Embed Size (px)
Citation preview

CREATIVE SOLUTIONS IN THE ERDr. Peter Viccellio addresses how economizing patient admissions and boarding can prevent overcrowding
eMerGenCY MeDICIne
Emergency care – close & fast .www.hollywoodpresbyterian.com | 213.413.3000
August 2011
PHOTO: SUNY AT STONY BROOK
an Independent advertIsIng supplement by medIaplanet to los angeles tImes
overcoming obstaclesturning tragedy into triumph
Careers in ersaving lives and helping others
addresses how economizing patient admissions and boarding can prevent overcrowding
eMerGenCY MeDICIne
addresses how economizing patient admissions and
eMerGenCY MeDICIne
ABOUT THE ER
eMerGenCY MeDICIneeMerGenCY MeDICIneeMerGenCY MeDICIne
ABOUT THE ER
3FACTS

2 · august 2011 an Independent advertIsIng supplement by medIaplanet to los angeles tImes
CHallenGesEvery day when I go to work as an emergency room physician, I see fi rsthand California’s health care safety net being stretched to its limit.
the state of emergency medicine
Ca l i f o r n i a ’ s e m e r g e n c y rooms are an essential pub-lic service that each of us relies on to be there
for our health crises 24 hours a day, 365 days a year. And yet, ERs face numerous challenges that threaten to undermine safe and timely care.
Emergency room crowdingCrowding is one of the biggest prob-lems ERs face today and the situation is only getting worse. Today, there are fewer ERs and hospital beds but more patient visits, resulting in a system that is stretched beyond capacity. Crowded ERs mean delayed care for people in waiting rooms and treatment in ER hallways. Crowded ERs mean ambulances can’t stop at the closest ER and instead must drive to the next one. Patients with serious conditions wait longer to see a doctor, and this impacts everyone. Numerous studies report that ER crowding causes poor health out-comes and each day emergency phy-
sicians witness delayed care putting lives in jeopardy.
The front door:Who is using the ERsUse of ERs continues to increase at twice the rate of population growth, but it is a myth that patients are flooding ERs with runny noses and minor illnesses. On the con-trary, a CDC study found that only eight percent of ER patients are considered “non-urgent,” which does not mean unnecessary. Most ER patients are experiencing true emergencies and are in the right place. The reality is, people who have chronic diseases like diabetes but can’t get in to see a doctor—even when they are insured—wind up in an ER with a medical crisis that was once a preventable problem.
The back door: Hospital crowdingWhile the front door brings an increasing number of patients with serious conditions, the major cause of ER crowding is hospital crowd-ing. Day and night, the hallways of
many ERs are lined with patients who no longer need emergency care. They wait uncomfortably and without any privacy for hours and sometimes days for a vacant hos-pital bed. This problem of “board-ing” can only be solved by focusing on the whole hospital, not just the ER. Every hospital must develop an ER crowding plan, or full-capacity protocol, outlining how all parts of the hospital will react as the ER gets more and more crowded. Hos-pitals are required to have disaster plans for uncommon events, such as major earthquakes and fl oods, but most lack a formal plan for the everyday disaster of ER crowding.
Keeping the promiseCalifornia ACEP has always been fi rst and foremost about patient safety. Seeking solutions that allow patients to receive the safest, most eff ective care under critical condi-tions remains emergency physi-cians’ primary goal.
PeterSokolove, MDpresident, California Chapter of the american College of emergency physicians
mediaplanet’s business is to create new customers for our advertisers by providing readers with high-quality editorial content that motivates them to act.
PETER SOKOLOVE, MD
(818) 409-8100Where the 2 and 134 freeways meetGlendaleAdvent ist .com
The ONLYCertifi ed Chest Pain Center andCertifi ed Primary Stroke Center
in all of Los Angeles County!
FOLLOW US ON FACEBOOK & TWITTER! www.facebook.com/MediaplanetUSAwww.twitter.com/MediaplanetUSA
“Hospitals are required to have disaster plans for uncommon events, such as major earthquakes and fl oods, but most lack a formal plan for the everyday disaster of er crowding.”
Sandra Palaciosbe inspired by her compelling story of survival.
WE RECOMMEND
page 5
EVERY 4 SECONDS, A CALIFORNIAN
ENTERS AN ER TO SEEK TREATMENT
an Independent advertIsIng supplement by medIaplanet to los angeles tImes
EVERY 4 SECONDS,
1FACT
EMERGENCY MEDICINE,1ST EDITION, AUGUST 2011
Publisher: Mariah [email protected] Developer: Elba Flamencoelba.fl [email protected] Designer and Sub-editor: Missy [email protected] Director: Allan [email protected]
Contributors: American College of Emergency Physicians, California Hospital Association, Cindy Riley, Jill Coody Smits
Distributed within: Los Angeles Times, August 2011This section was created by Mediaplanet and did not involve the Los Angeles Times or its Editorial Departments. Dedication: John, Mary, Drew, Jack and Doggies
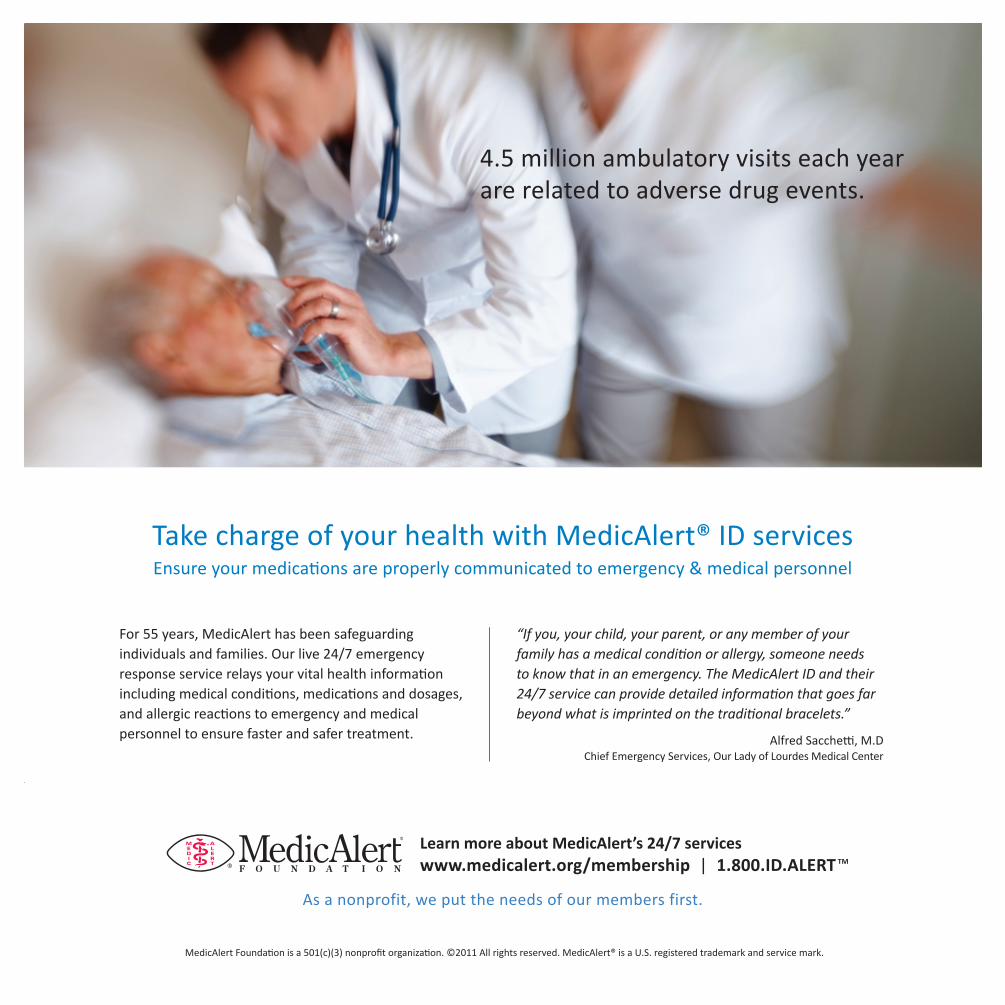
Take charge of your health with MedicAlert® ID servicesEnsure your medications are properly communicated to emergency & medical personnel
4.5 million ambulatory visits each year are related to adverse drug events.
MedicAlert Foundation is a 501(c)(3) nonprofit organization. ©2011 All rights reserved. MedicAlert® is a U.S. registered trademark and service mark.
Learn more about MedicAlert’s 24/7 services www.medicalert.org/membership | 1.800.ID.ALERT TM
For 55 years, MedicAlert has been safeguarding individuals and families. Our live 24/7 emergency response service relays your vital health information including medical conditions, medications and dosages, and allergic reactions to emergency and medical personnel to ensure faster and safer treatment.
As a nonprofit, we put the needs of our members first.
“If you, your child, your parent, or any member of your family has a medical condition or allergy, someone needs to know that in an emergency. The MedicAlert ID and their 24/7 service can provide detailed information that goes far beyond what is imprinted on the traditional bracelets.”
Alfred Sacchetti, M.DChief Emergency Services, Our Lady of Lourdes Medical Center

4 · august 2011 an Independent advertIsIng supplement by medIaplanet to los angeles tImes
InsIGHtPeter Viccellio, M.D., had finally had enough. Overwhelmed by the number of seriously ill patients being treated in the hallways of his hospital’s overcrowded emergency department—a practice known as boarding—he knew something had to give.
reducing er boarding to decrease mortality
a clinical professor and the vice chairman of the department of emergency medicine at the State University of New York at Stony Brook, Dr. Viccellio
telephoned a contact at the local health department, wanting to know why placing people in an upstairs hallway, instead of in the emergency department, violated health codes. It turns out, that simply wasn’t true. After further investigation, he devised a plan in 2001 that has sharply reduced the boarding problem and has been imple-mented at numerous facilities nationwide.
Why has emergency depart-ment overcrowding continued to be such a problem?
We’re trying to fi t a seven-day-a-week problem into a fi ve-day-a-week solution. Crowding is the
direct result. The fi rst question is whether the ED has the resources to provide appropriate care, and uses these resources judiciously. As for institutional crowding, hospitals can dramatically improve capacity simply by ‘smoothing’ elective admissions and discharges. This can be accomplished at no cost whatsoever.
When there are more admissions than beds, the worst solution is to leave all these patients in the ED. At least some should be distributed to the inpatient units, even if it means placing them in a hallway. The care is better, the staffi ng ratios are better, patients prefer it to being in an ED hallway, and studies have shown the total length of stay will be reduced by almost a full day.
How frustrating is the issue of boarding?
The fi rst article I ever wrote on this was in 1987. Some 23 years later, the problem is the same
as it was then. Terrible. What is diff er-ent is there are solutions which are now known to work, which benefit the patient, the doctor, and the institution, and yet there is a failure to implement these solutions. This, to me, represents a casual disregard for the safety of our patients.
Why has it taken so long for hospitals to see the light regarding this matter?
Although there has been recent data highlighting the profi t-ability of emergency admis-
sions, emergency patients have been historically and prejudicially viewed as less fi nancially desirable patients. I think this is factually in error, but, nonetheless, this has contributed to the systematic and almost studied disin-terest in fi xing this problem. In addi-tion, sadly, old habits die hard, and
institutions do need to change pro-cesses in order to improve capacity.
What else should readers be aware of regarding overcrowding?
The work done on smoothing of fl ow suggests that we might not actually have a capacity
issue, if we were only willing to change in a way which makes our work easier. Studies show crowding causes a signifi -cant increase in mortality. Also, in most EDs, lack of insurance, illegal immi-grants, and ED ‘abusers’ are quite explicitly not the cause of ED crowding. They simply provide a prejudicial tar-get for a frustrating problem.
CINDY RILEY
“When there are more admissions than beds, the worst solution is to leave all these patients in the ed.” Peter Viccellio, MD, FACEPClinical professor & vice Chairman, Clinical director emergency department
THE AVERAGE WAIT TIME IN A CALIFORNIA ER IS NOW MORE THAN 4 HOURS
an Independent advertIsIng supplement by medIaplanet to los angeles tImes
THE AVERAGE
2FACT

august 2011 · 5an Independent advertIsIng supplement by medIaplanet to los angeles tImes
■ Question: How does a determined young woman turn tragedy into triumph?■ Answer: by inspiring other trauma victims with her compelling story of survival.
For Sandra Palacios, the night of September 9, 2007 remains noth-ing but a blur. While returning home from an evening out with friends, the intoxicated driver of their vehicle lost control, eject-ing Sandra from the backseat and throwing her out the rear window.
“I landed on the concrete cen-ter divider of the 110 freeway,” explains, Sandra, now 24. “I was rushed to the hospital and had
immediate surgery. My critical condition left the doctors and my family unsure of my life being saved because I fell into a coma.”
Not knowing how bad it wasShe awakened four days later, but didn’t speak or open her eyes for two weeks.
“I didn’t recognize my own mother and sisters. My face was badly injured, and the doctors said I could lose my eye. I didn’t know how bad it was. I looked and saw my leg missing below the knee. It didn’t seem real. More like a nightmare.”
“I was in constant emotional and physical pain. My right leg was gone, my other leg was deformed
and large parts of my body would forever be covered in scars. I cried until I couldn’t anymore. I had been attending California State University, Los Angeles and I was six classes away from obtaining my bachelor’s degree in Child Devel-opment Youth Administration. I was very determined to go back to school, even in a wheelchair. It was extremely important for me to feel independent and look beyond my disability.”
Support and careSandra credits her sister, Imelda, and other family members for provid-ing a positive support system. Her spirituality also played a role in her
recovery. Sandra felt blessed to be at a hospital where everyone treated her like family and gave her the sup-port and care she needed to recover.
California Hospital Medical Cen-ter’s Chief of Trauma and General Surgery, Gudata Hinika, M.D. says, “Sandee showed such strength and determination during her recovery. She is such an inspiration to others by refusing to make excuses, and even graduating with honors.”
“It’s a daily challenge,” adds San-dra, who hopes to earn a Masters in Social Work. “But I try to keep going for my family, and because I want more.”
InspIratIon
.e J..omas McCarthy Center for Emergency Services at California Hospitalis the only full service, 24 hour emergency department in Downtown Los Angeles.�............�.......................................�......................................�..............�..................................�.............�................�....��.........................�........................�..................�.................�...........�.....�.............
�is level II facility provides a full range of medical procedures 24 hours a day, 7 days a week.......................................................................................................................................................................................................................................................
TIPS
Tips to help your loved one in the ER
1 Write down all the patient’s medications or put them in
a resealable bag and bring them with you. And don’t forget to include over-the-counter pills and any herbal medications.
2 If English isn’t the patient’s native language, bring an
adult translator. Often, people recruit school-aged children to translate, but medical proce-dures can be too complicated or inappropriate for them to talk about. The ER staff can call a translation service in a pinch. But things will go much more smoothly if a bilingual adult is available.
3 Don’t leave the emergency department without writ-
ten instructions. And don’t be afraid to ask questions and have the doctor clarify all aspects of the patient’s condition and fol-low up care. Carefully follow the aftercare instructions, including any additional doctor or special-ist appointments.
AMERICAN COLLEGE OF EMERGENCY PHYSICIANS
looking beyond tragedy
POSITIVE SUPPORTLEFT: Sandra and her dog ‘Lady’ who serves as a great support system for her.RIGHT: Sandra waiting to get her diploma from California State University, Los Angeles.PHOTO: COURTESY OF THE FAMILY
CINDY RILEY
InsIGHt
3
6 · august 2011 an Independent advertIsIng supplement by medIaplanet to los angeles tImes
Life is 24/7/365.So are we.
661.253.8000henrymayo.com
Welcome to Henry Mayo’s all-new Emergency Department In your most critical time, excellence is close at hand. 100% of our ER doctors are board-certified in emergency medicine, and, as a Level II Trauma Center, physician specialists are available 24/7/365. Combined with expanded facilities, state-of-the-art equipment, and an Emergency Department Approved for Pediatrics designation, we’re ready to exceed your expectations. Visit henrymayo.com to learn more.
HM Emergency Ad_final.indd 1 7/28/11 2:38 PM
neWs
■ Question: California’s hospital emergency rooms are there 24/7, when you and your family need them most. now, they face challenges that you should know about. since we’re all in this together, what are some ways we can all help?■ Answer: the California Hospital association currently has a protectmyer public advocacy campaign active to help our emergency departments receive the funding and attention they deserve.
Hospitals are working hard every day to keep emergency and other impor-tant health care services available to you and your family. Here’s how you can help protect those services today, tomorrow, and into the future.
Patients & hospital leadersConsumers and patients can help reduce ER overcrowding and wait times by using primary care physicians and clinic services for non-emergency health care needs. While continuing to provide high quality health care services to those in need, hospitals need to continue to look for ways to more eff ectively manage rising health care costs.
Community leaders & policymakersWorking with local health care organizations, community leaders can help fi nd cost-eff ective, inno-vative health care solutions that serve their communities and help address the needs of the growing uninsured population. Policy-
makers are urged to fund Medi-Cal at the highest level available under federal law and ensure that health care programs and services designed for California’s most vul-nerable citizens are not cut further. More Californians must not be put at risk.
Proactive public education & other critical issuesCHA’s Public Advocacy Program works to inform and educate the public about key financial and other critical issues impacting California’s community hospitals and emergency rooms. In 2010, hospitals provided $12.5 billion of uncompensated care, stem-ming mostly from the underfund-ing of government programs like Medi-Cal and Medicare. Today,
more than 50 percent of California’s community hospitals operate in the red. Counties across California are also struggling with fi nancial shortfalls —laying off hundreds of public health and mental health workers and shutting down com-munity health care programs. This is putting a further strain on Cali-fornia’s hospitals and emergency rooms as they care for these addi-tional patients who have no place else to go.
ers need your help
THE CALIFORNIA HOSPITAL ASSOCIATION
Become an advocate■ California hospitals & ERs are on the front lines of care, seeing more & more patients who have no place else to go. During the past decade, more than 70 hospitals & ERs have closed in California due to increasing fi nancial & other pres-sures. Become an advocate & sign up now at www.ProtectMyER.com to help California’s commu-nity hospitals & ERs become pro-tected—so that they will continue to be there for you & your family when you need them most. Hos-pitals can help advocate by cross-linking their hospital website to www.ProtectMyER.com.
THE CALIFORNIA HOSPITAL ASSOCIATION
1 MILLION CALIFORNIANS RECEIVED LIFE-SAVING CARE
IN ONE OF CALIFORNIA’S ERS
IN 2009
an Independent advertIsIng supplement by medIaplanet to los angeles tImes
1 MILLION
3FACT
HOW TO GET INVOLVED

august 2011 · 7an Independent advertIsIng supplement by medIaplanet to los angeles tImes
more than 50 percent of California’s community hospitals operate in the red. Counties across California are also struggling with financial shortfalls —laying off hundreds of public health and mental health workers and shutting down com-munity health care programs. This is putting a further strain on Cali-fornia’s hospitals and emergency rooms as they care for these addi-tional patients who have no place else to go.
panel of experts
When I became an EMT, I thought life would be like televi-sion: hip-deep in blood, gore and CPR. I touch lives every day in EMS, but the how is about the little moments: a hand held in comfort, a soothing voice in a crisis, another blanket on a cold night.
Question 1:What is the number one misconception about careers in Emergency Medicine? What is the reality?
Katie ThompsonEMT/Teaching Assistant, College of the Canyons
Marcus Godfrey, RNPresident-Elect, California Council, Emergency Nurses Association
Andrew Fenton, MD, FACEPPresident-Elect California ACEP
Marc Futernick, MD, FACEPMedical Director, Emergency Services, California Hospital Medical Center
That it isn’t a customer service oriented career, when of course it is. Patients recover faster and have better outcomes when they believe they are cared about and not just cared for. Many get into emergency medicine for the adrenaline rush, when really only 10 percent of patients are truly in a life threaten-ing crisis
Some believe we take care of trauma patients like on television while others feel we see mostly folks with minor illness. In reality, we see everyone with injuries or ill-ness from head to toe, some more serious than others. A lot of time is spent at the bedside listening and educating patients. That doesn’t always make it on television.
The most common misconcep-tion about Emergency Physicians is that we have private practices outside of the Emergency Depart-ment. We do not. We are specialists in Emergency Medicine. We work full time caring for people suffer-ing acute conditions. Our expertise is in the immediate management of serious illness and injury.
Nothing is more rewarding than the essence of my job: being a first responder. Walking into somebody’s worst day or biggest crisis and starting to restore order and sanity to the chaos around you is the greatest feeling in the world. Best of all, this happens every day I work.
Question 2:What is the most rewarding part of having a career in Emergency Medicine?
The everyday ability to make a difference in people’s lives. Some-times the outcome for the patient is poor and the family becomes your patient. Taking time to explain to them what’s next can make the dif-ference between the worst day of their lives and a beautiful moment of compassion.
My interaction with patients. Being able to hear their stories and share time with them is a true priv-ilege. Most importantly, I have the ability to help them in crisis when they are in true need. It is a very ful-filling profession.
The most rewarding part of Emergency Medicine is saving lives. Working in a busy trauma center, I save lives on a daily basis. We also relieve acute pain and suf-fering. For example, it’s very grati-fying to reduce a dislocated joint, bringing instant relief. I feel privi-leged to have this opportunity.