-
8/13/2019 Fat Necrosis in Autologous Abdomen Based Breast.3
1/10
BREAST
Fat Necrosis in Autologous Abdomen-BasedBreast Reconstruction: A
Systematic Review
Ibrahim Khansa, M.D.Adeyiza O. Momoh, M.D.
Priti P. Patel, M.D.John T. Nguyen, M.D.Michael J. Miller,
M.D.Bernard T. Lee, M.D.,
M.B.A.
Columbus, Ohio; Ann Arbor, Mich.;
and Boston, Mass.
Background: Fat necrosis is a common and potentially
exasperating complica-tion of autologous breast reconstruction. The
authors performed a systematicreview of the English literature on
autologous breast reconstruction to deter-mine significant patient
and surgical factors that are predictors of postoperativefat
necrosis.Methods: A PubMed search using the terms fat necrosis and
breast recon-struction was conducted. Articles were screened using
predetermined inclusionand exclusion criteria. Data collected
included patient characteristics, recon-structive techniques used,
and the specific postoperative morbidity of interest.Patient
cohorts were pooled, and the incidence of fat necrosis was
calculated inthe presence and absence of each risk factor.
Chi-square analysis was applied,and p 0.05 was considered
statistically significant.
Results: Of 172 articles found, 70 met the inclusion criteria.
The mean rate offat necrosis was 11.3 percent. Deep inferior
epigastric artery perforator flaps hadthe highest rate of fat
necrosis (14.4 percent), followed by pedicled transverserectus
abdominis musculocutaneous (12.3 percent), superficial inferior
epigas-tric artery (8.1 percent), and free transverse rectus
abdominis musculocutane-ous flaps (6.9 percent). Significant
predictors of fat necrosis included obesity(p 0.035),
prereconstruction irradiation (p 0.022),
postreconstructionirradiation (p 0.001), active smoking (p 0.001),
and abdominal scars (p0.05). Protective factors included
supercharging (p0.001) and bilateral re-construction (p
0.01).Conclusions: Although there is little agreement in the
literature regarding riskfactors for fat necrosis, the authors were
able to demonstrate several significantpredictors by systematically
analyzing 70 articles. Improved knowledge of the risk
factors for fat necrosis can help surgeons provide improved
preoperative coun-seling and take measures to minimize the risk of
this complication. (Plast.Reconstr. Surg. 131: 443, 2013.)
Fat necrosis is a common complication in au-tologous breast
reconstruction. It presents asa nodule or mass that can be palpated
after
reconstruction.1 It is caused by ischemia of thesubcutaneous
adipose tissue, leading to adiposecell necrosis, scarring, and
sometimes calcifica-tion. Although fat necrosis is not inherently
dan-gerous, it can mimic breast cancer recurrence
both clinically and radiographically. Clinically, itmay feel
benign when it consists of a smoothround nodule, but it can be an
irregular, fixedmass with skin retraction.1 On mammography, itcan
appear as an irregular density, spiculatedmass, or
microcalcifications.2When it mimics can-cer recurrence, fat
necrosis can lead to patientanxiety and additional biopsies.3 Fat
necrosis canalso negatively affect cosmetic outcome by
causingdistortion of the reconstructed breast.
There is no uniform definition of fat necrosisin the literature.
The most commonly used defi-
From the Department of Plastic Surgery, The Ohio StateUniversity
Wexner Medical Center; the Department of Sur-gery, Division of
Plastic and Reconstructive Surgery, Uni-versity of Michigan Medical
Center; and the Department of Surgery, Division of Plastic and
Reconstructive Surgery, BethIsrael Deaconess Medical Center,
Harvard Medical School.Received for publication July 18, 2012;
accepted September12, 2012.Copyright 2013 by the American Society
of Plastic Surgeons
DOI: 10.1097/PRS.0b013e31827c6dc2
Disclosure: The authors have no financial inter-ests in this
research project or in any of the tech-niques or equipment used in
this study. The authorshave no conflicts of interest to
disclose.
www.PRSJournal.com 443
-
8/13/2019 Fat Necrosis in Autologous Abdomen Based Breast.3
2/10
nition is that of a palpable subcutaneous firmnessnot due to
cancer.4 Other authors define fat ne-crosis based on size, with
some using firmnessmeasuring 1 cm in diameter3 and others
placingthe size threshold at 2 cm.5A less commonly useddefinition
of fat necrosis is radiologic, and definesit as an
ultrasound-detectable lesion greater than5 mm.6
Reported rates of fat necrosis vary widely, from3.04 to 37.9
percent.7 Although some risk factorsfor fat necrosis are consistent
in the literature,others such as obesity, irradiation, and
abdominalscars are the subject of debate.
Two studies have systematically examined fatnecrosis in
autologous breast reconstruction. Manet al. conducted a
meta-analysis of 36 studies,8 andSailon et al. conducted a
systematic review of eightstudies.9 Both reviews included only free
trans-
verse rectus abdominis musculocutaneous(TRAM) and deep inferior
epigastric artery per-forator (DIEP) flaps, and did not
specifically ex-amine risk factors for fat necrosis. The only
riskfactor analyzed was flap type, with both studiesconcluding that
the rate of fat necrosis was higherin DIEP flaps than in free TRAM
flaps.
In this systematic review, our objectives were(1) to calculate
the overall rate of fat necrosis inabdomen-based autologous breast
reconstruction,including pedicled TRAM, free TRAM, DIEP,
andsuperficial inferior epigastric artery (SIEA) flaps;
and (2) to identify potential predictors of fat ne-crosis,
including flap type, obesity, irradiation,smoking, abdominal scars,
recipient vessel selec-tion, surgical delay, supercharging, and
lateralityof reconstruction.
MATERIALS AND METHODS
Literature Search
A PubMed database search was conducted inMarch of 2011 using the
terms fat necrosis andbreast reconstruction as key words to
identify
studies in the English language published between1982 and 2011.
The articles were examined, andreferences were screened for further
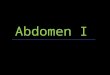
relevant ar-ticles. The search yielded a total of 172
citations.Inclusion criteria were English-language publica-tion,
human subjects, autologous breast recon-struction, extractable
outcomes on fat necrosis,and full-text availability. Exclusion
criteria weresystematic reviews and meta-analyses, case reportsand
case series with fewer than 15 patients, non-consecutive cases,
reconstructions that includedexpanders or implants, and
reconstructions that
included fat grafting. One hundred two studies
were excluded, yielding 70 articles suitable foranalysis (Fig.
1).
Data ExtractionFor each article, we extracted the data listed
in
Table 1. Not all data were available in every article.The fat
necrosis risk factors analyzed were flaptype, obesity, irradiation
(prereconstruction orpostreconstruction), smoking (former or
cur-rent), abdominal scars, recipient vessel, surgicaldelay,
supercharging, and laterality.
The flap types included were pedicled TRAM,free TRAM, DIEP, and
SIEA flaps. We excludedless commonly used flaps (e.g., superior
glutealartery perforator flaps) because of a scarcity ofdata.
Latissimus dorsi flaps were excluded, as fewarticles measured fat
necrosis rates.
Data Analysis and StatisticsWhen two or more articles from the
same in-
stitution had overlapping data collection dates,they were
assumed to be from the same cohort.When computing the overall rate
of fat necrosis,the article with the largest number of patients
wasincluded, and redundant articles were excluded.However, some of
the redundant articles analyzeddistinct predictors of fat necrosis,
and those wereincluded in the analysis of individual fat
necrosispredictors.
All articles that contained extractable data re-lated to
potential risk factors were used. The datawere pooled, and the
number of flaps with fatnecrosis was computed in the presence and
ab-sence of that risk factor. A chi-square test wasapplied, with
values ofp 0.05 signifying statis-tical significance.
RESULTSOverall Rate of Fat Necrosis
Forty-one articles3,5,6,1047 describeddistinct pa-tient cohorts
and were included in computation of
the overall rate of fat necrosis. Those representeda total of
10,764 flaps in 8970 patients; 1212 flapshad fat necrosis, for an
overall rate of 11.3 percent.
Flap TypeThirty-three articles3,6,7,2049 representing 7233
flaps in 6394 patients analyzed the rate of fat ne-crosis by
flap type (Table 2). The overall rate of fatnecrosis was 11.1
percent.
DIEP flaps had a significantly higher rate of fatnecrosis (14.4
percent) than free TRAM (6.9 per-cent, p 0.001), pedicled TRAM
(12.3 percent,
p
0.04), and SIEA flaps (8.1 percent, p
0.02).
Plastic and Reconstructive Surgery March 2013
444
-
8/13/2019 Fat Necrosis in Autologous Abdomen Based Breast.3
3/10
Free TRAM flaps had the lowest rate of fat necrosis(6.9
percent), which was significant in comparisonwith pedicled TRAM (p
0.001) and DIEP flaps(p 0.001).
ObesityFive articles4547,50,51 representing 1741 flaps in
1592 patients analyzed the rate of fat necrosis de-pending on
body mass index (Table 3). The rateof fat necrosis in obese
patients (body mass index
30) was 12.6 percent, significantly higher thannormal weight
(body mass index25, 7.8 percent;p 0.009) and nonobese patients
(body massindex 30, 8.7 percent; p 0.035). Fat necrosiswas also
nonsignificantly higher in obese patientsthan in overweight
patients (body mass index25and 30, 12.6 percent versus 8.7 percent;
nonsig-nificant). Fat necrosis was more common in obesepatients
than in normal weight patients receivinga pedicled TRAM flap (15.4
percent versus 9 per-cent,p 0.02) but not in free TRAM (7.8
percentversus 6.1 percent) or DIEP flaps (9.9 percent
versus 11.4 percent).
Radiation TherapyTwelve articles3,6,18,19,23,24,45,5256
representing 5059
flaps in 4587 patients analyzed the effect of radia-tion therapy
on fat necrosis (Table 4). The rate offat necrosis among patients
with no history of ir-radiation was 8.7 percent, significantly
lower thanin patients who had prereconstruction (11 per-cent, p
0.022) and postreconstruction irradia-tion (22.3 percent,p 0.001).
In pedicled TRAMflaps, those with prereconstruction irradiationhad
a higher rate of fat necrosis than patients with
no history of irradiation (13.4 percent versus 9.3percent,p
0.028).
Smoking
Seven articles3,6,22,44,45,51,57 representing 2347flaps in 2187
patients analyzed the rate of fat ne-crosis in relation to smoking
(Table 5). The rateof fat necrosis among current smokers was
15.6percent, which was significantly higher comparedwith patients
who had never smoked (7.1 percent,p 0.001), former smokers (8.7
percent, p
0.03), and non current smokers (9.7 percent,p
Fig. 1. Study attrition diagram.
Volume 131, Number 3 Fat Necrosis in Breast Reconstruction
445
-
8/13/2019 Fat Necrosis in Autologous Abdomen Based Breast.3
4/10
0.001). The difference between current smokersand noncurrent
smokers was significant in pedi-cled TRAM flaps (18.7 percent
versus 9.5 percent,p 0.004), but not in free TRAM (11.1
percentversus 7.7 percent,p 0.22) or DIEP flaps (14.5percent
versus12.8 percent,p 0.68). Fat necrosisin former smokers was no
higher than in neversmokers (8.7 percent versus 7.1 percent,p
0.47).
Abdominal ScarsThree articles22,45,58 representing 874 flaps
in
824 patients analyzed the effect of abdominal scars
on fat necrosis (Table 6). Fat necrosis among pa-
tients with abdominal scars was significantlyhigher than in
those without abdominal scars(14.9 percent versus 10.4 percent,p
0.05). Thisdifference was also present in pedicled TRAMflaps (16.8
percent versus 8.5 percent,p 0.005)but not any other flap type.
One of the three articles58 specified what typeof abdominal scar
each patient had and found thatpatients with Pfannenstiel,
laparoscopic, midline,and right lower quadrant scars did not have
anincreased rate of fat necrosis, whereas patientswith paramedian
(50 percent versus 15 percent,p 0.17) and subcostal scars (20
percent versus 15percent,p 0.75) had a nonsignificant increasein
fat necrosis.
Recipient Vessels
Five articles3,56,5961 representing 2064 flaps in1621 patients
analyzed the effect of recipient ves-sel choice on fat necrosis
(Table 6). The rate of fatnecrosis was no different when internal
mam-mary vessels were used compared with thora-codorsal vessels
(6.2 percent versus 7.6 percent,p 0.22). Among free TRAM flaps, the
rate offat necrosis was significantly lower when internalmammary
vessels were used compared with tho-racodorsal vessels (24.2
percent versus 14 per-cent, p 0.026).
Delay of Pedicled TRAM FlapsTwo articles62,63 representing 250
flaps in 181
patients analyzed the effect of surgical delay on fatnecrosis in
pedicled TRAM flap reconstruction(Table 7). The rate of fat
necrosis tended to belower when surgical delay was performed, but
thedifference was not statistically significant (5.7 per-cent
versus 11.8 percent, p 0.097).
Supercharge of Pedicled TRAM FlapsThree articles3133
representing 104 flaps in
104 patients analyzed the effect of microsurgical
supercharging of pedicled TRAM flaps on fat ne-crosis (Table 7).
Supercharged flaps were found tohave a significantly lower rate of
fat necrosis thannonsupercharged pedicled TRAM flaps (12.3 per-cent
versus 41 percent, p 0.001).
Unilateral versus Bilateral ReconstructionNine
articles6,20,21,43,51,6467 representing 1838
flaps in 1209 patients analyzed the effect of later-ality on fat
necrosis (Table 6). Bilateral recon-structions had a significantly
lower rate of fat ne-crosis than unilateral reconstructions
(10.7
percent versus 14.8 percent,p
0.01). The same
Table 1. Data Extracted from the Articles
Study characteristicsInstitutionDates of data collection
Patients and flapsNo. of patientsNo. of flapsFlap type
pTRAMfTRAMDIEPSIEA
Patient characteristicsBMI
Normal weight (25)Overweight (25 and 30)Nonobese (30)*Obese
(30)
IrradiationNo irradiationPrereconstruction
irradiationPostreconstruction irradiation
Smoking
Never smokedFormer smokerNoncurrent smokerCurrent smoker
Abdominal scarsNo scar(s)Scar(s)
Other surgical detailsRecipient vessel used
Internal mammaryThoracodorsal
Surgical delay of pTRAM flappTRAM without delaypTRAM with
delay
Supercharge of TRAM flapTRAM without supercharge
TRAM with superchargeLateralityUnilateral
reconstructionBilateral reconstruction
Fat necrosisDefinitionOverall ratePredictors
pTRAM,pedicled TRAM; fTRAM,free TRAM; BMI, body
massindex.*Obtained by combining the patients in the normal weight
andoverweight categories.Obtained by combining the patientsin the
never smoker and formersmoker categories.
Plastic and Reconstructive Surgery March 2013
446
-
8/13/2019 Fat Necrosis in Autologous Abdomen Based Breast.3
5/10
was true among free TRAM flaps (1 percent versus11.1 percent, p
0.003). There was also a notstatistically significant tendency
toward lower ratesof fat necrosis in bilateral DIEP (12.6 percent
ver-sus 16.7 percent,p 0.076) and pedicled TRAMflaps (10.3 percent
versus 12.6 percent,p 0.48)
compared with unilateral reconstructions.
DISCUSSIONThe studies analyzed cite a fat necrosis rate in
autologous breast reconstruction ranging from3.04 to 37.9
percent.7 The overall rate of fat ne-crosis was 11.3 percent across
all types of breastreconstruction in aggregate. In articles that
dif-
ferentiated by type of reconstruction, the overall
Table 2. Fat Necrosis Rates in the Systematic Review of the
Literature and Crude Pooled Analysis
Flap Type No. of Flaps Fat Necrosis (%) Range (%) p
pTRAM 2208 272 (12.3) 6.8376033 fTRAM 2423 168 (6.9) 2.14028.632
0.001 (vs. pTRAM)DIEP 2429 350 (14.4) 3.34242.920 0.04 (vs. pTRAM);
0.001 (vs. fTRAM)SIEA 173 14 (8.1) 5.73813.511 NS (vs. pTRAM); NS
(vs. fTRAM); 0.02 (vs. DIEP)
Total 7233 804 (11.1) 2.140
6033
pTRAM, pedicled TRAM; fTRAM, free TRAM.
Table 3. Obesity as a Predictor of Fat Necrosis
No. of Flaps Fat Necrosis (%) p
Normal weight (BMI 25) 965 75 (7.8) pTRAM 488 44 (9) fTRAM 442
27 (6.1) DIEP 35 4 (11.4)
Overweight (BMI 25, 30) 242 21 (8.7) pTRAM fTRAM 212 19 (9) DIEP
30 2 (6.7)
Nonobese (BMI 30) 1431* 125 (8.7)*
pTRAM 488 44 (9) fTRAM 654 46 (7) DIEP 289 35 (12.1)
Obese (BMI 30) 310 39 (12.6) 0.009 (vs. normal weight); NS (vs.
overweight);0.035 (vs. nonobese)
pTRAM 175 27 (15.4) 0.02 (vs. normal weight); 0.02 (vs.
nonobese)fTRAM 64 5 (7.8) NS (vs. normal weight, overweight and
nonobese)DIEP 71 7 (9.9) NS (vs. normal weight, overweight and
nonobese)
BMI, body mass index; pTRAM, pedicled TRAM; fTRAM, free TRAM;
NS, nonsignificant.*The numbers for nonobese patients may be larger
than the sum of the numbers for normal weight and overweight
patients, because somearticles report results as obese versus
nonobese rather than obese versus overweight versus normal weight.
No extractable data on obesity
were available for SIEA flaps.
Table 4. Radiation Therapy as a Predictor of Fat Necrosis
No. of Flaps Fat Necrosis (%) pPrereconstruction XRT 1051* 116
(11)*
pTRAM 343 46 (13.4) fTRAM 170 22 (12.9) DIEP 77 12 (15.6)
Postreconstruction XRT 188* 42 (22.3)* pTRAM 19 3 (15.8) fTRAM
32 14 (43.8) DIEP 55 14 (25.5)
No XRT 3820* 334 (8.7)* 0.022 (vs. prereconstruction XRT);0.001
(vs. postreconstruction XRT)
pTRAM 1169 109 (9.3) 0.028 (vs. prereconstruction XRT);NS (vs.
postreconstruction XRT)
fTRAM DIEP 233 39 (16.7) NS (vs. prereconstruction and
postreconstruction XRT)
XRT, radiation therapy; pTRAM, pedicled TRAM; fTRAM, free TRAM;
NS, nonsignificant.*The numbers for each category may be larger
than the sum of the subcategories by flap type, because some
articles that were included donot break their results down by flap
type. No extractable data on irradiation were available for free
TRAM and SIEA flaps.
Volume 131, Number 3 Fat Necrosis in Breast Reconstruction
447
-
8/13/2019 Fat Necrosis in Autologous Abdomen Based Breast.3
6/10
rate of fat necrosis was 11.1 percent. The mostimportant
predictor of fat necrosis was flap type,with free TRAM flaps having
the lowest rate of fatnecrosis (6.9 percent), followed by SIEA (8.1
per-cent), pedicled TRAM (12.3 percent), and DIEP
flaps (14.4 percent).
The lower rate of fat necrosis in free TRAMcompared with DIEP
flaps has been demonstratedin the past. In their meta-analysis, Man
et al. foundthat DIEP flaps were twice as likely as free TRAMflaps
to have fat necrosis.8 Sailon et al.9 and Scheeret al.20 had
similar findings. The free TRAM flapuses the dominant pedicle to
the lower abdominal
tissue, the deep inferior epigastric vessels, takingadvantage of
all perforators that course throughthe rectus muscle to the
overlying adipose tissueand skin.68 In contrast, the DIEP flap
selects onlythe largest perforators, potentially leading to
areaswith suboptimal perfusion. A recent advance inDIEP flap
reconstruction has been preoperativeperforator mapping using
computed tomo-graphic angiography or magnetic resonance
an-giography, which allows identification of a domi-nant perforator
preoperatively and likely shortensoperative times.69 More studies
are needed to show
whether this translates into lower rates of fat ne-
Table 5. Smoking as a Predictor of Fat Necrosis
No. of Flaps Fat Necrosis (%) p
Never smoked 680 48 (7.1) pTRAM 162 13 (8) fTRAM 518 35 (6.8)
DIEP
Former smoker 173 15 (8.7) pTRAM 21 2 (9.5) fTRAM 152 13 (8.6)
DIEP
Noncurrent smoker* 2026* 197 (9.7)* pTRAM 665 63 (9.5) fTRAM 757
58 (7.7) DIEP 399 51 (12.8)
Current smoker 321 50 (15.6) 0.001 (vs. never smoked); 0.03 (vs.
former smoker);0.001 (vs. noncurrent smoker)
pTRAM 107 20 (18.7) 0.009 (vs. never smoked); NS (vs. former
smoker);0.004 (vs. noncurrent smoker)
fTRAM 108 12 (11.1) NS (vs. never smoked, former smoker
andnoncurrent smoker)
DIEP 83 12 (14.5) NS (vs. noncurrent smoker)
pTRAM, pedicled TRAM; fTRAM, free TRAM.
*The numbers for noncurrent smokers may be larger than the sum
of the numbers for never smoked and former smokers, because
somearticlesreport results as current smoker vs. noncurrent smoker
rather thancurrentsmoker vs. former smoker vs. never smoker.
Extractabledata on smoking were not available for SIEA flaps.
Table 6. Recipient Vessel, Laterality, and AbdominalScars as
Predictors of Fat Necrosis in MicrosurgicalBreast
Reconstruction*
No. ofFlaps
FatNecrosis (%) p
Recipient vesselInternal mammary 776 48 (6.2)
fTRAM 143 20 (14) Thoracodorsal 1288 98 (7.6) NS
fTRAM 153 37 (24.2) 0.026LateralityUnilateral reconstruction 580
86 (14.8)
pTRAM 127 16 (12.6) fTRAM 99 11 (11.1) DIEP 354 59 (16.7)
Bilateral reconstruction 1258 135 (10.7) 0.01pTRAM 526 54 (10.3)
NSfTRAM 96 1 (1) 0.003DIEP 636 80 (12.6) NS
Abdominal scarsNo abdominal scars 566 59 (10.4)
pTRAM 413 35 (8.5) fTRAM 39 7 (17.9) DIEP 114 17 (14.9)
Abdominal scars 308 46 (14.9) 0.05
pTRAM 143 24 (16.8) 0.005fTRAM 61 7 (11.5) NSDIEP 104 15 (14.4)
NS
pTRAM, pedicled TRAM; fTRAM, free TRAM; NS, nonsignificant.*No
extractable data on recipient vessel selection were available
forDIEP and SIEA flaps. No extractable data on laterality or
abdominalscars were available for SIEA flaps.
Table 7. Surgical Delay and Supercharging asPredictors of Fat
Necrosis in Pedicled TRAM FlapReconstruction
No. ofFlaps
FatNecrosis (%) p
Surgical delayDelay 106 6 (5.7)No delay 144 17 (11.8) NS
Supercharging
pTRAM 39 16 (41)Supercharged pTRAM 65 8 (12.3) 0.001
NS, not significant; pTRAM, pedicled TRAM.
Plastic and Reconstructive Surgery March 2013
448
-
8/13/2019 Fat Necrosis in Autologous Abdomen Based Breast.3
7/10
crosis. Another potential explanation for differ-ences between
free TRAM and DIEP flaps may bethat articles analyzing DIEP flaps
were publishedby surgeons early in the learning curve.35
Obesity is considered a risk factor for fatnecrosis in
autologous breast reconstruction,with some studies demonstrating a
significantrelationship,3,20,22,24,41,45,67,70,71 and
othersnot.6,11,15,46,47,50 In our systematic analysis,
obesepatients had a significantly higher rate of fat ne-crosis than
nonobese patients. This relationshipwas true across all
reconstruction types combinedand for pedicled TRAM flaps alone.
This is likelyrelated to the larger size flap required in
obesepatients. In the past, zone IV has been included toincrease
the size of the reconstruction; however,current practices avoid use
of zone IV, as perfusionis less reliable. Using ex vivo angiograms,
Ohjimi
et al. demonstrated much lower perfusion in zoneIV.72 Vega et
al. lowered rates of fat necrosis byroutinely excising zone IV in
all patients.4 Krolllowered fat necrosis rates in DIEP flaps from
62.5percent to 17.4 percent by limiting the use of theDIEP flap to
70 percent of the flap, supporting thediscarding of zone IV.73
The literature on prereconstruction irradiationand fat necrosis
is inconclusive. In our analysis, pa-tients with a history of
prereconstruction irradiationwere at increased risk of fat necrosis
compared withno irradiation. One study demonstrated increased
rates of fatnecrosis after prereconstruction radiationtherapy
with pedicled TRAM flaps.70 Many studies,however, have not
demonstrated an increased rateof fat necrosis.3,6,23,65 Fosnot et
al. found that prere-construction irradiation made the dissection
andmicrovascular anastomosis more difficult.18
In our analysis, patients with postreconstruc-tion irradiation
had more than twice the rate of fatnecrosis compared with no
irradiation. Irradiationis known to affect the microcirculation,
and irra-diating a flap can compromise the blood supply tothe
adipose tissue, leading to fat necrosis. Multiple
studies have found a correlation between postre-construction
irradiation and fat necrosis.29,52,53,74
Some studies investigating the relationship be-tween smoking and
fat necrosis have demon-strated a relationship,3,4,29,44,75whereas
others havenot.6,11,45,57 In a review of 1195 breast
reconstruc-tions, Mehrara et al. found that smokers were at
noincreased risk of fat necrosis.15 In our analysis, activesmokers
had a significantlyhigher rate of fatnecrosiscompared with past
smokers and never smokers.Former smokers were at no increased risk
of fatnecrosis compared with never smokers, demonstrat-
ing that patients who quit smoking can safely un-
dergo autologous breast reconstruction. Smoking isknown to
adversely affect both microvasculature andmacrovasculature by
several mechanisms, includingnicotine-mediated vasospasm.
The literature is ambivalent on abdominalscars as a risk factor
for fat necrosis. Some studieshave demonstrated a relationship
between scarsand fat necrosis,15,45 whereas others have
not.22,58
In our analysis, patients with abdominal scars hadsignificantly
higher rates of fat necrosis. Parrett etal. found that women with a
Pfannenstiel scar wereat no increased risk of fat necrosis,
provided thatthe scar was included at the border and
notundermined.58 Midline scars were not a risk factorfor fat
necrosis, provided that the contralateralpart of the flap was
discarded in unilateral recon-structions. The highest rates of fat
necrosis werefound in paramedian and subcostal scars, as these
have the highest potential to interrupt perforatorsto the
abdominal wall. Interestingly, Mahajan et al.found that patients
with a Pfannenstiel scar hadlarger perforators and concluded that
the scareffectively led to surgical delay by ligation of
thesuperficial inferior epigastric vessels.76 Xu et al.have
advocated the use of bipedicle flaps for uni-lateral breast
reconstruction in patients with ab-dominal scars.14
On review of the literature, free flaps anasto-mosed to the
internal mammary and thoracodor-sal vessels had the same rate of
fat necrosis. Tem-
ple et al.56 and Saint-Cyr et al.60 reached a similarconclusion.
The choice of recipient vessel is oftenmade on a case-by-case
basis. The thoracodorsalvessels are exposed and readily available
in caseswhere axillary dissection is performed. However,with the
rise of sentinel lymph node biopsy, theneed for axillary dissection
has decreased, and useof the internal mammary vessels has become
morecommon.59
Surgical delay has been used to improve vas-cularity of axial
flaps. In pedicled TRAM flaps,ligation of the superficial and deep
inferior epi-
gastric vessels is performed 2 to 3 weeks before theplanned
reconstruction. On review of studies an-alyzing pedicled TRAM flaps
in high-risk patients,we found a nonsignificant decrease in fat
necrosisin patients who had undergone surgical delay.Codner et al.
found a nonsignificant trend towardlower rates of fat necrosis when
surgical delay wasperformed (3.3 percent versus 12 percent, p
0.14).62
Supercharging is another method of improv-ing blood flow in
pedicled TRAM flaps. It consistsof anastomosing the deep inferior
epigastric ves-
sels to recipient vessels in the chest in addition to
Volume 131, Number 3 Fat Necrosis in Breast Reconstruction
449
-
8/13/2019 Fat Necrosis in Autologous Abdomen Based Breast.3
8/10
the primary vascular supply of the superior epi-gastric pedicle.
We found that supercharged pedi-cled TRAM flaps have a
significantly lower rate offat necrosis. Most studies examining the
effect ofsupercharging found that it does improve out-comes,
namely, fat necrosis. Lee et al. demon-strated a significant
increase in the venous oxygenconcentration in the flap, and lower
rates of fatnecrosis.33 Because most fat necrosis tends to oc-cur
in zone IV of the flap, supercharging a uni-pedicled TRAM flap
through the contralateral in-ferior epigastric vessels may provide
improvedblood flow into zone IV, as shown by Yamamotoet al.32 Hamdi
et al. achieved a low rate of fatnecrosis by performing bipedicled
perforatorfree flaps with two microvascular anastomosesfor
unilateral reconstruction.77 This is an inno-
vative form of supercharging specific to perfo-rator flaps, and
further studies are warranted tomeasure its effectiveness.
We found that bilateral reconstructions hadsignificantly lower
rates of fat necrosis than uni-lateral reconstructions. Kroll
demonstrated a sim-ilar result in DIEP flaps.73 Paige et al. found
anonsignificant tendency toward lower rates of fatnecrosis in
bilateral pedicled TRAM flaps.67 Theeffect of laterality relates to
the size and reliabilityof the zones that are harvested. As
bilateral flaps,by definition, cannot use any tissue across the
mid-
line, these flaps are smaller and the blood supplyis more
reliable.
Although our systematic review has severalstrengths, including a
large number of patientsand flaps, and analysis of multiple risk
factors forfat necrosis across four different types of autolo-gous
breast reconstruction, it does have some lim-itations. The majority
of studies in our review areretrospective and observational, with
confoundersand biases beyond our control. Ideally, a meta-analysis
would be performed from randomizedcontrol studies, but these were
not found in ourreview and would be difficult to perform.
Oursystematic review can be considered a form ofpooled analysis or
meta-analysis from publisheddata. Finally, fat necrosis does not
have a consis-tent definition across studies, as discussed in
theIntroduction. This affects our ability to truly com-pare
studies. As a result of the heterogeneity of thedefinition of fat
necrosis, and different levels ofexperience among surgeons, the
results shown inthis article may not reflect each surgeons
indi-vidual experience, but are designed to identify risk
factors for fat necrosis in general.
CONCLUSIONSThere is significant variability in the
literature
regarding risk factors for fat necrosis in autolo-gous breast
reconstruction. By providing a com-prehensive review of risk
factors for fat necrosis,
this study can help plastic surgeons adequatelycounsel patients
preoperatively and take measuresto minimize the incidence of this
complication.
Bernard T. Lee, M.D., M.B.A.Department of Surgery
Division of Plastic and Reconstructive SurgeryBeth Israel
Deaconess Medical Center
Harvard Medical School110 Francis Street, Suite 5A
Boston, Mass. [email protected]
REFERENCES
1. Hogge JP, Robinson RE, Magnant CM, Zuurbier RA.
Themammographic spectrum of fat necrosis of the
breast.Radiographics 1995;15:13471356.
2. Kim SM, Park JM. Mammographic and ultrasonographicfeatures
after autogenous myocutaneous flap reconstructionmammoplasty. J
Ultrasound Med. 2004;23:275282.
3. Baumann DP, Lin HY, Chevray PM. Perforator number pre-dicts
fat necrosis in a prospective analysis of breast recon-struction
with free TRAM, DIEP, and SIEA flaps.
PlastReconstrSurg.2010;125:13351341.
4. Vega S, Smartt JM Jr, Jiang S, et al. 500 Consecutive
patientswith free TRAM flap breast reconstruction: A single
sur-geons experience. Plast Reconstr Surg. 2008;122:329339.
5. Lin SJ, Nguyen MD, Lee BT, et al. Tissue oximetry moni-toring
in microsurgical breast reconstruction decreases flaploss and
improves rate of flap salvage. Plast Reconstr
Surg.2011;127:10801085.
6. Peeters WJ, Nanhekhan L, Van Ongeval C, Fabre G, Vande-voort
M. Fat necrosis in deep inferior epigastric perforatorflaps: An
ultrasound-based review of 202 cases. Plast
ReconstrSurg.2009;124:17541758.
7. Garvey PB, Buchel EW, Pockaj BA, et al. DIEP and pedicledTRAM
flaps: A comparison of outcomes.Plast Reconstr
Surg.2006;117:17111719; discussion 17201721.
8. Man LX, Selber JG, Serletti JM. Abdominal wall followingfree
TRAM or DIEP flap reconstruction: A meta-analysis andcritical
review. Plast Reconstr Surg. 2009;124:752764.
9. Sailon AM, Schachar JS, Levine JP. Free transverse rectus
abdominis myocutaneous and deep inferior epigastric per-forator
flaps for breast reconstruction: A systematic review offlap
complication rates and donor-site morbidity.Ann
PlastSurg.2009;62:560563.
10. Casey WJ III, Chew RT, Rebecca AM, Smith AA, Collins
JM,Pockaj BA. Advantages of preoperative computed tomogra-phy in
deep inferior epigastric artery perforator flap
breastreconstruction. Plast Reconstr Surg. 2009;123:11481155.
11. Chun YS, SinhaI, Turko A, Lipsitz S, Pribaz JJ. Outcomes
andpatient satisfaction following breast reconstruction with
bi-lateral pedicled TRAMflaps in 105 consecutive patients.
PlastReconstr Surg.2010;125:19.
12. Knight MA, Nguyen DT IV, Kobayashi MR, Evans GR.
Insti-tutional review of free TRAM flap breast reconstruction.
Ann
Plast Surg. 2006;56:593598.
Plastic and Reconstructive Surgery March 2013
450
-
8/13/2019 Fat Necrosis in Autologous Abdomen Based Breast.3
9/10
13. Chang EI, Vaca L, DaLio AL, Festekjian JH, Crisera K.
As-sessment of advanced age as a risk factor in microvascularbreast
reconstruction. Ann Plast Surg.2011;67:255259.
14. Xu H, Dong J, Wang T. Bipedicle deep inferior
epigastricperforator flap for unilateral breast reconstruction:
Sevenyears experience. Plast Reconstr Surg.2009;124:17971807.
15. Mehrara BJ, Santoro TD, Arcilla E, Watson JP, Shaw WW,
Da
Lio AL. Complications after microvascular breast
reconstruc-tion: Experience with 1195 flaps. Plast Reconstr Surg.
2006;118:11001109; discussion 11101111.
16. Follmar KE, Prucz RB, Manahan MA, Magarakis M, Rad AN,Rosson
GD. Internal mammary intercostal perforators in-stead of the true
internal mammary vessels as the recipientvessels for breast
reconstruction. Plast Reconstr Surg. 2011;127:3440.
17. Clough KB, ODonoghue JM, Fitoussi AD, Vlastos G, FalcouMC.
Prospective evaluation of late cosmetic results followingbreast
reconstruction: II. TRAM flap reconstruction. PlastReconstr
Surg.2001;107:17101716.
18. Fosnot J, Fischer JP, Smartt JM Jr, et al. Does previous
chestwall irradiation increase vascular complications in free
au-
tologous breast reconstruction?Plast Reconstr
Surg.2011;127:496504.19. Albino FP, Koltz PF, Ling MN, Langstein
HN. Irradiated
autologous breast reconstructions: Effects of patient factorsand
treatment variables.Plast Reconstr Surg. 2010;126:1216.
20. Scheer AS, Novak CB, Neligan PC, Lipa JE.
Complicationsassociated with breast reconstruction using a
perforator flapcompared with a free TRAM flap. Ann Plast Surg.
2006;56:355358.
21. Nahabedian MY, Tsangaris T, Momen B. Breast reconstruc-tion
with the DIEP flap or the muscle-sparing (MS-2) freeTRAM flap: Is
there a difference? Plast Reconstr Surg. 2005;115:436444;
discussion 445446.
22. Elliott LF, Seify H, Bergey P. The 3-hour muscle-sparing
freeTRAM flap: Safe and effective treatment review of 111
con-secutive free TRAM flaps in a private practice setting.
PlastReconstr Surg.2007;120:2734.
23. Bristol SG, Lennox PA, Clugston PA. A comparison of
ipsi-lateral pedicled TRAM flap with and without previous
irra-diation. Ann Plast Surg. 2006;56:589592.
24. Bozikov K, Arnez T, Hertl K, Arnez ZM. Fat necrosis in
freeDIEAP flap: Incidence, risk and predictor factors. Ann
PlastSurg.2009;63:138142.
25. Bailey SH, Saint-Cyr M, Wong C, et al. The single
dominantmedial row perforator DIEP flap in breast
reconstruction:Three-dimensional perforasome and clinical results.
PlastReconstr Surg.2010;126:739751.
26. Banic A, Boeckx W, Greulich M, et al. Late results in
breastreconstruction with free TRAM flaps: A prospective multi-
centric study.Plast Reconstr Surg.1995;95:11951204; discus-sion
12051206.
27. Kim EK, Lee TJ, Eom JS. Comparison of fat necrosis
betweenzone II and zone III in pedicled transverse rectus
abdominismusculocutaneous flaps: A prospective study of 400
consec-utive cases. Ann Plast Surg.2007;59:256259.
28. Tran NV, Buchel EW, Convery PA. Microvascular complica-tions
of DIEP flaps.Plast Reconstr Surg.2007;119:13971405;discussion
14061408.
29. Gill PS, Hunt JP, Guerra AB, et al. A 10-year
retrospectivereview of 758 DIEP flaps for breast reconstruction.
PlastReconstr Surg.2004;113:11531160.
30. Chen CM, Halvorson EG, Disa JJ, et al. Immediate
postop-erative complications in DIEP versus free/muscle-sparing
TRAM flaps. Plast Reconstr Surg. 2007;120:14771482.
31. El-Mrakby HH, Milner RH, McLean NR. Supercharged pedi-cled
TRAM flap in breast reconstruction: Is it a worthwhileprocedure?
Ann Plast Surg. 2002;49:252257.
32. Yamamoto Y, Nohiro K, Sugihara T, Shintomi Y, Ohura
T.Superiority of the microvascularly augmented flap: Analysisof 50
transverse rectus abdominis myocutaneous flaps forbreast
reconstruction.Plast Reconstr Surg.1996;97:7983; dis-
cussion 8485.33. Lee JW, Lee YC, Chang TW. Microvascularly
augmented
transverse rectus abdominis myocutaneous flap for
breastreconstruction: Reappraisal of its value through clinical
out-come assessment and intraoperative blood gas
analysis.Mi-crosurgery2008;28:656662.
34. Takeishi M, Fujimoto M, Ishida K, Makino Y. Muscle
spar-ing-2 transverse rectus abdominis musculocutaneous flap
forbreast reconstruction: A comparison with deep inferior
epi-gastric perforator flap. Microsurgery2008;28:650655.
35. Busic V, Das-Gupta R, Mesic H, Begic A. The deep
inferiorepigastric perforator flap for breast reconstruction,
thelearning curve explored. J Plast Reconstr Aesthet Surg.
2006;59:580584.
36. Keller A. The deep inferior epigastric perforator free flap
forbreast reconstruction. Ann Plast Surg.2001;46:474479;
dis-cussion 479480.
37. Andrades P, Fix RJ, Danilla S, et al. Ischemic
complicationsin pedicled, free and muscle-sparing transverse rectus
ab-dominis myocutaneous flaps for breast reconstruction. AnnPlast
Surg. 2008;60:562567.
38. Dorafshar AH, Januszyk M, Song DH. Anatomical and tech-nical
tips for use of the superficial inferior epigastric artery(SIEA)
flap in breast reconstructive surgery. J Reconstr Mi-crosurg.
2010;26:381389.
39. Yap YL, Lim J, Yap-Asedillo C, et al. The deep inferior
epi-gastric perforator flap for breast reconstruction: Is this
theideal flap for Asian women? Ann Acad Med
Singapore2010;39:680686.
40. Elliott LF, Eskenazi L, Beegle PH Jr, Podres PE, Drazan
L.Immediate TRAM flap breast reconstruction: 128 consecu-tive
cases. Plast Reconstr Surg.1993;92:217227.
41. Figus A, Mosahebi A, Ramakrishnan V. Microcirculation inDIEP
flaps: A study of the haemodynamics using laser Dopp-ler flowmetry
and lightguide reflectance spectrophotometry.
J Plast Reconstr Aesthet Surg.2006;59:604612; discussion 613.42.
Ulusal BG, Cheng MH, Wei FC, Ho-Asjoe M, Song D. Breast
reconstruction using the entire transverse abdominal
adi-pocutaneous flap based on unilateral superficial or
deepinferior epigastric vessels.Plast Reconstr
Surg.2006;117:13951403; discussion 14041406.
43. Blondeel PN. One hundred free DIEP flap breast
recon-structions: A personal experience. Br J Plast Surg.
1999;52:104111.
44. Padubidri AN, Yetman R, Brown E, et al. Complications
ofpostmastectomy breast reconstructions in smokers, ex-smok-ers,
and nonsmokers. Plast Reconstr Surg. 2001;107:342349;discussion
350351.
45. Watterson PA, Botswick J III, Hester TR Jr, Bried JT,
TaylorGI. TRAM flap anatomy correlated with a 10-year
experiencewith 556 patients. Plast Reconstr Surg.
1995;95:11851194.
46. Wang HT, Hartzell T, Olbrich KC, Erdmann D, GeorgiadeGS.
Delay of transverse rectus abdominis myocutaneous
flapreconstruction improves flap reliability in the obese
patient.Plast Reconstr Surg. 2005;116:613618; discussion
619620.
47. Chang DW, Wang BG, RobbGL, etal. Effectof obesity onflapand
donor-site complications in free transverse rectus ab-dominis
myocutaneous flap breast reconstruction. Plast Re-
constr Surg.2000;105:16401648.
Volume 131, Number 3 Fat Necrosis in Breast Reconstruction
451
-
8/13/2019 Fat Necrosis in Autologous Abdomen Based Breast.3
10/10
48. Lee BT, Chen C, Nguyen MD, Lin SJ, Tobias AM. A
newclassification system for muscle and nerve preservation inDIEP
flap breast reconstruction. Microsurgery2010;30:8590.
49. Selber JC, Samra F, Bristol M, et al. A head-to-head
compar-ison between the free TRAM and the SIEA flaps: Is the rateof
flap loss worth the gain in abdominal wall function?PlastReconstr
Surg.2008;122:348355.
50. Garvey PB, Buchel EW, Pockaj BA, Gray RJ, Samson TD. Thedeep
inferior epigastricperforator flapfor breast reconstruc-tion in
overweight and obese patients. Plast Reconstr
Surg.2005;115:447457.
51. Guerra AB, Metzinger SE, Bidros RS, et al. Bilateral
breastreconstruction with the deep inferior epigastric
perforator(DIEP) flap: An experience with 280 flaps. Ann Plast
Surg.2004;52:246252.
52. Williams JK, Carlson GW, Bostwick J III, Bried JT, Mackay
G.The effects of radiation treatment after TRAM flap
breastreconstruction. Plast Reconstr Surg. 1997;100:11531160.
53. Rogers NE, Allen RJ. Radiation effects on breast
reconstruc-tion with the deep inferior epigastric perforator flap.
PlastReconstr Surg. 2002;109:19191924; discussion 19251926.
54. Baumann DP, Crosby MA, Selber JC, et al. Optimal timing
ofdelayed free lower abdominal flap breast reconstruction af-ter
postmastectomy radiation therapy. Plast Reconstr
Surg.2011;127:11001106.
55. Tran NV, Chang DW, Gupta A, Kroll SS, Robb GL. Com-parison
of immediate and delayed free TRAM flap breastreconstruction in
patients receiving postmastectomy radia-tion therapy. Plast
Reconstr Surg. 2001;108:7882.
56. Temple CL, Strom EA, Youssef A, Langstein HN. Choice
ofrecipient vessels in delayed TRAM flap breast reconstructionafter
radiotherapy. Plast Reconstr Surg.2005;115:105113.
57. Chang DW, Reece GP, Wang B, et al. Effect of smoking
oncomplications in patients undergoing free TRAM flap
breastreconstruction. Plast Reconstr Surg. 2000;105:23742380.
58. Parrett BM, Caterson SA, Tobias AM, Lee BT. DIEP flaps
in
women with abdominal scars: Are complication rates af-fected?
Plast Reconstr Surg. 2008;121:15271531.
59. Kropf N, Macadam SA, McCarthy C, et al. Influence of
therecipient vessel on fat necrosis after breast reconstructionwith
the free transverse rectus abdominis myocutaneous flap.Scand J
Plast Reconstr Surg Hand Surg. 2010;44:96101.
60. Saint-Cyr M, Youssef A, Bae HW, Robb GL, Chang DW.Changing
trends in recipient vessel selection for microvas-cular autologous
breast reconstruction: An analysis of 1483consecutive cases. Plast
Reconstr Surg. 2007;119:19932000.
61. Follmar KE, Prucz RB, Manahan MA, Magarakis M, Rad AN,Rosson
GD. Internal mammary intercostal perforators in-stead of the true
internal mammary vessels as the recipientvessels for breast
reconstruction. Plast Reconstr Surg. 2011;127:3440.
62. Codner MA, Bostwick J III, Nahai F, Bried JT, Eaves FF.TRAM
flapvascular delay for high-risk breast reconstruction.Plast
Reconstr Surg.1995;96:16151622.
63. Erdmann D, Sundin BM, Moquin KJ, Young H, GeorgiadeGS. Delay
in unipedicled TRAM flap reconstruction of the
breast: A review of 76 consecutive cases. Plast Reconstr
Surg.2002;110:762767.
64. Baldwin BJ, Schusterman MA, Miller MJ, Kroll SS, Wang
BG.Bilateral breast reconstruction: Conventional versus freeTRAM.
Plast Reconstr Surg. 1994;93:14101416; discussion1417.
65. Chun YS, Sinha I, Turko A, et al. Comparison of
morbidity,
functional outcome, and satisfaction following bilateralTRAM
versus bilateral DIEP flap breast reconstruction.PlastReconstr
Surg.2010;126:11331141.
66. Hamdi M, Blondeel P, Van Landuyt K, Tondu T, MonstreyS.
Bilateral autogenous breast reconstruction using perfora-tor free
flaps: A single centers experience.
PlastReconstrSurg.2004;114:8389; discussion 9092.
67. Paige KT, Bostwick J III, Jones G, Bried JT, Jones G. A
com-parison of morbidity from bilateral, unipedicled and
unilat-eral, unipedicled TRAM flap breast reconstructions.
PlastReconstr Surg.1998;101:18191827.
68. Kroll SS, Gherardini G, Martin JE, et al. Fat necrosis in
freeand pedicled TRAMflaps. Plast Reconstr Surg.
1998;102:15021507.
69. Massey MF, Spiegel AJ, Levine JL, et al. Perforator
flaps:Recent experience, current trends and future directionsbased
on 3974 microsurgical breast reconstructions. PlastReconstr
Surg.2009;124:737751.
70. Williams JK, Bostwick J III, Bried JT, Mackay G, Landry
J,Benton J. TRAM flap breast reconstruction after
radiationtreatment.Ann Surg.1995;221:756766; discussion 764766.
71. Nahabedian MY, Momen B, Galdino G, Manson PN.
Breastreconstruction with the free TRAM or DIEP flap:
Patientselection, choice of flap, and outcome. Plast Reconstr
Surg.2002;110:466475; discussion 476477.
72. Ohjimi H, Era K, Fujita T, Tanaka T, Yabuuchi R.
Analyzingthe vascular architecture of the free TRAM flap using
intra-operative ex vivo angiography. Plast Reconstr Surg.
2005;116:
106113.73. Kroll SS. Fat necrosis in free transverse rectus
abdominis
myocutaneous and deep inferior epigastric perforator flaps.Plast
Reconstr Surg.2000;106:576583.
74. Tran NV, Evans GR, Kroll SS, et al. Postoperative
adjuvantirradiation: Effects on transverse rectus abdominis
muscleflap breast reconstruction.Plast Reconstr
Surg.2000;106:313317; discussion 318320.
75. Selber JC, Kurichi JE, Vega SJ, Sonnad SS, Serletti JM.
Riskfactors and complications in free TRAM flap breast
recon-struction. Ann Plast Surg. 2006;56:492497.
76. Mahajan AL, Zeltzer A, Claes KE, Van Landuyt K, Hamdi M.Are
Pfannenstiel scars a boon or a curse of DIEP flap
breastreconstructions? Plast Reconstr Surg. 2012;129:797805.
77. Hamdi M, Khuthaila DK, Van Landuyt K, Roche N, MonstreyS.
Double-pedicle abdominal perforator free flaps for uni-lateral
breast reconstruction: New horizons in microsurgicaltissue transfer
to the breast.J Plast Reconstr Aesthet Surg.2007;60:904912.
Plastic and Reconstructive Surgery March 2013
452