Embed Size (px)
Citation preview

C
Prostate Cancer: Radical Prostatectomy
Extended Lymphadenectomy “Step by Step”in Patients Undergoing RadicalProstatectomyDaniar Kurmanbekovich Osmonov, Chaojun Wang, Jorg Hoenle, Aleksej Aksenov,Claudius Hamann, Carsten Maik Naumann, and Klaus Peter Juenemann
OBJECTIVES To describe a surgical technique of pelvic lymph node dissection (PLND) in prostate cancerpatients. The idea was to standardize the procedure of PLND and to increase the significance oflymphadenectomy as a part of radical prostatectomy (RP). The best ways to achieve this are (1)to describe the surgical procedure in detail, (2) to improve the knowledge of metastatic spread,and (3) to improve the management of complications.
METHODS One-hundred six patients with localized prostate carcinoma were treated with RP, includingextended PLND. The number of removed lymph nodes (LNs) was correlated with histology andcompared with that reported in the literature. Our aim was to observe technical differences thatprobably accrue in clinical outcomes. We proposed a conceptual schema of PLND.
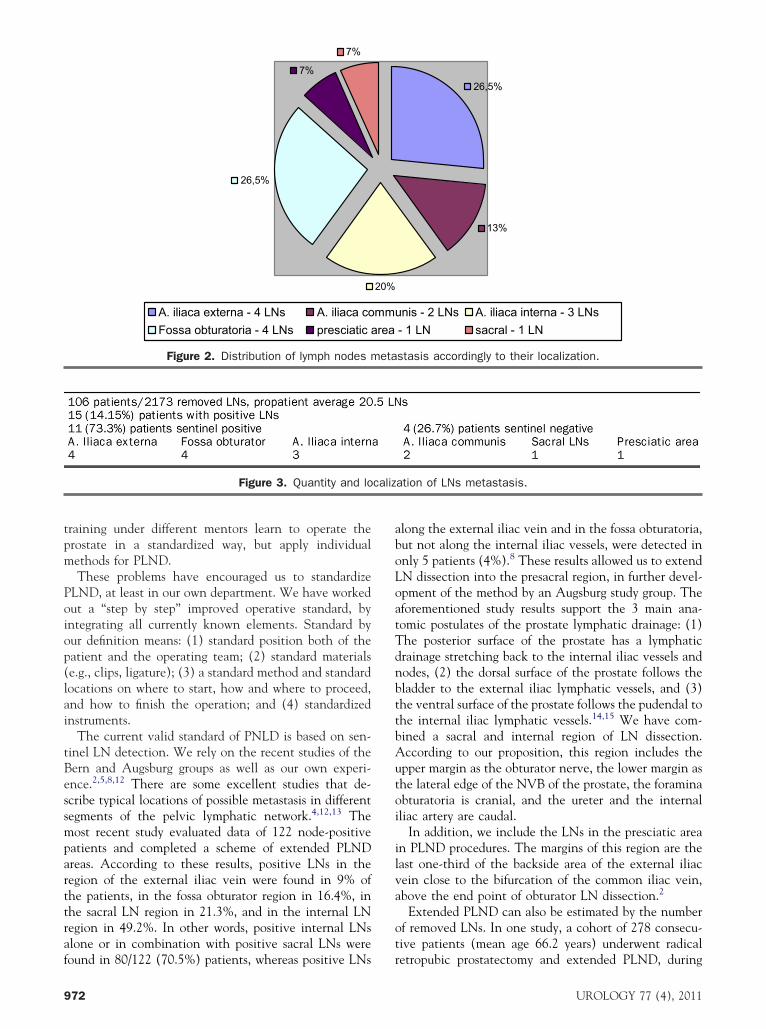
RESULTS LN metastases were detected in 15 of 106 patients (14.15%). Positive sentinel LNs were detectedin 11 of these 15 patients (73.3%). The average number of removed LNs was 20.5 (range �5).In 4 of 15 patients (26.5%), positive LNs were found in the fossa obturatoria; in 4 patients(26.5%) in the region of the external iliac artery; in 3 patients (20%) in the internal LN region;in 2 patients (13%) in the region of the common iliac artery; in 1 patient (7%) in the presciaticarea; and in 1 patient (7%) in the sacral region.
ONCLUSIONS The standard routine was: (1) dissection of LN tissue along the common iliac artery, (2)dissection of LN tissue in the presciatic area, (3) dissection of LN tissue parasacral, and (4)
peritoneal fenestration. UROLOGY 77: 969–975, 2011. © 2011 Elsevier Inc.ci
The specifics of lymphogenic drainage play an im-portant role in neoplastic progression of prostatecancer (pCA), which is crucial for the prognosis
of surgical outcome. We have analyzed these specificswith the purpose of optimizing and routinizing the oper-ative technique of open surgical pelvic lymph node dis-section (PLND) in pCA patients.
The technique of PLND has been developed on thebasis of classic standard PLND (dissection of obturatorlymph nodes [LNs], external and internal iliac vesselLNs) toward extended PLND (additional dissection ofthe common iliac vessel LNs up to the iliac crossing ofthe ureter, the fossa obturatoria LNs, the common iliacartery LNs, the sacral LNs, and the presciatic area LNs).
Classic PLND has been described in detail and hasbecome an integral part of radical prostatectomy (RP),1
which is generally mastered by surgeons. Even the devel-opment of laparoscopic procedures for pCA surgery has
From the Department of Urology, University Hospital Schleswig Holstein, Kiel, Ger-many
Reprint requests: Dr. med. D. K. Osmonov, Department of Urology, UniversityHospital Schleswig-Holstein, Kiel, Arnold-Heller-stra�e 7, D-24105 Kiel, Germany.
bE-mail: [email protected]
Submitted: December 24, 2009, accepted (with revisions): June 9, 2010
© 2011 Elsevier Inc.All Rights Reserved
not substantially affected the older standard. However,there are some features of laparoscopic procedures asso-ciated with the limitations of this method.2 Particularlyhallenging is LN dissection in the region of the internalliac artery and the presciatic area.2,3
Based on the most recent data, patients who under-went extended PLND showed an improvement of cancer-specific survival by up to 20%, without increasing therate of common surgical complications.4 The results ofsentinel-marked LN screening and extended PLND havedemonstrated an advantage of performing extended,rather than limited, PLND in “high-risk” patients.2,5 It istherefore extremely important to standardize and furtherrefine the method of extended PLND to promote a cer-tain routine in surgeons for better and faster handling ofthis method, while reducing the number of surgical mis-takes.
The principles of PLND are well known, but the actualperformance differs from clinic to clinic and depends onthe surgical conventions in each hospital. Conversely, arecent study shows that the surgeon with the highestsurgical experience removed more nodes and found morenodal metastases than less experienced surgeons.6 We
elieve, therefore that clearly defined operation stan-0090-4295/11/$36.00 969doi:10.1016/j.urology.2010.06.071
P he pr
dards in combination with the upgraded sentinel LNdetection principles can improve the oncological out-come of RP.
We have tried to optimize and standardize extendedPLND on the basis of the anatomical specifics of lym-phatic drainage in the pelvic area and the oncologicaloutcomes reported in different clinical studies.
MATERIAL AND METHODS
All patients (n � 106) underwent nerve-sparing or nonnerve-sparing RP. The number of removed LNs was correlated withhistologic LN status and compared with the literature.
We proceeded with the PLND as follows:
1. The patient was in the supine position and rotated to theside of LN dissection. After wound exposition of the fossaobturatoria by means of a Book-Walter retractor, a C-Trakgamma probe (AEA Technologies, Morgan Hills, CA) ws
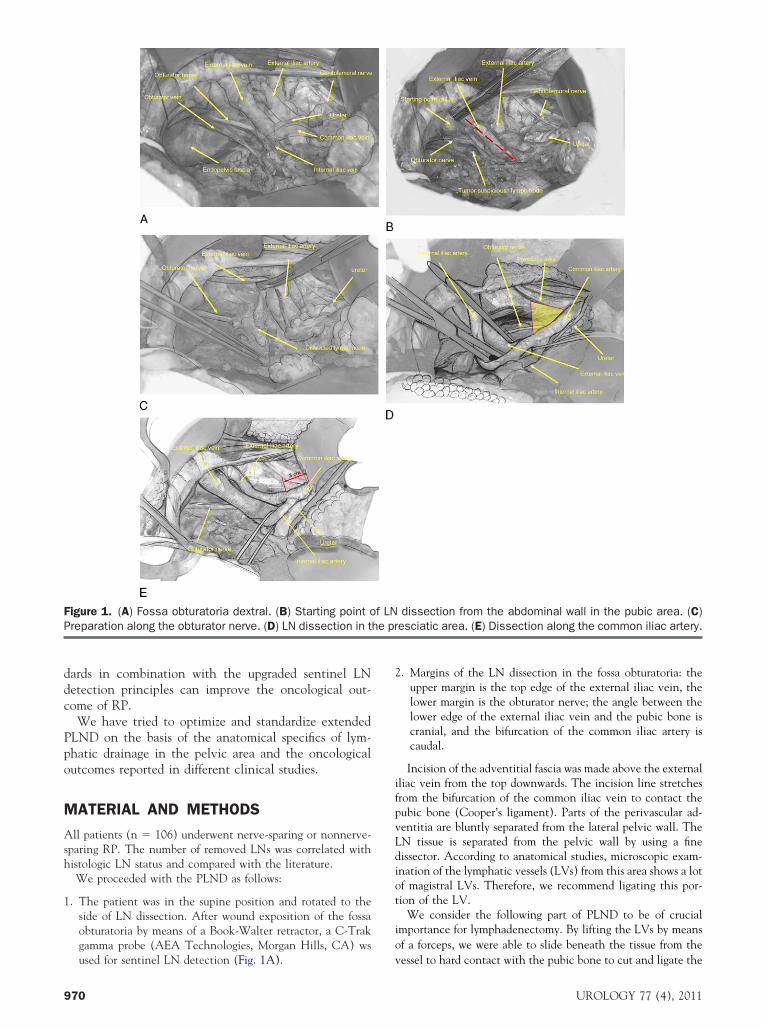
Figure 1. (A) Fossa obturatoria dextral. (B) Starting point oreparation along the obturator nerve. (D) LN dissection in t
used for sentinel LN detection (Fig. 1A).
970
2. Margins of the LN dissection in the fossa obturatoria: theupper margin is the top edge of the external iliac vein, thelower margin is the obturator nerve; the angle between thelower edge of the external iliac vein and the pubic bone iscranial, and the bifurcation of the common iliac artery iscaudal.
Incision of the adventitial fascia was made above the externaliliac vein from the top downwards. The incision line stretchesfrom the bifurcation of the common iliac vein to contact thepubic bone (Cooper’s ligament). Parts of the perivascular ad-ventitia are bluntly separated from the lateral pelvic wall. TheLN tissue is separated from the pelvic wall by using a finedissector. According to anatomical studies, microscopic exam-ination of the lymphatic vessels (LVs) from this area shows a lotof magistral LVs. Therefore, we recommend ligating this por-tion of the LV.
We consider the following part of PLND to be of crucialimportance for lymphadenectomy. By lifting the LVs by meansof a forceps, we were able to slide beneath the tissue from the
dissection from the abdominal wall in the pubic area. (C)esciatic area. (E) Dissection along the common iliac artery.
f LN
vessel to hard contact with the pubic bone to cut and ligate the
UROLOGY 77 (4), 2011

oriPotc
ahophR
LVs (Fig. 1B). This is the starting point for anatomical LNpreparation and dissection.
Parts of the adventitia are bluntly separated from the venouswall and the lateral pelvic wall. The minor LVs should beclipped by means of miniclips because their grip tends to bebetter than that of larger ones. We used Hemoclip Plus (Tele-flex Medical, Research Triangle Park, NC) (small and me-dium). Slight shifting of the dissected LN conglomerate tocranial helps to identify the obturator nerve (Fig. 1C). Further-more, gentle preparation is made strictly along and above theobturator nerve up to the meeting point with the internal iliacartery. We recommend retraction of the external iliac veinlaterally with a miniswab to expose the external obturatormuscle and the obturator veins, which are otherwise easilyinjured. We strongly recommend ligation of the prepared LNpacket as soon as the internal iliac artery is reached. In addi-tion, we systematically use miniclips to occlude lymphatic leak-age from the small peripheral LVs and to prevent lymphoceledevelopment.
3. The margins of sacral LN dissection include: the uppermargin is the obturator nerve, the lower margin is the lateraledge of the neurovascular bundle (NVB) of the prostate,cranial is the foramina obturatoria, caudal is the ureter.
Preparation is made along and above the obturator nerveusing miniclips from the top downward until contact with thefossa obturator and the preserved NVB of the prostate is ex-posed. The LN tissue in the fossa is ligated between the obtu-rator nerve and NVB. Gentle exposition, clipping, and dissec-tion are performed along the lateral edging of the NVB. In thisarea, the LNs have contact with the whole surface of the pelvicfloor through the connective tissue and small lymphatic vessels.Therefore, we recommend subtle clipping and careful dissectionto clear the undersurface and to expose the obturator muscle.We do not support the conventional method of uncontrolledpulling out of fat tissue with a surgical forceps in this region,because of the risk of lymphoceles and the adjacency of NVB.
The ureter, which ascends with the peritoneum, is identifiedand hitched. The crossing of the ureter at the bifurcation of thecommon iliac artery marks the caudal end of the dissection. TheLN tissue is separated from the ureter using a fine dissector. Werecommend ligating this portion of the LNs and not clipping it,or otherwise combining the clipping and ligation.
4. LN dissection in a so-called presciatic area include the lastone-third of the backside area of the external iliac vein closeto the bifurcation of the common iliac vein, above the endpoint of obturator LN dissection (Fig. 1D).
The external iliac artery and external iliac vein in the centerare hitched with a vessel loop. Further dissection starts fromcranial, beginning from the lateral pelvic wall downward tothe meeting point with the fossa obturator. Using a miniswab,the obturator nerve is moved medially to avoid a nerve in-jury. The dissector is moved downward along the nerve untilcontact with the pelvic bone and the branches of the instru-ment are carefully spread apart. Ligation in this region is com-plicated; therefore, we recommend double clipping with mini-clips.
5. LN dissection along the common iliac artery. Dissection andclipping is done in the same way in the caudal direction,with a careful stump separation of the LNs down from the
pelvic wall using a miniswab. We recommend pulling the vUROLOGY 77 (4), 2011
external iliac artery to lateral after reaching three-quarters ofthe dissection length, to clear the surface of the commoniliac vein. We recommend removal of LN tissue of at least 3cm along the common iliac artery or up to the ureter crossingpoint (Fig. 1E).
RESULTSHistologically, proven lymph node metastases were de-tected in 15 of 106 patients (14.15%). These 15 patientshad a prostate-specific antigen level �10 ng/mL or aGleason score �6, and a tumor stage of at least pT2.Positive sentinel lymph nodes were detected in 11 ofthese 15 patients (73.3%). The average number of re-moved lymph nodes was 20.5 (range �5). In 4 of 15patients (26.5%), positive LNs were found in the fossaobturator, and in another 4 patients (26.5%) in theregion of the external iliac artery; in 3 patients (20%)positive LNs were found in the internal LN region; in 2patients (13%) in the region of the common iliac artery;in 1 patient (7%) in the presciatic area; and in 1 patient(7%) in the sacral region (Fig. 2, Fig. 3 ).
The most common postoperative complication waslymphocele, which was diagnosed in 13 of 106 patients(12.3%). In 10 of these 13 patients (77%), the lympho-cele was treated successfully by means of lymphocelepunction, aspiration, and instillation of tetracycline. Thelymphocele was recurrent in three (23%) of these 13patients. We proceeded with a laparoscopic fenestrationof the lymphocele, which was performed bilaterally inthese 3 patients. One patient developed a pulmonaryembolism and underwent surgical revision after conser-vative anticoagulative surgery. We had no patients withlymphedema of the lower extremities.
COMMENTWe are not trying “to reinvent the bicycle” regardingPLND. The indications and therapeutic benefit of PLNDand its dependency on staging, as well as the complica-tions that are to be expected, have been well-establishedin the literature. However, there are a few recent publi-cations that have persuaded us to revise the establishedmethods critically.4,7,8 The problem is that the methodsf RP have been described in detail, from open RP to theecent laparoscopic and robotic procedures.3,9 However,n contrast with the well-described methods of RP,LND is usually mentioned as “routine procedure.” Inur opinion, the currently available anatomical descrip-ions of PLND methods are too approximate and impre-ise.
Many surgical schools routinize and standardize oper-tive procedures to help the surgeon develop systematicabits and to decrease the number of mistakes.6,10,11 Ourbservations have shed light on a number of generalroblems. It seems to be that: (1) every school of surgeonsas different methods of PLND, but the same method ofP; (2) surgeons pay more attention to RP but under-
alue the importance of PLND; and (3) urologists in971
mparttraf
aboLoatTdnbtt
eta
caliz
training under different mentors learn to operate theprostate in a standardized way, but apply individualmethods for PLND.
These problems have encouraged us to standardizePLND, at least in our own department. We have workedout a “step by step” improved operative standard, byintegrating all currently known elements. Standard byour definition means: (1) standard position both of thepatient and the operating team; (2) standard materials(e.g., clips, ligature); (3) a standard method and standardlocations on where to start, how and where to proceed,and how to finish the operation; and (4) standardizedinstruments.
The current valid standard of PNLD is based on sen-tinel LN detection. We rely on the recent studies of theBern and Augsburg groups as well as our own experi-ence.2,5,8,12 There are some excellent studies that de-scribe typical locations of possible metastasis in differentsegments of the pelvic lymphatic network.4,12,13 The
ost recent study evaluated data of 122 node-positiveatients and completed a scheme of extended PLNDreas. According to these results, positive LNs in theegion of the external iliac vein were found in 9% ofhe patients, in the fossa obturator region in 16.4%, inhe sacral LN region in 21.3%, and in the internal LNegion in 49.2%. In other words, positive internal LNslone or in combination with positive sacral LNs were
7%
7%
26,5%
A. iliaca externa - 4 LNs A. iliaca coFossa obturatoria - 4 LNs presciatic a
Figure 2. Distribution of lymph nodes m
Figure 3. Quantity and lo
ound in 80/122 (70.5%) patients, whereas positive LNs
972
long the external iliac vein and in the fossa obturatoria,ut not along the internal iliac vessels, were detected innly 5 patients (4%).8 These results allowed us to extendN dissection into the presacral region, in further devel-pment of the method by an Augsburg study group. Theforementioned study results support the 3 main ana-omic postulates of the prostate lymphatic drainage: (1)he posterior surface of the prostate has a lymphaticrainage stretching back to the internal iliac vessels andodes, (2) the dorsal surface of the prostate follows theladder to the external iliac lymphatic vessels, and (3)he ventral surface of the prostate follows the pudendal tohe internal iliac lymphatic vessels.14,15 We have com-
bined a sacral and internal region of LN dissection.According to our proposition, this region includes theupper margin as the obturator nerve, the lower margin asthe lateral edge of the NVB of the prostate, the foraminaobturatoria is cranial, and the ureter and the internaliliac artery are caudal.
In addition, we include the LNs in the presciatic areain PLND procedures. The margins of this region are thelast one-third of the backside area of the external iliacvein close to the bifurcation of the common iliac vein,above the end point of obturator LN dissection.2
Extended PLND can also be estimated by the numberof removed LNs. In one study, a cohort of 278 consecu-tive patients (mean age 66.2 years) underwent radical
13%
26,5%
unis - 2 LNs A. iliaca interna - 3 LNs- 1 LN sacral - 1 LN
stasis accordingly to their localization.
ation of LNs metastasis.
20%
mmrea
retropubic prostatectomy and extended PLND, during
UROLOGY 77 (4), 2011

crcPtfddp
ntt
sdta
ftt
tgf
oUK
which 10 or more nodes were removed and examined16;92.8% of these patients had a low or intermediate onco-logical risk. The mean number of lymph nodes examinedwas 17.5 (range, 10–38); 29 patients (10.4%) had lymphnode invasion (LNI). In the same study, 858 patientsaged 45–85 years were predominantly treated with ex-tended pelvic LN dissection before radical retropubicprostatectomy.17 The LNI rate increased with the num-ber of removed nodes (P �.001): 2–10 nodes removed,5.6% LNI rate; 10–14 nodes removed, 8.6% LNI rate;15–19 removed, 10.2% LNI rate; and 20–40 removed,17.6% LNI rate. These figures indicate that the removalof 28 nodes yields a 90% chance of detecting LNI.Conversely, the assessment of 10 or fewer nodes wasassociated with a virtually zero probability of finding LNI.The ability to remove more LNs is in direct affiliationwith the number of removed LNs. This outcome supportsan earlier study of Heidenreich et al with 103 patientswho underwent extended PLND compared with radicalretropubic prostatectomy and standard lymphadenec-tomy in 100 consecutive patients. A mean of 28 lymphnodes (range, 21–42) were dissected. Metastases werediagnosed in 27 of the 103 patients (26.2%) who under-went the extended procedure.18
Hypothetically, more injury means more complica-tions. Does this statement apply to PLND? What is therelation between the number of possible complicationsand the oncological benefit?
Older studies have reported a high frequency of intra-and perioperative complications caused by extendedPLND.19 These figures form a contrast with the compli-ations observed in patients who underwent adjuvantadiation therapy after RP. In an earlier study, the risk ofomplications caused by diagnostic and therapeuticLND has been compared with that caused by radiationherapy after RP. Patients undergoing limited dissectionollowed by pelvic irradiation have a 25% to 30% risk ofeveloping a debilitating complication. In patients un-ergoing complete (therapeutic) dissection followed byelvic irradiation, lymphedema were observed in 66%.20
All of the aforementioned patients were treated by radi-ation therapy and developed postirradiation, not postop-erative lymphedema, thus the findings cannot be stronglydependent on the extent of the dissection.
In a recent, earlier mentioned publication, the com-plication rates of diagnostic (7%) and extended thera-peutic PLND (19.8%) have been compared.4,10 There are
o major differences in the number of these complica-ions in both intraoperative and postoperative observa-ions.4,18 The most common postoperative complication
is a lymphocele, which can be expected after extendedPLND in 10.6% of all complications (in comparison,limited PNLD has a 9% lymphocele rate).18 We proposetandard fenestration of a perivesical room with an ab-ominal cavity, which can be performed bilaterally abovehe external iliac vessels down to the fossa obturatoria
fter completion of the main procedure. LaparoscopicUROLOGY 77 (4), 2011
enestration after analogous laparoscopic RP decreaseshe frequency of lymphoceles in a collective 100 patientso 10.32%.21
A few studies describe a proximate cause oflymphedema, which is probably connected to incorrectdissection above the external iliac artery.10,11 The LVs inhe region between the external iliac artery and theenitofemoral nerve primarily transport lymphatic fluidrom the lower extremities.4 In this area, positive LNs
have never been found; therefore, there is no need toremove LNs in this area. In summary, however, whenadding together the reported results and our experience,a rate of 7% to 13% perioperative complications must beexpected.
CONCLUSIONSWe have attempted to standardize a procedure. Wewould like to propose that the following are included inthe standard operating routine: dissection of LN tissuealong the common iliac vein, (2) dissection of LN tissuein the presciatic area, (3) dissection of LN tissue parasa-cral, and (4) fenestration to avoid lymphoceles. Thesestandards, as developed in our department, enable us toremove more than 20 LNs per PLND on average. Webelieve that standardized PNLD could improve both theoncological outcome and the quality of the surgical pro-cedure.
Acknowledgments. We appreciate the professional editingf the English text by Almut Kalz from the Department ofrology, University Hospital, Schleswig-Holstein, Campusiel.
References1. Hinmann F. Atlas of Urologic Surgery. Philadelphia: W. B. Saunders
Company; 1998.2. Meinhardt W, Valdés Olmos RA, van der Poel HG, et al. Lapa-
roscopic sentinel node dissection for prostate carcinoma: technicaland anatomical observations. BJU Int. 2008;102(6):714-717.
3. Rassweiler J, Stolzenburg J, Sulser T, et al. Laparoscopic radicalprostatectomy—the experience of the German LaparoscopicWorking Group. Eur Urol. 2006;49(1):113-119.
4. Heidenreich A, Ohlmann CH, et al. Anatomical extent of pelviclymphadenectomy in patients undergoing radical prostatectomy.Eur Urol. 2007;52(1):29-37.
5. Hautmann S, Beitz S, Naumann M, et al. Extended sentinel lymphnode dissection in radical prostatectomy for prostate cancer: a studyin the Kiel risk population. Urologe A. 2008;47(3):299-303.
6. Briganti A, Capitanio U, Chun FK, et al. Impact of surgical volumeon the rate of lymph node metastases in patients undergoing radicalprostatectomy and extended pelvic lymph node dissection for clin-ically localized prostate cancer. Eur Urol. 2008;54(4):794-804.
7. Heidenreich A. Radical prostatectomy in 2007: oncologic controland preservation of functional integrity. Eur Urol. 2008;53(5):877-879.
8. Schumacher MC, Burkhard FC, Thalmann GN, et al. Good out-come for patients with few lymph node metastases after radicalretropubic prostatectomy. Eur Urol. 2008;54(2):344-352.
9. Stolzenburg JU, Rabenalt R, Do M, et al. Endoscopic extraperito-neal radical prostatectomy: the University of Leipzig experience of
2000 cases. J Endourol. 2008;22(10):2319-2325.973

1
1
1
1
1
1
1
1
1
2
2
t
pnhtrm
2
3
9
10. Briganti A, Chun FK, Salonia A, et al. Complications and othersurgical outcomes associated with extended pelvic lymphadenec-tomy in men with localized prostate cancer. Eur Urol. 2006;50(5):1006-1013.
1. Clark T, Parekh DJ, Cookson MS, et al. Randomized prospectiveevaluation of extended versus limited lymph node dissection inpatients with clinically localized prostate cancer. J Urol. 2003;169(1):145-147.
2. Weckermann D, Dorn R, Trefz M, et al. Sentinel lymph nodedissection for prostate cancer: experience with more than 1,000patients. J Urol. 2007;177(3):916-920.
3. Weckermann D, Holl G, Wagner T, et al. Sentinel node dissectionin prostate cancer: current status. Urologe A. 2007;46(11):1500-1507.
4. Netter FH. Atlas of Human Anatomy. King of Prussia, Pa: Ritten-house Book Distributors Inc.; 1997.
5. Gil-Vernet JM. Prostate cancer: anatomical and surgical consider-ations. Br J Urol. 1996;78:161-168.
6. Briganti A, Karakiewicz PI, Chun FK, et al. Percentage of positivebiopsy cores can improve the ability to predict lymph nodeinvasion in patients undergoing radical prostatectomy and ex-tended pelvic lymph node dissection. Eur Urol. 2007;51(6):1573-1581.
7. Briganti A, Chun FK, Salonia A, et al. Critical assessment of idealnodal yield at pelvic lymphadenectomy to accurately diagnose prostatecancer nodal metastasis in patients undergoing radical retropubic pros-tatectomy. Nat Clin Pract Urol. 2007;4(10):528-529.
8. Heidenreich A, Varga Z, Von Knobloch R. Extended pelvic lymph-adenectomy in patients undergoing radical prostatectomy: highincidence of lymph node metastasis. J Urol. 2002;167(4):1681-1686.
9. Igel TC, Barrett DM, Segura JW, et al. Perioperative and postop-erative complications from bilateral pelvic lymphadenectomy andradical retropubic prostatectomy. J Urol. 1987;137(6):1189-1191.
0. Pilepich MV, Asbell SO, Mulholland GS, et al. Surgicalstaging in carcinoma of the prostate: the RTOG experience.Radiation Therapy Oncology Group. Prostate. 1984;5(5):471-476.
1. Stolzenburg JU, Wasserscheid J, Rabenalt R, et al. Reduction inincidence of lymphocele following extraperitoneal radical prosta-tectomy and pelvic lymph node dissection by bilateral peritonealfenestration. World J Urol. 2008;26(6):581-586.
EDITORIAL COMMENTAlthough the concept of extended pelvic lymphadenectomy forbladder cancer has gained traction, no current consensus existseither for the indications or extent of lymphadenectomy duringradical prostatectomy for prostate cancer. Although the thera-peutic value of lymphadenectomy in prostate cancer is debated,long-term survival is clearly possible in patients with solitarynodal metastasis.1,2 Accurate staging may affect treatment de-cisions, allowing for early adjuvant hormone therapy and pro-longed survival.3
Population-based cancer registry data on the adequacy oflymphadenectomy in the United States is lacking, but availabledata suggest that when lymphadenectomy is performed, it is fre-quently inadequate. Joslyn and Konety reported on SEER datafrom 1988 to 1991, and found that removing more than 10 lymphnodes decreased the risk of death from prostate cancer by 15%.2
How often is an “adequate” lymphadenectomy performed? We canonly infer from their data, but among patients with lymph nodesexamined and with complete data, fewer than 6 nodes were sam-pled in 31% of patients. I suspect that a limited sampling of theobturator fossa alone or in combination with external iliac nodes
accounts for a substantial number of these cases.74
A limited lymphadenectomy is chosen based on the prevailingbelief that the yield for finding node-positive disease is low. This isa self-fulfilling prophecy: the surgeon samples few nodes under theassumption that yields for node-positive disease will be low, thesurgeon finds few N� patients, and the cycle continues. Furthercomplicating matters is that the most widely available nomogramsare based on sampling of �10 lymph nodes and may underestimatehe true incidence of lymph node positivity.4
The present series,5 in which an appropriate template waserformed, demonstrates that sampling simply the external iliacodes, or the obturator nodes above the obturator nerve, wouldave mistakenly staged the vast majority of node-positive pa-ients as node negative. These data are not new; others haveepeatedly demonstrated that the more nodes sampled, theore likely one is to accurately discover node-positive disease.6
The authors’ observation is true that the literature containsan abundance of technical descriptions of prostatectomy tech-niques but lacks detailed “how-to” guides to PLND. Perhaps thisarticle is a small step toward breaking one of the many barriersto widespread adoption of PLND. As an aside, their technicalapproach can be expeditiously reproduced robotically withoutdifficulty, and the template should not be curtailed based on thechosen approach (open vs robotic). As with any procedure,having a well-defined, reproducible routine for PLND allowssurgeons to gain familiarity with a standardized procedure. Assuch, complications in this series are acceptable (lymphoceles�12%, no vascular injuries).
David Canes, M.D., Institute of Urology, Lahey Clinic,Burlington, Massachusetts
References1. Boorjian SA, Thompson RH, Siddiqui S, Bagniewski S, Bergstralh
EJ, Karnes RJ, et al. Long-term outcome after radical prostatectomyfor patients with lymph node positive prostate cancer in the prostatespecific antigen era. J Urol. 2007;178(3 Pt. 1):864-870.
. Joslyn SA, Konety BR. Impact of extent of lymphadenectomy onsurvival after radical prostatectomy for prostate cancer. Urology.2006;68(1):121-125.
. Messing EM, Manola J, Sarosdy M, Wilding G, Crawford ED, TrumpD. Immediate hormonal therapy compared with observation afterradical prostatectomy and pelvic lymphadenectomy in men withnode-positive prostate cancer. N Engl J Med. 1999;341(24):1781-1788.
4. Heidenreich A, Ohlmann CH, Polyakov S. Anatomical extent ofpelvic lymphadenectomy in patients undergoing radical prostatec-tomy. Eur Urol. 2007;52(1):29-37.
5. Osmonov DK, Wang C, Hoenle J, Aksenov A, Hamann C, Nau-mann CM, Juenemann KP. Extended Lymphadenectomy ‘Step byStep’ in Patients Undergoing Radical Prostatectomy. J Urol. 2011;77(4):969–975.
6. Briganti A, Chun FK, Salonia A, Gallina A, Zanni G, Scattoni V,et al. Critical assessment of ideal nodal yield at pelvic lymphade-nectomy to accurately diagnose prostate cancer nodal metastasis inpatients undergoing radical retropubic prostatectomy. Urology. 2007;69(1):147-151.
doi:10.1016/j.urology.2010.07.518UROLOGY 77: 974, 2011. © 2011 Elsevier Inc.
REPLYWe absolutely agree with the comments to our paper. It seemsthat the ability to remove more positive lymph nodes (LNs) is
directly related to the total number of removed LNs.UROLOGY 77 (4), 2011





























