Embed Size (px)
Citation preview

Feeding practices for infants and young children during andafter common illness. Evidence from South Asia
Kajali Paintal and Víctor M. AguayoRegional Office for South Asia, United Nations Children’s Fund (UNICEF), Kathmandu, Nepal
Abstract
Global evidence shows that children’s growth deteriorates rapidly during/after illness if foods and feeding practicesdo not meet the additional nutrient requirements associated with illness/convalescence. To inform policies andprogrammes, we conducted a review of the literature published from 1990 to 2014 to document how children0–23months old are fed during/after common childhood illnesses. The review indicates that infant and young childfeeding (IYCF) during common childhood illnesses is far from optimal. When sick, most children continue to bebreastfed, but few are breastfedmore frequently, as recommended. Restriction/withdrawal of complementary foodsduring illness is frequent because of children’s anorexia (perceived/real), poor awareness of caregivers’ about thefeeding needs of sick children, traditional beliefs/behaviours and/or suboptimal counselling and support by healthworkers. As a result, many children are fed lower quantities of complementary foods and/or are fed less frequentlywhen they are sick. Mothers/caregivers often turn to family/community elders and traditional/non-qualified practi-tioners to seek advice on how to feed their sick children. Thus, traditional beliefs and behaviours guide the use of‘special’ feeding practices, foods and diets for sick children. A significant proportion of mothers/caregivers turn tothe primary health care system for support but receive little or no advice. Building the knowledge, skills and capacityof community health workers and primary health care practitioners to providemothers/caregivers with accurate andtimely information, counselling and support on IYCF during and after common childhood illnesses, combined withlarge-scale communication programmes to address traditional beliefs and norms that may be harmful, is an urgentpriority to reduce the high burden of child stunting in South Asia.
Keywords: child feeding, common childhood illnesses, diarrhoea, pneumonia, South Asia.
Correspondence: Dr Kajali Paintal, UNICEF Regional Office for South Asia, PO Box 5815, Lekhnath Marg, Kathmandu, Nepal.E-mail: [email protected]
Introduction
About a quarter (26%) of the world’s children underfive live in South Asia. Thirty-eight per cent of themhave stunted growth (UNICEF 2015). Stunting, orlinear growth retardation during early childhood, is anoutcome of biological and/or psychosocial deprivation(Stewart et al. 2013). The short-term and long-termconsequences of stunting include impaired survival,physical growth and cognitive development in pre-school age children; poor school readiness, schoolenrolment and learning outcomes in school-age chil-dren; increased risk of obstetric complications and
mortality in women; and reduced height, productivityand earnings in adults (Grantham-McGregor et al.2007; Walker et al. 2007; de Onis et al. 2013).
A significant proportion of stunting can happen pre-natally. However, evidence indicates that most stuntingin low-income and middle-income countries occursduring the first 24months of life as a result of subopti-mal breastfeeding and complementary feeding prac-tices, often in combination with recurrent infections(Stewart et al. 2013; Jones et al. 2014). Furthermore,children’s nutritional status can deteriorate rapidlyduring/after illness if the additional nutrient require-ments associated with illness/convalescence are not
© 2016 The Authors. Maternal & Child Nutrition published by John Wiley & Sons LtdMaternal & Child Nutrition (2016), 12 (Suppl. 1), pp. 39–71 39
DOI: 10.1111/mcn.12222
Review Article
This is an open access article under the terms of the Creative Commons Attribution License, which permits use, distribution and reproduction in anymedium, provided the original work is properly cited.

met and nutrients are diverted from growth and devel-opment towards the immune response. Children’s poorappetite induced by illness can contribute to perpetuatethe vicious cycle of infection and stunting (Brown 2003;Ramachandran & Gopalan 2009; Gulati 2010;Neumann et al. 2012; Richard et al. 2014). Additionally,in low-income andmiddle-income countries, infant andyoung child feeding (IYCF) practices during and aftercommon childhood illnesses can be particularly poorowing to harmful traditional practices and the lowcoverage/quality of primary health care services(Bhutta & Salam 2012; de Onis et al. 2012; Stewartet al. 2013).
Recognizing the importance of optimal IYCFpractices for child survival, growth and development,the World Health Organization (WHO) launched in2003 the Global Strategy for Infant and Young ChildFeeding and issued in 2003 the Guiding Principlesfor Complementary Feeding of Breastfed and Non-Breastfed Children (WHO/UNICEF 2003; WHO2003a,b). These global frameworks highlight theimportance of optimal IYCF practices during andafter common childhood illnesses such as diarrhoeaand pneumonia and emphasize the need to increasefluid intake during illness while feeding is maintainedand increase food intake during convalescence. Inaddition, appropriate IYCF during and after illnessis part of the WHO-led Global Strategy for theIntegrated Management of Childhood Illnesses(WHO 2005). The definition and measurement of
the indicators for assessing IYCF practices – beyondthe scope of this paper – are comprehensively de-tailed elsewhere (WHO 2008, 2010).
In South Asia,1 breastfeeding is a quasi-universalpractice. An estimated 96% of children are breastfedat some point in their lives, and most (80%) continueto be breastfed at 2 years of age (Dibley et al. 2010;UNICEF 2015). However, data from householdsurveys across the region indicate that the majority ofSouthAsian children are not fed as per the internation-ally agreed upon recommendations: only a quarter(27%) of newborns start breastfeeding within 1 h ofbirth; less than half (48%) of infants 0–5months oldare exclusively breastfed; only about half (56%) ofinfants 6–8month olds are fed soft, semi-solid or solidfoods; and a mere 21% of children 6–23months oldare fed a diet that meets the minimum requirementsin terms of feeding frequency and diet diversity(Senarath et al. 2012; UNICEF 2015). In view of thissituation, researchers and practitioners have not hesi-tated to refer to IYCF in South Asia as a crisis (Memon2012). There is evidence that the incidence and severityof common childhood diseases are high in this region(Walker et al. 2013). However, less is known aboutIYCF practices during and after common childhoodillnesses in South Asia.
Key messages
• Information on infant and young child feeding (IYCF) behaviours and practices during common childhoodillnesses in South Asia is limited. Information of IYCF after illnesses is virtually inexistent. The evidenceavailable indicates that IYCF practices during common childhood illnesses are far from optimal.
• When sick, most children (up to 98%) continue to be breastfed although a significant proportion (up to 49%) isbreastfed less frequently than usual. Few sick children (<20%) are breastfed more frequently than usual, as isrecommended, to compensate for the additional fluid and nutrient requirements associated with illnesses.
• When sick, many children (up to 75%) see their complementary foods restricted in frequency, quantity and/orquality owing to children's anorexia (perceived or real), lack of awareness of caregivers' about the feedingneeds of sick children, traditional beliefs or suboptimal counselling and support by health workers.
• In general, health providers do not advise mothers to increase breastfeeding frequency while encouraging sickchildren to eat soft, varied and favourite foods during illness, as is recommended. Important policy, programmeand capacity gaps exist with respect to IYCF for children during and after common childhood illnesses in manySouth Asian countries.
1For the purpose of this paper, South Asia refers to the eightmember countries of the South Asia Association for RegionalCooperation, namelyAfghanistan, Bangladesh, Bhutan, India,Maldives, Nepal, Pakistan and Sri Lanka.
40 K. Paintal and V.M. Aguayo
© 2016 The Authors. Maternal & Child Nutrition published by John Wiley & Sons Ltd Maternal & Child Nutrition (2016), 12 (Suppl. 1), pp. 39–71

Thus, the objective of this paper is threefold: (1) doc-ument the current IYCF practices during and aftercommon childhood illnesses – particularly diarrhoea,fever and pneumonia – and their trends since 1990 inSouth Asia; (2) document caregiver’s behaviours andhealth providers’ practices with respect to IYCF duringand after common childhood illnesses in South Asia;and in light of the preceding objectives, (3) identify pri-orities in terms of policy formulation, programmedesign, research and advocacy to protect, promoteand support optimal IYCF practices during and aftercommon childhood illnesses in South Asia post 2015.
Methods
We reviewed data and information from two primarysources: Demographic Health Surveys (DHS) andpeer-reviewed publications. DHS collects informationon care-seeking and care-giving practices during diar-rhoea, fever and pneumonia using standardized sam-pling methodologies, interview tools and data analysesprocedures, with minor country-specific adaptations.We reviewed the national DHS surveys conducted inSouth Asia between 1990 and 2014 to document theprevalence of common childhood illnesses – diarrhoea,fever and pneumonia – in children 0–23months old, thefrequency and type of medical advice that caregiverssought, the type of treatment and/or advice thatchildren received and how children were fed duringcommon childhood illnesses. For countries with twodata points, trends in IYCF practices during and aftercommon childhood illness were estimated as well asthe average annual rate of improvement to quantifythe average improvement in a given indicator per yearbetween the base year and end year.
We also conducted a comprehensive review of thepeer-reviewed literature published between January1990 and December 2014. Peer-reviewed articleswere identified through an online PubMed searchusing the following search terms and searchfilters: (1) search terms: <feeding>, <sick>,<morbidity>, <pneumonia>, <diarrhea/diarrhoea>and <IMCI/IMNCI>, each term combinedwith <Afghanistan>, <Bangladesh>, <Bhutan>,<India>, <Maldives>, <Nepal>, <Pakistan>, <Sri
Lanka> and/or <Asia>; (2) search filters: age <child0–59months>; language: <English>; text availability:<abstract>; species :<human>; and search fields:<title/abstract>. Although children 0–23months oldare the focus of our analysis, we expanded our ‘childage’ search criteria to 0–59months to capture addi-tional publications that, while focusing on ‘childrenunder five’ or ‘preschool-age children’, also addressIYCF practices in the first 2 years of life.
The PubMed search identified 367 publicationswith one or more of the search terms in the titleand/or abstract. In-depth scrutiny of the titlesexcluded 158 publications as not relevant to ourreview and identified 209 as potentially relevant.In-depth scrutiny of the abstracts of these 209 publi-cations excluded 126 as not relevant to our reviewand identified 83 as likely relevant. Lastly, full-textscrutiny of these 83 publications excluded 54 as notrelevant to our review and identified 29 articles thatwere relevant to our review. In addition, we reviewedthe bibliographic references of these 29 papers toidentify any additional publication that could havebeen missed by our online search and found threeadditional publications that were relevant to ouranalysis. Hence, 32 publications were included inour analysis as they focused specifically on IYCFpractices during diarrhoea, fever and/or pneumoniain South Asian countries (Fig. 1).
In addition, we conducted interviews with 13 keyinformants. The purpose of the key informant inter-views was not to collect key informants’ views, opin-ions or recommendations but rather to help theauthors of the paper identify the existing nationalpolicies, guidelines and programmes related to IYCFduring and after common childhood illnesses in theeight countries included in the analysis. In the fivelarge countries (Afghanistan, Bangladesh, India,Nepal and Pakistan), we interviewed two UNICEFstaff by country, namely the Chief of Health and theChief of Nutrition, while in the three smallercountries (Bhutan, Maldives and Sri Lanka), weinterviewed one UNICEF staff per country, namelythe Chief of the Health and Nutrition programme.This made a total of 13 key informants who in turnconsulted with relevant national counterparts tocomplete the information-gathering process.
Infant feeding during and after illness in South Asia 41
© 2016 The Authors. Maternal & Child Nutrition published by John Wiley & Sons Ltd Maternal & Child Nutrition (2016), 12 (Suppl.1), pp. 39–71

Findings
Household survey evidence on infant and youngchild feeding and care practices during and afterillness
Six countries – Bangladesh, India, Maldives, Nepal,Pakistan and Sri Lanka – had at least one DHS sur-vey that included information on common childhoodillnesses and IYCF practices (Afghanistan’s 2010DHS did not include data collection on child morbid-ity, and no DHS survey was available for Bhutan).DHS survey data indicate that in the countriesincluded in the analysis, children 0–23months old
suffer from common childhood illnesses frequently.Up to 20–30% of the mothers/caregivers interviewedreported that their children had suffered fromdiarrhoea or pneumonia in the 2weeks prior to thesurvey. The prevalence of common childhood illnesses– diarrhoea, fever and pneumonia – was highest inPakistan. In all countries, the prevalence of fever washigher than the prevalence of diarrhoea orpneumonia. Similarly, in all countries, the prevalenceof common childhood illnesses was lowest during theexclusive breastfeeding period (0–5months) andhighest during the early complementary feedingperiod (6–11months) (Table 1).
Fig. 1. Flow diagram of literature review.
42 K. Paintal and V.M. Aguayo
© 2016 The Authors. Maternal & Child Nutrition published by John Wiley & Sons Ltd Maternal & Child Nutrition (2016), 12 (Suppl. 1), pp. 39–71
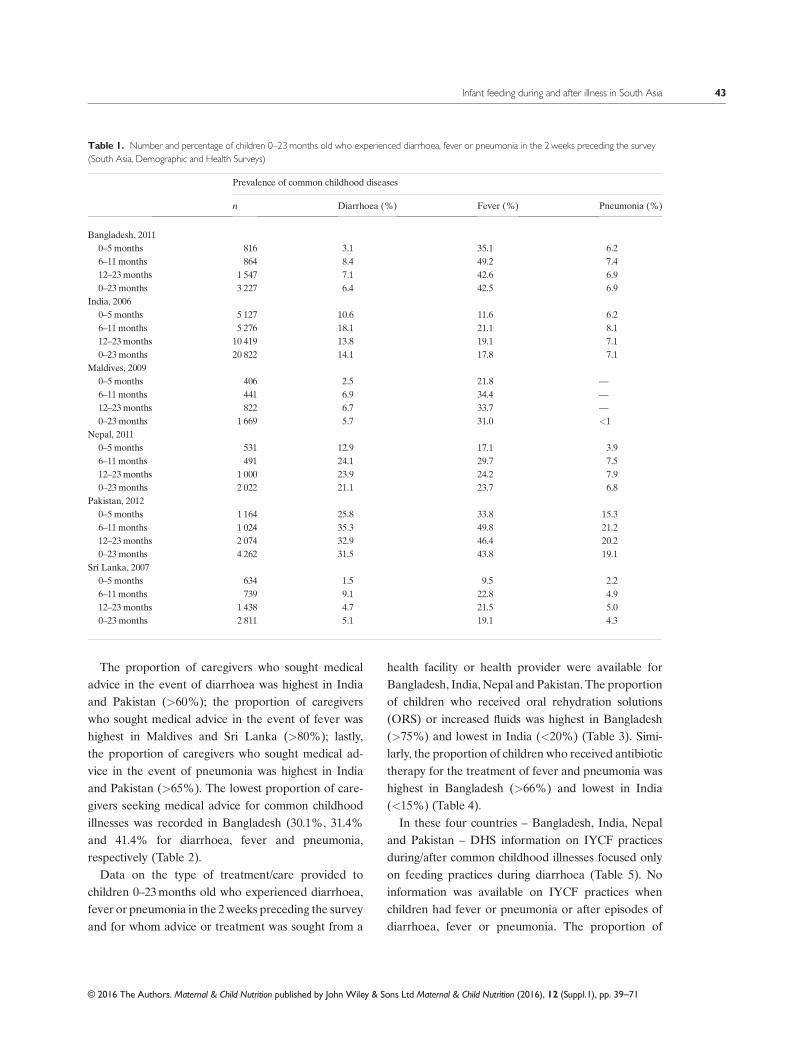
The proportion of caregivers who sought medicaladvice in the event of diarrhoea was highest in Indiaand Pakistan (>60%); the proportion of caregiverswho sought medical advice in the event of fever washighest in Maldives and Sri Lanka (>80%); lastly,the proportion of caregivers who sought medical ad-vice in the event of pneumonia was highest in Indiaand Pakistan (>65%). The lowest proportion of care-givers seeking medical advice for common childhoodillnesses was recorded in Bangladesh (30.1%, 31.4%and 41.4% for diarrhoea, fever and pneumonia,respectively (Table 2).
Data on the type of treatment/care provided tochildren 0–23months old who experienced diarrhoea,fever or pneumonia in the 2weeks preceding the surveyand for whom advice or treatment was sought from a
health facility or health provider were available forBangladesh, India, Nepal and Pakistan. The proportionof children who received oral rehydration solutions(ORS) or increased fluids was highest in Bangladesh(>75%) and lowest in India (<20%) (Table 3). Simi-larly, the proportion of children who received antibiotictherapy for the treatment of fever and pneumonia washighest in Bangladesh (>66%) and lowest in India(<15%) (Table 4).
In these four countries – Bangladesh, India, Nepaland Pakistan – DHS information on IYCF practicesduring/after common childhood illnesses focused onlyon feeding practices during diarrhoea (Table 5). Noinformation was available on IYCF practices whenchildren had fever or pneumonia or after episodes ofdiarrhoea, fever or pneumonia. The proportion of
Table 1. Number and percentage of children 0–23months old who experienced diarrhoea, fever or pneumonia in the 2 weeks preceding the survey(South Asia, Demographic and Health Surveys)
Prevalence of common childhood diseases
n Diarrhoea (%) Fever (%) Pneumonia (%)
Bangladesh, 20110–5 months 816 3.1 35.1 6.26–11months 864 8.4 49.2 7.412–23months 1 547 7.1 42.6 6.90–23months 3 227 6.4 42.5 6.9
India, 20060–5 months 5 127 10.6 11.6 6.26–11months 5 276 18.1 21.1 8.112–23months 10 419 13.8 19.1 7.10–23months 20 822 14.1 17.8 7.1
Maldives, 20090–5 months 406 2.5 21.8 —
6–11months 441 6.9 34.4 —
12–23months 822 6.7 33.7 —
0–23months 1 669 5.7 31.0 <1Nepal, 2011
0–5 months 531 12.9 17.1 3.96–11months 491 24.1 29.7 7.512–23months 1 000 23.9 24.2 7.90–23months 2 022 21.1 23.7 6.8
Pakistan, 20120–5 months 1 164 25.8 33.8 15.36–11months 1 024 35.3 49.8 21.212–23months 2 074 32.9 46.4 20.20–23months 4 262 31.5 43.8 19.1
Sri Lanka, 20070–5 months 634 1.5 9.5 2.26–11months 739 9.1 22.8 4.912–23months 1 438 4.7 21.5 5.00–23months 2 811 5.1 19.1 4.3
Infant feeding during and after illness in South Asia 43
© 2016 The Authors. Maternal & Child Nutrition published by John Wiley & Sons Ltd Maternal & Child Nutrition (2016), 12 (Suppl.1), pp. 39–71

Table 2. Among children 0–23months old who experienced diarrhoea, fever or pneumonia in the 2 weeks preceding the survey, number and percentagefor whom advice/treatment was sought from a health facility or health provider (South Asia, Demographic and Health Surveys)
Bangladesh 2011 India 2006 Maldives 2009 Nepal 2011 Pakistan 2012 Sri Lanka 2007
N (%) N (%) N (%) N (%) N (%) N (%)
Diarrhoea0–5months 25 (43.6) 542 (57.1) — 68 (32.6) 300 (60.0) —
6–11months 73 (30.1) 956 (60.3) — 118 (41.6) 361 (60.8) —
12–23months 109 (27.0) 1434 (66.1) — 239 (40.2) 682 (68.0) —
0–23months 207 (30.1) 2932 (62.5) — 425 (39.4) 1343 (64.3) —
Fever0–5months 155 (36.0) 593 (71.0) 88 (79.9) 91 (34.2) 394 (66.7) 60 (62.5)6–11months 284 (32.8) 1113 (76.4) 152 (86.2) 146 (45.9) 51 (64.9) 169 (87.5)12–23months 466 (29.0) 1991 (71.4) 277 (84.5) 242 (46.2) 962 (66.0) 310 (85.5)0–23months 905 (31.4) 3697 (72.8) 517 (84.2) 479 (43.8) 1407 (66.2) 539 (83.6)
Pneumonia0–5months 51 (39.8) 319 (70.7) — — 178 (70.7) 14 (0.0)6–11months 64 (42.8) 427 (76.9) — — 217 (62.7) 37 (67.6)12–23months 106 (41.4) 743 (69.0) — — 420 (65.5) 71 (65.7)0–23months 221 (41.4) 1489 (71.6) — — 815 (65.9) 122 (58.7)
Table 3. Among children 0–23months old who experienced diarrhoea in the 2 weeks preceding the survey and for whom advice or treatment wassought from a health facility or health provider, percentage according to the type of treatment/care that they were provided during the diarrhoea episode(South Asia, Demographic and Health Surveys)
ORS RHF
ChildrengivenORS orRHF
Childrengivenincreasedfluids
Zn treatment
Znsyrup
Zntablet
Znsupplements
Zn+ORS
Bangladesh, 20110-5 months 46.1 0.0 46.1 1.7 13.9 7.2 — 8.86–11months 73.4 9.3 76.2 23.0 39.4 21.9 — 35.812–23months 75.7 7.1 77.7 25.5 32.0 23.2 — 39.70–23months 71.3 9.8 73.4 21.7 32.4 21.5 — 34.6
India, 20060–5months 13.7 15.6 15.6 2.6 — — 0.0 —
6–11months 21.3 15.9 31.8 7.9 — — 0.5 —
12–23months 34.6 23.6 48.0 11.1 — — 0.3 —
0–23months 26.4 20.8 36.7 8.5 — — 0.3 —
Nepal, 20110–5months 5.8 — 5.8 13.6 — — 1.8 0.06–11months 35.2 — 35.2 9.3 — — 5.7 4.612–23months 48.2 — 48.2 17.7 — — 6.3 6.20–23months 37.8 — 37.8 14.7 — — 5.4 4.8
Pakistan, 20120–5months 25.9 3.3 27.2 7.9 — — 0.6 —
6–11months 38.8 10.5 42.7 5.3 — — 0.3 —
12–23months 44.4 11.0 48.5 8.2 — — 2.7 —
0–23months 38.8 23.6 42.2 7.4 — — 1.6 —
ORS, oral rehydration solution; RHF, recommended home fluids.
44 K. Paintal and V.M. Aguayo
© 2016 The Authors. Maternal & Child Nutrition published by John Wiley & Sons Ltd Maternal & Child Nutrition (2016), 12 (Suppl. 1), pp. 39–71

mothers/caregivers who fed their children more/samefluids as usual was highest in Bangladesh (72.6%) andlowest in India (Table 5).
We were able to examine time trends in four coun-tries – Bangladesh, India, Nepal and Pakistan, wherethree DHS surveys were available for the period1990–2014. Bangladesh and Nepal made significantprogress in reducing the prevalence of diarrhoea, feverand pneumonia in children 0–23months old, mirroredby significant increases in care-seeking behaviour forthese common childhood illnesses. Improvements inIndia were low to nil, while surveys in Pakistanreported a significant deterioration (Table 6).
Table 7 summarizes the trends in feeding and carepractices for children 0–23 during diarrhoea episodes.Over the 1990–2014 period, the proportion of childrenwith diarrhoea who were given Oral RehydrationSolution (ORS) increased in Bangladesh, India andNepal, while there was no improvement in Pakistan.The proportion of children who were not given ORS/recommended home fluids/increased fluids declined inall countries. The highest average annual rate of
reduction was recorded in Bangladesh (0.41) and thelowest in India (0.11). Detailed information on trendsin IYCF during diarrhoea was available only for Nepal(2006–2011) and Pakistan (2007–2012). In both coun-tries, most mothers reported that the amount of liquidsoffered to their infants during the diarrhoea episodewas ‘same as usual’ in both base year and end year.Only about half the mothers in Nepal and one-thirdof mothers in Pakistan reported that the amount offood offered to their children was ‘same than usual’ –with no improvement between base year and end year.
Research evidence on caregivers’ behaviours andhealth providers’ practices on infant and young childfeeding during and after common childhoodillnesses
The bibliographic search identified 32 peer-reviewedpublications that met the inclusion criteria for thisreview. One study (3%) was from Nepal, eight studies(25%)were fromBangladesh, seven studies (22%)werefrom Pakistan and 15 studies (47%) were from India.
Table 4. Among children 0–23months old who experienced fever or pneumonia in the 2 weeks preceding the survey and for whom advice or treatmentwas sought from a health facility or health provider, percentage according to the type of treatment/care that they were provided during the fever/pneumoniaepisode (South Asia, Demographic and Health Surveys)
No. ofchildrenwith fever
Percentage of children withfever who receivedantimalarial drugs
Percentage of children withfever who receivedantibiotic drugs
No. ofchildren withpneumonia
% of children withpneumonia who receivedantibiotic drugs
Bangladesh, 20110–5 months; 286 1.8 54.3 51 69.16–11months 425 0.1 66.9 64 81.812–23months 659 0.9 70.7 106 78.00–23months 1 370 0.8 66.1 221 77.0
India, 20060–5 months 5 127 7.5 14.6 319 14.66–11months 5 276 7.2 14.9 427 11.912–23months 10 419 9.2 13.8 743 12.70–23months 20 822 8.3 14.3 1489 12.9
Nepal, 20110–5 months 91 1.8 29.4 — —
6–11months 146 0 34.4 — —
12–23months 242 1.5 38.1 — —
0–23months; 479 1.1 35.3 — —
Pakistan, 20120–5 months 394 2.4 32 178 41.46–11months 51 5.3 41.1 217 44.112–23months 962 4.0 40.0 420 43.50–23months 1 407 3.6 37.8 815 43.2
Infant feeding during and after illness in South Asia 45
© 2016 The Authors. Maternal & Child Nutrition published by John Wiley & Sons Ltd Maternal & Child Nutrition (2016), 12 (Suppl.1), pp. 39–71
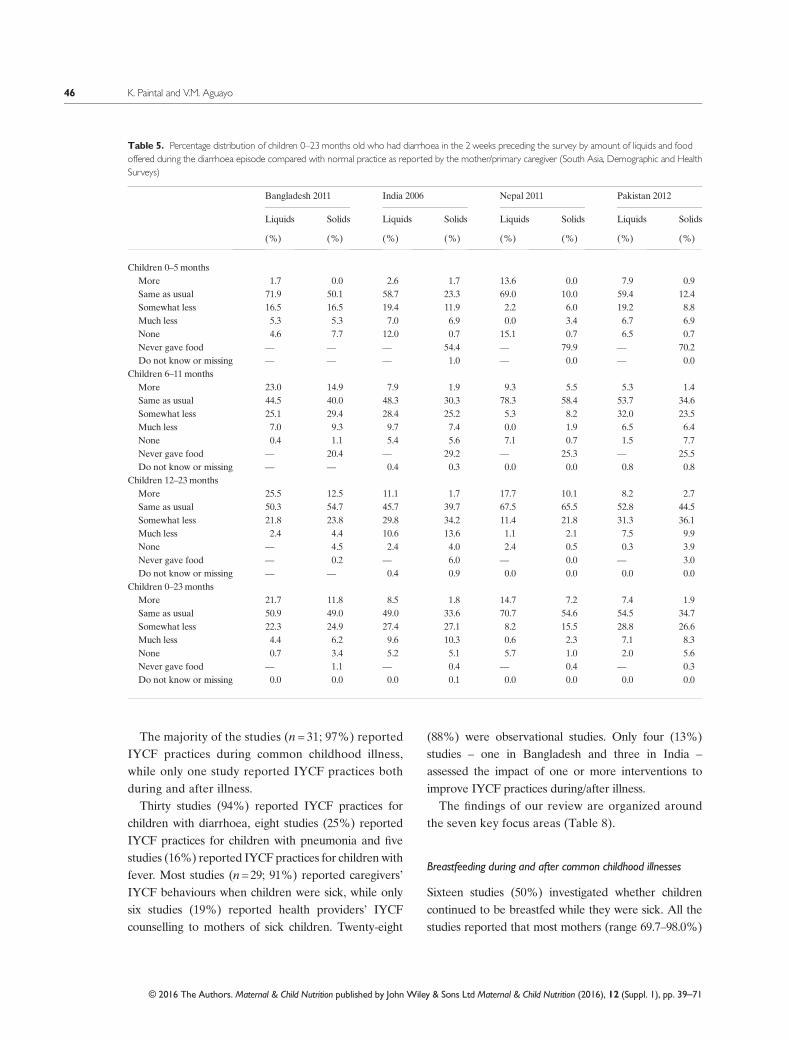
The majority of the studies (n = 31; 97%) reportedIYCF practices during common childhood illness,while only one study reported IYCF practices bothduring and after illness.
Thirty studies (94%) reported IYCF practices forchildren with diarrhoea, eight studies (25%) reportedIYCF practices for children with pneumonia and fivestudies (16%) reported IYCF practices for children withfever. Most studies (n=29; 91%) reported caregivers’IYCF behaviours when children were sick, while onlysix studies (19%) reported health providers’ IYCFcounselling to mothers of sick children. Twenty-eight
(88%) were observational studies. Only four (13%)studies – one in Bangladesh and three in India –
assessed the impact of one or more interventions toimprove IYCF practices during/after illness.
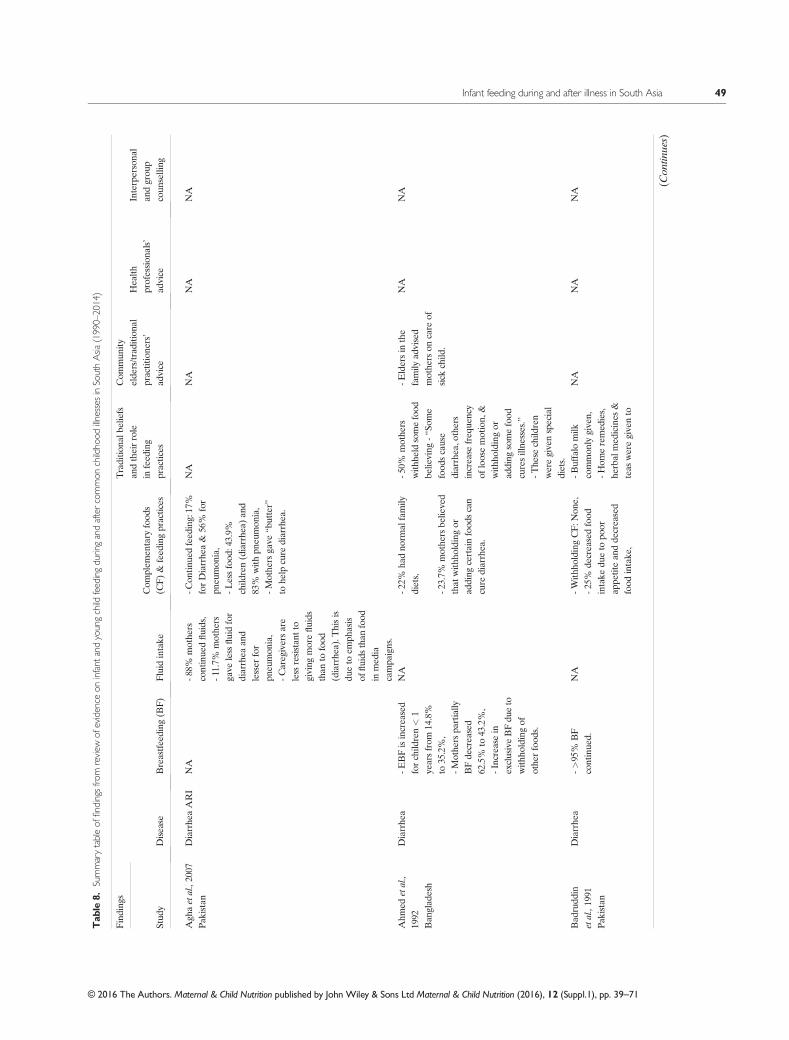
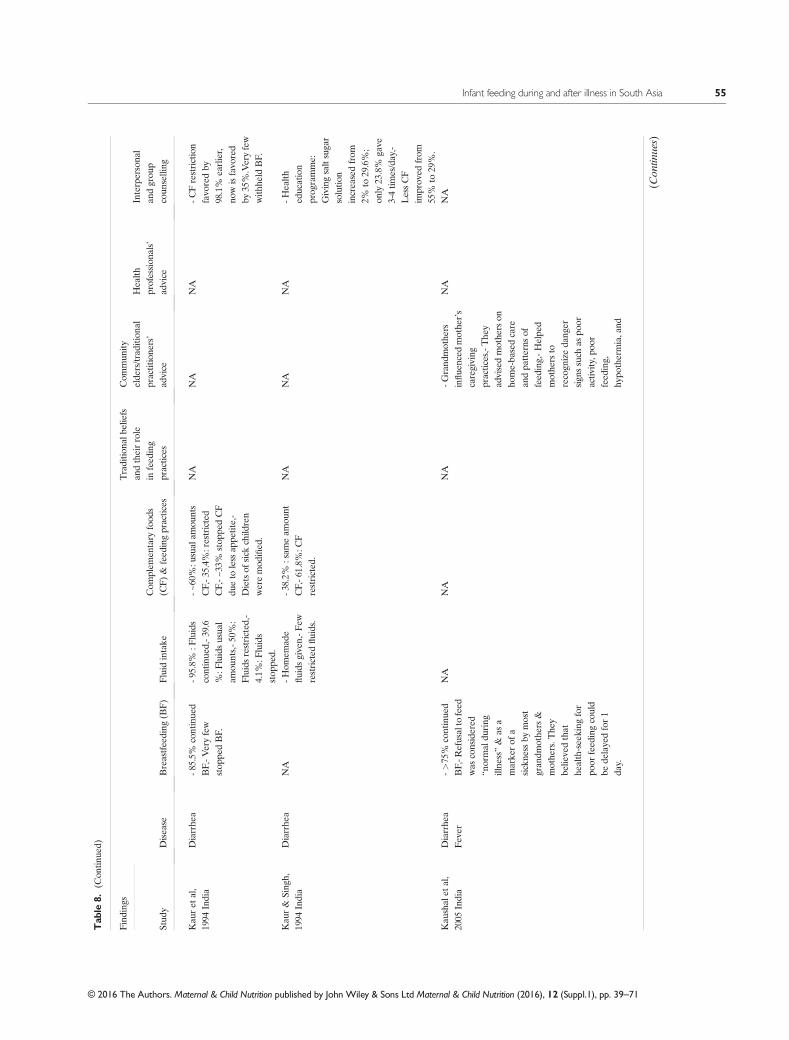
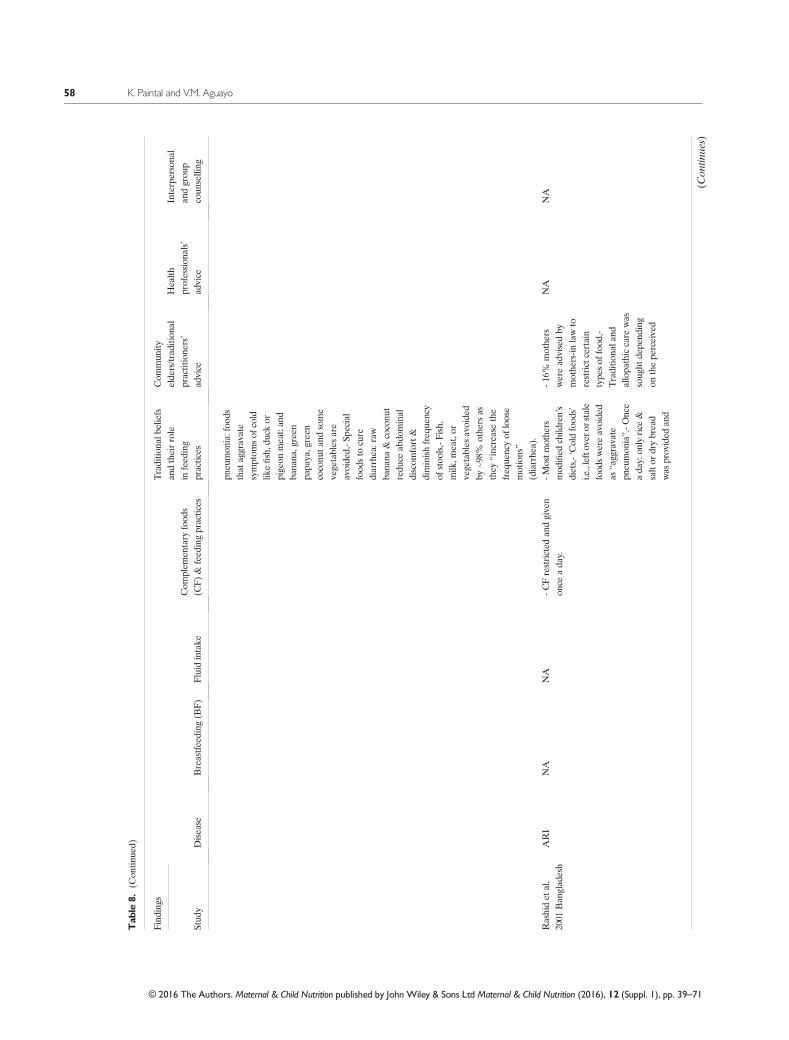
The findings of our review are organized aroundthe seven key focus areas (Table 8).
Breastfeeding during and after common childhood illnesses
Sixteen studies (50%) investigated whether childrencontinued to be breastfed while they were sick. All thestudies reported that most mothers (range 69.7–98.0%)
Table 5. Percentage distribution of children 0–23months old who had diarrhoea in the 2 weeks preceding the survey by amount of liquids and foodoffered during the diarrhoea episode compared with normal practice as reported by the mother/primary caregiver (South Asia, Demographic and HealthSurveys)
Bangladesh 2011 India 2006 Nepal 2011 Pakistan 2012
Liquids Solids Liquids Solids Liquids Solids Liquids Solids
(%) (%) (%) (%) (%) (%) (%) (%)
Children 0–5 monthsMore 1.7 0.0 2.6 1.7 13.6 0.0 7.9 0.9Same as usual 71.9 50.1 58.7 23.3 69.0 10.0 59.4 12.4Somewhat less 16.5 16.5 19.4 11.9 2.2 6.0 19.2 8.8Much less 5.3 5.3 7.0 6.9 0.0 3.4 6.7 6.9None 4.6 7.7 12.0 0.7 15.1 0.7 6.5 0.7Never gave food — — — 54.4 — 79.9 — 70.2Do not know or missing — — — 1.0 — 0.0 — 0.0
Children 6–11 monthsMore 23.0 14.9 7.9 1.9 9.3 5.5 5.3 1.4Same as usual 44.5 40.0 48.3 30.3 78.3 58.4 53.7 34.6Somewhat less 25.1 29.4 28.4 25.2 5.3 8.2 32.0 23.5Much less 7.0 9.3 9.7 7.4 0.0 1.9 6.5 6.4None 0.4 1.1 5.4 5.6 7.1 0.7 1.5 7.7Never gave food — 20.4 — 29.2 — 25.3 — 25.5Do not know or missing — — 0.4 0.3 0.0 0.0 0.8 0.8
Children 12–23monthsMore 25.5 12.5 11.1 1.7 17.7 10.1 8.2 2.7Same as usual 50.3 54.7 45.7 39.7 67.5 65.5 52.8 44.5Somewhat less 21.8 23.8 29.8 34.2 11.4 21.8 31.3 36.1Much less 2.4 4.4 10.6 13.6 1.1 2.1 7.5 9.9None — 4.5 2.4 4.0 2.4 0.5 0.3 3.9Never gave food — 0.2 — 6.0 — 0.0 — 3.0Do not know or missing — — 0.4 0.9 0.0 0.0 0.0 0.0
Children 0–23monthsMore 21.7 11.8 8.5 1.8 14.7 7.2 7.4 1.9Same as usual 50.9 49.0 49.0 33.6 70.7 54.6 54.5 34.7Somewhat less 22.3 24.9 27.4 27.1 8.2 15.5 28.8 26.6Much less 4.4 6.2 9.6 10.3 0.6 2.3 7.1 8.3None 0.7 3.4 5.2 5.1 5.7 1.0 2.0 5.6Never gave food — 1.1 — 0.4 — 0.4 — 0.3Do not know or missing 0.0 0.0 0.0 0.1 0.0 0.0 0.0 0.0
46 K. Paintal and V.M. Aguayo
© 2016 The Authors. Maternal & Child Nutrition published by John Wiley & Sons Ltd Maternal & Child Nutrition (2016), 12 (Suppl. 1), pp. 39–71

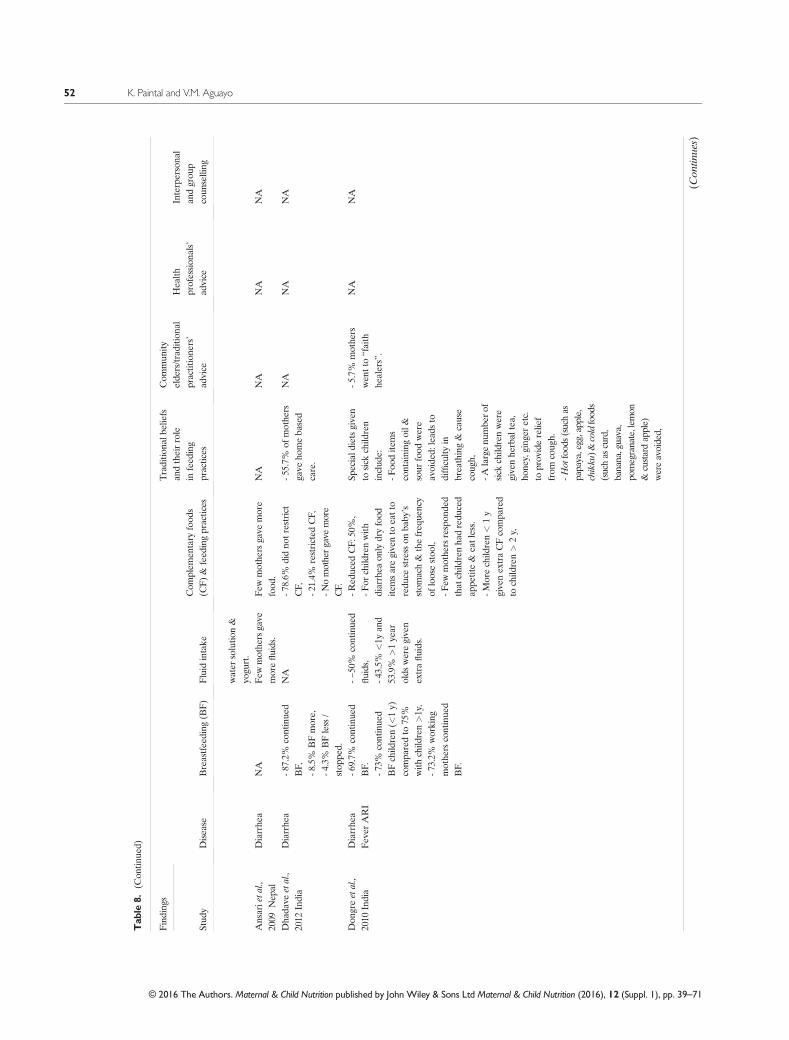
continued to breastfeed their sick children irrespectiveof children’s age or the nature of their illness(Huffman & Combest 1990; Malik et al. 1991;Badruddin et al. 1991, 1997; Kaur et al. 1994; Singh1994; Bhuiya & Streatfield 1995; Piechulek et al.1999; Gupta & Gupta 2000; Mangala et al. 2000;Kaushal et al. 2005; Shah et al. 2011; Benakappa &Shivamurthy 2012; Dhadave et al. 2012; Dongre et al.2010; Giri & Phalke 2014). Three studies reported thatsome mothers (range 8.5–17.0%) breastfed their chil-dren more frequently when children were sick(Mangala et al. 2000; Dhadave et al. 2012; Giri &Phalke 2014); conversely, four studies reported thatsome mothers (range 4.3–49.3%) breastfed their sickchildren less frequently (Piechulek et al. 1999; Shahet al. 2011; Benakappa & Shivamurthy 2012; Giri &Phalke 2014); lastly, six studies reported that somemothers (range 1–9%) ceased to breastfeed whenchildren were sick (Kaur et al. 1994; Gupta & Gupta
2000; Mangala et al. 2000; Shah et al. 2011; Dhadaveet al. 2012; Giri & Phalke 2014). The three main rea-sons given by mothers for reducing or ceasingbreastfeeding while children were sick are: (1) the be-lief that infants could not digest breast milk when theywere sick (two studies; Piechulek et al. 1999; Shah et al.2011); (2) the perception that children wereanorexic/had no appetite and/or refused to be fed(two studies; Bhuiya & Streatfield 1995; Benakappa &Shivamurthy 2012); and/or (3) the belief that breastmilkhad become harmful to the child because ofmystical/evil forces and/or that the illness had beentransmitted by the mother to the child throughmother’smilk (three studies) (Bhuiya&Streatfield 1995; Kaushalet al. 2005; Benakappa & Shivamurthy 2012). Twostudies reported that a significant proportion ofmothers (range 35–61%) – particularly among thosewith young infants 0–11months old and/or childrenwith diarrhoea – switched back to predominant or
Table 6. Percentage of children 0–23months old who experienced diarrhoea, fever or pneumonia in the 2 weeks preceding the survey and for whomadvice/treatment was sought from a heath facility or health provider (Demographic Health Surveys, 1990–2013)
Bangladesh 1994 2004 2011 AARI*Children 0–23months old with diarrhoea (%) 13.2 10.1 6.4 �0.40Children with diarrhoea seeking medical advice (%) 20.6 18.8 30.1 +0.56Children 0–23months old with fever (%) — 46.4 42.5 �0.56Children with fever seeking medical advice (%) — 22.8 31.4 +1.23Children 0–23months old with pneumonia (%) 26.8 26.9 6.9 �1.17Children with pneumonia seeking medical advice (%) 29.3 25.4 41.4 +0.71
India 1992 1998 2006 AARI*Children 0–23months old with diarrhoea (%) 13.2 21.1 14.1 +0.06Children with diarrhoea seeking medical advice (%) 61.9 61.5 62.5 +0.04Children 0–23months old with fever (%) 22.8 30.3 17.8 �0.36Children with fever seeking medical advice (%) 67.7 — 72.8 +0.36Children 0–23months old with pneumonia (%) 7.4 20.2 7.1 �0.02Children with pneumonia seeking medical advice (%) 68.3 63.6 71.6 +0.24
Nepal 1996 2006 2011 AARI*Children 0–23months old with diarrhoea (%) 31.2 18.2 21.1 �0.67Children with diarrhoea seeking medical advice (%) 14.1 27.1 39.4 +1.69Children 0–23months old with fever (%) 41.2 21.5 23.7 �1.17Children with fever seeking medical advice (%) — 33.1 43.8 +2.14Children 0–23months old with pneumonia (%) 37.8 7.2 6.8 �2.07Children with pneumonia seeking medical advice (%) 18.3 42.8 — +2.45
Pakistan 1991 2007 2012 AARI*Children 0–23months old with diarrhoea (%) 19.2 31.6 31.5 +0.59Children with diarrhoea seeking medical advice (%) 51.0 57.4 64.3 �0.01Children 0–23months old with fever (%) 35.6 36.4 43.8 +0.39Children with fever seeking medical advice (%) 66.4 68.6 66.2 �0.01Children 0–23months old with pneumonia (%) 19.1 15.9 74.1 +0.00Children with pneumonia seeking medical advice (%) 68.4 74.1 65.9 �0.12
*Average annual rate of improvement (AARI) quantifies the average rate of change between base year and end year.
Infant feeding during and after illness in South Asia 47
© 2016 The Authors. Maternal & Child Nutrition published by John Wiley & Sons Ltd Maternal & Child Nutrition (2016), 12 (Suppl.1), pp. 39–71

exclusive breastfeeding when children were sick(Ahmed et al. 1992; Shah et al. 2011).
Fluid intake during and after common childhood illnesses
Ten studies (31%) investigated whether children con-tinued to be given fluids when they experienced
common illnesses and/or whether fluid intake increasedor decreased when children were sick. Nine studies re-ported that most mothers (range 40–92%) continued toadminister fluids to their sick children (Kaur & Singh1994; Kaur et al. 1994; Piechulek et al. 1999; Gupta &Gupta 2000; Agha et al. 2007; Gupta et al. 2007; Dongreet al. 2010; Memon et al. 2010; Das et al. 2013). Two
Table 7. Percentage of children 0–23months old who experienced diarrhoea in the 2 weeks preceding the survey, by type of treatment/care they wereprovided and amount of liquids/food offered compared with normal practice (Demographic Health and Surveys, 1990–2013)
Bangladesh 1994 2004 2011 AARIChildren given ORS (%) 47.8 65.2 71.3 1.38Children given recommended home fluids (%) 14.3 17.9 7.0 �0.43Children given increased fluids (%) 48.8 48.6 21.7 �1.59Children not given ORS/recommended home fluids /increased fluids (%) 31.5 16.9 24.5 �0.41
India 1992 1996 2006Children given ORS (%) 17.8 25.5 26.4 0.61Children given recommended home fluids (%) 18.1 12.8 17.4 �0.05Children given increased fluids (%) 13.8 20.7 8.5 �0.38Children not given ORS/ recommended home fluids /increased fluids (%) 61.4 54.3 59.8 �0.11
Nepal 1996 2006 2011Children given ORS (%) 23.8 25.5 37.8 0.93Children given recommended home fluids (%) 4.2 — — —
Children given increased fluids (%) 33.1 20.1 14.7 �1.23Children not given ORS/recommended home fluids/increased fluids (%) 53.8 62.6 51.6 �0.15
Feeding practices: amount of liquids offered to children (%)More 20.1 14.7 �1.08Same as usual 63.4 70.7 1.46Less than usual 13.4 8.8 �0.92None 3.1 5.7 0.52
Feeding practices: amount of food offered to children (%)More 4.7 7.2 0.50Same as usual 53.3 54.6 0.26Less than usual 25.1 17.8 �1.46None 2.6 1.0 �0.32Never gave food 0.2 0.4 0.04
Pakistan 1991 2007 2012Children given ORS (%) 38.8 40.3 38.8 0.0Children given recommended home fluids (%) 14.7 15.8 9.1 �0.27Children given increased fluids (%) 9.4 18.2 7.4 �0.10Children not given ORS/recommended home fluids/increased fluids (%) 54.9 46.7 49.7 �0.25Feeding practices: amount of liquids offered to children (%)
More 18.2 7.4 �2.16Same as usual 43.3 54.5 2.24Less than usual 33.1 35.9 0.56None 5.2 2.0 �0.64Do not know or missing 0.2 0.0 0.0
Feeding practices: amount of food offered to children (%)More 6.3 1.9 �0.88Same as usual 34.2 34.7 0.10Less than usual 31.1 34.9 0.76None 4.8 5.6 0.16Never gave food 23.3 0.3 �4.6Do not know or missing 2.0 0.0 0.0
AARI, average annual rate of improvement; ORS, oral rehydration solution.
48 K. Paintal and V.M. Aguayo
© 2016 The Authors. Maternal & Child Nutrition published by John Wiley & Sons Ltd Maternal & Child Nutrition (2016), 12 (Suppl. 1), pp. 39–71
Tab
le8.
Summarytableof
findings
from
review
ofevidence
oninfant
andyoungchild
feedingduringandaftercommon
childho
odillnessesinSouthAsia
(1990–2014)
Finding
s
Disease
Breastfeeding
(BF)
Fluid
intake
Com
plem
entary
food
s(C
F)&
feed
ingpractices
Traditio
nalb
eliefs
andtheirrole
infeed
ing
practices
Com
mun
ityelde
rs/trad
ition
alpractitione
rs’
advice
Health
profession
als’
advice
Interpersona
lan
dgrou
pcoun
selling
Stud
y
Agh
aetal.,2007
Pak
istan
Diarrhe
aARI
NA
-88%
mothe
rscontinue
dfluids,
-Con
tinue
dfeed
ing:17%
forDiarrhe
a&
56%
for
pneu
mon
ia,
NA
NA
NA
NA
-11.7%
mothe
rsgave
less
fluidfor
diarrhea
and
lesser
for
pneu
mon
ia,
-Lessfood
:43.9%
child
ren(diarrhe
a)an
d83%
with
pneu
mon
ia,
-Caregiversare
less
resistan
tto
giving
morefluids
than
tofood
(diarrhe
a).T
hisis
dueto
emph
asis
offluids
than
food
inmed
iacampa
igns.
-Mothe
rsgave
“butter”
tohe
lpcure
diarrhea.
Ahm
edetal.,
1992
Ban
glad
esh
Diarrhe
a-E
BFisincreased
forchild
ren<
1yearsfrom
14.8%
to35.2%,
NA
-22%
hadno
rmal
family
diets,
-50%
mothe
rswith
held
somefood
belie
ving
-“So
me
food
scause
diarrhea,o
thers
increase
freq
uency
ofloosemotion,
&with
holdingor
adding
somefood
curesillne
sses.”
-Eldersin
the
family
advised
mothe
rson
care
ofsick
child
.
NA
NA
-Mothe
rspa
rtially
BFde
creased
62.5%
to43.2%,
-23.7%
mothe
rsbe
lieved
that
with
holdingor
adding
certainfood
scan
cure
diarrhea.
-Increasein
exclusiveBFdu
eto
with
holdingof
othe
rfood
s.-T
hese
child
ren
weregivenspecial
diets.
Bad
rudd
inetal.,1991
Pak
istan
Diarrhe
a->
95%
BF
continue
d.NA
-With
holdingCF:N
one,
-Buffalo
milk
common
lygiven,
NA
NA
NA
-25%
decreasedfood
intake
dueto
poor
appe
titean
dde
creased
food
intake
,
-Hom
eremed
ies,
herbal
med
icines
&teas
weregivento
(Con
tinues)
Infant feeding during and after illness in South Asia 49
© 2016 The Authors. Maternal & Child Nutrition published by John Wiley & Sons Ltd Maternal & Child Nutrition (2016), 12 (Suppl.1), pp. 39–71

Tab
le8.
(Con
tinue
d)
Finding
s
Disease
Breastfeeding
(BF)
Fluid
intake
Com
plem
entary
food
s(C
F)&
feed
ingpractices
Traditio
nalb
eliefs
andtheirrole
infeed
ing
practices
Com
mun
ityelde
rs/trad
ition
alpractitione
rs’
advice
Health
profession
als’
advice
Interpersona
lan
dgrou
pcoun
selling
Stud
y
child
renwith
diarrhea.
-Nature&
amou
ntof
fluids
&food
svaried
accordingto
disease
intensity
&du
ratio
n.Bad
rudd
inetal.,1997
Pak
istan
Diarrhe
a-~
98%
BF
continue
d.NA
NA
NA
NA
-46%
doctors
prov
ideno
nutrition
alad
vice,
-Treatmen
tgiven
with
expe
nsive
med
ications
&intraven
ousfluids.
NA
Becke
retal.,
1991
Ban
glad
esh
Diarrhe
aFever
NA
NA
-Foo
drestriction
common
NA
NA
NA
NA
Ben
akap
pa&
Shivam
urthy,
2012
India
ARIFever
-97%
BF
continue
d,NA
-57%
continue
dCF,
“Spe
cial
diets”
-19%
gave
home
remed
ieson
elde
rs’
advice.
-Doctors
aske
dto
avoid"cold"
food
,lik
ecurds,bu
tter
milk
,fruitjuices
andba
nana
sin
pneu
mon
ia(18%
).Fever:avo
idrice
–
15%,
NA
-3%
increasedBF,
-12.5%
dilutedtheCF;
70.5%
nochan
gesin
consistency,
-Firmly
rooted
belie
fsab
out“
hot”
and“cold“
food
slead
torestriction
offood
availableat
home,
-38.2%
decreased
BF,
-3%
stop
pedBFas
they
belie
vedthat
illne
sswou
ldbe
tran
smitted
tothe
child
,
-43%
caregivers
redu
ced
CF,
-Reasons
forde
creased
feed
s:child
istired
,”or
“ child
cann
otdigest
during
illne
ss.
-Preferred
food
swere‘id
li’(26.41%),rice
(18.46%)an
dbread(16.98%).
17%
-no
preferen
ce.O
ily(49%
)food
s,spicy
food
s(45.28%)an
d
-Reasons
for
decreasedBF:
“child
cann
otsuck”;or
”Mothe
rissick“.
-6%
restrictdiet
torice
andbu
tter
milk
(diarrhe
a),
-62%
:not
torestrict
anykind
offood
andto
follo
w
(Con
tinues)
50 K. Paintal and V.M. Aguayo
© 2016 The Authors. Maternal & Child Nutrition published by John Wiley & Sons Ltd Maternal & Child Nutrition (2016), 12 (Suppl. 1), pp. 39–71

Tab
le8.
(Con
tinue
d)
Finding
s
Disease
Breastfeeding
(BF)
Fluid
intake
Com
plem
entary
food
s(C
F)&
feed
ingpractices
Traditio
nalb
eliefs
andtheirrole
infeed
ing
practices
Com
mun
ityelde
rs/trad
ition
alpractitione
rs’
advice
Health
profession
als’
advice
Interpersona
lan
dgrou
pcoun
selling
Stud
y
food
considered
as"cold"
were
avoide
d.
theusua
ldiet
during
recovery.
Bha
rtietal.,2006
India
Pne
umon
iaNA
NA
-Whe
nchild
renweresick
with
pneu
mon
ia,the
rewerefeed
ingrestrictions
inalargenu
mbe
rof
cases.
NA
16.5%
soug
htad
vice
from
unqu
alified
practitione
rs.
NA
NA
Bhu
iya&
Streatfield,
1995
Ban
glad
esh
Diarrhe
aFever
-BFiscontinue
din
amajority,
NA
-~50%
continue
dCFfor
diarrhea
&fever,
NA
-Con
sulting
trad
ition
alhe
alth
care
prov
iderswas
quite
common
.
-100%
doctors
prov
ideno
nutrition
alad
vice,
NA
-Nomothe
rrepo
rted
increase
inBF,
-39%
redu
cedan
d10%
discon
tinue
dCF,
-16%
redu
cedBF,
-Non
egave
moreCF,
-Dep
ending
onillne
ss,practition
ers
advisedon
food
sto
eato
rrestrict.
-Adv
iceby
doctors
mainlyon
med
icine
oruseof
ORS
(diarrhe
a):9%,
-Red
uctio
nin
BF,
high
estfor
fever+
coug
h,fever&
diarrhea,
-Reasons
for
discon
tinuing
CF:(1)
refusaltoeat/an
orexia
(2)considered
harm
ful
(3)im
positio
nby
caregiver,
-5-10%
advisedto
redu
ceor
stop
feed
ingde
pend
ing
ontheillne
ss.
-Reasons
toredu
ceor
discon
tinue
BF
are:“refusalto
eat”
or“con
side
red
harm
ful”.
-Indiarrhea,normalfood
isbe
lievedto
beha
rmful.
Das
etal.,2013
Ban
glad
esh
Diarrhe
aNA
-61.3%
gave
sameam
ount,
-Nochild
was
givenmore
food
,NA
-39.5%
mothe
rswith
0–11
mba
bies
and20%
mothe
rswith
1–2ychild
ren
soug
htad
vice
from
uncertified
.trad
ition
alprov
iders.
NA
NA
-10.8%
offered
less,
-71.4%
gave
same
amou
nt,
-27.6%
gave
homem
adefluids
likethin
watery
porridge
ofmaize,
rice,o
rwhe
at,
soup
,sug
arsalt
-28.7%
gave
less
food
,-Y
oung
er0-1-ywere
encouraged
todrink/eat
more,
-Few
olde
rchild
ren(11–
24m)wereen
couraged
toeatm
ore,
(Con
tinues)
Infant feeding during and after illness in South Asia 51
© 2016 The Authors. Maternal & Child Nutrition published by John Wiley & Sons Ltd Maternal & Child Nutrition (2016), 12 (Suppl.1), pp. 39–71
Tab
le8.
(Con
tinue
d)
Finding
s
Disease
Breastfeeding
(BF)
Fluid
intake
Com
plem
entary
food
s(C
F)&
feed
ingpractices
Traditio
nalb
eliefs
andtheirrole
infeed
ing
practices
Com
mun
ityelde
rs/trad
ition
alpractitione
rs’
advice
Health
profession
als’
advice
Interpersona
lan
dgrou
pcoun
selling
Stud
y
water
solutio
n&
yogu
rt.
Ansarieta
l.,2009
Nep
alDiarrhe
aNA
Few
mothe
rsgave
morefluids.
Few
mothe
rsgave
more
food
.NA
NA
NA
NA
Dha
dave
etal.,
2012
India
Diarrhe
a-8
7.2%
continue
dBF,
NA
-78.6%
didno
trestrict
CF,
-55.7%
ofmothe
rsgave
homeba
sed
care.
NA
NA
NA
-8.5%
BFmore,
-21.4%
restricted
CF,
-4.3%
BFless
/stop
ped.
-Nomothergave
more
CF.
Don
greetal.,
2010
India
Diarrhe
aFever
ARI
-69.7%
continue
dBF.
-~50%
continue
dfluids,
-Red
uced
CF:50%
,Sp
eciald
ietsgiven
tosick
child
ren
includ
e:
-5.7%
mothe
rswen
tto“faith
healers”.
NA
NA
-73%
continue
dBFchild
ren(<
1y)
compa
redto
75%
with
child
ren>1y,
-43.5%
<1y
and
53.9%
>1year
olds
weregiven
extrafluids.
-For
child
renwith
diarrhea
only
dryfood
itemsaregivento
eatto
redu
cestress
onba
by’s
stom
ach&
thefreq
uency
ofloosestoo
l,
-Foo
dite
ms
containing
oil&
sour
food
were
avoide
d:lead
sto
difficulty
inbreathing&
cause
coug
h,
-73.2%
working
mothe
rscontinue
dBF.
-Few
mothe
rsrespon
ded
that
child
renha
dredu
ced
appe
tite&
eatless.
-Alargenu
mbe
rof
sick
child
renwere
givenhe
rbal
tea,
hone
y,ging
eretc.
toprov
iderelie
ffrom
coug
h.
-Morechild
ren<
1y
givenextraCFcompa
red
tochild
ren>
2y,
-Hot
food
s(suchas
papaya,egg,app
le,
chikku
)&coldfood
s(suchas
curd,
banana,guava,
pomegranate,lem
on&
custardapple)
wereavoided,
(Con
tinues)
52 K. Paintal and V.M. Aguayo
© 2016 The Authors. Maternal & Child Nutrition published by John Wiley & Sons Ltd Maternal & Child Nutrition (2016), 12 (Suppl. 1), pp. 39–71

Tab
le8.
(Con
tinue
d)
Finding
s
Disease
Breastfeeding
(BF)
Fluid
intake
Com
plem
entary
food
s(C
F)&
feed
ingpractices
Traditio
nalb
eliefs
andtheirrole
infeed
ing
practices
Com
mun
ityelde
rs/trad
ition
alpractitione
rs’
advice
Health
profession
als’
advice
Interpersona
lan
dgrou
pcoun
selling
Stud
y
Low
erprop
ortio
nof
child
renfrom
sche
duled
tribes/n
omad
ictribes
givenincreasedCF.
Med
icines,syrup
,injections
&tablets
arepreferredov
erho
meremed
ies.
Giri&
Pha
lke,
2014
India
Diarrhe
a-6
0%continue
dBF,
NA
-91%
continue
dCF,
-71%
:coldfood
berestricted
incold/
coug
h,
NA
NA
NA
-21%
decreased
BF,
-26.5%
:decreased
CF,
-89%
:curdbe
restricted
inARI,
-17%
increased
BF,
-9%:stopp
edCF,
-75%
:heavy
food
berestricted
indiarrhea,
-2%
stop
pedBF.
-Amon
gthosewho
continue
d:32%
preferredthinne
rconsistencyan
d8%
preferredthick
consistencyof
food
.-7
2%oily
food
berestricted
infever,
-Preferred
“spe
cial
diets”
during
illne
ss:
1)Feeding
khicha
di(81.5%
),milk
(67.5%
)&
biscuits
(59%
)forARI,
2)Ban
ana(95%
),sago
(92.5%
)&rice
water
(89%
)du
ring
diarrhea.
Gup
ta&
Gup
ta,
2000
India
Diarrhe
aFever
->75%
continue
dBF,
-92.2%
:continue
dfluids,
NA
-Hou
seho
ldremed
iessuch
asrice
grue
l,spices,
onionjuicewere
adop
tedby
8.6%
mothe
rs.
-Mothe
r-in-la
wad
visedmothe
rson
care
ofthesick
child
,
-47.3%
mothe
rsprefer
private
doctors,
NA
-7.8%
stop
pedBF.
-7.8%:stopp
edfluids,
-8.7%
child
ren<
1yearsstop
ped
-20.4%
mothe
rsprefer
govtdo
ctors,
-Majority
mothe
rs:
(Con
tinues)
Infant feeding during and after illness in South Asia 53
© 2016 The Authors. Maternal & Child Nutrition published by John Wiley & Sons Ltd Maternal & Child Nutrition (2016), 12 (Suppl.1), pp. 39–71

Tab
le8.
(Con
tinue
d)
Finding
s
Disease
Breastfeeding
(BF)
Fluid
intake
Com
plem
entary
food
s(C
F)&
feed
ingpractices
Traditio
nalb
eliefs
andtheirrole
infeed
ing
practices
Com
mun
ityelde
rs/trad
ition
alpractitione
rs’
advice
Health
profession
als’
advice
Interpersona
lan
dgrou
pcoun
selling
Stud
y
fluids
compa
red
to6.8%
child
ren
>1yr,
-Hom
eremed
ies
weregene
rally
advised.
-15.9%
gave
home-ba
sedfluids
&ORSas
first
actio
n.The
seinclud
eread
ymad
eORS,
sugar-salt
solutio
n,Lassior
Shikka
nji.
notg
iven
nutrition
alad
vice
-71%
govt.doctors
laid
emph
asison
useof
homeba
sed
fluids/O
RSas
compa
redto
27%
private
practitione
rs.
Gup
taetal.,2007
India
Diarrhe
aARI
NA
-42%
:con
tinue
dfluids,
50%:C
omplem
entary
feed
ing(C
F)continue
dNA
-Hom
eremed
ies
werefirstlineof
treatm
ent.
NA
-20%
:stopp
edfluids,
30%:gaveho
mecook
edfamily
food
s.-4
2%gave
home-
basedfluids.
Hiran
i,2012
Pak
istan
Diarrhe
aNA
NA
-CFrestrictioncommon
NA
-Mothe
rsprefer
trad
ition
alpractitione
rs.
NA
NA
-For
ARI:milk
&rice
restricted
,Huffm
an&
Com
best,1990
Ban
glad
esh
Diarrhe
a-Inmajority
BF
continue
dNA
->75%infantsoften
refuse
othe
rfood
s.NA
NA
NA
NA
Kasie
tal,
1995
Pak
istan
Diarrhe
aNA
NA
NA
NA
NA
-71%
doctorsgave
nonu
trition
alad
vice
instead
prescribed
drug
s&
ORS,-46%
doctors
prov
ided
advice
onBFan
dno
tCF,-
7%introd
uctio
nof
CFafterillne
ss.
NA
(Con
tinues)
54 K. Paintal and V.M. Aguayo
© 2016 The Authors. Maternal & Child Nutrition published by John Wiley & Sons Ltd Maternal & Child Nutrition (2016), 12 (Suppl. 1), pp. 39–71
Tab
le8.
(Con
tinue
d)
Finding
s
Disease
Breastfeeding
(BF)
Fluid
intake
Com
plem
entary
food
s(C
F)&
feed
ingpractices
Traditio
nalb
eliefs
andtheirrole
infeed
ing
practices
Com
mun
ityelde
rs/trad
ition
alpractitione
rs’
advice
Health
profession
als’
advice
Interpersona
lan
dgrou
pcoun
selling
Stud
y
Kau
ret
al,
1994
India
Diarrhe
a-8
5.5%
continue
dBF,-V
eryfew
stop
pedBF.
-95.8%
:Fluids
continue
d,-3
9.6
%:F
luidsusua
lam
ounts,-5
0%:
Fluidsrestricted
,-4.1%
:Fluids
stop
ped.
-~60%:u
sual
amou
nts
CF,-3
5.4%
:restricted
CF,-~
33%
stop
pedCF
dueto
less
appe
tite,-
Dietsof
sick
child
ren
weremod
ified
.
NA
NA
NA
-CFrestriction
favo
redby
98.1%
earlier,
nowisfavo
red
by35%.Veryfew
with
held
BF.
Kau
r&
Sing
h,1994
India
Diarrhe
aNA
-Hom
emad
efluids
given,-F
ewrestricted
fluids.
-38.2%
:sam
eam
ount
CF,-6
1.8%
:CF
restricted
.
NA
NA
NA
-Health
education
prog
ramme:
Givingsaltsugar
solutio
nincreasedfrom
2%to
29.6%;
only
23.8%
gave
3-4tim
es/day,-
LessCF
improv
edfrom
55%
to29%.
Kau
shal
etal,
2005
India
Diarrhe
aFever
->75%
continue
dBF,-R
efusalto
feed
was
considered
“normal
during
illne
ss”&
asa
marke
rof
asickne
ssby
most
gran
dmothe
rs&
mothe
rs.T
hey
believedthat
health-seeking
for
poor
feed
ingcould
bede
layedfor1
day.
NA
NA
NA
-Grand
mothe
rsinflue
nced
mothe
r’s
caregiving
practices,-The
yad
visedmothe
rson
home-ba
sedcare
andpa
tterns
offeed
ing,-H
elpe
dmothe
rsto
recogn
izeda
nger
sign
ssuch
aspo
oractiv
ity,p
oor
feed
ing,
hypo
thermia,and
NA
NA
(Con
tinues)
Infant feeding during and after illness in South Asia 55
© 2016 The Authors. Maternal & Child Nutrition published by John Wiley & Sons Ltd Maternal & Child Nutrition (2016), 12 (Suppl.1), pp. 39–71

Tab
le8.
(Con
tinue
d)
Finding
s
Disease
Breastfeeding
(BF)
Fluid
intake
Com
plem
entary
food
s(C
F)&
feed
ingpractices
Traditio
nalb
eliefs
andtheirrole
infeed
ing
practices
Com
mun
ityelde
rs/trad
ition
alpractitione
rs’
advice
Health
profession
als’
advice
Interpersona
lan
dgrou
pcoun
selling
Stud
y
respiratory
distress,-
Grand
mothe
rsha
dho
mem
ade
remed
iesfor
common
ailm
ents,
someof
which
couldbe
harm
ful.
Malik
etal,
1991
Pak
istan
Diarrhe
a-7
0%continue
dBF,
NA
-78%
-87%
:weregiven
norm
alfamily
food
s.Sick
child
renalso
received
solid
&semi-solid
diet
which
was
either
"Khitchri"
orba
nana
asmen
tione
dby
more
than
halfof
the
respon
dents.
NA
NA
NA
Man
gala
etal,
2000
India
Diarrhe
a-9
2.4%
continue
dBF,-1
5.1%
BF
morefreq
uently,-
8.6%
ceased
BF.
-47%
awareof
increasedfluids.
-30%
:Con
tinue
dCF,-
2.4%
:gave“spe
cial
diets”
i.e.,cook
ing
practices
mod
ified
i.e.,
food
mashe
dor
grou
ndfood
foreasier
digestion
(mod
ificatio
nin
food
quality
),-1
6.7%
more
CF,-E
ducatio
nal
interven
tion:
increase
ofmothe
rsmod
ifyingfood
tomak
eitsoft&
more
easily
digestible
2.4%
to26.2%-Increased
feed
ing
afterillne
ss:N
one.
NA
NA
NA
After
aned
ucationa
linterven
tion
improv
emen
tsin-B
Ffreq
uency
(15.1%
to47.2%)-
Mod
ificatio
nof
CFprep
aration
(2.4%
to26.2%)-
IncreasedCF
afterillne
ss(1.2%
to20%)
(Con
tinues)
56 K. Paintal and V.M. Aguayo
© 2016 The Authors. Maternal & Child Nutrition published by John Wiley & Sons Ltd Maternal & Child Nutrition (2016), 12 (Suppl. 1), pp. 39–71

Tab
le8.
(Con
tinue
d)
Finding
s
Disease
Breastfeeding
(BF)
Fluid
intake
Com
plem
entary
food
s(C
F)&
feed
ingpractices
Traditio
nalb
eliefs
andtheirrole
infeed
ing
practices
Com
mun
ityelde
rs/trad
ition
alpractitione
rs’
advice
Health
profession
als’
advice
Interpersona
lan
dgrou
pcoun
selling
Stud
y
Mem
onet
al,
2010
Pak
istan
Diarrhe
aARI
Fever
NA
-Mostm
othe
rscontinue
dfluids,-
40%:awareof
increasedfluids.
-53%
:gavemoreCFas
homecook
edmeals.
NA
NA
NA
NA
Mishraet
al,
1990
India
Diarrhe
aNA
NA
-60-66%
CFwas
givenas
usua
l,-27-30%
casesCF
mod
ified
tomak
efood
softas
norm
alfood
scan
triggerdiarrhea,-6.25%
CFwas
stop
pedto
help
child
recupe
rate
and
restrictingfood
redu
ces
stoo
ls.
-27%
to30%
cases:
speciald
ietswere
givento
sick
child
ren,-“
Hot”
food
sareavoide
d.
NA
NA
NA
Piechulek
etal,
1999
Ban
glad
esh
Diarrhe
a&
ARI
-BFcontinue
din
amajority,-22.2%
discon
tinue
dBFfor
diarrhea,-Reasons
forno
tBF&
giving
anim
almilk
:1)
Mothe
r’sbe
lieftha
tfluids
areha
rmful,
cann
otbe
absorbed
.Ano
ther
reason
for
restricting
breastmilk
2)Im
prov
emen
tsseen
indiminishe
dstoo
lvo
lume.
Diarrhe
a-Non
e:Increasedfluids,-
91.5%:con
tinue
dfluids,-0.8%
:stop
pedfluids,-
87%
Fluid
restriction
(diarrhe
a)an
d9.3%
(pne
umon
ia).
ARI-14.8%:
Restrictedfluids
until
fullrecovery.
-38%
:con
tinue
dCF,-
Non
e:increasedCF,-
>54.6%:restricted/
with
held
CF,-5
9.1%
restricted
fordiarrhea
&22.4%
forpn
eumon
ia,-
~30%
:stopp
edCFfor>
24hrs;of
thisasm
all
prop
ortio
nstop
pedun
tilchild
’srecovery,-
Mothe
rswith
hold
food
because1)
med
ical
advice;2)ow
nbe
liefo
f“k
eeping
bowelsat
rest”;
3)po
orap
petite,-
Edu
catedmothe
rsless
likelyto
with
hold
food
,-Foo
dqu
ality
mod
ified
to“cureillne
ss”.
-97%
mothe
rsgave
speciald
iettotheir
illchild
.According
totype
ofillne
ss,
certainfood
swere
avoide
dor
preferred,-Inall
illne
sses
food
slik
efish,m
eat&
vegetables
are
“avo
ided
”as
they
increase
loose
motions
orprolon
gdiseaseeffects,-
Speciald
iettocure
cold:w
arm
milk
&asyrupof
basil
“tulsi”leaves
(hot
food
s),-Sp
ecial
food
sto
cure
ARI/
-NA
-Man
ymothe
rswith
held
food
becauseof
doctors’
advice.
NA
(Con
tinues)
Infant feeding during and after illness in South Asia 57
© 2016 The Authors. Maternal & Child Nutrition published by John Wiley & Sons Ltd Maternal & Child Nutrition (2016), 12 (Suppl.1), pp. 39–71
Tab
le8.
(Con
tinue
d)
Finding
s
Disease
Breastfeeding
(BF)
Fluid
intake
Com
plem
entary
food
s(C
F)&
feed
ingpractices
Traditio
nalb
eliefs
andtheirrole
infeed
ing
practices
Com
mun
ityelde
rs/trad
ition
alpractitione
rs’
advice
Health
profession
als’
advice
Interpersona
lan
dgrou
pcoun
selling
Stud
y
pneu
mon
ia:foo
dsthat
aggravate
symptom
sof
cold
likefish,d
uckor
pigeon
meat;an
dba
nana
,green
papa
ya,g
reen
coconu
tand
some
vegetables
are
avoide
d,-S
pecial
food
sto
cure
diarrhea:raw
bana
na&
coconu
tredu
ceab
dominal
discom
fort&
diminishfreq
uency
ofstoo
ls,-Fish,
milk
,meat,or
vegetables
avoide
dby
~98%
othe
rsas
they
“increasethe
freq
uencyof
loose
motions”
(diarrhe
a).
Rashidet
al,
2001
Ban
glad
esh
ARI
NA
NA
-CFrestricted
andgiven
once
ada
y.-M
ostm
othe
rsmod
ified
child
ren’s
diets,-‘Coldfood
s’i.e.,leftov
eror
stale
food
swereavoide
das
“aggravate
pneu
mon
ia”,-O
nce
ada
y:on
lyrice
&saltor
drybread
was
prov
ided
and
-16%
mothe
rsweread
visedby
mothe
rs-in
lawto
restrict
certain
type
sof
food
,-Traditio
nala
ndallopa
thiccare
was
soug
htde
pend
ing
onthepe
rceived
NA
NA
(Con
tinues)
58 K. Paintal and V.M. Aguayo
© 2016 The Authors. Maternal & Child Nutrition published by John Wiley & Sons Ltd Maternal & Child Nutrition (2016), 12 (Suppl. 1), pp. 39–71

Tab
le8.
(Con
tinue
d)
Finding
s
Disease
Breastfeeding
(BF)
Fluid
intake
Com
plem
entary
food
s(C
F)&
feed
ingpractices
Traditio
nalb
eliefs
andtheirrole
infeed
ing
practices
Com
mun
ityelde
rs/trad
ition
alpractitione
rs’
advice
Health
profession
als’
advice
Interpersona
lan
dgrou
pcoun
selling
Stud
y
arede
prived
ofvegetables
&fruits.
severity
ofthe
illne
ss.
Shah
etal,
2011
India
Diarrhe
a-5
0%BF
continue
d,-4
9.3%
decreased/
stop
ped,-R
easons
forstop
ping
BF:
Ene
rgyde
nsefood
sthat
themothe
rsconsum
eissecreted
inthebreastmilk
that
thechild
cann
otdigest.
NA
NA
NA
29%
mothe
rsconsulted
trad
ition
almed
ical
practitione
rsor
quacks.
Sharma&
Tha
kur,1995
India
Diarrhe
aFever
NA
NA
-CFiscommon
lyrestricted
.-C
Fqu
ality
ismod
ified
,-Foo
dspreferreddu
ring
coug
han
dfever:
Cold&
light
food
si.e.,curd,fruits,
rice,sago,
barley,
andbiscuits.
NA
NA
Sing
het
al,
1994
India
Diarrhe
a-B
Fcontinue
din
mostc
ases.
NA
NA
-Feeding
was
not
with
held
but
chan
gesmad
ein
thena
ture
offood
sgivenwhich
varied
byillne
sstype
,Sp
eciald
ietsgiven
indiarrhea:-1)
daliya&
khitchri
because‘in
testines
becomeweak&
child
renareun
able
NA
NA
NA
(Con
tinues)
Infant feeding during and after illness in South Asia 59
© 2016 The Authors. Maternal & Child Nutrition published by John Wiley & Sons Ltd Maternal & Child Nutrition (2016), 12 (Suppl.1), pp. 39–71

Tab
le8.
(Con
tinue
d)
Finding
s
Disease
Breastfeeding
(BF)
Fluid
intake
Com
plem
entary
food
s(C
F)&
feed
ingpractices
Traditio
nalb
eliefs
andtheirrole
infeed
ing
practices
Com
mun
ityelde
rs/trad
ition
alpractitione
rs’
advice
Health
profession
als’
advice
Interpersona
lan
dgrou
pcoun
selling
Stud
y
todigesthe
avy
food
s”;-2)
Dilu
ted
tea&
bana
nato
freq
uencyof
stoo
ls;-3)
Cow
’smilk
as“evile
yeha
dcontam
inated
breastmilk
.-4)
Foo
dsavoide
dare
“whe
atflou
rbread”
&milk
asit
is“too
heavy”;and
“Hot
food
s’lik
eap
ple,man
go,
jaggery,ne
arly
all
pulses
asthese
coulden
hancethe
freq
uency&
intensity
ofdiarrhea.
Zeitly
net
al,
1993
Ban
glad
esh
Diarrhe
aNA
NA
->36%:restrictC
Fan
d64%
gave
norm
alho
me
cook
edmeals,-
With
holdingfood
isafirst
measure
totreat
diarrhea,-10%
stop
ped
CFto
give
bowelsarest,-
<25%:gaveCFas
usua
l.-Foo
disrestricted
asmothe
rsrecogn
izethat
child
renha
veredu
ced
appe
tites
&arereluctan
tto
forcefeed
toeat.
-Spe
cial
diets:
Normalfamily
diets
aremod
ified
tosoft
food
sto
aid
digestion,-F
oods
arerestricted
/mod
ified
dueto
cultu
raln
otions
“digestiv
epo
wer
inillne
ss”,-S
oftfoo
dsgivenchild
ren<10-
mon
thsas
mothe
rsbe
lieve
“illn
ess
-Afewmothe
rsrepo
rted
trad
ition
alpractitione
rsad
visedthem
towith
hold
food
swhe
ntheirchild
haddiarrhea,
includ
ing
breastmilk
,-Mothe
rsin
lawwas
themainsource
ofad
vice
tomothe
rson
homeremed
ies.
-Health
prov
iders
prov
ided
nutrition
relatedad
vice
onfeed
ingasick
child
during
illne
ss,-A
fewmothe
rsrepo
rted
that
health
prov
iders
advisedthem
towith
hold
food
swhe
ntheirchild
haddiarrhea,
(Con
tinues)
60 K. Paintal and V.M. Aguayo
© 2016 The Authors. Maternal & Child Nutrition published by John Wiley & Sons Ltd Maternal & Child Nutrition (2016), 12 (Suppl. 1), pp. 39–71

Tab
le8.
(Con
tinue
d)
Finding
s
Disease
Breastfeeding
(BF)
Fluid
intake
Com
plem
entary
food
s(C
F)&
feed
ingpractices
Traditio
nalb
eliefs
andtheirrole
infeed
ing
practices
Com
mun
ityelde
rs/trad
ition
alpractitione
rs’
advice
Health
profession
als’
advice
Interpersona
lan
dgrou
pcoun
selling
Stud
y
Working
mothe
rsdo
not
wan
ttoforcefeed
the
child
dueto
“tim
econstraints”-S
oftfoo
dsgivenchild
ren<10-
mon
thsas
mothe
rsbe
lieve
“illn
essw
eake
nsa
child
’sdigestivepo
wer
&softdietsin
theform
ofgrue
ls&
soup
sareeasier
todigest”.
weake
nsachild
’sdigestivepo
wer
&softdietsin
the
form
ofgrue
ls&
soup
sareeasier
todigest”,-M
aterna
lor
family
’spe
rcep
tions
of“h
otor
cold
food
s”an
dits
perceived
bene
ficial/h
armful
effects.-F
ishis
avoide
d:vehicle
attractin
g“evil”
forces
that
perpetua
teillne
ss.-
Cold&
stalefood
si.e.,food
scook
edseveralh
ours
earlierare
considered
breeding
grou
nds
forba
cteria.
includ
ing
breastmilk
.
BF,
breastfeed
ing;ARI,acuterespiratoryinspectio
n;NA,n
otap
plicab
le.
Infant feeding during and after illness in South Asia 61
© 2016 The Authors. Maternal & Child Nutrition published by John Wiley & Sons Ltd Maternal & Child Nutrition (2016), 12 (Suppl.1), pp. 39–71

studies reported that some mothers (range 6–28%)gave additional liquids/fluids to their children during ill-ness (Kaur et al. 1994; Das et al. 2013). Three studies re-ported that, in addition to water, mothers fed sickchildren home-made fluids such as watery porridgesmade from maize, rice or wheat; soups; sugar–salt–water solutions; and/or yogurt (Gupta & Gupta 2000;Gupta et al. 2007; Das et al. 2013). Six studies reportedthat mothers restricted the amount of liquids/fluidsgiven to sick children (Kaur & Singh 1994; Kaur et al.1994; Piechulek et al. 1999; Agha et al. 2007; Ansariet al. 2009; Das et al. 2013). Fluid restriction was morefrequent during diarrhoea episodes (range 4–87%)(Kaur & Singh 1994; Kaur et al. 1994; Piechulek et al.1999; Agha et al. 2007; Das et al. 2013) than during ep-isodes of fever or pneumonia (range 8.3–15%)(Piechulek et al. 1999; Gupta & Gupta 2000; Aghaet al. 2007). Only one study reported the reasons given
by mothers for restricting children’s fluid intake duringsickness (Piechulek et al. 1999); these were: (1) the be-lief that fluids could not be absorbed during diarrhoeaand thus were harmful; and (2) the perception that areduction in the stool volume in children withdiarrhoea was an improvement of the child’s condition.Two studies reported that the proportion of motherswho were aware that children need more fluids duringsickness ranged between 40% and 47% (Mangalaet al. 2000; Memon et al. 2010).
Complementary foods and feeding practices during and aftercommon childhood illnesses
Twenty studies (63%) investigated whether childrenwere fed lower, similar or larger amounts of soft,semi-solid or solid foods when they suffered fromcommon childhood illnesses. Thirteen studies reported
Table 9. Policies and programmes related to infant and young child feeding (IYCF) during and after illness in South Asian countries (1990–2014)
Afghanistan Bangladesh Bhutan India Nepal Maldives PakistanSriLanka
A national stand-alone policy for the protection,promotion and support of optimal IYCFpractices is available
Y X Y Y X X X Y
A national nutrition and/or food security policythat includes IYCF is available
Y X Y X Y X X X
The national IYCF/national nutrition/foodsecurity policy includes IYCF during and afterillness
X X X Y Y X X X
A national programme for the protection,promotion and support of optimal IYCFpractices exists
Y Y Y Y Y X Y Y
National guidelines for the protection,promotion and support of optimal IYCFpractices are available
Y Y Y Y Y Y Y Y
National guidelines for the protection,promotion and support of optimal IYCF includeIYCF during and after illness
X X Y Y X Y Y Y
The national training package for IYCFprotection, promotion and support includesIYCF during/after illness
X Y Y Y Y X X Y
A national programme for the integratedmanagement of childhood illness (IMCI) exists
Y Y Y Y Y Y Y Y
The national guidelines for IMCI includeguidance on feeding children when they are sick
Y Y Y Y X Y Y Y
The national guidelines for IMCI includeguidance on feeding children after being sick
Y Y Y Y X Y Y Y
The national training package on IMCI includesguidance on IYCF during and after illness
X Y X Y X Y X Y
Y: Yes, X: No
62 K. Paintal and V.M. Aguayo
© 2016 The Authors. Maternal & Child Nutrition published by John Wiley & Sons Ltd Maternal & Child Nutrition (2016), 12 (Suppl. 1), pp. 39–71

that children (range 25–79%) continued to be fed regu-lar family foods as usual, with no restrictions/changes infrequency and/or quantity (Becker et al. 1991;Badruddin et al. 1991; Malik et al. 1991; Ahmed et al.1992; Zeitlyn et al. 1993; Kaur et al. 1994; Bhuiya &Streatfield 1995; Gupta et al. 2007; Mangala et al.2000; Dongre et al. 2010; Memon et al. 2010; Dhadaveet al. 2012; Das et al. 2013).
However, a significant number of studies (18) indi-cated that feeding restrictions during common child-hood illnesses were frequent; these restrictionsaffected feeding frequency (4 studies: Mangala et al.2000; Dongre et al. 2010; Benakappa & Shivamurthy2012; Giri & Phalke 2014); food quality (11 studies:Mishra et al. 1990; Badruddin et al. 1991; Ahmed et al.1992; Zeitlyn et al. 1993; Sharma & Thakur 1995;Piechulek et al. 1999; Mangala et al. 2000; Agha et al.2007; Dongre et al. 2010; Benakappa & Shivamurthy2012;Giri& Phalke 2014); and/or food quantity (7 stud-ies: Kaur et al. 1994; Bhuiya & Streatfield 1995;Piechulek et al. 1999; Mangala et al. 2000; Agha et al.2007; Dhadave et al. 2012; Das et al. 2013). Food re-strictions seemed to be more common during diar-rhoea episodes (up to 83% of the mothersinterviewed) than during episodes of pneumonia andfever (up to 70% and 47% of the mothers interviewed,respectively). The reasons most commonly reported bymothers for restricting food intake when children weresick were: (1) caregivers’ perception that children hadless appetite or refused to eat/be fed (five studies:Zeitlyn et al. 1993; Kaur et al. 1994; Bhuiya &Streatfield 1995; Piechulek et al. 1999; Dongre et al.2010); (2) mothers’ reluctance to ‘force’ the child toeat (two studies: Zeitlyn et al. 1993; Bhuiya &Streatfield 1995); (3) mothers’ inability to feed the chil-dren more food/more frequently owing to resources(fuel) or time constraints (one study: Zeitlyn et al.1993); (4) mothers’ belief that illness ‘disturbed’ the di-gestive system and that feeding ‘normal’ foods washarmful to the sick child as the child’s digestive powerwas ‘diminished’ and ‘normal foods’would trigger diar-rhoea, produce cough and/or put stress on the child’sstomach (nine studies: Mishra et al. 1990; Ahmed et al.1992; Zeitlyn et al. 1993; Bhuiya & Streatfield 1995;Sharma & Thakur 1995; Mangala et al. 2000; Dongreet al. 2010; Benakappa & Shivamurthy 2012; Giri &
Phalke 2014); (5) mothers’ belief that withholdingcertain foods would help to cure diarrhoea whereasintroducing normal foods before the child was curedwould have a detrimental effect on the developmentof the child or would lead to a ‘big belly’ (threestudies: Mishra et al. 1990; Ahmed et al. 1992; Zeitlynet al. 1993); and/or (6) the belief that restricting foodintake was a first measure to manage diarrhoea athome and reduce the frequency of loose stools (fivestudies: Mishra et al. 1990; Zeitlyn et al. 1993;Piechulek et al. 1999; Dongre et al. 2010). Twostudies that measured food intake in sick children6–23months old reported that the mean energyintake of children was significantly lower than thatof healthy children and up to 70% below WHOrecommendations (Becker et al. 1991; Benakappa &Shivamurthy 2012). Two studies reported that somemothers (range 10–30%) ceased feeding their childfor 24 h or longer following medical advice, becausemothers perceived that the children had poor/noappetite and/or because social norms advised ‘to keepbowels at rest’ (Zeitlyn et al. 1993; Piechulek et al. 1999).None of the studies reported an increase in children’sfood intake (frequency, quantity and/or quality). Onlyfour studies assessed mothers’ knowledge about thefeeding needs of sick children; few mothers (range17–38%) recognized the importance of feeding sickchildren nutritious diets comprising vegetables, pulses,small fish and/or other nutrient-rich foods (Zeitlynet al. 1993; Piechulek et al. 1999; Agha et al. 2007;Benakappa & Shivamurthy 2012).
Traditional beliefs and their role in IYCF during and aftercommon childhood illnesses
Thirteen studies (41%) explored the importance of tra-ditional beliefs and perceptions on IYCF practices dur-ing and after common childhood illnesses. Nine studiesreported that when children were sick, caregivers(range 13–98%) replaced children’s usual diets with‘special diets’ owing to the belief that children’s usualdiets need to be modified to aid digestion ‘because in-testines become weak’ (Mishra et al. 1990; Ahmedet al. 1992; Zeitlyn et al. 1993; Dongre et al. 2010;Benakappa & Shivamurthy 2012; Giri & Phalke2014). Young children were often fed home remedies,
Infant feeding during and after illness in South Asia 63
© 2016 The Authors. Maternal & Child Nutrition published by John Wiley & Sons Ltd Maternal & Child Nutrition (2016), 12 (Suppl.1), pp. 39–71

herbal medicines and teas, and ‘soft foods’ in the formof soups and gruels (Badruddin et al. 1991; Zeitlynet al. 1993; Piechulek et al. 1999; Gupta & Gupta 2000;Dongre et al. 2010; Benakappa & Shivamurthy 2012;Giri & Phalke 2014) because they were perceived to‘be lighter on the stomach’, ‘be easier to digest’, ‘reduceabdominal pain’ and/or ‘diminish the frequency ofstools’. Conversely, foods like fish, milk, meat, fooditems containing oil or even vegetables were avoidedbecause they were considered ‘difficult to digest’ or‘too heavy to digest’ (Ahmed et al. 1992; Zeitlyn et al.1993; Piechulek et al. 1999; Giri & Phalke 2014).
Seven studies (Mishra et al. 1990; Zeitlyn et al. 1993;Piechulek et al. 1999; Rashid et al. 2001; Dongre et al.2010; Benakappa & Shivamurthy 2012; Giri & Phalke2014) reported that caregivers avoided giving specific‘hot’ or ‘cold’ foods to sick children because these foodswere considered inappropriate for certain diseases.Foods commonly avoided in case of diarrhoea wereeggs/meat (range 25% to >95%), roti/chapatti/wheatflour breads (~70%) and milk (47–50%); in case ofpneumonia, commonly avoided foods were fish/duck/pi-geon (>90%) or curd/buttermilk (range 76% to 93%);in case of fever, commonly avoided foods included rice(40%) and curd/butter milk (range 60–70%). Two stud-ies reported that some caregivers (range 16–23%)avoided giving sick children foods like fish, meat oreggs because ‘they attract evil forces’ and thus theywere harmful to children (Zeitlyn et al. 1993; Piechuleket al. 1999).
Community elders/traditional practitioners’ advice on IYCFduring/after childhood illnesses
Five studies (16%) reported on the role of mothers-in-law (four studies: Zeitlyn et al. 1993; Rashid et al. 2001;Kaushal et al. 2005; Gupta et al. 2007) or other family el-ders (Ahmed et al. 1992) on decision regarding IYCFpractices when children were sick. Common advicegiven by family elders to mothers when children weresick included the following: (1) to opt for home reme-dies as a first line of treatment (Zeitlyn et al. 1993;Gupta et al. 2007); (2) to accept children’s refusal toeat/be fed as ‘normal’ and delay feeding by one day(Kaushal et al. 2005); and/or (3) to refrain from givingsick children certain foods such as fish,meat, vegetablesor milk (Zeitlyn et al. 1993). Nine studies (28%)
reported that a varying proportion of mothers (range5.3–84%) sought help from traditional/unqualifiedpractitioners when their children were sick (Zeitlynet al. 1993; Kaur et al. 1994; Bhuiya & Streatfield 1995;Rashid et al. 2001; Bharti et al. 2006; Dongre et al.2010; Shah et al. 2011; Hirani 2012; Das et al. 2013).However, only one study described the role oftraditional/unqualified practitioners on IYCF counsel-ling to mothers when children were sick (Bhuiya &Streatfield 1995). This study reported that traditional/unqualified practitioners advised mothers to restrictchildren’s food intake; however, it did not provide spe-cific details on the types of foods that a mother shouldavoid when her child was sick.
Health professionals’ advice on IYCF during and after commonchildhood illnesses
Six studies (19%) investigated the role of health profes-sionals in providing IYCF advice to mothers when chil-dren were sick (Zeitlyn et al. 1993; Bhuiya & Streatfield1995; Kasi et al. 1995; Badruddin et al. 1997; Piechuleket al. 1999; Benakappa & Shivamurthy 2012). In gen-eral, health professionals gave little or no advice tomothers on how to feed their children during or afterthe illness episode: three studies reported that healthproviders (range 46–100%) advised mothers to con-tinue breastfeeding (Bhuiya & Streatfield 1995;Badruddin et al. 1997; Piechulek et al. 1999); two studiesreported that health providers (range 9–71%) advisedmothers to give oral rehydration solution/home-basedfluids to infants and young children suffering from diar-rhoea (Bhuiya & Streatfield 1995; Kasi et al. 1995). Nostudy reported that health providers advisedmothers toincrease fluid intake when children were sick. Similarly,no study reported that health providers advisedmothers to encourage their sick children to eat soft, var-ied and favourite foods during illness, as recommendedby WHO (WHO 2003a, 2003b). Conversely, two stud-ies (Zeitlyn et al. 1993; Bhuiya & Streatfield 1995) re-ported that health providers advised mothers(proportion not reported) to withhold breast milk andfoods such as rice and buttermilk (in case of diarrhoea),rice (in case of fever) or cold foods like curd, butter-milk, fruit juices and bananas (in case of pneumoniaor acute respiratory infections). Two studies reportedthat health professionals (range 7–62%) advised
64 K. Paintal and V.M. Aguayo
© 2016 The Authors. Maternal & Child Nutrition published by John Wiley & Sons Ltd Maternal & Child Nutrition (2016), 12 (Suppl. 1), pp. 39–71

mothers to feed their children soft and semi-solid foodsonly after children had recovered from the illness (Kasiet al. 1995; Benakappa & Shivamurthy 2012).
Interpersonal and group counselling on IYCF during/aftercommon childhood illnesses
Three studies (9%) – all in India – reported the impactof behaviour change communication interventions onmothers’ IYCF practices when children had diarrhoea(Kaur & Singh 1994; Kaur et al. 1994; Mangala et al.2000). Two studies reported the impact of home visitsand group counselling by trained community healthworkers. In these studies, the proportion of mothersgiving ‘less than usual’ amounts of food to their sickchildren declined from 98% to 35% and from 55% to29% (Kaur & Singh 1994; Kaur et al. 1994). The thirdstudy assessed the impact of cooking demonstrationsusing locally available foods and interpersonal counsel-ling sessions onmothers’ IYCF practices when childrenwere sick (Mangala et al. 2000). The results of the inter-vention indicated the following: (1) the proportion ofmothers who breastfed more frequently while childrenhad diarrhoea increased from 15% to 47%; (2) theproportion of mothers who modified family foods tomake them soft and digestible (i.e. more palatable)increased from 2% to 26%; and (3) the proportion ofmothers who fed their children additional food for atleast 2weeks after the diarrhoea episode increasedfrom 0% to 20%.
Review of national policy and programmeframeworks for infant and young child feedingduring and after common childhood illnesses
We reviewed national policy and programme docu-ments to assess whether national frameworks formaternal and child nutrition integrate IYCF duringand after illness. In addition, we conducted interviewswith 13 key informants to document the existingnational programmes that protect, promote andsupport optimal IYCF practices for children duringand after illness (Table 9).
Five of the eight countries have a national IYCF pol-icy, either as a stand-alone policy framework on infantfeeding or as part of a larger policy framework onnutrition/food security. However, only two countries –
India and Nepal – have integrated the feeding needsof children during and after illness in their IYCF policyframework.
All countries have national guidelines on IYCF,and seven countries have a national programme forthe protection, promotion and support of optimalIYCF. However, only five countries include in theirnational IYCF guidelines guidance on how childrenshould be fed during and after illness, and only fivecountries have developed a training package onIYCF for programme staff that includes IYCF forchildren during and after illness.
All countries have a national programme for theintegrated management of childhood illnesses (IMCI);six countries have national IMCI guidelines thatinclude guidance on feeding children during and after ill-ness; however, only four countries have developed anIMCI training package that includes guidance on howto feed children when they are sick and after being sick.
Discussion
We conducted a comprehensive review of the availableevidence on IYCF practices during and after commonchildhood illnesses – diarrhoea, fever and pneumonia– in South Asia (1990–2014) to inform policy formula-tion, programme design, advocacy and research priori-tization to protect, promote and support optimal IYCFpractices during and after common childhood illnessesin South Asia post 2015.
Demographic Health Survey data on IYCF duringcommon childhood illnesses were available only forBangladesh, India, Nepal and Pakistan, which arehome to ~96% of the children under 5 years of age inSouth Asia (UNICEF 2015). Similarly, the 32 publica-tions that met the inclusion criteria of our reviewfocused on these four countries. Furthermore, theavailableDHS data in these four countries were limitedto IYCF during diarrhoea episodes. No survey datawere available on IYCF practices after episodes of diar-rhoea or during/after episodes of fever or pneumonia.Similarly, the published research was primarily focusedon IYCF practices during diarrhoea and to a lesserextent during fever or pneumonia episodes. Researchevidence on IYCF after common childhood illnesseswas practically inexistent.
Infant feeding during and after illness in South Asia 65
© 2016 The Authors. Maternal & Child Nutrition published by John Wiley & Sons Ltd Maternal & Child Nutrition (2016), 12 (Suppl.1), pp. 39–71

Demographic Health Survey data indicate that in thecountries included in the analysis, children 0–23monthsold suffer from common childhood illnesses frequently,as nearly one-third of the mothers/caregivers reportedthat their children had suffered from diarrhoea or pneu-monia in the 2weeks prior to the survey. These findingsare in line with reports indicating that 39% of childdeaths in South Asia are due to diarrhoea and/or pneu-monia (UNICEF 2012). Importantly, DHS data indicatethat in all the countries included in our review, the occur-rence of diarrhoea, pneumonia and fever was lowestduring the exclusive breastfeeding period (0–5months)and highest during the early complementary feeding pe-riod (6–11months). This is most likely due to thewell-documented protective benefits of exclusive/predominant breastfeeding in the first 6months of lifeand the higher levels of infection in late infancy and earlychildhood due to children’s increased intake of comple-mentary foods and fluids that may be contaminated aswell as the ingestion of faecal bacteria throughmouthingsoiled fingers or household items when children begin tocrawl and explore their environment (Kosek et al. 2003;Dewey & Mayers 2011; WHO 2013).
Our review shows that in South Asia, IYCF behav-iours and practices during common childhood illnessesare far from optimal. Most infants and young childrencontinue to be breastfed when they are sick; however,few children (<20%) are breastfed more frequently asrecommended. Studies in other settings have reporteda similar practice, as most mothers continue tobreastfeed their sick children without altering the num-ber of nursing episodes, total amount of time of sucklingor energy derived from breast milk (Hoyle et al. 1980;Brown et al. 1990;Martz &Tomkins 1995; Brown 2003).
Similarly, most sick children continue to be fed fluids.However, few children (range 7.4–21.7% in Pakistanand Bangladesh, respectively) were fed fluids morefrequently as recommended. Mothers’ awarenessabout children’s need for more fluids during sicknessis low. This evidence is in line with reports indicatingthat in developing countries, less than a quarter(22%) of children are fed more fluids during illness(UNICEF/WHO 2009). Conversely, a significant pro-portion of mothers/caregivers in Bangladesh (26.7%),Pakistan (37.9%) and India (42.2%) fed their sick chil-dren less fluids than usual or no fluids at all in contrast
with reports from other countries (Bani et al. 2002;Saha et al. 2013).
We find that food restrictions are frequent. Manychildren were fed lower quantities and/or less fre-quently when they were sick. As many as 36% ofmothers/caregivers in Bangladesh, 41% in Pakistanand 43% in India reported that they fed their childrenless food than usual or no food at all during the last di-arrhoea episode. Only one-third (34%) of the mothers/caregivers in India to about half (55%) in Nepal re-ported that they fed their children same/similaramounts of food as usual during the diarrhoea episode.Studies in Latin America have indicated that anorexiais an important factor in the reduction of children’sdietary intake during illness (particularly whendiarrhoea or fever are present) as mothers/caregiverstend to give in when sick children send a ‘food reject’signal (Bentley et al. 1991, 1995). The combined effectsof anorexia and tradition-driven withdrawal of comple-mentary feeding during common childhood illnessescan be devastating (Scrimshaw & Sangiovanni 1997).
Our review indicates that in South Asian countries,mothers’/caregivers’ knowledge about the feedingneeds of sick children is limited and that feeding prac-tices are often guided by traditional beliefs and normsthat encourage the use of ‘special’ foods/diets to replace‘usual diets’ when children are sick. Similarly, manycaregivers seem to avoid giving certain ‘hot’ or ‘cold’foods to sick children because these foods are consid-ered inappropriate for specific diseases. Studies havereported that deeply held beliefs and traditionsdetermine the types of foods or preparation methodsthat are ‘healthy’ or ‘unhealthy’ for sick children, whenand what types of complementary foods are given tochildren and how to feed children who are sick and/ordo not want to eat. These beliefs are heavily influencedby the individuals who surround mothers – that is,husbands, mothers-in-law, grandmothers and otherfamily/community members – and the health care pro-viders upon whom caregivers depend for support(Martz & Tomkins 1995; Stewart et al. 2013).
Care-seeking practices in South Asia are said to bebelow global estimates for low-income and middle-income countries (Walker et al. 2012). However, thelatest DHS data available for the countries included inour review indicate that a significant proportion of
66 K. Paintal and V.M. Aguayo
© 2016 The Authors. Maternal & Child Nutrition published by John Wiley & Sons Ltd Maternal & Child Nutrition (2016), 12 (Suppl. 1), pp. 39–71

mothers/caregivers (ranging from 30% to 84%depend-ing on country and illness) took their sick children formedical advice during the last episode of diarrhoea,fever or pneumonia. Our review shows that fewpublished studies have investigated the quality ofhealth providers’ counselling on IYCF to mothers/caregivers when children are sick. The evidencereviewed indicates that when mothers/caregivers seekadvice/support in the primary health care system,health professionals provide little or no advice tomothers/caregivers on how to feed children when theyare sick/convalescent. In general, health providers donot advise mothers to increase children’s fluid intakeand encourage sick children to eat soft, varied andfavourite foods during illness, while increasingbreastfeeding frequency as is recommended. More-over, there is indication that a non-negligible propor-tion of health providers advise mothers to withdrawbreast milk and/or specific nutritious foods/all comple-mentary foods until children recover from illness.
Studies in other low-income and middle-incomecountries have found the following: (1) health workersdo not maximize their contacts with women andchildren to support optimal IYCF; (2) there is poorknowledge among health practitioners on how to feedand/or manage sick children and manage children withpoor appetite; (3) even when a national normative andguidance frameworks on IYCF for sick children are inplace, a limited proportion of paediatricians and familypractitioners follow them; and (4) the quality of careand advice among private practitioners is not necessar-ily better than among public health system providers(Bezerra et al. 1992; Bojalil et al. 1998; Baker et al.2013; Lutter et al. 2013).
Conclusion
Diarrhoea and pneumonia remain the leading infec-tious causes of childhood morbidity and mortality inSouth Asia (Fischer et al. 2013). Compelling evidenceindicates that childhood diarrhoea and pneumoniadeaths are avoidable and that scaling up optimalfeeding behaviours and practices in combination withappropriate case management can avoid most of thesedeaths (Bhutta et al. 2013).
Our review shows that information of IYCF behav-iours and practices during illnesses in South Asia islimited while information of IYCF after common child-hood illnesses is virtually inexistent. The evidencereviewed indicates that in South Asia, IYCF behav-iours and practices during common childhood illnessesare far from optimal. In general, sick children continueto be breastfed. However, few are breastfed morefrequently to compensate for the additional fluid andnutrient requirements associated with illnesses, whilea significant proportion of children is breastfed lessfrequently than usual. Restriction or withdrawal ofcomplementary foods during illness is frequent becauseof children’s anorexia (perceived or real), poorawareness by caregivers’ about the feeding needs ofsick children, traditional beliefs and behaviours,and/or suboptimal counselling and support by healthworkers. As a result, many sick children are fed lessfrequently and/or lower quantities of complementaryfoods.
Mothers/caregivers often turn to family/communityelders and traditional/non-qualified practitioners toseek advice on how to feed their sick children. Thus,traditional beliefs and behaviours often guide the useof ‘special’ feeding practices, foods and diets for sickchildren. Our review indicates that when children aresick, a significant proportion of families turn to theprimary health care system for advice and support. Ingeneral, health professionals give little or no advice tomothers/caregivers on how to feed their children whilethey are sick. However, the few intervention studiesavailable indicate that inter-personal and groupcounselling as part of primary health care can substan-tially improve mothers’ IYCF knowledge and practicesduring common childhood illnesses.
Global guidance and normative frameworks are inplace to address the feeding of sick children duringand after illness (WHO 2003a, 2003b; WHO/UNICEF2003; WHO 2005). All the countries included in ourreview have national guidelines on IYCF and a nationalprogramme for the IMCI. However, there seem to beimportant policy, guidance and capacity building gaps inthese frameworks with respect to IYCF when childrenare sick or convalescent. Our review indicates that alimited proportion of health practitioners follows allaspects of these guidance.
Infant feeding during and after illness in South Asia 67
© 2016 The Authors. Maternal & Child Nutrition published by John Wiley & Sons Ltd Maternal & Child Nutrition (2016), 12 (Suppl.1), pp. 39–71

In light of our findings, it seems reasonable to recom-mend the following as away forward to protect, promoteand support optimal IYCF practices during and aftercommon childhood illnesses in South Asia post 2015:
1. align national policy frameworks and programmaticguidance with internationally agreed upon recom-mendations on IYCF during and after commonchildhood illnesses, with a particular emphasis ondiarrhoea, fever and pneumonia;
2. expand the DHS and National Nutrition Surveys toinclude quantitative information on IYCF duringand after common childhood illnesses, with appro-priate geographic, socio-economic and genderdisaggregation;
3. collect qualitative and quantitative information oncaregivers’ behaviours and health workers’ prac-tices related to IYCF during and after commonchildhood illnesses to identify the most importantdrivers of current behaviours/practices and bottle-necks to optimal IYCF when children aresick/convalescent;
4. build the capacity of facility-based and community-based health workers to provide mothers/caregiverswith timely and accurate information, counsellingand support on IYCF when children are sick/convalescent;
5. design and implement effective communication strat-egies that combine interpersonal communicationand mass communication to address harmful beliefsand norms with respect to the nutrient and feedingneeds of children during/after common illnesses; and
6. document the effectiveness, impact and lessonslearned of the capacity building and communicationstrategies to improve IYCF during and after com-mon childhood illnesses and their implications forprogramme scale up and universalization.
Acknowledgements
The authors acknowledge inputs and feedback to thepreliminary drafts of this paper by the following indi-viduals: Aishnath Shahula Ahmed, Anirudra Sharma,France Begin, Gayatri Singh, Isabel Vashti Simbeye,Mohsin Ali, Pravin Khobragade, Renuka Jayatissa,Sherin Varkey, Tania Goldner and Wisal Khan.
Source of funding
TheUNICEFRegional Office for South Asia providedsupport for data analysis and paper writing. This re-search received no specific grant from any fundingagency in the commercial sector.
Conflicts of interest
The authors declare that they have no conflicts of inter-est. The opinions expressed on this paper are those ofthe authors and do not necessarily represent an officialposition of UNICEF.
Contributions
VMA designed the study, KP led data analysis. Bothauthors contributed equally to data interpretation andmanuscript writing and have read and approved thefinal submission.
References
AghaA.,White F., YounusM., KadirM.M., Alir S.& Fatmi Z.(2007) Eight key household practices of integrated manage-ment of childhood illnesses (IMCI) amongst mothers of chil-dren aged 6 to 59 months in Gambat, Sindh, Pakistan.Journal of Pakistan Medical Association 57 (6), 288–293.
Ahmed M.U., Rashid M. & Beguin S. (1992) Diarrhea andfeeding practices of young children attending two selectedurban clinics in Dhaka. Journal of Diarrheal DiseaseResearch 10 (4), 217–220.
Ansari M., Palaian S., IzhamM. & IbrahimM. (2009) The roleof mothers in the management of childhood diarrhea inNepal. Australasian Medical Journal 1 (14),235–238.
Badruddin S.H., Islam A., Hendricks K.M., Bhutta Z.A.,Shaikh S., Snyder J.D. et al. (1991) Dietary risk factors associ-atedwith acute and persistent diarrhea in children inKarachi,Pakistan.American Journal of Clinical Nutrition 54, 745–749.
Badruddin S.H., Inam S.N., Ramzanali S. & Hendricks K.(1997)Constraints to adoption of appropriate breast feedingpractices in a squatter settlement in Karachi, Pakistan.Journal of Pakistan Medical Association 47 (2), 63–68.
Baker J., Sanghvi T., Hajeebhoy N., Martin L. & Lapping K.(2013) Using an evidence-based approach to design large-scale programs to improve infant and young child feeding.Food and Nutrition Bulletin 34 (3), S146–S155.
Bani I.A., Saeed A.A.W., Mohammed A.A. & Othman A.I.(2002)Diarrhea and child feeding practices in Saudi Arabia.Public Health Nutrition 5 (6), 727–731.
68 K. Paintal and V.M. Aguayo
© 2016 The Authors. Maternal & Child Nutrition published by John Wiley & Sons Ltd Maternal & Child Nutrition (2016), 12 (Suppl. 1), pp. 39–71

Becker S., BlackR.E. &BrownK.H. (1991) Relative effects ofdiarrhea, fever, and dietary energy intake on weight gain inrural Bangladeshi children. American Journal of ClinicalNutrition 53, 1499–1503.
Benakappa A.D. & Shivamurthy P. (2012) Beliefs regardingdiet during childhood illness. Indian Journal of CommunityMedicine 37, 20–24.
Bentley M.E., Stallings R.Y., FukumotoM. & Elder J.A. (1991)Maternal feeding behavior and child acceptance of foodduring diarrhea, convalescence, and health in the CentralSierra of Peru. American Journal of Public Health 81, 43–47.
BentleyM.E., BlackM.M. &Hurtado E. (1995) Child-feedingand appetite: what can programmes do? Food and NutritionBulletin 16 (2), 70–82.
Bezerra J.A., Stathos T.H., DuncanB.,Gaines J.A.&Udall J.N.(1992) Treatment of infants with acute diarrhea: what isrecommended and what is practiced. Pediatrics 90, 1–4.
Bharti B., Bharti S. & Verma V. (2006) Severe pneumonia in aremote hilly area. Integrated management of childhoodillness. Indian Journal of Pediatrics 73 (1), 33–37.
Bhuiya A. & Streatfield K. (1995) Feeding, home-remedypractices, and consultationwith health care providers duringchildhood illness in rural Bangladesh. Journal of DiarrhealDisease Research 13 (2), 106–112.
Bhutta Z.A. & SalamR.A. (2012) Global nutrition epidemiol-ogy and trends. Annals of Nutrition and Metabolism 61 ,19–27.
Bhutta Z.A., Das J.K., Walker N., Rizvi A., Campbell H.,Rudan I., Black R.E. & for the Lancet Diarrhea andPneumonia Interventions StudyGroup. (2013) Interventionsto address deaths from childhood pneumonia and diarrheaequitably: what works and at what cost? Lancet 381,1417–1429.
Bojalil R., Guiscafre H., Espinosa P., Martinez H., Palafox M.,Romero G. et al. (1998) The quality of private and primaryhealth care management of childrenwith diarrhea and acuterespiratory infections in Tlaxcala,Mexico.Health Policy andPlanning 13 (3), 323–331.
Brown K.H. (2003) Diarrhea and malnutrition. Journal of Nu-trition 133, 328S–332S.
Brown K.H., Stallings R.Y., de Kanashiro H.C., de Romana G.L.& Black R.E. (1990) Effects of common illnesses oninfants’ energy intakes from breastmilk and other foodsduring longitudinal community-based studies in Huascar(Lima), Peru. American Journal of Clinical Nutrition 52,1005–1013.
Das S.K., NasrinD.,Ahmed S.,WuY., Ferdous F., FarzanaF.D.et al. (2013) Health care-seeking behavior for childhooddiarrhea in Mirzapur, rural Bangladesh. American Journalof Tropical Medicine and Hygiene 89 (1), 62–68.
De Onis M., Onyango A., Borghi E., Siyam A., Blössner M.& Lutter C. (2012) Worldwide implementation of theWHO Child Growth Standards. Public Health Nutrition15, 1603–1610.
De Onis M., Dewey K.G., Borghi E., Onyango A.W.,Blössner M., Daelmans B. et al. (2013) The World HealthOrganization’s global target for reducing childhoodstunting by 2025: rationale and proposed actions.Maternaland Child Nutrition 9 (Suppl. 2), 6–26.
Dewey K.G. & Mayers D.R. (2011) Early child growth: howdo nutrition and infection interact? Maternal & ChildNutrition 7 (Suppl. 3), 129–142.
Dhadave M.M., Kumar G.A., Reddy S., Vijayanath V. (2012)A study on diarrhea related practices. Awareness of ORSamong mothers of under-five children attending OPD,CHTC, Rajapur. Journal of Pharmaceutical and BiomedicalSciences 19 (11), 1–5.
Dibley M.J., Roy S.K., Senarath U., Patel A., Tiwari K.,Agho K.E. et al. (2010) Across-country comparisons ofselected infant and young child feeding indicators andassociated factors in four South Asian countries. Food andNutrition Bulletin 31 (2), 366–375.
Dongre A.R., Deshmukh P.R. & Garg B.S. (2010) Childhoodmorbidity, household practices and health care seeking forsick children in a tribal district of Maharashtra, India. IndianJournal of Medical Sciences 64, 7–16.
Fischer W.C.L., Rudan I., Liu L., Nair H., Theodoratou E.,Bhutta Z.A. et al. (2013) Global burden of childhoodpneumonia and diarrhea. Lancet 381, 1405–1416.
Giri P.A. & PhalkeD.B. (2014) Beliefs and practices regardingdiet in common childhood illnesses among rural caregivers.Journal of Medical Nutrition and Nutraceuticals 3, 219–221.
Grantham-McGregor S., Cheung Y.B., Cueto S., Glewwe P.,Richter L. & Strupp B. (2007) Developmental potential inthe first five years for children in developing countries.Lancet 369, 60–70.
Gulati J.K. (2010) Child malnutrition. Trends and issues.Anthropologist 12 (2), 131–140.
Gupta R.K. & Gupta R. (2000) First action management ofacute diarrhea in children by rural mothers. JK Science,Journal of Medical Education and Research 2 (2), 96–98.
Gupta N., Jain S.K., Chawla U., Hossain S. & Venkatesh S.(2007) An evaluation of diarrheal diseases and acute respi-ratory infections control programmes in a Delhi slum.Indian Journal of Pediatrics 74 (5), 471–476.
Hirani S.A.A. (2012)Malnutrition in young Pakistani children.A review article. Journal of Ayub Medical College 24 (2),150–153.
Hoyle B., Yunus M. & Chen L.C. (1980) Breast-feedingand food intake among children with acute diarrhealdisease. American Journal of Clinical Nutrition 33 (1),2365–2371.
Huffman S.L. & Combest C. (1990) Role of breast-feeding inthe prevention and treatment of diarrhea. Journal ofDiarrheal Disease Research 8 (3), 68–81.
Jones A.D., Ickes S.B., Smith L.E., Mbuya M.N.N.,Chasekwa B., Heidkamp R.A. et al. (2014) World HealthOrganization infant and young child feeding indicators and
Infant feeding during and after illness in South Asia 69
© 2016 The Authors. Maternal & Child Nutrition published by John Wiley & Sons Ltd Maternal & Child Nutrition (2016), 12 (Suppl.1), pp. 39–71

their associations with child anthropometry: a synthesis ofrecent findings.Maternal and Child Nutrition 10, 1–17.
Kasi M., Kausar P., Naz R. & Miller L.C. (1995) Treatmentof diarrhea in infants by medical doctors in Balochistan,Pakistan. Journal of Diarrheal Disease Research 13 (4),238–241.
Kaur P. & Singh G. (1994) Food practices during diarrhea.Indian Journal of Public Health 38 (2), 58–61.
Kaur A., Chowdhury S. & Kumar R. (1994) Mothers’ beliefsand practices regarding prevention and management of di-arrheal diseases. Indian Pediatrics 31 (1), 55–57.
Kaushal M., Aggarwal R., Singal A., Shukla H., Kapoor S.K.& Paul V.K. (2005) Breastfeeding practices and health-seeking behavior for neonatal sickness in a rural community.Journal of Tropical Pediatrics 51 (6), 366–376.
KosekM., Bern C. &Guerrant R.L. (2003) The global burdenof diarrheal disease, as estimated from studies published be-tween 1992 and 2000.Bulletin of theWorldHealthOrganiza-tion 81 (3), 197–204.
Lutter C.K., Iannotti L., Creed-Kanashiro H., Guyon A.,Daelmans B., Robert R. et al. (2013) Key principles to im-prove programmes and interventions in complementaryfeeding. Maternal and Child Nutrition 9 (2), 101–115.
Malik I.A., Azim S., Good M.J., Iqbal M., Nawaz M.,Ashraf L. et al. (1991) Feeding practices for young Pakistanichildren: usual diet and diet during diarrhea. Journal ofDiarrheal Disease Research 9 (3), 213–218.
Mangala S.,GopinathD., NarasimhamurthyN.S.&ShivaramC.(2000) Feeding practices in under-fives during diarrheabefore and after educational intervention. Indian Pediatrics37, 312–314.
Martz H. & Tomkins A.M. (1995) Nutritional management ofdiarrhea. Food and Nutrition Bulletin 16 (4), 349–355.
Memon P. (2012) The crisis of poor complementary feedingin South Asia: where next? Maternal and Child Nutrition8 (1), 1–4.
Memon S., Shaikh S., Kousar T. & Memon Y. (2010)Assessment of infant feeding practices at a tertiary carehospital. Journal of Pakistan Medical Association 60 (12),1010–1015.
Mishra C.P., Kumar S., Tiwari I.C. & Prasad D.N. (1990) Astudy on some diarrhea related practices in urbanMirzapur.Indian Journal of Public Health 34 (1), 6–10.
Neumann C.G., Marquardt M. & Bwibo N.O. (2012) The im-pact of morbidity on food intake in rural Kenyan children.South African Journal of Clinical Nutrition 25 (3), 142–148.
Piechulek H., Aldana J.M., Engelsmann B. & Hasan M.N.(1999) Dietary management during pregnancy, lactationand common childhood illnesses in rural Bangladesh.South-East Asian Journal of Tropical Medicine and PublicHealth 30 (2), 299–306.
Ramachandran P. & Gopalan H.S. (2009) Undernutrition andrisk of infections in preschool children. Indian Journal ofMedical Research 130 (11), 579–583.
Rashid S.F., Hadi A., Afsana K. & Begum S.A. (2001) Acuterespiratory infections in rural Bangladesh: cultural under-standings, practices and the role of mothers and communityhealth volunteers. Tropical Medicine and InternationalHealth 6 (4), 249–255.
Richard S.A., Black R.E., Gilman R.H., Guerrant R.L.,Kang G., Lanata C.F. et al. (2014) Catch-up growth occursafter diarrhea in early childhood. Journal of Nutrition144 (6), 965–971.
SahaD.,AkinsolaA., SharplesK.,AdeyemiM.O.,AntonioM.,Imran S. et al. (2013) Health care utilization and attitudessurvey: understanding diarrheal disease in rural Gambia.American Journal of Tropical Medicine and Hygiene89 (1), 13–20.
Scrimshaw N.S. & Sangiovanni J.P. (1997) Synergism of nutri-tion, infection, and immunity: an overview. American Jour-nal of Clinical Nutrition 66, 464S–477S.
SenarathU., AghoK.E., AkramD.-e.-S., Godakandage S.S.P.,Hazir T., Jayawickrama H. et al. (2012) Comparisons ofcomplementary feeding indicators and associated factors inchildren aged 6–23months across five South Asian coun-tries.Maternal and Child Nutrition 8 (1), 89–91.
Shah M.S., Ahmad A., Khalique N., Khan I.M., Ansari M.A.& Khan Z. (2011) Do the mothers in rural Aligarh knowabout home based management of acute diarrhea? Biologyand Medicine S3 (2), 76–80.
SharmaK.P. & Thakur A.K. (1995)Maternal beliefs regardingdiet during common childhood illnesses. Indian Pediatrics32 (8), 909–910.
Singh M.B. (1994) Maternal beliefs and practices regard-ing the diet and use of herbal medicines during measlesand diarrhea in rural areas. Indian Pediatrics 31 (3),340–343.
Stewart C.P., Iannotti L., Dewey K.G., Michaelsen K.F. &Onyango A.W. (2013) Contextualizing complementaryfeeding in a broader framework for stunting prevention.Maternal and Child Nutrition 9 (S2), 27–45.
UNICEF (2012) Pneumonia and diarrhea. Tackling thedeadliest diseases for the world’s poorest children. UnitedNations Children’s Fund, New York, New York.
UNICEF (2015) The state of the world children. Reimaginethe future: Innovation for every child. United Nation’sChildren’s Fund, New York; 116 pp.
UNICEF/WHO (2009) Diarrhea: why children are still dyingand what can be done? United Nations Children’s Fund,World Health Organization UNICEF/ WHO. New York.
Walker S.P., Wachs T.D., Gardner J.M., Lozoff B., WassermanG.A., Pollitt E. et al. (2007). Child development.Risk factorsfor adverse outcomes in developing countries. Lancet 369,145–157.
Walker C.L.F., Perin J., Aryee M.J., Boschi-Pinto C. &Black R.E. (2012) Diarrhea incidence in low- and middle-income countries in 1990 and 2010: a systematic review.BioMedCentral Public Health 12, 220–227.
70 K. Paintal and V.M. Aguayo
© 2016 The Authors. Maternal & Child Nutrition published by John Wiley & Sons Ltd Maternal & Child Nutrition (2016), 12 (Suppl. 1), pp. 39–71

Walker C.L.F., Rudan I., Liu L., Nair H., Theodoratou E.,Bhutta Z.A. et al. (2013) Global burden of childhoodpneumonia and diarrhea. Lancet 381 (9875), 1405–1416.
WHO (2003a) The guiding principles for complementaryfeeding of the breastfed child. World Health Organization,Geneva, Switzerland.
WHO (2003b) The guiding principles for complementary feed-ing of the non-breastfed child. World Health Organization,Geneva, Switzerland.
WHO (2005) Technical updates of the guidelines on the inte-grated management of childhood illness (IMCI). Evidenceand recommendations for further adaptations. WorldHealth Organization, Geneva, Switzerland.
WHO (2008) Indicators for assessing infant and young childfeeding practices. Part I: definitions. World HealthOrganization Geneva, Switzerland.
WHO (2010) Indicators for assessing infant and young childfeeding practices. Part II: measurement. World HealthOrganization Geneva, Switzerland.
WHO (2013) Essential nutrition actions. Improving maternal,newborn, infant and young child health and nutrition.WorldHealth Organization, Geneva, Switzerland.
WHO/UNICEF (2003) Global strategy for infant and youngchild feeding. World Health Organization and UnitedNations Children’s Fund, Geneva.
Zeitlyn S., Rowshan R., Mahalanabis D. & Faruque A. (1993)The ethno-physiology of digestion and diarrhea in aBangladeshi hospital population. Journal of DiarrhealDisease Research 11 (4), 243–248.
Infant feeding during and after illness in South Asia 71
© 2016 The Authors. Maternal & Child Nutrition published by John Wiley & Sons Ltd Maternal & Child Nutrition (2016), 12 (Suppl.1), pp. 39–71





























