Embed Size (px)
Citation preview

ORIGINAL ARTICLE
Extent of Pancreatic Fibrosis as a Determinant of SymptomResolution After the Frey Procedure: A Clinico-pathologicAnalysis
Michol A. Cooper & Martin A. Makary & Julie Ng &
Yunfeng Cui & Vikesh K. Singh & Karen Matsukuma &
Dana K. Andersen
Received: 11 June 2012 /Accepted: 21 November 2012# 2013 The Society for Surgery of the Alimentary Tract
AbstractObjective The aim of this study was to evaluate the association of histopathologic features of chronic pancreatitis and painrelief after the Frey procedure.Design We retrospectively analyzed 35 patients who underwent the Frey procedure for chronic pancreatitis over a 5-yearperiod (November 2005 to February 2011).Setting Thirty-five patients with varied etiologies of chronic pancreatitis and persistent symptoms were referred to a multi-disciplinary pancreatitis clinic where a consensus decision to recommend surgery was established. The Frey procedure wasthen performed.Main outcome measures We compared symptomatic outcomes with the degree of pancreatic fibrosis, duct dilatation, andpresence of pancreatic duct stones based on a blinded evaluation of resected pancreatic tissue.Results Symptom resolution was associated with severe or extensive (>75 %) fibrosis and absence of symptom resolutionwas associated with mild or minimal (<25 %) fibrosis (chi-squared, p value<0.05). Symptom resolution was associatedwith pancreatic duct >4 mm and absence of symptom resolution was associated with pancreatic duct ≤4 mm (chi-squared,p value<0.05). There was no difference in outcomes for patients with and without pancreatic duct stones.Conclusion Symptom resolution after the Frey procedure is more likely in the setting of severe or extensive fibrosis due tochronic pancreatitis.
Keywords Chronic pancreatitis . Pancreatic fibrosis . Freyprocedure
Introduction
Chronic pancreatitis causes functional disability, nutritionaldeficiency, and glucose dysregulation.1 The principal symp-tom that prompts diagnosis and treatment of the disease ispain.1,2 Medical, endoscopic, and surgical interventions havebeen advocated for pain relief, and in many patients all threeapproaches are employed. The medical treatment of chronicpancreatitis-associated pain usually fails in that narcotic de-pendency occurs in almost all patients. Even in those patientsin whom narcotic requirements are decreased with medicaltherapy, there is almost universal development of endocrinedysfunction and permanent disability.3 The endoscopic treat-ment of pancreatic duct stones and strictures is widely used,but recurrence of symptoms and the need for repeated proce-dures is common.4–6 In contrast, surgical treatment of chronicpancreatitis has been shown to eliminate pain in up to 87 % of
M. A. Cooper (*) :M. A. Makary : J. Ng :Y. Cui :D. K. AndersenDepartment of Surgery, Johns Hopkins Hospital,Blalock 655, 600 N. Wolfe St.,Baltimore, MD 21231, USAe-mail: [email protected]
V. K. SinghDepartment of Medicine, Johns Hopkins University,Baltimore, MD, USA
K. MatsukumaDepartment of Pathology, Johns Hopkins Pancreatitis Clinic,Baltimore, MD, USA
J Gastrointest SurgDOI 10.1007/s11605-012-2110-4

patients and return patients to pre-disease employment andquality-of-life status.7–13 Despite the evidence of improvedoutcomes with surgery, surgical therapy is reserved forpatients in whom other therapies have failed and who haveincapacitating pain or anorexia with a history and radiographicfeatures consistent with chronic pancreatitis.
Surgical therapies for chronic pancreatitis include denerva-tion, resection (with or without islet auto-transplantation),drainage (decompression), and hybrid (decompression com-bined with limited resection) procedures. These proceduresare used variably depending on the nature of the pancreatitis,the presence of anatomic abnormalities such as ductal dilata-tion, the response to prior interventions, and surgeon prefer-ence and experience.2 Surgical denervation procedures havebeen shown to be largely ineffective or infeasible as first-linetreatment, so that operative strategies have largely focused onresection, drainage, and hybrid procedures.2 However, it hasbeen demonstrated that the outcome of surgery depends lesson the procedure used and more on the preoperative severityand postoperative progression of the chronic pancreatitis.12
Despite surgical intervention, 15–35 % of patients have noimprovement in their pain symptoms after an operativeprocedure.2,8 There have been several studies attempting tocorrelate pre- and postoperative findings with pain relief.Current theories of the cause of pain in chronic pancreatitisinclude ductal hypertension with activation of stretch fibersand peripancreatic sensory nerve damage.2 Duct diameter,ductal hypertension, and severity of pain have not been con-sistently correlated with postoperative pain relief.14–16 Perio-perative pain severity has been correlated with histologicchanges in the pancreas including small cysts, foci of acinarcell necrosis, and areas of acute inflammation.17 However, theimpact of the extent of underlying fibrosis on the postopera-tive outcome has remained poorly understood.18
In this study, we hypothesized that patients with severe orextensive fibrosis have a higher rate of pain relief from surgerythan those with minimal or mild fibrosis. We also hypothe-sized that the presence of pancreatic duct stones is associatedwith a higher likelihood of pain relief. Finally, we hypothe-sized that pancreatic duct dilation is associated with a betterresponse to surgery. To test these hypotheses, we comparedthe results of a blinded histopathologic analysis of resectedpancreatic tissue as well as the results of preoperative imagingstudies with the symptomatic outcomes achieved after onetype of procedure performed for chronic pancreatitis.
Materials and Methods
Patients
We analyzed 35 consecutive patients who underwent the localresection of the pancreatic head with longitudinal pancreatico-
jejunostomy (LR–LPJ), or Frey procedure, over a 5-yearperiod (November 2005 to February 2011) for docu-mented chronic pancreatitis (CP) accompanied by persis-tent pain. All had one or more strictures, pseudocysts, orintraductal stones, which were accompanied by persistentpain that was refractory to medical and endoscopic treat-ment, and all had documented chronic inflammation ongross and/or microscopic analysis of the excavated tissueremoved from the pancreatic head.
Of the 35 patients in this study, 21 (60 %) were maleand the mean age was 55 years with a range from 22 to77 years at the time of surgery. Median preoperativeduration of CP with pain was 60.9 months with a rangeof 2.4–244 months. Thirty-four percent of patients haddisease due to alcohol abuse, 29 % were idiopathic inetiology, and 23 % had antecedent gallstone disease.Additionally, 66 % had undergone previous endoscopictherapy and 31 % were diabetic. Other characteristics ofthe CP and their prevalence in our patient populationare listed in Table 1.
Perioperative Evaluation
Preoperatively, contrast-enhanced computerized tomo-graphic (CT) scans were obtained on all patients andendoscopic ultrasound was performed on 10 (29 %) ofthe patients. The presence of pancreatic duct stones andthe degree of pancreatic duct dilatation were documentedbased on the most recent preoperative CT scan. Based oneach patient’s history of failure to resolve symptomsdespite medical and endoscopic treatment, a consensusdecision to recommend surgery was established by at-tending physicians in a multi-disciplinary pancreatitisclinic to which the patients were referred. All patientsunderwent preoperative evaluations by primary care and
Table 1 Etiologies of chronic pancreatitis in the experimental group
Etiology Number ofpatients
Percent ofpatients (%)
Alcohola 12 34
Idiopathic 10 29
Gallstonea 8 23
Pancreas divisum 4 11
Autoimmuneb 1 3
Sphincter of Oddi dysfunction 1 3
Etiologies included alcohol, idiopathic, gallstone, pancreas divisum,autoimmune, and sphincter of Oddi dysfunctiona One patient had both a history of heavy alcohol use and alcohol-induced acute pancreatitis as well as gallstones, and they are thus listedunder both etiologiesb One patient diagnosed preoperatively as idiopathic was found to havehistologic evidence of autoimmune pancreatitis
J Gastrointest Surg

anesthesiology personnel and were approved for surgery.The Frey procedure was performed by two surgeonsusing the method previously described.19
Intraoperatively, the resected pancreatic tissue wasevaluated by frozen section analysis to rule out malig-nancy. Formalin-fixed tissue was subsequently analyzedfor the degree (percent) of fibrosis based on hematoxylinand eosin (H&E) stained serial sections of the resectedtissue. To assess the degree of fibrosis, we used a fibro-sis scoring system based on one previously described byKloppel and Maillet.20 We used their definitions forperilobular and intralobular fibrosis and then further re-fined the criteria based on our study goals. To determinethe area of fibrosis in a sample, an experienced pancre-atic pathologist who was blinded to the outcome statusof each patient performed a visual estimate at ×20 mag-nification. The percent fibrosis for that sample was cal-culated by dividing the area of fibrosis by the totalparenchymal surface area. This was executed twice atseparate times. This was performed for all availableslides from the case. A mean value was then calculatedfor each subject. An average of five slides (range 2–14slides) were examined for each sample. In patients withmultiple pathology samples, the degree of fibrosis amongsamples was averaged.
Follow-Up
Thirty-four of 35 patients survived the postoperativeperiod; the one death in this series was secondary topneumonia 3 weeks after surgery. The 34 survivingpatients were followed in a series of clinic appointmentswhere pain status, continued narcotic dependency, andability to work and/or function were assessed. Symptomresolution was categorized as a dichotomous variable(complete or significant diminution of pain symptomswere coded as pain resolution, whereas persistence ofunchanged or minimally decreased symptoms was codedas no pain resolution). The average follow-up period was22 months (range 3–66 months).
Symptom resolution was compared to the mean percentof fibrosis recorded on serial sections of the resectedtissue. For analysis of the association of pain relief withthe degree of fibrosis, the patients were divided intogroups defined as (A) severe or extensive fibrosis (SEF)for those with greater than 75 % fibrosis, (B) intermediatefibrosis (INF) for those with 25–75 % fibrosis, and (C)minimal or mild fibrosis (MIF) for those with less than25 % fibrosis. Symptom resolution was also assessed withregard to duct dilatation, where duct dilatation was de-fined as a pancreatic duct >4 mm,15 and with regard to thepresence or absence of pancreatic duct stones as determinedby preoperative imaging.
Results
Symptom Resolution Versus Fibrosis
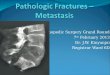
Of the 34 patients who were followed postoperatively,14 patients (41 %) had SEF on final pathology, sevenpatients (21 %) had INF, and the remaining 13 patients(38 %) had MIF. Representative histologic features ofminimal and extensive pancreatic fibrosis are shown inFig. 1.
The degree of fibrosis versus pain relief for all of thepatients is shown in Fig. 2. Of the 14 SEF patients, 11(79 %) had complete or near-complete resolution ofsymptoms and disability. Of the seven INF patients, five(71 %) had complete or near-complete pain resolution.Of the 13 MIF patients, eight (62 %) had completeor near-complete resolution of symptoms and disability(Table 2). A chi-squared analysis showed that symptomresolution was associated with SEF and no symptomresolution was associated with MIF (p 0 0.01). Therewas also a clear trend of increasing pain resolution withhigher rates of fibrosis (Fig. 3). Pain resolution rangedfrom 60 % for the 10 patients with less than 10 %fibrosis to 100 % pain resolution for the 10 patients withgreater than 80 % fibrosis.
The presence of pancreatogenic, or type 3c, diabetespreoperatively as well as the requirement for endoscopictherapy were also likely indicators of the severity of theunderlying chronic pancreatitis. Chi-squared analysis dem-onstrated that there was also an association between thepresence of preoperative diabetes and pain resolution afterthe LR–LPJ procedure (p 0 0.005) as well as between theuse of previous endoscopic therapy and pain relief after theLR–LPJ (p 0 0.002).
Postoperatively, continued opioid use was common, andwas reported in eight (57 %) of SEF patients, four (57 %) ofintermediate fibrosis, and in four (33 %) of MIF patients.However, opioid use typically decreased progressively overtime, and the patients’ ability to return to work and/ornormal activities correlated with symptom resolution. Also,most patients reported that, in contrast to preoperativesymptoms, they now had complete pain relief with opioidswhen pain occurred.
b
Fibrosis (replacing pancrea cparenchyma)
a
Perilobularfibrosis
Fig. 1 Pancreatic tissue pathology with varying degrees of fibroticchange. a Minimal fibrotic change with 10 % fibrosis and 85 % acinarcells. b Severe extensive fibrotic change with 90 % fibrosis and 5 %acinar cells
J Gastrointest Surg

Symptom Resolution Versus Duct Dilatation and Presenceof Pancreatic Duct Stones
Of the 23 patients with pancreatic duct dilatation (defined asduct >4 mm), 17 (74 %) had complete or near-completesymptom resolution. Of the 11 patients with no pancreaticduct dilatation, seven (63 %) had complete or near-completesymptom resolution (Table 3). A chi-squared analysisshowed symptom resolution was associated with pancreaticduct >4 mm and no symptom resolution was associated withpancreatic duct <4 mm (p<0.05).
Of the eight patients with pancreatic duct stones, six(75 %) had complete or near-complete symptom resolu-tion. Of the 26 patients without stones, 21 (81 %) hadcomplete or near-complete symptom resolution (Table 4).A chi-squared analysis showed no improvement in painrelief with the presence of pancreatic duct stones versus nostones (p00.23).
Discussion
Although randomized, prospective trials have shown surgi-cal therapy to be superior to endoscopic management ofsymptoms,21,22 controversy persists over the selection ofpatients for surgery and the selection of operative approach.A randomized, prospective trial of surgical treatment (thePuestow procedure) versus continued medical management
of 83 patients classified as having “mild or moderate” ob-structive chronic pancreatitis showed that 78 % of patientstreated medically progressed to “severe” disease over a 24-month period, whereas only 13 % of surgically treatedpatients demonstrated the same progression.23 The sameconclusion was found in a 26-year study of 388 patientstreated with the duodenum-preserving pancreatic head re-section (DPPHR) or Beger procedure.24 This finding sug-gested that operative treatment earlier in the course of thedisease might prevent or delay progressive dysfunction. Theoptimal timing of surgical intervention, vis-à-vis the severityof the disease, has not been established, however.
Hybrid procedures, which combine limited resection withdecompression, have been shown to achieve the same effi-cacy of long-term pain relief associated with resectionalprocedures but with the lower morbidity and mortality ofdecompression approaches.2 One type of hybrid procedure,the LR–LPJ, or Frey procedure, combines local resectionof the pancreatic head with longitudinal pancreatico-jejunostomy.22,25 In this procedure, excavation of the centralcore of the pancreatic head without division of the pancre-atic neck has been shown to be associated with reducedmorbidity but similar long-term pain resolution comparedto proximal pancreatectomy or the duodenum-preservingpancreatic head resection (DPPHR) procedure.23–28 In ourexperience, the Frey procedure is associated with fewerearly or late postoperative complications than pancreatico-duodenectomy or the DPPHR procedure and minimizes therisk of pancreatico-jejunostomy stricture. For these reasons,
Fig. 2 Percent fibrosis versus postoperative pain relief. Each diamondrepresents one patient
Table 2 Symptom relief with minimal (<25%), intermediate (25–75%),and severe extensive (>75 %) fibrosis
<25 %Fibrosis
25–75 %Fibrosis
>75 %Fibrosis
Symptom relief 8 5 11
No symptom relief 5 2 3
Fig. 3 Percent of patients with pain relief for those with mild orminimal (MIF, n 0 13), intermediate (INF, n 0 7), and severe orextensive (SEF, n 0 14) fibrosis. There is a trend of increasing symp-tom relief with higher percentage of fibrosis. p<0.05 for MIF vs. SEFgroups by chi-square analysis
Table 3 Symptom relief with pancreatic duct dilatation >4 mm versus≤4 mm
Pancreatic duct>4 mm
Pancreatic duct≤4 mm
Symptom relief 17 7
No symptom relief 6 4
J Gastrointest Surg

in the absence of a mass suspicious for malignancy, the Freyprocedure is our procedure of choice for chronic pancreatitispatients with evidence of obstructive pancreatopathy andpersistent symptoms.
Our data show that the degree of pancreatic fibrosiscorrelates with the resolution of pain symptoms in a seriesof patients treated with the Frey procedure. Our findingssuggest that the pain in patients with extensive fibrosis,possibly as a consequence of more advanced injury due torecurrent or chronic inflammation, may be better alleviatedby the combination of limited surgical resection and drain-age than those with recurrent or chronic inflammation ac-companied by only minimal degrees of pancreatic fibrosis.Of the 14 patients with greater than 75 % fibrosis, 11 (79 %)had pain relief; of the seven patients with between 25 % and75 % fibrosis, five (71 %) had pain relief; of the 13 patientswith less than 25 % fibrosis, eight (62 %) had pain reliefafter surgery. Additionally, of the 10 MIF patients with only0–10 % fibrosis, only six (60 %) had complete or near-complete resolution of symptoms and disability, whereasin those 10 patients with >80 % fibrosis, all had completeor near-complete resolution of symptoms. A chi-squaredanalysis showed that symptom resolution was associatedwith severe or extensive fibrosis and no symptom resolutionwas associated with mild or minimal fibrosis (p<0.05).
The positive correlation of degree of fibrosis and painrelief after the LR–LPJ procedure was further supported byour findings that there was an association between preoper-ative diabetes and postoperative pain relief as well as pre-operative endoscopic therapy and postoperative pain relief.Pancreatogenic diabetes due to advanced chronic pancreati-tis and the need for endoscopic intervention both indicate agreater severity of disease, and both of these historicalfeatures correlated with the degree of fibrosis.
Our findings imply that the presence of only mild orminimal fibrosis may decrease the likelihood of symp-tom resolution after the Frey procedure. They also sug-gest that patients with pain refractory to medical orendoscopic management who nevertheless harbor mildor minimal pancreatic fibrosis may respond more favor-ably to other procedures such as total pancreatectomywith islet auto-transplantation.
The degree of preserved acinar cell mass in our resectedspecimens was seen histologically to represent the reciprocal
of the degree of fibrosis. It is unclear if the presence of anincreased acinar cell mass or the persistence of peri-neuralinflammatory events resulted in continued pain in those withmild or minimal fibrosis. As with prior studies, we found nostatistically significant difference in pain resolution related tothe presence of pancreatic duct stones.
All of the patients in our study had evidence of ob-structive pancreatopathy due to pancreatic duct strictures,stones, or compression. Most (23/34) patients demonstrat-ed significant duct dilatation (>4 mm), but as a minoritydid not, we sought to evaluate whether ductal dilatationwas a predictor of pain relief in our patients. Althoughprevious studies have concluded that the effectiveness ofthe Frey or Beger procedure is not affected by the degreeof duct dilatation,29,30 our study did reveal an associationbetween duct dilatation greater than 4 mm and pain relief.One possible reason for this finding is that of the 11patients with minimal duct dilatation (≤4 mm), seven(64 %) also had mild or moderate fibrosis. Therefore, tothe extent that duct dilatation was a consequence of pro-gressive fibrosis in our patients, a higher likelihood ofpain resolution was found to be associated with bothcharacteristics. The number of patients with severe fibro-sis and no ductal dilatation in our series was too small formeaningful comparison, however, so our results shouldnot be interpreted to indicate that ductal dilatation is anindependent predictor of pain resolution after the Freyprocedure.
As pancreatic imaging technology continues to im-prove, it may be possible to better correlate the degreeof fibrosis seen on preoperative imaging with the actualdegree of fibrosis found in the resected pancreas. If theextent of pancreatic fibrosis can be reliably determinedpreoperatively, this might serve as an important addi-tional variable with which the likelihood of relief fromsymptoms by a surgical intervention could be moreaccurately predicted.
This study has some important limitations, including thatpain resolution was treated as a dichotomous variable tofocus on patients who did not have any pain relief. Further,our series of patients is modest, and follow-up has been, onaverage, less than 2 years. Therefore, continued observationof a larger series of patients is needed to confirm these initialfindings. In addition, stone disease can be difficult to dis-tinguish from duct calcifications, and this study was notadequately powered to study stone disease. While the pres-ence of stones did not impact pain outcomes in this series, itis well documented that patients are relieved of their painafter endoscopic extraction or surgical decompression inwhich pancreatic duct calculi are removed. Finally, fur-ther research is needed to better identify other patholog-ic and radiographic features which may be associatedwith improved outcomes.
Table 4 Symptom relief with pancreatic ducts stones versus withoutstones
Pancreaticduct stones
No pancreaticduct stones
Symptom relief 6 21
No symptom relief 2 5
J Gastrointest Surg

Conclusion
Complete or near-complete symptom resolution after the Freyprocedure is highly likely in the setting of severe or extensivefibrosis due to CP. Despite ductal dilatation or the presence ofpancreatic duct stones, mild or minimal fibrosis is associatedwith a lower likelihood of symptom resolution after the Freyprocedure. Improved methods to quantify the degree of pan-creatic fibrosis preoperatively may allow a more precise pre-diction of the success of the Frey procedure to relieve painsymptoms in CP patients, and allow a more informed recom-mendation of the selection of surgical therapy for this disease.
Acknowledgment Presented, in part, at the annual meeting of theAmerican Pancreatic Association, Chicago, IL, November 5, 2010
References
1. Fisher WE, Andersen DK, Bell RH Jr, Saluja AK, Brunicardi FC.Pancreas. In: Brunicardi FC, Andersen DK, Billiar TR, Dunn DL,Hunter JG, Matthews JB, Pollock RE (Eds). Schwartz’s Principlesof Surgery, 9th Ed. McGraw-Hill. New York, 2010, pp 1167–1243.
2. Andersen DK, Frey CF. The evolution of the surgical treatment ofchronic pancreatitis. Ann Surg 2010; 251(1):18–32.
3. Lankisch PG, Lohr-Happe A, Otto J, Creutzfeldt W. Natural coursein chronic pancreatitis. Pain, exocrine and endocrine pancreaticinsufficiency and prognosis of the disease. Digestion 1993;54(3):148–155.
4. Jacob L, Geenen JE, Catalano MF, et al. Prevention of pancreatitisin patients with idiopathic recurrent pancreatitis: A prospectivenon-blinded randomized study using endoscopic stents. Endoscopy2001; 33: 559–64.
5. Heyries L, Barthet M, Delvasto C, et al. Long-term results ofendoscopic management of pancreas divisum with recurrent acutepancreatitis. Gastrointest Endosc 2002; 55: 376–81.
6. Gabbrielli A, Mutignani M, Pandolfi M, et al. Endotherapy of earlyonset idiopathic chronic pancreatitis: Results with long-termfollow-up. Gastrointest Endosc 2002; 55: 488–93.
7. Buchler MW, Friess H, Muller MW, Wheatley AM, Beger HG.Randomized trial of duodenum-preserving pancreatic head resec-tion versus pylorus-preserving Whipple in chronic pancreatitis.Am J Surg 1995 Jan;169(1):65–9; discussion 69–70
8. Hartel M, Tempia-Caliera AA, Wente MN, Z'graggen K, Friess H,Buchler MW. Evidence-based surgery in chronic pancreatitis. Lan-genbecks Arch Surg 2003 Apr;388(2):132–139.
9. Nealon WH, Matin S. Analysis of surgical success in preventingrecurrent acute exacerbations in chronic pancreatitis. Ann Surg2001 Jun;233(6):793–800.
10. Sakorafas GH, Farnell MB, Nagorney DM, Sarr MG, RowlandCM. Pancreatoduodenectomy for chronic pancreatitis: long-termresults in 105 patients. Arch Surg 2000 May;135(5):517–23; dis-cussion 523–4.
11. Strate T, Taherpour Z, Bloechle C, Mann O, Bruhn JP, SchneiderC, et al. Long-term follow-up of a randomized trial comparing the
beger and frey procedures for patients suffering from chronicpancreatitis. Ann Surg 2005 Apr;241(4):591–598.
12. Riediger H, Adam U, Fischer E, Keck T, Pfeffer F, Hopt UT, et al.Long-term outcome after resection for chronic pancreatitis in 224patients. J Gastrointest Surg 2007 Aug;11(8):949–59; discussion959–60.
13. Howard TJ, Browne JS, Zyromski NJ, Lavu H, Baker MS, Shen C,et al. Mechanisms of primary operative failure and results ofremedial operation in patients with chronic pancreatitis. J Gastro-intest Surg 2008 Dec;12(12):2087–95; discussion 2095–6.
14. Ebbehoj N. Pancreatic tissue fluid pressure and pain in chronicpancreatitis. Dan Med Bull 1992 Apr;39(2):128–133.
15. Bradley EL, 3rd. Pancreatic duct pressure in chronic pancreatitis.Am J Surg 1982 Sep;144(3):313–316.
16. Manes G, Buchler M, Pieramico O, Di Sebastiano P, MalfertheinerP. Is increased pancreatic pressure related to pain in chronic pan-creatitis? Int J Pancreatol 1994 Apr;15(2):113–117.
17. Proca DM, Ellison EC, Hibbert D, Frankel WL. Major pancreaticresections for chronic pancreatitis. Arch Pathol Lab Med 2001Aug;125(8):1051–1054.
18. Hadidi A. Pancreatic duct diameter: sonographic measurement innormal subjects. J Clin Ultrasound 1983 Jan;11(1):17–22.
19. Makary MA, Andersen DK. What’s new in treating chronic pan-creatitis. Hybrid operations outperform traditional procedures.Contemp Surg 2007; 63: 172–6.
20. Kloppel G and Maillet B. Pseudocysts in chronic pancreatitis: amorphological analysis of 57 resection specimens and 9 autopsypancreata. Pancreas 1991 May; 6(3):266–74.
21. Bradley EL III. Long-term results of pancreaticojejunostomy inpatients with chronic pancreatitis. Ann Surg 1987; 153: 207
22. Cahen DL, Gouma DJ, Nio Y, et al. Endoscopic versus surgicaldrainage of the pancreatic duct in chronic pancreatitis. N Engl JMed 2007; 356: 676
23. Nealon WH, Thompson JC. Progressive loss of pancreatic functionin chronic pancreatitis is delayed by main pancreatic duct decom-pression. A longitudinal prospective analysis of the modifiedPuestow procedure. Ann Surg 1993; 217: 458–467.
24. Beger HG, Schlosser W, Friess HM, et al. Duodenum-preservinghead resection in chronic pancreatitis changes the natural course ofthe disease. A single-center 26-year experience. Ann Surg 1999;230: 512–520.
25. Frey CF, Smith GJ. Description and rationale of a new operationfor chronic pancreatitis. Pancreas 1987; 2: 701–7.
26. Farkas G, Leindler L, Daroczi M, et al. Prospective randomizedcomparison of organ-preserving pancreatic head resection withpylorus-preserving pancreaticoduodenectomy. Langenbecks ArchSurg 2006; 391: 338–42.
27. Köninger J, Seiler CM, Sauerland S, et al. Duodenum-preservingpancreatic head resection – a randomized controlled trial compar-ing the original Beger procedure with the Berne modification(ISRCTN No. 50638764). Surgery 2008; 143: 490–8.
28. Strate T, Bachmann K, Busch P, et al. Resection vs. drainage intreatment of chronic pancreatitis: Long-term results of a random-ized trial. Gastroenterol 2008; 134: 1406–11.
29. Ramesh H, Jacob G, Lekha V, et al. Ductal drainage with headcoring in chronic pancreatitis with small duct disease. J Hepato-biliary Pancreat Surg 2003; 10: 366–72.
30. Shrikhande SV, Kleeff J, Friess H, et al. Management of painin small duct chronic pancreatitis. J Gastrointest Surg 2006;10: 227–33.
J Gastrointest Surg