Embed Size (px)
Citation preview
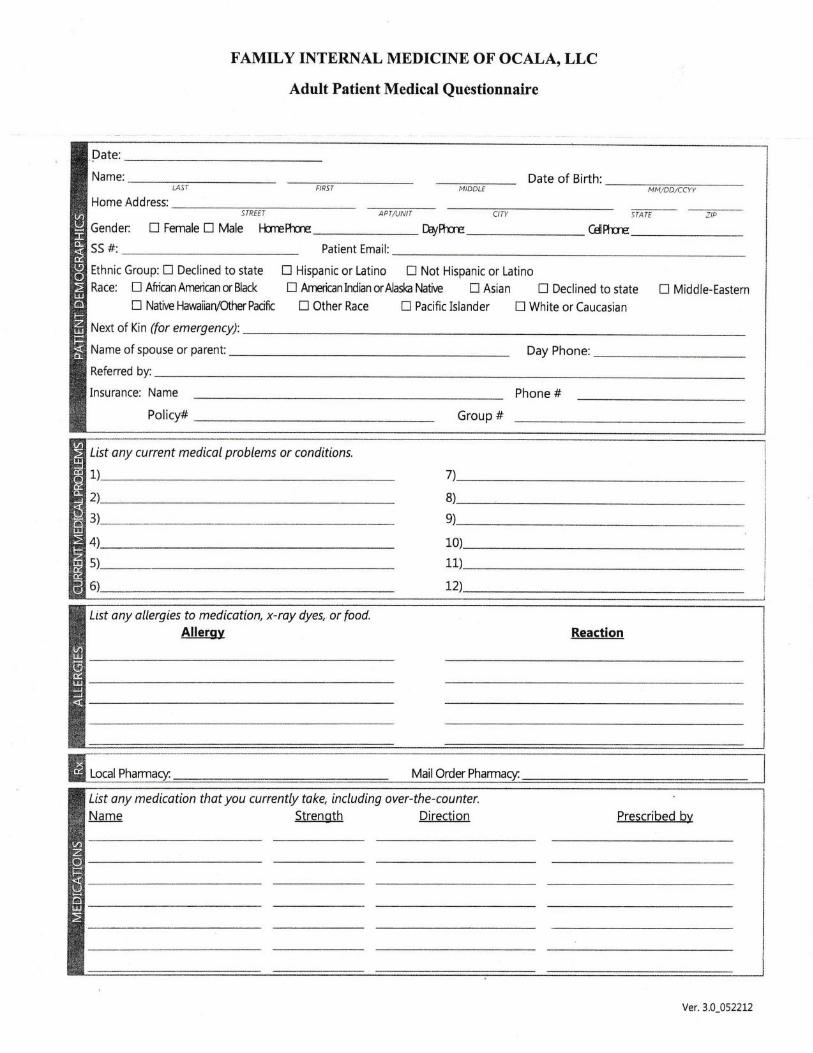
FAMILY INTERNAL MEDICINE OF OCALA, LLC
Adult Patient Medical Questionnaire
List any current medicol problems or conditions.
1)
2\
11)
t2)
List ony allergies to medication, x-ray dyes, or food.Allergv Reaction
7)
8)
e)
10)
Date:
Name: Date of Birth:LASi MM,IDD/CCYY
silff -.zF
Home Address:STREEI
Gender: fl Fennle tr Male llrrefttrE Dayfre CdPttrE
SS #: Patient Email:
Ethnic Group: E Declined to state E Hispanic or Latino tr Not Hispanic or Latino
Race: tl Afiilan Amrican or Black tr Arneican Indian orAlaslo Mtive tr Asian tr Declined to state tr Middle-Eastern
tr Native Hawaiiary'OtherPacift ! Other Race ! Pacific Islander tr White or Caucasian
Next of Kin (for emergency):
Name of spouse or parent: Day Phone:
Referred by:
Insurance: Name Phone #
Policy# Group #
Local MailOrder Pharmacu
List any medicotion thot you currently toke, including over-the-counter.Name Strenoth Direction Prescribed bv
Ver.3.0_0522L2
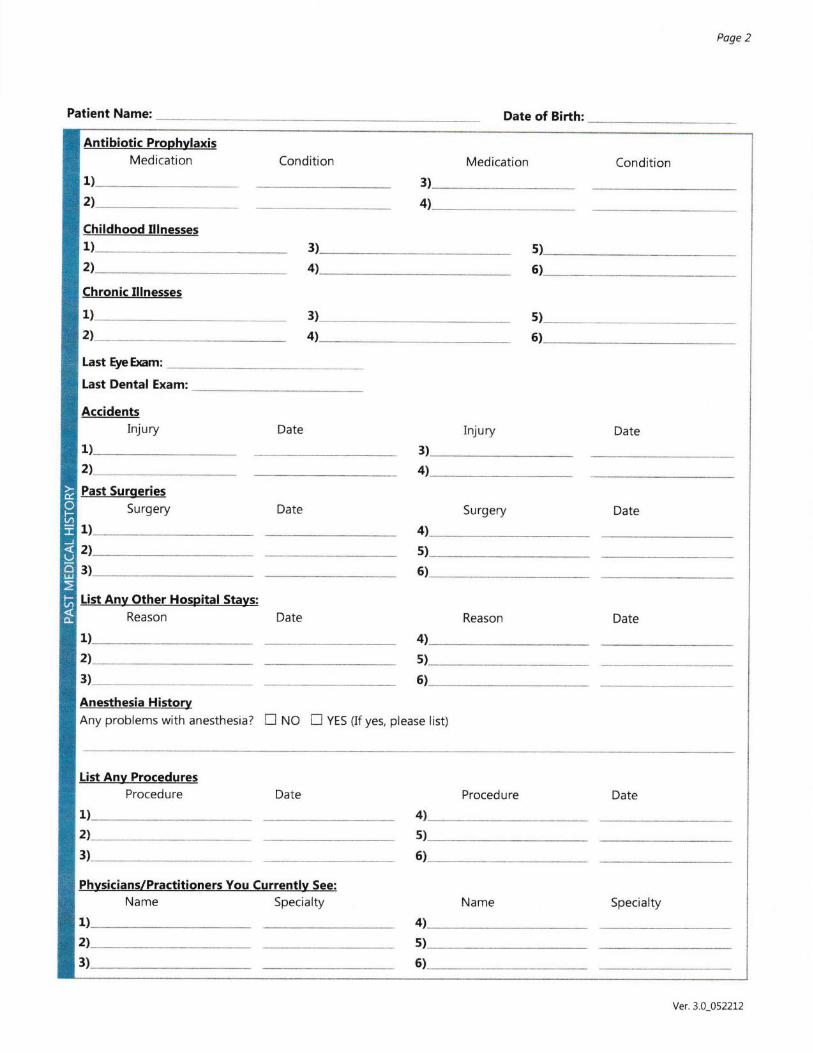
Patient Name:
Poge 2
Date of Birth:
Antibiotic ProphylaxisMedication Condition Medication Condition
1)
2l3)
4)
Childhood Illnesses1) 5)
4l 6)
Chronic Illnesses
1)_ __ 3)
4)
s)2)_Last EyeEnm:
5)
Last Dental Exam:
AccidentsInjury Date Injury Date
1)
2l
Past SurgeriesSurgery Date Surgery Date
1) 4)
2)_3)__
List Anv Other Hospital Stays:Reason
s)
5)
Reason Date
1)
2)
3)
4l
s)
5)
Anesthesia HistoryAny problems with anesthesia? tr ruO n VES (lf yes, please list)
List Any ProceduresProcedure Date Procedure Date
1)
2)
3)
4l
6)
Physicians/Practitioners You Currently See:Name Specialty
1)
2)
3)
Name Specialty
Yer.3.0_052212

Patient Name:
Poge 3
Date of Birth:
Please list ony heolth problems and couses of death if opplicobte.Family Member Age History
Father
MotherBrother(s)
Sister(s)
Mother's fatherMother's motherFather/s fatherFather's mother
Do you drink alcohol?......................fl No E Yes
lf yes, how much?
Are you sexually active?..................n No n yes
lf yes, whot form of controception
Do you consume caffeine?............f] trto n yes
lf yes, how much per doy?
Diet flBalanced fJVegetarian EDiabetic nLow Salt
ELow Fat nlow Carb EOther:---Have you ever been in anabusive relationship?.......................8 ruo n Yes
Are you afraid of your partnerZ...n ruo D yes
Education: nHign School ncollege nsome College
ETrade School EOther:Do you do some form ofregular exercise every day?...........E ruo n Yes
lf yes, how much?
Marital Status: IMarried Esingle EDivorcedEwidowed nother:
Occupation:
Place of Birth (City, State);
Haveyou lilred abroad morctran one monh?..... Eruo nYes
lf yes, where?
List everyone in your household, including pets:
Do you wear seatbelts?................... Eruo.nYes
Do you participate in any activities thatput you at risk of getting AIDS?...................... nUo EYes
Do you smoke or chew tobacco:....... f]trto f]Yes
lf yes, how much:
Spouse's occupation:
Do you use recreational drugs:..... Ewo nYes
lf yes, whot do you use? _
Pleose record the last year you hod the following. lf you do not know, leove blank.
Flu vaccine (shot)........................
Pneumonia vaccine (shot) .....
Tu berculosis Test...........................Positive PPD.................Tetanus Diphthaia vaccine (shot)....
Ver.3.0 0522L2
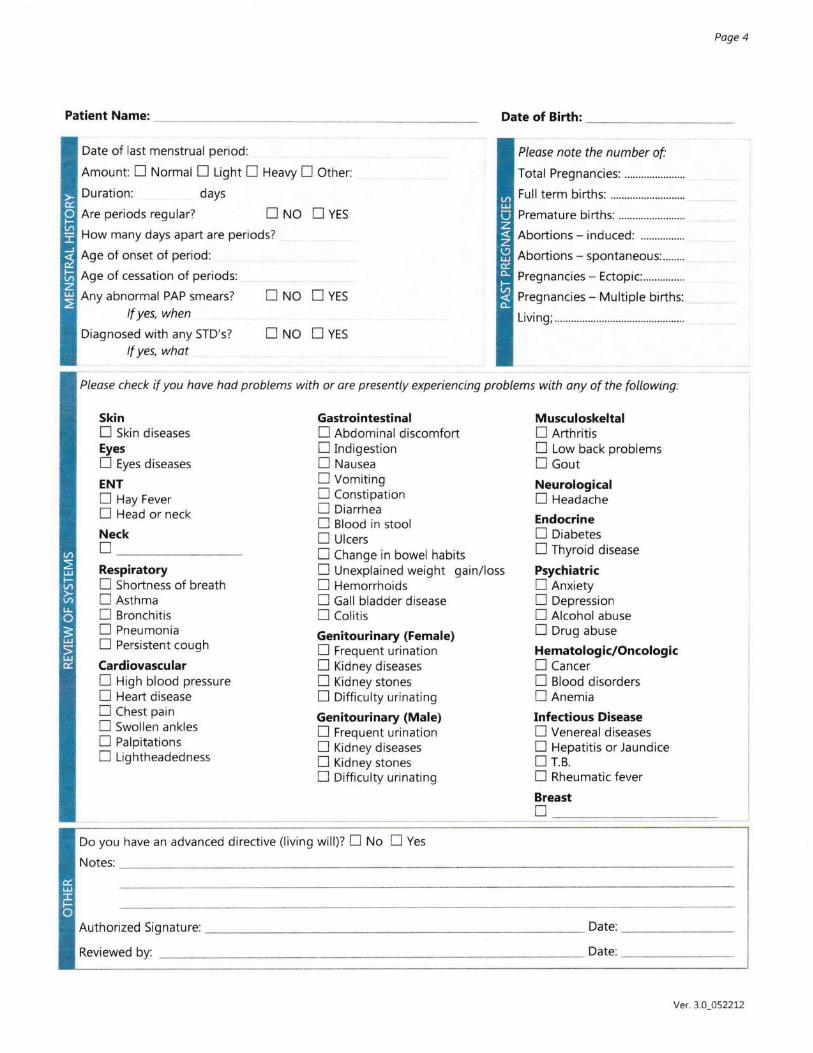
Poge 4
Patient Name:
Date of last menstrual period:
Amount: E Normal tr t-igfrt E Heavy n Other:
Duration: days
Are periods regular? n ruO I YfS
How many days apart are periods?
Age of onset of period:
Age of cessation of periods:
Any abnormal PAP smears? n NO n YES
lf yes, when
Diagnosed with any STD's? n ruO E VfSlf yes, what
Skinn stin diseasesEyesE Eyes diseases
ENTn Hay Fevern Head or neck
NecknRespiratoryn Shortness of breathE AsthmaE Bronchitisn PneumoniaE Persistent cough
Cardiovasculartr Higir blood pressureE Heart diseasen Chest painn Swollen anklesn Palpitationsn tightheadedness
GastrointestinalE AbdominaldiscomfortE IndigestionE Nausean VomitingE ConstipationE Diarrhean alood in stoolE Ulcersn Change in bowel habitsE Unexplained weight gain/lossfl Hemorrhoidsn Catt bladder diseasen cotitis
Genitourinary (Female)E Frequent urinationE ridney diseasesn ridney stonesE Difficulty urinating
Genitourinary (Male)n Frequent urinationn fidney diseasesn ridney stonesE Difficulty urinating
Date of Birth:
Please note the number of:
Total Pregnancies: ......................
Full term births:
Premature births:
Abortions - induced:
Abortions - spontaneous:........
Pregnancies - Ectopic...............
Pregnancies - Multiple births:
Living; ............
Musculoskeltaln RrthritisE Low back problemsE Gout
NeurologicalI Headache
Endocrine! DiabetesE Thyroid disease
Psychiatricn Anxietyfl DepressionE Alcohol abuseE Drug abuse
Hematologic/Oncologicn CancerI glood disordersE Anemia
Infectious DiseaseE Venereal diseasesn Hepatitis or Jaundicen r.e.f] Rheumatic fever
Breasttr
Please check if you have hod probtems with o, or" pr"r,"ntly experiencing problems with ony of the fottowing:
Do you have an advanced directive (living will)? n ruo I Yes
Notes:
Authorized Signature: Date:
Date:Reviewed by:
Ver. 3.0-052212

FAMILY INTERNAL MEDICINE OF OCALA, LLC
Patient Consent for Use and Disclosure of Protected Health Information
With my consent, Family Intemal Medicine of Ocala, LLC may use and disclose protected healthinformation (PHI) about me to carry out treatment, payment and healthcare operations (TPS).Please refer to Family lnternal Medicine of Ocala, LLC's Notice of Privacy Practices for a morecomplete description of such uses and disclosures.
I have the right to review the Notice of Privacy Practices prior to signing this consent.
Family Intemal Medicine of Ocala, LLC reserves the right to revise its Notice of PrivacyPractices at any time. A revised Notice of Privacy Practices may be obtained by forwarding a
written request to Family Internal Medicine of Ocala, LLC Privacy Officer at 1623 SW 1'tAvenue, Ocala, FL 3447 l.
With my consent Family Internal Medicine of Ocala, LLC may call my home or other designatedlocation and leave a message on voice mail or in person in reference to any items that assist thepractice in carrying out TPO, such as appointment reminders, insurance items and any callpertaining to my clinical care, including laboratory results among others.
With my consent, Family Intemal Medicine of Ocala, LLC may mail to my home or otherdesignated location any items that assist the practice in carrying out TPS, such as appointmentreminder cards and employee statements as long as they are marked Personal and Confidential.
By signing this form, I am consenting to Family Intemal Medicine of Ocala, LLC's use anddisclosure of my PHI to carry out TPO.
I may revoke my consent in writing except to the extent that the practice has already madedisclosures in reliance upon my prior consent. If I do not sign this consent Family InternalMedicine of Ocala, LLC may decline to provide treatment to me.
Signature of Patient or Legal Guardian
Printed Name of Patient or Legal Guardian
Date

FAMILY INTERNAL MEDICINE OF OCALA, LLC
AUTHORIZED REPRESENTATTVE FORM
Note: This form is used to confirm a Patient's permission that Family Internal Medicine ofOcala, LLC may discuss or disclose their protected health information to a particular person whoacts as their Authorized Representative. Use of their information is strictly limited to thatpu{pose described above.
SECTION A: Patient Information
By signing this form in Section E below, I understand that Family Internal Medicine of Ocala,LLC may release my personal health information as defined in Section B below to myAuthorized Representative(s) named in Section C below.
Patient Name:
Address:
Telephone Number:
Social Security Number:
Please note: This authorization does not provide you're "Authorized Representative" with anyauthority, either implied or direct, over any treatment or direct care decisions. IF you wish todesignate a health care partnerlproxy or a clinical personal health care rq)resentative or if youwant to set up a living will, please discuss this with your primary care physician or your attomey.Also, we promise that we will not condition treatment on the execution of this form.
SECTION B: Tlpe of lnformation
Personal Health Information, including but not limited to, billing information, diagnosis,procedures, dernographic information (but not including any psychotherapy notes).
SECTION C: Authorized Use/or Disclosure
Intended use or disclosure: I understand that your general policy is not to disclose my personalhealth information to other parties, except those directly involved in my care, without my writtenauthorization or as permitted or required by law. For this reason, I authorize you to discuss anddisclose my personal health information to the person(s) named below for the purpose ofassisting with, or facilitating, the coordination or payment of my health care. I also understandthat if my Authorized Representative is not a health care provider or another entity subject tofederal or applicable state and privacy laws and my personal health representative may furtherdisclose my personal health information without my authorization.I acknowledge that myauthorization is voluntary.
Authorized Representative # 1
Name: Phone Number:
Address:
Relationship to you:
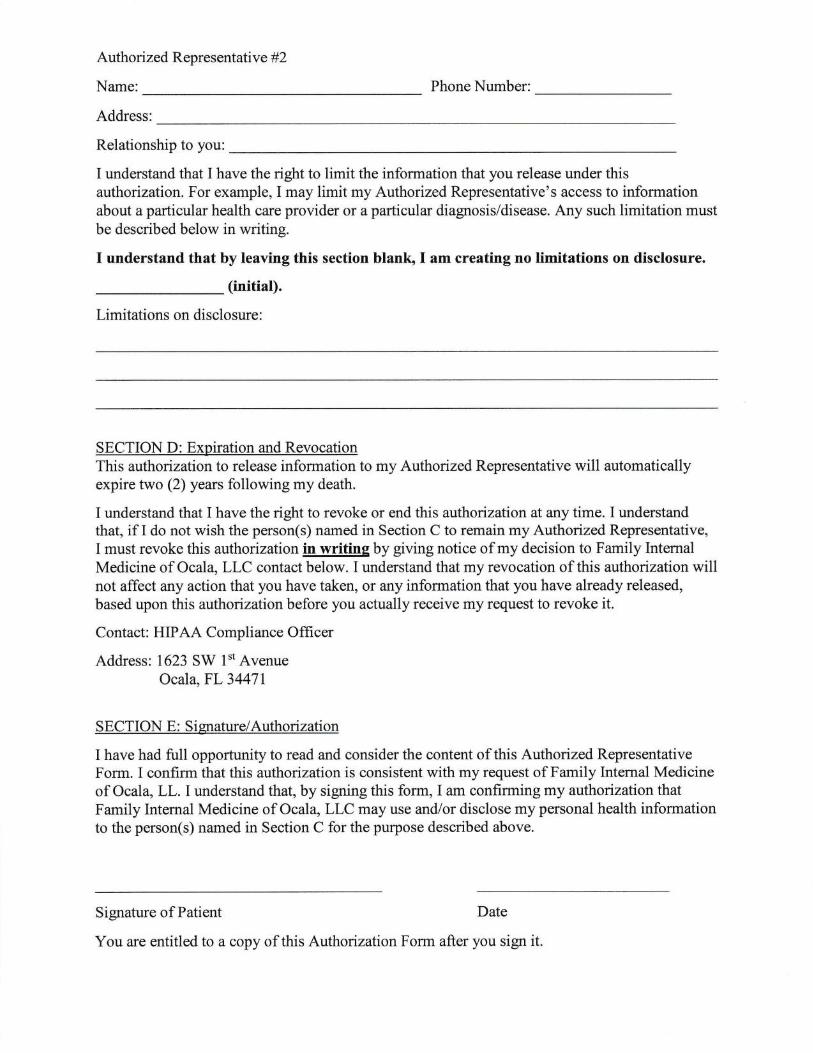
Authorized Representati v e #2
Name: Phone Number:
Address:
Relationship to you:
I understand that I have the right to limit the information that you release under thisauthorization. For example, I may limit my Authorized Representative's access to informationabout a particular health care provider or a particular diagnosis/disease. Any such limitation mustbe described below in writing.
I understand that by leaving this section blankr l am creating no limitations on disclosure.
(initial).
Limitations on disclosure:
SECTION D: Expiration and RevocationThis authorizationto release information to my Authorized Representative will automaticallyexpire two (2) years following my death.
I understand that I have the right to revoke or end this authorization at any time. I understandthat, if I do not wish the person(s) named in Section C to remain my Authorized Representative,I must revoke this authorizationin writine by giving notice of my decision to Family InternalMedicine of Ocala, LLC contact below. I understand that my revocation of this atthoization willnot affect any action that you have taken, or any information that you have already released,based upon this authorization before you actually receive my request to revoke it.
Contact: HIPAA Compliance Officer
Address: 1623 SW l't AvenueOcala, FL3447l
SECTION E : Si grrature/Authorization
I have had full opportunity to read and consider the content of this Authorized RepresentativeForm. I confirm that this authorization is consistent with my request of Family Internal Medicineof Ocala, LL. I understand that, by signing this form, I am confirming my authorization thatFamily Internal Medicine of Ocala, LLCmay use and/or disclose mypersonal health informationto the person(s) named in Section C for the purpose described above.
Signature of Patient Date
You are entitled to a copy of this Authorization Form after you sign it.
FAMILY INTERNAL MEDICINE OF OCALA, LLC
Patient Rights and Responsibilities
In recognition of our responsibility in rendering patient care, these rights and responsibilities are affrmed in the policiesand procedures of Family Intemal Medicine of Ocala, LLC and Internal Medicine Associates of Ocala, LLC.
The patient has the right to:
o Be treated with courtesy and respect, with appreciation of his or her individual dignity and with protection of hisor her privacy.
o Prompt and reasonable response to questions and requests.
o Know who is providing medical services and who is responsible for his or her care.o Know what patient support services are available, including whether an interpreter is available if he or she does
not speak English.o Know what rules and regulations apply to his or her conduct.o Be given infonrration conceming the diagnosis, the planned course of treatment, alternatives, risks, and prognosis
by the health care provider.o To refuse treatment, except as otherwise provide by law.e Be given, upon request, fuII information and necessary counseling on the availability of financial resources for his
or her care.
o Know, upon request and in advance of treatment, whether the healthcare provider or healthcare facility accepts theMedicare assignment rate.
o Receive, upon request and prior to treatment, a reasonable estimate of charges for medical care.o Receive a copy of a reasonably clear and understandable itemized bill and upon request to have charges
explained.o Receive impartial access to medical treatment or accommodations, regardless of race, national origin, religion,
physical handicap, or source ofpayment.o Receive treatment for any emergency medical condition that will deteriorate from failure to provide treatment.o Know if medical treatment is for purposes of experimental/research and to give his or her consent or refusal to
participate in such experimental research.. Express grievances regarding any violation of their rights, as stated in Florida law, through the grievance
procedure of the healthcare provider or healthcare facility that serviced them and to the appropriate state licensingagency.
o Participate in all aspects of their health care decisions, unless contraindicated by concerns for their health.. Appropriate assessment and management of pain.o For providing to the healthcare provider, to the best of his or her knowledge, accurate and complete information
about present complaints, past illnesses, hospitalizations, medication, and other matter relating to his or herhealth.
o For reporting unexpected changes in his or her condition to the healthcare provider.o For reporting to the healthcare provider whether he or she comprehends a contemplated course of action and what
is expected ofhim or her.o For following the treatment plan recommended by the healthcare provider.o For keeping appointments and for notiffing the Facility when he or she is unable to do so for any reason.
o For his or her actions if he or she refuses treatment or does not follow the healthcare provider's instruction.o For assuring that the financial obligation of his or her healthcare are fulfilled as promptly as possible.
o For following facility rules and regulation affecting patient care and conduct.o For consideration and respect ofthe facility staffand property.
o Telling the Center personnel about living will, medical power of attorney, or other documents that could affecttheir care.
'!a _Patient or Guardian Signature
Patient or Guardian Printed Name
Date
Filing complaints: If you have a complaint against a medical office:
Family Internal Medicine of Ocala, LLC
Internal Medicine of Ocala, LLC
Attn: Maria Vasquez, Manager
1623 SW I't Ave.
Ocala, FL 34471
(3s2)732-e844
OR
Write to the address listed below:
Agency for Health Care Administration
Consumer Assistance Unit
2727 Mahan Drive, Bldg. I
Tallahassee, FL 32306
If you have a complaint against a healthcare professional and want to receive a complaint form,call the Consumer Assistance Unit at 1-888-419-3456 (press 2)
OR
Write to the address listed below:
Agency for Health Care Administration
Consumer Assistance Unit
P.O. Box 14000
Tallahassee, FL 323 17-4000
Website for Medicare beneficiary Ombudsman www.cms.hhs.qov/center/ombudsman.asp
FAMILY INTERNAL MEDICINE OF OCALA, LLC
Dear Patient:
Florida statutes require that we provide our patients with information concerning their rights to aLiving Will and/or Advance Directive.
An ADVANCE DIRECTIVE is witnessed statement made by a competent admit regardinghis/trer wishes or desires in regards to future health care, (for example - Provide artificial lifesupport).
A LIVING WILL is a formalized version of an ADVANCE DIRECTIVE.
Please take this information home and carefully review it. If you wish to execute an AdvanceDirective or Living Will, please notifu this office on your next visit.
I have received a copy of Health Care Directives and understand my rights relating to AdvanceDirectives and Living Wills.
PLEASE CHECK ONE:
I do not have a Living WiIl I do have a living will and
will provide a copy to this office.
Florida Law requires that your healthcare provider or healthcare facility recognize your rightswhile you are receiving medical care and that you respect the healthcare providers or healthcarefacility's right to expect certain behavior on the part of patients. You may request a copy of thefull text of this law from your healthcare provider or healthcare facility.
I have received my copy of Patient's BilI of Rights and Responsibilities
Signature of Patient or Legal Guardian Date
Printed Name of Patient or Legal Guardian
Witness
FAMILY INTERNAL MEDICINE OF OCALA, LLC
Financial Policy
As your physician, we are committed to providing you with the best possible medical care. In order to achieve thisgoal, we need your assistance and your understanding of our payment policy.
PAYMENT FOR SERVICE IS DUE AT TIIE TIME SERVICES ARE RENDERED.
We accept cash, personal check, MasterCard, Visa, Discover and Debit cards. Returned checls less than $50.00 aresubject to a service charge (per Florida Statute 832.80) of $25.00. Checks between $50.00 and $300.00 have a fee of$30.00. For checks greater than $300.00, the fee is $40.00. You will also lose your privilege to write checks in ouroffice.
CANCELED APPOINTMENTS - Patients who do not cancel appointments may be discharged from the practiceafter three (3) no-shows. Additionally, a no-show fee of $15.00 permissed appointment will be charged.
ALL PRTVATE INSTJRANCES - CO-PAYMENT AND DEDUCTIBLE MUST BE PAID AT THE TIME OFSERVICE. Because we are under contract with these insurance companies we will file your insurance.
MEDICARE - Your deductible is due at the time of service. If you have already paid your deductible (please bringyour EOB showing you have met your deductible), and if Medicare is your only coverage, we will charge yotZlo/oof the Medicare allowable charges. Since we are a Medicare provider, we will frle your Medicare claim. If you havea secondary insurance company that we are providers for, we will file your claim with the secondary and bill youonly for tle remaining balance of allowable charges. If you have a secondary insurance, please check with our frontdesk to see if we file with that company. If we do not know the allowable charge for a specific service, we will billyou after Medicare pays.
MEDICAID - There is a $2.00 co-pay for each visit, except for children and pregnant women.
FINAIICIAL AGREEMENT - We will gladly discuss yoru proposed treatnent and do our best to answer anyquestions relating to your insurance. You must realize, however that:
l. Your insurance is a conffact between you, your employer, and the insurance company. We are not part tothat contract.
2. Not all services are a covered benefit in all contracts. Some insurance companies arbitrarily select certainservices they will not cover (e.g., yearly physicals).
We must emphasize that as your medical care providers, our relationship and concern is with you and your health,
not your insurance company. ALL CHARGES ARE YOUR RESPONSIBILITY FROM THE DATE SERVICESARE RENDERED. On any balance on your account over 90 days, including those that insurance has not paid,
collection action will be taken. We realize that emergencies do arise and may affect timely payment of your account.
If such extreme cases do occur, please contact us promptly for assistance in the management of your account.
Ifit becomes necessary to collect any sum due through an attorney, then the patient agrees to pay all reasonable
costs of collection, including attorney's fees, whether suit is filed or not.
Ifyou have any questions about the above information or any uncertainty regarding insurance coverage, please do
not hesitate to ask us. We are here to help you.
I have read and understand the Financial Policy.
'!a
Patient or Guardian Signature
Patient or Guardian Printed Name
Date
FAMILY INTERNAL MEDICINE OF OCALA, LLC
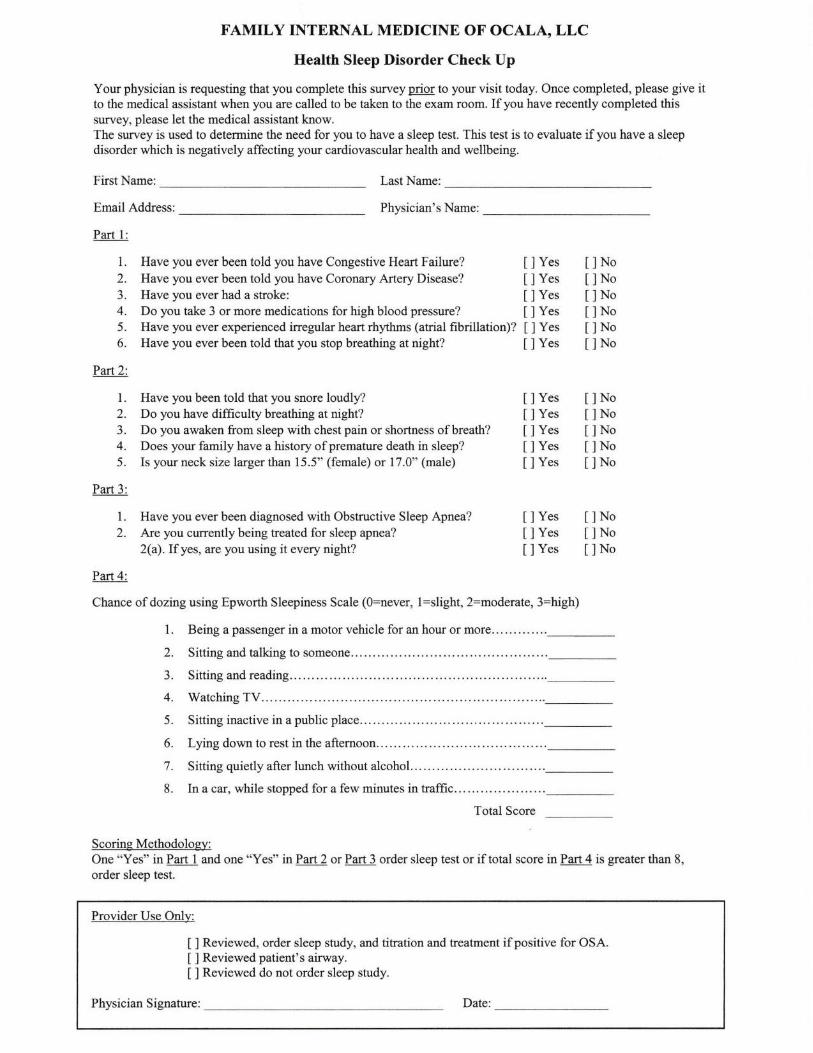
Health Sleep Disorder Check Up
Your physician is requesting that you complete this survey pMI to your visit today. Once completed, please give itto the medical assistant when you are called to be taken to the exam room. If you have recently completed thissuryey, please let the medical assistant know.The survey is used to determine the need for you to have a sleep test. This test is to evaluate if you have a sleepdisorder which is negatively affecting your cardiovascular health and wellbeing.
First Name: Last Name:
Email Address:
Part l:
Physician's Name:
1. Have you ever been told you have Congestive Heart Failure?2. Have you ever been told you have Coronary Artery Disease?
3. Have you ever had a stroke:4. Do you take 3 or more medications for high blood pressure?
5. Have you ever experienced irregular heart rhythms (atrial fibrillation)?6. Have you ever been told that you stop breathing at night?
Part2:
l. Have you been told that you snore loudly?2. Do you have difhculty breathing at night?3. Do you awaken from sleep with chest pain or shortness of breath?4. Does your family have a history of premature death in sleep?
5. Is your neck size larger than 15.5" (female) or 17.0" (male)
Part 3:
l. Have you ever been diagnosed with Obstructive Sleep Apnea?
2. Are you currently being treated for sleep apnea?
2(a). Ifyes, are you using it every night?
YesYesYesYesYesYes
YesYesYesYesYes
YesYesYes
NoNoNoNoNoNo
NoNoNoNoNo
NoNoNo
Part 4:
Chance of dozing using Epworth Sleepiness Scale (O:never, l:slight, 2:moderate, 3:high)
Being a passenger in a motor vehicle for an hour or more...
Sitting and talking to someone..
Sitting and reading..
Watching TV.........
Sitting inactive in a public place...
Lying down to rest in the afternoon
Sitting quietly after lunch without alcohol...
In a car, while stopped for a few minutes in traffic...
Total Score
Scorine Methodoloey:One "Yes" in Part 1 and one "Yes" in Part 2 or Part 3 order sleep test or if total score in Part 4 is greater than 8,
order sleep test.
Provider Use Only:
Reviewed, order sleep study, and titration and treatment if positive for OSA.Reviewed patient's airway.Reviewed do not order sleep study.
Physician Signature: Date:
![Ocala Banner. (Ocala, Florida) 1904-11-25 [p PAGE [FIVE]].€¦ · Genuine isdiscoveredand Clam Anti-milregs Monopoly Oo-QThakttii OCALA WAJLB-DTDIAIT Unperceived-a ... Ocala Rifies](https://img.dokumen.tips/doc/110x75/60046190c776f3441a6e7c13/ocala-banner-ocala-florida-1904-11-25-p-page-five-genuine-isdiscoveredand.jpg)
![Ocala Evening Star. (Ocala, Florida) 1901-06-07 [p ].ufdcimages.uflib.ufl.edu/UF/00/07/59/08/02809/00556.pdfchildren com-plete strange nutritive Things courte-ous patient peanuts charge](https://img.dokumen.tips/doc/110x75/5ac80da47f8b9a7d548bf00b/ocala-evening-star-ocala-florida-1901-06-07-p-com-plete-strange-nutritive.jpg)
![Ocala Evening Star. (Ocala, Florida) 1901-05-25 [p ].ufdcimages.uflib.ufl.edu/UF/00/07/59/08/02798/00510.pdf · eulogy formant special appear-to Ocala as Cholera realized Ocala engine](https://img.dokumen.tips/doc/110x75/5aeb45ea7f8b9a45568cdead/ocala-evening-star-ocala-florida-1901-05-25-p-formant-special-appear-to.jpg)


![Ocala Banner. (Ocala, Florida) 1908-12-18 [p ]](https://img.dokumen.tips/doc/110x75/616a2f9d11a7b741a34fbf4d/ocala-banner-ocala-florida-1908-12-18-p-.jpg)
![Ocala Banner. (Ocala, Florida) 1908-03-27 [p ]](https://img.dokumen.tips/doc/110x75/6242baa8e4eb9e1fa9076b21/ocala-banner-ocala-florida-1908-03-27-p-.jpg)


![Ocala Banner. (Ocala, Florida) 1909-10-22 [p ]](https://img.dokumen.tips/doc/110x75/61722251e6814f23d91f5433/ocala-banner-ocala-florida-1909-10-22-p-.jpg)

![Ocala Evening Star. (Ocala, Florida) 1903-01-30 [p ]](https://img.dokumen.tips/doc/110x75/6242bb2be4eb9e1fa907750e/ocala-evening-star-ocala-florida-1903-01-30-p-.jpg)
![Ocala Banner. (Ocala, Florida) 1908-10-23 [p ]](https://img.dokumen.tips/doc/110x75/616a2f9d11a7b741a34fbf48/ocala-banner-ocala-florida-1908-10-23-p-.jpg)
![Ocala Banner. (Ocala, Florida) 1903-03-27 [p ]](https://img.dokumen.tips/doc/110x75/61b5f476bcdf2d531b0e06f0/ocala-banner-ocala-florida-1903-03-27-p-.jpg)

![Ocala Evening Star. (Ocala, Florida) 1902-09-30 [p ]](https://img.dokumen.tips/doc/110x75/619e20531889cd14626a61f6/ocala-evening-star-ocala-florida-1902-09-30-p-.jpg)


![Ocala Banner. (Ocala, Florida) 1908-06-26 [p ]](https://img.dokumen.tips/doc/110x75/62388b81e8a89f359869929b/ocala-banner-ocala-florida-1908-06-26-p-.jpg)
![Ocala Banner. (Ocala, Florida) 1905-04-14 [p Page Ten]](https://img.dokumen.tips/doc/110x75/61dba0f99931030b291548ec/ocala-banner-ocala-florida-1905-04-14-p-page-ten.jpg)
![Ocala Evening Star. (Ocala, Florida) 1904-05-03 [p PAGE FOUR]](https://img.dokumen.tips/doc/110x75/618e9b0b90ae1569b01e48b4/ocala-evening-star-ocala-florida-1904-05-03-p-page-four.jpg)

![Ocala Evening Star. (Ocala, Florida) 1903-04-09 [p ]](https://img.dokumen.tips/doc/110x75/618bce4b3ebf59684d6e0ee4/ocala-evening-star-ocala-florida-1903-04-09-p-.jpg)

![Ocala Banner. (Ocala, Florida) 1908-08-21 [p ]](https://img.dokumen.tips/doc/110x75/6285fe13502e6b24304e88eb/ocala-banner-ocala-florida-1908-08-21-p-.jpg)
![Ocala Banner. (Ocala, Florida) 1902-01-17 [p ]](https://img.dokumen.tips/doc/110x75/623e58cd11134f7ff01347eb/ocala-banner-ocala-florida-1902-01-17-p-.jpg)


![Ocala Evening Star. (Ocala, Florida) 1906-07-26 [p PAGE TWO]](https://img.dokumen.tips/doc/110x75/628ba50718a7d63ba160113f/ocala-evening-star-ocala-florida-1906-07-26-p-page-two.jpg)
![Ocala Banner. (Ocala, Florida) 1901-09-27 [p ]](https://img.dokumen.tips/doc/110x75/620ac733da6caf2a536f95fb/ocala-banner-ocala-florida-1901-09-27-p-.jpg)