Embed Size (px)
Citation preview

CHHS 15/080
Canberra Hospital and Health ServicesClinical ProcedureFalls Prevention and Management (including safe use of bed rails)Contents
Contents....................................................................................................................................1
Purpose.....................................................................................................................................3
Alerts.........................................................................................................................................3
Scope........................................................................................................................................ 3
Section 1 – Falls and Falls Injury Prevention and Management................................................4
Step 1 Falls Risk Screening....................................................................................................4
Step 2 Falls Risk Assessment.................................................................................................4
Step 3Cognitive Impairment Screening for patients 65years and older or 45years and older if of Aboriginal or Torres Strait Islander background............................................................5
Step 4 Patient Education.......................................................................................................5
Step 5 Falls Prevention Interventions and Management......................................................5
Step 6 Falls Reporting and Management Post-Fall in an In-patient Setting..........................5
1. Immediate Care......................................................................................................5
2. Notification.............................................................................................................6
3. Observation............................................................................................................ 6
4. Ongoing Care..........................................................................................................6
5. Documentation/reporting.......................................................................................7
Step 7 Discharge Planning.....................................................................................................7
Step 8 Safe Use of Bed Rails (inpatients only).......................................................................7
Step 9 Measuring Orthostatic Blood Pressure (inpatients)...................................................8
Implementation........................................................................................................................ 8
Related Policies, Procedures, Guidelines and Legislation.........................................................9
References................................................................................................................................ 9
Definition of Terms................................................................................................................. 10
Search Terms.......................................................................................................................... 11
Attachments............................................................................................................................11
Attachment A: Falls Risk Screening Tool (Ambulatory/Community Care)...........................12
Doc Number Version Issued Review Date Area Responsible PageCHHS15/080 1 14/04/2015 05/02/2019 QGR - CSQU 1 of 21
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS 15/080
Attachment B: Modified Stratify Falls Risk Assessment Tool (in-patients)..........................13
Attachment C: Intrinsic & Extrinsic Falls Risk Factors and Falls Injury Prevention Interventions.......................................................................................................................14
Attachment D: Falls Management Process Flowcharts.......................................................18
Attachment E: Bed rail Risk Assessment Matrix..................................................................21
Doc Number Version Issued Review Date Area Responsible PageCHHS15/080 1 14/04/2015 05/02/2019 QGR - CSQU 2 of 21
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS 15/080
Purpose
This document provides ACT Health with a procedure for reducing falls and injury from falls in all patients, particularly older people aged 65 and over, or 55 years and older for Aboriginal and Torres Strait Islander adults. It is acknowledged, however, that there may be non-preventable falls risks present in adults and children due to a medical condition, cognitive and other disability.
The purpose of this procedure is to: Provide direction to ALL clinical staff to improve the safety of patients by identifying their
falls risk through screening and assessment and implementing appropriate falls prevention interventions.
Establish a consistent approach to the prevention and management of falls that is in accordance with Australian best practice guidelines.
Increase awareness of the importance of being proactive in the prevention of falls and falls related injury.
Establish a consistent approach to the safe use of bed rails in accordance with best practice evidence.
Clarify the governance infrastructure in place that outlines responsibilities in relation to the prevention and management of falls and falls’ injury.
Provide direction to ALL staff to maintain a safe and clean environment.
Scope
Alerts
The alerts throughout this procedure signify a specific patient safety issue that staff must comply with.
Scope
This procedure relates to all ACT Health staff providing care to any patient within Canberra Hospital and Health Services.
This procedure is based on the Australian Commission on Safety and Quality in Health Care, 2009. Preventing Falls and Harm from Falls in Older People: Best Practice Guidelines for Australian Hospitals 2009.
The procedure includes the following steps in falls and fall-related injury prevention and management: 1. Falls Risk Screening in designated areas eg ED, Ambulatory and Community Settings; 2. Falls Risk Assessment;3. Cognitive Impairment Screening – Inpatient settings only;
Doc Number Version Issued Review Date Area Responsible PageCHHS15/080 1 14/04/2015 05/02/2019 QGR - CSQU 3 of 21
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS 15/080
4. Falls Education for the Patient and their Family and/or Carer;5. Falls and Fall-related Injury Prevention Interventions and Ongoing Management;6. Falls Reporting and Post-fall Management;7. Discharge planning; 8. Safe Use of Bed Rails; and 9. Measuring Orthostatic Blood Pressure.
Section 1 – Falls and Falls Injury Prevention and Management
Patient Care and Accountability Plan contains:o Modified Stratify Falls Risk Assessmento Cognitive Impairment Screen
Bed Rail Risk Assessment Matrix Falls Prevention Information
Step 1 Falls Risk Screening Falls Risk Screening (Ambulatory and Community Care) A falls risk screen is conducted for patients on presentation recognised at being at risk of
falling. (Attachment A – Screening tool). For community/ambulatory patients “at risk” consider referral to appropriate services
such as the patient’s GP, physiotherapy and/or the Community Falls Assessment and Prevention Clinic if patient is over 65 years.
Additional screening tools may be used by allied health.
Step 2 Falls Risk AssessmentFalls Risk Assessment (in-patients) All patients admitted will have a Falls Risk Assessment (Modified Stratify Risk
Assessment Tool- Attachment B) completed on arrival and documented on the Patient Assessment & Accountability Plan. If they are deemed at being a “High Risk” of falls (score of 3 or more) a minimum of three appropriate prevention strategies must be implemented and documented immediately after assessment is completed.
Other assessment tools may be used in other clinical areas. Timely referrals are made to allied health professionals according to risk factors, for
further assessment and provision of falls risk mitigating strategies. For inpatients identified at high risk of falls a medication review is required. (Refer table
page 14 and 15). A documented falls risk assessment should be repeated daily, as soon as possible
following a fall, when patient’s condition or environment changes, and on discharge. Some inpatient areas such as Mental Health may have patients who are ambulant and
mostly independent and therefore may be excluded from the daily falls risk reassessment. However reassessment must be completed if their condition changes.
Alert: Staff must be alert to the risk of bleeding following a fall for any patient on anticoagulants (refer to Haematology Department for advice).
Doc Number Version Issued Review Date Area Responsible PageCHHS15/080 1 14/04/2015 05/02/2019 QGR - CSQU 4 of 21
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS 15/080
Step 3Cognitive Impairment Screening for patients 65years and older or 45years and older if of Aboriginal or Torres Strait Islander background A four (4) question cognitive screen and clock drawing test has been included on the
Patient Assessment and Accountability Plan and must be completed on admission to inpatient services.
If the patient is unable to answer any of the questions correctly or draw a clock as instructed, the screen is positive and the Cognitive Impairment policy should be followed.
Step 4 Patient Education After screening and/or assessment, information regarding falls risks, prevention and
interventions should be discussed with patient and family and/or carer. Provide patients and/or carer with information brochures and relevant fact sheet. This is
to be documented in the clinical record/care plan. For inpatients, if it is deemed safer for the patient to use a walking aid, the appropriate
health professional will educate the patient, family and/or carer as to why the equipment is needed and how to use it correctly. If identified as “at risk” then explain the need for referral to other health professionals, as required.
Maintain appropriate levels of mobility. Ensure patient/carer understands the reasons for using the “Falls Risk” sign that is placed
above the bed. Involve patient/carer in bedside handover.
Step 5 Falls Prevention Interventions and Management A multi factorial and team approach is needed to achieve a significant reduction in falls
and falls related injury. Interventions should address both the intrinsic (individual) and extrinsic (environmental)
risk factors as indicated from assessment (Attachment C). Interventions and a plan of care will be determined by the falls risk assessment and the
identified falls risk factors. Individual falls prevention programs and interventions should be flexible enough to
accommodate the patient’s needs and circumstances. The falls risk level and management plan must be documented and handed over to other
care providers for ongoing care at transfer and/or discharge. Falls injuries can include fractures. Management of osteoporosis should be addressed in
those who are at risk to minimise the risk of fractures.
Step 6 Falls Reporting and Management Post-Fall in an In-patient Setting1. Immediate Care Basic Life Support (D-danger, R-respond, S-send for help. A-airway, B-breathing, C-
circulation, D-defibrillation) Conduct baseline vital signs (full MEWS) and reassure the patient. If patient meets the
MET Criteria -Dial 8 and activate Code Blue for in-patients. Continue with hourly
Doc Number Version Issued Review Date Area Responsible PageCHHS15/080 1 14/04/2015 05/02/2019 QGR - CSQU 5 of 21
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS 15/080
observations on all patients who have fallen including neurological observations if head injury is suspected (Glasgow Coma Scale)
Do not move the patient initially - call for assistance. If an inpatient, notify medical officer. Stabilize the patient before moving. Immobilise the spine if head and neck pain is
reported. Observe for any changes in condition i.e. increased pain, reduced mobility or change in
vital signs. Clean and dress any wounds. If fall is not witnessed consider further imaging if clinically indicated. If the fall occurs in the community, refer to the GP for a medical review or call an
ambulance if injury suspected.
Alert: Staff must be alert to the risk of bleeding following a fall for any patient on anticoagulant.
2. Notification Call a “huddle”, a multidisciplinary meeting immediately following the fall to discuss
what had happened and how it can be prevented in the future. Contact medical officer for review. The medical officer is to complete the Post Fall
Medical Assessment Form 35557 found on the Clinical Forms Register on the Intranet Notify registrar/consultant (if required). Notify CNC/Team Leader and JMO. Inform relatives/carer of the fall and, where appropriate, discuss ongoing management
plan. Document interaction with relatives/carer.
3. Observation Record vital signs hourly for 4 hours then review and continue as per medical orders and
clinical condition (MEWS score) Notify Medical Officer immediately if any changes in patient observations or condition Observe for signs of bleeding if on anticoagulants.
4. Ongoing Care Review environment (e.g. high-low bed, position of locker/belongings, call bell, and
mobility aids). Review of clothing to ensure long gowns, socks and footwear are not contributing to
falls. Reassess the patient and arrange any additional interventions that may be required such
as hip protectors, physiotherapy or a specialist review. Plan interventions using a multidisciplinary approach which may include:
o Medication review o Geriatrics/Rehabilitation reviewo Nutrition reviewo Physiotherapy reviewo Occupational Therapy review
Doc Number Version Issued Review Date Area Responsible PageCHHS15/080 1 14/04/2015 05/02/2019 QGR - CSQU 6 of 21
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS 15/080
o Optometrist, podiatry, social worker, Vision Australia or other specialisto Community Falls Assessment and Prevention Clinic on discharge
5. Documentation/reporting Document the fall in the clinical record, including any injuries and observations. Include
in the progress notes the Post Falls Sticker to easily identify when a fall has occurred. For a patient who has sustained a significant injury, a “Significant Fall Incident Review”
document must be completed. Complete a RiskMan report, including the extension module, record Riskman incident
number on care plan. A RiskMan should be completed within the community/ambulatory settings if the fall occurs while staff member is present.
Manager should provide follow up information into RiskMan (investigations and controls) with the outcome from the fall.
Handover appropriate information to all staff caring for the patient. Complete the Post Falls Audit and take appropriate action from findings. A family member/carer/guardian must be notified after any fall.
For patients who fall in the community, arrange for review with GP or emergency department if injury is suspected.
NOTE: For inpatients, a post fall analysis should be conducted to identify why the fall occurred and include changes to management. If serious injury or death has occurred as a result of the fall an in-depth clinical review of the fall must be conducted.
Step 7 Discharge Planning For patients at risk of falls, include interventions to reduce the risk of falls and harm from
falls in discharge planning. Planning for discharge should commence at admission. Include specific falls information in all discharge, transfer and referral information for all
patients at risk of falls or who have fallen. For inpatients, including the physiotherapist and occupational therapist as an integral
part of the discharge plan enables a home safety assessment, at discharge, to be done. Allow adequate time for equipment availability and education of patient and carer to
prevent any delays in discharge from inpatient settings. Consider a referral, where appropriate, to the Falls Assessment and Prevention Clinic and
other community services. Referrals can be made via CHI.
Refer to the flowcharts at Attachment D for a summary of these procedures.
Step 8 Safe Use of Bed Rails (inpatients only)Bed rails may be used to reduce the risk of a patient accidently slipping, sliding, falling or rolling out of bed. Bed rails will not prevent a patient from leaving their bed and falling elsewhere and should not be used for this purpose (restraint). Patient risk assessment must be carried out and the result documented in the care plan with regard to the decision to not use (or use) bedrails prior to their use. This decision will be reviewed in line with changes to the patient’s condition.
Doc Number Version Issued Review Date Area Responsible PageCHHS15/080 1 14/04/2015 05/02/2019 QGR - CSQU 7 of 21
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS 15/080
On all occasions, the default position is bed rails DOWN, unless clinically indicated through risk assessment.
All patients will be assessed using the Bedrail Risk Assessment Matrix (Attachment E). The decision to use or not use bedrails will be documented on the care plan. All patients will be assessed for the appropriateness of use of bedrails on admission and
reviewed in response to changes in their condition. Whenever possible the decision to use or not use bedrails will be communicated to all
staff/carers responsible for the care of the patient.
Alert:Default position for bed rails is down unless a bed rail risk matrix is completed.
Step 9 Measuring Orthostatic Blood Pressure (inpatients)Postural hypotension or orthostatic hypotension is defined as the ‘reduction in systolic blood pressure of ≥ 20mmHg or a reduction in diastolic blood pressure of ≥ 10mmHg during the first 3 minutes of standing’ from lying down (1). This is typically associated with autonomic failure and can be multi-factorial.(2) This is a common cause of patients falling and needs to be included in the risk assessment for a patient who has sustained a fall as multiple strategies can be employed to reduce the subsequent risk of falls and related injury in these patients.
Postprandial hypotension is defined as a reduction of systolic blood pressure of ≥ 20mmHg 1 hr post meal (3).
Alert: Any type of chemical or physical restraint should not be used as a falls prevention intervention. Refer to ACT Health Policy (DGD11-080) – Restraint of Patients and Health Directorate SOP (DGD11-081) – Restraint of Patients.
Alert: In-patient settings –any environmental or equipment hazard that compromises patient safety and increases falls risk must be attended to immediately and reported through appropriate channels.
Back to Table of Contents
Implementation
Information contained in this document will be disseminated to staff via educational forums, falls champion workshops and via e learning modules.
Back to Table of Contents
Related Policies, Procedures, Guidelines and Legislation
Legislation
Doc Number Version Issued Review Date Area Responsible PageCHHS15/080 1 14/04/2015 05/02/2019 QGR - CSQU 8 of 21
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS 15/080
Work Health and Safety Act (2011) Patient Health and Safety ACT (2003) Human Rights Act (2004)
Related Policies Restraint of Patients Policy (DGD11-080) & SOP (DGD11-081) ACT Health RiskMan Incident Reporting Policy (CED07-032) ACT Health Occupational Health & Safety (OH&S) Policy (CED08-066)
Standards Australian Commission on Safety and Quality in Health Care. Safety and Quality
Improvement Guide Standard 10: Preventing Falls and Harm from Falls (October 2012). Sydney. ACSQHC, 2012.
Back to Table of Contents
References
Australian Commission on Safety and Quality in Health Care. 2009. Preventing Falls and Harm from Falls in Older People: Best Practice Guidelines for Australian Hospitals. Available at the commission website http://www.safetyandquality.gov.au/ The Royal Children’s Hospital Melbourne Falls Prevention Clinical Guidelines http://www.rch.org.au/rchcpg/index.cfm?doc_id=15422
Centre for Rural Health Website: Falls Prevention University of Tasmania http://www.ruralhealth.utas.edu.au/falls/
Queensland Stay on your Feet Website – Preventing falls in older Queenslandershttp://www.health.qld.gov.au/stayonyourfeet/
The definition of orthostatic hypotension, pure autonomic failure, and multiple system atrophy. J Auton Nerv Syst 1996; 58:123-4.
Freeman R, Neurogenic orthostatic hypotension N Engl J Med 2008; 358:615-24.
Fisher A et al, Postprandial Hypotension Predicts All-Cause Mortality in Older, Low-Level Care Residents J Am Geriatr Soc. 2005 Aug;53(8):1313-20.
Back to Table of Contents
Definition of Terms
A fall: An event which results in a person coming to rest inadvertently on the ground or floor or other lower level.
Doc Number Version Issued Review Date Area Responsible PageCHHS15/080 1 14/04/2015 05/02/2019 QGR - CSQU 9 of 21
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS 15/080
A paediatric fall: Paediatric falls should be considered in the context of normal physical growth and cognitive development. Children are likely to experience falls as they become more active and begin to explore their environments. However, some falls are preventable along the growth and development continuum. Newborns are at risk of falling from high surfaces such as a change table, bed or lounge, so care must be taken to keep one hand on newborns when they are not in their crib or cot. Mobility increases in the first year of life, including crawling, rolling and standing. Infants at this stage of development should not be left unsecured in a high chair or on any elevated surface, and when placed in their cot the sides must be elevated and secured. Further, stairways should be secured with doors or gates to prevent a fall which could result in significant injury. Gross motor skills improve when infants become toddlers, allowing them greater mobility, including moving chairs to counters or railings. Therefore, close supervision is required to keep them from falling from high surfaces. Children of preschool age are able to function more independently and they often engage in adventurous activities. They may need constant reminders to modify these behaviours, such as running or climbing. School aged children and adolescents sequentially reach greater levels of independence, becoming less risk adverse, so falls prevention is also relevant in this older age range (Ball, Bindler & Cowen, 2012).
ED: Emergency Department
Interventions can be described as:Single intervention: an intervention targeting one risk factor, such as a balance and strength exercise program or medication adjustment.Multifactorial intervention: an intervention made up of a set of single interventions that are intended to address some or all of the specific risk factors that were identified through an individual’s fall injury risk assessment. This is ideally provided by a multidisciplinary team.
MEWS: Modified Early Warning Score
JMO: Junior Medical Officer
Patient: Any person, client or consumer of Health Directorate services
Older Person: A person aged 65 years of age or over, or 55 years and over for Aboriginal and Torres Strait Islander adults.
Back to Table of Contents
Doc Number Version Issued Review Date Area Responsible PageCHHS15/080 1 14/04/2015 05/02/2019 QGR - CSQU 10 of 21
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS 15/080
Search Terms
Falls Prevention and ManagementFalls and Falls Injury PreventionFalls ScreenFalls AssessmentBed Rails
Bed rails risk matrixRestraintFalls prevention interventionsMeasuring Hypostatic blood pressure
Back to Table of Contents
Attachments
Attachment A: Falls Risk Screening Tool & Delirium Screening ToolAttachment B: Modified Stratify Falls Risk Assessment ToolAttachment C: Intrinsic and Extrinsic Falls Risk Factors and Falls Injury Prevention
InterventionsAttachment D: Falls Management Process Flowcharts Attachment E: Bedrail Risk Assessment Matrix
Disclaimer: This document has been developed by ACT Health, Canberra Hospital and Health Services specifically for its own use. Use of this document and any reliance on the information contained therein by any third party is at his or her own risk and Health Directorate assumes no responsibility whatsoever.
Policy Team ONLY to complete the following:Date Amended Section Amended Divisional Approval Final Approval16/03/2018 Information to Cognitive
Impairment addedLinda Kohlhagen, Exec Sponsor Std 10
CHHS-PC Chair
This document supersedes the following: Document Number Document Name
Doc Number Version Issued Review Date Area Responsible PageCHHS15/080 1 14/04/2015 05/02/2019 QGR - CSQU 11 of 21
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS 15/080
Attachment A: Falls Risk Screening Tool (Ambulatory/Community Care)
The following two questions constitute the Falls Risk Screen:
1. Is the patient 65 years or older, or 55 years for Aboriginal and Torres Strait Islander adults
2. Does the patient have a history of falls in the past 12 months?
If the patient responds “yes” to either of these two questions, consider appropriate action.
Neurological (Delirium) Screening Tool
Doc Number Version Issued Review Date Area Responsible PageCHHS15/080 1 14/04/2015 05/02/2019 QGR - CSQU 12 of 21
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS 15/080
Attachment B: Modified Stratify Falls Risk Assessment Tool (in-patients)
Management Plan (extract from Patient Assessment & Accountability Plan)
Doc Number Version Issued Review Date Area Responsible PageCHHS15/080 1 14/04/2015 05/02/2019 QGR - CSQU 13 of 21
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS 15/080
Attachment C: Intrinsic & Extrinsic Falls Risk Factors and Falls Injury Prevention Interventions
Intrinsic (Individual) Factors Possible InterventionsHistory of falls both recent & old Alert all staff of increased risks
Consider use of hip protectors Consider use of bed and chair alarms Place patient under close observation and supervision
Patient’s age Increased awarenessMedicationsAny agent which can cause increased falls risk e.g. psychotropic, antihypertensive drugs, diuretics, sedatives, and analgesia.
Collaborate with the pharmacistNote: Risk of bleeding greater after a fall if patient is on anticoagulant therapy. Consider referral to Haematology
Recent change in medications. Increased awarenessPolypharmacy => 4 medications Collaborate with medical staff and pharmacistOsteoporosis and use of Vitamin D/Calcium.
Consider Vitamin D, Calcium and as anti-osteoporotic medications (Bisphosphonate or Denosumab)
Long stay patients – time in sunshine where possibleCognitive impairment(confusion/dementia/delirium and depression)
Awareness and appropriate review to identify cause and/or triggers
Address reversible causes of acute or progressive cognitive decline
Treat orthostatic hypotension (common in pts with dementia)
Closer observation, supervision and assistance Medication review Modify environment Exercise programs to improve gait, balance, mobility
& flexibility Consider hip protectors Lower beds Use fall alarm devices
Impulsiveness. Education of staff Close observation and supervision Medication review
Lack of insight/capacity. Education of carers Closer observation Consider chair/bed alarms Sitters Hourly rounding
Fear of falling Patient education Balance /exercise classes Psychologist referral/disability counsellor
Doc Number Version Issued Review Date Area Responsible PageCHHS15/080 1 14/04/2015 05/02/2019 QGR - CSQU 14 of 21
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS 15/080
Withdrawal from any substances. Utilise relevant withdrawal chart Refer drug and alcohol service Patient education Medication review
The need for oxygen – hypoxic agitation. Ensure appropriate and safe oxygen useHypotension. Measure postural blood pressure
Education Medication review Investigate other causes of syncope Ensure good hydration Encourage patient to take their time when moving
from a lying positionIncontinence – bladder and bowel. Screen for UTI
Use incontinence aids i.e. for catheters (IDC/SPC) consider a leg bag
Regular toileting Continence health professional referral Medication review Minimise environmental risk factors i.e. clutter free
pathway to toilet, easy to undo clothing, hand rails, leave toilet light on.
Sensory loss- vision impairment- somatosensory loss (i.e. from peripheral neuropathy)- hearing loss- vestibular system(inner ear)
Optometrist referral Ensure patient has spectacles/hearing aids with them Educate patient re bifocals and multifocal risk when
walking Adequate lighting Medical review e.g. if cataracts present Assist with mobility and walking aids Medication review Vestibular health professional referral Audiologist review Diagnose and treat BPPV(Benign paroxysmal
positional vertigo)Nutritional status. Nutritionist/dietician referral
Assist with nutritional intakeRecent lower limb surgery- for example knee replacement.
Physiotherapist and occupational therapist referral Appropriate equipment and aids available
Musculoskeletal pain - increased risk if in two sites.
Physiotherapist referral Assist with mobility Medication review Medical review
Muscle strength. Physiotherapist and occupational therapist referral
Doc Number Version Issued Review Date Area Responsible PageCHHS15/080 1 14/04/2015 05/02/2019 QGR - CSQU 15 of 21
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS 15/080
Encourage functional activity and exerciseGait and balance disorders. Medical review
Walking aids Assist with mobility medication review Vestibular health professional referral Close supervision when ambulating
Foot pain/deformities Appropriate review by medical and podiatry
Doc Number Version Issued Review Date Area Responsible PageCHHS15/080 1 14/04/2015 05/02/2019 QGR - CSQU 16 of 21
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS 15/080
Extrinsic (Environmental) Factors Possible InterventionsRestraint – physical or chemical Avoid use of restraint
Investigate possible causes for ’risky behaviour’ such as agitation and implement appropriate strategies: sitters/companionship/carer diversionary activity low beds decreasing environmental noise and activity
meeting patient’s physical and comfort needs Complete bed rail risk matrix before use
Unsafe environment e.g. slippery floor, spills, floor mats.
Ensure environment is safe: clean spills promptly ensure flooring is non slip Signage for steps / cords
Poor Lighting. Consider night lighting particularly in toiletsExcess furniture. De clutter environmentFurniture. Use low bed
Brakes on bed Consider use of cot sides Have seating at correct height Report environmental safety issues to Work and
Safety Representative/Manager and RiskManFailure of walking aids. Inspection to ensure safe e.g. rubber stoppers on
walking sticks, etc. Ensure correct use of walking aids
Inappropriate footwear Educate patient Ensure correct footwear is available Discourage patient from walking in socks or bare feet
Walking aids/personal belongings not in reach.
Ensure call bells, walking aids and belongings within easy reach
Sleep deprivation. Refer to appropriate health professional Normalise diurnal cycle
Patients require assistance when transferring/mobility.
Educate patient to call for assistance Regular toileting
Issues with language and understanding Use interpreter family/carer
Doc Number Version Issued Review Date Area Responsible PageCHHS15/080 1 14/04/2015 05/02/2019 QGR - CSQU 17 of 21
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS 15/080
Attachment D: Falls Management Process Flowcharts
Doc Number Version Issued Review Date Area Responsible PageCHHS15/080 1 14/04/2015 05/02/2019 QGR - CSQU 18 of 21
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS 15/080
Doc Number Version Issued Review Date Area Responsible PageCHHS15/080 1 14/04/2015 05/02/2019 QGR - CSQU 19 of 21
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS 15/080
Doc Number Version Issued Review Date Area Responsible PageCHHS15/080 1 14/04/2015 05/02/2019 QGR - CSQU 20 of 21
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS 15/080
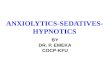
Attachment E: Bed rail Risk Assessment Matrix
Mobility
Patient is very immobile Patient is neither independent nor immobile
Patient can mobilise without help from staff
Orie
ntati
on
Patient is confused and disorientated
Use bedrails with care Bedrails not recommended
Bedrails not recommended
Patient is Drowsy Bedrails recommended Use bedrails with care Bedrails not recommended
Patient is orientated and alert Bedrails recommended Use bedrails with care Bedrails not recommended
Patient is unconscious Bedrails recommended N/A N/A
Instructions for use:Determine patient orientation (i.e. Patient is drowsy) then determine mobility (i.e. Patient can mobilise without help from staff) Follow matrix across until both orientation and mobility meet (i.e. Bedrails not recommended). Use of bedrails must be reassessed when patient’s condition changes. On all occasions, the default position should be bed rails DOWN, unless clinically indicated through assessment. Adapted from the National Patients Safety Agency’s safer practice notice “Using Bedrails Safely & Effectively
Doc Number Version Issued Review Date Area Responsible PageCHHS15/080 1 14/04/2015 05/02/2020 HCID 21 of 21