Embed Size (px)
Citation preview

Expression Profiling of Nuclear Receptors IdentifiesKey Roles of NR4A Subfamily in Uterine Fibroids
Hanwei Yin,* Jay H. Lo,* Ji-Young Kim, Erica E. Marsh, J. Julie Kim,Asish K. Ghosh, Serdar Bulun, and Debabrata Chakravarti
Division of Reproductive Biology Research, Department of Obstetrics and Gynecology (H.Y., J.H.L., J.-Y.K., E.E.M., J.J.K., S.B., D.C.), Feinberg Cardiovascular Research Institute (A.K.G.), and Robert H. LurieComprehensive Cancer Center (E.E.M., J.J.K., S.B., D.C.), Feinberg School of Medicine, NorthwesternUniversity, Chicago, Illinois 60611
Uterine fibroids (UFs), also known as uterine leiomyomas, are benign, fibrotic smooth muscletumors. Although the GnRH analog leuprolide acetate that suppresses gonadal steroid hormonesis used as a treatment, it has significant side effects, thereby limiting its use. Availability of moreeffective therapy is limited because of a lack of understanding of molecular underpinnings of thedisease. Although ovarian steroid hormones estrogen and progesterone and their receptors areclearly involved, the role of other nuclear receptors (NRs) in UFs is not well defined. We usedquantitative real-time PCR to systematically profile the expression of 48 NRs and identified severalNRs that were aberrantly expressed in UFs. Among others, expression of NR4A subfamily membersincluding NGFIB (NR4A1), NURR1 (NR4A2), and NOR1 (NR4A3) were dramatically suppressed inleiomyoma compared with the matched myometrium. Restoration of expression of each of theseNR4A members in the primary leiomyoma smooth muscle cells decreased cell proliferation. Im-portantly, NR4As regulate expressions of the profibrotic factors including TGF�3 and SMAD3, andseveral collagens that are key components of the extracellular matrix. Finally, we identify NR4Amembers as targets of leuprolide acetate treatment. Together, our results implicate several NRsincluding the NR4A subfamily in leiomyoma etiology and identify NR4As as potential therapeutictargets for treating fibrotic diseases. (Molecular Endocrinology 27: 0000–0000, 2013)
Uterine fibroids (UFs), which are also referred to asuterine leiomyomas, are benign smooth muscle tu-
mors derived from the transformation of cells within theuterine myometrium (uterine smooth muscle layer). Al-though the presence of UFs is rarely associated with mor-tality, symptoms caused by leiomyomas like abnormaluterine bleeding, pelvic pain, and increased urinary fre-quency significantly affect a woman’s morbidity andquality of life (1). UF is a fibroproliferative disease. It iswell accepted that ovarian steroid hormones (estrogenand progesterone) and their receptors (estrogen receptor[ER] and progesterone receptor [PR]) play essential rolesin maintaining and promoting the growth of UFs (2). Asecond feature of UFs is deposition of excessive extracel-lular matrix (ECM) primarily composed of collagen (3).To date, surgical removal of UFs (hysterectomy) is the
only definitive treatment for the disease. Uterine myomec-tomy, a conservative surgical approach removing only theUF, is limited in its scope because of concerns of fertilityloss and the associated risks of postoperative complica-tions and morbidity due to hemorrhage, bowel injury,and adhesion formation as well as the high incidence ofrecurrence of tumors (3, 4). Effective oral medications fortreating and controlling UFs are still very limited (2, 3, 5).Leuprolide acetate (LA) is a GnRH analog used for treat-ment of UFs and functions by downregulating synthesis ofgonadal steroid hormones. A recent report showed that in
ISSN Print 0888-8809 ISSN Online 1944-9917Printed in U.S.A.Copyright © 2013 by The Endocrine SocietyReceived September 5, 2012. Accepted March 6, 2013.
* H.Y. and J.H.L contributed equally to this work.Abbreviations: COL1A1, collagen type I, alpha 1; COL16A1, collagen, type XVI, alpha 1;COL6A1, collagen type VI, alpha 1; COL6A2, collagen, type VI, alpha 2; Ct, cycle thresh-old; E2, estradiol; ECM, extracellular matrix; ER, estrogen receptor; FBS, fetal bovineserum; GR, glucocorticoid receptor; HDAC3, histone deacetylase 3; LSMC, leiomyomasmooth muscle cell; MR, mineralocorticoid receptor; NBRE, NGFIB-binding response ele-ment; NOR1, neuron-derived orphan receptor 1; NR, nuclear receptor; PR, progesteronereceptor; pSmad3, phosphorylated Smad3; qPCR, quantitative PCR; SBE, Smad3-bindingelement; Smad3, mothers against decapentaplegic homolog 3; SMRT, silencing mediatorfor retinoid and thyroid-hormone receptors; SRC, steroid receptor coactivator; TGF�3,transforming growth factor �3; UF, uterine fibroid.
O R I G I N A L R E S E A R C H
doi: 10.1210/me.2012-1305 Mol Endocrinol mend.endojournals.org 1
Molecular Endocrinology. First published ahead of print April 2, 2013 as doi:10.1210/me.2012-1305
Copyright (C) 2013 by The Endocrine Society

human trials, ulipristal acetate reduced fibroid size beforesurgery, suggesting that use of selective PR modulatorscan be a viable treatment option (6). Other agents such asmifepristone, an antiprogesterone; pirfenidone and ha-lofuginone, which are antifibrotic drugs; and aromataseinhibitors have been evaluated in treating UFs with vary-ing degrees of effectiveness and side effects (7, 8). Afterreceiving LA treatment, patients often suffer from the sideeffects including decrease in bone mineral density or car-diovascular morbidity, and UFs tend to regrow when thepatients stop the medication (9, 10). Therefore, a betterunderstanding of the molecular underpinnings of UF isneeded to allow for the identification of potential thera-peutic targets other than ER and PR.
Nuclear receptors (NRs) comprise a superfamily of con-served transcription factors regulated by small lipophilic li-gands and cellular signaling pathways. NRs play essentialroles in organismal physiology and are major drug targetsfor treatment of reproductive abnormalities, cancer, diabe-tes, cardiovascular disease, and metabolic syndrome (11–13). There are 48 members of the NR superfamily in hu-mans. These receptors function as monomers and homo/heterodimers and directly regulate transcription ofhormone-inducible genes. Mechanistically, in the absence ofhormone, some NRs function as transcriptional repressorsby recruiting silencing mediator for retinoid and thyroid-hormone receptors (SMRT)/nuclear receptor corepressor(NCoR)-histone deacetylase 3 (HDAC3) corepression com-plexes. In the presence of hormone, the receptors changeconformation, leading to release of corepression complexesand recruitment of cAMP response element-binding protein(CREB)-binding protein (CBP)/E1A binding protein p300-steroid receptor coactivator (SRC) coactivation complexes(14, 15). Finally, orphan receptors have no known ligands,although they have transcriptional repressing and activatingfunctions. Recent advancements in biological tools affordedanalysis of all 48 NRs in various cellular and biologicalcontexts including the NCI60 collection of 51 cancer celllines, which revealed that specific NR expression patternscan be used to predict drug sensitivity of individual cell lines(16). These results suggest that NR expression profilingmight also identify receptors for novel therapeutic interven-tion of UFs.
In the current study, we report the mRNA expressionprofile of 48 NRs in uterine leiomyoma and the matchedmyometrium. Although expression of several NRs wasdysregulated, orphan NR4A subfamily members weredramatically underexpressed in leiomyoma comparedwith normal myometrial tissue. Downregulation ofNR4A proteins have functional proproliferative andstrong profibrotic effects. Restoration of NR4A expres-sion decreased proliferation of leiomyoma smooth muscle
cells (LSMCs). Targeted gene and protein expressionanalysis demonstrated a critical role of NR4A members inregulating key signaling, transcriptional, and structuralgenes involved in uterine fibrosis. Our data thereforeidentify NR4A subfamily members as key regulators ofuterine leiomyoma and suggest NR4As as potential tar-gets for treating UFs.
Materials and Methods
Study subjects and human tissue specimensHuman uterine leiomyoma and matched myometrial tissues
were collected from subjects (n � 22) undergoing hysterectomyor myomectomy. The average age was 44.0 � 4.86 years (range36–52 years). Of 22 subjects, there were 10 Caucasian, 8 Afri-can-American, 2 Hispanic, and 2 Asian-American (Table 1). Nosubject had received any hormonal treatment during the 3months before their surgeries except for the 4 LA-treated sub-jects (E9, 131, 262, and 263). Written informed consent wasobtained from each subject, and the use of human tissue speci-mens was approved by the Institutional Review Board of North-western University. All surgeries were performed at Northwest-ern’s Prentice Women’s Hospital.
The tissue specimens were collected from pathologists withinan hour of being removed from the subjects. The size of UFsranged from 14.1 to 138.8 g in weight. Tumor samples werealways obtained at the outer 25% of the fibroid, whereas adja-cent myometrium samples were collected 2 cm outside of the
Table 1. Characteristics of Study Subjects
SubjectNo.
Age,y Race
CyclePhase
HormoneMedicationa
E27 52 His NA NE29 42 C Lut NE63 49 AA Lut NE91 41 His Fol NE97 41 C Lut NE98 51 C Lut NE102 51 C Lut NE105 45 As Fol NE106 40 AA MC NE116 44 AA Fol NE122 36 C Lut NE123 47 AA NA NE124 52 C NA NE145 48 AA MC NE148 38 AA MC NE162 38 AA Lut NE254 46 As Fol NE255 41 C Lut NE9 42 C Am LAE131 41 AA Am LAE262 42 C Am LAE263 40 C Am LA
Abbreviations: AA, African-American; Am, amenorrhea; As,Asian-American; C, Caucasian; Fol, follicular; His, Hispanic; LA,leuprolide acetate; Lut, luteal; MC, middle cycle; N, no medication; NA,not available.a Medication records in last 3 months.
2 Yin et al Nuclear Receptors in Uterine Fibroids Mol Endocrinol

border of the fibroid, and 36% (8 of 22) of the tumors wereremoved during the luteal phase of the menstrual cycle, 18% (4of 22) during the follicular phase, and 14% (3 of 22) during themiddle cycle (Table 1). Four of the subjects had amenorrheasecondary to LA treatment.
Cell cultureBoth leiomyoma and myometrial primary cells were cultured
in DMEM/F12 1:1 (GIBCO/BRL, Grand Island, New York)containing 10% fetal bovine serum (FBS); 293T/17 cells werecultured in DMEM (GIBCO/BRL) containing 10% FBS. Allcells were grown in a humidified incubator at 37°C with 5%CO2. Primary cells used in these experiments were passaged nomore than 2 times.
RNA isolation and quantitative RT-PCRHuman uterine leiomyoma and myometrial tissue samples
were homogenized by using rotor-stator homogenizers accord-ing to the QIAGEN (Valencia, California) RNeasy protocol.Total RNA was isolated from tissue samples or cultured pri-mary cells using the QIAGEN RNeasy mini kit according to themanufacturer’s instructions. First-strand cDNA was synthe-sized with 1 �g of total RNA using qScript cDNA synthesis mix(Quanta Biosciences, Gaithersburg, Maryland) containing bothrandom hexamer and oligo-deoxythymidine primers. Quantita-tive PCR (qPCR) was performed with diluted cDNA using anABI PRISM 7900HT 384-well real-time PCR machine (AppliedBiosystems, Foster City, California). Each PCR was performedby using SYBR green PCR master mix (Applied Biosystems) andgene-specific primers in a final volume of 20 �L. Primers weredesigned by Primer3 software (Whitehead/MIT, Cambridge,Massachusetts) or according to previous literature (16, 17). Thecycle threshold (Ct) value was first normalized to �-actin or36B4 ribosomal protein to calculate relative gene expression(�Ct), which was further normalized to determine fold changesin mRNA levels by using ��Ct.
Retrovirus production of NR4A expression plasmidNR4A expression plasmids cloned into pMSCV-pac con-
structs were kind gifts from Dr. Peter Tontonoz (18). Vesicularstomatitis virus G glycoprotein (VSVG)-pseudotyped retroviruswas produced in 293T/17 cells (6-well plate) by cotransfectionwith pCMV-VSVG (0.5 �g), pMLV-GagPol (1 �g), and retro-viral construct (1.5 �g) using Lipofectamine 2000 (Invitrogen,Carlsbad, California) according to manufacturer’s instructions.After overnight transfection, fresh DMEM was added to cells.Cells were allowed to equilibrate for several hours at 37°C in anincubator before being transferred to a 32°C/5% CO2 humidi-fied cell incubator for additional 24 hours. Retrovirus was har-vested and cleared of 293T/17 cells by centrifugation and storedat �80°C for future use.
Retroviral transduction and stable cell productionLeiomyoma and myometrial primary cells were cultured in
6-well plates to generate pools stably expressing either emptyvector or individual NR4A proteins. Cells were transduced witha 1:4 mixture of viral supernatant and fresh medium, adjusted to8 �g/mL polybrene (Sigma, St Louis, Missouri), and spinfectedat 500g for 2 hours at 32°C. Two days after transduction, cellswere split to 10-cm2 dishes containing 2 �g/mL puromycin.
Cells were grown under selection for 3 days and harvested forfurther analysis. Overexpression of NR4As was always vali-dated by qPCR and Western blot.
Protein extraction and immunoblot analysisHuman uterine leiomyoma and adjacent normal myometrial
tissue samples were homogenized in appropriate volume of T-PER buffer (Pierce, Rockford, Illinois) for 2 hours at 4°C. Ho-mogenates were subsequently centrifuged at 20 000g for 15minutes at 4°C, and supernatants were collected. Cultured leio-myoma and myometrial primary cells were incubated at 4°C for15 minutes in the presence of modified RIPA buffer (20mMTris-HCl [pH 7.6], 150mM NaCl, 1mM EDTA, 1mM EGTA,1% IGEPAL CA-630, 0.5% sodium deoxycholate, 0.1% so-dium dodecyl sulfate). Whole-cell extracts were collected bycentrifugation at 20 000g for 15 minutes at 4°C. Protein con-centrations of tissue samples and cultured cells were determinedby bicinchoninic acid assay (Pierce).
Denatured proteins (20–40 �g) extracted from tissue sam-ples and cultured cells were separated on 8% to 16% polyacryl-amide gels (Invitrogen) and electrophoretically transferred tonitrocellulose membrane. Membranes were blocked in PBSTween-20 buffer containing 5% BSA or nonfat dry milk for 1hour and incubated overnight at 4°C with primary antibodydiluted in the same buffer. Appropriate horseradish peroxidase-conjugated secondary antibodies were then applied and incuba-tion continued for 1 hour. Blots were detected using ECL plus(GE Life Sciences, Piscataway, New Jersey) or SuperSignal WestPico (Thermo Scientific, Pittsburgh, Pennsylvania) detection re-agents, and �-actin was used as a loading control. The commer-cially available primary antibodies used for immunoblottingwere antibodies to NGFIB (nerve growth factor IB)/Nur77/NR4A1 (Santa Cruz sc-5569; Santa Cruz Biotechnology, SantaCruz, California), Nurr1 (nuclear receptor related protein 1)/NR4A2 (Santa Cruz sc-991), NOR1 (neuron-derived orphanreceptor 1)/NR4A3 (Santa Cruz sc-22519), TGF�3 (transform-ing growth factor �3) (R&D Systems, Minneapolis, Minnesota;MAB243), Smad3 (mothers against decapentaplegic homolog3) (Cell Signaling Technology, Danvers, Massachusetts; 9523),pSmad3 (phosphorylated Smad3) S423/425 (Cell Signaling9520), COL1A1 (collagen, type I, alpha 1) (Santa Cruz sc-28657), COL6A1 (collagen, type IV, alpha 1) (Santa Cruz sc-20649), COL6A2 (collagen, type VI, alpha 2) (Santa Cruz sc-83607), COL16A1 (collagen, type XVI, alpha 1) (Santa Cruzsc-68451), and �-actin (Sigma A5441). Horseradish peroxi-dase-conjugated antimouse, antirabbit, and antigoat secondaryantibodies were purchased from Sigma.
The alamarBlue cell proliferation assayProliferation of leiomyoma and myometrial primary cells
with NR4A overexpression was determined using the alamar-Blue cell viability reagent according to the manufacturer’s in-structions (Invitrogen). Puromycin-selected leiomyoma andmyometrial primary cells were seeded at 5000 cells per well inblack-wall 96-well tissue culture plates in 100 �L of DMEM/F12 1:1 containing 10% FBS (n � 8). The alamarBlue reagentwas added (10 �L per well) to the 96-well plate for 2 hoursincubation at 37°C. Fluorescence measurements were then per-formed with a BioTek Synergy HT multidetection microplatereader equipped with 540-nm excitation and 590-nm emission
doi: 10.1210/me.2012-1305 mend.endojournals.org 3

filters. This process was repeated every 24 hours for 5 consecu-tive days using one replicate 96-well plate per day.
Statistical analysisP values were calculated by using the Student’s 2-tailed t test.
P values � .05 were considered statistically significant.
Results
Expression profiling of NRs in uterine leiomyomaand the matched myometrium
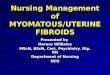
Quantitative RT-PCR was used to analyze expressionpattern of human NR superfamily using primer sets asdescribed (16, 17). Figure 1 summarizes receptor expres-sion levels in matched uterine myometrium and leiomy-oma tissues. To validate our analysis, we also determinedexpression of HMGA2 in our leiomyoma and normalmyometrial samples. In agreement with previous reports,leiomyoma consistently showed a higher mRNA level of
HMGA2 than that of the matched myometrium (6.35 �
2.12 fold difference), which is a hallmark of UFs (19, 20)(Supplemental Figures 1 and 2, published on The Endo-crine Society’s Journals Online web site at http://mend.en-dojournals.org). Based on real Ct values, our results showthat there is a subgroup of receptors that are expressed atvery high levels (Ct �20) in both myometrium and leio-myoma (PR, COUP-TFII, and AR). Expression of somereceptors are very low to undetectable (CAR, HNF4�,and ERR�) in both leiomyoma and myometrial samples(Ct �35), suggesting that they may not be involved in thedisease pathology. A subset of receptors was hyperex-pressed (NOR1, NGFIB, NURR1, and LXR�) in myo-metrium tissues when compared with leiomyoma sam-ples. Finally, only a few receptors (ROR�, VDR, andPNR) were hyperexpressed in leiomyoma (Figure 1). Todetermine whether there is a specific pattern of receptorexpression based on their subgroup in the family, we per-
Figure 1. Gene expression profile of all 48 NRs in matched human leiomyoma and myometrial tissues. Paired leiomyoma and myometrial tissuemRNAs were isolated from 3 independent human samples. Complete expression profiles of NRs were measured by qRT-PCR and normalized to PRexpression in myometrium (set as 100% relative gene expression). Real Ct values are also shown on top to indicate the relative abundance of allNRs in tissue samples. Values represent the mean � SD with 3 independent human samples.
4 Yin et al Nuclear Receptors in Uterine Fibroids Mol Endocrinol

formed subfamily-specific expression analyses, which areshown in Figure 2 and summarized in Table 2.
Expression profiling of NR subfamily 1Except for PPAR�, most NRs in this subfamily has
been unexplored in UFs. Of 19, 7 members in this familydisplayed significantly different expression patterns inuterine leiomyoma versus matched myometrium. Al-though no major changes in expression of TR�, TR�,RARs (�, �, and �), PPAR�, LXR�, and Rev-Erbs (� and�) were observed (Supplemental Figure 1A), the mRNAlevels of PPAR�, PPAR�, ROR�, ROR�, and LXR�
were found to be significantly lower, whereas ROR� andVDR were higher in leiomyoma when compared withmatched myometrium. Expression of FXR� and PXR didnot vary significantly, whereas CAR was undetected inboth leiomyoma and myometrial samples (Figure 2A andSupplemental Figure 1A).
Expression profiling of NR subfamily 2There is little to no information available on the role of
subfamily 2 NRs in UFs. Our expression profiling showedthat HNF4� expression was not detected in either leio-myoma or normal myometrium. However, although lowbut quantifiable in overall expression, HNF4� expressionwas much higher in leiomyoma tissues. Among RXRsthat form heterodimers with NRs, RXR� expression wasfound to be significantly lower in uterine leiomyoma, sug-gesting that RXR� is probably important in UF develop-ment. Expression of TR2, TR4, and TLX also did notchange, although PNR expression was higher in leiomy-oma tissues. Interestingly, although expression of COUP-TFIII did not change, COUP-TFI and II consistentlyshowed moderately lower expression in leiomyoma tis-sues (Figure 2B and Supplemental Figure 1B).
Expression profiling of NR subfamily 3Consistent with the published literature (21), both
ER� and ER� are upregulated in leiomyoma. PR, whichplays critical roles in UFs, showed a slight increase inexpression pattern in leiomyoma. This is not surprisingconsidering that PR is the most highly expressed receptorin normal myometrium and leiomyoma tissues. Interest-ingly, the glucocorticoid receptor (GR) and mineralocor-ticoid receptor (MR) were consistently lower in leiomy-oma (Figure 2E and Supplemental Figure 1C).
Expression profiling of NR subfamily 4This family consists of 3 members including NGFIB
(NR4A1), NURR1 (NR4A2), and NOR1 (NR4A3).Strikingly, mRNA levels of these 3 NRs decreased dra-matically in leiomyoma (Figure 2C). Although some hu-
man fibroid tissue samples showed a measurable decreasein NR4A1 protein levels (E29, E102, E105, and E254),most leiomyoma samples displayed a significant reduc-tion of NR4A2 and NR4A3 protein levels when com-pared with adjacent normal myometrial tissues (Figure2D). The quantitative heterogeneity in protein expressionlevels from sample to sample of leiomyoma and normaltissues is probably due to variations in physiological sta-tus of human subjects, sites of tissues harvested, and par-tial compensation of lower mRNA levels by altered trans-lational efficiency. Nonetheless, the expression of NR4Amembers in normal myometrium and significant drop oftheir levels in fibroids strongly suggest a possible but un-explored role of this subfamily in the etiology of UFs. Thissubfamily was further analyzed in subsequent studies (seebelow).
Expression profiling of NR subfamily 5, 6, and 0The NR5A members SF-1 and LRH-1 are functionally
similar with overlapping and distinct targets. They werecritical players in the regulation of cholesterol homeosta-sis in the liver and in steroidogenic tissues. We found thatmRNA levels of both SF1 and LRH1 were lower in leio-myoma. DAX-1 and SHP are unusual in that they don’thave a classic DNA-binding domain and in a broad senseare corepressors of other NRs. We found that mRNAlevel of DAX-1 was higher whereas that of SHP waslower in leiomyoma. Finally, the stand-alone member dis-tantly related to other NRs that forms the sixth sub-branch, GCNF, had a moderately higher mRNA level inleiomyoma tissues (Figure 2E).
Expression profiling of coregulatorsThe functions of NRs are modulated by coactivators
and corepressors (15, 22). Because we observed alteredexpression of several NRs in UFs, we also analyzedwhether expression of coregulators (HMGA2, ACF1,SWI, BRG1, SNF2H, HDAC3, Sin3A, NCOR1, SMRT,PGC1�, SRC1, SRC2, and SRC3) was also affected (Sup-plemental Figure 2). Consistent with published literature,we find that HMGA2 is significantly upregulated in uter-ine leiomyoma. No significant change in expression wasobserved for components of the repression complex,HDAC3, Sin3A, NCOR1, and SMRT. Among chromatinremodelers, whereas ACF1 showed a slight downregula-tion, SWI, BRG1, and SNF2H expression remain unal-tered. When coactivators were analyzed, SRC3 expres-sion was down slightly, but no major changes wereobserved in PGC1� and SRC1/2 expressions (Supple-mental Figure 2). Although these results suggest that co-regulators analyzed here remain unchanged in UFs, addi-tional analyses are clearly necessary for a firm conclusion.
doi: 10.1210/me.2012-1305 mend.endojournals.org 5

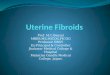
Figure 2. Subfamily-specific gene expression profiles of NRs in matched human leiomyoma (Leio) and myometrial (Myo) tissues. Using data fromFigure 1, subfamily-specific gene expression profiles of selected NRs from subfamily 1 (A), subfamily 2 (B), subfamily 4 (C), and subfamily 0, 3, 5,and 6 (E) in leiomyoma tissues were normalized to its expression in matched myometrium (set as 1.0-fold change). Values represent the mean �SD with 3 independent human samples. Protein levels of NR subfamily 4 were confirmed by Western blot in matched myometrial (M) andleiomyoma (L) tissues in 8 independent human samples (D). *P � .01; **P � .001 by Student’s t test.
6 Yin et al Nuclear Receptors in Uterine Fibroids Mol Endocrinol

Overexpressing NR4As decrease LSMCproliferation
Human UFs can be considered as a fibroproliferativedisease in the sense that leiomyoma-associated smoothmuscle cells and connective tissue fibroblasts not onlyproduce increased amounts of collagen and other ECMcomponents but also proliferate at a slightly higher ratethan that of normal myometrial cells. Because NR4A1(NGFIB), NR4A2 (NURR1), and NR4A3 (NOR1) wereall downregulated in leiomyoma tissues and NR4A mem-bers were shown to play roles in regulating cell apoptosisand proliferation (23), we reasoned that restoration ofNR4A expression should decrease growth of LSMCs.Therefore, primary LSMCs stably transduced with con-trol or NR4A expression constructs were generated.mRNA and protein expression of NR4A family membersin these cells are shown in Figure 3, A and B, respectively.These cells were analyzed for cell growth using alamar-Blue cell proliferation assay. Our results showed thatLSMCs overexpressing NR4As at levels approximatelyequal to those present in primary myometrial cells (Figure3B) proliferated more slowly than LSMCs transfectedwith empty expression construct (Figure 3C). As a con-trol, similar overexpression of NR4A members did notshow any effect on normal myometrial cell growth (Sup-plemental Figure 3). These results suggest that loss ofNR4A family members have functional proliferation con-sequences in LSMCs, and the wild-type levels of NR4Amembers are sufficient to maintain growth properties of
primary myometrial cells. Future studies will analyze themolecular targets of NR4A-dependent proliferation reg-ulation of myometrial and leiomyoma cells.
NR4A subfamily members regulate the expressionof genes implicated in UFs
Enhanced synthesis and deposition of ECM proteins,primarily composed of collagen, is a common feature inUF and other fibrotic tissues (24). Enhanced TGF� sig-naling has been shown to play a critical role in UFs, and inmicroarray analysis, NR4A1 (NGFIB/Nur77) was re-ported to be regulated by TGF� signaling in leiomyoma(25, 26). However, the functional significance of NR4Aexpression in UFs and its regulation by TGF� are stillunknown. Therefore, we systematically analyzed the geneexpression patterns of components of TGF� signalingand collagen genes in human myometrial and leiomyomatissue samples (Figure 4A and data not shown). AlthoughTGF�1 expression remained unchanged, TGF�3 expres-sion was significantly upregulated in uterine leiomyomasamples. We also noted higher expression of SMAD3, akey transcription factor and signal transducer of TGF�
signaling and fibrogenesis. Consistent with mRNA levels,immunoblot assays showed a similar upregulation ofTGF�3 and Smad3 protein levels in a majority of leiomy-oma tissue samples (Figure 4B). Interestingly, the level ofphosphorylated Smad3 (pSmad3 S423/425) was also en-hanced in at least 5 leiomyoma samples (E27, E63, E91,E102, and E254), suggesting the overall hyperactivation
Table 2. NR Gene Expression Profile During UF Development
InducedExpression Repressed Expression Constitutive Expression
UndetectableExpression
Subfamily 1 ROR� PPAR�/� TR�/� CARVDR ROR�/� RAR�/�/�
LXR� PPAR�RevERB�/�LXR�FXR�PXR
Subfamily 2 HNF4� RXR� RXR�/� HNF4�PNR COUP-TFI TR2
COUP-TFII TR4TLXCOUP-TFIII
Subfamily 4 NGFIBNURR1NOR1
Subfamily 0, 3, 5, 6 DAX-1 SHP PR ERR�ER�/� ERR� ERR�GCNF GR AR
MRSF1LRH1
For induced expression, ratio of mRNA levels in leiomyoma over myometrial tissues (Leio/Myo) � 1.6; repressed expression, Leio/Myo � 0.625;constitutive expression, 1.6 � Leio/Myo � 0.625; and undetectable expression, Ct value � 35.
doi: 10.1210/me.2012-1305 mend.endojournals.org 7

of TGF�3/Smad3 signaling pathway in UFs. When colla-gen genes were analyzed, we found that mRNAs for col-lagen 1A1, 6A1, 6A2, and 16A1 were upregulated in leio-myoma (Figure 4A). However, expression of some othercollagen genes, including COL3A1 and COL7A1, didnot change between human leiomyoma and myometrialtissue samples (data not shown).
To confirm that the tissue mRNA and protein levels ofthese genes reflect a consequence of decreased NR4A ex-pression in uterine leiomyoma, we generated primarymyometrial cells and LSMCs from matched tissue sam-ples and stably reconstituted expression of NR4A mem-bers individually in leiomyoma cells. Empty vector-trans-
fected myometrial and leiomyomaprimary cells served as controls.Consistent with tissue analyses re-sults, leiomyoma primary cellsshowed increased levels of TGF�3,SMAD3, and collagen gene expres-sion when compared with matchednormal myometrial primary cells(Figure 5A, compare first 2 lanes).Importantly, overexpression ofNR4As in primary leiomyoma cellsdecreased the expression of TGF�3,SMAD3, and collagen genes 1A1,6A1, 6A2, and 16A1 to the levelsobserved in primary myometrialcells. Consistent with mRNA ex-pression data (Figure 5A), immuno-blot assays also demonstrated resto-ration of TGF�3, Smad3, andcollagen protein expression inNR4A-overexpressed leiomyomaprimary cells at or near their levels inmyometrial primary cells (Figure5B). These results suggest that pri-mary cells recapitulate results ob-served in tissues and that NR4Amembers directly or indirectly regu-late key fibroid-associated genes.
To determine whether these genescould be direct targets of NR4As, weanalyzed the sequences of these tar-get genes spanning the �5kb to �2kb regions for the presence ofNGFIB-binding response elements(NBREs). Interestingly, we foundthat SMAD3 and TGF�3 harborsNBRE-related octanucleotide se-quence AAAT(GA)(CT)CA in theirregulatory regions; however, no
such sequences were observed in collagen genes exceptCOL16A1 gene, which contains multiple NBRE-relatedoctanucleotides, suggesting that the SMAD3, TGF�3,and COL16A1 genes may be directly regulated by NR4Amembers (Table 3). Because other collagen genes ana-lyzed here lacked NBREs near the �5 kb to �2 kb regu-latory regions but were regulated by NR4A expression,we analyzed for the presence of Smad3-binding elements(SBEs) in these genes. Indeed, there are multiple SBEs butno NBREs in COL1A1, -6A1, and -6A2 gene promoter/enhancer (Table 4). These analyses imply that NR4A reg-ulates expression of TGF�3 and SMAD3, which in turnregulate expression of collagen genes such as COL1A1,
Figure 3. Overexpression of NR4As decreased LSMC growth. Verifications of NR4Aoverexpression (OE) were performed by qRT-PCR (A) and Western blot (B) in primary LSMCsexpressing the indicated plasmid. In (B), primary myometrial cells are included as controls forcomparison of protein levels. mRNA levels are expressed as fold change using expression inLSMCs transduced with empty vector (Leio-empty) as 1.0. Shown on bottom right panels areresults of alamarBlue cell proliferation assays of LSMCs expressing the indicated plasmid (C).Values represent the mean�SD with 3 biological replicates (n � 8). * P � .01 by Student’s t test.
8 Yin et al Nuclear Receptors in Uterine Fibroids Mol Endocrinol

COL6A1, and COL6A2. Because COL16A1 gene hasNBRE-related octanucleotides in its promoter/enhancerelement, it is possibly regulated directly by NR4A mem-bers. Further genomic binding analyses will be necessaryto confirm these predictions.
LA treatment restores expression of a subset ofNRs and fibroid-associated genes
LA, a GnRH analog, is used for treatment of UFs. LAfunctions by downregulating sex steroid signaling. How-ever, it is not known whether LA also interferes with otherNR signaling and whether it has additional targets in UFetiology. To address this question, we performed expres-sion analyses of NRs, TGF�, SMAD, and collagen genesin tissue samples from patients treated with or withoutLA. mRNA of paired leiomyoma and myometrial tissue
samples (n � 3 for untreated or LA-treated) were ex-tracted for qRT-PCR analysis (Figure 6, A, C, and D, andSupplemental Figure 4). Surprisingly, our results showthat LA treatment restores gene expression and proteinlevels of NR4A1 and NR4A3, but not NR4A2, to thelevels present in untreated or LA-treated normal myome-trial samples (Figure 6, A and B). Previous clinical ob-servation reported that GnRH therapy lowered PRexpression in the UFs partially through inducing hypoes-trogenism (27). Our analysis shows that in addition to PRdownregulation, LA treatment also altered expression ofER�, GR, MR, and PPAR�/�, but not ER� or VDR at thelevel present in normal myometrial samples (Figure 6C).Finally, although leiomyoma tissues responded to LAtreatment in restoring expression of some but not all NRs,it has minimal effect on normal myometrial tissues. Theseresults therefore identify NR4A1, NR4A3, GR, MR, andPPAR� as additional downstream mediators of LA actionand may in part explain LA’s mode of action in UF treat-ment. We also analyzed whether LA treatment caused anychanges in mRNA and protein levels of TGF�, SMAD,and collagen (Figure 6, D and E). Although LA treatmentdid not change TGF�1 expression, mRNA and proteinlevels of TGF�3 were lower in LA-treated leiomyomatissues and comparable to those in normal myometrialtissues. Consistent with our results, Dou et al (28) re-ported a similar decrease in TGF�3 mRNA expression inLA-treated leiomyoma samples. Interestingly, we did notsee any major change in SMAD3 mRNA level in LA-treated samples (Figure 6D), although Smad3 protein andpSmad3 levels were comparable between LA-treated leio-myoma and myometrial samples (Figure 6E). Among col-lagen genes, mRNA levels of COL6A1 and -6A2 showedsignificant change, whereas no major changes were ob-served in COL1A1 and -16A1 mRNA levels. Similar re-sults were reported previously on the effect of LA treat-ment on COL1A1 expression (29, 30).
Discussion
The roles of estrogen, progesterone, and their receptorsare well established in the proliferation of both normaluterine epithelium and fibroids (2, 31). We tested thepossibility that other NRs may be causally involved inUFs. In this study, we report the comprehensive analysisof expression of all 48 NRs in matched myometrial andleiomyoma tissues. We identified several NRs, includingthe NR4A subfamily (NR4A1 or NGFIB, NR4A2 orNURR1, and NR4A3 or NOR1), as new candidate recep-tors playing critical roles in UFs. Using reconstitution ex-periments in primary leiomyoma cells, we show that the
Figure 4. Expression profiles of fibroid-associated genes in matchedhuman leiomyoma and myometrial tissues. A, Expression profiles ofselected TGF�/Smad signaling and collagen genes in matchedleiomyoma (Leio) and myometrial (Myo) tissues were measured by qRT-PCR. Values are expressed as fold change using expression inmyometrial tissues as 1.0. Values represent the mean � SD with 3independent human samples. B, Protein levels of TGF�/Smad signalingcomponents were measured by immunoblot assays in matchedmyometrial (M) and leiomyoma (L) tissues in the same 8 independenthuman samples shown in Figure 2D. *P � .05; **P � .01 by Student’st test.
doi: 10.1210/me.2012-1305 mend.endojournals.org 9

NR4A members play a previously unrecognized role inleiomyoma cell proliferation and ECM production.NR4As were reported to have both pro- and antiapop-totic effects depending on the cellular context and differ-ent extracellular signals (23). Consistent with our obser-vation that forced NR4A expression blocks leiomyomacell proliferation, in vascular smooth muscle cells, gain-and loss-of-function experiments revealed that both NG-FIB and NURR1 inhibit proliferation, although NOR1has been reported to enhance mitogenesis (32). How ap-parently redundant functions of NR4As regulate leiomy-oma cell proliferation remains to be determined. How-ever, consistent with our results, redundant functions of
all 3 members of the NR4A subfamily in other physiolog-ical processes, including memory formation, adipocytedifferentiation, cell metabolism, inflammation, and tu-mor angiogenesis, have been demonstrated (18, 33–37).
UFs are tumors featuring excessive synthesis and accu-mulation of disordered ECM proteins by activated myo-metrial smooth muscle cells or transformed myofibro-blasts derived from connective tissue fibroblasts. Thecritical role of TGF� in promoting uterine fibrosis hasbeen well documented (3). Upregulation of TGF�3 mayalso be associated with epithelial to mesenchymal transi-tion (EMT), and therefore, myofibroblasts derived fromthis transition may contribute to collagen accumulation
Table 3. Presence of NBRE-Related Octanucleotide Sequence on TGF�3, SMAD3, and Collagen Gene Promoters/Enhancers (�5 kb to �2 kb From Transcription Start Site [�1])
TargetsNBRE-Related Octanucleotide: AAAT(GA)(CT)CA
(Position, bp)TGF�3 �15863�1579SMAD3 181831825COL1A1 Not PresentCOL6A1 Not PresentCOL6A2 Not presentCOL16A1Site 1 �11113�1104Site 2 �10633�1056Site 3 �3083�301Site 4 134031347
Figure 5. NR4As regulate the expression of fibroid-associated genes. Gene expression profiles (A) and protein levels (B) of selected TGF�/Smadsignaling and collagen genes in leiomyoma (Leio) and paired myometrial (Myo) primary cells expressing the indicated plasmid were, respectively,measured by qRT-PCR and Western blot. mRNA values are expressed as fold change using expression in myometrial primary cells transduced withempty vector as 1.0 and represent the mean � SD with 3 biological replicates. *P � .05; **P � .01 by Student’s t test. For verification of NR4Aoverexpression in leiomyoma primary cells, please see Figure 3, A and B.
10 Yin et al Nuclear Receptors in Uterine Fibroids Mol Endocrinol

in UFs (3). However, the roles of NR4A in regulation ofthis profibrotic signaling pathway were not known. Weshowed that restoration of expression of each NR4A inLSMCs not only decreased the levels of TGF�3 andSmad3 but also downregulated expression of several col-lagens that are major ECM components. This indicatesthat loss of NR4A expression has a phenotypic conse-quence in UFs and implies that NR4As may protect nor-mal myometrium from fibrogenesis by controlling ex-pression of profibrotic genes (TGF�3, SMAD3, andmajor ECM protein) as shown in the model (Figure 7).
NR4As are generally described as constitutively activeorphan NRs with no identified endogenous ligands (34,36, 37). In our analysis, NR4As appear to function astranscriptional repressors of target genes. Consistent withour results, these receptors have been previously shown tofunction as transcriptional repressors in inflammation,ovarian development, and osteoblastic differentiation(38–40). NR4As function by binding to NBREs as mono-mers or to an everted repeat of the NBRE-related oc-tanucleotide (NurRE) as either homodimers or NR4Aheterodimers. As shown in Table 3, we find NBRE-re-lated octanucleotide on TGF�3 and SMAD3 gene en-hancers. We also find NBRE-related octanucleotides onCOL16A1 gene promoter, suggesting that it may be di-rectly regulated by NR4As. Because COL1A1, -6A1, and-6A2 did not have NBREs but contain several SBEs, wepropose that NR4As may thus function as a repressor ofTGF�3 and SMAD3, which in turn regulates expressionof some of these key collagen genes (Figure 7). It is alsoconceivable that NR4As may function as transcriptionalrepressors by interacting with other transcription factors.
Future studies will determine the mechanisms by whichNR4As regulate these and other target genes in UFs.
How NR4A expression is decreased in UFs is not clearat present. However, it has been demonstrated that ex-pression and activity of NR4As can be modulated by mul-tiple cell-signaling pathways, including cAMP/protein ki-nase/CREB, Wnt/�-catenin, G protein-coupled receptors,and MAPKs (34, 37, 40, 41). Whether these pathways canfunction as potential regulators of NR4A expression inUFs remains to be seen. Given that gene expression of all3 NR4As can be upregulated at varying levels by recon-stitutive expression of a single NR4A member in leiomy-oma primary cells, it is possible that NR4A transcriptioncan be autoregulated by NR4A subfamily members (Fig-ure 3A). However, more experiments are definitely re-quired to clarify the mechanism.
In addition to observing significant downregulation ofNR4As, we noted upregulation of ER, whereas PPAR�
and -� are significantly downregulated in UFs, which isconsistent with previous literature (21). Of the 3 isotypes,PPAR� is linked to UF. Treating leiomyoma cells withPPAR�- but not PPAR�- or PPAR�-specific agonists in-hibits estradiol (E2)-stimulated proliferation and gene ex-pression (42). The concomitant decreased mRNA levelsof PPARs and their heterodimeric partner RXRs in UFsuggests that suppression of the normal functions ofPPAR� may be necessary for growth and fibroid forma-tion in leiomyoma. PPAR� is negatively regulated bySmad-dependent TGF� signaling and lack of cellularPPAR� is associated with constitutively active Smad-de-pendent TGF�-induced profibrotic signaling (43) (Figure7). Additionally, ligand-activated PPAR� ameliorates fi-brosis in murine models. Therefore, PPAR� is regarded asa potent antifibrotic agent (44). Consistent with thesereports, we observed downregulation of antifibroticPPAR� and upregulation of profibrotic TGF�3/Smad3signaling and collagens in human uterine leiomyoma tis-sues (Figure 7).
How and whether estrogen signaling cross talk withNR4As in regulating fibroid-associated gene expressionin UFs is unclear. However, it appears that a complexcross talk among NRs may eventually manifest estrogenresponsiveness and UF phenotype. Specific changes inRORs in UFs are noteworthy because ROR� and -� havealso been linked to steroid metabolism (45). Doubleknockout of ROR� and ROR� in mice resulted in anincreased mRNA level of 17�-hydroxysteroid dehydroge-nase (17�-HSD) type 7 in liver, an enzyme convertingestrone to E2, suggesting that simultaneous downregula-tion of ROR� and ROR� might be associated with ele-vated E2/ER-mediated proliferative response in UFs (46).The correlation between upregulated ROR� and UFs is
Table 4. Presence of SBE Sequence on Collagen GenePromoters/Enhancers (�5 kb to �2 kb fromTranscription Start Site [�1])
Targets
SBE for Smad3:CAGACA
(Position, bp)COL1A1
Site 1 �36763�3671Site 2 �34523�3447Site 3 �24033�2398Site 4 �23613�2356Site 5 �6273�622Site 6 9583963Site 7 134131346Site 8 141731422
COL6A1Site 1 983103Site 2 136231367
COL6A2Site 1 �15133�1508Site 2 �7413�736Site 3 3503355
doi: 10.1210/me.2012-1305 mend.endojournals.org 11

unknown at present. Downregulation of COUP-TFI andII in UFs is also important to note. An in vitro study inhuman endometrial carcinoma cells demonstrated thatCOUP-TFs can suppress ER-activated response by com-peting for a composite ER-binding module of Ltf (47).COUP-TFs not only can compete for DNA binding butalso interact directly with ER to inhibit activation of ER-targeted genes (48). In addition, studies by Kurihara et al(49) implicated COUP-TFII in maintaining progesteronesuppression of uterine epithelial ER activity to establishproper implantation and showed an increased level ofuterine ER� mRNA in the uterus-specific COUP-TFIIknockout mice. The lower mRNA levels of COUP-TFI
and II may therefore contribute to enhanced ER/E2 sig-naling in UFs.
The NR5A proteins, SF-1 and LRH-1, are orphan NRsthat play major roles in regulating steroidogenesis in tis-sues such as adrenals and gonads. It seems paradoxicalthat LRH-1 and SF-1 were downregulated in UFs in viewof the importance of ovarian steroids in UF etiology.However, a study showed that granulosa cell-specificLRH-1–null mice are sterile due to anovulation (50). Theabsence of LRH-1 in granulosa cells causes increased aro-matase (CYP19) and E2 production as well as decreasedexpression of Silt1e1, an estrogen-specific sulfotrans-ferase contributing to a reduction in E2 bioavailability,
Figure 6. LA treatment restores expression of a subset of NRs and fibroid-associated genes in human leiomyoma tissues. Paired leiomyoma (Leio)and myometrial (Myo) tissue mRNAs were isolated from 3 independent untreated (LA�) and 3 independent LA-treated (LA�) human samples.Gene expression profiles of the NR4A subfamily (A), selected NRs (C), and TGF�/Smad signaling and collagen genes (D) were measured by qRT-PCR and normalized to its expression in Myo-LA� (set as 1.0-fold change). Values represent the mean � SD with 3 tissue samples for the LA� orLA� group. Protein levels of NR4A1/4A3 (B), and selected TGF�/Smad signaling components and collagens (E) were measured by Western blot inmatched myometrial (M) and leiomyoma (L) tissues from 3 independent LA-treated human samples (LA�). *P � .05; **P � .01 by Student’s t test.
12 Yin et al Nuclear Receptors in Uterine Fibroids Mol Endocrinol

which results in enhanced intrafollicular E2 signaling anddefective cumulus expansion. Further characterizationsare necessary to elucidate the functions of NR5As andtheir targets in UFs. Downregulation of SHP in UFs isexpected because it was shown that SHP has a preventa-tive role in hepatic and renal fibrosis (51, 52). Changes inGR and MR levels in UFs are also noteworthy. Consid-ering that proinflammatory factors are one of the effec-tors in UF development and glucocorticoids have potentanti-inflammatory activity, decreased GR expressionmay represent dampening of anti-inflammatory path-ways in UFs (3). A report by Beggah et al (53) showed thatheart-specific MR knockdown in the mice caused severecardiac fibrosis and heart failure. We wonder whetherMR downregulation in UFs plays a similar role. We ob-served significant upregulation of VDR expression inUFs. Although in vitro studies using immortalized humanleiomyoma cell lines showed that 1,25-dihydroxyvitaminD3 can suppress TGF�3-induced fibrogenic effects (54),VDR-null mice displayed significantly lower levels of se-rum E2 and ovarian aromatase expression compared withwild-type (55). Overall, it appears that coordinated
downregulation of RORs, COUP-TFs, SF1/LRH1, GR/MR, and SHPand upregulation of VDR and en-hanced VDR function may be neces-sary for E2-induced fibroprolifera-tive function of UFs.
Treatment options for UFs arelimited at best. Because agonists andantagonists are available for most ofthe NRs reported here, targetingsome of the identified NRs may pro-vide a viable option for better treat-ment of UFs. For example, pharma-cological agents regulating NR4Aactivities may be useful in UF treat-ment. Interestingly, 6-mercaptopu-rine, which is widely used as an an-tineoplastic and anti-inflammatoryagent and a specific activator ofNR4As, could be one such com-pound (56, 57). Recently, Ishikawaet al (58) described a xenograftmodel that can faithfully maintainthe original histological characteris-tics of human UFs by grafting leio-myoma tissue or cells beneath therenal capsule of immune-deficientmice. It will therefore be of great in-terest to use this model to evaluatethe effect of 6-mercaptopurine on
uterine leiomyoma tissue xenografts. In this context, wenote that LA treatment restored mRNA and protein ex-pression of NR4A1 and NR4A3 but not NR4A2 levels.Similarly, LA treatment promoted downregulation ofTGF�3/Smad3 signaling and only a few collagen genes.Although analysis of a larger cohort of tissue samples byimmunohistochemistry and immunoblot is clearly neces-sary for confirmation of these observations, our resultsnonetheless suggest that LA probably targets only a sub-set of NRs and fibroid-associated genes. These observa-tions raise the possibility that a combinatorial therapy ofLA with NR4A modulators may be more effective intreating UFs. Similarly, PPAR�-selective ligands in com-bination with NR4A modulators may be a novel treat-ment option over LA for uterine fibrosis. Finally, in con-trast to cardiac or liver fibrosis, UFs show bothproliferative and fibrotic phenotype, and similar fi-broproliferative symptoms are also noted in keloid for-mation in skin (59). Therefore, it would be interesting aswell to determine whether agents used for treatment ofkeloids will also be effective in UFs. In conclusion, thiswork demonstrates the power of focused comprehensive
Figure 7. Model proposing the novel roles of NR4A transcription factors in regulating TGF�/Smad signaling and fibroid-associated genes in normal myometrium and UFs. In normalmyometrial tissues, expression of NR4A transcription factors negatively regulates TGF�3, SMAD3,and COL16A1 to maintain the normal expression level of these genes. A high level of PPAR�,which inhibits Smad3 function, also contributes to maintain the normal expression of COL1A1,-6A1, and -6A2. In UFs, a significant drop of NR4As enhances levels of TGF�3, Smad3/pSmad3,and COL16A1. Smad3/pSmad3 in turn binds to SBEs on target collagen gene promoters andupregulates their expression. Levels of Smad3/pSmad3 are also enhanced by decreased levels ofPPAR� in UFs. Hyperexpression of these collagen genes can further lead to abnormal ECMproduction and uterine fibrosis. For more details, please see Discussion.
doi: 10.1210/me.2012-1305 mend.endojournals.org 13

expression analysis and identifies NR4A transcriptionfactors as potential and previously uncharacterized regu-lators of UFs and possibly other fibroproliferative dis-eases. Our hope is that novel therapeutic interventionscan be developed based on the differential expression ofspecific NR subfamilies that has been identified in thisreport.
Acknowledgments
We thank Dr Peter Tontonoz (the University of California, LosAngeles, Los Angeles, California) for providing NR4A con-structs and Stacy A. Druschitz for her assistance with collectionof leiomyoma tissues and generation of primary cells.
Address all correspondence and requests for reprints to: DrDebabrata (Debu) Chakravarti, Feinberg School of Medicine,Northwestern University, 303 E. Superior Street, Lurie 4-119,Chicago, Illinois 60611. E-mail: [email protected].
This work was supported in part by National Institutes ofHealth Grant P01 HD057877.
D.C. conceived the research plan. J.H.L., H.Y., and D.C.devised experiments. H.Y., J.H.L., and J.-Y.K. conducted ex-periments as follows: NR receptor and coregulator expressionprofile (J.H.L. and H.Y.); leio/myo primary cell proliferation(H.Y.); NR4A target mRNA and protein expression profile intissue and primary cells (H.Y.); NRs and NR4A target mRNAand protein expression analyses with LA treatment (H.Y. andJ.-Y.K.). H.Y., J.H.L., and D.C. analyzed data. J.H.L., H.Y.,and D.C. wrote the manuscript. E.E.M. provided reagents, an-alyzed human subjects and tissue collection data, and edited themanuscript. A.K.G., J.J.K., and S.B. provided inputs during thestudy and edited the manuscript.
Disclosure Summary: The authors state that they have noconflicts of interest.
References
1. Parker WH. Etiology, symptomatology, and diagnosis of uterinemyomas. Fertil Steril. 2007;87:725–736.
2. Marsh EE, Bulun SE. Steroid hormones and leiomyomas. ObstetGynecol Clin North Am. 2006;33:59–67.
3. Chegini N. Proinflammatory and profibrotic mediators: principaleffectors of leiomyoma development as a fibrotic disorder. SeminReprod Med. 2010;28:180–203.
4. Parker WH. Uterine myomas: management. Fertil Steril. 2007;88:255–271.
5. Ciarmela P, Islam MS, Reis FM, et al. Growth factors and myome-trium: biological effects in uterine fibroid and possible clinical im-plications. Hum Reprod Update. 2011;17:772–790.
6. Donnez J, Tatarchuk TF, Bouchard P, et al. Ulipristal acetate versusplacebo for fibroid treatment before surgery. N Engl J Med. 2012;366:409–420.
7. Sabry M, Al-Hendy A. Medical treatment of uterine leiomyoma.Reprod Sci. 2012;19:339–353.
8. Grudzien MM, Low PS, Manning PC, Arredondo M, Belton RJ Jr,Nowak RA. The antifibrotic drug halofuginone inhibits prolifera-
tion and collagen production by human leiomyoma and myometrialsmooth muscle cells. Fertil Steril. 2010;93:1290–1298.
9. Friedman AJ, Daly M, Juneau-Norcross M, Gleason R, Rein MS,LeBoff M. Long-term medical therapy for leiomyomata uteri: aprospective, randomized study of leuprolide acetate depot plus ei-ther oestrogen-progestin or progestin ’add-back’ for 2 years. HumReprod. 1994;9:1618–1625.
10. Stovall TG, Ling FW, Henry LC, Woodruff MR. A randomized trialevaluating leuprolide acetate before hysterectomy as treatment forleiomyomas. Am J Obstet Gynecol. 1991;164:1420–1423; discus-sion 1423–1425.
11. Germain P, Staels B, Dacquet C, Spedding M, Laudet V. Overviewof nomenclature of nuclear receptors. Pharmacol Rev. 2006;58:685–704.
12. Jeong Y, Xie Y, Xiao G, et al. Nuclear receptor expression definesa set of prognostic biomarkers for lung cancer. PLoS Med. 2010;7:e1000378.
13. Bensinger SJ, Tontonoz P. Integration of metabolism and inflam-mation by lipid-activated nuclear receptors. Nature. 2008;454:470–477.
14. Buranapramest M, Chakravarti D. Chromatin remodeling and nu-clear receptor signaling. Prog Mol Biol Transl Sci. 2009;87:193–234.
15. Rosenfeld MG, Lunyak VV, Glass CK. Sensors and signals: a co-activator/corepressor/epigenetic code for integrating signal-depen-dent programs of transcriptional response. Genes Dev. 2006;20:1405–1428.
16. Holbeck S, Chang J, Best AM, Bookout AL, Mangelsdorf DJ, Mar-tinez ED. Expression profiling of nuclear receptors in the NCI60cancer cell panel reveals receptor-drug and receptor-gene interac-tions. Mol Endocrinol. 2010;24:1287–1296.
17. Xie CQ, Jeong Y, Fu M, et al. Expression profiling of nuclearreceptors in human and mouse embryonic stem cells. Mol Endocri-nol. 2009;23:724–733.
18. Chao LC, Bensinger SJ, Villanueva CJ, Wroblewski K, Tontonoz P.Inhibition of adipocyte differentiation by Nur77, Nurr1, and Nor1.Mol Endocrinol. 2008;22:2596–2608.
19. Fusco A, Fedele M. Roles of HMGA proteins in cancer. Nat RevCancer. 2007;7:899–910.
20. Klemke M, Meyer A, Nezhad MH, et al. Overexpression ofHMGA2 in uterine leiomyomas points to its general role for thepathogenesis of the disease. Genes Chromosomes Cancer. 2009;48:171–178.
21. Englund K, Blanck A, Gustavsson I, et al. Sex steroid receptors inhuman myometrium and fibroids: changes during the menstrualcycle and gonadotropin-releasing hormone treatment. J Clin Endo-crinol Metab. 1998;83:4092–4096.
22. Kininis M, Kraus WL. A global view of transcriptional regulationby nuclear receptors: gene expression, factor localization, and DNAsequence analysis. Nucl Recept Signal. 2008;6:e005.
23. Li QX, Ke N, Sundaram R, Wong-Staal F. NR4A1, 2, 3–an orphannuclear hormone receptor family involved in cell apoptosis andcarcinogenesis. Histol Histopathol. 2006;21:533–540.
24. Ohara N. Sex steroidal modulation of collagen metabolism in uter-ine leiomyomas. Clin Exp Obstet Gynecol. 2009;36:10–11.
25. Luo X, Ding L, Xu J, Chegini N. Gene expression profiling ofleiomyoma and myometrial smooth muscle cells in response totransforming growth factor-�. Endocrinology. 2005;146:1097–1118.
26. Luo X, Ding L, Xu J, Williams RS, Chegini N. Leiomyoma andmyometrial gene expression profiles and their responses to gonad-otropin-releasing hormone analog therapy. Endocrinology. 2005;146:1074–1096.
27. Kim JJ, Sefton EC. The role of progesterone signaling in the patho-genesis of uterine leiomyoma. Mol Cell Endocrinol. 2012;358:223–231.
28. Dou Q, Zhao Y, Tarnuzzer RW, et al. Suppression of transforming
14 Yin et al Nuclear Receptors in Uterine Fibroids Mol Endocrinol

growth factor-� (TGF�) and TGF� receptor messenger ribonucleicacid and protein expression in leiomyomata in women receivinggonadotropin-releasing hormone agonist therapy. J Clin Endocri-nol Metab. 1996;81:3222–3230.
29. Stewart EA, Rhoades AR, Nowak RA. Leuprolide acetate-treatedleiomyomas retain their relative overexpression of collagen type Iand collagen type III messenger ribonucleic acid. J Soc GynecolInvest. 1998;5:44–47.
30. Britten JL, Malik M, Levy G, Mendoza M, Catherino WH. Gonad-otropin-releasing hormone (GnRH) agonist leuprolide acetate andGnRH antagonist cetrorelix acetate directly inhibit leiomyoma ex-tracellular matrix production. Fertil Steril. 2012;98:1299–1307.
31. Li Q, Kannan A, DeMayo FJ, et al. The antiproliferative action ofprogesterone in uterine epithelium is mediated by Hand2. Science.2011;331:912–916.
32. van Tiel CM, de Vries CJ. NR4All in the vessel wall. J SteroidBiochem Mol Biol. 2012;130:186–193.
33. Hawk JD, Abel T. The role of NR4A transcription factors in mem-ory formation. Brain Res Bull. 2011;85:21–29.
34. Pearen MA, Muscat GE. Nuclear hormone receptor 4A signaling:implications for metabolic disease. Mol Endocrinol. 2010;24:1891–1903.
35. Pei L, Waki H, Vaitheesvaran B, Wilpitz DC, Kurland IJ, TontonozP. NR4A orphan nuclear receptors are transcriptional regulators ofhepatic glucose metabolism. Nat Med. 2006;12:1048–1055.
36. McMorrow JP, Murphy EP. Inflammation: a role for NR4A orphannuclear receptors? Biochem Soc Trans. 2011;39:688–693.
37. Mohan HM, Aherne CM, Rogers AC, Baird AW, Winter DC, Mur-phy EP. Molecular pathways: the role of NR4A orphan nuclearreceptors in cancer. Clin Cancer Res. 2012;18:3223–3228.
38. Bonta PI, van Tiel CM, Vos M, et al. Nuclear receptors Nur77,Nurr1, and NOR-1 expressed in atherosclerotic lesion macro-phages reduce lipid loading and inflammatory responses. Arterio-scler Thromb Vasc Biol. 2006;26:2288–2294.
39. Wu Y, Ghosh S, Nishi Y, Yanase T, Nawata H, Hu Y. The orphannuclear receptors NURR1 and NGFI-B modulate aromatase geneexpression in ovarian granulosa cells: a possible mechanism forrepression of aromatase expression upon luteinizing hormonesurge. Endocrinology. 2005;146:237–246.
40. Rajalin AM, Aarnisalo P. Cross-talk between NR4A orphan nu-clear receptors and �-catenin signaling pathway in osteoblasts.Arch Biochem Biophys. 2011;509:44–51.
41. Chen HZ, Liu QF, Li L, et al. The orphan receptor TR3 suppressesintestinal tumorigenesis in mice by downregulating Wnt signalling.Gut. 2012;61:714–724.
42. Houston KD, Copland JA, Broaddus RR, Gottardis MM, FischerSM, Walker CL. Inhibition of proliferation and estrogen receptorsignaling by peroxisome proliferator-activated receptor � ligands inuterine leiomyoma. Cancer Res. 2003;63:1221–1227.
43. Ghosh AK, Wei J, Wu M, Varga J. Constitutive Smad signaling andSmad-dependent collagen gene expression in mouse embryonic fi-broblasts lacking peroxisome proliferator-activated receptor-�.Biochem Biophys Res Commun. 2008;374:231–236.
44. Ghosh AK, Vaughan DE. Fibrosis: is it a coactivator disease? FrontBiosci. 2012;4:1556–1570.
45. Jetten AM. Retinoid-related orphan receptors (RORs): critical rolesin development, immunity, circadian rhythm, and cellular metabo-lism. Nucl Recept Signal. 2009;7:e003.
46. Kang HS, Angers M, Beak JY, et al. Gene expression profilingreveals a regulatory role for ROR� and ROR� in phase I and phaseII metabolism. Physiol Genom. 2007;31:281–294.
47. Liu Y, Yang N, Teng CT. COUP-TF acts as a competitive repressorfor estrogen receptor-mediated activation of the mouse lactoferringene. Mol Cell Biol. 1993;13:1836–1846.
48. Klinge CM, Silver BF, Driscoll MD, Sathya G, Bambara RA, Hilf R.Chicken ovalbumin upstream promoter-transcription factor inter-acts with estrogen receptor, binds to estrogen response elementsand half-sites, and inhibits estrogen-induced gene expression. J BiolChem. 1997;272:31465–31474.
49. Kurihara I, Lee DK, Petit FG, et al. COUP-TFII mediates proges-terone regulation of uterine implantation by controlling ER activ-ity. PLoS Genet. 2007;3:e102.
50. Duggavathi R, Volle DH, Mataki C, et al. Liver receptor homolog1 is essential for ovulation. Genes Dev. 2008;22:1871–1876.
51. Zhang Y, Hagedorn CH, Wang L. Role of nuclear receptor SHP inmetabolism and cancer. Biochim Biophys Acta. 2011;1812:893–908.
52. Jung GS, Kim MK, Choe MS, et al. The orphan nuclear receptorSHP attenuates renal fibrosis. J Am Soc Nephrol. 2009;20:2162–2170.
53. Beggah AT, Escoubet B, Puttini S, et al. Reversible cardiac fibrosisand heart failure induced by conditional expression of an antisensemRNA of the mineralocorticoid receptor in cardiomyocytes. ProcNatl Acad Sci U S A. 2002;99:7160–7165.
54. Halder SK, Goodwin JS, Al-Hendy A. 1,25-Dihydroxyvitamin D3reduces TGF-�3-induced fibrosis-related gene expression in humanuterine leiomyoma cells. J Clin Endocrinol Metab. 2011;96:E754–E762.
55. Kinuta K, Tanaka H, Moriwake T, Aya K, Kato S, Seino Y. VitaminD is an important factor in estrogen biosynthesis of both female andmale gonads. Endocrinology. 2000;141:1317–1324.
56. Wansa KD, Muscat GE. TRAP220 is modulated by the antineo-plastic agent 6-mercaptopurine, and mediates the activation of theNR4A subgroup of nuclear receptors. J Mol Endocrinol. 2005;34:835–848.
57. Ordentlich P, Yan Y, Zhou S, Heyman RA. Identification of theantineoplastic agent 6-mercaptopurine as an activator of the or-phan nuclear hormone receptor Nurr1. J Biol Chem. 2003;278:24791–24799.
58. Ishikawa H, Ishi K, Serna VA, Kakazu R, Bulun SE, Kurita T.Progesterone is essential for maintenance and growth of uterineleiomyoma. Endocrinology. 2010;151:2433–2442.
59. Mukhopadhyay A, Chan SY, Lim IJ, Phillips DJ, Phan TT. The roleof the activin system in keloid pathogenesis. Am J Physiol CellPhysiol. 2007;292:C1331–C1338.
doi: 10.1210/me.2012-1305 mend.endojournals.org 15