Embed Size (px)
Citation preview

Journal of Orthopaedic
Research www.elsevier.com/locate/ort hres
ELSEvlER Journal of Orthopaedic Research 22 (2004) 479486
Failure of trabecular bone with simulated lytic defects can be predicted non-invasively by structural analysis
James Hong, Greg D. Cabe, John R. Tedrow, John A. Hipp, Brian D. Snyder * Ortliopedic Bbmechunir.s Luhorutorj: Beth Isruel Deaconess Metlicnl Center, Boston, Mussuchicsrtts 02215. USA
~~ ~~
Abstract
Pathologic fracture is a significant risk for patients afflicted with metastatic or benign skeletal tumors. The quandary for phy- sicians who treat these patients is that after making the diagnosis they must try to predict the load bearing capacity of the involved bone and the fracture risk from images seen in radiological examinations. Since bone fails at a relatively constant strain independent of density we demonstrate that using a mechanics of materials approach that the cross-sectional structural properties of the bone most affected by the lytic defect governs the load bearing capacity of the entire bone.
Homogeneous cylindrical cores of trabecular bone were harvested from the vertebral bodies of whale spines, and prepared with circular or slotted through-hole defects of varying sizes to simulate lytic skeletal tumors. Each specimen was imaged using quan- titative computed tomography (CT), dual energy X-ray absorptiometry (DXA), and magnetic resonance imaging (MRI) to obtain data for calculating cross-sectional structural properties: axial, flexural, and torsional rigidity. The specimens were then divided into groups uniformly distributed with respect to defect sizes and shapes, and subjected to uniaxial tension, four-point bending or torsion until failure.
A strong positive relationship was found between measured tensile yield loads, bending, and torsional yield moments vs. axial, flexural and torsional structural rigidities respectively, calculated from QCT, DXA, and MRI data [QCT: tension r’ = 0.951, bending r’ = 0.909, torsion 9 = 0.914 ( p < 0.001); DXA: tension t2 = 0.926, bending r2 = 0.841, torsion rZ = 0.916 (p < 0.001); MRI: tension Y’ = 0.916; bending r’ = 0.856, torsion r2 = 0.852 ( p < 0.00l)l.
For cylindrical cores of trabecular bone with simulated lytic defects, the load bearing capacity of the entire core was directly proportional to the axial, bending, or torsional rigidity at the weakest cross-section through the core containing the defect. Therefore structural rigidity analysis of cross-sectional geometric data measured non-invasively by QCT, DXA, and MRI of bones containing lytic defects may be used to predict the load bearing capacity of the involved bone and the relative fracture risk in vivo. 0 2003 Orthopaedic Research Society. Published by Elsevier Ltd. All rights reserved.
Ki~.vivorcl.c; Non-invasive; Trabecular: Failure
Introduction
Improved guidelines are needed for preventing path- ologic fractures and evaluating response to treatment in the large numbers of patients with benign and malignant lytic skeletal tumors. Pathological fractures through lytic defects in the appendicular and axial skeleton occur at all ages and are often associated with intractable pain, loss of function, and other morbidities. Lytic bone de- fects that can cause pathologic fracture include both
* Corresponding author. Address: Department of Orthopedic Sur- gery, Children’s Hospital, 300 Longwood Avenue, Boston, MA 021 15. USA. Tel.: +1-617-355-8361.
E-mud utldress: [email protected] (B.D. Sny- der).
malignant and benign tumors in children and in adults. Benign skeletal tumors were diagnosed as an incidental finding in 8-33Y0 of long bone radiographs in children [7]; 20-7OYn of cystic bone tumors ultimately fractured. In adults, the skeleton is the third most common site for metastatic spread of carcinoma [3]. Approximately 30”/0 of bone metastases subsequently fracture or produce symptoms severe enough to require treatment with radiation, bisphosphonates, glucocorticoids or calcito- nin [27].
The dilemma for the physician managing these pa- tients is multifaceted. First, one must decide if the lesion is benign or malignant, and second if the defect has weakened the bone to cause pathological fracture. Pre- vious investigations have considered defect geometry, pain, anatomic site, lesion type and activity levels to be predictors of fracture risk for the appendicular skeleton
0736-0266/$ - see front matter 0 2003 Orthopaedic Research Society. Published by Elsevier Ltd. All rights reserved doi: 10.1016/j.orthres.2003.09.006

480 J. Hong et ul. I Journul of Ortl?opuedic Research 22 (2004) 479-486
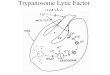
i' I LyticDefect A Axial (EA), I Transmural
w v Rigidity ' 1 I A I
Tension Bending Torsion
Tc Y r = - = G Mc
+ M = k,(El) -+ T = k,(GJ)
o=-- - EE F p = - = E & A i J
+ F = k,(EA)
Fig. I . Derivation of the relationship between failure load and structural rigidity. Applying basic principles of mechanics of material and assuming constant strain to failure, the load bearing capacity of bone is directly proportional to the structural rigidity (EA, El, and GJ) in each respective mode of loading: tension, bending, and torsion. View A-A is a transverse cross-section through the defect where minimum rigidities can be measured. u is stress. F is applied uniaxial load, A is cross-sectional area, E is Young's modulus of elasticity, i: is strain at failure, which is constant, M is applied bending moment, c is the distance from the outermost surface to the neutral bending axis, I is the minimum moment of inertia normal to the bending axis. T is shear stress, T is the applied torque, J is the polar moment of inertia, G is the shear modulus of elasticity, 7 is shear strain, and kl-k3 are constant coefficients, where k , ix ~ p ~ , ~ ~ ~ ~ , k2 o( ~ ~ ~ , ~ ~ ~ ~ / c , and ki ix eft,,luce/c,
in clinical studies [8,16,20]. Since plane radiographs are routinely obtained when treating these patients, several investigators have used guidelines based solely on geo- metry to estimate the load bearing capacity of a bone from simple radiographic measurements. Two such guide- lines are frequently cited [12]: ( I ) a defect >2.5 cm in diameter should be considered at risk for fracture, and (2) greater than 50%) cortial destruction is an indication for prophylactic stabilization. However, these guidelines have never been shown to be specific for predicting fracture and they are also insensitive to the loading mode and relative location of the defect. Three ortho- pedic oncologists were provided radiographs and com- puted tomography (CT) scans of proximal femora with simulated lytic defects and intact contralateral femora as controls [12]. Each surgeon was asked to predict the relative strength reductions imposed by the defect. There was no consistency among the physicians in their pre- dicted strength reductions and no correlation between their predicted and the experimentally measured strength reductions.
Optimal treatment for bone defects remains contro- versial [10,14,15,23], in part because there are no ob- jective methods for evaluating the success of various treatment protocols. The prevention of pathological fracture depends on better techniques and more objec- tive criteria for evaluating the tumor response to sys- temic and/or local therapy, so that if a patient has failed to respond, treatment can be altered.
Because trabecular bone is metabolically more active than cortical bone, many pathologic changes first ap- pear at sites comprised primarily of trabecular bone. While there have been several studies investigating the effect of holes in cortical bone, to the best of our knowl- edge there have been no previous studies investigating
the effect of simulated lytic defects in cylindrical cores comprised entirely of trabecular bone.
The microstructure of human trabecular bone is similar to other engineering open-cell porous materials [ I 11; its strength and stiffness vary as power law func- tions of porosity (or density). Recent studies strongly suggest that trabecular bone fails at a constant strain irrespective of apparent bone density [6,9,18,26]. Based on the principles of mechanics of material, we hypoth- esize that the behavior of whole bones with lytic defects can be predicted from the cross-sectional geometry and material properties of the bone at the defect. If bone fails at constant strain, for structures with the same external geometry and symmetry about the loading axis, the failure load is proportional to the structural rigidity at the weakest cross-section (Fig. 1).
The aims of this study were: (1) determine if measures of structural rigidity calculated from non-invasive imaging (quantitative-CT, DXA, and MRI) data predict failure of trabecular bone cylindrical cores with and without simulated lytic defects subjected to uniaxial tension, four-point bending, and torsion, (2) determine the effect of defect shape (slotted vs. circular holes) on failure load and on the relationships between failure load and the corresponding rigidity for each imaging modality, and ( 3 ) determine if the reduction in rigidity predicts the reduction in load carrying capacity for the entire bone core.
Methods
Specimen prepurution
In order to create a range of physiologically relevant defect sizes without risking the structural integrity of the specimen itself or vio-

J. Hong et al. I Journal of Orthopaedic Research 22 (2004) 479-486 48 1
Y ’
lating the continuum nature of trabecular bone, large diameter speci- mens of homogeneous trabecular bone were required. We harvested cylindrical cores (n = 200; Diam= 12.7 mm; L = 73 mm) of trabecular bone from the thoracic to caudal vertebral bodies of six whale spines (Physeier macrorynclius, Baelenu rnystecetus, Koju breviaceps: North Slope Borough Wildlife Management, Barrow AK and National Marine Fisheries, Miami FL). A one-half inch diameter diamond tip coring tool was used to extract cylindrical cores in the superior to inferior direction. Specimens were initially screened using plane radiographs for naturally occurring discontinuities (e.g. vascular channels) and misalignment of trabeculae along the axial direction. One hundred five cylindrical cores were selected for mechanical testing. Each end of the cylindrical core was embedded in polymethylmeth- acrylate to facilitate mechanical testing and ensure compatibility with MRI scanning. Symmetric through-hole defects were created in the middle of the cores using a Bridgeport mill (Bridgeport CT) and car- bide endmill bits (SGS, Munroe Falls OH). Five cylindrical cores were distributed to each of seven groups: no defect, three groups with cir- cular-hole diameter to specimen diameter ratios of 28%, 47%). and 56% (Diam of circular defects, 0 : W’ .-.., are 3.56, 5.97, and 7.1 1 mm), and
:wi three groups with slotted holes with the same slot-width to specimen diameter ratios as the circular defect groups, but with a 2.1 slot length
dy p,=converted apparent density
f - Y
~~
to width ratio (Slotted defects had rounded ends, - i :w ..... ,
L:w = 2:l). Thirty-five cylindrical cores (5 specimens for each of 7 groups) were prepared for each of three modes of testing: uniaxial tension, four-point bending, and torsion.
Quantitative imaging
QCT-Specimens were encased in saline filled tubes, and placed in a vacuum chamber to remove air from the pore spaces (Precision, Hingham MA; Labconoco, Kansas City MO). A density phantom, consisting of six hydroxyapatite cores (Computerized Imaging Refer- ence Systems, Northfolk VA), with ash densities of 0.005, 0.0432, 0.142, 0.526, 1.071, and 1.544 glcm’, was scanned with the specimens
in a high speed helical C T scanner (GE Medical Systems, Milwaukee WT). Three millimeter thick slices were taken with a 0.234 nimlpixel resolution. Images were transferred to a Spare 10 workstation (Sun Microsystems, Palo Alto CA), and using AVS (Advanced Visual Systems; Waltham MA) software, the images were converted from gray level intensity (Hounsfield units) to equivalent hydroxyapatite bone density images based on the linear regression calibration between the average Hounsfield units and corresponding ash densities for all the hydroxyapatite phantoms.
The elastic and shear moduli for whale trabecular bone were de- termined from empirically determined relationships between apparent bone density and modulus. Published literature on the relationship between Young’s modulus and bone density has typically shown a power law function for bovine and human trabecular bone [5.17, 241, and Ford and Keaveny [9] demonstrated that a linear relation- ship exists between shear modulus and apparent density for bovine trdbecular bone. This has been shown to hold true for whale trdbec- ular bone ( E = 4677pId7 + 169, r2 = 0.829, p < 0.01, n = 22; G = 5 3 7 . 6 ~ ~ ~ ~ - 101, = 0.884, p < 0.01, n = 10). Structural rigidities were estimated by weighting the cross-sectional area ( A ) , bending moment of inertia ( I ) , and polar moment of inertia ( J ) . of each pixel by the empirically derived density dependent relationship for the shear and elastic moduli, then summing the rigidity of each pixel about the modulus weighted centroid or neutral axis (Fig. 2).
DXA-Examinations were performed with the trdbecular bone specimens submerged in water to simulate soft tissue and to establish a steady baseline. Cross-sectional measurements were obtained perpen- dicular to the long axis of the specimen. Specimens were scanned using a Hologic QDR 2000 (Waltham MA) in pencil beam mode at 70 KVp and 140 KVp and a point resolution of 0.0127 cm. The attenuation at each point was converted to areul bone mineral density (i.e. BMD is not true density, it is defined a s the mass divided by the projected area with units g/cm2) [2]. A cross-sectional profile of BMD in the plane of the cross-section was generated and used to compute the BMD mo- ment of inertia [I91 and BMD based area, I r l . ~ ~ ~ . I\?.BMD and A B M D (Fig. 3). These cross-sectional properties describe the distribution of bone mineral in space, similar to the mass moment of inertia rather than cross-sectional geometric moment of inertia calculated from the
I - X
Eq 1 Neutral Axis; Centroid:
Eq 2 Axial Rigidity:
Eq 3 Flexural Rigidity:
Eq 4 Torsional Rigidity:
Fig. 2. Schematic illustration of the algorithm to determine axial (EA), flexural (EI), and torsional (GJ) rigidities from QCT and MRI data. Each pixel is filtered through a bone density threshold, and converted to material modulus ( E or G depending on the loading mode) and using empirically derived relationships for whale trabecular bone as a function of apparent bone density (E, = 4677i1:’~ + 169. rz = 0.829, p < 0.01; Gi = 537.6p, ~ 101, r2 = 0 . 8 8 4 , ~ < 0.01). The relative distance between pixels is determined by the calibration of the imaging modality. The modulus weighted neutral axis and centroid (Eq I ) are determined based on the coordinates of the ith pixel, its modulus (En) , area (da), and total number of pixels in the bone cross-section (n). Axial rigidity (Eq 2) is the sum of the products of each pixel’s elastic modulus (E , ) and pixel area (da). Flexural rigidity about the y-axis (Eq 3) is the sum of the products of the elastic modulus (E,) , square of the ith pixel distance to the neutral axis (jj), and the pixel area (da). Torsional rigidity (Eq 4) is the sum of the products of the density dependent shear modulus (G)), square of the pixel distance to the centroid (f.?), and the pixel area (da).

482
1 B O O i / 0.2% Strain
1.600- ,/ Offset Line ~
Ultimate load / I
-f X
--f Y
Fig. 3. Schematic illustration of DXA quantitative algorithm. The bone mineral density (BMD) profile measured by DXA through the core cross- section is used to determine: ( I ) the BMD-weighted section area (ABMD), which is the area under the BMD profile and represents the amount of bone mineral in the cross-section of analysis, and (2) the BMD-weighted moment of inertia ( IBMD) . which is the second moment of bone mineral about the centroid (.?.,V) of the BMD profile (IHMU) and represents the distribution of bone mineral in the cross-section of analysis perpendicular to the scan direction. These parameters are analogous to axial rigidity, EA, and bending rigidity, El. respectively. A and B illustrate scans with the specimen oriented in its two principal directions. The BMD-weighted polar moment of inertia ( J B M ~ ) . is analogous to torsional rigidity GJ. and is determined by the sum of the BMD-weighted moments of inertia along the two principal axes ( I > ? . B M D and I,, BMD).
QCT data. Two mutually perpendicular scans were taken to represent BMD moments of inertia at cross-sections through the defect in the principal directions: one with the defect oriented perpendicular to the pencil beam (Fig. 3A) and the other with the defect oriented parallel to the pencil beam (Fig. 3B). The BMD polar moment of inertia (JBMD)
was given by I,, H M D + I , , R M D .
MRI-Marrow content was left in situ, and the specimens sub- merged in corn oil. Corn oil simulates the image intensity character- istics of fatty marrow [21], and the MRI sequence used in the study was custom designed to reduce the signal intensity differences between red and fatty marrow [13]. Air trapped within marrow pores was removed using a vacuum chamber. Overlapping 3 mm consecutive transverse images were obtained through the defect site and contiguous bone using a 1.5T Signa Imager (GE Medical Systems, Milwaukee WI) and quadrature head coil. A proton density sequence with repetition and echo times of TR/TE = 5000/18 ms and a resolution of 0.781 mm/pixel was used to homogenize the different signal characteristics between hematopoietic (red) and fatty (yellow) marrow. Since MRI measures free protons. the signal of the marrow phase is more prominent than the bone phase. Therefore a porosity phantom, manufactured from open-celled polyurethane foams (Quality Foam, Eddystone PA) was used to convert the gray level of each pixel to an equivalent volume fraction of the marrow (V,,,,,,) or bone porosity. MRI images of trabecular bone were analyzed using AVS and converted to apparent bone density images [21] based on the tissue density of whale trabec- ular bone ( ( I , ~ , , ~ ~ = 2.6 f 0.2 glcc) and bone porosity measurements { ~ ~ ~ l p p d r c , l , = p,,s5ue * (1 - V,,,,,,,)}. Similar to the method described previously for QCT, elastic and shear moduli were determined from empirically derived relationships for whale trabecular bone, and structural rigidities (EA, EI. and GJ) of the entire cross-section cal- culated using an image processing algorithm (Fig. 2).
slope of the load vs. displacement curve deviated 30% from the slope of the linear (elastic) portion of the curve; this corresponds roughly to a 2% offset used to define yield [or conventional stress vs. strain curves (Fig. 4).
Load
1.000
1.400
1.200
0.600
0.400
0.800 (Nm)
Mecliuiiicd tcstiiig
Prior to mechanical testing, specimens were thawed for approxi- mately 1 h and tested at 21 "C and 63'%1 relative humidity. Linear and angular displacements for each testing device were measured using an infrared optical system (Qualysis MacReflex, East Windsor CT) capable of resolving 1 1 pm displacements in three-dimensional space. One-millimeter square infrared (IR) reflective markers were attached to the specimen with cyanoacrylate. and the relative positions of the markers monitored using Biopac (Santa Barbara CA) as the specimens deformed under applied load. Failure of the specimens was defined as the yield load that corresponded to the point where the instantaneous

J. Hong er ul. I Journtrl of Ortliopaedic R~serrrch 22 (2004) 4 7 9 4 % 483
U17iusiuI terision-Tension tests were conducted under displace- ment control with a single ramp to failure at an average strain rate of 0.08’Ws. A ball-joint attached to a cable was used to couple the specimen to a uniaxial servohydraulic actuator (Instron, Canton MA) to reduce parasitic forces and moments. Relatively weaker specimens with an apparent density less than 0.44 glcc and defect diameter greater than or equal to 47% of the specimen diameter were tested with a 500 Ib load cell: all other specimens were tested with a 2000 Ib loadcell in order to capture the actual failure load. The MacReflex system was used to measure displacement at the gauge length from IR markers; Lagrangian strain was determined as the ratio of axial displacement to the nominal gauge length.
Four-point hending-Bending tests were conducted about the spec- imen axis associated with the minimum flexural rigidity (i.e. the lon- gitudinal axis of the defect was collinear with the direction of the applied load) using a four-point bending apparatus mounted onto a uniaxial servo-hydraulic actuator. Tests were conducted with a 100 Ib loadcell (Sensotec. Columbus OH) under displacement control, with a single ramp to failure at an average strain rate of 0.08‘KJs. The four- point bending jig included four load points spaced symmetrically about the center of the specimen. The moment arm on each side of the specimen was 38 mm and the gage length of the specimen was 46 mm. Three of the four load points were roller bearings, allowing axial deformation (which occurs during bending) without introduction of undesired axial loads. A bearing allowed the top of the test jig to rotate about an axis perpendicular to the plane of bending. thus ensuring identical loads, rather than identical displacements, at all load points. Four reflective IR-markers were placed along the neutral bending axis with 8 mm increment spacing, and a MacReflex system was used to determine the deflection curve as the specimen deformed. Instanta- neous strain at the cross-section where most of the deformation oc- curred at failure was determined by fitting a parabola to the digitized markers along the length of the specimen and taking the 1st derivative at the inflection point.
Torsior7-Torsion tests were performed using a custom built system mounted to a biaxial servo-hydraulic actuator (Interlaken, Eden Prairie MN). The testing system was designed to reduce the parasitic forces and moments associated with the out-of-plane warping of the specimen that can result from material anisotropy or specimen mis- alignment. Tests were conducted under displacement control with a single ramp to failure at an average strain rate of 0.1%1/s. The torsional load was measured with a 6-component loadcell (AMTI. Watertown MA) and was recorded synchronously with the three-dimensional positions of two reflective IR-markers. The reflective markers were symmetrically placed on either side of the defect collinear with the longitudinal axis of twist. The product of the relative angular dis- placement and the ratio of the specimen radius to the gauge length determined relative shear strain between the markers.
Srtiristicul 1?1etl70tl,~
To determine if non-invasive measures of structural rigidity predict failure of trabecular bone with or without defects, cylindrical core specimens were grouped according to mechanical testing mode, and linear regressions were applied to determine the correlations between Failure (6, M , , and T , ) vs. QCT. DXA, and MRI measurements of the corresponding minimum cross-sectional rigidities (EA, EI, and GJ). Core specimens with and without defects were included together be- cause the mechanics analysis should reflect the cross-sectional geo- metry of the core regardless of the size or shape of the core or defect, and should be irrespective of the presence of the defect. A Fisher’s z-test was used to determine if there was a statistical difference between correlation coefficients among the imaging modalities for each mech- anical test.
To determine the effect of circular holes vs. slotted defects on the failure load of the trabecular bone cores, an analysis of covariance (ANCOVA) was used with failure load as the dependent variable, hole shape as the grouping variable, and density and hole width ratio as the covariates. QCT, DXA, and MRI based measurements of rigidity were also used to test the ability of these non-invasive methods to detect the differences in the load bearing capacity of the core due to defect shape; specimens were categorized by defect shape for each test mode, and a two-tailed Student’s t-test was performed to determine
the differences between the slope of the regressions for circular and slotted defects.
To determine if the reduction in rigidity predicted the reduction in strength of trabecular specimens, a linear correlation was applied to the relationship between the reduction in the load-bearing capacity of the cylindrical core and the reduction in structural rigidity measured non-invasively. The reduction in the load carrying capacity was determined from the ratio of the measured failure load to the e.sti- rmtrcl failure load of each cylindrical core specimen before the defect was created. The estimated failure load of the “intact” specimen was calculated from the average of QCT measured structural rigidity on either side of the defect and a n empirical relationship between fail- ure load and moments and the corresponding rigidity calculated from QCT for whale bone (Tension: F, = 3626 * EA - 6.89, r2 = 0.90, p = 0.013; Bending: M , = 0.879 * El + 0.106, Y’ = 0.93, p = 0.002; Torsion: = 0.225 * GJ + 0.504. ? = 0.85, p < 0.001) [4]. The re- duction in the rigidity was determined from the ratio of the mini- mum measured rigidity for serial cross-sections through the defect to the average rigidity measured for cross-sections on either side of the defect.
Results
Minimum structural rigidity correlates tvith fuilure load
Four specimens and three in the torsion and tension groups, respectively, fractured before being tested and were eliminated. Entrained air within the marrow space introduces error in the measure of porosity by MRI; therefore, 5 MRI-bending specimens were eliminated from analysis because of entrained air artifacts. Group- ing by mechanical test mode, the linear regressions be- tween failure (4; M,; T,) , and minimum structural rigidity (EA; EI; GJ) were significantly correlated. For tension: QCT F, = 3636 * EA - 12.4, r2 = 0.951, p < 0.001, n = 32, DXA F, = 2926 * EA - 74.6, r2 = 0.926, p < 0.001, n = 32, and MRI F, = 5465 * EA- 99.3, r2 = 0.916, p < 0.001, n = 32. For four-point bending: QCT M, = 0.967 * EI + 0.133, r2 = 0.909, p < 0.001, n = 35; DXA M, = 77.1 * El - 0.038, r2 = 0.841, p < 0.001, n = 35; MRI M , = 1.89 * EI + 0.043, r2 = 0.856, p < 0.001, n = 30. For torsion: QCT T, = 0.303 * GJ + 0.018, r2 = 0.914, p < 0.001, n = 31; DXA T, = 30.7 * GJ - 0.44, r2 = 0.916, p < 0.001, n = 31;
31. There were no statistical differences in the coeffi- cients of determination (7’) among the imaging modal- ities (tension: 0.50 < p < 0.75; bending: 0.25 < p < 0.5; torsion: 0.25 < p < 0.5.
MRI T, = 2.97 * GJ - 0.514, r2 = 0.852, p < 0.001, ~2 =
Efect of circular holes us. slotted defects
There was a significant difference in mean failure loads between circular and slotted defects failed in tor- sion 0, = 0.006), which was expected theoretically, but not in tension (p = 0.219) or bending (p = 0.710). Defect shape inconsistently affected the slopes of the regressions between failure load and non-invasive measurements of structural rigidity (Table 1).

484 J. Hong et CII. I Jounzal of Orfhopuedic Re.sctrrcl1 22 (2004) 479-486
Table 1 Dependence of linear regression on shape of defect for each imaging mode
Imaging mode Mechanical test mode Aspect ratio ( L / d ) Slope r- Student's t-test on slope
QCT Tension 1 3790 0.983 11 < 0.05 3 i 3200 0.938
2 I .07 0.957
2 0.29 0.982
Bending I 1.32 0.949 11 < 0.05
Torsion I 0.37 0.92 p < 0.05
DXA Tension
Bending
Torsion
3280 0.953 p < 0.05 2690 0.934 I04 0.925 p > 0.20 99.2 0.954 29.7 0.875 p > 0.20 31.7 0.958
MRI Tension 1 6150 0.951 p < 0.05
Bending 1 2 0.918 p > 0.20
Torsion 1 2.5 0.717 p < 0.05
2 4670 0.89
- 1.72 0.538
2 3.5 0.913
7
Results for specimens with circular and slotted through-hole defects were grouped separately for each mechanical testing mode. L / d is defined as slot length ( L ) to defect width (d ) ratio: L / d = I for circular holes and L / d = 2 for slots. Bivariate linear regression was applied to the load at failure vs. minimum structural rigidity data. The effect of defect shape (slot vs. circle) on the fit relationships was assessed using paired Student's t-test for each set of slopes of the regression line corresponding to defect width.
Table 2 Coefficient of determination for linear regression for reductions in failure loads vs. reduction in rigidity for each imaging mode
QCT 0.838 0.804 0.706 DXA 0.842 0.822 0.773 MRI 0.709 0.677 0.608
Reduction in rigidity predicts the reduction in strength
The coefficients of determination for the linear regressions comparing the reduction in failure load vs. the reduction in structural rigidity caused by the defect were significant 0, < 0.001) for all imaging methods and all modes of failure (Table 2). With the exception of MRI, the reductions in axial, bending and torsional rigidity measured using QCT and DXA predicted nearly 80% of the reduction in the load bearing capacity of the trabecular core when a circular or slotted effect was present. Rigidity measured by MRI predicted 60-70'%, of the reduction in the load carrying capacity.
Discussion
The results of this study support the hypothesis that fracture of bones with lytic defects depends on the minimum cross-sectional structural properties of the
region encompassing the defect. The axial, bending, and torsional rigidities of homogeneous cores of trabecular bone with circular or slotted defects, measured non- invasively by QCT, DXA, or MRI, correlated highly with the corresponding yield loads in uniaxial ten- sion, four-point bending, and torsion, which validate the following assumptions: (1) the overall structural behavior of the trabecular core is largely governed by the weakest cross-section, (2) at a continuum level, tra- becular bone fails at a constant strain independent of bone density, and (3) at the continuum level the struc- tural behavior of trabecular bone with regularly shaped defects is minimally influenced by stress concentration factors-85-95'%1 of the variation in yield load and moment was explained by variation in minimum cross- sectional rigidity alone. As expected the length of the defect (i.e. slot vs. circular) affects the torsional rigidity of the structure, therefore affecting the magnitude of failure. The minimal cross-sectional structural rigidity accounted for at least 85% of the variation in failure load for cylindrical cores of trabecular bone, suggesting that the influence of defect shape is small relative to the overall effect of the defect on the cross-sectional prop- erties of the specimen. The reduction in cross-sectional rigidity (e.g. EAdcfeLt/EA,nt,,t) as a consequence of the lytic defect accounted for 80% of the variation in the reduction in the load carrying capacity. We model tra- becular bone as a linear elastic rigid porous foam, and Lissume the stress concentration from the defect has little effect on the overall structural behavior of the core. We ignore plastic and inelastic behavior at the margins of

the defect, and assume the remainder of the core is homogeneous in its cross-sectional structural properties. In reality the trabecular bone specimen is heterogeneous in its structural properties and theoretically failure may occur at a less rigid cross-section away from the defect instead of at the minimally rigid cross-section through the defect, if such a region existed. However, in spite of all these simplifying assumptions the ratio of the mini- mum cross-sectional rigidity through the defect com- pared to the corresponding cross-sectional properties of the intact specimen predicted the reduction in the load carrying capacity of the core well.
Radiographic criteria that rely on measuring defect size alone account for the geometry of the defect only; however, the mechanical behavior of a structure depends on both the material and geometric properties of the structure. Current imaging techniques allow measure- ment of bone density (or porosity), which determines bone material properties, and the entire bone cross- sectional geometry, so that the cross-sectional structural properties of the bone can be estimated and be used to predict fracture risk. Accounting for structural proper- ties may help explain how the compensatory effect of periosteal expansion and sclerotic margination that oc- curs as an adaptive response to slow growing, benign, lytic bone tumors in children never cause fracture even through the defect size exceeds current radiographic guidelines for increased fracture risk. A potential limi- tation of this technique is that i t assumes that pathologic bone follows the same power law relationship between apparent bone density and modulus as derived for nor- mal bone [24]. While this may be valid for osteoporotic bone, it remains unclear whether this relationship holds for pathologic bone conditions such as metastatic car- cinoma, osteomalacia, and benign bone tumors such as fibrous dysplasia. To this aim, we have recently com- pleted a study demonstrating that bone containing metastatic carcinoma with Iytic, blastic, and mixed le- sions follows the same power law relationship between apparent bone density and modulus as measured for normal and osteoporotic bone [22].
Another potential limitation of the study is that the precise nature of loading in bones is often unknown. Due to the location of muscle origins and insertions and ground reaction forces, bending may not occur about the minimum principal axis of the bone. However, estimating failure about the minimum axis represents an extreme case, and is a conservative assumption that al- lows some uniformity when comparing cross-sectional structural properties of bones, Furthermore, composite beam theory allows for the superposition of multiple modes of loading, and the stress (or strain) at a partic- ular cross-section through the bone can be calculated for simple two-dimensional multiaxial load states. Nor- malizing the cross-sectional structural rigidity of the affected bone through the defect by the cross-sectional
structural rigidity of the unaffected contralateral bone at the homologous region should mollify this potential problem in clinical applications since the ratio of de- fected to intact bone core structural rigidity correlated highly with the reduction in the core containing the defect.
The differences in the slopes of the linear regressions between yield load and minimum cross-sectional rigid- ity calculated using QCT or MRI data are due to the inherent differences between the direct and indirect measurements of bone density using QCT and MRI, respectively. Our MRI technique assumes that the tissue density of whale bone remains constant and that varia- tions in apparent bone density essentially reflect changes in bone morphology represented by variations in the volume fraction of bone. For the range of specimens and bone defect geometries investigated, the variation in bone tissue density did not preclude the use of MRI for deriving cross-sectional structural properties. However the moduli calculated using MRI-based density mea- surements were consistently higher than QCT-based density measurements, and therefore affected the slopes of the linear regression while the coefficients of variation remained high. Any disease state, such as osteomalacia, where the mineralization of the bone tissue is affected would preclude the use of MRI since the bone tissue density would be abnormal and inhomogeneous.
It is not possible to directly measure cross-sectional geometry of trabecular bone with the DXA algorithm used in this study; however, the second moment of the cross-sectional BMD profile provided a parameter anal- ogous to a modulus weighted moment of inertia, which highly correlated with the corresponding yield loads and moments for all test modes. The low ionizing radiation, relatively inexpensive cost, and increasing availability for osteoporosis diagnosis make DXA an attractive tool for serially evaluating patients. Applying the algorithm presented here, DXA and can potentially be used to predict the load carrying capacity of bones affected by benign or metastatic tumors.
In this study, there were no significant differences among the predictive capabilities of the three imaging modalities examined. The ultimate choice clinically will be a function of accuracy, cost, radiation exposure and accessibility. However, when extensive remodeling of cortical and trabecular bone by a neoplastic process significantly influences cross-sectional structural rigidity, only QCT will be able to discriminate changes in both the cortical and trabecular bone. Because DXA inte- grates across cortical and trabecular bone regions, it is unable to distinguish changes in trabecular and/or cor- tical bone cross-sectional geometry and actual apparent density that may affect the structural properties. There- fore, even though DXA is cheaper and exposes the pa- tient to less radiation, and MRI is non-irradiating, QCT may still be the most useful modality.

486 J . Hung r f crl. I Joirrnal of Ortlzopedic Rewurch 22 (2004) 479-486
This study examined the feasibility of applying mechanics of materials principles to predict failure of axisymmetric cores of homogeneous trabecular bone with regularly shaped defects. It does not necessarily imply that these algorithms will be valid for irregularly shaped defects in whole bones that are heterogeneous in both their material composition and structural organi- zation. However, we have successfully demonstrated the validity of these methods to predict failure loads of thoracic and lumbar vertebrae with irregularly shaped lytic defects that simulated common clinical cases of combined axial compression and forward flexion [28]. Currently we are evaluating these algorithms in vivo to predict fracture risk in the appendicular skeleton with benign bone tumors [25] and the spine from women with metastatic breast cancer [I].
Acknowledgements
We wish to thank the Whitaker Foundation (Grant 96-0208) and the NIH (NIH CA 40211) for their sup- port. Part of this paper was presented at ORS 1998 New Orleans.
References
[I] Aaron M, Snyder BD. Wilson S, et al. Non-invasive prediction of fracture risk in patients with metastatic breast cancer to the spine. Transactions of the 48th Orthopaedic Research Society 2002; Poster # 745.
[2] Blake GM, Wanner HW, Fogelman 1. The evaluation of osteo- porosis: dual energy X-ray absorptiometry and ultrasound in clinical practice. London: Blackwell Science, Inc.; 1999.
[3] Body J. Metastatic bone disease: clinical and therapeutic aspects. Bone 1992;13:S52-7.
[4] Cabe GD. Non-invasive measurement of load capacity of trabec- ular bones with defects. Cambridge: Department of Mechanical Engineering, Massachusetts Institute of Technology; 1997.
[5] Carter DR, Hayes WC. The compressive behavior of bone as a two-phase porous structure. J Bone Joint Surg [Am] 1977;59A: 954-62.
[6] Chang WC, Christensen TM, Pinilla TP, Keaveny TM. Uniaxial yield strains for bovine trabecular bone are isotropic and asymmetric. J Orthop Res 1999; 17582-5.
[7] Copley L, Dormans JP. Benign pediatric bone tumors: evaluation and treatment. Pediatr Clin North Am 1996;43:949-66.
[S] Fidler M. Prophylactic internal fixation of secondary neoplastic deposits in long bones. Br Med J 1973;10:341-3.
[9] Ford CM, Keaveny TM. The dependence of shear failure properties of trabecular bone on apparent density and trabecular orientation. J Biomech 1996;29:1309-17.
[lo] Gartland JJ, Cole FL. Modern concepts in the treatment of unicameral bone cysts of the proximal humerus. Orthop Clin North Am 1975;6:487-98.
[ I I ] Gibson LJ, Ashby MF. Cellular solids structures and properties. Cambridge: Cambridge Press; 1997.
[l2] Hipp JA, Springfiled DS, Hayes WC. Predicting pathologic fracture risk in the maimgenient of metastatic bone defects. Clin Orthop 1995;312:120-35.
[I31 Hong J, Hipp JA, Mulkern RV, et al. Magnetic resonance imaging measurements of bone density and cross-sectional geometry. Calcified Tissue Int 2000;66:74 8.
[I41 Houston SJ, Rubens RD. The systemic treatment of bone metastases. Clin Orthop 199S;3 I2:9S-104.
[I51 Inoue 0, Ibaraki K, Shimabukuro H, Shingaki Y. Packing with high-porosity hydroxyapatite cubes alone for the treatment of simple bone cyst. Clin Orthop 1993;293:287-92.
[I61 Keene J, Sellinger D, McBeath A, et al. Metastatic breast cancer in the femur a search for the lesion at risk of fracture. Clin Orthop Re1 Res 1986;203:282-8.
[17] Keller TS. Predicting the compressive mechanical behavior of bone. J Biomech 199427:1159-68.
[I81 Kopperdahl D, Keaveny TM. Yield strain behavior of trabecular bone. J Biomech 1998;11(7):601-8.
[19] Martin RB, Burr DB. Noninvasive measurement of long bone cross-sectional moment of inertia by photon absorptiometry. J Biomech 1984; 17: 195-201.
[20] Mirels H. Metastatic disease in long bones. Clin Orthop Re1 Res 1989;206:25&64.
[21] Mulkern RV, Meng J, Bowers JL. In vivo bone marrow lipid characterization with line scan Carr-Purcell-Meiboom-Gill proton spectroscopic imaging. Magn Reson Imaging 1997:15: 823-37.
[22] Nazarian A, von Stechow D, Cordio MS, et al. Analytical model to predict mechanical behavior of skeletal metastasis. J Bone Miner Res 2002;17(SI):S416.
[23] Neer CS, Francis KC, Johnston AD, Kieman Jr H. Current concepts on the treatment of solitary unicameral bone cysts. Clin Orthop 1973;97:40-5 I ,
[24] Rho JY, Hobatho MC, Ashman RB. Relations of mechanical properties to density and C T numbers in human bone. Med Eng Phys 1995;17:347-55.
[25] Snyder BD, Hecht AC, Tedrow JR, et al. Structural rigidity measured by C T accurately predicts fracture in children with benign tumors of the appendicular skeleton. Transactions of the 46th Orthopaedic Research Society 2000;25:243.
[26] Turner CH. Yield behavior of bovine cancellous bone. J Biomech Eng 1989;111(3):256-60.
[27] Walls J, Bundred N, Howell A. Hyperclacemia and bone resorption in malignancy. Clin Orthop 1995;312:SI 63.
[28] Whealen K, Kwak S, Tedrow J, et al. Non-invasive imaging predicts failure loads of spine defects. J Bone J Surg 2000;82(9): 1240-5 1 ,