Embed Size (px)
Citation preview

Health Policy Advisory Committee on
Technology
Technology Brief
External aortic root support in Marfan syndrome
November 2012

© State of Queensland (Queensland Health) 2012
This work is licensed under a Creative Commons Attribution Non-Commercial No Derivatives 2.5 Australia licence. In essence, you are free to copy and communicate the work in its current form for non-commercial purposes, as long as you attribute the authors and abide by the licence terms. You may not alter or adapt the work in any way.
To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/2.5/au/.
For further information, contact the HealthPACT Secretariat at:
HealthPACT Secretariat c/o Clinical Access and Redesign Unit, Health Service and Clinical Innovation Division, Queensland Health Lobby 2, Level 2, Citilink Business Centre 153 Campbell Street, Bowen Hills QLD 4006
Postal Address: GPO Box 48, Brisbane Qld 4001
Email: [email protected] Telephone: +61 7 3131 6969
For permissions beyond the scope of this licence contact: Intellectual Property Officer, Queensland Health, GPO Box 48, Brisbane Qld 4001, email [email protected], phone (07) 3234 1479.
Electronic copies can be obtained from: http://www.health.qld.gov.au/healthpact
DISCLAIMER: This brief is published with the intention of providing information of interest. It is based on information available at the time of research and cannot be expected to cover any developments arising from subsequent improvements to health technologies. This brief is based on a limited literature search and is not a definitive statement on the safety, effectiveness or cost-effectiveness of the health technology covered.
The State of Queensland acting through Queensland Health (“Queensland Health”) does not guarantee the accuracy, currency or completeness of the information in this brief. Information may contain or summarise the views of others, and not necessarily reflect the views of Queensland Health.
This brief is not intended to be used as medical advice and it is not intended to be used to diagnose, treat, cure or prevent any disease, nor should it be used for therapeutic purposes or as a substitute for a health professional's advice. It must not be relied upon without verification from authoritative sources. Queensland Health does not accept any liability, including for any injury, loss or damage, incurred by use of or reliance on the information.
This brief was commissioned by Queensland Health, in its role as the Secretariat of the Health Policy Advisory Committee on Technology (HealthPACT). The production of this brief was overseen by HealthPACT. HealthPACT comprises representatives from health departments in all States and Territories, the Australian and New Zealand governments and MSAC. It is a sub-committee of the Australian Health Ministers’ Advisory Council (AHMAC), reporting to AHMAC’s Hospital Principal Committee (HPC). AHMAC supports HealthPACT through funding.
This brief was prepared by Dr Yasoba Atukorale and Dr Alun Cameron from the Australian Safety and Efficacy Register of New Interventional Procedures – Surgical (ASERNIP-S).

External aortic root support in Marfan syndrome: November 2012 1
TECHNOLOGY BRIEF
Register ID WP136
Name of Technology ExoVasc® External aortic root support
Purpose and target group The treatment of aortic distension in patients with Marfan syndrome
Speciality Cardiovascular disease and vascular surgery
Technology type Device
Setting Specialist hospital
Stage of development in Australia
Yet to emerge Established
Experimental Established but changed indication or modification of technique
Investigational Should be taken out of use
Nearly established
Australian Therapeutic Goods Administration approval
Yes ARTG number
No
Not applicable
International utilisation
Country Level of Use
Trials underway or
completed
Limited use Widely diffused
Belgium
UK
Impact summary
The external aortic root support device, ExoVasc®, has been developed by Exstent
Limited for the treatment of aortic distension in patients with Marfan syndrome. The
device is tailored to the anatomy of the patient’s aorta, and provides support to the
distended vessel to reduce the risk of aneurysm formation, dissection and rupture.
The procedure is an alternative to radical aortic replacement surgeries.
Evidence is limited to three low-level included studies which are based on a single
cohort of twenty patients. The results of the studies are limited by a small number of
patients and short-term follow-up (to a median of 20 months). There are occasional

External aortic root support in Marfan syndrome: November 2012 2
adverse events: two patients required additional surgery as a result of ill-fitting
devices. There were no deaths and no devices required removal. The device
appeared to maintain aortic diameter, and may provide a less invasive option to
Marfan patients who risk aortic distension and rupture.
Background
Marfan syndrome is an autosomal dominant disorder of the connective tissues. The
syndrome is typically caused by mutations in gene FBN1, which encodes the
connective tissue protein fibirillin-1.1 The disease is highly variable in its presentation
between patients; clinical features commonly appear with age, primarily involving
the cardiovascular, skeletal and ocular systems.2 The cardiovascular features of the
syndrome range from mild to severe. Common symptoms may include fatigue,
dyspnoea, palpitation, tachycardia, arrhythmia and angina. Progression of the
syndrome results in mitral and aortic regurgitation, degeneration and prolapse of
valves. The clinical features of the advanced disease are aortic dilatation and
aneurism leading to aortic dissection and rupture.3
Aortic dissection in Marfan syndrome has a high risk of mortality (reported at 50-
70% survival at 10 years).4 It occurs due to tears in the inner wall of the aorta caused
by the inability to make normal fibrillin. Over time the tears expand causing bleeding
into and along the aorta wall and leading to further aortic dilatation, aneurism and
aortic rupture.5 Rupture of the aorta is the most common cause of death
(approximately 70%) among patients with Marfan syndrome.6
Pathological dilatation of the aorta and dissection are commonly managed by
prophylactic ascending aorta replacement. Total aortic root replacement (TARR) is
considered the ‘gold standard surgery’,7 although the procedure carries a risk of
death of 1-2 per cent.4 During the procedure, the aortic valve is also removed and
the root replaced with a composite mechanical valve conduit graft. Coronary arteries
are reimplanted if total aortic root replacement is performed. Cardiopulmonary
bypass with full heparanisation is required.
The timing of the surgery is predicted based on history of the disease. The size of the
aorta and its rate of dilation is monitored from an early stage using
echocardiography until the aortic root diameter reaches 5 cm, or 4.5 cm in the
presence of other risk factors (such as family history or rapid aortic growth) .4 If the
diameter of the aorta remains constant, the risk for aortic dissection or rupture is
likely to be reduced.8
External aortic root support (EARS) is a new device for the treatment of aortic
dilatation. High quality digital magnetic resonance images of each patient’s aortic
root are used to manufacture a former, shaped to the individual’s anatomy, using a
dedicated computer-aided design (CAD) routine. This is used as the basis to make a

External aortic root support in Marfan syndrome: November 2012 3
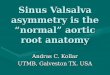
bespoke mesh external support which exactly fits the patient’s aorta (Figure 1). The
external support has a vertical seam and is manufactured from a medical-grade
polymer mesh.6 During the procedure the EARS is used to wrap the root of the aorta,
from the aortoventricular junction to beyond the brachiocephalic artery. The device
may obviate or at least postpone the need for aortic replacement surgery.
Figure 1 An example of a custom-made EARS on a former designed for an individual patient’s aorta. (Image supplied by Exstent Limited.9 Reproduced with approval.)
The procedure of insertion of the device to the ascending aorta is a less invasive
surgery compared to conventional TARR. The mesh support is sutured into place
around the ascending aorta via a median sternotomy. During the procedure the
aorta and coronary arteries are left intact; therefore, patients have a minimum risk
of thromboembolism and stroke. The procedure is likely to require less blood and
fewer blood product transfusions compared to TARR. In addition, cardiopulmonary
bypass or suppression of coronary circulation is not necessary to perform EARS
surgery.
In terms of total procedure time, conventional TARR takes about five to seven hours,
whereas EARS takes approximately two hours. Following implantation of EARS,
ongoing medication, including anticoagulation therapy, is not required. As a result,
EARS may allow young women to become pregnant and undergo C-section.
EARS was introduced and manufactured by Exstent Limited. The initial trial began in
2004 and was completed in June 2009, based at the Royal Brompton Hospital,
London, United Kingdom (UK). The current prototype of EARS device is marketed as
ExoVasc®.9
Clinical need and burden of disease
Marfan syndrome is the most common inherited connective tissue disorder and has
a world-wide prevalence of 1 in 5,000 live births.4, 10 Data from the Australian
Institute of Health and Welfare (AIHW) shows that for the primary diagnosis of

External aortic root support in Marfan syndrome: November 2012 4
Marfan syndrome (ICD-10-AM code Q87.4) there were 15 separations in 2009-10,
and 15 separations in 2008-09.11
Diffusion of the technology in Australia
Diffusion of the device is self-limiting, as the device is custom-made according to
each patient’s aortic measurements. It is not entitled to the CE mark.9 The device
ExoVasc® is not registered with the Federal Drug Administration (United States of
America), the European Medicine Agency (European Union) or the Therapeutic
Goods Administration (Australia). The procedure has been the subject of a National
Institute for Health and Clinical Excellence (NICE) interventional procedures overview
(IP 885)12 and interventional procedure guidance (394, issue date May 2011)13 which
indicate that the procedure should only be undertaken with special arrangements for
clinical governance, consent and audit or research.
A focused search on the use of the device in Australia did not identify any published
local use. The procedure appears not to be undertaken in Australia, and no local
trials are underway (Professor J Smith, personal communication).
Comparators
There are two main comparators to EARS: TARR and valve-sparing aortic root
replacement (VART).
Defined by the first operation performed by Bentall at Hammersmith Hospital in the
1960s, TARR is currently the gold standard surgery to prevent and treat dissection of
the ascending aorta.14 During the surgery, the ascending aorta and aortic valve are
removed and replaced with an artificial Dacron graft incorporating a mechanical or
bioprosthetic aortic valve. The operation is named after Bentall. To prevent blood
clots forming on the graft or valve the patient has to take ongoing anticoagulant
therapy. The implication for an active lifestyle and childbearing versus the risk of
thromboembolism from the mechanical valve is an important consideration.
In VART surgery the aortic root is replaced without a prosthetic aortic valve, and is
possible in patients who have isolated root pathology with functionally normal valve
leaflets.15 The technique preserves native valves, so bears less risk for
thromboembolism; however, this procedure may be prone to valve failure and re-
intervention as a result of Marfan progression.16 17
Clinical expert input indicates that both TARR and VART are available in Australia for
the treatment of aortic root dilatation in Marfan syndrome. TARR is the most
common approach, due to the concern regarding progressive aortic valve
degeneration. The final decision would be based on patient presentation.

External aortic root support in Marfan syndrome: November 2012 5
According to the AIHW there were 126 procedures in 2009-10 for the replacement
of the ascending thoracic aorta with aortic valve replacement (ICD procedure code
38553-03). It is unclear how many of these replacements would have been
undertaken in Marfan patients. There are a number of MBS items for aorta
replacement and repair procedures (Table 1). TARR is commonly utilised via MBS
item 38556 in the current context; in the presence of aortic dissection or rupture
MBS item 38572 would be used. In 2011-12 there were 286 services for repair or
replacement of the ascending thoracic aorta, with aortic valve replacement or repair
(MBS item 38556). During the same year 57 items were used for management of
acute rupture or dissection (MBS item 38572). However, it is unclear how many of
these services would have been provided to Marfan patients.
Table 1 Aorta repair procedures currently on the MBS list18
Item number
Description Full fee 75% Total services (2011-12)a
38550 ASCENDING THORACIC AORTA, repair or
replacement of, not involving valve replacement or
repair or coronary artery implantation
$2,106.15 $1,579.65 64
38553 ASCENDING THORACIC AORTA, repair or
replacement of, with aortic valve replacement or
repair, without implantation of coronary arteries
$2,669.05 $2,001.80 407
38556 ASCENDING THORACIC AORTA, repair or
replacement of, with aortic valve replacement or
repair, and implantation of coronary arteries
$3,046.80 $2,285.10 286
38572 OPERATIVE MANAGEMENT OF ACUTE
RUPTURE OR DISSECTION, in conjunction with
procedures on the thoracic aorta
$1,950.00 $1,462.50 57
Notes: a Total services reflects the number of procedures performed privately, as procedures performed in public
hospitals do not require the use of an MBS item number. Consequently, there may be more activity than
reflected in the MBS statistics. MBS: Medicare Benefits Schedule.
Safety and effectiveness
Three studies were included, one comparative study (NHMRC level III-3)19 and two
case series (NHMRC level of evidence IV)6, 20 that assessed the safety and efficacy of
EARS. All the studies were based on the same trial, which took place at the Royal
Brompton Hospital in the UK.
There was patient overlap between the studies, as they were all based on the same
cohort of twenty patients. Pepper et al 2010a provided initial results of the first ten
patients.6 Pepper et al 2010b provided results of the entire cohort of twenty patients
who received treatment from 2004 to 2009.20 The retrospective case control study,
Treasure et al compared results of the same trial with a matched group of patients
who received total aortic root replacement during the same time period.17

External aortic root support in Marfan syndrome: November 2012 6
Pepper et al 2010b6
Study description
The UK-based prospective case series was conducted over 2004-2009 to assess
safety and efficacy of EARS patients in twenty patients with Marfan syndrome.
Patient inclusion criteria were aortic root diameter of 40-55 mm without clinically
important aortic regurgitation. No patient was excluded for any other technical
reason. Study outcomes were not predefined. Out of the 20 patients who received
the device, 13 were male. The patients were 16-58 years old (median 33 years).
Each patient had a device custom-made from magnetic resonance imaging (MRI)
images of their aorta taken pre-operatively. Patients were followed for a median of
20 months (range 0-67 months). The authors compared the EARS treatment with 28
consecutive patients who underwent total aortic replacement of the ascending
aorta. This comparison was not formally planned within the study design. Seven of
this cohort had Marfan syndrome and 21 had other pathologies. Of the patients with
Marfan syndrome, two received TARR and the remaining five received valve-sparing
operations.
Safety
No deaths following the procedure were recorded at the time of last follow-up. In no
patient was there a need to convert to root replacement or other form of surgery.
Two patients experienced technical problems. One patient experienced
postoperative cardiac arrest with ventricular fibrillation. The circulation was restored
after additional surgery to remove the anterior closing suture on the EARS device to
prevent complications. Misinterpretation of MRI images of coronary artery origins
appeared to have led to this difficulty. The patient recovered and was discharged
eight days after surgery. The second patient experienced a technical problem due to
an anatomical anomaly of the coronary arteries which was identified during the
initial operation. Additional imaging was undertaken to clarify the anatomy, and the
EARS was completed as planned in the following week.
Cardiopulmonary bypass was used for 20 minutes in the first patient only. The
reasons for this requirement are not reported.
Effectiveness
In terms of procedural effectiveness, patients who received EARS did so
comparatively within a shorter operation time. Median operation time to perform
EARS was 148 minutes (range 125-415 min) compared to the patients treated by
aortic root replacement (median 374 min, range 240-493 min, n=7). Only the first
patients who received EARS required cardiopulmonary bypass, which was required

External aortic root support in Marfan syndrome: November 2012 7
for 20 minutes. In contrast, patients who received aortic root replacement required
139-323 minutes of bypass and 100-243 minutes of cross-clamp. EARS patients
were discharged sooner compared to the comparator group. Median length of stay
for EARS patients was 6 days (range 3-16), while aortic root replacement patients
were hospitalised a median of 8 days (range 4-119 days). The anticoagulant warfarin
was administered to three non-EARS patients for the potential risk of
thromboembolism. None of the EARS patients required warfarin.
Postoperative follow-up at a median of 20 months on 16 EARS patients showed a
median aortic root reduction of 1 mm (inter quartile range -2 to +1 mm).
Pepper et al 2010a20
Study description
This study reports data of the initial 10 patients as reported in Pepper et al 2010b
who received EARS in the Royal Brompton Hospital between May 2004 and March
2007.6
Prospective technical data was reported. The ascending aorta at the level of closure
of the aortic valve cusps was measured using MRI preoperatively and at one-year
follow-up. Images were also taken from 37 randomly-selected Marfan patients in
order to provide an indication of measurement error and were examined by a
blinded, experienced radiologist. The largest difference in aortic root diameter was
calculated.
Safety
No deaths, late events or detected changes in aortic valve function were reported.
Arrhythmia (transient atrial fibrillation) was recorded in two patients.
Effectiveness
Eight of the ten EARS patients showed a reduction in the diameter of the aortic root
of up to 1.2 cm. Statistical analysis was not undertaken.
Treasure et al19
This retrospective case control study by Treasure et al19 compared the first 20
patients who received EARS at Royal Brompton Hospital (London, UK) with matched
patients of similar age, aortic diameter and aortic valve function, who received
conventional aortic replacement surgery during the same time period (between May
2004 and December 2009). Patients in the EARS group were aged 16-58 years while
those in the comparison group were 18-63 years old. Aortic root diameters were
40-54 mm in the EARS group and 38-58mm in the aortic root replacement group.
Patients in the aortic root replacement group were excluded if they had repeat

External aortic root support in Marfan syndrome: November 2012 8
cardiac surgery, aortic root diameter beyond the range 4-5.5 cm, or aortic
regurgitation. Sixteen patients had valve-sparing surgery and four received TARR
with composite valved grafts.
Safety
There were no deaths, late events or detected changes in aortic valve function in
either patient population.
Effectiveness
Details of the reported procedural outcomes are provided in Table 2. All procedural
outcomes were improved in favour of the EARS patients. Statistical analysis was not
reported.
Table 2 Effectiveness outcomes
Outcome EARS TRR
Duration of cardiopulmonary bypass
0 (0-20) min 134 (52-316) min
Myocardial ischaemic time 0 (0-0) min 114 (41-250) min
4h blood loss 50 (25-400) ml 218 (85-735) ml
Patients required blood transfusion
1/20 9/18
Patients required platelet transfusion
0/20 9/18
Patients required frozen plasma transfusion
0/20 12/18
EARS: External aortic root support; TRR: Total root replacement.
Cost impact
No studies assessing the cost-effectiveness of external aortic root support in the
treatment of aortic dissection in patients with Marfan syndrome were identified.
The manufacturer, Exstent Limited, confirmed that:
for each patient, costs incurred in preparing an ExoVasc include the preparation
from the CT image data of a CAD model the patient’s aorta and the production of a
rigid former of the aorta on which is formed the porous, textile implant.
To allow for loss or damage to one implant in the operating room, the manufacturer
supplies two sterile implants for each patient. Preparation and supply of a pair of
ExoVasc implants personalised for a single patient is charged at £6,500
(approximately A$10,110 (at an exchange rate of A$1=£0.643)). The costs of surgical
implantation are unclear.
For the comparator procedures, the 100 per cent MBS service fee for repair or
replacement of the ascending thoracic aorta with aortic valve replacement or repair

External aortic root support in Marfan syndrome: November 2012 9
is A$3,046.80 (Table 1). This fee does not include associated hospital costs or the
costs of the prosthesis. The total cost for coronary artery bypass grafting (CABG)
surgery with cardiopulmonary bypass in a tertiary cardiothoracic centre in the United
Kingdom has recently been estimated at $7,43121 (approximately A$11,559).
However, it must be noted that aortic replacement surgery is more complex, takes
longer and has greater risks than CABG, therefore is likely to cost more.
Ethical, cultural or religious considerations
No ethical, cultural or religious concerns were identified relating to the use of the
external aortic root supports. Due to the relatively rare nature of Marfan syndrome,
high quality trials or EARS with large numbers of participants may not be possible.
Other issues
Change in the diameter of the aorta is the most important variable determining the
likelihood of dissection in Marfan syndrome. Studies with long-term follow-up are
necessary to inform on the stability of aortic root diameter in EARS patients.12
Clinical trial databases - clinicaltrials.gov, Current Controlled Trials (www.controlled-
trials.com), WHO International Clinical Trials Search Portal
(www.apps.who.int/trialsearch/) and Australian New Zealand Clinical Trials Registry
(www.anzctr.org.au) were searched using the terms EARS or ExoVasc to identify
trails currently in progress. No trials were identified as of 24 September 2012.
One of the authors, Tal Golesworthy, is a shareholder and director of Exstent limited,
which holds intellectual property in the EARS project. He is also the first recipient of
EARS.20 Professor John Pepper, a consultant surgeon of Royal Brompton Hospital and
Harefield NHS Trust, and Professor Tom Treasure are clinical advisors to the Exstent
Limited and also authors of the included studies.
Current guidelines of NICE (UK) indicate that the procedure should be only used with
special arrangements for clinical governance, consent and audit or research.13 In the
UK, the procedure appears to be undertaken under local health board approval and
is subject to formal progress and adverse events reporting.
Summary of findings
The evidence included in this technology brief is limited by a single patient cohort of
twenty patients. Based on this cohort, no deaths, late events or detected changes in
aortic valve function were reported following placement of the device. However, two
adverse events were reported: a postoperative cardiac arrest that was resolved after
removing the anterior closing suture on the device, and one technical problem of an
ill-fitting device that necessitated a second procedure for successful implantation.

External aortic root support in Marfan syndrome: November 2012 10
The studies did not provide a long-term comparison of change of ascending aorta
diameter, which is likely to be the primary outcome of interest. Median 20 month
follow-up on 16 patients showed a median aortic root reduction of 1 mm;6 therefore,
aorta diameter can be maintained. Comparison with a matched cohort who
underwent aortic root replacement surgery showed that the EARS procedure is
much less invasive than aorta replacement surgery, including avoidance of
cardiopulmonary bypass and a reduced risk for myocardial ischemia.
HealthPACT assessment
Based on the evidence from low-level studies which were based on a single cohort of
20 patients, and given the potential uptake of the device is very low, it is
recommended that the technology brief be archived.
Number of studies included
All evidence included for assessment in this Technology Brief has been assessed
according to the revised NHMRC levels of evidence. A document summarising these
levels may be accessed via the following link on the HealthPACT web site.
Total number of studies: 3
Total number of level lll-3 studies: 1
Total number of level IV studies: 2
References
1. Judge, D. P. & Dietz, H. C. (2005). 'Marfan's syndrome'. Lancet, 366 (9501), 1965-76.
2. Ramirez, F. & Dietz, H. C. (2007). 'Marfan syndrome: from molecular pathogenesis to clinical treatment'. Curr Opin Genet Dev, 17 (3), 252-8.
3. Ranasinghe, A. (2011). 'EASILY MISSED? Acute aortic dissection'. British Medical Journal, 343 (7818), 317.
4. CSANZ (2011). Guidelines for the diagnosis and management of Marfan Syndrome. [Internet]. The Cardiac Society of Australia and New Zealand. Available from: http://www.csanz.edu.au/LinkClick.aspx?fileticket=Kh0nvYrYlV0%3D&tabid=148 [Accessed 25 September 2012].
5. Rehders, T. C., Ince, H., Nienaber, C. A. 'Aortic dissection: from aetiology to therapeutic management'. Aortic dissection: Elsevier Ltd.; 2006.
6. Pepper, J., Golesworthy, T. et al (2010a). 'Manufacturing and placing a bespoke support for the Marfan aortic root: description of the method and technical results and status at one year for the first ten patients'. Interact Cardiovasc Thorac Surg, 10 (3), 360-5.

External aortic root support in Marfan syndrome: November 2012 11
7. Benedetto, U., Melina, G. et al (2011). 'Surgical management of aortic root disease in Marfan syndrome: a systematic review and meta-analysis'. Heart, 97, 955-8.
8. Kim, S. Y., Martin, N. et al (2005). 'Management of aortic disease in Marfan Syndrome: a decision analysis'. Arch Intern Med, 165 (7), 749-55.
9. Exstent (2012). ExoVasc® External Aortic Root Support. [Internet]. Exstent limited. Available from: www.exstent.com [Accessed 21 September 2012].
10. Williams, A., Davies, S. et al (2008). 'Medical treatment of Marfan syndrome: a time for change'. Heart, 94 (4), 414-21.
11. AIHW (2012). Marfan syndrome, Hospital data. [Internet]. Australian Institute of Health and Welfare. Available from: http://www.aihw.gov.au/hospitals-data/ [Accessed 25 September 2012].
12. NICE (2010). Interventional procedure overview of external aortic root support in Marfan syndrome. [Internet]. National Institute for Health and Clinical Excellence. Available from: http://www.nice.org.uk/nicemedia/live/13160/52568/52568.pdf [Accessed 21 September 2012].
13. NICE (2011). External aortic root support in Marfan syndrome, Interventional procedure guidance 394. [Internet]. National Institute for Health and Clinical Excellence. Available from: http://guidance.nice.org.uk/IPG394 [Accessed 25 September 2012].
14. Bentall, H. & De Bono, A. (1968). 'A technique for complete replacement of the ascending aorta'. Thorax, 23 (4), 338-9.
15. Kirsch, M. E., Ooka, T. et al (2009). 'Bioprosthetic replacement of the ascending thoracic aorta: what are the options?' Eur J Cardiothorac Surg, 35 (1), 77-82.
16. Treasure, T. (2010). 'The evolution of aortic root surgery for Marfan
syndrome'. Interact Cardiovasc Thorac Surg, 10 (3), 353-5.
17. Treasure, T. & Pepper, J. R. (2011). 'Aortic root surgery in Marfan syndrome'. Heart, 97 (12), 951-2.
18. MBS (2012). MBS Search Results - aorta [Internet]. Australian Government Department of Health and Ageing. Available from: http://www9.health.gov.au//mbs/search.cfm?q=aortic+valve+replacement&sopt=S [Accessed 25 September 2012].
19. Treasure, T., Crowe, S. et al (2012). 'A method for early evaluation of a recently introduced technology by deriving a comparative group from existing clinical data: a case study in external support of the Marfan aortic root'. BMJ Open, 2 (2), e000725.
20. Pepper, J., John Chan, K. et al (2010b). 'External aortic root support for Marfan syndrome: early clinical results in the first 20 recipients with a bespoke implant'. J R Soc Med, 103 (9), 370-5.
21. Al-Ruzzeh, S., Epstein, D. et al (2008). 'Economic evaluation of coronary artery bypass grafting surgery with and without cardiopulmonary bypass: cost-

External aortic root support in Marfan syndrome: November 2012 12
effectiveness and quality-adjusted life years in a randomized controlled trial'.
Artif Organs, 32 (11), 891-7.
Search criteria to be used (MeSH terms)
Marfan Syndrome (MeSH); Aorta, Thoracic (MeSH); Aortic Aneurysm, Thoracic
(MeSH); Aneurysm, Dissection (MeSH).