.-����&�4���&���%�������'�����������������%��������%����������%�����9�������)1:*+����������������8 6�%��������������-���������%����-&�������'������-�����������������
��������'���&����������'����%������������+�1���$�)$8+2�;*�������������������%�����������-����������������� 2�)8�+6�;*����������-������������������� 8�)�+!�;*�������������'������������������%���������%�������������&-����&�����������-��&�����������&��������'�������������� ������)�+6�;*� �������������'������������������%��������������&-��������������������������)1*+(������������� "����'������-��&��5.7� )11*���� 38�-��&�7�5.7�������� )111*�-���
�������+� 1� �&�� �5.� ��������1���������� ��������� �%������ �� �6� %������� )3 �;*�����������%������-��&����&�'�'��&�����'�������6�) 6�;*��������������%�����������'��&�����'�������'�������8�)�!;*+�1��&��7�5.��������&����������'�%�'����-����28�)36�;*�����) ��;*�����&����)$�;*��������������+���1����&�������������������'&���������������������������<���������������%���&�����������%��5.���������������������-&��&���������������������������������������������)11*������7�5.����������������%�����&��'������&���������'&��������)111*+1��-����� �&���������������%�����&���%��������������������&�'&�������������������� �
���'���������������&��������-�������-+�,&����������%��-����-��&��������%���&���������������������%�����������������%����'��������������)=3!;*+�,&���������%�����������������'��&��������'�%���������%����������������'������)1:*+
���� ����(��'��������������%�������������������������'������������������������������%�������1���5.�������������'�������'������7�5.����������%����������������&���%�������'���������������������������%��������%�����9������
������� ����!����� ��������"���#���������� ��#��������!� $������$���%�$�����!������������� ����!��&'()*+)��������!�������
>�0��&���/���� !�!
1..5��3$�73 !31.45�"�67"�7$$27��387"��#�#��#��#����7� �$!8�)&���#99��+��+��9������?��@��#�#��#��#����7� �$!8*

“I have walked that long road to freedom. I have tried not to
falter; I have made missteps along the way. But I have
discovered the secret that after climbing a great hill, one only
finds that there are many more hills to climb. I have taken a
moment.”
Nelson Mandela
To my family Sofia Maria Jacob Rose-Marie


List of Papers
This thesis is based on the following papers, which are referred to in the text by their Roman numerals.
I. Amini H, Antonsson P, Papadogiannakis N, Ericson K,
Pilo C, Eriksson L, Westgren M, Axelsson O. Comparison of ultrasound and autopsy findings in pregnancies terminated due to fetal anomalies. Acta Obstet Gynecol Scand. 2006; 85:1208-16.
II. Amini H, Axelsson O, Raiend M, Wikström J.
The Clinical Impact of Fetal Magnetic Resonance Imaging on Management of CNS Anomalies in the Second Trimester of Pregnancy. Submitted for publication.
III. Amini H, Wikström J, Ahlström H, Axelsson O.
The Clinical Impact of Fetal Magnetic Resonance Imaging on Management of Non-CNS Anomalies in the Second Trimester of Pregnancy. Manuscript.
IV. Amini H, Axelsson O, Ollars B, Annerén G. The Swedish
Birth Defects Registry: Ascertainment and Incidence of Spina Bifida and Cleft Lip/Palate.
Acta Obstet Gynecol Scand. 2009; 88:654-9.
Reprints were made with permission from the respective publishers.


Contents
Introduction...................................................................................................11 Second trimester ultrasound .....................................................................11
False negative and false positive ultrasound findings .........................12 Safety of ultrasound.............................................................................12
Magnetic Resonance Imaging ..................................................................13 Fetal Magnetic Resonance Imaging .........................................................13
Safety of fetal MRI ..............................................................................14 CNS anomalies.........................................................................................15 Psychological aspects of ultrasound and MRI .........................................16 Fetal autopsy ............................................................................................16 Surveillance of fetal anomalies ................................................................17
Aims..............................................................................................................18
Material and Methods ...................................................................................19 Study I ......................................................................................................19
Subjects................................................................................................19 Study design ........................................................................................19
Study II and III .........................................................................................20 Study populations ................................................................................20 Ultrasound and MRI examinations ......................................................20 Study design ........................................................................................21
Study IV ...................................................................................................22 Registries .............................................................................................22
The Swedish Birth Defects Registry (BDR) ...................................22 The Swedish Medical Birth Registry (MBR)..................................22 The Hospital Discharge Registry (HDR) ........................................22 The Committee for Forensic Psychiatry Social and Medical Legal Questions at the National Board of Health and Welfare (CFQ) .....22 The Qualitative Registry of Cleft Lip/Palate (QRC).......................22
Ethical Considerations..............................................................................23 Statistical Methods ...................................................................................23
Results...........................................................................................................24 Study I ......................................................................................................24 Study II.....................................................................................................27 Study III ...................................................................................................30

Body Mass Index......................................................................................33 Invasive procedures in study I-III ............................................................33 Study IV ...................................................................................................34
Discussion.....................................................................................................36 Study I ......................................................................................................36
Improvement in ultrasound diagnosis over time..................................36 Shortcomings of ultrasound.................................................................37 Types of anomalies ..............................................................................37 Fetal autopsy........................................................................................38
Study II and III .........................................................................................38 Classification .......................................................................................39 Benefit of fetal MRI in CNS anomalies...............................................39
Follow up ........................................................................................39 Neurosonography and 3-D ultrasound as alternatives?...................40
Non-CNS anomalies ............................................................................40 False positive ultrasound findings .......................................................42 Maternal obesity and oligohydramnios................................................42 Strength and limitation ........................................................................42
Study IV ...................................................................................................43 High ascertainment of birth defects in newborns ................................43 Low/unknown ascertainment of pregnancy terminations ....................43 Spina bifida..........................................................................................44
Folic acid.........................................................................................44 Incidences and the changes over time.............................................44 Comparison of incidence between and within countries.................44
Cleft lip/palate .....................................................................................45 Incidences and differences over time..............................................45 Ascertainment increased with severity of CLP...............................45
Conclusions...................................................................................................46
Clinical implications .....................................................................................47
Future Studies ...............................................................................................48
Sammanfattning på svenska (Summary in Swedish) ....................................49
Acknowledgements.......................................................................................53
References.....................................................................................................56

Abbreviations
AC Amniocentesis BDR The Swedish Birth Defects Registry BMI Body mass index CCAM Congenital cystic adenomatoid malformation CFQ The Committee for Forensic Psychiatry, Social and
Medical Legal Questions CHAOS Congenital high airway obstruction syndrome CI Confidence interval (95 %) CLaP Cleft lip and palate CLO Cleft lip only CNS Central nervous system CLP Cleft lip/palate CPO Cleft palate only CVS Chorionic villous sampling 2-D, 3-D Two-, Three-dimensional GA Gestational age (weeks) HDR The Swedish Hospital Discharge Registry ICD International Classification of Disease IUFD Intrauterine fetal death IUGR Intrauterine growth retardation MBR The Swedish Medical Birth Registry MI Mechanical index MRI Magnetic resonance imaging PROM Premature rupture of membranes SBU The Swedish Council on Technology Assessment in
Health Care SSFP Steady-state free precession SS-TSE Single-Shot Turbo Spin Echo TI Thermal index TRAP Twin reversed arterial perfusion UK United Kingdom VACTERL Vertebral-,anorectal-, cardiovascular-, trachea-,
esophageal-, renal-, and limb-anomalies QRC The Qualitative Registry of Cleft Lip/Palate


11
Introduction
Second trimester ultrasound Congenital anomalies are present in 2-4 % of newborns and are an important cause of fetal and neonatal mortality and morbidity.
In the late 1950s, the use of ultrasound was introduced for obstetrical and gynecological purposes by the Scottish obstetrician Ian Donald [1, 2]. In Sweden, Bertil Sundén in Lund was the first obstetrician to use ultrasound. His thesis, “On the diagnostic value of ultrasound in obstetrics and gynecology”, was published in 1964 and reported the first case of ultrasonographic diagnosis of anencephaly [3]. In 1972, the first termination of pregnancy due to fetal anomaly, was performed after ultrasound diagnosis of anencephaly and was reported in the Lancet by Campbell et al [4].
Malmö, in southern Sweden, was the first centre in Sweden to invite pregnant women to participate in an ultrasound examination. The benefits of ultrasound at that time were early detection of twins, improved estimation of gestational age and detection of intrauterine growth retardation in late pregnancy. In the 1990s, diagnosis of fetal anomalies became part of routine ultrasound in Sweden [5]. Since 1998, according to a recommendation from SBU, besides identifying twins and dating the pregnancy, detailed examination to detect fetal anomalies has been an important part of the routine ultrasound in the second trimester [5]. Virtually all pregnant women accept the offer of routine ultrasound.
The screening of fetal anomalies is preliminary performed by specially trained and educated midwives. When anomalies are found or suspected at the routine ultrasound, an expert obstetrician is called upon to make a final ultrasound diagnosis. Ultrasound technique and skill have improved and new methods such as 3-D imaging and colour Doppler have become useful. In a majority of cases of detected anomalies an invasive procedure is carried out in order to detect or rule out chromosomal aberrations.
Fetal medicine has appeared as subspecialty in obstetrics at University hospitals. The diagnostic work-up of fetal anomalies is a multi-disciplinary task [6]. Other experts, such as clinical geneticists, pediatric cardiologists, pediatric surgeons and pediatric neurologists may also be consulted. In some cases the women decide to terminate the pregnancy. The women’s decisions depend to a high degree on the information received concerning the diagnosis and the prognosis for the fetus. Correct antenatal information

12
about diagnosis and prognosis of fetal anomalies is of utmost importance for the woman and her partner when making a decision on termination or continuation of the pregnancy and for obstetricians to monitor the pregnancy and plan the delivery.
Despite the increasing rate of ultrasound examinations in pregnancy, there is no evidence for the use of more than one routine ultrasound during pregnancy [5].
False negative and false positive ultrasound findings There are two major problems with ultrasound diagnosis of fetal anomalies. False negative cases mean that detectable anomalies are not detected antenatally and are diagnosed only after birth. Apart from negative psychological effects for the woman and her partner, such cases also imply medical drawbacks for the management of the pregnancy, planning of the delivery and neonatal care [5, 7]. False positive cases mean that antenatally diagnosed anomalies are not verified at birth or after termination. Such cases are a major concern since termination of pregnancy might be performed when the fetus is either normal or has less severe anomalies than those diagnosed by ultrasound. There have been reports on such cases as well as on cases where the autopsy has given complementary information of substantial importance [8-16].
It is important that the quality of the organization and of the ultrasound examinations is ensured, for example by education and certification. Autopsy of all fetuses terminated because of anomalies detected by ultrasound is important for quality control. Today, we do not know if fetal autopsy is a clinical routine in all centres that diagnose fetal anomalies in Sweden.
Safety of ultrasound Diagnostic ultrasound, particularly Doppler examination, has a potentially harmful effect on the development of the fetus, especially the CNS, by thermal effects and cavitations [5, 17]. Thermal index (TI) and Mechanical index (MI) are indices on the ultrasound screen indicating the magnitude of heating and non-thermal effects. A TI of 1.0 indicates a risk of heating by 1° Celsius. The largest risk to damage biologic tissue by ultrasound waves is in the border layer between bone and soft tissue, as in the CNS. Heating is a risk especially when Doppler ultrasound is used. If ultrasound contrast medium consisting of microbubbles in the blood is not used, cavitation would probably not be found in the fetus.
There are two relatively large randomised studies in Norway [18] and Sweden [19] stating a significant association between ultrasound and left- handedness in boys indicating an effect of ultrasound on the fetal CNS. All

13
these scans were performed in the 1970-1980s. The ultrasound and especially Doppler ultrasound of today can give higher intensities and the exposure times are possibly longer. Therefore, caution is recommended and ultrasound should only be used when there is a medical indication. Ultrasound as a ”souvenir” is thus inappropriate [20].
Magnetic Resonance Imaging Nuclear magnetic resonance imaging was first described in 1946 as a physico-chemical phenomenon independently by Felix Bloch [21] and Edward M Purcell [22]. The finding that certain nuclei placed in a strong magnetic field could absorb and emit energy in the radio frequency range became a foundation of a new imaging modality. In 2003, Paul C. Lauterbur and Sir Peter Mansfield were awarded the Nobel price for their work in nuclear magnetic resonance imaging (NMRI) [23, 24]. Because of negative association of the word nuclear (nuclear weapon), NMRI became MRI.
The magnetic field used can be dangerous to persons with metallic implants or pacemakers. Claustrophobia is a relative contraindication for MRI examination. Subject motion during acquisition degrades image quality.
There are many ways to vary the acquisition technique in MRI resulting in different types of information. Examples include magnetic resonance angiography for the vascular system, functional MRI by monitoring deoxygenated haemoglobin for brain function and magnetic spectrometry to assess chemical and physical information about molecules [25].
The basic components of the MRI setup are static magnetic field, magnetic field gradients, and radio frequency pulses. Among the most interesting nuclei for MRI are 1H, 13C, 19F, 23Na and 31P with the proton 1H being the most commonly used, and the one used for morphological imaging. All of these nuclei occur naturally in the body.
Fetal Magnetic Resonance Imaging The use of MRI in pregnant woman was first described in 1983 [26]. Early studies of fetal MRI were limited by fetal motions [27, 28]. Maternal and fetal sedation were frequently needed to achieve motion-free fetal imaging. These included intravenous sedation of the pregnant woman with benzodiazepines and direct intramuscular injection to the fetus with pancuronium bromide [28-30]. The use of such drugs might cause health risks for the fetus and mother. Gradient-echo and turbo-spin-echo sequences were used to try to eliminate motion artefacts as far as possible. However, the images obtained using these sequences had limited clinical utility.

14
Nowadays, ultra-fast scanning techniques, such as single shot fast spin-echo sequences, allow for acquisition of images in 300-400 milliseconds. Images without movement artefacts can now be obtained without maternal or fetal sedation, either during breath-holding of the mother or using breathing synchronization [31]. Good fetal anatomic visualization is therefore usually achieved.
Fetal MRI as an adjunct to ultrasound is an established method in many countries for example in the USA and UK, but not yet in Sweden. MRI is an established method for evaluation of fetal anomalies mainly in the third trimester. MRI permits imaging in multiple planes, provides excellent soft-tissue contrast and has a large field of view. MRI is less dependent on maternal BMI and amniotic fluid for image quality than ultrasound.
Ultrasound nonetheless remains the primary screening modality for antenatal diagnosis because of its relative low cost, probable lack of harmful effects on the fetus and mother, and possibility of real time imaging, which allows dynamic assessment of the fetus.
Safety of fetal MRI MRI is a non-invasive procedure and does not involve ionizing radiation. The safety of fetal MRI has not been fully evaluated. At present, no harmful effects on the fetus have been identified following fetal MRI examinations, but it is recommended that exposure above 1.5 Tesla as well as during the first trimester should be avoided [32-38]. The safety committee of the society for MRI issued guidelines for patient safety [36] recommended that patients should be informed that, to date, there has been no indication that the use of MRI during pregnancy has produced deleterious effects; however, safety has not been proven.
The fetus imaged by MRI is exposed to a combination of three electromagnetic fields of varying strengths and frequencies; a static magnetic field, a radiofrequency field and a fast-switching gradient field. Exposure to the radiofrequency field causes tissue heating.
According to Health Production Agency (UK) the fetus is particularly sensitive to radiofrequency fields because normal pathways for heat loss in mammals are not available to the fetus [39]. In 2004 the International Commission of Non-Ionizing Radiation stated that there is a need to more precisely define the spatial deposition of radiofrequency energy during an MRI procedure and the corresponding temperature fields in the human body including modeling of the pregnant woman and fetus [40].
As with ultrasound, heating by MRI has a potential to cause biological tissue damage. Tissue heating is, however, most pronounced at the maternal body surface and should be negligible for the fetus [41].

15
Research is needed to develop better computer and animal exposure models of the pregnant woman to more accurately investigate the different field effects [42].
The possibility of teratogenic effects of fetal MRI at 1.5 Tesla was studied in two follow-up studies of children at 9 months of age in one study and up to 9 years of age in another study. They concluded that no harmful effects due to MRI were detected [43, 44]. There are, however, a small number of animal studies showing a possible teratogenic effect of MRI [45, 46]. Magin et al, showed no significant changes in fetal growth in animals exposed to either ultrasound or MRI. However, when both ultrasound and MRI were performed, the crown-rump length was reduced. A biological effect at sensitive stages of fetal development was thus concluded [46].
A less obvious concern is the potential risk of acoustic damage to the fetus due to loud noises generated by the MRI scanner coil, especially with echo planar imaging [47]. This damage is more a theoretical than a real concern [37, 48].
It is essential that the potential side effects of MRI be followed up in the future, possibly by register studies. For future information, it could be valuable to record fetal MRI in the maternal records and register this in the Medical Birth Registry (MBR). One concern is, however, that fetuses undergoing MRI are not healthy, in contrast to a vast majority of fetuses undergoing second trimester routine ultrasound examination.
CNS anomalies CNS anomalies are found in 35-48 % of terminated pregnancies due to non-chromosomal fetal anomalies detected by ultrasound [8, 10, 11, 16, 49]. This is most likely due to a relatively high sensitivity of routine ultrasound to detect such anomalies [12, 50, 51]. CNS anomalies are among the most common prenatally diagnosed anomalies [52-55]. Diagnosis of complex CNS anomalies by routine ultrasound is a challenge for obstetricians. However, the most common CNS diagnosis among terminated pregnancies is anencephaly (51 %) [56], which is relatively easy to diagnose by ultrasound. A sensitivity of almost 100 % for ultrasound diagnosis of anencephaly is a sign of quality in an organisation dealing with fetal anomaly diagnosis.
Because of the serious prognosis of many CNS anomalies a false negative diagnosis often has substantial consequences for the family and newborns. On the other hand, false positive cases might lead to unnecessary termination of pregnancies, which is a great concern.
Ultrasound evaluation of CNS anomalies is limited by ossification which makes it difficult to visualize the structures in the posterior fossa. Multiplane views of the CNS can be difficult to obtain with ultrasound due to the fetal

16
position in the pelvis. Moreover, the diagnostic accuracy of ultrasound is limited in some complex anomalies, such as microcephaly, neuronal migration anomalies, ischemic lesions, white matter diseases as well as when oligohydramniosis or maternal obesity are present [57, 58].
Fetal MRI provides multiplanar images and a detailed visualization of the CNS anatomy [59]. Fetal MRI might have additional diagnostic value where antenatal ultrasound is inconclusive or poses difficulties. Examples of such cases include agenesis of corpus callosum, posterior fossa cysts, cerebral clefts, migration disorders and cortical dysgenesis [31].
For the perinatal pathologist diagnosis of CNS anomalies such as hydrocephalus or posterior fossa cysts is a challenge despite improvements in technique. MRI could be helpful in improving ante- and postnatal diagnosis of CNS anomalies [60, 61].
MRI has been utilized to complement ultrasound in cases of suspected CNS anomalies [62], but relatively few studies on the diagnostic value of fetal MRI in non-CNS anomalies have been published.
Psychological aspects of ultrasound and MRI Routine ultrasound is attractive to women [51] mainly because it provides the parent-to-be with early visual confirmation and reassurance of fetal well-being. On the other hand, false negative diagnoses might have negative long term effects on the woman’s mental health [63].
There are reports on psychological reactions in women undergoing fetal MRI [64]. Distressing factors can be the duration of the examination, anxiety for the fetus, the noise level and physical restraint. Pre-imaging information by the referring physician has been reported to influence the woman’s experience of MRI [65]; as is shown for ultrasound examinations [66].
Apart from the general need for psychological support to women undergoing prenatal examinations, there may be a need for additional support to women undergoing fetal MRI. Further research should focus on the effect of pre-imaging information on women’s experiences from fetal MRI examinations [64].
Fetal autopsy Perinatal pathology is a subspecialty first described in a lecture on antenatal pathology and teratology in Edinburgh in 1900 [67]. In Sweden perinatal pathologists are available at some University hospitals but seldom at secondary or primary units. High autopsy rates have been considered an indicator of high hospital standards [68].

17
The practice of perinatal pathology varies widely even between university hospitals, and in Sweden there is no national policy of centralization. The quality of perinatal autopsy varies and at many hospitals pathologists with no special training or interest in perinatal pathology perform autopsies [69]. It is important to realize that an inadequately performed autopsy can be misleading [70].
Perinatal pathologists as well as clinical geneticists and radiologists are important members of the fetal medicine team. Fetal autopsy by a perinatal pathologist is an important part of quality control of antenatal diagnosis of fetal anomalies [10, 11, 13, 53-55, 71]. Obstetricians and others in the fetal medicine team receive feed-back, which is of importance for quality assurance.
Surveillance of fetal anomalies The need for a surveillance registry of congenital anomalies became clear
during the period of the thalidomide-induced embryopathies in 1958-1962 [72]. The information on the Swedish incidence of congenital anomalies originates from the official statistics of the Swedish Birth Defects Registry (BDR), established in 1964. Worldwide, registries of congenital anomalies vary in quality and ascertainment levels [73, 74]. A report from the UK showed that the surveillance of congenital anomalies was inadequate, since the ascertainment in the national registry was low and non-uniform and since no data existed from pregnancy terminations performed on the grounds of prenatal diagnosis of fetal anomalies [74].
Since January 1, 1999, pregnancy terminations carried out because of fetal anomalies have also been reported to the BDR [75]. In Sweden reporting of newborns with birth defects is compulsory, while that of terminated pregnancies is only recommended. Having a good registry for newborns only is not a guarantee for surveillance, since an increase of antenatally diagnosed anomalies lead to an increased number of pregnancy terminations.

18
Aims
The overall aims of this thesis were to study the accuracy of ultrasound for diagnosis of structural fetal anomalies, to evaluate the additional value of second trimester fetal MRI on pregnancy management, and to estimate the ascertainment in the Swedish Birth Defects Registry and the incidence of two typical congenital anomalies, spina bifida and cleft lip/palate.
The specific aims of the studies were:
To evaluate the diagnostic accuracy of second trimester ultrasound by comparing the ultrasound diagnosis with autopsy findings in pregnancies terminated after ultrasound detection of fetal anomalies and to study the quality of antenatal ultrasound over a 12-year period (study I). To evaluate the additional information of second trimester MRI compared to ultrasound in fetuses with identified or suspected CNS anomalies (study II) and in fetuses with non-CNS anomalies (study III) and to study the clinical impact of the MRI information on pregnancy management. To assess the ascertainment in the Swedish Birth Defects Registry as well as true incidence of spina bifida and cleft lip/palate in newborns and fetuses from pregnancy terminations (study IV).

19
Material and Methods
Study I All fetal autopsies in Uppsala and southern Stockholm between 1992 and 2003 (12 years) were identified through the Departments of Pathology at Karolinska University Hospital Huddinge, Uppsala University Hospital and during the period 1992-1996 also at South General Hospital in Stockholm. Only autopsies of fetuses from pregnancies terminated because of ultrasound diagnosis of anomalies were included. Terminations primarily carried out for chromosomal aberrations were excluded. Cases referred from other hospitals were included if the mother had been examined antenatally at any of the three centres.
Subjects The final number of cases included was 328, of which 139 came from Karolinska University Hospital, Huddinge, 90 from South General Hospital and 99 from Uppsala University Hospital. Data on birth rates were collected from the MBR.
Study design The findings at the last ultrasound report before termination were used for comparison with the autopsy reports. The comparisons were performed, with minor modifications, as proposed by Brand et al [8] and the results were allocated into four categories:
A. Ultrasound findings exactly matched the postnatal findings. B. The main ultrasound findings were confirmed postnatally but other anomalies were either misdiagnosed or not detected at ultrasound. C. Ultrasound findings were not confirmed but the postnatal findings were at least as severe as the antenatal ones. D. Postnatal findings did not confirm the ultrasound findings, which meant that the information given to the woman/couple on the severity and prognosis of the fetal condition was incorrect. The postnatal findings were less severe than the antenatal ultrasound diagnosis.

20
One of the authors (HA) decided primarily in which category, A-D, each case belonged. Independently of HA the cases managed in Stockholm were reviewed by a junior pathologist from Uppsala (KE) and the cases managed in Uppsala by a junior pathologist from Stockholm (PA). Any differences of opinion between HA/KE and HA/PA were resolved through a joint discussion between two senior authors, a perinatal pathologist and an experienced obstetrician. For the Uppsala cases, MW and NP made the decisions, and for the Stockholm cases OA and LE. Finally, all D cases were discussed by all the authors to reach consensus.
Study II and III These studies were performed prospectively at the Fetal Medicine Unit and Department of Radiology at Uppsala University Hospital, and lasted from January 2004 to November 2007 (study II) and November 2003 to June 2007 (study III). Pregnant women where the second trimester ultrasound raised suspicion of a CNS (study II) or non-CNS (study III) anomaly were informed both verbally and by letter about the study and asked if they were willing to participate. The MRI examination was planned to be performed within three days after ultrasound.
Study populations The pregnant women included were recruited from Uppsala County or as referrals from other hospitals in the region. The mean age of the 29 women included in CNS study was 30 years (range17-42). The mean gestational age (GA) at the last ultrasound before MRI was 18+1 weeks (range 15+4-20+2). The mean interval between ultrasound and MRI was 1.6 days (range 0-7). In 23 (79 %) cases MRI was performed within three days (study II).
The mean age of the 63 women included in the non-CNS study was 29.2 years (range 19-38). The mean gestational age at the last ultrasound before MRI was 18+1 weeks (range 13+0-21+5). The mean interval between ultrasound and MRI was 2.6 days (range 0-15). In 42 (67 %) cases MRI was performed within three days (study III).
The number of pregnancies in which CNS and non-CNS anomalies were demonstrated at the Fetal Medicine Unit during the study period was 57 and 166 of which 29 (51 %) and 63 (38 %) were included in each study, respectively.
Ultrasound and MRI examinations Ultrasound was performed by obstetricians with special knowledge in fetal medicine using commercially available real-time machines: Acuson Sequoia
21
512 (Acuson, Mountain View CA, UAS) or Siemens sonoline SI-400 (Erlangen Germany) with a 3.5 or 4 MHZ transabdominal convex probe.
The radiologist was informed about the ultrasound findings before the MRI examination. The responsible obstetricians were informed about the MRI findings and continued the clinical management.
The MRI examinations were performed on a 1.5 T scanner (Gyroscan ACS Intera, Philips Medical Systems, Best, The Netherlands) using a pelvic phased array coil. T2-weighted images were acquired in the three main planes of the fetus (sagittal, coronal, and axial) using a Single-Shot Turbo Spin Echo (SS-TSE) sequence with a slice thickness of 3 mm. In addition, a T1-weighted sequence was performed in the axial plane with a slice thickness of 5 mm. Imaging was performed during free breathing with respiratory gating to avoid artefacts. In addition, some women were also examined with 2D- or 3D- steady-state free precession (SSFP) sequences (Balanced-fast field echo (FFE), Philips Medical Systems, Best, The Netherlands) and/or with single slice dynamic SS-TSE or SSFP-sequences.
Study design If more than one ultrasound examination had been performed before the MRI, the last ultrasound was used for the review.
The classification was made in consensus between the authors HA, JW and OA, and allocated into three categories:
I MRI provided no additional information. II MRI provided additional information but did not change the
pregnancy management. III MRI provided additional information which changed the
pregnancy management.
The following BMI (kg/m2) categories were used: 18.5-24.9 (normal weight), 25-29.9 (grade 1 overweight, herein referred to as overweight), 30-39.9 (grade 2 overweight or obesity) and � 40 (grade 3 overweight or morbid obesity) [76].

22
Study IV The study period lasted from January 1, 1999 to December 31, 2004.
Registries The Swedish Birth Defects Registry (BDR) The BDR was established in 1964. It contains data on congenital anomalies observed during the first year of life. Since January 1, 1999, the BDR has also registered pregnancies terminated because of fetal anomalies. The reporting of anomalies in newborns is compulsory, whereas reporting of fetal anomalies from termination of pregnancies is only recommended. In cases of newborns, but not of terminated pregnancies, the mother’s personal identification number is registered. Fetal anomalies in stillbirths after gestational week 22 are included. Fetal anomalies in spontaneous abortions before week 22 are not registered. Twice a year, a record linkage is carried out between the BDR and MBR.
The Swedish Medical Birth Registry (MBR) The MBR contains prospectively collected information on more than 99 % of all births in Sweden since 1973, but nothing on terminated pregnancies [77, 78]. This register includes data on maternal demographics, reproductive history and complications during pregnancy, delivery and the post-partum period, as well as neonatal diagnoses. The information is provided through antenatal, obstetrical and neonatal records, which is filled in by midwives and physicians. The diagnoses are set according to ICD-10.
The Hospital Discharge Registry (HDR) The HDR includes data on each hospital admission, the main discharge diagnosis, and secondary diagnoses. The diagnoses are classified and recorded by the treating physician according to ICD-10, as above. All recorded diagnoses are forwarded by computer medium to HDR. The register has provided nationwide coverage of diagnoses in inpatient care since 1987 and includes care in both adult and pediatric clinics.
The Committee for Forensic Psychiatry Social and Medical Legal Questions at the National Board of Health and Welfare (CFQ) After 18 completed weeks, pregnancy terminations are allowed only after permission from this committee. Permission is seldom given after 22 weeks of gestation. The mother’s personal identification number is not registered.
The Qualitative Registry of Cleft Lip/Palate (QRC) The QRC was established in 1999 at Uppsala University Hospital, Uppsala, Sweden. It includes all children born in 1999 or later with CLP, which
23
means cleft palate without cleft lip and cleft lip with or without cleft palate, who have received care at six centres in Sweden. The diagnosis codes are set according to ICD-10 by the responsible physicians. By combining data from the BDR, MBR, HDR and QRC for cleft lip/palate and from BDR, MBR, HDR and CFQ for spina bifida, we estimated the level of ascertainment in the BDR and the incidence rates.
Ethical Considerations Study I was approved by the Ethics Committee of the Medical Faculties at Uppsala University and Karolinska Institute. Study II, III and IV were approved by the Ethics Committee of the Medical Faculty at Uppsala University.
Statistical Methods A linear regression test was used to see if the number of cases changed over time. Fisher Exact Test was used to compare A, B, C and D cases during the time periods (study I) and to see if the ascertainment of CLP increased with the type and severity of the anomaly (study IV); p <0.05 was considered as statistically significant. The confidence interval (CI) was calculated at the level of 95 %.

24
Results
Study I The mean gestational age at the last ultrasound examination was 17+3 weeks (range 11-24 weeks). Of the 328 cases, 175 (53.4 %) were in category A, 124 (37.8 %) in B, 23 (7.0 %) in C and six (1.8 %) in D. The final diagnoses based on autopsy and cytogenetics are listed in Table 1.
Category A can be regarded as technically correct and categories A-C as clinically correct at least in the context of antenatal decision making. Thus, the agreement from the technical aspect was 53.4 % and from the clinical aspect 98.2 %. In 299 cases (91.2 %) the ultrasound findings either exactly matched the postnatal findings (category A) or were mainly confirmed (category B).
CNS anomalies were the most common anomalies, leading to termination of pregnancies in 114 cases (34.8 %), the majority being neural tube defects. In 45 cases (13.7 %) the main diagnosis established was based on chromosomal aberrations. Turner’s syndrome was the most common finding in this group (14 cases), followed by Down syndrome (10 cases). Cardiac anomalies were the main findings in 12 cases (3. 7 %). Eleven of these were seen by a pediatric cardiologist.
In category B fetal autopsy provided 141 additional findings that were not detected by ultrasound. Major cardiac or vessel anomalies were not observed by ultrasound in 26 B cases. Minor skeletal anomalies such as syndactyly, polydactyly, radial aplasia, scoliosis, and nasal or orbital anomalies were not recorded in 20 B cases. Cleft lip/palate was not recorded in 15 B cases (Fig 1) and bowel malrotation was not recorded in 11 cases. In 28 B cases autopsy provided a syndrome diagnosis. Refining of the diagnosis was noted in 12 B cases. In 19 B cases only the main diagnosis was confirmed at autopsy but not the other diagnoses. Ultrasound diagnoses not verified at autopsy were hydrocephalus (five cases), hygroma/hydrops (five cases), ventricular septal defect (three cases), gastroschisis/omphalocoele (two cases), hydronephrosis (two cases), corpus callosum agenesis (one case) and vertebral anomaly (one case).

25
Eight of 23 cases in category C (7.0 %) had chromosomal aberrations and six had complex anomalies as the main diagnosis. In four cases of category C fetal autopsy provided a syndrome diagnosis.
Six cases were allocated to category D. The ultrasound diagnoses, but not the final diagnoses, were hydrocephalus in two cases, encephalocele in one case, anhydramnios in two cases and omphalocele in one case.
Figure 1. Autopsy images of a fetus with omphalocele and cleft lip/palate. This case was judged to be a B case because ultrasound detected only the omphalocele.
The number of terminated pregnancies because of ultrasonographically diagnosed fetal anomalies was 1.66 per 1000 births in the first period and 2.96 in the second period. In the first period the number of A, B, C and D cases were 69 (61.0 %), 38 (33.6 %), three (2.7 %) and three (2.7 %), compared to 105 (48.8 %), 87 (40.5 %), 20 (9.3 %) and three (1.4 %), respectively, in the second period (Fig 2). The decrease of A cases as well as the increase of C cases was significant (p=0.04 and 0.02, respectively). The decrease of D cases and the increase of B cases were not significant (p=0.4 and 0.2, respectively). The allocation of cases to the A-D categories differed significantly (p= 0.03) between the two time periods.

26
Table 1. The final diagnosis based on autopsy and cytogenetics
Diagnosis
number Diagnosis number
1. Cerebrospinal 114 (34.8 %) 7. Complex anomalies / defined syndromes
45 (13.7 %)
Spina bifida including Arnold- Chiaris malformation
30 Multiple complex anomalies 10
Anencephaly 53 Amniotic band 13 Holoprosencephaly 7 Sirenomelia 1 Isolated hydrocephalus 15 Meckel-Gruber syndrome 5 Occipital meningocele 3 Body-wall complex 2 Occipital encephalocele 1 Jeune´s syndrome 1 Dandy-Walker cyst 4 Beckwith-Wiedemann syndrome 1 Microcephaly 1 Majewski syndrome 1 Acardiac syndrome 1 2. Pulmonary 7 (2.1 %) Prune-belly syndrome 3 Diaphragmatic hernia 6 Jarcho-Levin syndrome/ 2 Hyperlobation 1 spondylocostal dystosis CCAM type 2 3 3. Cardiac 12 (3.7 %) Lethal pterygium syndrome 2 Complex defect 6 Jeune´s syndrome 1 Hypoplastic left heart 4 Fallot’s tetralogy 1 8. Chromosomal 45 (13.7 %) Atresia of descending aorta and arch 1 Trisomy 21 10 Trisomy 18 12 4. Gastrointestinal 12 (3.7 %) Trisomy 13 5 Omphalocele 9 Tetrasomy 12 1 Gastroschisis 3 Turner’s syndrome 14 Triploidy 3 5. Renal 43 (13.1 %)
Bilateral renal agenesis 7 9. Tumour 1 (0.3 %) Bilateral dysplastic kidney 13 Sacrococcygeal teratoma 1 Unilateral renal agenesis & dysplastic kidney
6
Infantile polycystic disease 6 10. Twin-related 1 (0.3 %) Outflow obstruction 9 Conjoined twins 1
Complex renal anomaly 1 Nephrotic syndrome of Finnish type 1 11. Miscellaneous 24 (7.3 %) Hydrops/ cystic hygroma of
unknown aetiology
17
6. Musculoskeletal 24 (7.3 %) Severe oligohydramnios of unknown etiology
5
Severe phocoemelia, osteochondrodysplasy
6 Hydrothorax 1
Achondrogenesis 4 Subcutaneous oedema 1 Osteogenesis imperfecta 3
Thanatorphoric dwarf 4 Campomelic dysplasia 4 Diastrophic dysplasia 2
Radial aplasia/humeral hypoplasia 1

27
010203040506070
Firstperiod
Secondperiod
Wholeperiod
ABCD
Figure 2. The percentages of cases of categories A, B, C and D during the first (1992-1997), second (1998-2003) and whole (1992-2003) study period. The number of cases in the first and second period were 113 (34.5 %) and 215 (65.5 %), respectively. The decrease of A and the increase of C cases was statistically significant.
Study II In total, 29 cases were included. All MRI examinations were assessable. In 18 fetuses (62 %) MRI provided no additional information. The ultrasound findings were verified by MRI in all these cases. In 8 fetuses (28 %) MRI provided additional information but did not change the management and in 3 fetuses (10%), MRI provided additional information that changed the management.
Of the 29 pregnancies 19 (66 %) were terminated, two (7 %) ended as IUFD:s, one (3 %) as spontaneous abortion and seven (24 %) as births. Fetal autopsy was performed in 16 (84 %) of the terminated pregnancies, one of the IUFD:s and in the case of spontaneous abortion. In one case the fetal autopsy was inconclusive since the posterior fossa contents were not possible to assess because of autolysis. A final diagnosis of a Dandy-Walker anomaly was assigned to this case based on the MRI findings (Fig. 3).
All four cases of isolated hydrocephalus belonged to category I. Myelomeningocele with dilated ventricles was the most common final diagnosis followed by holoprosencephaly (Table 2).
Fetal autopsy provided additional non-CNS information in many cases.

28
a b
c d Figure 3. A case in category II. Ultrasound suspected a dilated cisterna magna (a, b) MRI diagnosed a Dandy-Walker anomaly (c, d), with widely splayed cerebellar peduncles (arrows in c) and upward rotation of the vermis (arrow in d). Fetal autopsy was inconclusive due to severe autolysis.
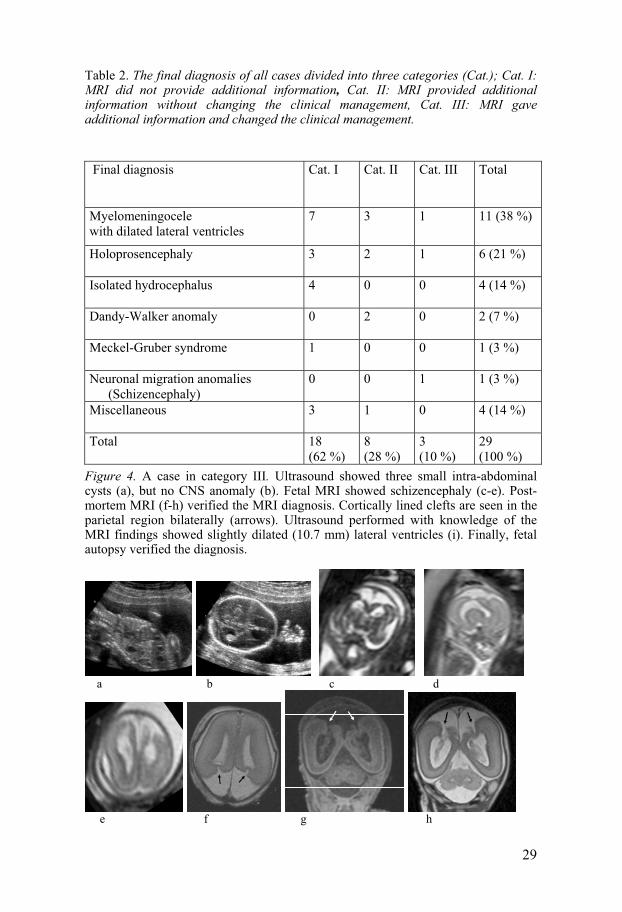
In two out of three cases in category III ultrasound had poor resolution due to maternal obesity. In the first case the MRI diagnosis (dilation of the lateral ventricles, suspected herniation of the cerebellum into the foramen magnum and suspected lumbar bony defect) was confirmed by fetal autopsy. In the second case the decision for termination of pregnancy was made before the karyotype was known. Ultrasound had difficulties visualizing the brain structure supratentorially, the woman was obese. MRI showed holo-prosencephaly. No fetal autopsy was performed. In the third case ultrasound found intra-abdominal cysts at GA 17+6 and 20+1. The woman had normal weight. The MRI examination revealed schizencephaly, which led to a decision to terminate the pregnancy. A repeated ultrasound performed with knowledge of the MRI findings showed slightly dilated lateral ventricles. Fetal autopsy and post-mortem MRI confirmed the in utero MRI diagnosis (Fig 4)
29
Table 2. The final diagnosis of all cases divided into three categories (Cat.); Cat. I: MRI did not provide additional information, Cat. II: MRI provided additional information without changing the clinical management, Cat. III: MRI gave additional information and changed the clinical management.
Final diagnosis
Cat. I Cat. II Cat. III Total
Myelomeningocele with dilated lateral ventricles
7 3 1 11 (38 %)
Holoprosencephaly
3 2 1 6 (21 %)
Isolated hydrocephalus
4 0 0 4 (14 %)
Dandy-Walker anomaly
0 2 0 2 (7 %)
Meckel-Gruber syndrome
1 0 0 1 (3 %)
Neuronal migration anomalies (Schizencephaly)
0 0 1 1 (3 %)
Miscellaneous
3 1 0 4 (14 %)
Total
18 (62 %)
8 (28 %)
3 (10 %)
29 (100 %)
Figure 4. A case in category III. Ultrasound showed three small intra-abdominal cysts (a), but no CNS anomaly (b). Fetal MRI showed schizencephaly (c-e). Post- mortem MRI (f-h) verified the MRI diagnosis. Cortically lined clefts are seen in the parietal region bilaterally (arrows). Ultrasound performed with knowledge of the MRI findings showed slightly dilated (10.7 mm) lateral ventricles (i). Finally, fetal autopsy verified the diagnosis.
a b c d
e f g h

30
i
Study III MRI examinations of all 63 cases were assessable. In 43 (68 %) fetuses MRI provided no additional information. In 17 (27 %) fetuses MRI provided additional information without affecting the management and in three (5 %) fetuses MRI provided additional information that changed the management.
The 63 pregnancies resulted in 36 (57 %) births, 23 (36 %) terminations, three (5 %) IUFD: s and one (2 %) missed abortion. There were no births in category III.
Aside from two cases showing chromosomal aberrations and one case of bilateral renal agenesis, fetal autopsy was performed in all terminated pregnancies, IUFD: s and the missed abortion case. One postnatal death due to asphyxia was not followed up by autopsy. Fetal autopsy provided additional diagnostic information in many cases.
Oligohydramnios was present in 13 (21 %) cases, of which eight were in category I, two in category II and three in category III. The causes leading to oligohydramnios were bilateral renal agenesis in three, dysplastic kidneys in three, VACTERL syndrome (with a fistula between the urinary bladder and rectum) in one, Meckel-Gruber syndrome in one, PROM in three and IUGR in two cases. All three cases in category III had oligohydramnios (Fig 5).
a b c d Figure 5. A case in category III. Ultrasound (a, b) showed anhydramnios and suspected enlarged and hyperechogenic kidneys (b). Fetal MRI (c, d) showed normal kidneys (arrows), which was verified by fetal autopsy after missed abortion. The anhydramnios was probably due to PROM. The woman was obese.

31
Left-sided diaphragmatic hernia was present in six cases, all in category II (Fig 6). CHAOS in category I (Fig 7) and CCAM in category II were two other thoracic anomalies. All cases with musculoskeletal or twin-related diagnoses belonged to category I. The most common final diagnosis was a urinary tract anomaly (Table 3).
In seven (11 %) cases the finding of a fetal anomaly by ultrasound or MRI was not verified postnatally. Nuchal oedema or neck hygroma diagnosed by MRI and ultrasound could not be found postnatally in two of three cases. Intra-abdominal cystic lesions were observed postnatally only in one of two cases. Abdominal ascites observed at ultrasound at 16 weeks GA was not verified by MRI five days later, by ultrasound four weeks later or postnatally. The finding of dilated renal pelvises by ultrasound and MRI was not verified postnatally in three cases. Ultrasound performed in the third trimester showed no renal pelvic dilation in two of these cases and only discrete dilation in one.
a b c d Figure 6. A case in category II. Ultrasound (a, b) showed left-sided diaphragmatic hernia containing stomach and bowels. A pediatric cardiologist diagnosed a hypoplastic left heart. MRI (c, d) showed left-sided diaphragmatic hernia containing stomach (filled arrow), bowels and left liver lobe (unfilled arrow). The volume of the left lung was approximately a third of the right one. The pregnancy was terminated. Fetal autopsy verified the cardiac anomaly and the MRI findings concerning the diaphragmatic hernia.
Besides the 63 cases in study III, there were 11 cases in study II that also had non-CNS anomalies. Two cases in study III had also CNS anomalies, but the main diagnoses where MRI added information or changed the management were diaphragmatic hernia and oligohydramnios (Meckel-Gruber), respectively.

32
Table 3. The final diagnosis of all cases divided into the three categories (Cat.); Cat. I: MRI did not provide additional information, Cat. II: MRI provided additional information without changing the clinical management, Cat. III: MRI provided additional information and changed the clinical management
Final diagnosis
Cat. I Cat. II Cat. III Total
1. Thoracic
1 7 0 8 (13 %)
Diaphragmatic hernia 0 6 0 6 CHAOS 1 0 0 1 CCAM 0 1 0 1 2. Renal/Urinary
13 3 1 17 (27 %)
Outflow obstruction 6 2 0 8 Open urachus 1 0 0 1 Unilateral multicystic kidney 2 0 0 2 Bilateral renal agenesis (oligohydramnios)
2 0 1 3
Dysplastic kidneys (oligohydramnios)
2 1 0 3
3. VACTERL syndrome (oligohydramnios)
1 0 0 1 (1.7 %)
4. Meckel-Gruber syndrome (oligohydramnios)
0 0 1 1 (1.7 %)
4. Oligohydramnios without renal anomalies
3 1 1 5 (8%)
5. Gastrointestinal
8 2 0 10 (16 %)
Gastroschisis 5 0 0 5 Omphalocele 3 1 0 4 Anal atresia 0 1 0 1 6. Musculoskeletal
7 0 0 7 (11 %)
Diastrophic dysplasia 1 0 0 1 Thanatorphoric dwarf 2 0 0 2 Bilateral clubfeet 2 0 0 2 Tibial aplasia 1 0 0 1 Radial aplasia 1 0 0 1 7. Sacrococcygeal teratoma 0 1 0 1 (1.6 %) 8. Twin-related 2 0 0 2 (3 %) 9. Miscellaneous 8 3 0 11 (17 %) Total
43 (68 %)
17 (27 %)
3 (5 %)
63 (100 %)
33
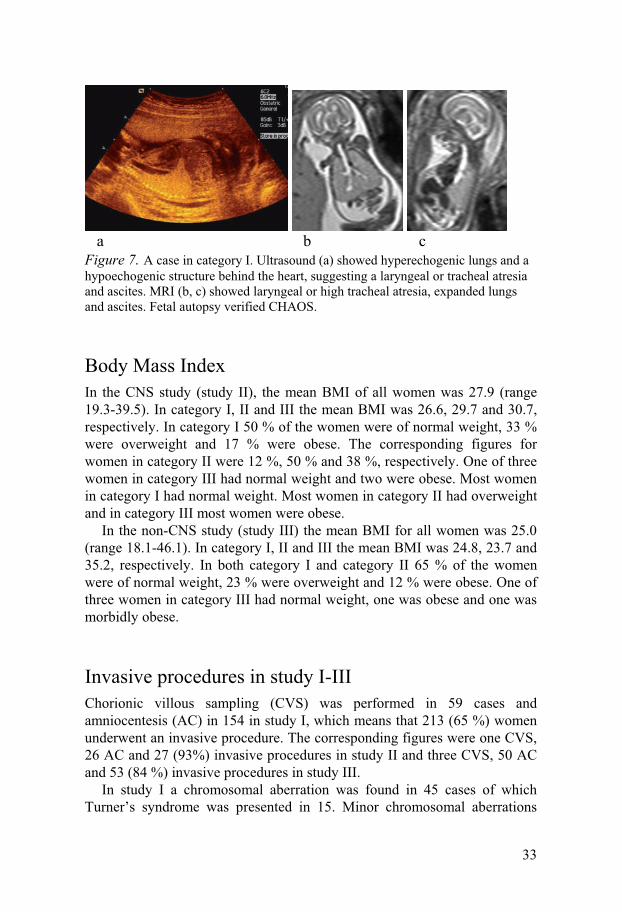
a b c Figure 7. A case in category I. Ultrasound (a) showed hyperechogenic lungs and a hypoechogenic structure behind the heart, suggesting a laryngeal or tracheal atresia and ascites. MRI (b, c) showed laryngeal or high tracheal atresia, expanded lungs and ascites. Fetal autopsy verified CHAOS.
Body Mass Index In the CNS study (study II), the mean BMI of all women was 27.9 (range 19.3-39.5). In category I, II and III the mean BMI was 26.6, 29.7 and 30.7, respectively. In category I 50 % of the women were of normal weight, 33 % were overweight and 17 % were obese. The corresponding figures for women in category II were 12 %, 50 % and 38 %, respectively. One of three women in category III had normal weight and two were obese. Most women in category I had normal weight. Most women in category II had overweight and in category III most women were obese.
In the non-CNS study (study III) the mean BMI for all women was 25.0 (range 18.1-46.1). In category I, II and III the mean BMI was 24.8, 23.7 and 35.2, respectively. In both category I and category II 65 % of the women were of normal weight, 23 % were overweight and 12 % were obese. One of three women in category III had normal weight, one was obese and one was morbidly obese.
Invasive procedures in study I-III Chorionic villous sampling (CVS) was performed in 59 cases and amniocentesis (AC) in 154 in study I, which means that 213 (65 %) women underwent an invasive procedure. The corresponding figures were one CVS, 26 AC and 27 (93%) invasive procedures in study II and three CVS, 50 AC and 53 (84 %) invasive procedures in study III.
In study I a chromosomal aberration was found in 45 cases of which Turner’s syndrome was presented in 15. Minor chromosomal aberrations

34
were detected in 12 cases, including inversion, balanced inversion, and partial trisomy de novo and long arm 11. These 12 cases were classified according to the main structural anomaly diagnosed (Table 1).
In study II a normal karyotype was found in 20 cases, trisomy 18 in four, trisomy 13 in two and a deletion of chromosome seven [46XY, del(7)(q32)] in one case.
In study III a normal karyotype was found in 49 cases, trisomy 18 in three and a deletion of chromosome seven [46XY, del(7)(q32)] in one case.
Study IV The number of newborns with spina bifida reported to the BDR during the period 1999-2004 was 108. After record linkage between the BDR and MBR, this number increased to 129. Another 8 cases were retrieved from HDR, making the total number 137. This corresponds to an incidence of spina bifida in newborns of 2.41/10,000 births (CI: 2.01 to 2.82). Seventy-nine percent of the cases were reported to the BDR. After record linkage between the BDR and MBR, this figure increased to 94 %.
The number of terminated pregnancies showing spina bifida (Fig 8) registered in the BDR was 155 of which 46 were performed after 18 weeks. Another 17 terminated pregnancies after 18 weeks were retrieved from the CFQ, making the total number of late terminated pregnancies showing spina bifida 63. Thus, 73 % of the late terminated pregnancies were reported to the BDR. The ascertainment of spina bifida in pregnancy terminations before 18 weeks can not be estimated.
The estimated incidence of spina bifida in pregnancy terminations was 3.03/10,000 births (CI 2.58 to 3.48). Seventy percent (109/155) of the terminated pregnancies with spina bifida reported to BDR occurred before the 18th week of gestation.
Since the data from the QRC and HDR were not available for the period 2003-2004, the complete evaluation of CLP was only possible for the years 1999-2002. The number of newborns reported to the BDR in 1999-2002 with any kind of CLP was 542, corresponding to a reported incidence of 14.76/10,000 births. After record linkage between the BDR and MBR, the number of cases increased to 605. Another 90 cases were retrieved from the QRC and HDR registries, making the total number 695, which corresponds to an incidence of 18.92/10,000, births (CI: 17.52 to 20.33). Seventy-eight percent of the cases were reported to the BDR. This figure increased to 87 % after record linkage with the MBR.
The number of terminated pregnancies with cleft lip/palate in BDR was 43, giving an incidence of 1.17/10,000 births (CI: 0.82 to 1.52). Except for one pregnancy, all pregnancy terminations with CLP were combined with

35
other multiple anomalies/syndromes. The ascertainment of terminated pregnancies with CLP could not be estimated.
Figure 8. An autopsy image of a fetus terminated in the second trimester because of spina bifida.
The sub-categories of CLP consisted of cleft palate only (CPO; 39 %), cleft lip only (CLO; 26 %) and cleft lip and palate (CLaP; 35 %). The ascertainments of these sub-categories in the BDR were 75 %, 74 % and 84 %, respectively. These figures increased to 85 %, 84 % and 91 % after record linkage with the MBR. The ascertainment was statistically higher in CLaP than in CLO and CPO (P 0.03 and 0.03, respectively). There was no difference in ascertainment between CLO and CPO.
36
Discussion
Study I Improvement in ultrasound diagnosis over time During the study period an increasing number of births took place in Sweden. This could only partly explain the increment of cases in the second period. Thus, improvements in ultrasound equipment and skills seem to be the main reasons that the number of pregnancies terminated as a result of ultrasound diagnosis of anomalies was almost twice as large in the second six-year period as in the first six-year period (215 vs. 113 cases). This increase is in agreement with the results from a previous study [9].
The significant decrease in A cases during the second period is most probably an effect of the improved quality of fetal autopsy. A contributing factor could be the establishment of the centre of perinatal pathology in Stockholm 1996. The significant increase in C cases in the second period might also be due to this improved service in perinatal pathology. The number of D cases (the genuine false positive cases) decreased from 3/113 (2.7 %) in the first period to 3/215 (1.4 %) in the second period. This may reflect an improved organisation of the Fetal Medicine Units as a consequence of the SBU report in 1998 [5]. The existence of D cases indicates, however, that there is room for further improvement.
Our way of classifying cases as A, B, C or D is subjective. This is illustrated by the 30 % lack of concordance between the observers. To minimise bias, cases from Stockholm with primary disagreement were finally classified by senior authors from Uppsala, and the corresponding Uppsala cases by senior authors from Stockholm. The recorded lack of concordance is substantially higher (30 %) than that found by Brand (4.2 %), [8]. A large majority of the disconcordant cases were, however, moved one step only and the number of D cases was rather constant, varying from six to eight.
Only a few studies have been published on this subject [8, 79]. Our study included three rather large hospitals with obstetricians with a special knowledge in antenatal diagnostics. The strength is the large number of cases included and the fact that the classifications were made by both obstetricians and pathologists. A caution should be issued on how our results
37
could be generalised as valid to other types of hospital with different equipment, training and routines.
The percentage of genuine false positive ultrasound findings in previous studies was 0.5 (2 cases) reported by Brand et al [8], 6.5 % (10 cases) reported by Weston et al [10], 2.7 % (5 cases) reported by Julian-Reynier et al [13] and 1.6 % (3 cases) reported by Tennstedt et al [12]. The diagnostic spectrum of false positive cases in three studies [10, 12, 13] is similar to that found by us. It seems, however, as if none of their cases was terminated on the grounds of suboptimal information.
Isaksen et al [49, 80] have published reports on diagnostic accuracy concerning CNS and renal anomalies. In contrast to our results they found no genuine false positive cases. This divergence might be due to differences in the quality of the antenatal diagnosis and/or autopsy, as well as to differences in the way of classifying the cases.
Shortcomings of ultrasound Two of our six cases in category D had severe oligo- or anhydramnios. It is a well-known fact that ultrasound examination in such cases is a challenge, because of the difficulty in attaining images of good quality. The three main causes for oligohydramnios are renal anomalies, PROM and severe IUGR. The prognosis can be quite different and repeated ultrasound examinations are recommended to see if amniotic fluid reappears. Fetal MRI as a complementary method might be a future solution for improvement of the antenatal diagnosis in such cases [60].
Two D cases were diagnosed antenatally as having hydrocephalus, which might be a problem for the pathologist. In the second period of this study CNS examinations were markedly improved. Since these D cases occurred in the second period, we believe that fetal autopsy can be seen to reflect the final diagnosis. In five B and five C cases, however, an ultrasound diagnosis of hydrocephalus was not verified at fetal autopsy. It is possible that in some of these cases autopsy failed to demonstrate a true hydrocephalus. This is in line with a report from Carroll et al [81] concerning Dandy Walker anomalies, where autopsy verified the antenatal finding in only six out of 14 cases [81]. MRI might also be helpful to improve antenatal and post-mortem diagnosis of CNS anomalies [60].
Types of anomalies Cerebral and spinal anomalies were the most common (34.8 %) types of fetal anomalies diagnosed in study I, most likely as a result of the high sensitivity for antenatal detection of such anomalies [12, 49, 51, 82]. This figure is in accordance with other findings [7, 10], although it is somewhat lower than that reported by Brand et al [8].

38
Cardiac anomalies are relatively common [49]. Nevertheless they accounted for only 3.7 % here. The reasons for this are probably the low antenatal detection rate and the fact that many of these are classified as complex anomalies or chromosomal aberrations [5, 61, 80]. All our fetuses with cardiac anomalies as a main diagnosis were categorised as A or B cases. This is most likely an effect of our policy to have all fetuses with suspected cardiac anomalies examined in utero by a pediatric cardiologist.
Cardiac anomalies were rarely diagnosed by ultrasound in the 1980s [51]. Nowadays, the sensitivity for detection of cardiac anomalies has increased significantly because of improved training of the midwives performing the routine scans. Today, MRI has no established additional value in such diagnoses.
Fetal autopsy Fetal autopsies provided further diagnostic information in 47 % of our cases and in 10 % a syndrome diagnosis was established. Fetal autopsy by an experienced pathologist is necessary to provide this relevant additional information, which is most useful when counselling the couple concerning future pregnancies. Furthermore, obstetricians and others in the fetal medicine team are given feed-back, which is of importance for quality assurance. However, due to limited resources and logistic difficulties perinatal pathology is not available in all hospitals and therefore regional services are needed to provide adequate quality and standard of care. It is important that pregnancies terminated due to structural anomalies are examined by fetal autopsy as a routine. If the parents do not consent to a fetal autopsy, post-mortem MRI might be an alternative.
Study II and III Many observational studies and case reports about MRI of fetal anomalies have been published with a mixture of second and third trimester cases, most often performed retrospectively [31, 58, 60, 83-87]. According to some studies [88, 89] fetal MRI provides more additional information in the third than in the second trimester.
Evaluations in the second trimester are important in countries with a gestational age limit for pregnancy termination. The diagnostic performance of fetal MRI in early pregnancy is, however, challenging because of the small sizes of the assessed structures and of the higher degree of fetal movements compared to late gestation. No previous study has focused on the diagnostic impact of fetal MRI in the second trimester. Our two studies are the first prospective ones dealing only with second trimester fetal MRI in CNS and non-CNS anomalies.

39
Classification The cases in category III illustrate how fetal MRI findings in the second trimester can provide an improved basis for the woman’s decision to terminate or continue her pregnancy. However, the additional information obtained in category II is also valuable and may be of help in making a more exact diagnosis improving the counselling concerning forthcoming pregnancies and providing feed-back to the ultrasonographer. The confirmation of ultrasound findings found in all cases in category I provides assurance for both the woman and the obstetrician.
The classification was made in consensus between obstetricians (HA, OA) and the radiologist (JW) as in the majority of similar studies [60, 84, 90]. We chose this method of evaluation in order to assure consistent assignments.
Benefit of fetal MRI in CNS anomalies We found that MRI provided additional information in 38 % of the cases, which resulted in altered management in 10 % of all cases. The corresponding figures provided by MRI in non-CNS anomalies were lower, 32 % and 5 %, respectively. This particular benefit of MRI in evaluation of CNS anomalies is in line with other studies [59, 91]. Another contributing factor to this difference could be that women in the CNS study had a higher BMI, 27.9 compared to 25.0 for women in the non-CNS study.
Follow up All MRI examinations were assessable in both studies. We had no false positive MRI findings among the cases with follow up (24/29) in study II. Three out of five cases in which follow up was incomplete or lacking belonged to category I, where ultrasound and MRI findings were identical. In one case in category II, where MRI showed a Dandy-Walker anomaly the autopsy was inconclusive because of severe autolysis. In this case we chose to base the final diagnosis on the unequivocal MRI findings (Fig 3). This is in line with previous reports concerning Dandy-Walker anomalies stating that autopsy verified this diagnosis in a minority of cases [81, 92]. In one case in category III no autopsy was performed. The final diagnosis was based on an obvious holoprosencephaly at MRI (study III). Aside from two cases in which chromosomal aberrations were found, fetal autopsy was performed in almost all terminated pregnancies, IUFD:s and the missed abortion case in study III. One postnatal death due to asphyxia was not followed up by autopsy. Fetal autopsy provided additional diagnostic information in many of the cases. It demonstrated encephalocele, polydactyly and holoprosencephaly, not seen at MRI or ultrasound, and diagnosed Meckel-Gruber syndrome in this case with maternal morbid
40
obesity and oligohydramnios. This was the only false negative CNS finding at MRI (study III).
Neurosonography and 3-D ultrasound as alternatives? Neurosonography has been described as another diagnostic adjunct to ultrasound of CNS anomalies, giving the same additional diagnostic information as MRI [90]. This comparison is limited, however, because the neurosonographer was more experienced than the neuroradiologist at the beginning of that study.
Transvaginal neurosonography has been reported as another way to evaluate fetal CNS [94-96]. Three- and 4-dimensional (D) ultrasound might also serve as a complement [97]. However, all kinds of abdominal ultrasound examinations will meet with the same difficulties as 2-D ultrasound in cases of oligohydramnios and maternal obesity. There is a need for a prospective study to investigate the additive effect of 3D- or 4D- ultrasound to 2D-ultrasound and/or fetal MRI.
Non-CNS anomalies Fetal MRI in non-CNS anomalies gives less additional information than in CNS anomalies, except for cases of diaphragmatic hernia or oligohydramnios (study III). MRI provided additional information in all cases of diaphragmatic hernia without altering the management (Fig 6). It gave additional information about lung volume and liver position, which often is difficult with 2-D ultrasound. This information has evident prognostic value for the infants [98-101]. Three-D ultrasound might be an alternative to MRI to measure lung volumes [102]. In two other cases of thoracic anomalies, MRI verified the ultrasound diagnosis of CHAOS (Fig 7) and correctly diagnosed CCAM, where ultrasound was uncertain. CHAOS is a relatively rare but most often a lethal anomaly. The incidence of CCAM has been estimated to be 1 in 25,000 to 35,000 pregnancies [103]. There are three different types, I-III. Type I is the most common (more than 50 %) with cysts larger than 2 cm. The prognosis depends on the size of the mass which compresses the mediastinum, leading to polyhydramnios or hydrops. Hydrops is a negative prognostic factor [104, 105].
In two previous studies on thoracic anomalies, MRI provided additional information in all five cases [91] and all 14 cases [86], well in line with our results (7/8).
In cases of oligohydramnios, MRI provided additional diagnostic information in five out of 13 cases. The management was altered in three. The cause of oligohydramnios, renal or non-renal, is important when evaluating the prognosis. Our series contains five cases with a non-renal cause, three PROM:s and two IUGR:s. In a recent publication, it was reported that in 27% of cases with PROM before 24 weeks of gestation, the

41
infants survived without any major morbidity [106]. In an MRI study [107] from the third trimester, additional diagnostic information was provided in five of 12 cases of oligohydramnios similar to our results (5/13).
We had 17 cases of urinary tract anomalies. MRI provided additional information in four of these leading to altered management in one. In a previous study of 15 cases, MRI provided additional information in 10 and the management was altered in five [108]. Other authors [107, 109] have presented similar results. The lower proportion with additional information presented here could be due to a high quality of our ultrasound diagnosis of renal anomalies as well as differences in inclusion criteria including GA.
MRI of gastrointestinal anomalies gave additional information in 2/10 cases by correctly diagnosing omphalocele in one case. In another case of anal atresia, MRI gave additional information concerning the level of obstruction, which is in accordance with a previous study concluding that MRI is informative in cases of bowel atresia [110]. However, MRI did not diagnose a case with a minor omphalocele and in another case was not able to differentiate between omphalocele and gastroschisis. This is probably due to the difficulty of MRI to visualise thin membranes.
Musculoskeletal anomalies are a heterogeneous group with varying prognosis. MRI gave no additional information in cases of musculoskeletal anomalies and in one case ultrasound was superior to MRI, which is in line with a previous report [111]. Fetal movements make it difficult to obtain the anatomic planes of the extremities by MRI and the region of interest may move outside the imaging plane. In this group a correct post-mortem diagnosis often requires fetal autopsy and skeletal X-ray. A correct diagnosis is important due to the risk of a hereditary basis for some of these anomalies.
In a case of sacrococcygeal teratoma MRI added information by excluding a connection with the spinal canal. This fits with a previous report showing that MRI provides more information than ultrasound concerning involvement or compression of adjacent organs [112].
In twin-related anomalies, ultrasound is probably superior to MRI due to information from Doppler flow examinations [113].
We had one case where ultrasound showed a hypoplastic left heart. MRI could not reveal this anomaly. This was not surprising, since our MRI evaluation primarily was based on a SS-TSE sequence, by which the cardiac anatomy can not be visualised. Today, fetal echocardiography with high resolution, real time imaging and Doppler flow is superior to MRI. However, using another sequence (SSFP), the different compartments of the heart can be revealed. Recently, this method has shown promising results regarding assessment of cardiovascular anomalies [114].

42
False positive ultrasound findings In previous studies comparing ultrasound and MRI there were many cases (8-24 %) of false positive ultrasound findings [60, 84, 90, 91, 115], which would lead to a large proportion of cases with additional information from MRI. We had no cases with false positive ultrasound findings in the CNS study (study II).
We had seven cases where the finding of a fetal anomaly by ultrasound could not be confirmed at postnatal follow up (study III). The importance of repeated ultrasound or MRI examinations over time, before discussing the diagnosis and prognosis with the woman and her partner, is clearly illustrated by the case of abdominal ascites. Other anomalies detected at second trimester ultrasound, e.g. renal pelvic dilation or abdominal cysts might also disappear at later ultrasound examinations or postnatally. Such findings have sometimes been categorised as false positive cases [79].
Maternal obesity and oligohydramnios The negative impact of maternal obesity on ultrasound detection of fetal anomalies [116] and ultrasound estimation of GA [117] is well demonstrated. The evident additional information from MRI in obese women shown in the CNS study could not be demonstrated in non-CNS study. One explanation could be the smaller number of cases of maternal obesity in the non-CNS study.
Many reports have concluded that MRI in cases of maternal obesity is adjunctive, but our CNS study is the first one that systematically showed this correlation. However, this correlation was not shown in the non-CNS study to the same extent.
An increase in the fertile women’s BMI by two units has been observed over a period of 20 years in Sweden, according to data from Statistics Sweden. High maternal BMI is a risk factor not only for the woman’s health but also for the pregnancy [118, 119].
The diagnostic capacity of ultrasound is limited in cases of obesity [31] and oligohydramnios [120], while fetal MRI is less affected by these conditions. Our results from the MRI studies are well in line with these findings, with two of three women in category III being obese in the CNS study and all three fetuses in category III having oligohydramnios in the non-CNS study.
Strength and limitation The strength of the studies is that the impact of fetal MRI on the clinical management was investigated. Moreover, all MRI examinations were assessable and the follow-up by fetal autopsy or postnatal diagnosis was

43
available in a great majority of cases. In addition, our studies focused on the second trimester and showed that MRI in early pregnancy can be a useful tool with results in line with studies on cases including the third trimester [86, 91, 107-113]. The non-CNS study was relatively large compared with most previous studies.
A limitation is that the number of cases in the CNS study and in the subgroups in study III was relatively low. Moreover, during the study period a majority of eligible cases were not included despite our intention. The reasons were lack of scanner availability, non-adherence to the study protocol by obstetricians and unwillingness of some women to participate. Selection bias can not be excluded. For example, no cases of anencephaly were included. This might have led to an overrepresentation of cases in which additional information was shown at fetal MRI.
Study IV High ascertainment of birth defects in newborns This study showed that the ascertainments in newborns with spina bifida and CLP were relatively high, 91 % and 87%, respectively. This is of importance for the long-term follow-up of newborns, but since the majority of pregnancies with spina bifida is terminated (> 60 %), good ascertainment of newborns only is not sufficient.
Low/unknown ascertainment of pregnancy terminations Since it is compulsory to obtain permission from the CFQ to terminate a pregnancy after 18 weeks’ gestation, it was possible to calculate the ascertainment (73 %) of late terminated pregnancies with spina bifida. However, the majority (70 %) of pregnancies with spina bifida were terminated before the 18th gestational week, and we do not know whether the ascertainment of spina bifida in early terminations is comparable to that of the late ones. Since methods for prenatal diagnosis continuously improve, an increased number of prenatally detected cases of spina bifida will probably be diagnosed and terminated [5, 56, 81, 121].
The present system, with a high rate of pregnancy terminations with low or unknown ascertainment, will lead to an imperfect surveillance of spina bifida. If the BDR is to fulfill its purpose, improved routines for the reporting of terminated pregnancies seem necessary.

44
Spina bifida Folic acid It has been shown that the risk of spina bifida is decreased by preconception supplementary intake of folic acid [122-124]. In Sweden, there is a recommendation for periconception supplementary intake of folic acid [125]. If the ascertainment of spina bifida in pregnancy terminations is uncertain, the effect of increased intake of folic acid by the pregnant population will be difficult to estimate. For example, a reported decrease in the incidence of spina bifida could be due to an increased, but not reported, number of pregnancy terminations or to an effect of an increased intake of folic acid.
Incidences and the changes over time Provided that the under-ascertainment of early terminations of spina bifida pregnancies is in the same range as that of late terminations, the estimated total incidence of spina bifida will be 6.14/10,000 births.
The reported incidence of newborns with spina bifida decreased from 3.89/10,000 births in 1973-84[75] to 1.94/10,000 births during our study period. This change depends mainly on an increased rate of terminated pregnancies. Nowadays, routine ultrasound in the second trimester detects a majority of fetuses with spina bifida and most often Swedish women choose to have the pregnancy terminated [126]. The total reported incidence found here, 4.63/10,000 births, is almost in the same range as that recorded in 1973-84.
Comparison of incidence between and within countries Differences in the incidence of spina bifida between and within countries are due both to different degrees of ascertainment and to genetic variations. Environmental and nutritional factors, for instance folic acid, are also of importance, and their effects are difficult to evaluate. It is essential to be aware of this difficulty when comparing incidence rates of congenital anomalies between and even within countries [125, 126]. The attitude towards termination of pregnancies varies between countries, which might affect the willingness to report to a register which will affect the ascertainment. Registrations of fetal anomalies in pregnancy terminations are either non-existent or have an unsatisfactory quality in many countries compared with registrations of birth defects in newborns [73, 126].
Sweden, together with Norway, Finland, Italy, France and Spain, has one of the lowest incidences of spina bifida in the world. The reported incidence of spina bifida in newborns in Sweden is 1.94/10,000 births, compared to more than 10.0/10,000 births in South America, Mexico and the United Arab Emirates, which have the highest incidence in newborns [73 ]. The reasons for the difference in the incidence rates of spina bifida between countries are complex and imperfectly understood [127].
45
Cleft lip/palate Incidences and differences over time Very few pregnancies with CLP were terminated and the ascertainment of CLP in terminated pregnancies could not be estimated.
The estimated under-ascertainment of all pregnancy terminations during the years 1999-2004 was 31 %, with only minor variation [128]. Supposing that this figure was the same for CLP, the estimated incidence of CLP in terminated pregnancies would be 1.86/10,000 births, which should result in only a minor increase in the total incidence of CLP from 20.09 to 20.80. It is possible however, that comparatively minor anomalies such as CLP are under-ascertained to a higher degree than more severe ones.
The reported incidence/10,000 births of newborns with CLP to BDR was 18.12 during 1973-84 and 15.33 during 1985-98, compared to 14.76 in the present study [9]. The decreasing incidence over time might be due to an increased rate of pregnancy terminations, since CLP often is seen as part of more severe anomalies or syndromes.
Worldwide, the incidence of newborns with CLP is about 15.0/10,000 births. The incidence of CLP found in this study was 16.5/10,000 births after combining the BDR with the MBR. This incidence is comparable to that in Norway, Mexico, and Texas in the USA (18.8-15.9). South Africa, the Czech Republic and Spain have the lowest reported incidences (4.7-7.4/10,000 births), while Finland, Western Australia and Bolivia have the highest (24.1-28.6/10,000 births) [73] The reasons for these differences between countries are unknown, but genetic variation and environmental and nutritional factors are most certainly involved.
Ascertainment increased with severity of CLP The ascertainment of newborns with CLP in BDR increases with the severity of the anomaly, which is in agreement with the findings in the Norwegian study which also showed an increase in ascertainment with the severity of CLP [129]. In the present study the ascertainment of cleft palate was higher when it was accompanied by a cleft lip. The severity of an anomaly might be a factor encouraging doctors to report to the BDR. We found an ascertainment of CPO of 75 %, which is higher than the 57 % found in the Norwegian study [129]. This difference could be due to better routines in Sweden for diagnosis and reporting.
No reporting system exists for spontaneous abortions, which might affect the incidence of spina bifida and especially of CLP. CLP is often associated with complex anomalies, syndromes and chromosomal aberrations, especially trisomy 13 and 18, and such pregnancies have a high rate of spontaneous abortions [130, 131].

46
Conclusions
The following conclusions can be drawn from these studies:
1. Terminations of pregnancy due to structural fetal anomalies are based on a clinically correct antenatal diagnosis in 98.2 % of cases. In 1.8 %, six cases, the decision of termination seems to be based on suboptimal diagnostic and prognostic information to the woman/couple.
2. Fetal autopsy should always be performed when a pregnancy is
terminated due to ultrasound findings of structural fetal anomalies. 3. Fetal MRI in the second trimester of pregnancy is feasible. 4. Fetal MRI of CNS anomalies in the second trimester provided additional
diagnostic information compared to the ultrasound examination in 38 % of the cases, which resulted in altered management in 10 % of the cases.
5. Fetal MRI of CNS anomalies in the second trimester might be a
valuable adjunct to ultrasound in cases of maternal obesity. 6. Fetal MRI of non-CNS anomalies gives additional information in nearly
a third of cases, which resulted in altered management in 5 % of the cases. It might be a clinically valuable adjunct to ultrasound especially in cases of fetal diaphragmatic hernia or oligohydramnios.
7. In newborns, the ascertainments of spina bifida and cleft lip/palate in the
Swedish Birth Defects Registry are relatively high and assessable, but in pregnancy terminations they are lower and difficult or impossible to estimate. Since the majority of pregnancies with spina bifida are terminated in Sweden today, the surveillance is uncertain. There is room for improvement of the routines concerning the reporting of pregnancy terminations.

47
Clinical implications
• Ultrasound is the primary method for diagnosis of fetal anomalies.
• It is important to inform the woman that false negative and false positive ultrasound findings do exist.
• To reduce false positive ultrasound findings, it is important to perform a
second opinion ultrasound and/or an MRI examination preferably with a reasonable time interval.
• Fetal autopsies provide extra information that can be used to inform and
counsel women/couples and to give feed-back to the fetal-medicine team. Fetal autopsy should be routine in terminations due to structural anomalies.
• Fetal MRI in the second trimester is feasible.
• Fetal MRI provides additional information in CNS anomalies especially
when ultrasound is inconclusive due to maternal obesity.
• Fetal MRI of non-CNS anomalies gives valuable additional information in cases of fetal diaphragmatic hernia or oligohydramnios.
• There is room for improvement of the routines concerning reporting of
birth defects from terminated pregnancies.

48
Future Studies
• Three-dimensional (3-D) ultrasound is reported to be a complement to 2-D ultrasound in diagnosis of fetal CNS anomalies [97]. There are many case reports but no systematic studies on the additional value of 3-D ultrasound compared to 2-D ultrasound or MRI. A prospective study to compare 2-D with 3-D ultrasound and fetal MRI in relation to the final diagnosis is suggested.
• A study to evaluate the woman’s own opinion on the value of fetal MRI findings concerning their influence on her decision to terminate or continue the pregnancy.
• A study to evaluate what kind of psychological reactions women experience in connection with fetal MRI.
• A study to assess the ascertainment of Down syndrome in the BDR, in line with the presented study on the BDR.
• A study to estimate the value of post-mortem fetal MRI.

49
Sammanfattning på svenska (Summary in Swedish)
Nästan alla gravida kvinnor (97 %) i Sverige genomgår ultraljuds- undersökning i 17-18: e graviditetsveckan. Syftet med denna undersökning är att bestämma graviditetslängden, diagnostisera ev. flerbörd och att söka efter missbildningar. Missbildningsdiagnostiken har under senare tid blivit en allt viktigare del av rutinultraljudet och man har dessutom blivit allt skickligare på att identifiera fostermissbildningar. Fynd av missbildning kan leda till att graviditeten avbryts och det är därför ytterst viktigt att kvinnan/paret får information om rätt diagnos och därmed även rätt prognos beträffande missbildningen.
Målet med denna avhandling var att studera brister i fosterdiagnostik (studie I), studera en ny fosterdiagnostisk metod, magnetkamera- undersökning (magnetisk resonanstomografi, MR) (studie II-III) och studera om missbildningsregistret fungerar beträffande rapportering av två typmissbildningar samt beräkna om den årliga förekomsten (incidensen) av dessa missbildningar har ändrats över tid (studie IV).
Målet med studie I var att studera samstämmigheten mellan den prenatala ultraljudsdiagnosen och obduktionsfyndet i de fall där graviditets- avbrytanden primärt var baserade på ultraljudsfynden. Studien var retrospektiv och omfattade fosterobduktioner utförda i Uppsala och södra Stockholm under åren 1992-2003.
Vi inkluderade 328 fosterobduktioner där graviditeten avbrutits pga. strukturella fostermissbildningar.
I 175 (53 %) fall överensstämde ultraljudsdiagnosen med foster- obduktionen, i 124 (38 %) fall hade mindre missbildningar antingen missats eller överdiagnostiserats och i 23 (7 %) fall var ultraljudsdiagnosen fel, men obduktion identifierade andra diagnoser av minst samma prognostiska valör, dvs. underlaget till beslutet om avbrytande var ur klinisk synpunkt korrekt. I 6 (2 %) fall hittades antingen ingen avvikelse alls eller en missbildning av mindre prognostisk valör, dvs beslutet om avbrytande var grundat på felaktigt information. Totala antalet fall ökade från 113 (35 %) i första perioden (1992-1997) till 215 (66 %) i den andra perioden (1998-2003), talande för ökat antal avbrytanden pga. utvidgad fosterdiagnostik under den senare perioden. Fosterobduktion tillförde viktig information i 47 % av fallen som kan användas till rådgivning till föräldrar inför nästkommande

50
graviditet och inte minst som ”feedback” till obstetriker och för att kvalitetssäkra verksamheten.
Sammanfattningsvis var graviditetsavbrytandena inte alltid baserade på en korrekt antenatal diagnostik och i 2 % av fallen var diagnosen felaktig, innebärande att beslutet om avbrytande var baserat på icke korrekt information (I). MR av foster har visat sig ha tilläggsvärde till ultraljud vid fostermissbildningar. Tack vare snabb MR-teknik krävs numera ingen sedering av den gravida kvinnan. Hittills har inga negativa effekter på fostret observerats, men det finns rekommendationer att undvika MR i första trimestern och magnetfält över 1.5 Tesla. I en hög andel av graviditetsavbrytanden pga. fostermissbildning (35-48 %) finns avvikelsen i CNS (centrala nervsystemet). Dessa missbildningar har oftast en allvarlig prognos. Det finns ingen studie om MR:s förmåga att diagnostisera fostermissbildningar specifikt i andra trimestern. Tidigare studier har undersökt fall från både andra och tredje trimestern. Dessutom är de oftast retrospektiva.
Vi genomförde en prospektiv studie (II) i Uppsala under 2004-2007. Målet var att studera om MR har tilläggsvärde vid CNS-missbildningar hos foster samt om informationen påverkar handläggningen av graviditeten. Alla gravida kvinnor där ultraljud misstänkte eller konstaterade CNS missbildningar erbjöds att delta i studien. Tjugonio fall inkluderades. MR-undersökningen planerades att utföras inom 3 dagar efter ultraljudsundersökningen. Ultraljud jämfördes med MR och bedömdes i relation till fosterobduktion vid avbrytanden eller postnatala diagnoser hos födda barn. MR genomfördes inom 3 dagar i 79 % av fallen.
Vi fann att MR verifierade ultraljudsdiagnosen utan att tillföra information hos 18 foster (62 %) och att MR tillförde information utan att påverka handläggningen hos 8 foster (28 %). MR gav information som påverkade handläggningen av graviditeten i 3 fall (10 %). I 2 av dessa förelåg maternell obesitas .
Sammanfattningsvis tycks MR vara ett kliniskt värdefullt komplement till ultraljud för diagnostik av CNS-missbildningar hos foster i andra trimestern, framför allt när ultraljud inte är konklusivt pga. maternell obesitas (II). I studie III med samma upplägg som i studie II undersökte vi om MR har tilläggsvärde vid icke-CNS-missbildningar misstänkta vid ultraljud samt om informationen påverkar handläggningen av graviditeten. Alla gravida kvinnor där ultraljud misstänkte eller konstaterade icke- CNS-missbildningar erbjöds att delta i studien. Sextiotre fall inkluderades. MR-undersökningen

51
planerades att utföras inom 3 dagar. MR genomfördes inom 3 dagar i 67 % av fallen.
Vi fann att MR verifierade ultraljudsdiagnosen utan att tillföra information hos 43 foster (68 %) och att MR gav information utan att påverka handläggningen hos 17 foster (27 %). MR gav information som påverkade handläggningen av graviditeten i 3 fall (5 %). Alla dessa fall hade oligohydramnios och i två fall hade den gravida kvinnan obesitas. MR gav tilläggsinformation i alla 6 fall med diafragmabråck och i 5 av 13 fall med oligohydramnios. MR tillförde ingen information vid muskuloskeletala eller tvillingrelaterade missbildningar.
Sammanfattningsvis har MR vid icke-CNS-missbildningar hos foster begränsat tilläggsvärde, men kan tillföra information vid diafragmabråck eller när ultraljud inte är konklusivt pga. oligohydramnios (III). Missbildningsregistret i Sverige etablerades 1964 efter neurosedyn- (thalidomid) katastrofen och har som främsta uppgift att övervaka missbildningar både långsiktigt och kortsiktigt. För att registret ska fungera optimalt förutsätts att en god rapportering av alla missbildningar sker samt att kännedom om bortfallet i rapporteringen finns. Sedan 1999 finns det i Sverige ett register for aborterade foster pga. missbildningar. Det är i dessa fall inte tillåtet att registrera den gravida kvinnans personnummer. Rapporteringen är dessutom frivillig. Rapporteringen av nyfödda barn är obligatorisk.
Målet med studien var att med hjälp av register beräkna incidensen och rapporteringsfrekvensen för två typmissbildningar; ryggmärgsbråck och läpp/käk/gomspalt (LKG). Ryggmärgsbråck diagnostiseras allt oftare prenatalt vilket leder till en hög andel graviditetsavbrytanden. LKG diagnostiseras sällan prenatalt. Missbildningsregistret samkördes med ytterligare fyra register.
Incidensen av ryggmärgsbråck hos nyfödda var 2,40/10,000 födda. Rapporteringsfrekvensen till missbildningsregistret var 79 % och 94 % efter samkörning med medicinska födelseregistret. Av 155 graviditeter som avbröts pga. ryggmärgsbråck, genomfördes 46 avbrytanden efter graviditets- vecka 18 (sena). För dessa beräknades rapporteringen till 73 %. Tidiga avbrytanden utgjorde majoriteten (70 %) av avbrytandena och rapporterings- frekvensen kunde inte beräknas då det inte finns någon källa att jämföra med. Incidensen av avbrytanden beräknades till 3,74/ 10,000 födda och därmed totala incidensen av ryggmärgsbråck till 6,14/10,000 födda. Det innebär att 61 % av graviditeterna där fostret hade ryggmärgsbråck avbröts under perioden 1999-2004.
Hos nyfödda med läpp/käk/gomspalt beräknades incidensen till 18,92/10,000 födda. Rapporteringsfrekvensen till missbildningsregistret var
52
78 %, vilket ökade till 87 % efter samkörning med medicinska födelseregistret. Rapporteringen var högre när läpp- och gomspalt var kombinerade (91 %) jämfört med isolerad gomspalt ( 84 %) respektive läppspalt (85 %). Antalet rapporterade avbrytanden var 43. Rapporterings- frekvensen kunde inte beräknas, då alla avbrytanden utom ett skedde pga. komplexa fostermissbildningar där läpp/käk/gomspalt ingick och endast de allvarligare missbildningarna uppgivits vid ansökan om avbrytande.
Sammanfattningsvis är rapporteringsfrekvensen av dessa missbildningar hos nyfödda barn relativt hög och mätbar, men hos foster där graviditeten avbrutits lägre och svår/omöjlig att beräkna. Rutiner kring rapporteringen av fostermissbildningar kan förbättras (IV).

53
Acknowledgements
I would like to express my sincere gratitude to Uppsala University, Centre for Research and Development Uppsala University/Gävle, Ultrasound foundation Uppsala and Gillbergska foundation Uppsala for financial support and all the pregnant women who participated in the MRI studies.
This thesis could not have been accomplished without the help and support of many people. Particularly I would like to thank: Professor Ove Axelsson, my main supervisor, for patiently reading my manuscripts over and over again, for your enthusiasm, friendship and for sharing your fantastic knowledge in fetal medicine and guiding me through the scientific and ethical aspects of investigation. For always being available even if your time was engaged by your leadership of the department, you always had time to read manuscripts or have a meeting in the “green room”. Associate Professor Johan Wikström, Department of Radiology, my co-supervisor, for your friendship and encouragement when I best needed it. For directing invaluable critism on manuscripts sent by mail. For your fantastic knowledge in MRI and CNS and for teaching me to put the Swedish words together. I hope to have fruitful collaboration with you in the future.
Professor Göran Annerén, Department of Genetics and Pathology, my “inofficial co-supervisor” for giving me the opportunity to cooperate with you in a fantastic field and sharing your knowledge in congenital anomalies and syndromes. For your generosity by inviting us to your beautiful home when we worked on the manuscript. We have at least one manuscript about Down syndrome together. All my co-authors, Per Antonsson, Nikos Papadogiannakis and Magnus Westgren at Huddinge for fruitful cooperation in the field. Christina Pilo at SÖS. Katharina Ericson for also being such a good friend and Lars Eriksson. Birgitta Ollars for taking care of me when I was in your office in Stockholm. Marie Raiend for helping me to collect the MRI papers and for being part of the fetal MRI team. Håkan Ahlström for critically revising one manuscript making it even much better.
54
Associate Professor Tord Naessén, for being a fantastic friend through ups and downs during my PhD studies and in life. For being so generous and for being my second opinion “boll plank”. The heads of department in Gävle Dr Inger Blomberg for being a fantastic chief and understanding my situation, giving me so much time for my investigations and for being my clinical tutor; Henning Thejls, for valueing the investigations and for good cooperation. All my collegues in Gävle for friendship and support. The late Charlotta Hall, who wished so much to enjoy my PhD party. Professor Marianne Högman, the head of Research Centre Uppsala University/Gävle for being engaged in my thesis, my situation and for providing me with financial time.
The late professor Ulf Ulmsten, previous head of the Department of Women’s and Children’s Health for encouragement, friendship and always having an open door, Ulf Hanson, Gunilla Hallberg and Elisabeth Darj the former clinical heads for providing me working condition and time. Bo Sultan, the present head of the department for allowing me to keep my room which I used intensively the last months. All my other collegues in Uppsala University Hospital for friendship and support.
My clinical tutor in the beginning of my residensy in Västerås, Kaj Wedenberg, for being a fantastic teacher in the field of obstetrics and giving me so much of your clinical experience and for encouraging me coming to Uppsala to join my investigation study. Lars-Olov Svensson, the former head of the department in Västerås for believing in me and all my collegues in Västerås for being so nice and friendly. All midwives, nurses and staff nurses at the antenatal centre in Uppsala. I still feel at home when I come to your ward. Thank you for your friendship and co-operation during my studies. Helena Holmgren for generous help with ultrasound views and Susan Rousu for helping with antenatal papers.
Mrs. Maud Marsden and in particular my collegue Dr Steven Lucas for making this thesis and my works more convincing by your excellent linguistic skills.
My mother and father in Iran for always being my support. Excuse me for not being able to come to you for the last 25 years. My sisters for your
55
fantastic ability to not forget me, always keeping contact. My “little” brother in Iran for support to my parents. Ahmad, my big brother in Uppsala and Rezvan, Ehsan and Annahita for your fantastic support and for always being there when we need you. Our wonderful three children, Jacob, Maria and Sofia being the meaning of my life and a fantastic energy source, always shining as the sun and for making everything worthwile. Thank you for your understanding the last months when I did not have enough time to spend with you. Thanks for your support: “Pappa, hur går det med handlingen?” Last but not least, my wonderful wife, Rose-Marie for always believing in me, without your support I never could have finished this work. For your love and patience and for puting up with me.

56
References
1. Donald I, Macvicar J, Brown TG. Investigation of abdominal masses by pulsed
ultrasound. Lancet. 1958 Jun 7;1(7032):1188-95. 2. Donald I, Brown TG. Demonstration of tissue interfaces within the body by
ultrasonic echo sounding. Br J Radiol. 1961 Sep;34:539-46. 3. Sunden B. On the Diagnostic Value of Ultrasound in Obstetrics and
Gynaecology. Acta Obstet Gynecol Scand. 1964;43:SUPPL 6:1-191. 4. Campbell S, Johnstone FD, Holt EM, May P. Anencephaly: early ultrasonic
diagnosis and active management. Lancet. 1972 Dec 9;2(7789):1226-7. 5. SBU. The Swedish Council on Technology Assessment in Health Care. Routine
utrasound under pregnancy, report, September 1998. ISBN 91-87890-52-6. 1998.
6. Hagmann CF, Robertson NJ, Leung WC, Chong KW, Chitty LS. Foetal brain imaging: ultrasound or MRI. A comparison between magnetic resonance imaging and a dedicated multidisciplinary neurosonographic opinion. Acta Paediatr. 2008 Apr;97(4):414-9.
7. Lys F, De Wals P, Borlee-Grimee I, Billiet A, Vincotte-Mols M, Levi S. Evaluation of routine ultrasound examination for the prenatal diagnosis of malformation. Eur J Obstet Gynecol Reprod Biol. 1989 Feb;30(2):101-9.
8. Brand IR, Kaminopetros P, Cave M, Irving HC, Lilford RJ. Specificity of antenatal ultrasound in the Yorkshire Region: a prospective study of 2261 ultrasound detected anomalies. Br J Obstet Gynaecol. 1994 May;101(5):392-7.
9. Richmond S, Atkins J. A population-based study of the prenatal diagnosis of congenital malformation over 16 years. BJOG. 2005 Oct;112(10):1349-57.
10. Weston MJ, Porter HJ, Andrews HS, Berry PJ. Correlation of antenatal ultrasonography and pathological examinations in 153 malformed fetuses. J Clin Ultrasound. 1993 Jul-Aug;21(6):387-92.
11. Shen-Schwarz S, Neish C, Hill LM. Antenatal ultrasound for fetal anomalies: importance of perinatal autopsy. Pediatr Pathol. 1989;9(1):1-9.
12. Tennstedt C, Chaoui R, Bollmann R, Korner H, Dietel M. Correlation of prenatal ultrasound diagnosis and morphological findings of fetal autopsy. Pathol Res Pract. 1998;194(10):721-4.
13. Julian-Reynier C, Macquart-Moulin G, Philip N, Scheiner C, Potier A, Gambarelli D, et al. Fetal abnormalities detected by sonography in low-risk pregnancies: discrepancies between pre- and post-termination findings. Fetal Diagn Ther. 1994 Sep-Oct;9(5):310-20.
57
14. Sun CC, Grumbach K, DeCosta DT, Meyers CM, Dungan JS. Correlation of prenatal ultrasound diagnosis and pathologic findings in fetal anomalies. Pediatr Dev Pathol. 1999 Mar-Apr;2(2):131-42.
15. Faber R, Stepan H, Schilde M, Froster UG, Horn LC. [Accuracy of prenatal diagnoses in terminated pregnancies--a retrospective analysis of results and influences]. Z Geburtshilfe Neonatol. 2001 Mar-Apr;205(2):54-9.
16. Boyd PA, Tondi F, Hicks NR, Chamberlain PF. Autopsy after termination of pregnancy for fetal anomaly: retrospective cohort study. BMJ. 2004 Jan 17;328(7432):137.
17. Barnett S. Ultrasound-induced. Ultrasound Med Biol. 1998;24(9):1501-10. 18. Salvesen KA, Vatten LJ, Eik-Nes SH, Hugdahl K, Bakketeig LS. Routine
ultrasonography in utero and subsequent handedness and neurological development. BMJ. 1993 Jul 17;307(6897):159-64.
19. Kieler H, Axelsson O, Haglund B, Nilsson S, Salvesen KA. Routine ultrasound screening in pregnancy and the children's subsequent handedness. Early Hum Dev. 1998 Jan 9;50(2):233-45.
20. Axelsson O, Marsal K, Valentin L. [Prenatal ultrasonography requires medical indication. The risks are mostly uninvestigated, some findings are unsettling]. Lakartidningen. 2007 Apr 18-24;104(16):1216-7.
21. Bloch F, Hansen, WW, Packard ,M. Nuclear Induction. Physical Review. 1946;70(7-8):460-74.
22. Purcell E, Torrey, HC, Pound, RV. Resonance absorption by nuclear magnetic moments in a solid. Physical Review. 1946;69(1-2):37-8.
23. Lauterbur P. Image formation by induced local interactiobns: Examples employing nuclear magnetic resonance. Nature. 1973;242:190-1.
24. Manfield p. Multi-planar Image Formation using NMR spin echoes. Journal of Physics C-solid state physics 1977;50(591):188-94.
25. Kullberg J. Assessment of body composition using magnetic resonance imaging. Acta universitatis upsaliensis. 2007.
26. Smith FW, Adam AH, Phillips WD. NMR imaging in pregnancy. Lancet. 1983 Jan 1;1(8314-5):61-2.
27. Johnson IR, Symonds EM, Kean DM, Worthington BS, Broughton Pipkin F, Hawkes RC, et al. Imaging the pregnant human uterus with nuclear magnetic resonance. Am J Obstet Gynecol. 1984 Apr 15;148(8):1136-9.
28. Weinreb JC, Lowe T, Cohen JM, Kutler M. Human fetal anatomy: MR imaging. Radiology. 1985 Dec;157(3):715-20.
29. Lowe TW, Weinreb J, Santos-Ramos R, Cunningham FG. Magnetic resonance imaging in human pregnancy. Obstet Gynecol. 1985 Nov;66(5):629-33.
30. Angtuaco TL, Shah HR, Mattison DR, Quirk JG, Jr. MR imaging in high-risk obstetric patients: a valuable complement to US. Radiographics. 1992 Jan;12(1):91-109; discussion 10.
31. Levine D, Barnes PD, Madsen JR, Abbott J, Mehta T, Edelman RR. Central nervous system abnormalities assessed with prenatal magnetic resonance imaging. Obstet Gynecol. 1999 Dec;94(6):1011-9.
32. Shellock FG. Biological effects and safety aspects of magnetic resonance imaging. Magn Reson Q. 1989 Oct;5(4):243-61.

58
33. Kanal E, Gillen J, Evans JA, Savitz DA, Shellock FG. Survey of reproductive health among female MR workers. Radiology. 1993 May;187(2):395-9.
34. Yip YP, Capriotti C, Talagala SL, Yip JW. Effects of MR exposure at 1.5 T on early embryonic development of the chick. J Magn Reson Imaging. 1994 Sep-Oct;4(5):742-8.
35. US Food and Drug Adminstration. Guidance for content and review of a magnetic resonance diagnostic device 510(k) application. Washington DC:FDA. 1998.
36. Shellock FG, Kanal E. Policies, guidelines, and recommendations for MR imaging safety and patient management. SMRI Safety Committee. J Magn Reson Imaging. 1991 Jan-Feb;1(1):97-101.
37. Baker PN, Johnson IR, Harvey PR, Gowland PA, Mansfield P. A three-year follow-up of children imaged in utero with echo-planar magnetic resonance. Am J Obstet Gynecol. 1994 Jan;170(1 Pt 1):32-3.
38. Myers C, Duncan KR, Gowland PA, Johnson IR, Baker PN. Failure to detect intrauterine growth restriction following in utero exposure to MRI. Br J Radiol. 1998 May;71(845):549-51.
39. Health Protection Agency RPD. Protection of patients and voluntrees undergoing MRI procedures: a document for consultation. 2008.
40. Medical magnetic resonance (MR) procedures: protection of patients. Health Phys. 2004 Aug;87(2):197-216.
41. Kanal E, Barkovich AJ, Bell C, Borgstede JP, Bradley WG, Jr., Froelich JW, et al. ACR guidance document for safe MR practices: 2007. AJR Am J Roentgenol. 2007 Jun;188(6):1447-74.
42. Reddy UM, Filly RA, Copel JA. Prenatal imaging: ultrasonography and magnetic resonance imaging. Obstet Gynecol. 2008 Jul;112(1):145-57.
43. Clements H, Duncan KR, Fielding K, Gowland PA, Johnson IR, Baker PN. Infants exposed to MRI in utero have a normal paediatric assessment at 9 months of age. Br J Radiol. 2000 Feb;73(866):190-4.
44. Kok RD, de Vries MM, Heerschap A, van den Berg PP. Absence of harmful effects of magnetic resonance exposure at 1.5 T in utero during the third trimester of pregnancy: a follow-up study. Magn Reson Imaging. 2004 Jul;22(6):851-4.
45. Mevissen M, Buntenkotter S, Loscher W. Effects of static and time-varying (50-Hz) magnetic fields on reproduction and fetal development in rats. Teratology. 1994 Sep;50(3):229-37.
46. Magin RL, Lee JK, Klintsova A, Carnes KI, Dunn F. Biological effects of long-duration, high-field (4 T) MRI on growth and development in the mouse. J Magn Reson Imaging. 2000 Jul;12(1):140-9.
47. Chen MM, Coakley FV, Kaimal A, Laros RK, Jr. Guidelines for computed tomography and magnetic resonance imaging use during pregnancy and lactation. Obstet Gynecol. 2008 Aug;112(2 Pt 1):333-40.
48. Glover P, Hykin J, Gowland P, Wright J, Johnson I, Mansfield P. An assessment of the intrauterine sound intensity level during obstetric echo-planar magnetic resonance imaging. Br J Radiol. 1995 Oct;68(814):1090-4.

59
49. Isaksen CV, Eik-Nes SH, Blaas HG, Torp SH. Comparison of prenatal ultrasound and postmortem findings in fetuses and infants with central nervous system anomalies. Ultrasound Obstet Gynecol. 1998 Apr;11(4):246-53.
50. Pilu G, Perolo A, Falco P, Visentin A, Gabrielli S, Bovicelli L. Ultrasound of the fetal central nervous system. Curr Opin Obstet Gynecol. 2000 Apr;12(2):93-103.
51. Eurenius K, Axelsson O, Cnattingius S, Eriksson L, Norsted T. Second trimester ultrasound screening performed by midwives; sensitivity for detection of fetal anomalies. Acta Obstet Gynecol Scand. 1999 Feb;78(2):98-104.
52. Sabbagha RE, Sheikh Z, Tamura RK, DalCompo S, Simpson JL, Depp R, et al. Predictive value, sensitivity, and specificity of ultrasonic targeted imaging for fetal anomalies in gravid women at high risk for birth defects. Am J Obstet Gynecol. 1985 Aug 1;152(7 Pt 1):822-7.
53. Rutledge JC, Weinberg AG, Friedman JM, Harrod MJ, Santos-Ramos R. Anatomic correlates of ultrasonographic prenatal diagnosis. Prenat Diagn. 1986 Jan-Feb;6(1):51-61.
54. Gant HW MG, Chambers SE, Keeling JW, Muir BB. Prenatal ultrasound diagnosis: a review of fetal outcome. Pediatr Surg Int. 1993;300:295-7.
55. Chescheir NC, Reitnauer PJ. A comparative study of prenatal diagnosis and perinatal autopsy. J Ultrasound Med. 1994 Jun;13(6):451-6.
56. Amini H, Antonsson P, Papadogiannakis N, Ericson K, Pilo C, Eriksson L, et al. Comparison of ultrasound and autopsy findings in pregnancies terminated due to fetal anomalies. Acta Obstet Gynecol Scand. 2006 2006;85(10):1208-16.
57. Girard N, Raybaud C, Dercole C, Boubli L, Chau C, Cahen S, et al. In vivo MRI of the fetal brain. Neuroradiology. 1993;35(6):431-6.
58. Resta M, Greco P, D'Addario V, Florio C, Dardes N, Caruso G, et al. Magnetic resonance imaging in pregnancy: study of fetal cerebral malformations. Ultrasound Obstet Gynecol. 1994 Jan 1;4(1):7-20.
59. Levine D. Obstetric MRI. J Magn Reson Imaging. 2006 Jul;24(1):1-15. 60. Whitby EH, Paley MN, Sprigg A, Rutter S, Davies NP, Wilkinson ID, et al.
Comparison of ultrasound and magnetic resonance imaging in 100 singleton pregnancies with suspected brain abnormalities. BJOG. 2004 Aug;111(8):784-92.
61. Whitby EH, Variend S, Rutter S, Paley MN, Wilkinson ID, Davies NP, et al. Corroboration of in utero MRI using post-mortem MRI and autopsy in foetuses with CNS abnormalities. Clin Radiol. 2004 Dec;59(12):1114-20.
62. McCarthy SM, Filly RA, Stark DD, Callen PW, Golbus MS, Hricak H. Magnetic resonance imaging of fetal anomalies in utero: early experience. AJR Am J Roentgenol. 1985 Oct;145(4):677-82.
63. McNeil TF, Nimby GT. Anomalies and the mental health professional. Ann N Y Acad Sci. 1998 Jun 18;847:10-20.
64. Leithner K, Pornbacher S, Assem-Hilger E, Krampl E, Ponocny-Seliger E, Prayer D. Psychological reactions in women undergoing fetal magnetic resonance imaging. Obstet Gynecol. 2008 Feb;111(2 Pt 1):396-402.
65. Quirk ME, Letendre AJ, Ciottone RA, Lingley JF. Anxiety in patients undergoing MR imaging. Radiology. 1989 Feb;170(2):463-6.
60
66. Whynes DK. Receipt of information and women's attitudes towards ultrasound scanning during pregnancy. Ultrasound Obstet Gynecol. 2002 Jan;19(1):7-12.
67. Ballantyne J. The manual of antenatal pathology. Edingburg: William Green and Sons. 1902.
68. Dorsey DB. A perspective on the autopsy. Am J Clin Pathol. 1978 Feb;69(2 Suppl):217-9.
69. Antonsson P, Sundberg A, Kublickas M, Pilo C, Ghazi S, Westgren M, et al. Correlation between ultrasound and autopsy findings after 2nd trimester terminations of pregnancy. J Perinat Med. 2008;36(1):59-69.
70. Rushton DI. Prognostic role of the perinatal postmortem. Br J Hosp Med. 1994 Nov 2-15;52(9):450-4.
71. Manchester DK, Pretorius DH, Avery C, Manco-Johnson ML, Wiggins J, Meier PR, et al. Accuracy of ultrasound diagnoses in pregnancies complicated by suspected fetal anomalies. Prenat Diagn. 1988 Feb;8(2):109-17.
72. Kallen B, Winberg J. A Swedish register of congenital malformations. Experience with continuous registration during 2 years with special reference to multiple malformations. Pediatrics. 1968 Apr;41(4):765-76.
73. The International Centre on Birth Defects. International Clearinghouse for Birth Defects Monitoring Systems. ISSN 0743-5703. [Reports]. 2001, 2003, 2005.
74. Boyd PA, Armstrong B, Dolk H, Botting B, Pattenden S, Abramsky L, et al. Congenital anomaly surveillance in England--ascertainment deficiencies in the national system. BMJ. 2005 Jan 1;330(7481):27.
75. Registration of congenital malformations 2003. The Swedish National Board of Health and Welfare, Centre for Epidemiology. ISBN 91-7201-914-X [In Swedish]. 2003.
76. Physical status: the use and interpretation of anthropometry. Report of a WHO expert Committee.WHO Health Organ Teach Rep Ser. Technical Report series Geneva: WHO. 1995;24:1-15.
77. Cnattingius S, Ericson A, Gunnarskog J, Kallen B. A quality study of a medical birth registry. Scand J Soc Med. 1990 Jun;18(2):143-8.
78. Axelsson O. The Swedish medical birth register. Acta Obstet Gynecol Scand. 2003 Jun;82(6):491-2.
79. Romosan G, Henriksson E, Rylander A, Valentin L. Diagnostic performance of routine ultrasound screening for fetal abnormalities in an unselected Swedish population in 2000-2005. Ultrasound Obstet Gynecol. 2009 Nov;34(5):526-33.
80. Isaksen CV, Eik-Nes SH, Blaas HG, Torp SH. Fetuses and infants with congenital urinary system anomalies: correlation between prenatal ultrasound and postmortem findings. Ultrasound Obstet Gynecol. 2000 Mar;15(3):177-85.
81. Carroll SG, Porter H, Abdel-Fattah S, Kyle PM, Soothill PW. Correlation of prenatal ultrasound diagnosis and pathologic findings in fetal brain abnormalities. Ultrasound Obstet Gynecol. 2000 Aug;16(2):149-53.
82. Stoll C, Tenconi R, Clementi M. Detection of Congenital Anomalies by Fetal Ultrasonographic Examination across Europe. Community Genet. 2001 Jun;4(4):225-32.
83. Levine D, Hatabu H, Gaa J, Atkinson MW, Edelman RR. Fetal anatomy revealed with fast MR sequences. AJR Am J Roentgenol. 1996 Oct;167(4):905-8.
61
84. Ismail KM, Ashworth JR, Martin WL, Chapman S, McHugo J, Whittle MJ, et al. Fetal magnetic resonance imaging in prenatal diagnosis of central nervous system abnormalities: 3-year experience. J Matern Fetal Neonatal Med. 2002 Sep;12(3):185-90.
85. Sonigo PC, Rypens FF, Carteret M, Delezoide AL, Brunelle FO. MR imaging of fetal cerebral anomalies. Pediatr Radiol. 1998 Apr;28(4):212-22.
86. Quinn TM, Hubbard AM, Adzick NS. Prenatal magnetic resonance imaging enhances fetal diagnosis. J Pediatr Surg. 1998 Apr;33(4):553-8.
87. Poutamo J, Vanninen R, Partanen K, Ryynanen, Kirkinen P. Magnetic resonance imaging supplements ultrasonographic imaging of the posterior fossa, pharynx and neck in malformed fetuses. Ultrasound Obstet Gynecol. 1999 May;13(5):327-34.
88. Levine D, Barnes PD, Robertson RR, Wong G, Mehta TS. Fast MR imaging of fetal central nervous system abnormalities. Radiology. 2003 Oct;229(1):51-61.
89. Twickler DM, Magee KP, Caire J, Zaretsky M, Fleckenstein JL, Ramus RM. Second-opinion magnetic resonance imaging for suspected fetal central nervous system abnormalities. Am J Obstet Gynecol. 2003 Feb;188(2):492-6.
90. Malinger G, Ben-Sira L, Lev D, Ben-Aroya Z, Kidron D, Lerman-Sagie T. Fetal brain imaging: a comparison between magnetic resonance imaging and dedicated neurosonography. Ultrasound Obstet Gynecol. 2004 Apr;23(4):333-40.
91. Breysem L, Bosmans H, Dymarkowski S, Schoubroeck DV, Witters I, Deprest J, et al. The value of fast MR imaging as an adjunct to ultrasound in prenatal diagnosis. Eur Radiol. 2003 Jul;13(7):1538-48.
92. Woodward PJ, Sohaey R, Harris DP, Jackson GM, Klatt EC, Alexander AL, et al. Postmortem fetal MR imaging: comparison with findings at autopsy. AJR Am J Roentgenol. 1997 Jan;168(1):41-6.
93. Griffiths PD, Variend D, Evans M, Jones A, Wilkinson ID, Paley MN, et al. Postmortem MR imaging of the fetal and stillborn central nervous system. AJNR Am J Neuroradiol. 2003 Jan;24(1):22-7.
94. Ben-Amin M, Perlitz Y, Peleg D. Transvaginal sonographic appearance of the cerebellar vermis at 14-16 weeks' gestation. Ultrasound Obstet Gynecol. 2002 Feb;19(2):208-9.
95. Timor-Tritsch IE, Monteagudo A. Transvaginal fetal neurosonography: standardization of the planes and sections by anatomic landmarks. Ultrasound Obstet Gynecol. 1996 Jul;8(1):42-7.
96. Monteagudo A, Timor-Tritsch IE. Normal sonographic development of the central nervous system from the second trimester onwards using 2D, 3D and transvaginal sonography. Prenat Diagn. 2009 Apr;29(4):326-39.
97. Mueller GM, Weiner CP, Yankowitz J. Three-dimensional ultrasound in the evaluation of fetal head and spine anomalies. Obstet Gynecol. 1996 Sep;88(3):372-8.
98. Cannie M, Jani J, Meersschaert J, Allegaert K, Done E, Marchal G, et al. Prenatal prediction of survival in isolated diaphragmatic hernia using observed to expected total fetal lung volume determined by magnetic resonance imaging based on either gestational age or fetal body volume. Ultrasound Obstet Gynecol. 2008 Oct;32(5):633-9.

62
99. Jani J, Cannie M, Sonigo P, Robert Y, Moreno O, Benachi A, et al. Value of prenatal magnetic resonance imaging in the prediction of postnatal outcome in fetuses with diaphragmatic hernia. Ultrasound Obstet Gynecol. 2008 Nov;32(6):793-9.
100. Nishie A, Tajima T, Asayama Y, Ishigami K, Hirakawa M, Nakayama T, et al. MR prediction of postnatal outcomes in left-sided congenital diaphragmatic hernia using right lung signal intensity: comparison with that using right lung volume. J Magn Reson Imaging. 2009 Jul;30(1):112-20.
101. Worley KC, Dashe JS, Barber RG, Megison SM, McIntire DD, Twickler DM. Fetal magnetic resonance imaging in isolated diaphragmatic hernia: volume of herniated liver and neonatal outcome. Am J Obstet Gynecol. 2009 Mar;200(3):318 e1-6.
102. Kalache KD, Espinoza J, Chaiworapongsa T, Londono J, Schoen ML, Treadwell MC, et al. Three-dimensional ultrasound fetal lung volume measurement: a systematic study comparing the multiplanar method with the rotational (VOCAL) technique. Ultrasound Obstet Gynecol. 2003 Feb;21(2):111-8.
103. Laberge JM, Flageole H, Pugash D, Khalife S, Blair G, Filiatrault D, et al. Outcome of the prenatally diagnosed congenital cystic adenomatoid lung malformation: a Canadian experience. Fetal Diagn Ther. 2001 May-Jun;16(3):178-86.
104. De Santis M, Masini L, Noia G, Cavaliere AF, Oliva N, Caruso A. Congenital cystic adenomatoid malformation of the lung: antenatal ultrasound findings and fetal-neonatal outcome. Fifteen years of experience. Fetal Diagn Ther. 2000 Jul-Aug;15(4):246-50.
105. Nagata K. Pediatr Surg Int. 2009;25:753-7. 106. Manuck TA, Eller AG, Esplin MS, Stoddard GJ, Varner MW, Silver RM.
Outcomes of expectantly managed preterm premature rupture of membranes occurring before 24 weeks of gestation. Obstet Gynecol. 2009 Jul;114(1):29-37.
107. Poutamo J, Vanninen R, Partanen K, Kirkinen P. Diagnosing fetal urinary tract abnormalities: benefits of MRI compared to ultrasonography. Acta Obstet Gynecol Scand. 2000 Jan;79(1):65-71.
108. Alamo L, Tarek L, Pierre S, Reto M, Yvan V, Maria-Chiara O, et al. Fetal MRI as complement to US in the diagnosis and characterization of anomalies of the genito-urinary tract. Eur J Radiol. 2009 Jul 28.
109. Barseghyan K, Jackson HA, Chmait R, De Filippo RE, Miller DA. Complementary roles of sonography and magnetic resonance imaging in the assessment of fetal urinary tract anomalies. J Ultrasound Med. 2008 Nov;27(11):1563-9.
110. Veyrac C, Couture A, Saguintaah M, Baud C. MRI of fetal GI tract abnormalities. Abdom Imaging. 2004 Jul-Aug;29(4):411-20.
111. Blaicher W, Mittermayer C, Messerschmidt A, Deutinger J, Bernaschek G, Prayer D. Fetal skeletal deformities - the diagnostic accuracy of prenatal ultrasonography and fetal magnetic resonance imaging. Ultraschall Med. 2004 Jun;25(3):195-9.

63
112. Danzer E, Hubbard AM, Hedrick HL, Johnson MP, Wilson RD, Howell LJ, et al. Diagnosis and characterization of fetal sacrococcygeal teratoma with prenatal MRI. AJR Am J Roentgenol. 2006 Oct;187(4):W350-6.
113. Hu LS, Caire J, Twickler DM. MR findings of complicated multifetal gestations. Pediatr Radiol. 2006 Jan;36(1):76-81.
114. Manganaro L, Savelli S, Di Maurizio M, Perrone A, Francioso A, La Barbera L, et al. Assessment of congenital heart disease (CHD): is there a role for fetal magnetic resonance imaging (MRI)? Eur J Radiol. 2009 Oct;72(1):172-80.
115. Simon EM, Goldstein RB, Coakley FV, Filly RA, Broderick KC, Musci TJ, et al. Fast MR imaging of fetal CNS anomalies in utero. AJNR Am J Neuroradiol. 2000 Oct;21(9):1688-98.
116. Dashe JS, McIntire DD, Twickler DM. Maternal obesity limits the ultrasound evaluation of fetal anatomy. J Ultrasound Med. 2009 Aug;28(8):1025-30.
117. Simic M, Wahlin IA, Marsal K, Kallen K. Maternal obesity is a potential source of error in mid-trimester ultrasound estimation of gestational age. Ultrasound Obstet Gynecol. 2010 Jan;35(1):48-53.
118. Davies GA, Maxwell C, McLeod L, Gagnon R, Basso M, Bos H, et al. Obesity in pregnancy. J Obstet Gynaecol Can. Feb;32(2):165-73.
119. Landres IV, Milki AA, Lathi RB. Karyotype of miscarriages in relation to maternal weight. Hum Reprod. Feb 26.
120. Pistorius LR, Hellmann PM, Visser GH, Malinger G, Prayer D. Fetal neuroimaging: ultrasound, MRI, or both? Obstet Gynecol Surv. 2008 Nov;63(11):733-45.
121. Nicolaides KH, Azar G, Byrne D, Mansur C, Marks K. Fetal nuchal translucency: ultrasound screening for chromosomal defects in first trimester of pregnancy. BMJ. 1992 Apr 4;304(6831):867-9.
122. Kirke PN, Molloy AM, Daly LE, Burke H, Weir DG, Scott JM. Maternal plasma folate and vitamin B12 are independent risk factors for neural tube defects. Q J Med. 1993 Nov;86(11):703-8.
123. Wald NJ, Hackshaw AD, Stone R, Sourial NA. Blood folic acid and vitamin B12 in relation to neural tube defects. Br J Obstet Gynaecol. 1996 Apr;103(4):319-24.
124. De Wals P, Tairou F, Van Allen MI, Uh SH, Lowry RB, Sibbald B, et al. Reduction in neural-tube defects after folic acid fortification in Canada. N Engl J Med. 2007 Jul 12;357(2):135-42.
125. SBU. The Swedish Council on Technology Assessment in Health Care, report 183 (2007). ISBN:978-91-85413-15-17. 2007.
126. Nikkila A, Rydhstrom H, Kallen B. The incidence of spina bifida in Sweden 1973-2003: the effect of prenatal diagnosis. Eur J Public Health. 2006 Dec;16(6):660-2.
127. Frey L, Hauser WA. Epidemiology of neural tube defects. Epilepsia. 2003;44 Suppl 3:4-13.
128. The occurance of congenital malformation in sweden, Article 2004-112-2. A qualitative evaluation of the Swedish Birth Defects Registry. The Swedish Board of Health and Welfare. ISBN 91-7201-876-3. 2004.
64
129. Kubon C, Sivertsen A, Vindenes HA, Abyholm F, Wilcox A, Lie RT. Completeness of registration of oral clefts in a medical birth registry: a population-based study. Acta Obstet Gynecol Scand. 2007;86(12):1453-7.
130. Berge SJ, Plath H, Van de Vondel PT, Appel T, Niederhagen B, Von Lindern JJ, et al. Fetal cleft lip and palate: sonographic diagnosis, chromosomal abnormalities, associated anomalies and postnatal outcome in 70 fetuses. Ultrasound Obstet Gynecol. 2001 Nov;18(5):422-31.
131. Ljunger E, Cnattingius S, Lundin C, Anneren G. Chromosomal anomalies in first-trimester miscarriages. Acta Obstet Gynecol Scand. 2005 Nov;84(11):1103-7.


&��'��%�!�������'(������������������� �������������� ������������������� ������� ����������������������������
�$���!")*�+����,�*���& ��-�,��$�&���
$�&��!��$����!������,!� �*���& ��-�,��$�&���.'((����'��%�!���-.�� � ���-�� �!-�,�� #�!�,(�(�!�/,�0&�(����,�*�&� (����$����!�������!�1�(��� �2�!�0�$��*!����!&*��#!�!���.0*����*�� �!-�������$���!�# ��$����!���������-�*!� 3*�*���!���+�3����4� (!�*����%�� �!����,'((����+����!�������,!� �*���& ��-�,��$�&���/56!��!��7�� �!-.����.�*���!���0��( #���*�$ �$�!�*������84� (!�*����%�� �!����,'((����+����!�������,!� �*���& ��-�,��$�&���9/:
+���!�# ����"( #��&������/ /�� !�"�#�"��" "$�%��������
������������������� ���������� �
����





![Medicine, Nursing and Health Sciences Reducing venous leg ... · Standardise diagnosis of CVD [GS] – Ultrasound scans: practical and reproducible to identify valvular reflux and](https://img.dokumen.tips/doc/110x75/5f0d4a237e708231d4399c57/medicine-nursing-and-health-sciences-reducing-venous-leg-standardise-diagnosis.jpg)























