Embed Size (px)
Citation preview

GENES, CHROMOSOMES & CANCER 49:935–947 (2010)
Feasibility of Differential Diagnosis of Kidney Tumorsby Comparative Genomic Hybridization ofFine Needle Aspiration Biopsies
Joana Vieira,1 Rui Henrique,2,3 Franclim R. Ribeiro,1 Joao D. Barros-Silva,1 Ana Peixoto,1
Catarina Santos,1 Manuela Pinheiro,1 Vera L. Costa,1 Maria J. Soares,1 Jorge Oliveira,4
Carmen Jeronimo,1,3 and Manuel R. Teixeira1,3*
1Departmentof Genetics,Portuguese Oncology Institute,Porto,Portugal2Departmentof Pathology,Portuguese Oncology Institute,Porto,Portugal3Departmentof Pathology and Molecular Immunology,Abel Salazar Biomedical Sciences Institute (ICBAS),Universityof Porto,Portugal4Departmentof Urology,Portuguese Oncology Institute,Porto,Portugal
The association of a genetic analysis that could improve the diagnostic accuracy of renal cell tumors in biopsy samples
would allow better-informed therapeutic decisions. We performed comparative genomic hybridization (CGH) on an ex
vivo fine-needle aspiration (FNA) biopsy and a tumor fragment obtained from 75 patients consecutively diagnosed with re-
nal tumors and subjected to radical nephrectomy. The pattern of genomic changes by CGH was used blindly to classify the
renal tumors and the genetic findings were subsequently compared with the histopathologic diagnosis. In particular cases,
including in two carcinomas with morphologically distinct tumor areas, we performed FISH with several locus-specific
probes, and looked for VHL point mutations, exonic rearrangements, or promoter methylation. CGH was successful in
82.7% FNA biopsies and in 96% tumor fragments, with the former allowing genetic diagnosis in 75% of renal cell tumors.
The genetic and the initial histological classification differed in two renal neoplasias, but the genetic diagnosis was con-
firmed after review. The genetic pattern correctly diagnosed 93.5% of clear cell renal cell carcinomas (RCC), 61.5% of
chromophobe RCC, 100% of papillary RCC, and 14.3% of oncocytomas, with the negative predictive value being 93.9,
90.7, 100, and 90.2%, respectively. The positive predictive value and specificity of copy number profiles was 100%. We
demonstrate that genetic diagnosis by CGH on FNA biopsies can improve differential diagnosis in patients with kidney
tumors. VVC 2010 Wiley-Liss, Inc.
INTRODUCTION
The histological classification of epithelial kid-
ney neoplasias was traditionally based on the type
of nephron cell from which it was originated (clear
cell, chromophilic, or chromophobe carcinoma)
and its growth pattern (papillary or nonpapillary).
However, overlapping morphological characteris-
tics can make difficult the differential diagnosis of
a small, but significant, number of renal tumors,
even to highly experienced pathologists analyzing
nephrectomy samples (Young et al., 2006; Liu
et al., 2007; Cheng et al., 2009). From a genetic
point of view, most clear cell RCC display losses
at chromosome arm 3p, papillary RCC present
multiple whole chromosome gains (usually of
chromosomes 7, 12, 16, 17, and 20), whereas chro-
mophobe RCC often show several whole chromo-
some losses (namely of chromosomes 1, 2, 6, 10,
13, 17, 21, X, and/or Y) and oncocytomas may have
loss of 1p, 14, or Y, translocations involving 11q13,
gain of 11q, or a normal karyotype (Speicher et al.,
1994; Bugert et al., 1997; Jhang et al., 2004; Zans-
sen et al., 2004; Brunelli et al., 2005; Fuzesi et al.,
2005). These characteristic patterns of genomic
changes are nowadays incorporated in the classifi-
cation of renal cell tumors (Young et al., 2006;
Cheng et al., 2009). About 6–7% of renal carcino-
mas remain unclassified based on morphology,
including a significant proportion of kidney carci-
nomas of children and young adults that bear spe-
cific chromosome translocations involving the
TFE3/TFEB genes (Teixeira, 2006).
Conflict of Interest: The authors declare no conflict of interests.
Supported by: Ministerio da Saude; Liga Portuguesa Contra oCancro—Nucleo Regional do Norte.
*Correspondence to: Manuel R. Teixeira, Department ofGenetics, Portuguese Oncology Institute, Rua Dr. Antonio Bernar-dino Almeida, 4200-072 Porto, Portugal.E-mail: [email protected]
Received 13 January 2010; Accepted 9 June 2010
DOI 10.1002/gcc.20805
Published online 13 July 2010 inWiley Online Library (wileyonlinelibrary.com).
VVC 2010 Wiley-Liss, Inc.

The widespread use of modern imaging techni-
ques has led to an increased detection of inciden-
tal kidney tumors, leading to the difficult
decision on when and to what extent to intervene
surgically. Most suspicious solid renal masses are
managed surgically with radical nephrectomy
(Herr, 2008), but patients with benign lesions
could be spared a total nephrectomy if the diag-
nosis was safely established before the treatment
was decided (Wunderlich et al., 2005). To avoid
unnecessary nephrectomy, image-guided percuta-
neous renal tumor biopsy can be used, but a de-
finitive diagnosis is of course even more difficult
in such min samples than in nephrectomy speci-
mens (Wunderlich et al., 2005; Lebret et al.,
2007; Volpe et al., 2007). The possibility to asso-
ciate a genetic analysis in a biopsy sample is
likely to improve the evaluation of renal tumors
and to contribute to better informed therapeutic
decisions. In this study, we evaluated the possi-
bility to perform comparative genomic hybridiza-
tion (CGH) analysis on ex vivo fine needle
aspiration (FNA) biopsies of renal tumors, as well
as the contribution of the genomic copy number
changes thus detected for the differential diagno-
sis of renal cell tumors.
MATERIALS AND METHODS
Patients and Sample Selection
Seventy-five patients consecutively diagnosed
with renal tumors and subjected to radical
nephrectomy at the Portuguese Oncology Insti-
tute—Porto were selected for this study after
informed consent. For each patient, one ex vivo
fine-needle aspiration biopsy (obtained through
four to six passes of a 23-gauge needle attached
to a 10-mL syringe) and one tumor tissue frag-
ment (approximately with 1 cm3) were collected
by a pathologist and fresh-frozen and stored at
�80�C until further analysis, representing a total
of 150 samples. The remaining tissue was forma-
lin-fixed and paraffin-embedded for routine histo-
pathological evaluation. Histopathologic and
CGH findings were only compared at the end of
the study.
Comparative Genomic Hybridization
CGH analysis followed the procedure of Kallio-
niemi et al. (1994), with modifications previously
described (Ribeiro et al., 2006). Scoring was per-
formed using a customized standard reference
interval that was automatically scaled onto each
sample (Kirchhoff et al., 1998). Aberrations were
scored whenever the case profile and the standard
reference profile at 99% did not overlap. For the
scoring of amplifications, the threshold of 1.5 was
chosen. Description of copy number changes
followed the guidelines suggested by the Interna-
tional System for Human Cytogenetic Nomencla-
ture (ISCN, 2005).
Genetic Classification of Renal Cell Tumors
A genetic classification system adapted from
Receveur et al. (2005) was followed in this study.
Briefly, the pattern of copy number alterations at
chromosomes 3p, 7, and 17 was first assessed.
Tumors with 3p deletions were classified as clear
cell RCC. Cases with whole chromosome gains of
7 and 17 would be classified as papillary renal
cell tumors, whereas the diagnosis of papillary
RCC required gains of at least three of chromo-
somes 3, 7, 12, 16, 17, or 20. Two whole-chromo-
some losses without other numerical or structural
alterations or at least three losses involving chro-
mosomes 1, 2, 6, 10, 13, 17, 21, or X were indica-
tive of chromophobe RCC. Oncocytomas were
diagnosed when loss of 1p and/or 14q or gain of
11q were observed. Tumors presenting copy
number patterns not covered by this hierarchical
classification remained unclassified from the
genetic point of view.
Hierarchical Clustering
The genetic similarity between tumor samples
was further evaluated by unsupervised hierarchi-
cal clustering of CGH data using the clustering
software J-Express Pro v2.5 (Molmine, Bergen,
Norway). Unsupervised hierarchical clustering of
genomic imbalances was performed with average
linkage (cluster method) and Pearson correlation
(distance metric). The resulting dendogram
groups the tumor samples according to the degree
of genetic similarity.
Fluorescence In Situ Hybridization
Whenever the CGH findings were atypical for
a given histological diagnosis (patients 140, 157,
180, and 181), as well as in the two unclassifiable
RCC (patients 139 and 149), FISH analyses were
subsequently performed to assess 3p deletions
below the resolution level of chromosome CGH,
as well as to look for translocations involving the
TFE3/TFEB genes (Teixeira, 2006). Patients 139
and 149 (unclassifiable tumors with separate areas
936 VIEIRA ET AL.
Genes, Chromosomes & Cancer DOI 10.1002/gcc

of clear cell morphology and of papillary growth)
were also screened for copy number aberrations of
chromosomes 3, 7, 16, and 17 and for copy number
aberrations of chromosome 18, respectively. Com-
mercially available probes were used to target
FHIT (3p14) (ZytoVision, Germany), CBFB(16q22), the centromeres of chromosomes 3, 17, 18
(Abbott Laboratories), and 7 (Kreatech Diagnos-
tics, Amsterdam, The Netherlands). Bacterial
artificial chromosome (BAC) clones targeting
VHL (3p25, RP11-402P11), TFE3 (Xp11, CTD-
3009K20, and CTD-2311N12), ASPL (17q25,
RP11-51H16, and RP11-634L10), were selected
using the UCSC Human Genome Browser and
obtained from the BACPAC Resources Center.
TFEB (6p21) translocation was assessed by dual-
color FISH using BAC clones RP11-533O20 and
RP11-328M4, as previously described (Davis
et al., 2003). BAC DNA was extracted using the
Plasmid DNA Purification Kit (MACHEREY-
NAGEL GmbH KG, Duren, Germany) and
amplified using the GenomiPhi V2 DNA amplifi-
cation kit (WGA kit, GE, Healthcare, UK) accord-
ing to the manufacturer’s instructions. After a 5-
min pretreatment at 90�C, BAC DNA was labeled
with SpectrumGreen or SpectrumRed (Abbott
Laboratories, IL) conjugated nucleotides in nick
translation reactions using the same protocol as
described for CGH (Ribeiro et al., 2006). About
700 ng of each labeled BAC probe was then mixed
with 30 lg unlabeled Cot-1 DNA (Life Technolo-
gies, Rockville, MD), ethanol precipitated, dried,
and dissolved in hybridization buffer (Abbott Lab-
oratories). Adequate mapping and probe specific-
ity of all BAC clones was confirmed by
hybridization onto normal human metaphases.
Paraffin-embedded renal tumor samples were ana-
lyzed as previously described (Ribeiro et al.,
2007).
VHL Point or Exonic Mutations and Methylation
Point mutations were screened in the entire
coding regions of VHL by sequencing and multi-
plex ligation-dependent probe amplification
(MLPA; MRC-Holland, Amsterdam) was used to
detect large exonic VHL rearrangements (includ-
ing deletions not detectable by CGH, FISH, or
sequencing). Mutation screening and MLPA anal-
yses of the VHL gene were performed in the
same cases analyzed by FISH, with the exception
of patient 139 due to lack of DNA. VHL methyla-
tion analysis was performed by Methylation-spe-
cific MLPA, according to the SALSA MS-MLPA
ME002A1 Tumor suppressor-2 Kit (MRC-Hol-
land) instructions. VHL methylation was per-
formed in the same cases analyzed by FISH,
with the exception of patient 139 due to lack of
DNA. We interpreted ratios as absence of hyper-
methylation (0.00–0.25), mild hypermethylation
(0.25–0.50), moderate hypermethylation (0.50–
0.75), and extensive hypermethylation (>0.75),
(Jeuken et al., 2007).
RESULTS
Genetic Diagnosis by Comparative
Genomic Hybridization
CGH analysis was possible in 62 (82.7%) ex
vivo FNA biopsies and in 72 (96%) tumor tissue
fragments of the 75 patients (detailed findings are
provided in Table 1). The pattern of genetic
alterations in FNA biopsies allowed the differen-
tial diagnosis in 42 out of 62 (67.7%) kidney
tumors, representing 42 of 56 (75%) renal cell
tumors (Fig. 1). Of the 20 (32.3%) biopsies
unclassified from the genetic point of view, six
turned out not to be renal cell tumors.
Comparison of Genetic and Histological
Classifications
The genetic diagnosis on FNA biopsies was
histologically confirmed on the nephrectomy
specimen in 40 out of the 42 cases (95.2%).
Regarding the two tumors with discrepant find-
ings, Case 136 was genetically classified as chro-
mophobe instead of clear cell RCC because it
presented numerical losses of chromosomes 6, 13,
and 17 and no 3p deletion, whereas Case 162 was
genetically classified as oncocytoma instead of
chromophobe RCC due to the presence of 1p de-
letion and 11q gain and not multiple numerical
chromosome losses. Histological reevaluation of
these two samples in the presence of the CGH
findings was then performed. Case 136 was ini-
tially classified as clear cell RCC owing to the
negativity of Hale’s colloidal iron stain. However,
a more detailed observation revealed the pres-
ence of perinuclear halos, which were consistent
with the diagnosis of chromophobe RCC (Fig.
2A). Concerning Case 162, the original diagnosis
was based on the focal positivity to Hale’s colloi-
dal iron stain and the presence of perinuclear
halos. Upon reevaluation, the case was reclassi-
fied as oncocytoma instead of eosinophylic variant
of chromophobe RCC (Fig. 2B). Considering only
the cases in which CGH analysis of the FNA
GENETIC DIAGNOSIS OF KIDNEY TUMORS 937
Genes, Chromosomes & Cancer DOI 10.1002/gcc
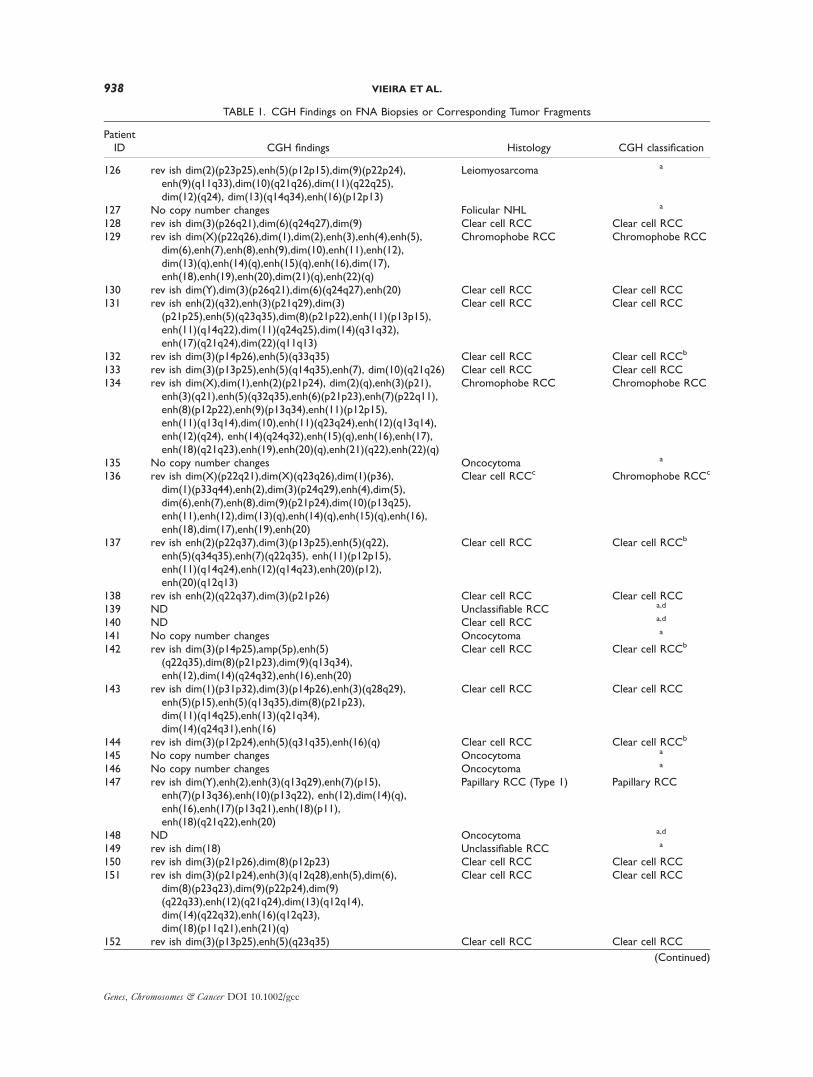
TABLE 1. CGH Findings on FNA Biopsies or Corresponding Tumor Fragments
PatientID CGH findings Histology CGH classification
126 rev ish dim(2)(p23p25),enh(5)(p12p15),dim(9)(p22p24),enh(9)(q11q33),dim(10)(q21q26),dim(11)(q22q25),dim(12)(q24), dim(13)(q14q34),enh(16)(p12p13)
Leiomyosarcoma a
127 No copy number changes Folicular NHL a
128 rev ish dim(3)(p26q21),dim(6)(q24q27),dim(9) Clear cell RCC Clear cell RCC129 rev ish dim(X)(p22q26),dim(1),dim(2),enh(3),enh(4),enh(5),
dim(6),enh(7),enh(8),enh(9),dim(10),enh(11),enh(12),dim(13)(q),enh(14)(q),enh(15)(q),enh(16),dim(17),enh(18),enh(19),enh(20),dim(21)(q),enh(22)(q)
Chromophobe RCC Chromophobe RCC
130 rev ish dim(Y),dim(3)(p26q21),dim(6)(q24q27),enh(20) Clear cell RCC Clear cell RCC131 rev ish enh(2)(q32),enh(3)(p21q29),dim(3)
(p21p25),enh(5)(q23q35),dim(8)(p21p22),enh(11)(p13p15),enh(11)(q14q22),dim(11)(q24q25),dim(14)(q31q32),enh(17)(q21q24),dim(22)(q11q13)
Clear cell RCC Clear cell RCC
132 rev ish dim(3)(p14p26),enh(5)(q33q35) Clear cell RCC Clear cell RCCb
133 rev ish dim(3)(p13p25),enh(5)(q14q35),enh(7), dim(10)(q21q26) Clear cell RCC Clear cell RCC134 rev ish dim(X),dim(1),enh(2)(p21p24), dim(2)(q),enh(3)(p21),
enh(3)(q21),enh(5)(q32q35),enh(6)(p21p23),enh(7)(p22q11),enh(8)(p12p22),enh(9)(p13q34),enh(11)(p12p15),enh(11)(q13q14),dim(10),enh(11)(q23q24),enh(12)(q13q14),enh(12)(q24), enh(14)(q24q32),enh(15)(q),enh(16),enh(17),enh(18)(q21q23),enh(19),enh(20)(q),enh(21)(q22),enh(22)(q)
Chromophobe RCC Chromophobe RCC
135 No copy number changes Oncocytoma a
136 rev ish dim(X)(p22q21),dim(X)(q23q26),dim(1)(p36),dim(1)(p33q44),enh(2),dim(3)(p24q29),enh(4),dim(5),dim(6),enh(7),enh(8),dim(9)(p21p24),dim(10)(p13q25),enh(11),enh(12),dim(13)(q),enh(14)(q),enh(15)(q),enh(16),enh(18),dim(17),enh(19),enh(20)
Clear cell RCCc Chromophobe RCCc
137 rev ish enh(2)(p22q37),dim(3)(p13p25),enh(5)(q22),enh(5)(q34q35),enh(7)(q22q35), enh(11)(p12p15),enh(11)(q14q24),enh(12)(q14q23),enh(20)(p12),enh(20)(q12q13)
Clear cell RCC Clear cell RCCb
138 rev ish enh(2)(q22q37),dim(3)(p21p26) Clear cell RCC Clear cell RCC139 ND Unclassifiable RCC a,d
140 ND Clear cell RCC a,d
141 No copy number changes Oncocytoma a
142 rev ish dim(3)(p14p25),amp(5p),enh(5)(q22q35),dim(8)(p21p23),dim(9)(q13q34),enh(12),dim(14)(q24q32),enh(16),enh(20)
Clear cell RCC Clear cell RCCb
143 rev ish dim(1)(p31p32),dim(3)(p14p26),enh(3)(q28q29),enh(5)(p15),enh(5)(q13q35),dim(8)(p21p23),dim(11)(q14q25),enh(13)(q21q34),dim(14)(q24q31),enh(16)
Clear cell RCC Clear cell RCC
144 rev ish dim(3)(p12p24),enh(5)(q31q35),enh(16)(q) Clear cell RCC Clear cell RCCb
145 No copy number changes Oncocytoma a
146 No copy number changes Oncocytoma a
147 rev ish dim(Y),enh(2),enh(3)(q13q29),enh(7)(p15),enh(7)(p13q36),enh(10)(p13q22), enh(12),dim(14)(q),enh(16),enh(17)(p13q21),enh(18)(p11),enh(18)(q21q22),enh(20)
Papillary RCC (Type 1) Papillary RCC
148 ND Oncocytoma a,d
149 rev ish dim(18) Unclassifiable RCC a
150 rev ish dim(3)(p21p26),dim(8)(p12p23) Clear cell RCC Clear cell RCC151 rev ish dim(3)(p21p24),enh(3)(q12q28),enh(5),dim(6),
dim(8)(p23q23),dim(9)(p22p24),dim(9)(q22q33),enh(12)(q21q24),dim(13)(q12q14),dim(14)(q22q32),enh(16)(q12q23),dim(18)(p11q21),enh(21)(q)
Clear cell RCC Clear cell RCC
152 rev ish dim(3)(p13p25),enh(5)(q23q35) Clear cell RCC Clear cell RCC
(Continued)
938 VIEIRA ET AL.
Genes, Chromosomes & Cancer DOI 10.1002/gcc

TABLE 1. CGH Findings on FNA Biopsies or Corresponding Tumor Fragments (Continued)
PatientID CGH findings Histology CGH classification
153 rev ish dim(X),dim(1),enh(2),enh(3),enh(4),enh(5),dim(6),enh(7)(p15),enh(7)(q31q32), enh(8),enh(9)(p21p24),enh(9)(q13q33),enh(10)(p13),enh(10)(q21q26),enh(11)(p12p15),enh(11)(q13q24),enh(12)(q14q23),enh(13)(q14q34),dim(14),enh(15)(q21q26),enh(18)(q12q23),enh(20)(p12p13),enh(21)(q21q22)
Chromophobe RCC Chromophobe RCC
154 rev ish dim(3)(p21p26),enh(5)(q33q35),enh(18) Clear cell RCC Clear cell RCC155 rev ish dim(Y),dim(3)(p21p25),enh(7)(p14p21),
enh(7)(q22q36),dim(8)(p12p23)Clear cell RCC Clear cell RCC
156 rev ish dim(1)(p36),dim(11)(p15) Chromophobe RCC a
157 rev ish enh(5)(p15),enh(5)(q14q23) Cystic multilocular RCCe a,b
158 rev ish dim(Y),enh(2)(q22q37),dim(3)(p),enh(5),enh(22)(q12q13)
Clear cell RCC Clear cell RCC
159 rev ish dim(3)(p13p26),dim(14)(q) Clear cell RCC Clear cell RCC160 rev ish enh(2)(q21q37),amp(2)(q22q32),
dim(3)(p13p25),enh(22)(q11q13)Clear cell RCC Clear cell RCC
161 rev ish dim(1)(q41q44),dim(3)(p25q21) Clear cell RCC Clear cell RCCb
162 rev ish dim(1)(p),enh(11)(q),amp(11)(q22q23) Chromophobe RCCc Oncocytomac
163 rev ish enh(2)(q31q33),dim(3)(p21p25),enh(5)(q22q35),dim(14)(q22q32)
Clear cell RCC Clear cell RCCb
164 rev ish dim(Y),enh(2)(p23q33),dim(2)(q37), dim(3)(p25q21),enh(3)(q21q29),enh(7)(p15p21),enh(7)(p13),enh(7)(q21q36),dim(8)(p12p21),enh(8)(q21q23),dim(10),enh(11) (p12p15),enh(11)(q13q23),dim(13)(q31q34),dim(15)(q21q22),enh(16)(q13q24),dim(18)(p11q22),enh(20)(p12p13),enh(20)(q),enh(21)(q21q22)
Clear cell RCC Clear cell RCC
165 rev ish dim(3)(p21p25),enh(5)(q22q35) Clear cell RCC Clear cell RCC166 rev ish dim(Y),dim(1)(p36),dim(3)(p12p25),enh(5),
amp(5)(q14q31),enh(7),enh(11)(p12p15),dim(14)(q)Clear cell RCC Clear cell RCC
167 rev ish dim(Y),enh(3)(q21q29),dim(4),enh(5)(p),dim(5)(q13q35),dim(8)(p21p22),dim(9)(p21p23),dim(10)(q23q24),dim(11)(q23q25),enh(16)(q),dim(17)(q11q21),enh(20)
Urothelial carcinoma a
168 rev ish enh(7)(p14p21),enh(7)(q31q35) Clear cell RCC a
169 rev ish enh(8)(q22q23) Chromophobe RCC a
170 rev ish enh(1)(q25q42),enh(2),dim(3)(p21p25),enh(5)(q31q35),dim(14)(q)
Clear cell RCC Clear cell RCC
171 No copy number changes Oncocytoma a
172 rev ish dim(3)(p),enh(5),dim(11)(q21q25),enh(12),dim(14)(q),enh(21)(q22)
Clear cell RCC Clear cell RCC
173 rev ish dim(Y),dim(3)(p25q21),enh(6)(p21),dim(6)(q14q27),dim(9)(p13p24)
Clear cell RCC Clear cell RCC
174 rev ish dim(Y),dim(3),enh(5) Clear cell RCC Clear cell RCCb
175 No copy number changes Chromophobe RCC a
177 rev ish dim(Y),enh(1)(q21q42),dim(3)(p22p24),dim(3)(p12p14),enh(5)(q31q35),dim(6),enh(7)(q31q36),enh(8)(p21),enh(8)(q22),dim(9)(p),enh(11)(q13q14),enh(12)(q13q24),dim(13)(q),dim(14)(q),dim(15)(q11q22),enh(16)(q),dim(18)(p11q12),enh(20)
Clear cell RCC Clear cell RCC
178 rev ish dim(Y),dim(1),enh(11)(q13q14),enh(13)(q),dim(21)(q) Oncocytoma a
179 rev ish dim(Y),enh(3),enh(12),enh(16),enh(17) Papillary RCC (Type 2) Papillary RCC180 No copy number changes Clear cell RCC a,b
181 rev ish dim(8) Clear cell RCC a,b
182 rev ish enh(3),enh(7),enh(16) Papillary RCC (Type 2) Papillary RCC183 rev ish dim(1)(p34p36),enh(1)(p31),dim(1)(p13p22),
enh(1)(q21q43),dim(2),enh(3)(p13p26),dim(3)(q11q21),enh(3)(q22q29),enh(4),enh(5),dim(6),enh(7),enh(8),enh(9),enh(10)(p11p13),dim(10)(q21q26),enh(11),enh(12),dim(13)(q),enh(14)(q),enh(15)(q),enh(16)(q12q24),dim(17),enh(18),enh(20),enh(21)(q),enh(22)(q12q13)
Chromophobe RCC Chromophobe RCC
(Continued)
GENETIC DIAGNOSIS OF KIDNEY TUMORS 939
Genes, Chromosomes & Cancer DOI 10.1002/gcc

TABLE 1. CGH Findings on FNA Biopsies or Corresponding Tumor Fragments (Continued)
PatientID CGH findings Histology CGH classification
184 rev ish dim(Y),enh(1)(p32p33),amp(1)(q21),enh(2)(p13p23),dim(2)(q34q37),enh(3),dim(4)(p),enh(4)(q),enh(5)(p15),dim(5)(q),enh(7)(p13p21),enh(7)(q31q35),dim(8)(p),enh(8)(q),dim(9)(p),enh(10)(p),dim(10)(q21q26),dim(11)(q23q24),enh(12)(q15q23),enh(13)(q12q21),dim(14)(q),enh(16)(q23q24),dim(17)(p),enh(17)(q),dim(18),enh(19)(q13),dim(20)(p),enh(20)(q),amp(20)(q11q12),enh(21)(q21q22)
Papillary urothelial carcinoma a
185 No copy number changes Angiomyolipoma a
186 rev ish dim(3)(p21p26),enh(4)(q26q28),enh(5)(q14q35),enh(7),enh(12),enh(17)(q21q25), amp(17)(q25),dim(22)(q)
Clear cell RCC Clear cell RCC
187 rev ish dim(1)(p35p36),dim(1)(q32),dim(1)(q42),enh(2),enh(3)(p13p24),enh(3)(q21q26),dim(5)(q33q35),enh(7),enh(8),dim(10)(p12p13),enh(12)(p12p13),enh(12)(q14q24),enh(13)(q13q34),dim(15)(q21q22),enh(16) (q12q23),enh(18)(p11q22)
Papillary RCC (Type 2) Papillary RCC
188 rev ish dim(Y),dim(3)(p26q21),enh(5),dim(6)(p21p25),enh(7),dim(9),enh(10)(p13q21),dim(11)(q22q25),enh(12),dim(13)(q12q21),dim(14)(q21q32),enh(20)(q)
Clear cell RCC Clear cell RCC
189 rev ish dim(2),enh(3)(q),amp(5)(p),dim(5)(q13 q35),enh(7)(p15),enh(7)(q21q36),dim(8)(p23q23),dim(9)(p13p24),dim(9)(q21q34),dim(11)(p),enh(11)(q),amp(11)(q14q23),enh(12),enh(13)(q),enh(14)(q),dim(15)(q), dim(17)(p12p13),enh(17)(q21q25),enh(20)
Papillary urothelial carcinoma a
190 rev ish dim(3)(p13p26),enh(5),dim(9),enh(12),dim(14)(q),enh(20)(p12q13)
Clear cell RCC Clear cell RCC
191 rev ish dim(Y),dim(2)(q37),dim(3)(p26q21),enh(5) Clear cell RCC Clear cell RCC192 No copy number changes Chromophobe RCC a
193 rev ish dim(2),dim(17) Chromophobe RCC Chromophobe RCC194 rev ish enh(Y),dim(1),dim(2),enh(3),enh(4),enh(5),
dim(6),enh(7),enh(8),enh(9),dim(10),enh(11),enh(12),enh(13)(q21),enh(14)(q24q32),enh(15)(q),enh(16),dim(17),enh(18)(q12q23),enh(19),enh(20),enh(21)(q),enh(22)(q)
Chromophobe RCC Chromophobe RCC
195 rev ish dim(X),dim(1),dim(2),enh(3),enh(4),dim(5),dim(6),enh(7),enh(8),enh(9),dim(10),enh(11),enh(12),enh(13)(q),enh(14)(q),enh(15)(q),enh(16),dim(17),enh(18),enh(19),enh(20),enh(21)(q),enh(22)(q)
Chromophobe RCC Chromophobe RCC
196 No copy number changes Chromophobe RCC a
197 rev ish dim(3)(p21p25),enh(5)(q33q35) Cystic multilocular RCCe Clear cell RCC198 rev ish enh(7)(p13p21),enh(7)(q21q36),enh(16),enh(20) Papillary RCC (Type 1) Papillary RCCb
199 rev ish dim(Y),dim(1)(p13p36),enh(1)(q22q24),enh(1)(q31),enh(1)(q41),enh(2)(q21q32),dim(3)(p21p26),enh(3)(q21),dim(4),enh(5)(q14q35),dim(6)(q14q16),enh(7),enh(9)(p22q34),enh(11)(p12p15),enh(11)(q23),enh(12)(q13q24),dim(14)(q22q32),enh(16),enh(21)(q22)
Clear cell RCC Clear cell RCC
200 rev ish dim(3)(p13p26),enh(5),dim(8)(p23q13) Clear cell RCC Clear cell RCC201 rev ish dim(Y),dim(3)(p),enh(5),dim(6)(q25q27),dim(14)(q) Clear cell RCC Clear cell RCC
Abbreviations: ND, not determined; rev ish, reverse in situ hybridization; enh, enhanced; dim, diminished; amp, amplified; descriptions follow the
ISCN (2005) guidelines. NHL, Non-Hodgkin lymphoma; RCC, renal cell carcinoma. When FNA was insufficient for analysis, the genetic finding
from the correspondent tumor tissue fragment is presented.aNot possible to establish a genetic diagnosis based on CGH findings.bGenetic analysis possible in resected tumor only, due to FNA biopsy DNA insufficiency.cDivergent histologic and genetic classification. Diagnosis after reevaluation by the pathologist was as suggested by the genetic data.dBoth FNA biopsy and resected tumor were not analyzable by CGH.eLow-grade variant of ccRCC.
940 VIEIRA ET AL.
Genes, Chromosomes & Cancer DOI 10.1002/gcc

Figure 1. Examples of genetic diagnosis of renal cell tumors basedon the typical patterns of genomic copy number changes (metaphasespread to the left and copy number profile to the right). A: Clear cellrenal cell carcinoma (RCC; Case no. 199) with deletion of 3p, amongother copy number changes. B: Chromophobe RCC (Case no. 153)with losses of chromosomes 1, 6, 14, and X, among other copy number
changes. C: Papillary RCC (Case no. 179) with gains of chromosomes3, 12, 16, and 17. D: Oncocytoma (Case no. 162) with 1p loss and 11qgain. Red bars to the left represent copy number losses, whereas greenbars to the right represent regions of copy number gains. [Color figurecan be viewed in the online issue, which is available atwileyonlinelibrary.com.]
GENETIC DIAGNOSIS OF KIDNEY TUMORS 941
Genes, Chromosomes & Cancer DOI 10.1002/gcc

biopsy was possible, a correct genetic diagnosis
was achieved in 29 out of 31 (93.5%) clear cell
RCC, 8 out of 13 (61.5%) chromophobe RCC, 4
out of 4 (100%) papillary RCC, and 1 out of 7
(14.3%) oncocytomas, representing 41 out of 49
(83.7%) of RCC (one of them an unclassified
RCC). The positive predictive value (PPV) and
specificity of copy number profiles was 100%.
The negative predictive value (NPV) was 93.9,
90.7, 100, and 90.2% for clear cell RCC, chromo-
phobe RCC, papillary RCC, and oncocytomas,
respectively. CGH analysis of the tumor tissue
fragments was able to correctly classify eight
additional cases. The combined genetic analysis
of both FNA biopsy and tumor tissue fragment
samples thus allowed a correct genetic subclassifi-
cation on 36 out of 41 (87.8%) clear cell RCC, 8
out of 13 (61.5%) chromophobe RCC, 5 out of 5
(100%) papillary RCC, and 1 out of 8 (12.5%)
oncocytomas, representing 69.4% of all kidney
tumors, 75.8% of all renal cell tumors, and 83.0%
of all RCC. Six tumors indistinguishable by the
genetic pattern were not of renal cell origin, rep-
resenting one angiomyolipoma, one follicular
lymphoma, one leiomyosarcoma, and three uro-
thelial carcinomas.
Hierarchical Clustering
Unsupervised hierarchical clustering of CGH
copy number changes revealed three main groups
of renal tumor samples. Group I included papil-
lary RCC and urothelial carcinomas, Group II
was comprised of only clear cell RCC, and Group
III included chromophobe RCC and oncocytoma
cases. Two renal cell tumors clustered separately
of their respective group.
Overall Pattern of Copy Number Changes
Tumor copy number profiles were produced
based mostly on the FNA biopsy findings, with
the tumor fragment results being used only when
the respective FNA analysis was unsuccessful. All
but one clear cell RCC showed genomic copy
number changes, with the chromosomal arms
most often lost including 3p (92%), 14q (36%), 8p
(23%), and Y (21%) and recurrent gains occurring
in 5q (69%), 5p (33%), 7q (26%), 2q and 12q
(23% each), and 7p (21%). Three chromophobe
RCC had no numerical changes, whereas the
remaining displayed losses at 1p (80%), 1q, 2q, 6,
10q, and 17 (60% each), 2p and 10p (50% each),
X (40%) and 13q (23%), and gains of 7, 8, 11,
12q, 15q, and 18q (70% each), and 3p, 4, 9, 14q,
16q, 18p, and 20 (60% each). All papillary RCC
showed copy number gains at different chromo-
somes, most often at 16q (100%), 3q, 7, and 16p
(80% each), 3p and 12 (60% each), and 2, 17, 18,
and 20 (40% each) whereas chromosome Y was
most commonly lost. Only two out of eight onco-
cytomas showed detectable copy number
changes, namely losses at 1p (in both cases), 1q,
21q, and Y (in one case each) and gains at 11q
(in both cases) and 13q (in one case). A small
degree of intratumor heterogeneity was detected
between FNA biopsy and tumor tissue fragments
for seven (all clear cell RCC) of the 62 cases in
which a comparison was possible (Fig. 3). No
copy number changes were detected in the angio-
myolipoma and the follicular lymphoma, whereas
Figure 2. Representative images of Cases 136 (A) and 162(B) which were reviewed following the results of CGH analysis. Case136 was genetically classified as chromophobe instead of clear cellRCC because it presented numerical losses of chromosomes 6, 13,and 17 and no 3p deletion, whereas Case 162 was genetically classi-fied as oncocytoma instead of chromophobe RCC due to the pres-ence of 1p deletion and 11q gain and not multiple numericalchromosome losses. [Color figure can be viewed in the online issue,which is available at wileyonlinelibrary.com.]
942 VIEIRA ET AL.
Genes, Chromosomes & Cancer DOI 10.1002/gcc

the three urothelial carcinomas and the leiomyo-
sarcoma were genetically very complex.
FISH Findings
None of the six tumors analyzed presented
deletion of the VHL or FHIT genes or translocations
involving the TFE3/TFEB genes. Patient 139
showed three copies of chromosomes 3, 7, 16, and
17 in both clear cell morphology and papillary
growth areas and patient 149 showed one copy of
chromosome 18 also in both morphologically dis-
tinct tumor areas (Fig. 4). In this latter case we also
performed immunohistochemical analyses for Cyto-
keratin 7 and alpha methylcyl coenzyme A race-
mase (AMACR) (Fig. 4). Whereas AMACR
expression was observed in both papillary and clear
cell components, Cytokeratin 7 expression was
mainly restricted to the papillary component of the
neoplasm.
VHL Molecular Genetic and Methylation Findings
None of the tumors analyzed presented point
mutations or exonic rearrangements of the VHLgene. One of the five renal tumors analyzed
(Case 181) presented mild hypermethylation of
the VHL gene (ratio 0.4), whereas the remaining
four showed no methylation. No deletion of the
VHL gene was detected also by MS-MLPA in
these cases.
DISCUSSION
FNA biopsy of the kidney is usually performed
to establish the diagnosis of a renal tumor that
cannot be resected due to the patient’s inability
to tolerate surgery or advanced disease at diagno-
sis, as well as to determine whether the renal
tumor is primary or metastatic in a patient with
a previously diagnosed cancer involving another
organ. This procedure can also be used to es-
tablish the definitive diagnosis before medical
treatment (Renshaw et al., 1997; Truong et al.,
1999). Volpe et al. made a literature review on
the use of percutaneous needle core biopsy and
FNA biopsy of renal tumors and concluded that
the procedure is safe and carries minimal risk of
tumor spread (Volpe et al., 2007). Although di-
agnosis of RCC can be made on FNA samples,
cytologic examination alone cannot predict the
Furhman nuclear grade nor does it allow a reli-
able subclassification into its histological sub-
types (Garcia-Solano et al., 2008; Kummerlin
et al., 2009; Masoom et al., 2009). On the other
hand, renal core biopsies can be used for histo-
pathological diagnosis, but the rate of nondiag-
nostic or inaccurately read biopsies can be high
(Dechet et al., 2003; Neuzillet et al., 2004;
Shannon et al., 2008). Overlapping morphologi-
cal characteristics can make the differential di-
agnosis difficult in some kidney tumors, even in
nephrectomy specimens in the hands of an
experienced pathologist. The eosinophilic vari-
ant of chromophobe RCC may look as an onco-
cytoma or an eosinophilic variant of clear cell
RCC, whereas the classical variant of chromo-
phobe RCC may resemble clear cell RCC (Liu
et al., 2007).
We show here that genetic analysis is a helpful
ancillary tool for kidney tumor diagnosis, as
Figure 3. Genetic heterogeneity in tumor samples from a clear cell renal cell carcinoma (Case no.186). A: CGH findings in the fine needle aspiration biopsy; B: CGH findings in the tumor fragment. Thediagnostic 3p deletion (among other changes) was detected in both samples, but the gain of 7 and lossof 22q were detected only in the fine needle aspiration biopsy. [Color figure can be viewed in the onlineissue, which is available at wileyonlinelibrary.com.]
GENETIC DIAGNOSIS OF KIDNEY TUMORS 943
Genes, Chromosomes & Cancer DOI 10.1002/gcc

exemplified by the diagnostic change that occurred
in two cases from our series after histological revi-
sion of the nephrectomy specimens in light of the
genetic information (one clear cell RCC and a chro-
mophobe RCC were reclassified as chromophobe
RCC and oncocytoma, respectively). The contribu-
tion of genetic typing for the correct diagnosis of
renal cell tumors is potentially much higher in
Figure 4. Selected H&E, immunostains, and FISH findings on renalcell carcinoma with mixed clear cell and papillary morphology. A: Caseno. 139, showing areas with clear cell (right side of the image) and pap-illary (left side of the image) growth pattern. B: Case no. 149, display-ing clear cell (right side of the image) and papillary (left side of theimage) areas. Immunostains for cytokeratin 7 (C) and AMACR (D) in
the transition areas are displayed in the middle panels for Case no.149. In the bottom panels, representative FISH images from Case no.139 show three copies of the VHL gene (in green) and of Chromosome3 centromere (in red) in both clear cell (E) and papillary (F) areas.[Color figure can be viewed in the online issue, which is available atwileyonlinelibrary.com.]
944 VIEIRA ET AL.
Genes, Chromosomes & Cancer DOI 10.1002/gcc

percutaneous FNA due to the sampling limitations
to identify cell type and growth pattern. The pat-
tern of genetic alterations in FNA biopsies alone
allowed a correct genetic diagnosis in 75% of the
renal cell tumors successfully analyzed, with a spec-
ificity and PPV of 100%, and a sensitivity of 93.5,
61.5, 100, and 14.3% and a NPV of 93.9, 90.7, 100,
and 90.2% for clear cell RCC, chromophobe RCC,
papillary RCC, and oncocytomas, respectively.
Besides distinguishing between benign and malig-
nant tumors, a precise diagnosis is relevant not
least because different carcinoma subtypes have
diverse prognosis (Amin et al., 2002; Gudbjartsson
et al., 2005; Patard et al., 2005).
Our study is the first to use CGH on FNA
biopsies for differential diagnosis of renal cell
tumors, but other investigators have used FISH
to augment the accuracy of histhopathological di-
agnosis (Barocas et al., 2007). However, the use
of FISH for genetic diagnosis has limitations,
since no information is obtained on the genome
regions not probed. Contrarily to FISH with
locus-specific probes, CGH is a genome-wide
screening methodology that allows the detection
of DNA copy number changes across all chromo-
somes in one single experiment, without need
for a priori knowledge for probe selection. CGH
has also higher success rate than chromosome
banding analysis for renal cell tumor diagnosis
because it does not require tumor cell culturing.
However, CGH does not detect balanced translo-
cations and may be sensitive to ploidy shifts,
which is probably why unsupervised hierarchical
clustering analysis is less efficient than critical
interpretation of the most relevant genetic find-
ings for genetic diagnosis of renal cell tumors.
Our combined CGH findings on FNA and tis-
sue fragment samples showed 3p deletions in
92% of the clear cell RCC, which is higher than
most previous CGH studies (61–63%) (Jiang
et al., 2000; Reutzel et al., 2001). The four
remaining clear cell RCC tumors (as well as the
two unclassifiable RCC with separate clear cell
morphology and papillary growth areas) did not
present deletion of VHL or FHIT nor TFE3/TFEB translocations by FISH. With the excep-
tion of mild VHL hypermethylation in one case,
all remaining five cases showed no evidence of
VHL molecular alterations, indicating the exis-
tence of biological entities with clear cell mor-
phology yet to be genetically defined, as
suggested also by others (Gobbo et al., 2008).
Characteristic chromosome gains were found in
the five papillary RCC analyzed, namely those of
chromosomes 7, 12, 16, 17, and 20. Gains of
Chromosome 7 and of Chromosome 17 were not
found in all papillary RCC, but multiple trisomies
are the defining feature (Henke and Erbersdo-
bler, 2002; Gunawan et al., 2003). One unclassifi-
able RCC with separate clear cell morphology
and papillary growth areas (Patient 139) showed,
by FISH, three copies of chromosomes 3, 7, 16,
and 17 and no VHL or FHIT alterations, or rear-
rangements involving the TFE3/TFEB genes. As
both clear cell and papillary areas shared the
same genetic features (multiple trisomies), this
tumor can be considered biologically as a papil-
lary RCC (Gobbo et al., 2008). On the other
hand, the second unclassifiable RCC (Patient
149) presented the same isolated genetic altera-
tion, monosomy of chromosome 18, in both clear
cell and papillary areas, suggesting that it might
belong to a distinct histopathologic and molecular
genetic entity (Gobbo et al., 2008). Our finding
of shared cytogenetic changes in the two morpho-
logically distinct tumor areas of these two unclas-
sified tumors indicates a common clonal origin
and subsequent phenotypic divergence (illus-
trated also by the diverse immunoreactivity to
Cytokeratin 7 in Case 149), as opposed to a colli-
sion of two independent neoplasms.
Eight of the 13 chromophobe RCC presented
the expected genetic pattern that included the
typical multiple monosomies, but recurrent gains
on several chromosomes were also found. The
apparent complexity of these karyotypes is par-
tially explained by the ploidy of the tumor, as rel-
ative gains may result from the presence of two
copies of some chromosomes in a hyper-haploid
tumor or from four copies of those same chromo-
somes after polyploidization (hyper-triploidy)
(Gerharz et al., 1995; Bugert et al., 1997). Two
cases displayed small and atypical alterations and
the remaining three showed no copy number
changes, as has been reported in a minority of
the cases in the literature (Speicher et al., 1994;
Iqbal et al., 1996; Brunelli et al., 2005). Finally,
only two out of eight oncocytomas were geneti-
cally abnormal by CGH, showing the typical 1p
loss and 11q gain. Tumors without demonstrable
copy number changes by CGH may indicate the
presence of contaminating normal cells, the exis-
tence of genetic alterations below the resolution
of chromosomal CGH, or the presence of bal-
anced translocations, as has been shown to occur
in oncocytomas (Fuzesi et al., 2005).
Genetic analyses of neoplasms are usually per-
formed in a single sample and therefore
GENETIC DIAGNOSIS OF KIDNEY TUMORS 945
Genes, Chromosomes & Cancer DOI 10.1002/gcc

intratumor genetic heterogeneity may go unno-
ticed. Such intratumor genetic heterogeneity
could theoretically affect the accuracy of the
genetic tumor classification. We found intratumor
heterogeneity in seven of the 62 cases in which a
comparison was possible (all clear cell RCC), with
evidence of focal progression and clonal diver-
gence. However, the genetic diagnosis was not
affected in any of the seven clear cell RCC, since
the defining 3p deletion was always detected in
both samples. Since primary genetic events occur
early and are unlikely to be lost during carcinogen-
esis, it is conceivable that intratumor genetic het-
erogeneity occurs only with secondary
chromosomal changes, which are less relevant than
primary events for genetic classification in general
and in renal cell tumors in particular.
To the best of our knowledge, this is the first
study to evaluate CGH as an ancillary method to
diagnose renal cell tumors on FNA biopsies. We
demonstrate that genetic diagnosis by CGH on
FNA biopsies is feasible in patients with kidney
tumors and that it is a useful ancillary methodology
to improve the differential diagnosis of renal cell
tumors.
REFERENCES
Amin MB, Tamboli P, Javidan J, Stricker H, de-Peralta VenturinaM, Deshpande A, Menon M. 2002. Prognostic impact of histo-logic subtyping of adult renal epithelial neoplasms: An experi-ence of 405 cases. Am J Surg Pathol 26:281–291.
Barocas DA, Mathew S, DelPizzo JJ, Vaughan ED, Jr, Sosa RE,Fine RG, Akhtar M, Scherr DS. 2007. Renal cell carcinomasub-typing by histopathology and fluorescence in situ hybridiza-tion on a needle-biopsy specimen. BJU Int 99:290–295.
Brunelli M, Eble JN, Zhang S, Martignoni G, Delahunt B, ChengL. 2005. Eosinophilic and classic chromophobe renal cell carci-nomas have similar frequent losses of multiple chromosomesfrom among chromosomes 1, 2, 6, 10, and 17, and this patternof genetic abnormality is not present in renal oncocytoma. ModPathol 18:161–169.
Bugert P, Gaul C, Weber K, Herbers J, Akhtar M, Ljungberg B,Kovacs G. 1997. Specific genetic changes of diagnostic impor-tance in chromophobe renal cell carcinomas. Lab Invest76:203–208.
Cheng L, Zhang S, MacLennan GT, Lopez-Beltran A, MontironiR. 2009. Molecular and cytogenetic insights into the pathogene-sis, classification, differential diagnosis, and prognosis of renalepithelial neoplasms. Hum Pathol 40:10–29.
Davis IJ, Hsi BL, Arroyo JD, Vargas SO, Yeh YA, Motyckova G,Valencia P, Perez-Atayde AR, Argani P, Ladanyi M, FletcherJA, Fisher DE. 2003. Cloning of an Alpha-TFEB fusion in re-nal tumors harboring the t(6;11)(p21;q13) chromosome translo-cation. Proc Natl Acad Sci USA 100:6051–6056.
Dechet CB, Zincke H, Sebo TJ, King BF, LeRoy AJ, FarrowGM, Blute ML. 2003. Prospective analysis of computerized to-mography and needle biopsy with permanent sectioning todetermine the nature of solid renal masses in adults. J Urol169:71–74.
Fuzesi L, Frank D, Nguyen C, Ringert RH, Bartels H, GunawanB. 2005. Losses of 1p and chromosome 14 in renal oncocyto-mas. Cancer Genet Cytogenet 160:120–125.
Garcia-Solano J, Acosta-Ortega J, Perez-Guillermo M, Benedicto-Orovitg JM, Jimenez-Penick FJ. 2008. Solid renal masses inadults: Image-guided fine-needle aspiration cytology and imag-
ing techniques—‘‘Two heads better than one?’’ Diagn Cytopa-thol 36:8–12.
Gerharz CD, Moll R, Storkel S, Ramp U, Hildebrandt B, Mols-berger G, Koldovsky P, Gabbert HE. 1995. Establishment andcharacterization of two divergent cell lines derived from ahuman chromophobe renal cell carcinoma. Am J Pathol 146:953–962.
Gobbo S, Eble JN, Grignon DJ, Martignoni G, MacLennan GT,Shah RB, Zhang S, Brunelli M, Cheng L. 2008. Clear cell pap-illary renal cell carcinoma: A distinct histopathologic and molec-ular genetic entity. Am J Surg Pathol 32:1239–1245.
Gudbjartsson T, Hardarson S, Petursdottir V, Thoroddsen A,Magnusson J, Einarsson GV. 2005. Histological subtyping andnuclear grading of renal cell carcinoma and their implicationsfor survival: A retrospective nation-wide study of 629 patients.Eur Urol 48:593–600.
Gunawan B, von Heydebreck A, Fritsch T, Huber W, RingertRH, Jakse G, Fuzesi L. 2003. Cytogenetic and morphologictyping of 58 papillary renal cell carcinomas: Evidence for acytogenetic evolution of type 2 from type 1 tumors. Cancer Res63:6200–6205.
Henke RP, Erbersdobler A. 2002. Numerical chromosomal aberra-tions in papillary renal cortical tumors: Relationship with histo-pathologic features. Virchows Arch 440:604–609.
Herr HW. 2008. Surgical management of renal tumors: A historicalperspective. Urol Clin North Am 35:543–549.
Iqbal MA, Akhtar M, Ali MA. 1996. Cytogenetic findings in renalcell carcinoma. Hum Pathol 27:949–954.
ISCN. 2005. An International System for Human Cytogenetic No-menclature. Switzerland: Karger S. Basel.
Jeuken JW, Cornelissen SJ, Vriezen M, Dekkers MM, Errami A,Sijben A, Boots-Sprenger SH, Wesseling P. 2007. MS-MLPA:An attractive alternative laboratory assay for robust, reliable,and semiquantitative detection of MGMT promoter hyper-methylation in gliomas. Lab Invest 87:1055–1065.
Jhang JS, Narayan G, Murty VV, Mansukhani MM. 2004. Renaloncocytomas with 11q13 rearrangements: Cytogenetic, molecu-lar, and immunohistochemical analysis of cyclin D1. CancerGenet Cytogenet 149:114–119.
Jiang F, Desper R, Papadimitriou CH, Schaffer AA, KallioniemiOP, Richter J, Schraml P, Sauter G, Mihatsch MJ, Moch H.2000. Construction of evolutionary tree models for renal cellcarcinoma from comparative genomic hybridization data. CancerRes 60:6503–6509.
Kallioniemi OP, Kallioniemi A, Piper J, Isola J, Waldman FM, GrayJW, Pinkel D. 1994. Optimizing comparative genomic hybridiza-tion for analysis of DNA sequence copy number changes in solidtumors. Genes Chromosomes Cancer 10:231–243.
Kirchhoff M, Gerdes T, Rose H, Maahr J, Ottesen AM, Lunds-teen C. 1998. Detection of chromosomal gains and losses incomparative genomic hybridization analysis based on standardreference intervals. Cytometry 31:163–173.
Kummerlin IP, Smedts F, Ten Kate FJ, Horn T, Algaba F, TriasI, Wijkstra H, de la Rosette JJ, Laguna MP. 2009. Cytologicalpunctures in the diagnosis of renal tumours: A study on accu-racy and reproducibility. Eur Urol 55:187–195.
Lebret T, Poulain JE, Molinie V, Herve JM, Denoux Y, Guth A,Scherrer A, Botto H. 2007. Percutaneous core biopsy for renalmasses: Indications, accuracy and results. J Urol 178:1184–1188.
Liu L, Qian J, Singh H, Meiers I, Zhou X, Bostwick DG. 2007.Immunohistochemical analysis of chromophobe renal cell carci-noma, renal oncocytoma, and clear cell carcinoma: An optimaland practical panel for differential diagnosis. Arch Pathol LabMed 131:1290–1297.
Masoom S, Venkataraman G, Jensen J, Flanigan RC, Wojcik EM.2009. Renal FNA-based typing of renal masses remains a usefuladjunctive modality: Evaluation of 31 renal masses with correla-tive histology. Cytopathology 20:50–55.
Neuzillet Y, Lechevallier E, Andre M, Daniel L, Coulange C.2004. Accuracy and clinical role of fine needle percutaneous bi-opsy with computerized tomography guidance of small (lessthan 4.0 cm) renal masses. J Urol 171:1802–1805.
Patard JJ, Leray E, Rioux-Leclercq N, Cindolo L, Ficarra V, Zis-man A, De La Taille A, Tostain J, Artibani W, Abbou CC,Lobel B, Guille F, Chopin DK, Mulders PF, Wood CG, Swan-son DA, Figlin RA, Belldegrun AS, Pantuck AJ. 2005. Prognos-tic value of histologic subtypes in renal cell carcinoma: Amulticenter experience. J Clin Oncol 23:2763–2771.
Receveur AO, Couturier J, Molinie V, Vieillefond A, Desangles F,Guillaud-Bataille M, Danglot G, Coullin P, Bernheim A. 2005.
946 VIEIRA ET AL.
Genes, Chromosomes & Cancer DOI 10.1002/gcc

Characterization of quantitative chromosomal abnormalities inrenal cell carcinomas by interphase four-color fluorescence insitu hybridization. Cancer Genet Cytogenet 158:110–118.
Renshaw AA, Lee KR, Madge R, Granter SR. 1997. Accuracy offine needle aspiration in distinguishing subtypes of renal cellcarcinoma. Acta Cytol 41:987–994.
Reutzel D, Mende M, Naumann S, Storkel S, Brenner W, ZabelB, Decker J. 2001. Genomic imbalances in 61 renal cancersfrom the proximal tubulus detected by comparative genomichybridization. Cytogenet Cell Genet 93:221–227.
Ribeiro FR, Jeronimo C, Henrique R, Fonseca D, Oliveira J,Lothe RA, Teixeira MR. 2006. 8q gain is an independentpredictor of poor survival in diagnostic needle biopsies fromprostate cancer suspects. Clin Cancer Res 12:3961–3970.
Ribeiro FR, Henrique R, Martins AT, Jeronimo C, Teixeira MR.2007. Relative copy number gain of MYC in diagnostic needlebiopsies is an independent prognostic factor for prostate cancerpatients. Eur Urol 52:116–125.
Shannon BA, Cohen RJ, de Bruto H, Davies RJ. 2008. The valueof preoperative needle core biopsy for diagnosing benignlesions among small, incidentally detected renal masses. J Urol180:1257–1261.
Speicher MR, Schoell B, du Manoir S, Schrock E, Ried T,Cremer T, Storkel S, Kovacs A, Kovacs G. 1994. Specific loss of
chromosomes 1, 2, 6, 10, 13, 17, and 21 in chromophobe renalcell carcinomas revealed by comparative genomic hybridization.Am J Pathol 145:356–364.
Teixeira MR. 2006. Recurrent fusion oncogenes in carcinomas.Crit Rev Oncog 12:257–271.
Truong LD, Todd TD, Dhurandhar B, Ramzy I. 1999. Fine-nee-dle aspiration of renal masses in adults: Analysis of results anddiagnostic problems in 108 cases. Diagn Cytopathol 20:339–349.
Volpe A, Kachura JR, Geddie WR, Evans AJ, Gharajeh A, Sara-vanan A, Jewett MA. 2007. Techniques, safety and accuracy ofsampling of renal tumors by fine needle aspiration and corebiopsy. J Urol 178:379–386.
Wunderlich H, Hindermann W, Al Mustafa AM, Reichelt O,Junker K, Schubert J. 2005. The accuracy of 250 fine needlebiopsies of renal tumors. J Urol 174:44–46.
Young AN, Dale J, Yin-Goen Q, Harris WB, Petros JA, DattaMW, Wang MD, Marshall FF, Amin MB. 2006. Current trendsin molecular classification of adult renal tumors. Urology67:873–880.
Zanssen S, Gunawan B, Fuzesi L, Warburton D, Schon EA. 2004.Renal oncocytomas with rearrangements involving 11q13 containbreakpoints near CCND1. Cancer Genet Cytogenet 149:120–124.
GENETIC DIAGNOSIS OF KIDNEY TUMORS 947
Genes, Chromosomes & Cancer DOI 10.1002/gcc





























