Embed Size (px)
Citation preview

Extended Anticoagulation in VTE
Geoffrey Barnes, MDCardiovascular and Vascular Medicine
University of Michigan, USA
1st Qatar Conference on Safe Anticoagulation Management
February 27, 2015

Outline
• VTE Recurrence Risk• Patient Selection for Extended Therapy• Medication Selection for Extended Therapy• My Approach

Definitions
• Venous Thromboembolism (VTE)– Deep Venous Thrombosis (DVT)– Pulmonary Embolism (PE)
• Treatment Phases– Acute/Initial – first few days– Intermediate/Long-term – up to 3-6 months– Chronic/Extended – beyond first 3-6 months
• Provoked– Transient surgical procedure– Immobilization– Pregnancy or Hormone-related (e.g estrogen
contraceptives)
Lancet. 2012; 379: 1835-1846

Clinical Case
• 65 year old man with CAD and a first unprovoked femoral-popliteal DVT
• Completed 3 months of warfarin therapy
• What is his recurrence risk?• Does he need further therapy?• If so, what is the best medication to use?

Outline
• VTE Recurrence Risk• Patient Selection for Extended Therapy• Medication Selection for Extended Therapy• My Approach

Provoked vs Unprovoked
BMJ. 2011; 342:d3036

Provoked vs Unprovoked
Surgically Provoked
Non-surgically Provoked
Unprovoked Cancer-related0
5
10
15
20
25
0.7
4.2
7.4
20.7
Recu
rren
ce R
isk (%
)
Arch Int Med 2010;170:1710-1716Blood 2002; 100:3484-8

VTE Location
BMJ. 2011; 342:d3036
HR 0.49 (0.34-0.71)

Age and Obesity
Arch Intern Med. 2000;160(6):761-8

Gender
NEJM 2004;350:2558-2563
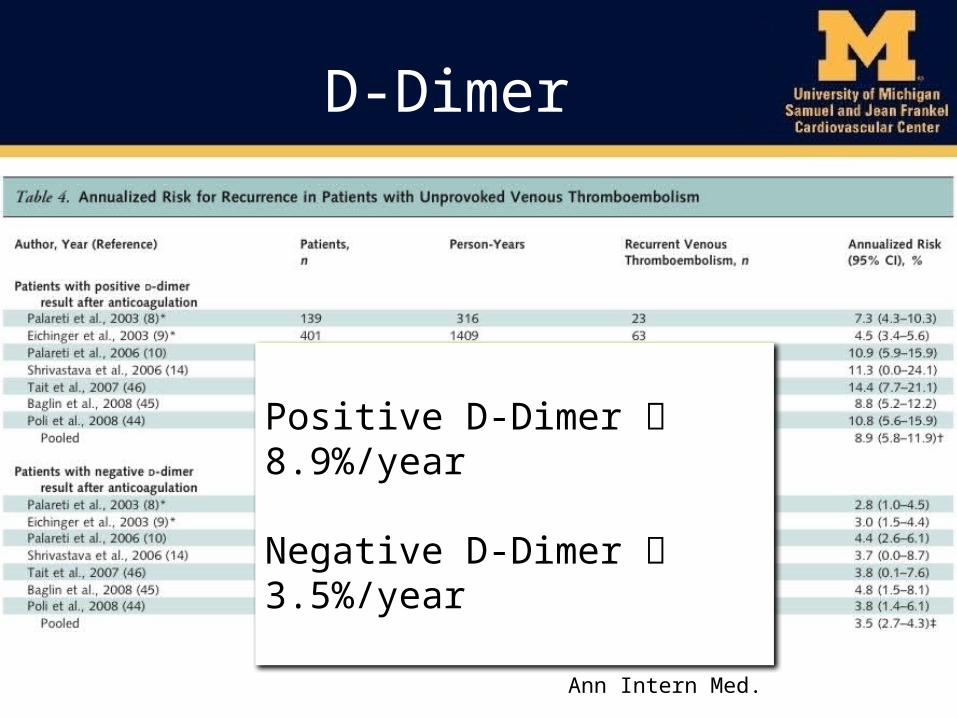
D-Dimer
Positive D-Dimer 8.9%/year
Negative D-Dimer 3.5%/year
Ann Intern Med. 2008;149:481-490

D-Dimer
Kearon Ann Int Med 2015;162:27
3%
97%
15%85%

D-Dimer
Blood 2010; 115: 481–488CMAJ 2008; 179: 417–426
On Anticoagulation
Negative D-Dimer
Positive D-Dimer
28%
4 weeks without Anticoagulation

Hypercoagulable States
• Factor V Leiden• Protein C/S Deficiency• Antithrombin Deficiency• Elevated Homocysteine• Dysfibrinogenemia• Antiphospholipid Antibodies

Hypercoagulable States
• Considerations– How significant is the increased VTE recurrence
risk?– How frequently is the hypercoagulable state
found?– Can testing be done on anticoagulation?– Are there treatment implications?
Blood 2013;122:817-824Circulation 2014;130:283-287

Hypercoagulable States
• Factor V Leiden• Protein C/S Deficiency• Antithrombin Deficiency• Elevated Homocysteine• Dysfibrinogenemia• Antiphospholipid Antibodies– VTE Recurrence Risk (RR ~2)– Favor use of Warfarin over DOACs currently
Blood 2013;122:817-824Circulation 2014;130:283-287

Outline
• VTE Recurrence Risk• Patient Selection for Extended Therapy• Medication Selection for Extended Therapy• My Approach

VTE Recurrence Predictors
• Provoked vs Unprovoked• PE and Proximal DVT vs Distal DVT• Age• Obesity• Gender• D-dimer• Hypercoagulable States

Risk Prediction Models
CMAJ 2008;179:417-426Circulation 2010; 121:1630-1636J Thromb Haemost 2012; 10: 1019–1025
Men and HERDOO
Vienna Risk Model
DASH
Gender X X XD-Dimer X X X
Signs of Post-Thrombotic Syndrome
X
Obesity XAge X
Location of DVT/PE XProvoked? X

Men and HERDOO-2
High Risk:• All Men• Women with 2+ of• Post-thrombotic
Syndrome• Elevated D-dimer• Obesity
75% of patients are High Risk
Freedom from Recurrent VTE
CMAJ 2008;179:417-426

Outline
• VTE Recurrence Risk• Patient Selection for Extended Therapy• Medication Selection for Extended Therapy• My Approach

Medication Options
• Warfarin• Dabigatran• Rivaroxaban• Apixaban• Aspirin

Warfarin
NEJM 2003;348:1425-1434 and NEJM 2003;349:631-639

Dabigatran
Recurrent VTE Any Bleeding
NEJM 2013;368:709-718
War
farin
Plac
ebo

Rivaroxaban
NEJM 2010;363:2499-2510

Apixaban
Recurrent VTE Major and CRNM Bleeding
NEJM 2012;368:699-708

Aspirin
INSPIRE Collaborative (WARFASA & ASPIRE)
Circulation 2014;130:1062-1071
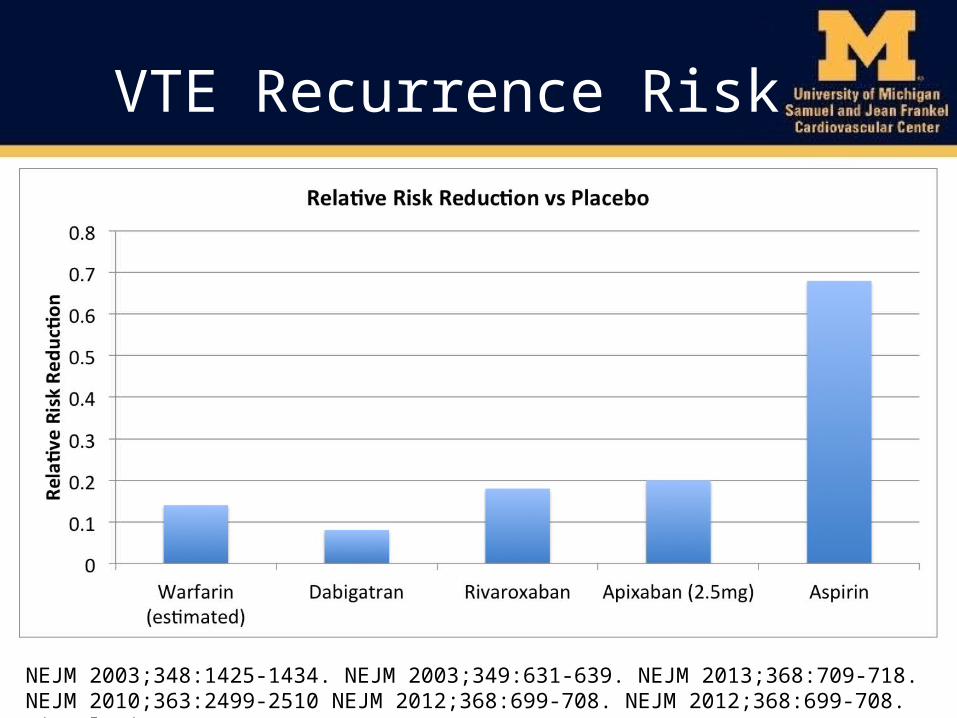
VTE Recurrence Risk
NEJM 2003;348:1425-1434. NEJM 2003;349:631-639. NEJM 2013;368:709-718. NEJM 2010;363:2499-2510 NEJM 2012;368:699-708. NEJM 2012;368:699-708. Circulation 2014;130:1062-1071

Outline
• VTE Recurrence Risk• Markers of Recurrence Risk• Patient Selection for Extended Therapy• Medication Selection for Extended Therapy• My Approach

My Approach
Barnes GD Vascular Medicine 2015 (in press)
Predictive Factors:• Provoked• D-Dimer• Gender

My Approach
• Drug Selection– Another indication?• Example: Aspirin for CAD
– Prefer to continue current medication?– Balance efficacy and risk• Usually use apixaban or rivaroxaban

Clinical Case
• 65 year old man with CAD and a first unprovoked femoral-popliteal DVT
• Completed 3 months of warfarin therapy
• What is his recurrence risk?– High: >7-10% per year
• Does he need further therapy?– Yes
• If so, what is the best medication to use?– Apixaban or Rivaroxaban if CAD stable– Aspirin if recent PCI or MI requiring clopidogrel

Thank You

Louzada/Ottawa Score
Risk Factor Point Number of Points
VTE Recurrence Risk (per year)
Female 1 ≤0 ≤5%Lung Cancer 1 1 13-16%Prior VTE 1 2 18%Breast Cancer -1 3 25-50%TNM Stage = I -2
Cancer-associated VTE
Circulation 2012;126:448-454





























