Embed Size (px)
Citation preview

FDATransmissible Spongiform Encephalopathies
Advisory Committee23rd Meeting 01 August 2011
Gaithersburg MD
Donor Deferral/Ineligibility for Time Spent in Saudi Arabia to Reduce Risk of vCJD Transmitted by Blood and Blood Products and by Human Cells, Tissues and
Cellular and Tissue-Based Products (HCT/Ps)
David M. Asher<[email protected]>
Laboratory of Bacterial & TSE AgentsDivision of Emerging & Transfusion-Transmitted Diseases
Office of Blood Research & ReviewCenter for Biologics Evaluation & Research
US Food & Drug Administration

2
AcknowledgementsCBER
Steven Anderson OBE Bryan Emery OM Jay Epstein OBRR Joe Giglio OBRR Melissa Greenwald OCTGT Luisa Gregori OBRR Ginette Michaud OBRR Pedro Piccardo OBRR Martin Ruta OBRR Jennifer Scharpf OBRR Alan Williams OBRR Hong Yang OBE
Judith Badoo OD Joan Blair OD Diane Maloney OD
Other FDA Sousan Altae OC OIP Layla Batarseh OC OIP Burt Pritchett CVM
TSEAC Frank Rentas DoD Mo Salmon CO State U
Other Robert Will UK CJDSU Michael Coulthart HPA Canada Lawrence Schonberger CDC David Lincoln DoD
Kingdom of Saudi Arabia Food and Drug Authority
3
Introduction
Terminology: “deferral” for blood/plasma donors = “ineligibility” for donors of HCT/Ps
Issue for TSEAC
General background on vCJD and blood safety (and HCT/P safety)
vCJD in 3 long-time residents of Saudi Arabia
Potential dietary exposure to BSE agent in Saudi Arabia
4
Introduction (2)
FDA considerations for possible additional deferrals /ineligibility of donors resident in Saudi Arabia
Potential impact of deferrals on supply of blood donors (by implication on eligible HCT/P donors)
Compare Canadian deferrals of blood donors resident in Saudi Arabia with those of FDA
Questions for TSEAC

5
FDA seeks advice from TSEAC on whether, based on three cases of vCJD in individuals likely to have been infected with the BSE agent in Saudi Arabia, to modify current vCJD-related safety recommendations deferring certain blood and plasma donors or finding certain donors of HCT/Ps ineligible to
donate for time spent in Saudi Arabia.
Issue for TSEAC
6
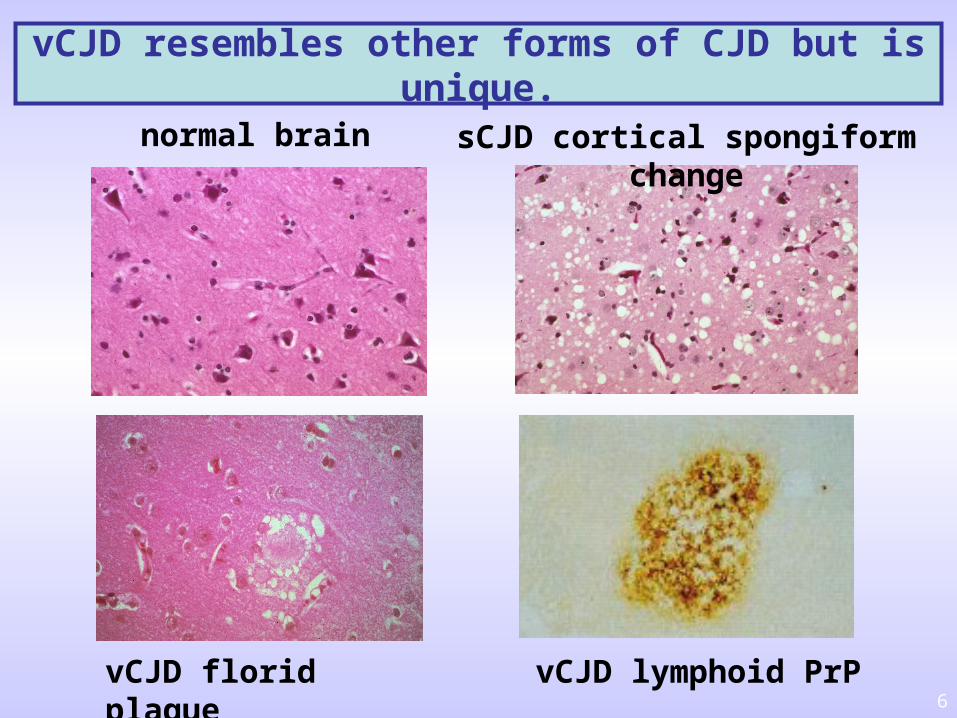
vCJD resembles other forms of CJD but is unique.
0
50
100
1stQtr
3rdQtr
East
West
North
normal brain sCJD cortical spongiform change
vCJD florid plaque
vCJD lymphoid PrP

7
vCJD and blood safety
Variant CJD: a human infection with BSE agent (= a “zoonosis”)
Most vCJD infections food-borne Five vCJD infections in UK attributed to blood
products Only one risk-reduction strategy available for blood
components and HCT/Ps: reduce number of donors exposed to BSE agent = geographic donor deferral/ineligibility
Donor testing not yet available Reliable infectivity removal techniques not yet
available (except for plasma derivatives)

8
vCJD and blood safety (2)
Geographic donor deferrals reduce risk but non-specific, inefficient
Donor deferral recommendations not fully effective, not completely consistent
When persons in new countries are recognized to pose a potential vCJD risk, FDA believes it prudent to consider modifying FDA geographic BSE-related recommendations for suitability/eligibility.

BSE and vCJD deaths in UK
9
0
5000
10000
15000
20000
25000
30000
35000
40000
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
BS
E d
eath
s
0
5
10
15
20
25
30
vCJD
dea
ths
Feedban
4 transfusion infections
pdFVIII case
12/03 7/04 2/06 1/07 2/09
BSE vCJD

Estimated incubation periods of vCJD
Food-borne vCJD• Estimated median of 12-13 yr for cases to
datein persons with PRNP 129-MM genotype (~ 40% of normal UK
population). • Predicted median ?? 32 yr in persons with genotypes MV (~ 50% UK) and VV (~ 10% UK).Small numbers of cases predicted up to ? > 40 yr
after exposureTransfusion-transmitted vCJD
1st case 6.3 yr2nd case > 5 yr (PrPTSE-pos lymphoid
tissues)
3rd case 7.8 yr4th case 8.5 yr (same donor as 3rd case)
Plasma-derivative associated case? 11 yr
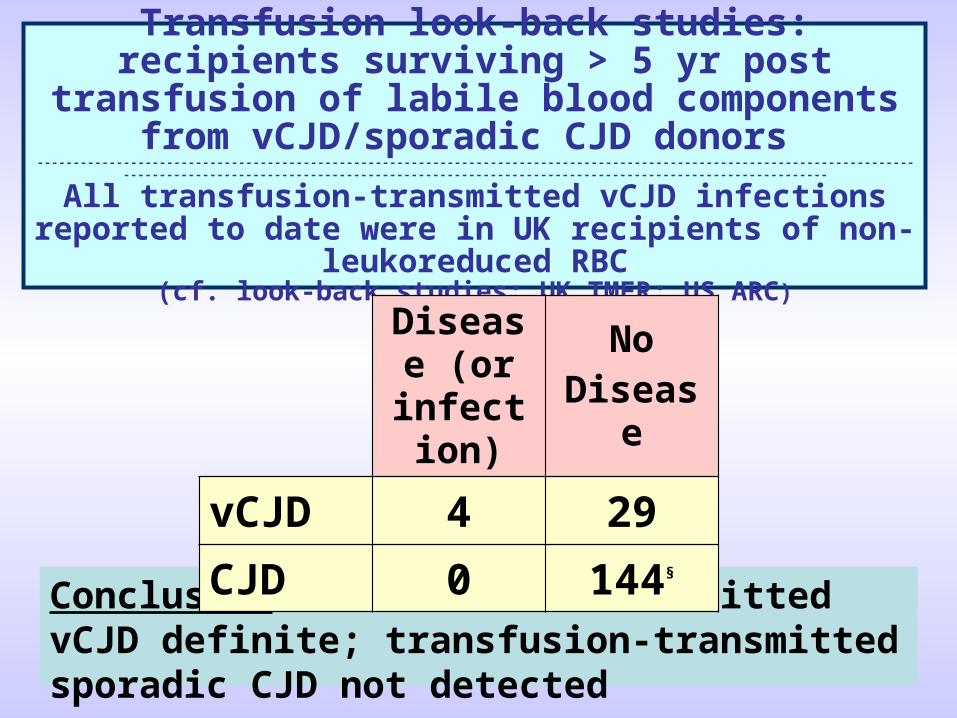
Transfusion look-back studies:recipients surviving > 5 yr post
transfusion of labile blood components from vCJD/sporadic CJD donors
----------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------
All transfusion-transmitted vCJD infections reported to date were in UK recipients of non-
leukoreduced RBC(cf. look-back studies: UK TMER; US ARC)
Conclusion: Transfusion-transmitted vCJD definite; transfusion-transmitted sporadic CJD not detected
Disease (or
infection)
NoDisease
vCJD 4 29
CJD 0 144§

12
How long before onset of clinical vCJD
is blood infectious? Intervals between blood donations and onset of vCJD
case or infection for 3 implicated UK donors
to 4 infected recipients of non-leukoreduced packed RBC:
1.4, 1.5, 1.7, 3.5 years
Conclusion:During the last 3.5 years of incubation period, blood of [some] clinically healthy PRNP-codon-129-MM donors who later developed vCJD is already infectious.

13
vCJD attributed to infection in Saudi Arabia
3 vCJD cases in long-time residents of Saudi Arabia All had common vCJD PRNP-129 genotype (MM) No history of transfusion, surgery Presumably food-borne infection Dates of residence in Saudi Arabia for all 3 cases
encompass plausible vCJD food-borne incubation periods.
Other countries less likely places where infection might have acquired, though not impossible
14
vCJD attributed to infection in Saudi Arabia (2)
No vCJD case has been convincingly attributed to residence in any other country of the region.
US (CDC) and Canadian (HPA/Health Canada ) authorities concluded that vCJD was most likely acquired in Saudi Arabia.
Before they became clinically ill, all 3 Saudi-associated vCJD cases would have been considered suitable/eligible to donate blood, plasma and HCT/Ps per current FDA recommendations.
Three UK-associated cases in Dx in N America would have been deferred/ineligible.

15
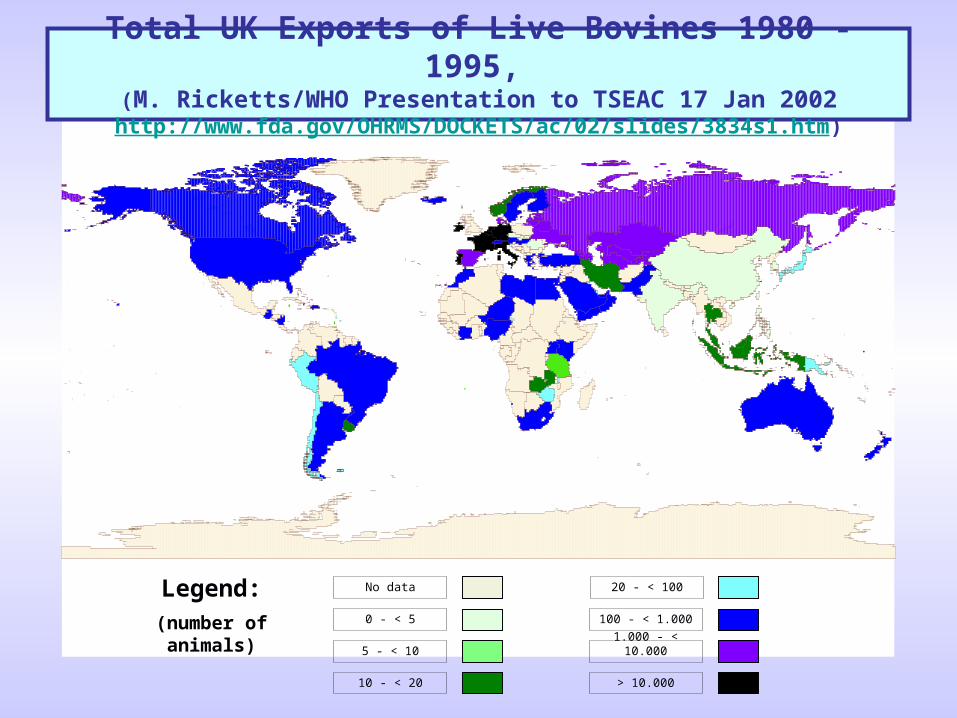
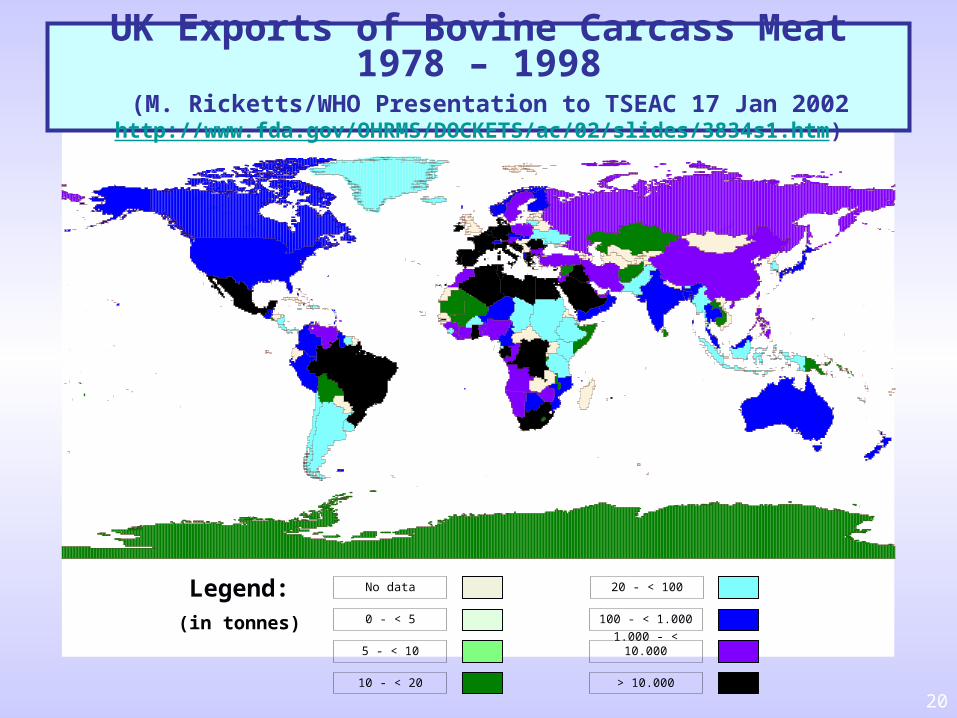
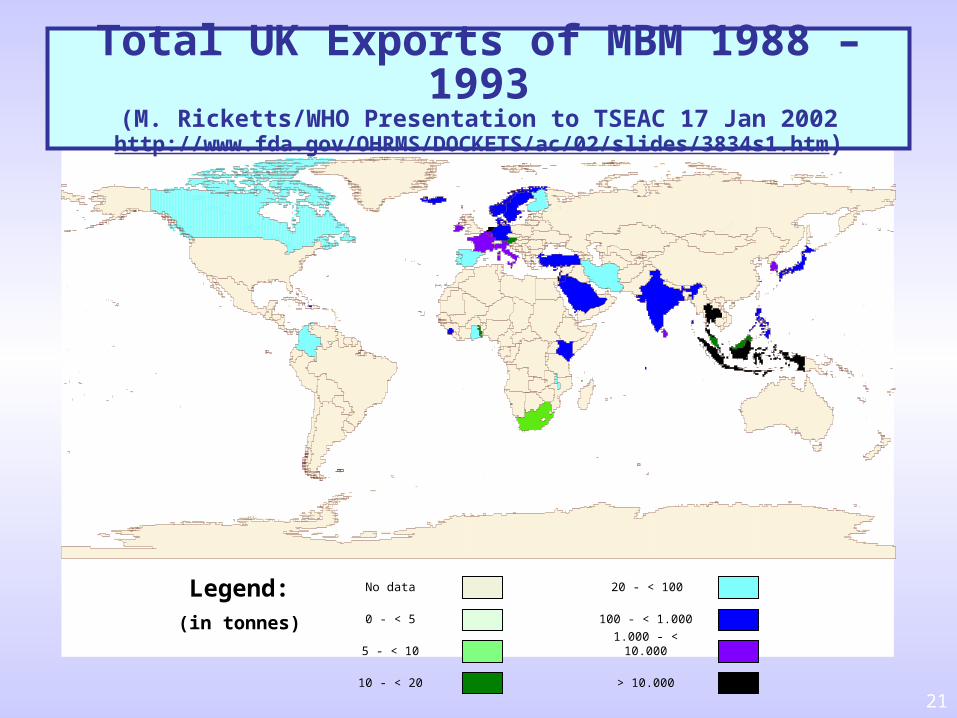
UK probably exported to Saudi Arabia products potentially contaminated with the BSE agent during the generally-accepted UK BSE-highest-risk period (1980-1996).─ Live cattle─ Beef products─Meat-and-bone meal (MBM)
Saudi Arabia has not recognized BSE in native cattle. BSE has been recognized rarely in two other
countries in the Middle East.─Oman: 2 bovines imported from UK in 1989─ Israel: 1 native bovine in 2002
Estimating possible risk of dietary exposureto BSE agent in Saudi Arabia
16
UK exports to other countries of the region 1980-1996 Exports to the region from other BSE countries Cross border trade in the region Risk that undetected indigenous BSE was established
in bovines and (theoretically) in other ruminants in Saudi Arabia from
Rendering practices and feeding of MBM to ruminants
Estimating possible risk of dietary exposureto BSE agent in Saudi Arabia (2)
_________________________________________________
Uncertain but possibly relevant BSE risks

17
Estimating possible risk of dietary exposureto BSE agent in Saudi Arabia (3)
_________________________________________________
Information FDA considered
Crude rates of recognized vCJD cases 1996-present attributed to time spent in various countries
UK bovine-related exports to Saudi Arabia Estimated fraction of UK beef in Saudi Arabia Overall beef consumption in Saudi Arabia [Anecdotal information] Caveat. Information available uncertain, mostly
unverified, and reliability of some sources not known
18
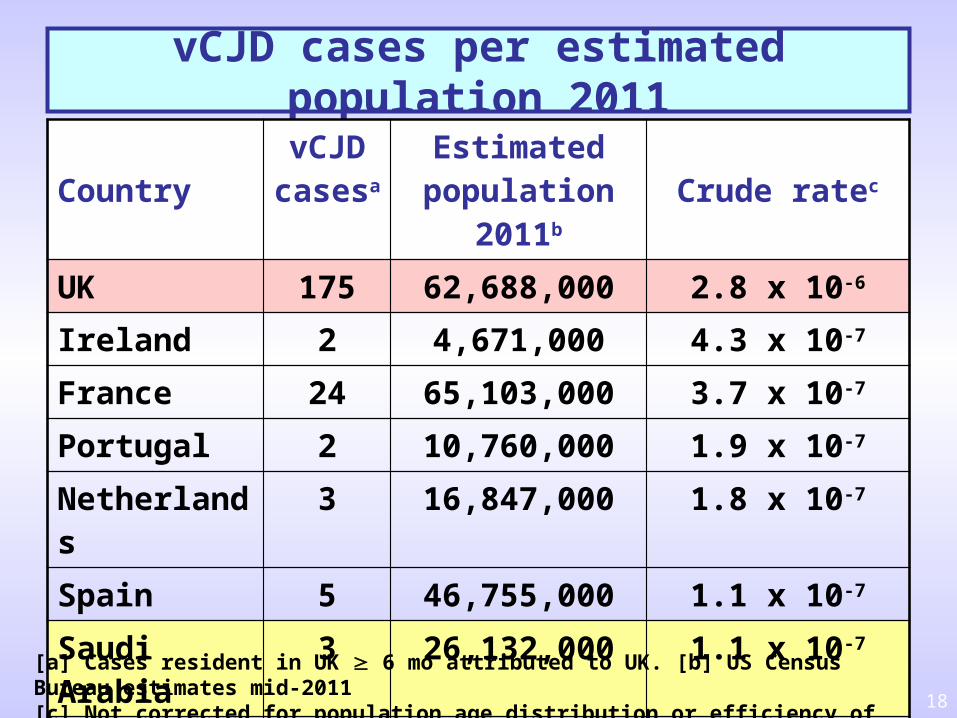
vCJD cases per estimated population 2011
CountryvCJDcasesa
Estimated population 2011b Crude ratec
UK 175 62,688,000 2.8 x 10-6
Ireland 2 4,671,000 4.3 x 10-7
France 24 65,103,000 3.7 x 10-7
Portugal 2 10,760,000 1.9 x 10-7
Netherlands 3 16,847,000 1.8 x 10-7
Spain 5 46,755,000 1.1 x 10-7
Saudi Arabia 3 26,132,000 1.1 x 10-7
Italy 2 61,017,000 3.3 x 10-8
Japan 1 126,476,000 7.9 x 10-9
[a] Cases resident in UK 6 mo attributed to UK. [b] US Census Bureau estimates mid-2011[c] Not corrected for population age distribution or efficiency of case recognition/reporting.
No data
0 - < 5
5 - < 10
10 - < 20
20 - < 100
100 - < 1.000
1.000 - < 10.000
> 10.000
Legend:(number of animals)
Total UK Exports of Live Bovines 1980 - 1995, (M. Ricketts/WHO Presentation to TSEAC 17 Jan 2002
http://www.fda.gov/OHRMS/DOCKETS/ac/02/slides/3834s1.htm)
No data
0 - < 5
5 - < 10
10 - < 20
20 - < 100
100 - < 1.000
1.000 - < 10.000
> 10.000
Legend:(in tonnes)
20
UK Exports of Bovine Carcass Meat 1978 – 1998 (M. Ricketts/WHO Presentation to TSEAC 17 Jan 2002
http://www.fda.gov/OHRMS/DOCKETS/ac/02/slides/3834s1.htm)
No data
0 - < 5
5 - < 10
10 - < 20
20 - < 100
100 - < 1.000
1.000 - < 10.000
> 10.000
Legend:(in tonnes)
21
Total UK Exports of MBM 1988 – 1993(M. Ricketts/WHO Presentation to TSEAC 17 Jan 2002
http://www.fda.gov/OHRMS/DOCKETS/ac/02/slides/3834s1.htm)

22
Sanchez-Juan P et al. Source of variant Creutzfeldt-Jakob diseaseoutside United Kingdom. Emerg Infect Dis 2007;13:1166-9
Estimating possible risk of dietary exposureto BSE agent in Saudi Arabia
_____________
Cattle imports from the UK (1980–1990)
23
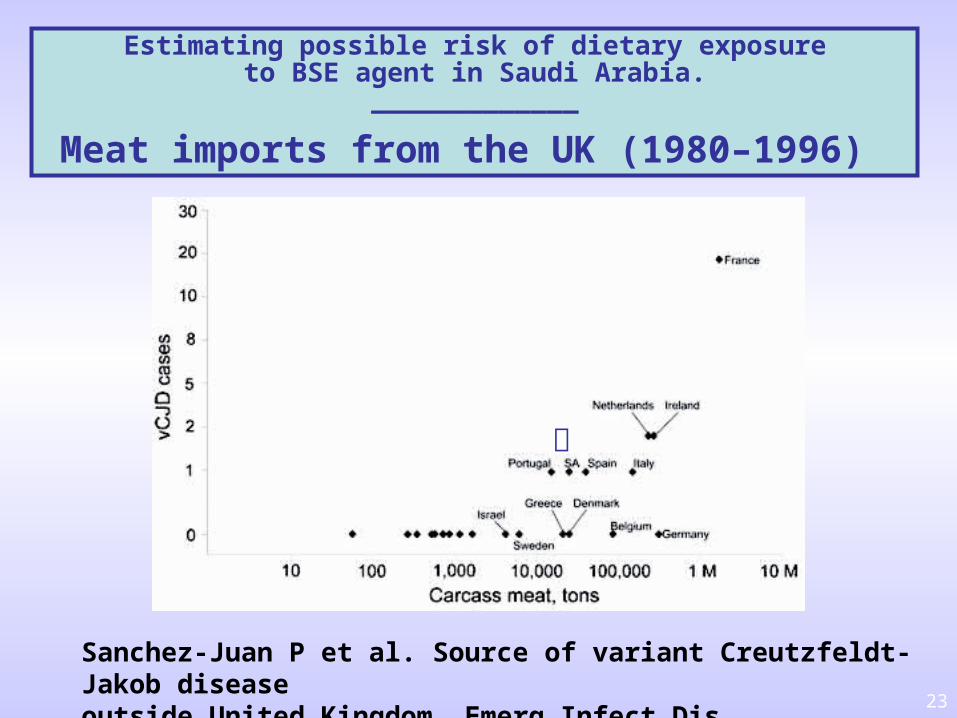
Sanchez-Juan P et al. Source of variant Creutzfeldt-Jakob diseaseoutside United Kingdom. Emerg Infect Dis 2007;13:1166-9
Estimating possible risk of dietary exposureto BSE agent in Saudi Arabia.
_____________
Meat imports from the UK (1980–1996)

24
Limitations of UK Customs and Excise DataRegarding BSE-related Exports 1980-1996(M. Ricketts/WHO Presentation to TSEAC 17 Jan 2002
http://www.fda.gov/OHRMS/DOCKETS/ac/02/slides/3834s1.htm)
Not informative about bovine exports from BSE countries except UK
Export data did not tally with national import records.
No information about re-packaging/“onward sales” (possibly obscuring UK origin of products)
Ignores illegal/other uncontrolled shipments No information about actual use of products (e.g.,
MBM as additive in animal feeds [higher risk] vs. fertilizer [lower risk])

25
vCJD cases per estimated population 2011
CountryvCJDcasesa
Estimated population 2011b Crude ratec
UK 175 62,688,000 2.8 x 10-6
Ireland 2 4,671,000 4.3 x 10-7
France 24 65,103,000 3.7 x 10-7
Portugal 2 10,760,000 1.9 x 10-7
Netherlands 3 16,847,000 1.8 x 10-7
Spain 5 46,755,000 1.1 x 10-7
Saudi Arabia 3 26,132,000 1.1 x 10-7
Italy 2 61,017,000 3.3 x 10-8
Japan 1 126,476,000 7.9 x 10-9
[a] Cases resident in UK 6 mo attributed to UK. [b] US Census Bureau estimates mid-2011[c] Not corrected for population age distribution or efficiency of case recognition/reporting.
26
FDA Considerations Regarding Saudi vCJD Cases
Crude rate of total vCJD cases for Saudi Arabia not greatly different from rates for several European countries
Overall risk for dietary exposure to BSE agent by the Saudi Arabian population as a whole, based on public information, less than that in UK
Since 1999, FDA used model to estimate risk of dietary exposure to BSE agent in various countries as % of risk in UK (risk in UK 1980-1996 taken to be 100%)
FDA adjusts recommended geographic deferrals taking into consideration risk relative to UK risk.
Caveat. Underlying information is highly uncertain.
27
FDA previously recommended BSE-related deferral of certain blood donors based on estimated
geographic risk relative to UK risk 1980-1996
Main BSE risk of concern: eating UK beef Donor dietary histories not reliable Proxy for history of beef consumption: time donor
spent in BSE risk country Assumption: dietary risk is stochastic, directly
related to time spent in BSE country of concern Relative to UK 1980-1996 = 1.00─ France = 0.05─ Switzerland = 0.015─Other Western European countries = Switzerland─ US military bases in Europe = 0.35

28
Estimating risk of exposure to BSE agent in Saudi Arabia 1980-1996
What might be a reasonable BSE-exposure risk estimate relative to UK and period of concern for donors resident in Saudi Arabia?
Saudi populations of concern 1980-1996
1. US military (very few US military dependents lived in Saudi Arabia)
2. US military contract workers and dependents3. Non-military contract workers and dependents4. Saudi nationals

29
FDA current considerations regarding possible additional deferrals/ineligibility criteria for certain blood and HCT/P
donors resident in Saudi Arabia 1990-1996.1. US Military
US military in Saudi ArabiaFDA assumes that the risk of dietary exposure
to the BSE agent on Saudi bases was similar to the risk on US military bases in Europe South of the Alps = 35% UK risk 1980-1996.
DoD recently estimated that actual procurements of UK beef might have been somewhat less than on European bases.
30
FDA current considerations regarding possible additional deferrals/ineligibility criteria for certain blood and HCT/P
donors resident in Saudi Arabia 1990-1996.1. US Military (2)
US military in Saudi Arabia 1980-1996 FDA currently recommends
deferral/ineligibility for donors of blood Source Plasma and HCT/Ps US military and dependents who spent 6 mo on bases South of the Alps 1980-1996.
New FDA consideration Recommend similar suitability criteria for
donors who served as US military personnel resident on Saudi bases 1980-1996

31
2. Other residents of Saudi Arabia.Military and Non-military Contractors
and Saudi Nationals
FDA assumes that BSE exposure risk of all contract workers is similar to that for the general Saudi population, because they all purchased food from local (non-US-military) establishments.
Caveat: Diets and medical care of contractors might not have been the same as that of the general Saudi population, possibly resulting in
─? Greater consumption of all beef and UK beef─? Greater likelihood of diagnosing vCJD

32
2. Other Residents of Saudi Arabia.Saudi Nationals (2)
Dietary risk of BSE exposure by Saudi nationals was probably much lower than the risk for the UK population 1980-1996:
UK export/Saudi import records suggest only ~ 10% of Saudi beef imported from UK
Average per-capita beef consumption in Saudi Arabia ~ 25% UK
Total estimated Saudi dietary BSE exposure risk ~ 2.5% UK risk
33
2. Other Residents of Saudi Arabia (3)Military and Non-military Contractors and Saudi Nationals
FDA assumes that risk of dietary exposure to UK beef by contract workers and Saudi nationals was similar to risk in non-UK Western European countries during years 1980-1996.
Non-UK countries of Western Europe with highest vCJD risk: France (and Ireland). A prudent precautionary assumption is that the risk in Saudi Arabia is unlikely to exceed the risk in France.
FDA assumes that BSE-exposure risk in Saudi Arabia, unlike France (which has had BSE in native bovines), is attributable almost entirely to imports of UK beef products, so that risk became negligible after the end of 1996.

34
2. Other Residents of Saudi Arabia (4)
FDA currently recommends deferral/ineligibility for all donors of blood, Source Plasma and HCT/Ps who spent 5 yr in France (as well as for donors with history of transfusion in France) from 1980 to the present time.
New FDA consideration for non-US-military residents of Saudi Arabia
Recommend suitability/eligibility criteria for any donor of Whole Blood, Source Plasma or HCT/Ps who spent cumulative 5 years or longer in Saudi Arabia during the years 1980-1996 (similar to recommendations for residents of France but not extending to the present time and not including deferral for history of transfusion)
35
US RecommendationsCompared with Canadian Donor Deferrals
Canadian blood establishments now defer blood donors resident in Saudi Arabia for any aggregate period 6 mo from 1980 to 1996 (end of UK BSE risk period).
US and Canadian blood and HCT/P donor deferral policies, while somewhat similar, are not identical.
(Implications of donor deferrals—especially for former military—differ for Canada and US.)

36
Geographic vCJD-related Blood Donor Deferralsin US and Canada
US FDAa
Canadian Blood Services Héma-Québec
UK 3 mo 1980-96 3 mo 1980-96 1 mo 1980-96
France ³ 5 yr1980-present
³ 5 yr1980-present
³ 3 mo³1980-present
Other Western Europe (WE)
³ 5 yr1980-present³ 28 countries
³ 5 yr1980-present12 countries
³ 6 mo1980-present12 countries
Hx of transfusion
UK, France1980-present
UK, France, WE 1980-present
UK, France, WE 1980-present
Saudi Arabia no deferral 6 mo 1980-96 6 mo 1980-96
a FDA recommends deferral of personnel resident on US military bases in Europe:North of Alps 1980-1990; South of Alps 1980-1996.
37
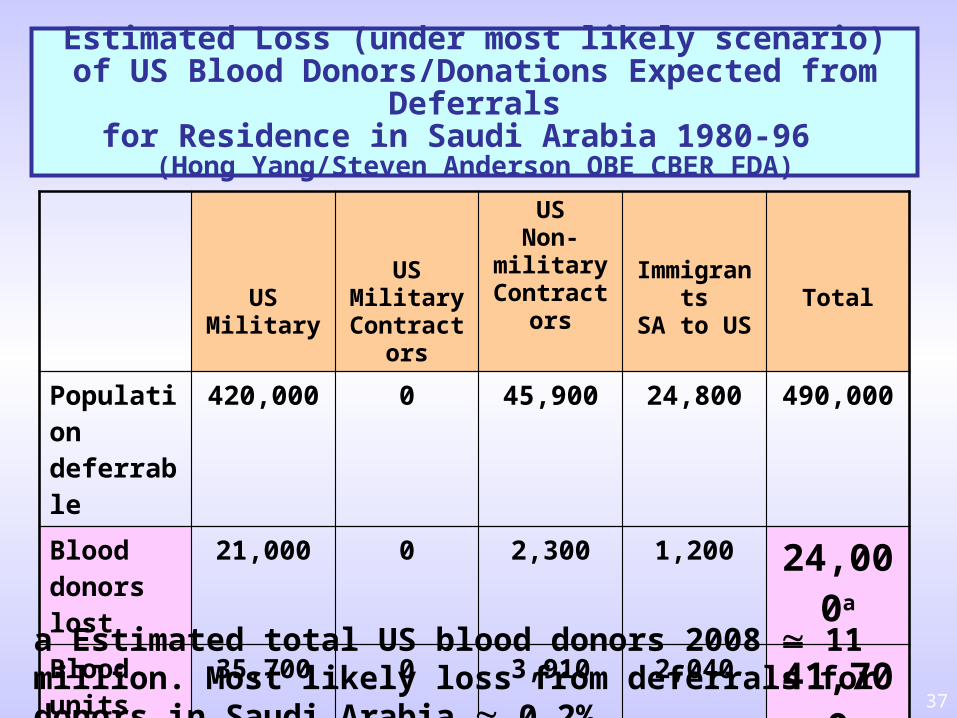
Estimated Loss (under most likely scenario) of US Blood Donors/Donations Expected from Deferrals
for Residence in Saudi Arabia 1980-96 (Hong Yang/Steven Anderson OBE CBER FDA)
US MilitaryUS Military Contractors
USNon-
military Contractors
ImmigrantsSA to US Total
Population deferrable
420,000 0 45,900 24,800 490,000
Blood donors lost
21,000 0 2,300 1,200 24,000a
Blood units lost
35,700 0 3,910 2,040 41,700
a Estimated total US blood donors 2008 11 million. Most likely loss from deferrals for donors in Saudi Arabia 0.2%

38
Conclusions
Three cases of vCJD are attributed to dietary exposures to BSE agent in Saudi Arabia 1980-1996.
Under current FDA recommendations, those donors would have been suitable/eligible donors of blood, plasma and HCT/Ps.
Crude prevalence of vCJD cases in Saudi Arabia is not markedly less than those in several European countries.
The most likely source of dietary exposure to the BSE agent in Saudi Arabia was imported UK beef.

39
Conclusions (2)
UK beef exports to Saudi Arabia ceased by the end of 1996.
FDA acknowledges a theoretical possibility that Saudi Arabia might have imported BSE-contaminated products from other countries after 1996 or introduced BSE into its own cattle herds; those are less likely sources of exposure.

40
Conclusions (3)
The US military procured an unknown but possibly significant amount of beef from the UK in 1980-1996 for bases in Saudi Arabia.
FDA considers a plausible worst-case assumption that the amount of UK beef consumed by US military in Saudi Arabia 1980-1996 might have been similar to that on European US military bases South of the Alps 1980-1996.
FDA assigned a geographical BSE risk of 35% UK risk 1980-1996 to European US military bases South of the Alps during the same years.
41
Conclusions (4)
FDA currently recommends deferral/ineligibility for donors of blood, Source Plasma and HCT/Ps who served in the US military and for their dependents who spent 6 mo on bases South of the Alps 1980-1996.
FDA is considering a recommendation to defer/consider ineligible donors who served as for 6 mo on US military bases in Saudi Arabia 1980-1996.

42
Conclusions (5)
At least 10% beef consumed by Saudi nationals living in Saudi Arabia 1980-1996 might have been imported from the UK.
Estimated per-capita beef consumption in Saudi Arabia appears to be less than that in UK (~25%).
FDA has tentatively assigned to Saudi Arabia a risk of dietary exposure to the BSE agent 1980-1996 = 2.5% that in the UK.
Contractors bought beef products in the same establishments as did Saudi nationals.

43
Conclusions (6)
FDA considers all contractors to have had the same potential risk of dietary exposure to BSE agent in Saudi Arabia 1980-1996 as did Saudi nationals.
Considering current estimates of crude prevalence of vCJD in Saudi Arabia compared with European countries, FDA considers it prudent to assume, as a realistic worst case, that true prevalence of vCJD in Saudi Arabia is unlikely to exceed that in France.
FDA believes that opportunities for dietary exposure to BSE agent in Saudi Arabia—unlike France—became negligible after the end of 1996.

44
Conclusions (7)
FDA currently recommends deferral/ineligibility for all donors of blood, Source Plasma and HCT/Ps who spent 5 yr in France 1980 to present
FDA is considering a similar recommendation to defer/consider ineligible donors of Whole Blood, Source Plasma and HCT/Ps who spent a cumulative period of 5 yr or longer in Saudi Arabia 1980-1996.
FDA estimates that the likely number of additional otherwise suitable blood donors who would be deferred under the new recommendations would be relatively small (perhaps 0.2% of current donors).

45
Questions for TSEAC
1. Do available data support the consideration by FDA to recommend deferring donors of blood and blood components, including Source Plasma, and to determine to be ineligible donors of HCT/Ps, who
a) spent six months or more cumulatively in Saudi Arabia as US military personnel from the beginning of 1980 through the end of 1996 or
b) otherwise spent more than five years cumulatively in Saudi Arabia from the beginning of 1980 through the end of 1996?

46
Questions for TSEAC (2)
2. Please discuss the likely contribution of those recommendations to the safety of the products involved and the possible impact on supplies of blood, blood components, plasma derivatives and HCT/Ps.
3. Please comment on additional information that might better inform FDA’s consideration of the proposed or any further safety measures.

47
TSEAC 23rd Meeting 01 Aug 2011
0
50
100
1stQtr
3rdQtr
East
West
North
normal brain sCJD cortical spongiform change
vCJD florid plaque
vCJD lymphoid PrP