Embed Size (px)
Citation preview

http://ajs.sagepub.com/Medicine
The American Journal of Sports
http://ajs.sagepub.com/content/41/12/2759The online version of this article can be found at:
DOI: 10.1177/0363546513503448
2013 41: 2759 originally published online September 17, 2013Am J Sports MedMelissa A. Kluczynski, John M. Marzo and Leslie J. Bisson
Cruciate Ligament Reconstruction: A Prospective StudyFactors Associated With Meniscal Tears and Chondral Lesions in Patients Undergoing Anterior
Published by:
http://www.sagepublications.com
On behalf of:
American Orthopaedic Society for Sports Medicine
can be found at:The American Journal of Sports MedicineAdditional services and information for
http://ajs.sagepub.com/cgi/alertsEmail Alerts:
http://ajs.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
What is This?
- Sep 17, 2013OnlineFirst Version of Record
- Nov 27, 2013Version of Record >>
at St Petersburg State University on January 13, 2014ajs.sagepub.comDownloaded from at St Petersburg State University on January 13, 2014ajs.sagepub.comDownloaded from

Factors Associated With MeniscalTears and Chondral Lesionsin Patients Undergoing AnteriorCruciate Ligament Reconstruction
A Prospective Study
Melissa A. Kluczynski,* MS, John M. Marzo,y MD, and Leslie J. Bisson,*z MDInvestigation performed at the University at Buffalo, The State University of New York,Buffalo, New York
Background: Increased time from anterior cruciate ligament (ACL) injury to surgery is known to be associated with increasedmedial meniscal tears. Few studies have examined the predictors of meniscal tears and chondral lesions, including instabilityepisodes.
Purpose: To examine the predictors of meniscal tears and chondral injuries in patients undergoing ACL reconstruction.
Study Design: Case-control study; Level of evidence, 3.
Methods: Data were collected prospectively from 541 patients undergoing ACL reconstruction. Logistic regression was used tocalculate adjusted odds ratios and 95% confidence intervals for predictors of meniscal tears, tear management, and chondralinjuries. Predictors included age, sex, body mass index (25-29.99 and �30 vs �24.99 kg/m2), mechanism (contact vs noncontact)and type (high-impact sports [basketball, football, soccer, and skiing] and other sports vs not sports related) of injury, interval frominjury to surgery (�6 vs .6 weeks and �12 vs .12 weeks), and instability episodes (vs none).
Results: A total of 211 lateral meniscal tears (35.3% untreated, 48.3% meniscectomized, 16.4% repaired), 197 medial meniscaltears (25% untreated, 52% meniscectomized, 23% repaired), and 82 chondral injuries occurred. Age predicted chondral injuries.Male sex predicted more lateral meniscal tears overall, untreated lateral tears, and lateral meniscectomies as well as predictingmedial meniscal tears overall and medial meniscectomies. Obesity predicted more chondral injuries. Sports-related injuries pre-dicted fewer medial meniscal tears overall and medial meniscectomies. Injuries �6 weeks from surgery predicted more lateralmeniscal repairs but fewer medial meniscectomies. Injuries �12 weeks from surgery predicted more chondral injuries. More insta-bility episodes predicted medial meniscal tears overall, untreated medial tears, medial meniscectomies, and medial repairs.
Conclusion: Male sex predicted lateral meniscal tears and management. Male sex, sports, injuries �6 weeks from surgery, andpreoperative episodes of instability predicted medial meniscal tears and management. Age predicted chondral injuries. This wasone of the first studies to examine the number of instability episodes as a predictor of an intra-articular injury.
Keywords: knee; ligament; ACL; meniscus; chondral
Intra-articular injuries are commonly found in anteriorcruciate ligament (ACL)–injured patients. Approximatelyhalf of all ACL-injured patients have lateral or medialmeniscal tears,2,18,22 and 16% to 46% have chondral inju-ries.4 It has been shown that delaying ACL reconstructionbeyond 6 months of injury increases the risk of medialmeniscal tears.1 Concomitant injuries have been shownto be associated with a higher prevalence of developingosteoarthritis compared with isolated ACL injuries.14
Obtaining a better understanding of the associationbetween these injuries might influence prevention andtreatment strategies. Few studies have examined risk fac-tors of intra-articular injuries in the presence of ACL tears.
zAddress correspondence to Leslie J. Bisson, MD, University atBuffalo, The State University of New York, 4949 Harlem Road, Amherst,NY 14226 (e-mail: [email protected]).
*University at Buffalo, The State University of New York, Amherst,New York.
yUniversity at Buffalo, The State University of New York, Buffalo, NewYork.
One or more of the authors has declared the following potential con-flict of interest or source of funding: This study was funded by a grantfrom the Ralph C. Wilson Foundation.
The American Journal of Sports Medicine, Vol. 41, No. 12DOI: 10.1177/0363546513503448� 2013 The Author(s)
2759 at St Petersburg State University on January 13, 2014ajs.sagepub.comDownloaded from

In one study, Bowers et al3 found that greater body massindex (BMI) and age were predictive of chondral lesionsamong patients undergoing ACL reconstruction.
One objective of this study was to identify the predictorsof intra-articular injuries in patients undergoing ACLreconstruction. The second objective of this study was toexamine the predictors of meniscal tear management (ie,meniscectomy, meniscal repair, or meniscal tear leftuntreated). Our hypothesis was that 1 or more of these pre-dictors would be associated with intra-articular injuriesand meniscal tear management.
MATERIALS AND METHODS
A prospective study of the association between demo-graphic and historical factors and intra-articular injurieswas initiated in 2005, and institutional review boardapproval was obtained. Between 2005 and 2011, therewere 651 consecutive ACL reconstructions performed atour institution by 2 fellowship-trained orthopaedic sur-geons. Fourteen patients had bilateral ACL tears, fromwhich 1 knee was randomly selected for inclusion. Of thesepatients, 96 were excluded because of previous surgery onthe affected knee or the occurrence of grade 2 or 3 medialcollateral ligament, lateral collateral ligament, or posteriorcruciate ligament tears in addition to the ACL tear. Thus,541 patients were included in this prospective case series.
Age at injury, sex, BMI, history of surgery, mechanismand type of injury, and number of instability episodes weredocumented on standard forms preoperatively by the sur-geon. Body mass index was categorized as normal(�24.99 kg/m2), overweight (25-29.99 kg/m2), and obese(�30 kg/m2) in accordance with the World Health Organi-zation.20 Type of injury was categorized as involving high-impact sports (basketball, football, soccer, and skiing),other sports, and not sports related or of unknown origin.Because the interval from injury to surgery was skewed,the interval was categorized as (1) �6 weeks and .6 weeksfrom injury to surgery and (2) �12 weeks and .12 weeksfrom injury to surgery. The presence and characteristicsof meniscal tears and chondral injuries observed duringarthroscopic surgery were documented by the surgeonimmediately after surgery. Management of lateral andmedial meniscal tears was categorized as a meniscal tearnot requiring treatment, meniscectomy performed, ormeniscal repair performed. Stable longitudinal tears ofthe lateral meniscus posterior to the popliteal hiatuswere left in situ, as were small (\1 cm), incomplete, andstable tears of the medial meniscus. Technically repairabletears in the vascular zones (ie, red-red, red-white) wererepaired. Tears not meeting these criteria were treatedwith partial resection.
Statistical Analysis
Descriptive statistics were calculated for demographic fac-tors and arthroscopic findings. The mean number of insta-bility episodes was stratified by meniscal injury andcompared with t tests. Next, we examined the predictors
of lateral and medial meniscal tears as well as chondralinjuries. We also examined the predictors of the manage-ment of lateral and medial meniscal tears. Each categoryof meniscal tear management was compared with patientswho did not have a meniscal tear (ie, the referent group).
Predictor variables included the following: age at injury(years); sex (female patients as referent group); BMI (nor-mal [referent group], overweight, and obese); mechanismof injury (noncontact [referent group] and contact); typeof injury (high-impact sports related, other sports related,and not sports related or of unknown origin [referentgroup]); time from ACL injury to surgery (.6 or .12 weeksas referent group); and number of instability episodesbefore surgery (0 episodes as the referent group). Predic-tors of chondral and meniscal injuries were tested withmultivariate logistic regression for binary outcomes. Pre-dictors of meniscal tear management were tested withmultivariate polytomous logistic regression, which allowsfor outcomes with more than 2 categories.17 Two differentintervals from injury to surgery were examined, and thus,2 logistic regression models were built for each outcome. Inmodel 1, �6 weeks versus .6 weeks from injury to surgerywas examined as a predictor, and in model 2, �12 weeksversus .12 weeks from injury to surgery was examinedas a predictor. All other predictors (listed above) were iden-tical in models 1 and 2. Adjusted odds ratios (ORs) and 95%confidence intervals (CIs) were calculated for each predic-tor variable. The number of instability episodes was alsomodeled as a continuous variable to test for linear trend.Patients were excluded from regression analysis if theirmechanism of injury was unknown or dropped from theanalysis if predictor data were missing (see Table 1 formissing data). Results were considered to be statisticallysignificant when the null value (1.00) was absent fromthe CI or P \ .05. Statistical analyses were performedwith SAS 9.3 (SAS Institute Inc, Cary, North Carolina).
RESULTS
Sample characteristics are presented in Table 1. Patientsranged in age from 7 to 62 years (mean, 25.9 years). Mostpatients were male (57.7%), had a BMI �24.99 kg/m2
(52.0%), had a noncontact injury (69.5%), and had a high-impact sports–related injury (57.3%). About 30% of patientshad surgery within 6 weeks of injury, and approximately35% had surgery within 12 weeks of injury. About 60% ofpatients reported at least 1 instability episode before sur-gery. The number of instability episodes stratified by menis-cal injury is shown in Table 2. Patients with a medialmeniscal tear had significantly more instability episodesthan those without a medial meniscal tear (P = .0001). How-ever, the number of instability episodes did not differ signif-icantly for patients with and without a lateral meniscal tear(P = .29).
Arthroscopic findings are presented in Table 3. A lateralmeniscal tear was found arthroscopically in 211 patients, ofwhich the anterior horn was involved in 2.8%, the middleone third in 33.2%, and the posterior horn in 77.7%. Man-agement of lateral meniscal injuries included the following:
2760 Kluczynski et al The American Journal of Sports Medicine
at St Petersburg State University on January 13, 2014ajs.sagepub.comDownloaded from
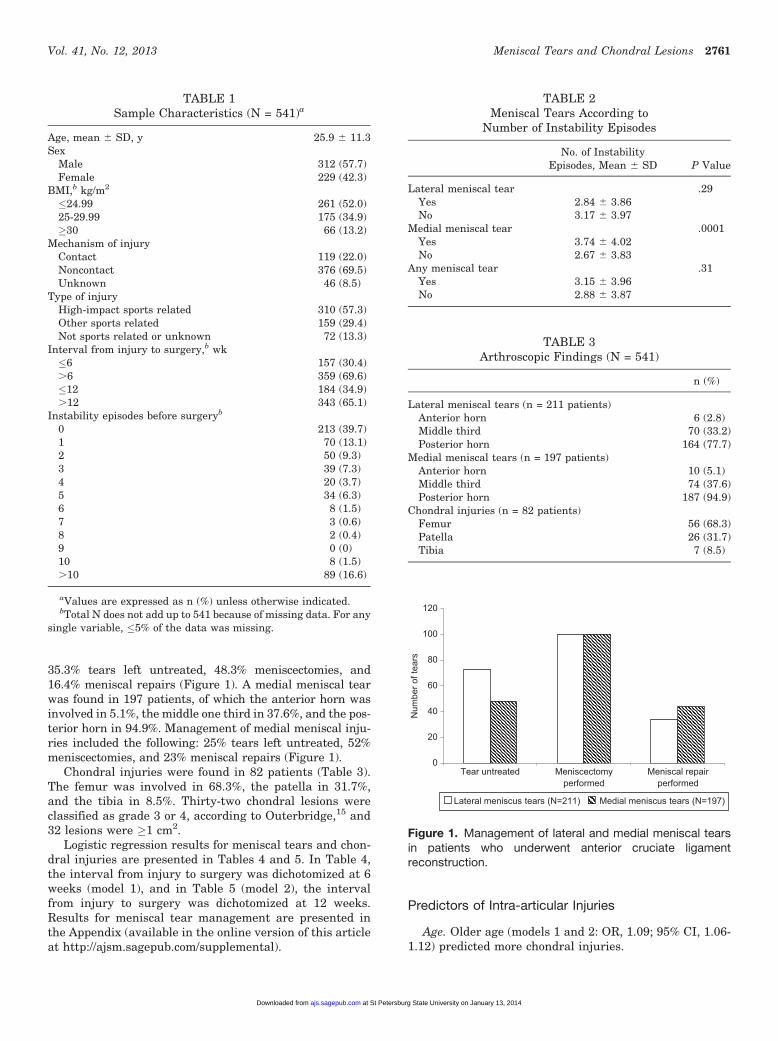
35.3% tears left untreated, 48.3% meniscectomies, and16.4% meniscal repairs (Figure 1). A medial meniscal tearwas found in 197 patients, of which the anterior horn wasinvolved in 5.1%, the middle one third in 37.6%, and the pos-terior horn in 94.9%. Management of medial meniscal inju-ries included the following: 25% tears left untreated, 52%meniscectomies, and 23% meniscal repairs (Figure 1).
Chondral injuries were found in 82 patients (Table 3).The femur was involved in 68.3%, the patella in 31.7%,and the tibia in 8.5%. Thirty-two chondral lesions wereclassified as grade 3 or 4, according to Outerbridge,15 and32 lesions were �1 cm2.
Logistic regression results for meniscal tears and chon-dral injuries are presented in Tables 4 and 5. In Table 4,the interval from injury to surgery was dichotomized at 6weeks (model 1), and in Table 5 (model 2), the intervalfrom injury to surgery was dichotomized at 12 weeks.Results for meniscal tear management are presented inthe Appendix (available in the online version of this articleat http://ajsm.sagepub.com/supplemental).
Predictors of Intra-articular Injuries
Age. Older age (models 1 and 2: OR, 1.09; 95% CI, 1.06-1.12) predicted more chondral injuries.
TABLE 1Sample Characteristics (N = 541)a
Age, mean 6 SD, y 25.9 6 11.3Sex
Male 312 (57.7)Female 229 (42.3)
BMI,b kg/m2
�24.99 261 (52.0)25-29.99 175 (34.9)�30 66 (13.2)
Mechanism of injuryContact 119 (22.0)Noncontact 376 (69.5)Unknown 46 (8.5)
Type of injuryHigh-impact sports related 310 (57.3)Other sports related 159 (29.4)Not sports related or unknown 72 (13.3)
Interval from injury to surgery,b wk�6 157 (30.4).6 359 (69.6)�12 184 (34.9).12 343 (65.1)
Instability episodes before surgeryb
0 213 (39.7)1 70 (13.1)2 50 (9.3)3 39 (7.3)4 20 (3.7)5 34 (6.3)6 8 (1.5)7 3 (0.6)8 2 (0.4)9 0 (0)10 8 (1.5).10 89 (16.6)
aValues are expressed as n (%) unless otherwise indicated.bTotal N does not add up to 541 because of missing data. For any
single variable, �5% of the data was missing.
TABLE 2Meniscal Tears According to
Number of Instability Episodes
No. of InstabilityEpisodes, Mean 6 SD P Value
Lateral meniscal tear .29Yes 2.84 6 3.86No 3.17 6 3.97
Medial meniscal tear .0001Yes 3.74 6 4.02No 2.67 6 3.83
Any meniscal tear .31Yes 3.15 6 3.96No 2.88 6 3.87
TABLE 3Arthroscopic Findings (N = 541)
n (%)
Lateral meniscal tears (n = 211 patients)Anterior horn 6 (2.8)Middle third 70 (33.2)Posterior horn 164 (77.7)
Medial meniscal tears (n = 197 patients)Anterior horn 10 (5.1)Middle third 74 (37.6)Posterior horn 187 (94.9)
Chondral injuries (n = 82 patients)Femur 56 (68.3)Patella 26 (31.7)Tibia 7 (8.5)
0
20
40
60
80
100
120
Tear untreated Meniscectomyperformed
Meniscal repairperformed
Lateral meniscus tears (N=211) Medial meniscus tears (N=197)
Num
ber o
f tea
rs
Figure 1. Management of lateral and medial meniscal tearsin patients who underwent anterior cruciate ligamentreconstruction.
Vol. 41, No. 12, 2013 Meniscal Tears and Chondral Lesions 2761
at St Petersburg State University on January 13, 2014ajs.sagepub.comDownloaded from
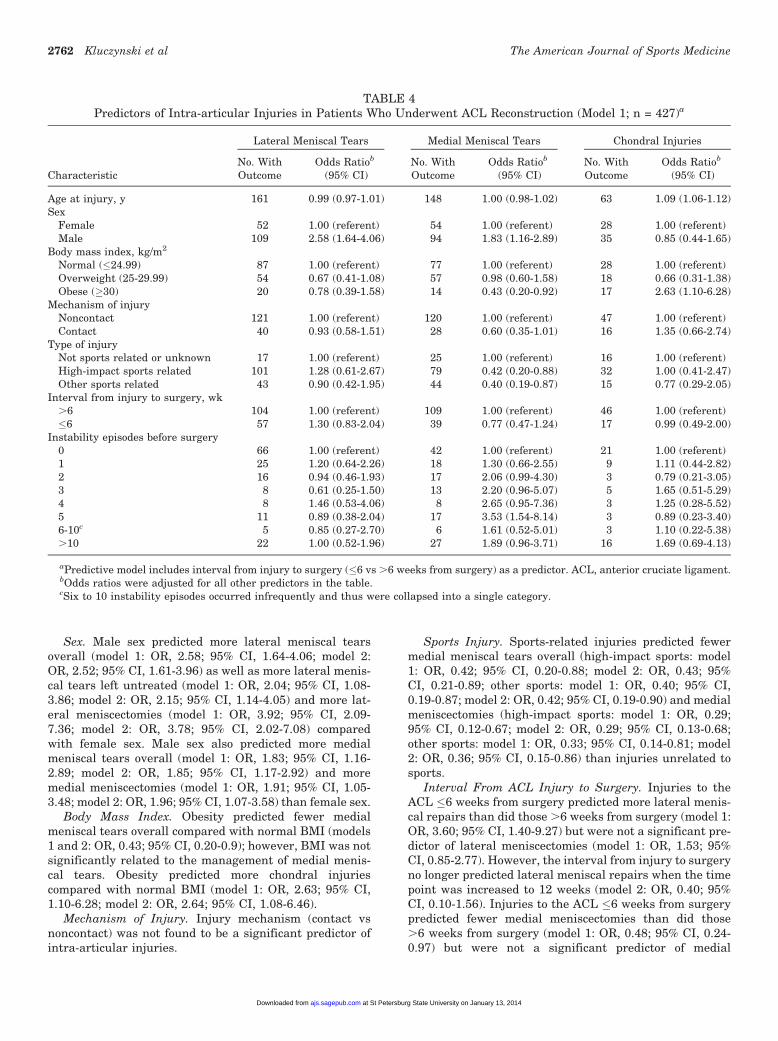
Sex. Male sex predicted more lateral meniscal tearsoverall (model 1: OR, 2.58; 95% CI, 1.64-4.06; model 2:OR, 2.52; 95% CI, 1.61-3.96) as well as more lateral menis-cal tears left untreated (model 1: OR, 2.04; 95% CI, 1.08-3.86; model 2: OR, 2.15; 95% CI, 1.14-4.05) and more lat-eral meniscectomies (model 1: OR, 3.92; 95% CI, 2.09-7.36; model 2: OR, 3.78; 95% CI, 2.02-7.08) comparedwith female sex. Male sex also predicted more medialmeniscal tears overall (model 1: OR, 1.83; 95% CI, 1.16-2.89; model 2: OR, 1.85; 95% CI, 1.17-2.92) and moremedial meniscectomies (model 1: OR, 1.91; 95% CI, 1.05-3.48; model 2: OR, 1.96; 95% CI, 1.07-3.58) than female sex.
Body Mass Index. Obesity predicted fewer medialmeniscal tears overall compared with normal BMI (models1 and 2: OR, 0.43; 95% CI, 0.20-0.9); however, BMI was notsignificantly related to the management of medial menis-cal tears. Obesity predicted more chondral injuriescompared with normal BMI (model 1: OR, 2.63; 95% CI,1.10-6.28; model 2: OR, 2.64; 95% CI, 1.08-6.46).
Mechanism of Injury. Injury mechanism (contact vsnoncontact) was not found to be a significant predictor ofintra-articular injuries.
Sports Injury. Sports-related injuries predicted fewermedial meniscal tears overall (high-impact sports: model1: OR, 0.42; 95% CI, 0.20-0.88; model 2: OR, 0.43; 95%CI, 0.21-0.89; other sports: model 1: OR, 0.40; 95% CI,0.19-0.87; model 2: OR, 0.42; 95% CI, 0.19-0.90) and medialmeniscectomies (high-impact sports: model 1: OR, 0.29;95% CI, 0.12-0.67; model 2: OR, 0.29; 95% CI, 0.13-0.68;other sports: model 1: OR, 0.33; 95% CI, 0.14-0.81; model2: OR, 0.36; 95% CI, 0.15-0.86) than injuries unrelated tosports.
Interval From ACL Injury to Surgery. Injuries to theACL �6 weeks from surgery predicted more lateral menis-cal repairs than did those .6 weeks from surgery (model 1:OR, 3.60; 95% CI, 1.40-9.27) but were not a significant pre-dictor of lateral meniscectomies (model 1: OR, 1.53; 95%CI, 0.85-2.77). However, the interval from injury to surgeryno longer predicted lateral meniscal repairs when the timepoint was increased to 12 weeks (model 2: OR, 0.40; 95%CI, 0.10-1.56). Injuries to the ACL �6 weeks from surgerypredicted fewer medial meniscectomies than did those.6 weeks from surgery (model 1: OR, 0.48; 95% CI, 0.24-0.97) but were not a significant predictor of medial
TABLE 4Predictors of Intra-articular Injuries in Patients Who Underwent ACL Reconstruction (Model 1; n = 427)a
Lateral Meniscal Tears Medial Meniscal Tears Chondral Injuries
CharacteristicNo. WithOutcome
Odds Ratiob
(95% CI)No. WithOutcome
Odds Ratiob
(95% CI)No. WithOutcome
Odds Ratiob
(95% CI)
Age at injury, y 161 0.99 (0.97-1.01) 148 1.00 (0.98-1.02) 63 1.09 (1.06-1.12)Sex
Female 52 1.00 (referent) 54 1.00 (referent) 28 1.00 (referent)Male 109 2.58 (1.64-4.06) 94 1.83 (1.16-2.89) 35 0.85 (0.44-1.65)
Body mass index, kg/m2
Normal (�24.99) 87 1.00 (referent) 77 1.00 (referent) 28 1.00 (referent)Overweight (25-29.99) 54 0.67 (0.41-1.08) 57 0.98 (0.60-1.58) 18 0.66 (0.31-1.38)Obese (�30) 20 0.78 (0.39-1.58) 14 0.43 (0.20-0.92) 17 2.63 (1.10-6.28)
Mechanism of injuryNoncontact 121 1.00 (referent) 120 1.00 (referent) 47 1.00 (referent)Contact 40 0.93 (0.58-1.51) 28 0.60 (0.35-1.01) 16 1.35 (0.66-2.74)
Type of injuryNot sports related or unknown 17 1.00 (referent) 25 1.00 (referent) 16 1.00 (referent)High-impact sports related 101 1.28 (0.61-2.67) 79 0.42 (0.20-0.88) 32 1.00 (0.41-2.47)Other sports related 43 0.90 (0.42-1.95) 44 0.40 (0.19-0.87) 15 0.77 (0.29-2.05)
Interval from injury to surgery, wk.6 104 1.00 (referent) 109 1.00 (referent) 46 1.00 (referent)�6 57 1.30 (0.83-2.04) 39 0.77 (0.47-1.24) 17 0.99 (0.49-2.00)
Instability episodes before surgery0 66 1.00 (referent) 42 1.00 (referent) 21 1.00 (referent)1 25 1.20 (0.64-2.26) 18 1.30 (0.66-2.55) 9 1.11 (0.44-2.82)2 16 0.94 (0.46-1.93) 17 2.06 (0.99-4.30) 3 0.79 (0.21-3.05)3 8 0.61 (0.25-1.50) 13 2.20 (0.96-5.07) 5 1.65 (0.51-5.29)4 8 1.46 (0.53-4.06) 8 2.65 (0.95-7.36) 3 1.25 (0.28-5.52)5 11 0.89 (0.38-2.04) 17 3.53 (1.54-8.14) 3 0.89 (0.23-3.40)6-10c 5 0.85 (0.27-2.70) 6 1.61 (0.52-5.01) 3 1.10 (0.22-5.38).10 22 1.00 (0.52-1.96) 27 1.89 (0.96-3.71) 16 1.69 (0.69-4.13)
aPredictive model includes interval from injury to surgery (�6 vs .6 weeks from surgery) as a predictor. ACL, anterior cruciate ligament.bOdds ratios were adjusted for all other predictors in the table.cSix to 10 instability episodes occurred infrequently and thus were collapsed into a single category.
2762 Kluczynski et al The American Journal of Sports Medicine
at St Petersburg State University on January 13, 2014ajs.sagepub.comDownloaded from
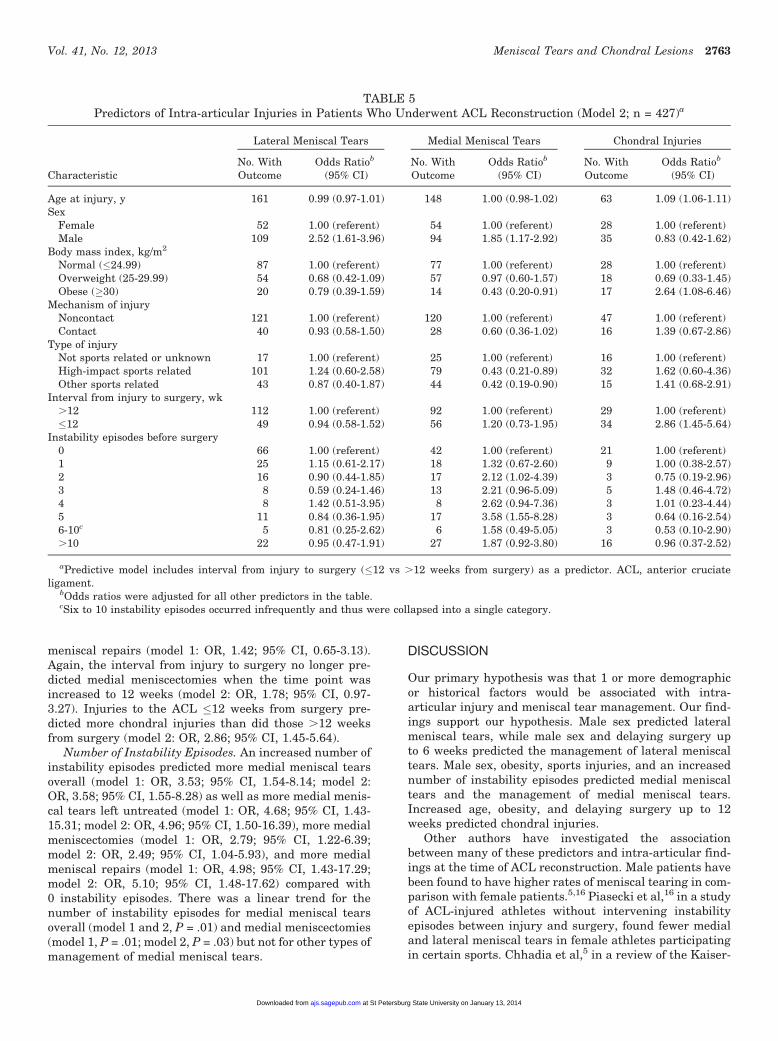
meniscal repairs (model 1: OR, 1.42; 95% CI, 0.65-3.13).Again, the interval from injury to surgery no longer pre-dicted medial meniscectomies when the time point wasincreased to 12 weeks (model 2: OR, 1.78; 95% CI, 0.97-3.27). Injuries to the ACL �12 weeks from surgery pre-dicted more chondral injuries than did those .12 weeksfrom surgery (model 2: OR, 2.86; 95% CI, 1.45-5.64).
Number of Instability Episodes. An increased number ofinstability episodes predicted more medial meniscal tearsoverall (model 1: OR, 3.53; 95% CI, 1.54-8.14; model 2:OR, 3.58; 95% CI, 1.55-8.28) as well as more medial menis-cal tears left untreated (model 1: OR, 4.68; 95% CI, 1.43-15.31; model 2: OR, 4.96; 95% CI, 1.50-16.39), more medialmeniscectomies (model 1: OR, 2.79; 95% CI, 1.22-6.39;model 2: OR, 2.49; 95% CI, 1.04-5.93), and more medialmeniscal repairs (model 1: OR, 4.98; 95% CI, 1.43-17.29;model 2: OR, 5.10; 95% CI, 1.48-17.62) compared with0 instability episodes. There was a linear trend for thenumber of instability episodes for medial meniscal tearsoverall (model 1 and 2, P = .01) and medial meniscectomies(model 1, P = .01; model 2, P = .03) but not for other types ofmanagement of medial meniscal tears.
DISCUSSION
Our primary hypothesis was that 1 or more demographicor historical factors would be associated with intra-articular injury and meniscal tear management. Our find-ings support our hypothesis. Male sex predicted lateralmeniscal tears, while male sex and delaying surgery upto 6 weeks predicted the management of lateral meniscaltears. Male sex, obesity, sports injuries, and an increasednumber of instability episodes predicted medial meniscaltears and the management of medial meniscal tears.Increased age, obesity, and delaying surgery up to 12weeks predicted chondral injuries.
Other authors have investigated the associationbetween many of these predictors and intra-articular find-ings at the time of ACL reconstruction. Male patients havebeen found to have higher rates of meniscal tearing in com-parison with female patients.5,16 Piasecki et al,16 in a studyof ACL-injured athletes without intervening instabilityepisodes between injury and surgery, found fewer medialand lateral meniscal tears in female athletes participatingin certain sports. Chhadia et al,5 in a review of the Kaiser-
TABLE 5Predictors of Intra-articular Injuries in Patients Who Underwent ACL Reconstruction (Model 2; n = 427)a
Lateral Meniscal Tears Medial Meniscal Tears Chondral Injuries
CharacteristicNo. WithOutcome
Odds Ratiob
(95% CI)No. WithOutcome
Odds Ratiob
(95% CI)No. WithOutcome
Odds Ratiob
(95% CI)
Age at injury, y 161 0.99 (0.97-1.01) 148 1.00 (0.98-1.02) 63 1.09 (1.06-1.11)Sex
Female 52 1.00 (referent) 54 1.00 (referent) 28 1.00 (referent)Male 109 2.52 (1.61-3.96) 94 1.85 (1.17-2.92) 35 0.83 (0.42-1.62)
Body mass index, kg/m2
Normal (�24.99) 87 1.00 (referent) 77 1.00 (referent) 28 1.00 (referent)Overweight (25-29.99) 54 0.68 (0.42-1.09) 57 0.97 (0.60-1.57) 18 0.69 (0.33-1.45)Obese (�30) 20 0.79 (0.39-1.59) 14 0.43 (0.20-0.91) 17 2.64 (1.08-6.46)
Mechanism of injuryNoncontact 121 1.00 (referent) 120 1.00 (referent) 47 1.00 (referent)Contact 40 0.93 (0.58-1.50) 28 0.60 (0.36-1.02) 16 1.39 (0.67-2.86)
Type of injuryNot sports related or unknown 17 1.00 (referent) 25 1.00 (referent) 16 1.00 (referent)High-impact sports related 101 1.24 (0.60-2.58) 79 0.43 (0.21-0.89) 32 1.62 (0.60-4.36)Other sports related 43 0.87 (0.40-1.87) 44 0.42 (0.19-0.90) 15 1.41 (0.68-2.91)
Interval from injury to surgery, wk.12 112 1.00 (referent) 92 1.00 (referent) 29 1.00 (referent)�12 49 0.94 (0.58-1.52) 56 1.20 (0.73-1.95) 34 2.86 (1.45-5.64)
Instability episodes before surgery0 66 1.00 (referent) 42 1.00 (referent) 21 1.00 (referent)1 25 1.15 (0.61-2.17) 18 1.32 (0.67-2.60) 9 1.00 (0.38-2.57)2 16 0.90 (0.44-1.85) 17 2.12 (1.02-4.39) 3 0.75 (0.19-2.96)3 8 0.59 (0.24-1.46) 13 2.21 (0.96-5.09) 5 1.48 (0.46-4.72)4 8 1.42 (0.51-3.95) 8 2.62 (0.94-7.36) 3 1.01 (0.23-4.44)5 11 0.84 (0.36-1.95) 17 3.58 (1.55-8.28) 3 0.64 (0.16-2.54)6-10c 5 0.81 (0.25-2.62) 6 1.58 (0.49-5.05) 3 0.53 (0.10-2.90).10 22 0.95 (0.47-1.91) 27 1.87 (0.92-3.80) 16 0.96 (0.37-2.52)
aPredictive model includes interval from injury to surgery (�12 vs .12 weeks from surgery) as a predictor. ACL, anterior cruciateligament.
bOdds ratios were adjusted for all other predictors in the table.cSix to 10 instability episodes occurred infrequently and thus were collapsed into a single category.
Vol. 41, No. 12, 2013 Meniscal Tears and Chondral Lesions 2763
at St Petersburg State University on January 13, 2014ajs.sagepub.comDownloaded from

Permanente Registry of ACL injuries (N = 1252), foundfewer lateral meniscal tears in female patients comparedwith male patients (OR, 0.65; 95% CI, 0.51-0.83). Similarto our findings, obesity3 and increased age5 have beenfound to be associated with chondral injuries. Bowerset al,3 in a prospective study of 456 ACL-injured patients,found that BMI was a predictor of medial femoral condylar,medial tibial plateau, and medial meniscal damage, whileChhadia et al5 found an increased incidence of chondralinjuries with older age and an increased time to surgery.Contrary to previous studies,3 we found obesity to be a pre-dictor of fewer medial meniscal tears. As an exploratoryanalysis, we examined BMI as a continuous variable inthe regression models instead of BMI categories and foundit to remain associated with chondral injuries but not withmeniscal tears (data not shown). It is possible that dividingBMI into categories may have led to a spurious association.Our findings are similar to the above studies, with theadditional strength of also collecting data on the numberof instability episodes while adjusting the ORs for all otherdemographic and historical factors.
There have been multiple studies exploring the associa-tion between the timing of surgery and meniscal tears,with the majority demonstrating higher rates of medialmeniscal tears when ACL surgery is delayed.2,5,8-10,13,19,21,23
Our study differed somewhat from those previously pub-lished because we analyzed each potential predictor withan adjustment for the other predictors. We found that thenumber of instability episodes correlated with medial menis-cal tears, even when adjusted for time from injury to surgery,but time, when adjusted for the number of instability epi-sodes, did not predict meniscal tearing. The presence ofmeniscal and chondral injuries becomes an important factorwhen long-term results of ACL reconstruction are consideredbecause these findings have been linked to an increased inci-dence of osteoarthritis at longer follow-up intervals.12 Ideally,patients with isolated ACL tears would be able to determinetheir risk of subsequent meniscal damage with nonoperativemanagement particularly because there is evidence that ACLreconstruction may actually increase the risk of later osteoar-thritis.11 Lacking such information, many surgeons currentlybase their recommendations for management on the activityto which the patient anticipates returning, with frequent par-ticipation in high-impact sports being one primary reason torecommend reconstruction.
We examined the association between an intra-articularinjury and delaying surgery by 6 weeks or 12 weeks frominjury. Performing surgery within 6 weeks was not predic-tive of intra-articular injuries but was predictive of morelateral meniscal repairs and fewer medial meniscectomies.Performing surgery within 12 weeks was predictive ofmore chondral injuries but was not predictive of the man-agement of lateral or medial meniscal tears. Our finding ofa relationship between medial meniscal tearing and thenumber of instability episodes, coupled with the lack ofa relationship between intra-articular injuries and delay-ing surgery by 6 weeks, may make providers more comfort-able recommending initial nonoperative management.While our study did not compare operative and nonopera-tive management, we did find that a delay in
reconstruction had no effect on intra-articular injurieswhen other factors were adjusted. When counselinga patient with an isolated ACL tear, our data suggestfocusing on the number of instability episodes after the ini-tial injury rather than the interval from injury to surgeryas a more accurate predictor of subsequent medial menis-cal tears. Other authors have found no difference in therates of subsequent meniscal surgery when patients under-going immediate ACL reconstruction were compared withthose undergoing initial nonoperative management andreconstruction only if they had subsequent instability.6,7
Our data demonstrate that patients who reported 5 insta-bility episodes were about 4 times as likely to have a medialmeniscal tear left untreated or a medial meniscal repaircompared with 0 instability episodes. Also, patients whoreported �10 instability episodes were about 2 times aslikely to have a medial meniscectomy compared with0 instability episodes. This information may help the sur-geon to quantify risk when discussing treatment options.
Strengths of our study include its prospective design,large sample size, consistency with previous epidemiologi-cal data, confirmation of a complete ACL tear by directarthroscopic visualization, and addition of the number ofinstability episodes before surgery as a new quantitativevariable, which we found to affect medial meniscal tearrates and management but not the management of chon-dral injuries or lateral meniscal tears.
There are also limitations to our study. Even though allof our data were collected prospectively, it is possible thatpatients did not accurately recall the number of instabilityepisodes suffered after their initial injury. Althoughpatients were questioned by experienced sports medicinesurgeons directly about instability episodes, with caretaken to specify pivot-shift instability versus giving waybecause of quadriceps weakness, these may still havebeen confused. Our results only pertain to patients electingsurgery, which may not allow generalization to all patientspresenting with an ACL tear. Time from injury to surgerywas not a predictor of a meniscal injury as one wouldexpect. Although we adjusted for potential confounders,there may have been additional confounders that we didnot measure, or the method that we used for quantifyingtime from injury to surgery may have prevented us fromobserving an association with meniscal injuries. Decisionsregarding meniscal tear management may have varied bysurgeon preference and thus could have biased the results.
CONCLUSION
In our prospective study of 541 patients undergoing ACLreconstruction, age at the time of injury was associatedwith chondral injuries, male patients had more lateraland medial meniscectomies, obesity was associated withmore chondral injuries, surgeries performed within 6weeks were associated with more lateral meniscal repairsbut fewer medial meniscectomies, and sports-related inju-ries had fewer medial meniscal tears. Increasing numbersof instability episodes led to more medial meniscal tearsand more medial meniscectomies.
2764 Kluczynski et al The American Journal of Sports Medicine
at St Petersburg State University on January 13, 2014ajs.sagepub.comDownloaded from

REFERENCES
1. Anstey DE, Heyworth BE, Price MD, Gill TJ. Effect of timing of ACL
reconstruction in surgery and development of meniscal and chondral
lesions. Phys Sportsmed. 2012;40(1):36-40.
2. Borchers JR, Kaeding CC, Pedroza AD, Huston LJ, Spindler KP,
Wright RW. Intra-articular findings in primary and revision anterior cru-
ciate ligament reconstruction surgery: a comparison of the MOON and
MARS study groups. Am J Sports Med. 2011;39(9):1889-1893.
3. Bowers AL, Spindler KP, McCarty EC, Arrigain S. Height, weight, and
BMI predict intra-articular injuries observed during ACL reconstruc-
tion: evaluation of 456 cases from a prospective ACL database.
Clin J Sport Med. 2005;15(1):9-13.
4. Brophy RH, Zeltser D, Wright RW, Flanigan D. Anterior cruciate liga-
ment reconstruction and concomitant articular cartilage injury: inci-
dence and treatment. Arthroscopy. 2010;26(1):112-120.
5. Chhadia AM, Inacio MC, Maletis GB, Csintalan RP, Davis BR, Funahashi
TT. Are meniscus and cartilage injuries related to time to anterior cruciate
ligament reconstruction? Am J Sports Med. 2011;39(9):1894-1899.
6. Frobell RB, Roos EM, Roos HP, Ranstam J, Lohmander LS. A ran-
domized trial of treatment for acute anterior cruciate ligament tears.
N Engl J Med. 2010;363(4):331-342.
7. Frobell RB, Roos HP, Roos EM, Roemer FW, Ranstam J, Lohmander
LS. Treatment for acute anterior cruciate ligament tear: five year out-
come of randomised trial. BMJ. 2013;346:f232.
8. Granan LP, Bahr R, Lie SA, Engebretsen L. Timing of anterior cruciate
ligament reconstructive surgery and risk of cartilage lesions and
meniscal tears: a cohort study based on the Norwegian National
Knee Ligament Registry. Am J Sports Med. 2009;37(5):955-961.
9. Keene GC, Bickerstaff D, Rae PJ, Paterson RS. The natural history of
meniscal tears in anterior cruciate ligament insufficiency. Am J Sports
Med. 1993;21(5):672-679.
10. Kennedy J, Jackson MP, O’Kelly P, Moran R. Timing of reconstruc-
tion of the anterior cruciate ligament in athletes and the incidence
of secondary pathology within the knee. J Bone Joint Surg Br.
2010;92(3):362-366.
11. Kessler MA, Behrend H, Henz S, Stutz G, Rukavina A, Kuster MS.
Function, osteoarthritis and activity after ACL-rupture: 11 years
follow-up results of conservative versus reconstructive treatment.
Knee Surg Sports Traumatol Arthrosc. 2008;16(5):442-448.
12. Louboutin H, Debarge R, Richou J, et al. Osteoarthritis in patients
with anterior cruciate ligament rupture: a review of risk factors.
Knee. 2009;16(4):239-244.
13. Naranje S, Mittal R, Nag H, Sharma R. Arthroscopic and magnetic
resonance imaging evaluation of meniscus lesions in the chronic
anterior cruciate ligament-deficient knee. Arthroscopy. 2008;24(9):
1045-1051.
14. Oiestad BE, Engebretsen L, Storheim K, Risberg MA. Knee osteoar-
thritis after anterior cruciate ligament injury: a systematic review. Am
J Sports Med. 2009;37(7):1434-1443.
15. Outerbridge RE. The etiology of chondromalacia patellae. J Bone
Joint Surg Br. 1961;43:752-757.
16. Piasecki DP, Spindler KP, Warren TA, Andrish JT, Parker RD. Intraar-
ticular injuries associated with anterior cruciate ligament tear: find-
ings at ligament reconstruction in high school and recreational
athletes. An analysis of sex-based differences. Am J Sports Med.
2003;31(4):601-605.
17. Rothman KJ, Greenland S, Lash TL. Modern Epidemiology. 3rd ed.
Philadelphia: Wolters Kluwer Health; 2008.
18. Spindler KP, Schils JP, Bergfeld JA, et al. Prospective study of osse-
ous, articular, and meniscal lesions in recent anterior cruciate liga-
ment tears by magnetic resonance imaging and arthroscopy. Am J
Sports Med. 1993;21(4):551-557.
19. Sri-Ram K, Salmon LJ, Pinczewski LA, Roe JP. The incidence of sec-
ondary pathology after anterior cruciate ligament rupture in 5086
patients requiring ligament reconstruction. Bone Joint J. 2013;
95B(1):59-64.
20. World Health Organization. Obesity: Preventing and Managing the
Global Epidemic. Geneva: World Health Organization; 2000.
21. Yoo JC, Ahn JH, Lee SH, Yoon YC. Increasing incidence of medial
meniscal tears in nonoperatively treated anterior cruciate ligament
insufficiency patients documented by serial magnetic resonance
imaging studies. Am J Sports Med. 2009;37(8):1478-1483.
22. Yoon KH, Yoo JH, Kim KI. Bone contusion and associated meniscal
and medial collateral ligament injury in patients with anterior cruciate
ligament rupture. J Bone Joint Surg Am. 2011;93(16):1510-1518.
23. Yuksel HY, Erkan S, Uzun M. The evaluation of intraarticular lesions
accompanying ACL ruptures in military personnel who elected not to
restrict their daily activities: the effect of age and time from injury.
Knee Surg Sports Traumatol Arthrosc. 2006;14(11):1139-1147.
For reprints and permission queries, please visit SAGE’s Web site at http://www.sagepub.com/journalsPermissions.nav
Vol. 41, No. 12, 2013 Meniscal Tears and Chondral Lesions 2765
at St Petersburg State University on January 13, 2014ajs.sagepub.comDownloaded from





























