Embed Size (px)
Citation preview

Extrapolation of General
Population Hypertension
Treatment Guidelines to CKD and
ESRD Patients: Appropriate or
Inappropriate?
Csaba P Kovesdy, MD FASN
University of Tennessee, Memphis TN
Memphis VA Medical Center, Memphis TN

Objectives
Review general population guidelines for the
treatment of hypertension
Discuss rationale of using general population
guidelines for hypertension treatment in patients
with CKD and ESRD
Examine similarities and differences in CVD
and hypertension therapy between the general
population and patients with CKD and ESRD

What this talk is not meant to do…
Question the need to treat hypertension in the
general population or in patients with CKD and
ESRD
Question the validity of general population
guidelines for the treatment of hypertension


Stephen Hales (1677-1761)
Booth J. Proc Roy Soc Med. 1977;70:793-799

Ludwig’s kymograph (1847)
Booth J. Proc Roy Soc Med. 1977;70:793-799

Vierordt’s sphygmograph (1852)
Direct sphygmograph (Marey, cca 1881)
Booth J. Proc Roy Soc Med. 1977;70:793-799

Booth J. Proc Roy Soc Med. 1977;70:793-799
Von Basch's sphygmomanometer and stand (cca 1881)

History of BP measurements
Scipione Riva-Rocci: Introduction of modern
circumferential BP cuff (1896)
Friedrich von Recklinghausen: Started using
larger size cuff (1901)
Nikolai Korotkoff: Introduction
of the auscultatory technique (1905)
Nikolai Sergeyevich Korotkov
(1874-1920) Booth J. Proc Roy Soc Med. 1977;70:793-799

Messerli F. N Engl J Med 1995;332:1038-1039

Diastolic and Systolic Arterial Pressure of FDR
Messerli F. N Engl J Med 1995;332:1038-1039

Age Blood
pressure
Reduction in life
expectancy (years)
(mm Hg) Man Woman
35 years 130/90 4 -
140/95 9 -
150/100 16.5 -
45 years 130/90 3 1.5
140/95 6 5
150/100 11.5 8.5
55 years 130/90 1 0.5
140/95 4 3
150/100 6 4
METROPOLITAN LIFE INSURANCE COMPANY. "Blood pressure: insurance
experience and its implications". New York: Metropolitan Life Insurance Company; 1961.

Hypertension in Medicine: Key
Moments
Framingham Study: Kannel et al, Ann Intern
Med. 1961 Jul;55:33-50
First clinical trials of BP lowering
Hamilton M, Thompson EN: The role of blood
pressure control in preventing complications of
hypertension. Lancet 1964; 1:235-239
VA Cooperative Study Group: Effects of treatment
on morbidity of hypertension. JAMA 1967;
202:1028-1033

Relationship of BP with CV risk is “strong,
continuous, independent, predictive and
etiologically significant.”
JNC 6, Arch Intern Med. 1997;157:2413-46.

Patients with CKD are in the "highest-risk" group for CVD (Strong). Patients with CKD are at increased risk of CVD. Hypertension is a risk factor for CVD events in CKD. However, there have been few controlled trials to demonstrate the efficacy of blood pressure lowering to reduce the risk of CVD in CKD; therefore, the Work Group made recommendations for CKD based on extrapolation from evidence on the efficacy of antihypertensive therapy in the general population.
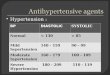
K/DOQI Clinical Practice Guidelines on Hypertension and Antihypertensive Agents in Chronic Kidney Disease

For Individuals With: BP Goal: Hypertension (no diabetes or renal disease)
Diabetes Mellitus
Renal Disease
with proteinuria >1 gram/24 hours or diabetic kidney disease
<140/90 mmHg
(JNC 7)
<130/80 mmHg
(ADA, JNC 7)
<135/85 mmHg
<125/75 mmHg
(NKF)
Chobanian AV et al. JAMA. 2003;289:2560–2571. American Diabetes Association. Diabetes Care. 2002;25:134–147. National Kidney Foundation. Am J Kidn Dis. 2002;39(suppl 1):S1–S266.
Target Blood Pressure

Criteria for Extrapolation of General
Population Guidelines to CKD Patients
1) The mechanism and expression of CVD in CKD should be similar to those observed in the general population. Specifically, the features of CVD, the relationship of CVD outcomes to hypertension, the mechanism of blood pressure lowering, and the responsiveness of risk factors to lifestyle modifications and pharmacological therapy should be similar in patients with CKD and the general population.
2) Therapies in patients with CKD should be as safe, or nearly so, as in the general population. In particular, there should not be additional adverse effects of a specific therapy that limits its usefulness in patients with CKD, either because of altered pharmacokinetics, drug interactions, or increased risk of toxicity to the kidney.
3) The duration of therapy required to improve CVD outcomes in the general population should not exceed the life expectancy of patients with CKD. Numerous studies of CVD in the general population have shown a benefit of interventions within 2 to 5 years, with greater and earlier benefits in patients at highest risk. Thus, it is likely that patients with CKD Stages 1-4 could benefit from more effective treatment of CVD.
Levey AS et al, NKF Task Force on CVD Am J Kidney Dis 32:853-906, 1998

Rationale for Extrapolation of General
Population Guidelines to CKD Patients
1) The mechanism and expression of CVD in CKD should be similar to those observed in the general population. Specifically,
1) the features of CVD,
2) the relationship of CVD outcomes to hypertension,
3) the mechanism of blood pressure lowering, and
4) the responsiveness of risk factors to lifestyle modifications and pharmacological therapy should be similar in patients with CKD and the general population.
Levey AS et al, NKF Task Force on CVD Am J Kidney Dis 32:853-906, 1998

General population
N=310,232,863 (July 2010 est.)
Median age: 36.8 years
Ethnic composition
White 79.96%
Black 12.85%
Hispanic 15.1%
Expected remaining life time: 25.2 years
ESRD
N=368,544 (December 31, 2007)
Median age: 59.1 years
Ethnic composition
White 55.7%
Black 37.1%
Hispanic 15.6%
Expected remaining life time: 5.9 years
https://www.cia.gov/library/publications/the-world-factbook/geos/us.html
http://www.cdc.gov/NCHS/data/nvsr/nvsr58/nvsr58_19.pdf
U S Renal Data System, USRDS 2009 Annual Data Report

Platinga et al, Hypertension 2009;54;47-56

General
population
CKD p
Mean SBP (95%CI) 135.9 (135.0
to 136.9)
141.3 (139.7
to 142.9)
<0.001
Mean DBP (95%CI) 76.1 (75.4 to
76.8)
67.5 (66.1
to 68.9)
<0.001
Mean pulse pressure
(95%CI)
59.8 (58.9 to
60.7)
73.8 (71.6
to 75.9)
<0.001
On antihypertensive
medications (%,
95%CI)
37.2 (34.9 to
39.7)
66.4 (63.7 to
69.0)
<0.001
Platinga et al, Hypertension 2009;54;47-56

Platinga et al, Hypertension 2009;54;47-56

Diabetes: Major CV Risk Factor Multiplier
in Hypertension
SBP and CV mortality in the general
population
Stamler et al, Diabetes Care 1993;16:434-444

High-normal BP and CV events in the general population
Vasan et al, N Engl J Med 2001;345:1291-7

Incidence of ESRD by SBP: MRFIT
100
80
60
40
20
0
SBP, mmHg
Incid
en
ce o
f E
SR
D/
100,0
00 p
ers
on
-yrs
, %
White
African American
Klag MJ et al. JAMA. 1997;277:1293–1298.
<117 117–123 124–130 131–140 >140
15.8
5.4
27.3
5.4
26.2
9.1
37.2
14.2
83.1
32.4

15-Month CV Death Risk in 40,933 HD Patients
Pre-Dialysis Systolic BP (mmHg)
<110
110-119.9
120-129.9
130-139.9
140-149.9
150-159.9
160-169.9
170-179.9
180-189.9
>=190
CV
Dea
th H
azar
d R
atio
0.5
0.6
0.7
0.80.9
2
3
4
5
1
Kalantar-Zadeh et al, Hypertension 2005

0.2
0.4
0.6
0.8
1
1.2
1.4
<133 133-154 155-170 >170
Systolic Blood Pressure (mmHg)
Ha
za
rd R
atio
Unadjusted Adjusted
Kovesdy et al, Nephrol Dial Transplant 21(5):1257-62, 2006

Unadjusted Adjusted
0
0.2
0.4
0.6
0.8
1
1.2
1.4
<65 65-75 76-86 >86
Diastolic Blood Pressure (mmHg)
Haza
rd R
atio
Kovesdy et al, Nephrol Dial Transplant 21(5):1257-62, 2006

0
0.2
0.4
0.6
0.8
1
1.2
<64 64-75 76-86 >86
DBP (mmHg)
Hazard
Rati
o
No CVD CVD
Kovesdy et al, Nephrol Dial Transplant 21(5):1257-62, 2006

Palmer BF, N Engl J Med 2002; 347(16):1256-1261

Changes in renal vasculature
Afferent arteriolar endothelial dysfunction
leading to impaired vasodilatation
Hyaline arteriosclerosis
Myointimal hyperplasia
Result is impaired autoregulatory capacity
Intraglomerular pressure begins to vary directly
with changes in systemic pressure Ditscherlein G, Hypertension 1985;7:II-29–II-32.
Bidani et al, Hypertension 1994;24:309-16.
Pelayo and Westcott, J Clin Invest 1991;88:101-5.
Hayashi et al, J Hypertens 1996;14:1387-401.
Palmer BF, Am J Med Sci 2001;321:388-400.

Abuelo JG, N
Engl J Med 2007;357:797-805.

Rationale for Extrapolation of General
Population Guidelines to CKD patients
2) Therapies in patients with CKD should be as safe, or nearly so, as in the general population. In particular, there should not be additional adverse effects of a specific therapy that limits its usefulness in patients with CKD, either because of altered pharmacokinetics, drug interactions, or increased risk of toxicity to the kidney.
Levey AS et al, NKF Task Force on CVD Am J Kidney Dis 32:853-906, 1998

Antihypertensive therapy and diastolic hypotension in CKD
Peralta et al, Hypertension. 2007;50:474-480

The role of diastolic blood pressure in ISH
Somes et al, Arch Intern Med. 1999;159:2004-2009

The role of diastolic blood pressure in ISH
Somes et al,
Arch Intern Med. 1999;159:2004-2009

Aggressive BP lowering and outcomes: The INVEST
Study
Messerli FH et al,
Ann Intern Med. 2006;144:884-893.

Messerli FH et al, Ann Intern Med. 2006;144:884-893.
Aggressive BP lowering and
outcomes: The INVEST Study

Aggressive BP lowering and outcomes: The
INVEST Study
Messerli FH et al, Ann Intern Med. 2006;144:884-893.

Stopping ACEI/ARB in advanced CKD
Ahmed AK et al, Nephrol Dial Transplant 2009 Oct 10. [Epub ahead of print]

Conclusions
The applicability of the current general
population guidelines for HTN control in
patients with CKD and ESRD is questionable.
Changes in vascular biology and subsequent
alterations in autoregulatory capacity make
patients with CKD and ESRD more susceptible
to the deleterious effects of both high and low
BP.

Conclusions
Epidemiologic studies support the possibility that low blood pressure, especially low diastolic blood pressure may be associated with adverse outcomes.
Some clinical trials in patients with characteristics similar to those found in CKD and ESRD (elderly, presence of CVD) support the idea that diastolic hypotension may be deleterious.

Conclusions
The lack of clinical trials of blood pressure
control in CKD and ESRD makes it difficult to
establish specific BP goals for this patient
population.
Management in CKD should be individualized,
taking into account patient characteristics (age,
comorbidities) and response to therapy
(Opinion).