Embed Size (px)
Citation preview

FATE O F PATIENTS W I T H RECURRENT CARCINOMA OF T H E BREAST
Recurrence Five or M o w Years after Initial Trea tmen t ANAXAGORAS N. PAPAIOANNOU, MD,” FREDERICK J. TANZ, M D , ~ AND
HERBERT VOLK, MD”
E
The appearance of metastases many years after primary treatment is not rare. The factors which determine prolonged latent periods are unknown. The belief that metastases which are latent for many years pursue a slow course after clinically evident, was not substantiated in several instances. This study under- took to identify possible characteristics of such patients and determine their fate. Fif ty-seven women with breast cancer whose recurrences developed 5 years or more after treatment were studied. Whereas the mean interval from treat- ment to recurrence was 10.4 years, the mean survival time after recurrence aver- aged 1.9 years. A comparison of this group with another group of 66 patients who developed recurrences between one and 2 years after treatment revealed only a slight and statistically insignificant (P < .09) difference in survival time after recurrence between these groups. In the majority of patients in this study metastatic breast cancer remaining latent for prolonged periods tends to pur- sue a comparatively rapid course once it becomes clinically manifest; this is only slightly different from the patient with early recurrence. However, a small percentage of patients in both groups will survive for long periods of time after metastases appear.
ECURRENT MAMMARY CANCER IN PATIENTS R who presumably have remained “cured” for many years following treatment has been reported in many isolated instances.3.4, 7 ,
Whereas the development of such late recur- rences no longer is viewed as a surprising phe- nomenon, the biological setting that renders some patients with breast cancer likely to re- main free of disease for a long time is not un- derstood. Also, the fate of these patients once they manifest their recurrences is not precisely
known. The belief that metastatic disease which remained latent for many years is likely to pursue a slow course5 when i t becomes clini- cally evident was not substantiated in our ex- perience in several instances.
Therefore, the present study was under- taken to examine the behavior of mammary cancer in all our patients who enjoyed a long “free-of-disease” interval and in whom even- tually recrudescent disease developed 5 years or more after their original treatment.
From the Department of Surgery, Albert Einstein College of Medicine of Yeshiva University, New York, N. Y.
* Assistant Professor of Surgery, Albert Einstein Col- lege of Medicinc of Yeshiva University, New York, N. Y.
t Present Address: U. S. Naval Hospital, St. Albans, N. Y.
Supported in part by research grant CA 03359 and undergraduate cancer training grant CA 5067 from the National Cancer Institute, U. S. Public Health Service.
The authors thank Dr. Boyce Bennett, Assistant Professor of Pathology, for studying all histologic sections; Dr. Arthur Krauss, Assistant Professor of Preventive Medicine, for the statistical analyses; and Dr. William Metcalf, Professor of Surgery, for his constructive criticism during the preparation of the manuscript.
Received for publication August 1, 1966.
MATERIAL AND METHODS
T h e records of the Bronx Municipal Hospi- tal Center (BMHC) Tumor Registry were re- viewed and 239 patients with recurrent can- cer of the breast were registered from 1954 through 1964. These patients originally were diagnosed and treated either at the Bronx Municipal Hospital Center or elsewhere and subsequently were cared for at some stage of their disease at this Center. Only patients with microscopically proved cancer of the breast who were free of disease for at least 5 years after their definitive treatment and in whom subsequently recurrence or metastatic cancer
37 1
372 CANCER March 1967 Vol. 20
developed, were selected. Sixty-one such pa- tients were found. One patient in this group was male and was excluded from the study. Also excluded were 3 female patients for whom inadequate data were available. Thus, 57 female patients were eligible for study and hereafter are called the “late recurrence group.” All patients were followed for at least one year after the development of their recur- rence.
One pathologist reclassified all procurable original and recurrent histologic material; the degree of nuclear anaplasia on each case, graded on the basis of Broder’sl criteria, was compared with that of the recurrent lesions.
T o determine what factors might influence a long vs. a short interval without evidence of neoplastic disease, we compared this group of 57 patients with all patients with cancer of the breast from our Tumor Registry whose re- crudescent disease developed between one and 2 years after original treatment. These latter patients also were followed for at least one year; 66 patients composed this group, which is hereafter referred to as the “early recurrence group.” These particular patients were se- lected for comparison because in our Tumor Registry they represent the “usual” mammary cancer patients who are destined to recur.
Factors generally considered of prognostic significance in mammary cancer, such as meno- pausal status, parity, etc., were examined criti- cally in an effort to identify specific features which might characteriLe the patients in the “late recurrence group.”
RESULTS
Analysis of “Late Recurrence Group” Personal data: At the time of original treat-
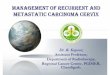
ment the mean age of this group was 53 years, with median of 52.3, range of 32 to 76 and peak age incidence in the sixth decade. Com- pared with a large series of unselected pa- tients3 in whom the peak age incidence was the fifth decade, our study group consists of somewhat older patients (Fig. 1).
Nineteen of these patients (33%) were pre- menopausal at the time of original treatment and 33 (58y0) were in or after the menopause. In 5 the menopausal status was unknown.
Nineteen patients were nulliparous and 32 were parous, with an average of 3 children. T h e status of parity of 6 patients could not be determined. This incidence of 33% nullipa- rity in this series is slightly higher than that
40 Unselected.Breast
I- z w 20 z w a 10
0 Ages 20-29 30-39
FIG. 1. Comparison of age distribution at diagnosis between unselected breast cancer patients and patients of this study. *From Haagensen, E. F.: Diseases of the Breast. Philadelphia/London, W. B. Saunders, 1956; p. 333.
reported in a large unselected group of breast cancer patients (2670).6
Forty-eight per cent of these patients were Jewish; 34y0 were Catholic; 10% were Prot- estant and 8% were of other religions. Only 3 patients in this group were Negro, the re- maining being Caucasian. These figures most likely reflect the composition of the popula- tion about the Bronx Municipal Hospital Cen- ter, which consists predominantly of Jewish and Catholic families.
I n many patients the data regarding loca- tion and delay between discovery of disease and institution of therapy were inadequate and therefore are not presented.
T u m o r characteristics: The location of the original lesion within the breast was known only in 38 patients; of these 19 were in outer quadrants, 13 were in central and 6 were in inner guadrants. This incidence is similar to that OT patients in tinselected cases.6
Histologically, 83.8% of the lesions were in- filtrating scirrhous duct cell carcinoma, an in- cidence similar to that of a large unselected series (76’%).7
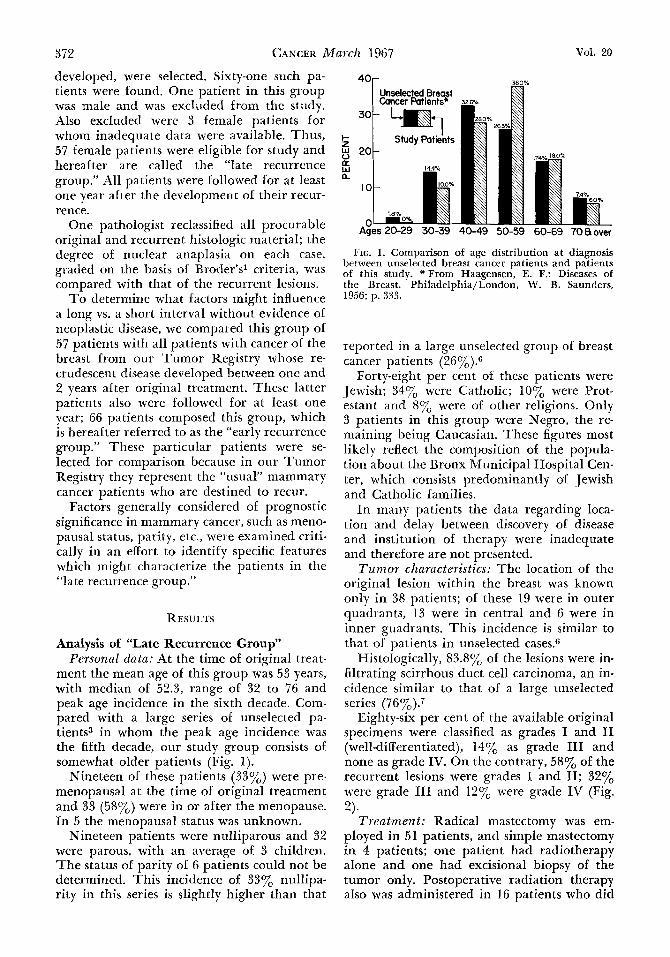
Eighty-six per cent of the available original specimens were classified as grades I and I1 (well-differentiated), 14% as grade I11 and none as grade IV. On the contrary, 58% of the recurrent lesions were grades I and 11; 32y0 were grade I11 and 12% were grade IV (Fig.
Trea tmen t : Radical mastectomy was em- ployed in 51 patients, and simple mastectomy in 4 patients; one patient had radiotherapy alone and one had excisional biopsy of the tumor only. Postoperative radiation therapy also was administered in 16 patients who did
2).
No. 3 RECURRENT CARCINOMA OF BREAST * Papaioannou et al. 373
local survived the longest and patients with visceral metastases survived the shortest pe- riods. Patients with osseous metastases pursued an intermediate course. This is in keeping with observations of other^.^
Free from clinical disease interval: The in- terval without evidence of neoplastic disease between treatment and recurrences ranged from 5 to 30 years, with a mean of 10.4 and a median of 8 years. For 9 patients still living at the time of this analysis this latent period ranges from 5 to 30 years, with a mean of 10.8
G r I G r I I Grm G r E years; 48 patients who now are dead had a latent period from 5 to 25 years, with a mean of 9.9 years (Table 3). FIG. 2. Nuclear grading (after Broders) of original
and recurrent lesions.
not differ from the remainder of the group in terms of stage of original disease or incidence of subsequent local or distant metastases.
After recurrence developed, these patients were treated by 2 or more of a variety of ther- apeutic modalities. Oophorectomy or ovarian irradiation, various natural, synthetic hor- monal or cytotoxic agents and radiotherapy were used as indicated in each case. In addi- tion, 2 patients underwent bilateral adrenalec- tomy and 2 others underwent hypophysectomy.
Site of initial recurrence: As the first mani- festation of recrudescent disease, local recur- rences developed in 24 patients, bone metas- tases in 20 and metastases in various viscera in 13 patients (Table 1). The site of recurrence is correlated with length of survival in Table 2. Patients whose initial site of recurrence was
TABLE 1. Site of Initial Recurrence of Patients with Late Recurrences
Site No. of patients yo of total
Local 24 42 Osseous 20 35 Visceral 13 23
TOTAL 57 100 __ -
TABLE 2. Initial Site of Recurrence and Subsequent Survival of Patients with Late Recurrences
Duration of survival Site (years) _ _ _ - _ _ ~ of original
metastases (1 1-2 2-3 3+ Average
Local 6 6 4 4 2.1 - ~
Osseous 6 5 4 1 1.9 Visceral 6 6 0 0 1 . 0 -
TOTAL 18 17 8 5
TABLE 3. Survival of Patients with Late Recurrences
Mean No. interval Mean Mean of free of survival total
Status pts. recurrence after recur. survival
Living 9 1 0 . 8 ~ 3.1 + y 14 + y Expired 48 9 . 9 y 1 . 7 y 11.5 y
Particularly interesting are 2 patients who lived 25 and 30 years prior to the develop- ment of their recurrences; their course is de- scribed below:
Case 1-M.B. (BMHC #158,086). This 62-year-old nulliparous woman came to the Bronx Municipal Hospital Center on May 13, 1960, complaining of pain in her back and both arms and legs for about 6 months. She had a left radical mastectomy for histologically proved carcinoma else- where in 1935. Physical examination on admission revealed a left radical mastec- tomy scar and no evidence of local recur- rence or tumor in the opposite breast. Skeletal survey revealed multiple lytic le- sions of the skull, spine, pelvis and other bones. Alkaline phosphatase was 4.8 Bod- ansky units on admission and shortly later rose to 7.6. Extensive work-up for detec- tion of a possible new primary was unre- vealing. Needle biopsy of the second and third lumbar vertebrae on June 1, 1960 revealed metastatic adenocarcinoma, most likely of mammary origin.
Palliative radiotherapy was adminis- tered to the symptomatic areas of the spine and the patient was started on 1 1 p-hydroxy-l7a-methyltestosterone propi- onate. This medication was not well toler-
374 CANCER March 1967 VOl. 20
ated and it was changed to testosterone propionate but without demonstrable change in her lesions. She expired at home one month later (October 23 , 1960) while on this medication.
Case 2-A.R.K. (BMHC #2,422). This 65- year-old woman, mother of one child, had a left radical mastectomy at another hos- pital on October 20, 1933 for histologi- cally proved cancer of the breast. She was apparently well for approximately 30 years. She came to the Bronx Municipal Hospital Center in May 1963, complain- ing of a 40-pound weight loss during the previous 6 months and a 3.0 X 2.0 cm cutaneous mass in the left side of her neck present for 3 months. A few other small cutaneous lesions were present on her back, the right side of her chest and the right axilla. No masses could be felt in the right breast and the liver was not palpable. Two mammograms of the right breast showed no pathologic findings. Skeletal survey revealed lytic lesions of the skull, ilium and right shoulder. Uri- nalysis, hematocrit, total protein, calcium, phosphorus and alkaline phosphatase were all within normal limits. Biopsy of the left cervical nodule on July 24, 1963 and of the nodule in the right axilla on October 20, 1964 revealed adenocarci- noma, most likely of breast origin. The original histologic material was not avail- able for comparison. On August 19, 1963, the patient was placed on norandrolone phenpropionate. There was no demon- strable change in her clinical status for 6 months. A new skeletal survey then re- vealed progression of her osseous lesions; the androgen was stopped and she was started on stilbestrol on December 7, 1964. Objective remission lasted for 9 months but at the time of this report her disease is progressing while on prednisone.
Survival after recurrence: At the time of this study, 84% (48 of 57) of the patients with late recurrences were dead. The mean survival time after recurrence for these 48 patients was 1.7 years, with a range one to 7 years. T h e mean total survival time from diagnosis to death for the 48 patients was 1 1.5 years and for the 9 living patients from diagnosis to present is 14 years (Table 3). Thus, it becomes ap- parent that, despite the long interval without evidence of neoplastic disease, most of these
patients will survive for less than 2 years once the disease recurs (Table 3).
Analysis of “Early Recurrence Group” and Comparison with “Late Recurrence Group”
T h e patients in the “early recurrence group” were selected because they represent the “usual” patient with metastatic breast cancer in our Registry. They also form the basis for comparison between 2 groups of patients dis- tinctly different in terms of latent period prior to recurrence. Some other characteristics of the control group are compared with those of the study group in Table 4. I t is shown that
TABLE 4. Comparison between Groups with Late and Earlv Recurrences
Late Early rccur. recur.
(57 pts.)* (66 pts.)+
No. % No. % ____
Menstrual status Menstruating 19 33 36 55 Postmenopausal 33 58 27 41 Unknown 5 9 3 4
Radical mastectomy 51 89 - . 59 89 Simple mastectomy
or other 6 11 7 11
Original treatment
Postop. radiotherapy 16 28 38 58
* Mean age a t mastectomy--53; range-32 to 76. t Mean age a t mastectomy--53; range-28 to 84.
the ages in both groups are comparable. T h e ratio of postmenopausal to premenopausa1 patients is roughly 2: 1 in the “late recurrence group” and 1:1 in the “early recurrence group.” The types of original treatment and treatment after recurrence were similar except for postoperative radiation therapy, which was given to patients more frequently with early recurrences. No attempt was made to correlate type of therapy to survival after re- currence owing to the great variety of thera- peutic modalities employed after the develop- ment of recurrence in both groups.
The mean difference in the interval free of recurrent cancer between the 2 groups was about 9 years. In Table 5 the survival of the two groups is compared. For the patients fol- lowed until death, the mean survival of pa- tients with early recurrences was 2.7 years and that of patients with late recurrences was 1 1.5 years; however, the mean survival after recurrence of the patients with early recur-
No. 3 RECURRENT CARCINOMA OF BREAST - Papaioannou et al. 375
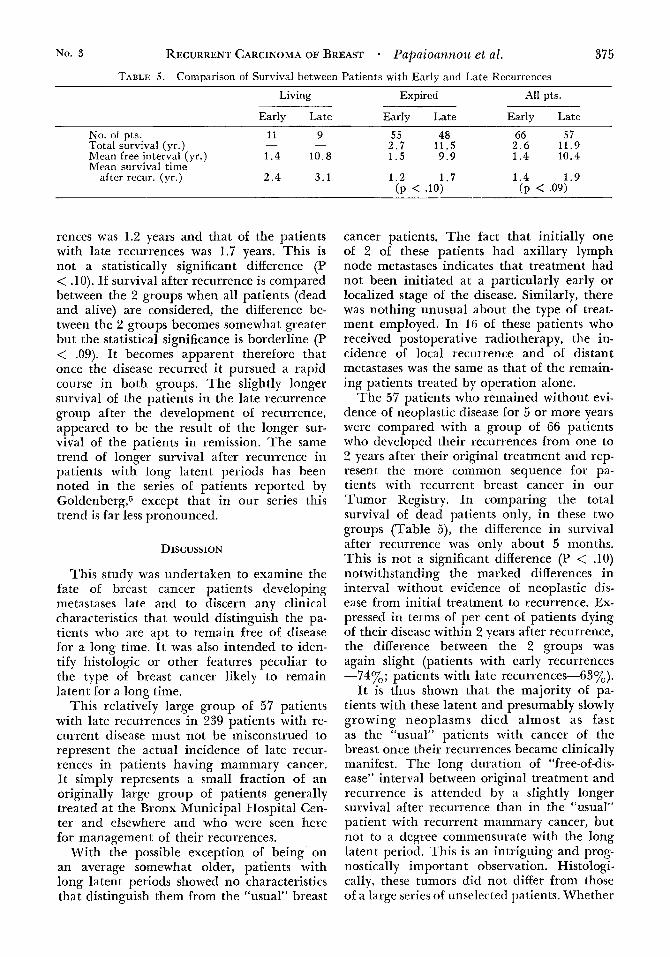
TABLE 5. Comparison of Survival between Patients with Early and Late Recurrences
Living Expired All pts.
Early Late Early Late Early Late ___- -
No. of pts. 11 9 55 48 66 57 Total survival (yr.) - - 2 . 7 11.5 2.6 11.9 Mean free interval (yr.) 1 . 4 10.8 1.5 9.9 1.4 10.4 Mean survival time
after recur. (yr.) 2 .4 3.1 1 . 2 1.7 1.4 1.9 (P .lo) (P .09)
rences was 1.2 years and that of the patients with late recurrences was 1.7 years. This is not a statistically significant difference (P < .lo). If survival after recurrence is compared between the 2 groups when all patients (dead and alive) are considered, the difference be- tween the 2 groups becomes somewhat greater but the statistical significance is borderline (P < .09). I t becomes apparent therefore that once the disease recurred i t pursued a rapid course in both groups. The slightly longer survival of the patients in the late recurrence group after the development of recurrence, appeared to be the result of the longer sur- vival of the patients in remission. The same trend of longer survival after recurrence in patients with long latent periods has been noted in the series of patients reported by Goldenberg,5 except that in our series this trend is far less pronounced.
DISCUSSION
This study was undertaken to examine the fate of breast cancer patients developing metastases late and to discern any clinical characteristics that would distinguish the pa- tients who are apt to remain free of disease for a long time. I t was also intended to iden- tify histologic or other features peculiar to the type of breast cancer likely to remain latent for a long time.
This relatively large group of 57 patients with late recurrences in 239 patients with re- current disease must not be misconstrued to represent the actual incidence of late recur- rences in patients having mammary cancer. It simply represents a small fraction of an originally large group of patients generally treated at the Bronx Municipal Hospital Cen- ter and elsewhere and who were seen here for management of their recurrences.
With the possible exception of being on an average somewhat older, patients with long latent periods showed no characteristics that distinguish them from the “usual” breast
cancer patients. The fact that initially one of 2 of these patients had axillary lymph node metastases indicates that treatment had not been initiated at a particularly early or localized stage of the disease. Similarly, there was nothing unusual about the type of treat- ment employed. In 16 of these patients who received postoperative radiotherapy, the in- cidence of local recurrence and of distant metastases was the same as that of the remain- ing patients treated by operation alone.
The 57 patients who remained without evi- dence of neoplastic disease for 5 or more years were compared with a group of 66 patients who developed their recurrences from one to 2 years after their original treatment and rep- resent the more common sequence for pa- tients with recurrent breast cancer in our Tumor Registry. In comparing the total survival of dead patients only, in these two groups (Table 5), the difference in survival after recurrence was only about 5 months. This is not a significant difference (P < .lo) notwithstanding the marked differences in interval without evidence of neoplastic dis- ease from initial treatment to recurrence. Ex- pressed in terms of per cent of patients dying of their disease within 2 years after recurrence, the difference between the 2 groups was again slight (patients with early recurrences -74yOb; patients with late recurrences-6B~o).
It is thus shown that the majority of pa- tients with these latent and presumably slowly growing neoplasms died almost as fast as the “usual” patients with cancer of the breast once their recurrences became clinically manifest. The long duration of “free-of-dis- ease” interval between original treatment and recurrence is attended by a slightly longer survival after recurrence than in the “usual” patient with recurrent mammary cancer, but not to a degree commensurate with the long latent period. This is an intriguing and prog- nos tically important observation. Histologi- cally, these tumors did not differ from those of a large series of unselected patients. Whether

376 CANCER March 1967 VOl. 20
this change in the clinical behavior of the tumor represents a sudden increase in its malignant potential or a decrease in the re- sistance of the host remains conjectural: how- ever, comparison of the nuclear grading be- tween original and recurrent lesions revealed a significantly higher degree of anaplasia in the recurrent lesions. This is not an unusual phenomenon with recurrent lesions in gen- eral but i t was very impressive in this study and the difference of the nuclear grading be- tween original and metastatic lesions corre- lated well with the change in the clinical be- havior of the neoplasms in our series.
A possible explanation of the comparatively sudden rapid growth of a latent neoplastic focus is that it had been implanted at or be- fore operation and continued to grow stead- ily and at the same rate but remained clini- cally imperceptible for a long time; when the recurrent tumor assumed sufficient size to be- come clinically evident, the course of the dis- ease actually kept the same pace of growth and i t was not explosive but consistent with the concept of exponential growth of tumors.2 Unfortunately, the information concerning
change in tumor size between clinical detec- tion of the tumor and their initial treatment is grossly inadequate and we are therefore unable to compare their growth rates prior to the initial treatment and after recurrences developed.
This study demonstrated that the majority of patients who develop metastases, either late (5 years or after) or early (within one to 2 years), will die from their disease between one and 2 years after clinical manifestations of recurrence; however, a small number of patients in both groups will live considerably longer after manifesting recrudescence. T h e numbers are too small to draw conclusions a t this time.
This study has revealed one of the many eccentricities of the behavior of breast cancer for which there is no satisfactory explanation at present. The all too commonly incrimi- nated but essentially unknown complex of biological factors referred to as host resistance, as well as the basic mechanisms of cancer growth have to be elucidated before these peculiarities of tumor behavior are under- stood.
REFERENCES
1. Broders, A. C.: The grading of carcinoma. Minn.
2. Collins, V. P.: Observations on lung metastases.
5. Goldenberg, I. S., Bailar, J. C., and Lowry, R.: Med. 8:726-730, 1925. Survival of women with hormonally treated breast
Am. J. Roentgen. 76:988-1000, 1956. 6. Haagensen, C. D.: Disease Of The Breast.
7. Lewison, E. F.: Breast Cancer and Its Diagnosis M* Long metastasis in mammary carci- and Treatment. Baltimore, Williams and Wilkins Co.,
1955. 8. Woolsey, G.: Late recurrence after radical opera-
tion for carcinoma of the breast. Ann. Surg. 80:928-932.
cancer. Surg. Gynec. Obstet. 119:785-789, 1964.
Philadelphia/London, W. B. Saunders, 1956. 3. Degnanj T. J.. G. *., and Dockerty,
noma. Minn. Med. 43:620-624, 1960. 4. Doyle, J. C., and Hummer, G. J.: Peritoneal car-
cinomatosis forty-one years after radical mastectomy. JAMA 149~1543.1545, 1952. 1924.