Embed Size (px)
Citation preview

American Journal of Medical Genetics 43:762-763 (1992)
Familial Aplasia Cutis Congenita and Coarctation of the Aorta B. Dallapiccola, A. Giannotti, B. Marino, C. Digilio, and G. Obregon Divisions of Medical Genetics (A.G., C.D., G.O.) and Cardiology (B.M.), Bambino Gesu’ Children’s Hospital, Institute for Scientific Research, and Chair of Human Genetics, Department of Public Health and Cell Biology, Tor Vergata University (B.D.), Rome, and C.S.S. Hospital, Sun Gwvanni Rotondo, Italy
We report on the association of aplasia cutis congenita (ACC) in the midline of the scalp vertex and coarctation of the aorta (CAI in mother and son. The acronym of ACCCA syn- drome is proposed for this condition. Autoso- ma1 dominant inheritance is most commonly implicated in the familial cases of ACC. The familial aggregation of CA is attributed, in general, to a multi-factorial causation, with a few reported families suggesting autosomal dominant inheritance. The ACCCA syndrome could be due to a Mendelian mutation. o 1992 Wiley-Liss, Inc.
KEY WORDS: aplasia cutis congenita, coarc- tation of the aorta, ACCCA syndrome, autosomal domi- nant inheritance
INTRODUCTION Aplasia cutis congenita (ACC) is characterized by a
defect in the scalp, possibly extending to the underlying calvaria. In about one-fourth of patients, this defect is isolated and, in general, is not associated with addi- tional clinical manifestations. Most cases are sporadic, although several familial instances have been recorded. Autosomal dominant inheritance with incomplete pene- trance and variable expressivity is the most frequent occurrence [Sybert, 19851.
Familial aggregation of coarctation of the aorta (CAI has been considered compatible with multifactorial in- heritance [Boon and Roberts, 19761. However, Beekman and Robinow (1985) have described a family in which CA affected 4 generations in a pattern consistent with autosomal dominant inheritance.
We report on a mother and son with a syndrome of ACC and CA.
Received for publication May 23,1991; revision received October 28, 1991.
Address reprint requests to Bruno Dallapiccola, M.D., Diparti- mento di Sanita’ Pubblica e Biologia Cellulare, Tor Vergata Uni- versity, Via Orazio Raimondo, 1-00157 Rome, Italy.
CLINICAL REPORTS
Patient 1, a 28-year-old woman, was the third child of healthy, nonconsanguineous parents. Father was 42 and mother 38 years old at the time of her birth. An older sister had a duplicated left femoral artery, which was corrected at 18 years.
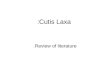
Pregnancy was normal and delivery at term. Birth- weight was 2,850 g. A membranous defect (2.8 x 0.6 cm) near the midline of the scalp was noticed at birth. Hairs were absent. This defect extended to full skin thickness, without calvaria involvement. Until age 15 years, the affected skin progressively increased in size. At present, ACC involves an area of 17 x 3 cm (Fig. la).
At 14 years, she was admitted to a hospital for evalua- tion of pain and coldness of the lower limbs and a coarc- tation of the aorta was found. Coarctectomy with patch was performed. The postoperative course was normal.
At 17 years, the patient again had acute pain and swelling of the right leg. A diagnosis of duplication of the right femoral artery was suggested, and was surgically repaired.
A heart ultrasound at 28 years showed normal cardiac function without intracardiac anomalies, and a 15 mm Hg gradient at the side of coarctectomy.
Patient 2, a boy, was the only child of patient 1. He was born at term of a pregnancy complicated by 2nd trimes- ter threatened abortion due to cervical incontinence. Birthweight was 2,630 g (3rd centile). At 15 days, the infant was referred for evaluation of a cardiac murmur. On clinical examination, he had a loud systolic murmur and an ejection click. The femoral pulses were absent and the systolic pressure of the arms was 120 mm Hg. A chest radiography showed cardiomegaly. The ECG showed biventricular hypertrophy. The ultrasono- graphic study showed a parachute, non-stenotic mitral valve with mild regurgitation. The aortic valve was bi- cuspid and there was a coarctation of the aorta. The ductus arteriosus was closed. The patient underwent coarctectomy with sub-clavian flap at 5 months.
A 2.5 x 0.7 cm midline scalp defect with characteris- tics similar to those observed in the mother was diag- nosed at birth.
The patient was revaluated by us at 3 8/12 years. Weight was 15 kg (50th centile), height 98 cm (25th
0 1992 Wiley-Liss, Inc.

Aplasia Cutis Congenita 763
Fig. 1. Aplasia cutis congenita in mother (a) and son (b).
centile) and OFC 51 cm (50th centile). The oval-shaped scalp defect was increased in size (3 x 0.8 cm) and was characterized by a residual athropic scar with alopecia (Fig. lb).
The femoral artery morphology has not been evalu- ated. Routine laboratory investigations and a chromo- some analysis were normal.
DISCUSSION Aplasia cutis congenita is a component manifestation
of many syndromes, and also occurs on a disruptive,
infectious and teratogenic basis. Association of ACC with many isolated malformations is well documented [Gorlin et al., 19901, including congenital heart defects [Deeken and Caplan, 1970; Dubosson and Schneider, 19781. ACC with CA has never been reported. We pro- pose the acronym ACCCA to designate this possibly new syndrome.
The presence of the same constellation of defects in mother and son does not disagree with the idea that this syndrome is inherited in a Mendelian fashion.
Autosomal dominant inheritance of ACC is well docu- mented [Sybert, 19851. Familial aggregation of CA has been found in 26 families reviewed by Beekman and Robinow (1985). A pattern of Mendelian inheritance is little supported by known families. In agreement with inheritance proposed for most other types of congenital heart disease, familial CA is, in general, attributed to a multifactorial causation.
However, the possibility that, in rare instances, CA can be inherited as an autosomal dominant trait with high penetrance and variable expressivity, is suggested by a family in which 5 members in 4 generations were affected [Beekman and Robinow, 19851 and by a 4 gener- ation pedigree in which a ptosis-CA syndrome was seg- regating [Cornel et al., 19871.
On the basis of the familial case described here, it is virtually impossible to conclude whether the association of ACC and CA is due to the cosegregation of the ACC autosomal dominant gene (MIM”107600) and the puta- tive CA gene (MIM 120000), or if it results from a differ- ent genetic mechanism, or even, but less likely, if these defects were associated in 2 generations purely by chance. The relationship between femoral artery dupli- cation found in 2 members of this family and the ACCCA syndrome is unclear.
REFERENCES Beekman RH, Robinow M (1985): Coarctation of the aorta inherited as
an autosomal dominant trait. Am J Cardiol 56:818-819. Boon AR, Roberts DF (1976): A family study of coarctation of the aorta.
J Med Genet 13:420-423. Cornel G, Sharratt GP, Virmani S, Rosales T, LacsonA (1987): Familial
coarctation of the aortic arch with bilateral ptosis: A new syn- drome? J Pediat Surg 22:724-726.
Deeken JH, Caplan RM (1970): Aplasia cutis congenita. Arch Dermatol
Dubosson JD, Schneider P (1978): Manifestation familiale d’une aplasie cutanee circonscrite du vertex (ACCV) associee dans un cas a une malformation cardiaque. J Genet Hum 26:351-365.
Gorlin RJ, Cohen MM, Levin SL (1990): “Syndromes of the Head and Neck.” New York-Oxford: Oxford University Press, pp 417-419.
Sybert VP (1985): Aplasia cutis congenita. A report of 12 new families and review of the literature. Pediatr Dermatol 3:l-14.
102:386-389.