Embed Size (px)
Citation preview

Bioelectromagnetics 21:413^421 (2000)
Exposure to Strong ELFMagnetic FieldsDoes Not Alter Cardiac Autonomic
Control Mechanisms
Charles Graham,1* Antonio Sastre,1 Mary R. Cook,1 Robert Kavet,2
Mary M. Gerkovich,1 and Donald W. Riffle1
1Midwest Research Institute, Kansas City, MO2EPRI, PaloAlto, CA
Clinical and epidemiological studies attest that alterations in heart rate variability (HRV) arepredictive of specific types of cardiovascular morbidity and mortality in otherwise healthy persons.Recent reports also suggest that changes in HRV may be associated with exposure to intermittentmagnetic fields (60 Hz, 28.3 mT) in the laboratory and that mortality is increased in cardiac diseasecategories related to altered HRV for utility workers whose jobs involve longer exposure to elevatedmagnetic fields. This study combined three approaches to learn more about the specific exposurecircumstances under which changes in HRV occur. First, cardiac autonomic control, as indexed byHRV spectral analysis measures, was measured in 24 men during exposure to a much higherintensity field than any previously examined (resultant flux density� 127.3mT [1273 milliGauss,mG]). Second, HRV measures from the same individual were compared across three relevant testconditions: intermittent and continuous field exposure and during a no-exposure, control condition.Third, electrocardiographic data were analyzed to determine if the precise timing of when themagnetic field switched on or off in relation to the cardiac cycle results in phase-resetting of thehuman cardiac rhythm. HRV measures were not altered by either field exposure conditioncompared to the control condition, and no evidence for a phase-resetting mechanism was found.Further research is needed to resolve the differences between the present and the earlier laboratory-based studies of HRV and to determine if cardiac rhythm disturbances are associated with exposureto the more complex magnetic fields found in the man-made environment. Bioelectromagnetics21:413±421, 2000. ß 2000 Wiley-Liss, Inc.
Key words: EMF; human studies; ECG; autonomic nervous system; cardiovascular; heartdisease
INTRODUCTION
Heart rate variability (HRV) is a well-establishedphysiological phenomenon arising from the interplayof the sympathetic and parasympathetic branches ofthe autonomic nervous system (ANS). Quantitativeassessment of HRV provides a reliable, noninvasivemethod to assess autonomic control of cardiac activity[Akselrod et al., 1981; Malik and Camm, 1995]. Thismeasure is of particular interest because of its value inpredicting future types of cardiovascular morbidityand mortality in otherwise healthy persons. Forexample, reductions in speci®c components of theHRV frequency spectrum have recently predicted thedevelopment of heart disease in four large prospectivecohort studies [Martin et al., 1987; Tsuji et al., 1996;Decker et al., 1997; Liao et al., 1997]. The prognosticvalue of this measure has also been demonstrated instudies of coronary artery disease [Hayano et al.,
1990], post-infarction risk [Bigger et al., 1993], andsudden cardiac death [Malik et al., 1990].
Sastre et al. [1998] described three double-blind,laboratory-based studies in which suf®cient cardiacdata were collected to make the ®rst detailedexamination of magnetic ®eld exposure effects onHRV. The 77 healthy, young men in these studies wereexposed during night sleep to circularly polarized
ß2000Wiley-Liss, Inc.
ÐÐÐÐÐÐContract grant sponsors: EPRI; Contract grant number: WO8021-12; Contract grant sponsor: US Department of Energy; Contractgrant number: 85X-SN602C.
*Correspondence to: Charles Graham, Ph.D., Midwest ResearchInstitute, 425 Volker Boulevard, Kansas City, MO 64110.E-mail: [email protected]
Received for review 13 October 1998; Final revision received 20October 1999

60 Hz magnetic ®elds at resultant ¯ux densities ofeither 14.1mT or 28.3mT (141 mG or 283 mG),respectively. When the men were intermittentlyexposed to the higher intensity magnetic ®eld,statistically signi®cant alterations in the HRV fre-quency measures were observed compared to shamcontrol conditions. These effects did not occur whenexposure to the ®elds was continuous, nor did theyoccur when the men were exposed to the lowerintensity ®eld. The speci®c pattern of effects observedwith intermittent, high-intensity ®eld exposure was areduction in power in the Low band (0.04±0.15 Hz) ofthe HRV frequency spectrum and an increase in powerin the High band (0.15±0.40 Hz) of the spectrum.Power alterations in the Low spectral band re¯ect theactions of thermoregulatory and blood pressure controlmechanisms on the heart, primarily mediated throughthe sympathetic branch of the ANS. Alterations inpower in the High spectral band re¯ect respiratorycontrol mechanisms and consequent sinus arrhythmia,mediated through the parasympathetic branch of theANS. Overall, these studies suggest that ®eld intensityand exposure pattern may be important, and perhapsinteractive, factors determining the type and extent ofcardiac effects observed.
One hypothesis to be derived from the exposureresults reported by Sastre et al. [1998], when combinedwith medical knowledge about the potential healthconsequences of reduced HRV, is that mortality fromarrhythmia-related disease and acute myocardialinfarction (i.e., heart attack) may be increased inworkers with prolonged elevated exposure to magnetic®elds. In contrast, mortality from atherosclerosis andchronic coronary heart disease should not be asso-ciated with such exposure. The former two diseasecategories are linked to altered cardiac autonomiccontrol, while the latter two are not [Tsuji et al., 1994,1996; Dekker et al., 1997].
Savitz and colleagues [1999] recently tested theabove hypothesis in their examination of mortalityfrom cardiovascular disease in relation to occupationalmagnetic ®eld exposure in a well-characterized cohortof approximately 140,000 male electric utility workersemployed in the U.S. between 1950 and 1988. Afteradjusting for age, race, social class, year, and activework status, mortality from arrhythmia-related diseaseand acute myocardial infarction was found to beassociated with longer duration in jobs with elevatedmagnetic ®eld exposure. Mortality ratios ranged from1.5±3.3 in the uppermost categories. Mortality due toatherosclerosis and chronic coronary heart disease wasnot associated with these exposure indices. Theseresults are consistent with the hypothesis that arosefrom Sastre et al. [1998], and they suggest an
association between magnetic ®eld exposure andspeci®c types of cardiac disease.
The present research combined three approachesto learn more about the speci®c circumstances underwhich changes in HRV occur. First, we evaluatedcardiac autonomic control, as indexed by HRV spec-tral analysis measures, during nocturnal exposureto a much higher intensity magnetic ®eld thanany previously examined (resultant ¯ux density�127.3mT). This intensity is relevant to the upper rangeof occupational exposures and to the recommendationsof the International Commission on Non-IonizingRadiation Protection (ICNIRP) limiting exposure inthe general population to 100 mT at 50 Hz [ICNIRP,1998]. Second, we compared HRV measures obtainedfrom the same individual across three relevant testconditions: intermittent and continuous ®eld exposureand in a no-exposure, sham control condition. Third,we performed a detailed analysis of electrocardio-graphic data obtained during intermittent magnetic®eld exposure to determine if a known physiologicalmechanism was responsible for the reported alterationsin HRV. Previous research using a variety of cellularand tissue preparations has demonstrated that when astimulus occurs at selected time points within thecardiac cycle; this can either delay or accelerate thetiming of subsequent cardiac impulses [Clay et al.,1984, 1990; Chay and Lee, 1985; Anumonwo et al.,1991; Demir et al. 1999]. This phenomenon isgenerally referred to as phase-resetting behavior. Theaim of our analysis was to determine whether theprecise timing of the switching on or switching offof the intermittent magnetic ®eld in relation to thecardiac cycle resulted in phase-resetting of the humancardiac rhythm.
MATERIALS AND METHODS
Subjects
The research participants were 24 healthy malevolunteers recruited from the local community (meanage 21 yr, range 19±34 yr), who had regular sleep anddietary habits and were not taking medications. Thestudy protocol was reviewed and approved by theMidwest Research Institute (MRI) InstitutionalReview Board for Human Studies and writteninformed consent was obtained from each volunteerprior to his participation.
Experimental Design
The biological magnitude of the reduction inHRV observed by Sastre et al. [1998] was approxi-mately 17%. The statistical power in the present study
414 Graham et al.

was greater than 0.92 to detect a similar degree ofsuppression in HRV at the 0.05 level of signi®cance.The exposure study used a randomized, double-blind,cross-over design in which each subject served as hisown control. The subjects slept in the exposure facilityat MRI on three test nights from 23:00 hours to 07:00hours. On the sham control night, the magnetic ®eldgeneration coils were not energized, and the men wereexposed only to the ambient 60 Hz magnetic ®eldmeasured in the laboratory (�0.2mT, 2 mG). Thisintensity range is characteristic of residential expo-sures. On another night, they were continuouslyexposed to a generated 60 Hz magnetic ®eld at aresultant ¯ux density of 127.3mT. On a third night, themen were again exposed to the 127.3 mT ®eld, butthis time using the intermittent exposure protocoldescribed in Sastre et al. [1998]. This consisted ofalternating 1 h ®eld-on and ®eld-off periods. During®eld-off hours, the coils were not energized. Duringthe ®eld-on hours, the ®eld cycled on and off at15 s intervals. The order of sham control and ®eldexposure sessions was counterbalanced such thatequal numbers of subjects participated in each con-dition on each night. Eight subjects were randomlyassigned to be tested in order 1 (sham/intermittent/continuous, SIC), eight in order 2 (ICS), and eight inorder 3 (CSI). The electrocardiogram (ECG) wasrecorded continuously throughout each test session forlater quantitative analysis of HRV and other cardiacendpoints.
Exposure Facility
The characteristics of the exposure facility havebeen documented as part of the US National EMFRAPID research program and are described in Doynovet al. [1999]. Brie¯y, the subject slept on a bed inthe exposure test room with his body oriented north-south. The horizontal axis of the uniform (� 2.5%)circularly polarized ®eld was oriented north-south,and the vertical axis was perpendicular to the ¯oor.The ®elds were generated by two Merritt-typeconcentric coil systems located out of sight behindthe ceiling, walls, and ¯oor of the exposure test room(a cube about 2.4 m on a side). A zero-crossingtechnique allowed the magnetic ®elds to be switchedon and off without at the same time generating highfrequency magnetic ®eld transients. The facility'sautomated double-blind control system preventedsubjects and investigators from knowing when shamcontrol or ®eld exposure conditions were in effectin any given session. This system has proveneffective in multiple human exposure studies [e.g.,Cook et al., 1992; Graham et al., 1994; Sastre et al.,1998].
Measures
ECG recording sensors were attached to skinsites on the right clavicle and the seventh intercostalspace under the left axillary midline, corresponding tothe standard ECG Lead II con®guration. The ECGwas recorded continuously through the night using aNeurodata Physiological Data Acquisition System(Model 15, Astro-Med, Inc., West Warwick, RI).ECG data were sampled at 256 Hz, stored on magneticmedia for later off-line analysis, and custom softwarewas used to identify the R waves (ventricularcontractions) in the ECG. Cardiac data were processedand analyzed as described in Sastre et al. [1998].Brie¯y, the time between each two R waves corre-sponds to one cardiac interbeat interval (IBI). Theseries of IBI values was ®rst converted to instantaneousheart rate to provide a regularly spaced time series witha 1 s resolution. The time period selected for analysiswas midnight to 06:00 hours. Each hour was dividedinto three equal periods containing 1024 points. ADigital Fourier Transform was performed on eachperiod with the results expressed as the power densityspectrum; i.e., power at a given frequency in thephysiological ranges of interest for HRV within theNyquist limit (0.0±0.5 Hz). Spectral data were sub-mitted to statistical analysis to evaluate differencesbetween sham control, and the intermittent andcontinuous exposure conditions for each subject.Analyses were conducted for total power in allfrequency bands of the HRV spectrum, absolute andpercent power in the Low and High frequency bands,and for the power ratio between the Low and Highbands. The Low (0.04±0.15 Hz) and High (0.15±0.40 Hz) frequency spectral bands were de®nedaccording to consensus guidelines issued by theEuropean Society of Cardiology and the NorthAmerican Society of Pacing and Electrophysiology[Anonymous, 1996].
In addition, the Field Status Questionnaire (FSQ,Cook et al. [1992]) was completed in the morning aftereach session to assess the effectiveness of the double-blind control system in preventing conscious percep-tion of the presence of the magnetic ®eld. Subjects andinvestigators independently answered three questions:`̀ In your judgment, was the ®eld on or off?'' `̀ Howcon®dent are you of this judgment? (a 1±5 scale)''`̀ What are you basing this judgment on?''
Procedures
Subjects were instructed to refrain from consum-ing alcohol for 24 h prior to a test session and to haveno caffeine after 17:00 hours on the day of a session.They arrived at the laboratory at 22:00 hours, changed
Cardiac Autonomic Control Under Magnetic Fields 415

into sleep wear, vital signs were recorded, and the ECGrecording sensors were attached. The men got into bedin the exposure test room, and at 23:00 hours the lightswere turned off and the double-blind/®eld-controlsystem was activated. Subjects remained in bed until07:00 hours and were monitored through the night viaclosed-circuit TV, open audio intercom and thephysiological recording system. The FSQ was com-pleted in the morning.
Analysis of variance for mixed designs(ANOVA) was the primary statistical technique usedto evaluate the HRV spectral analyses results. Expo-sure Type (sham control, intermittent, continuous),Hour (midnight to 06:00 hours), and Period (1±3 ineach h) were the within-subject variables, andExposure Order (1, 2, or 3) was the between-subjectsvariable. Results were considered statistically signi®-cant if P� 0.05. The probability values were correctedfor lack of sphericity by using the Huynh-Feldt epsilontechnique. Signi®cant main effects or interactions werefollowed up with simple effects analyses.
Analysis of Possible Phase-Resetting of theCardiac Rhythm
The present intermittent exposure protocol calledfor the magnetic ®eld to be presented in alternating 1 h®eld-on and ®eld-off periods and for the ®eld to cycleon and off at 15 s intervals throughout each ®eld-onhour. Thus, in the four ®eld-on hours betweenmidnight and 07:00 hours, each volunteer was exposedto a magnetic ®eld that changed in intensity (either0.0 mT or 127.3mT) a total of 960 times.
The cardiac cycle consists of an orderly series ofbioelectrical events within each heart beat which trackthe depolarization (associated with contraction) andrepolarization of the specialized muscle cells of themain pumping chambers of the heart. Since the ®eldtransitions were presented on a ®xed time schedule andthe heart beat to its own intrinsic rhythm, eachtransition occurred by chance at some random timepoint within the cardiac cycle. Analyses were per-formed to test two hypotheses. First the presence ofphase-resetting in our data should be re¯ected bymeasurable differences in cardiac cycle duration forthose heart beats that occur immediately after vs.immediately before a ®eld transition. Second, whetherthe timing differences re¯ect a slowing or accelerationof heart rate will depend on when in the cardiac cyclethe ®eld transition occurs.
Final technical preparations for the phase-reset-ting analyses were completed after the study wasstarted; thus, the required combination of ®eldexposure and cardiac data was available only for thelast 18 all-night intermittent exposure test sessions.
The computerized data records from these sessionscontained the raw ECG in one channel. A secondchannel was used to continuously record the magnetic®eld waveform from a standard pick-up coil placed inthe exposure facility. Both channels were simulta-neously digitized at 256 Hz. This allowed the exacttime for each ®eld transition and for any point withinthe cardiac cycle, to be resolved with an error ofmeasurement of � 3.9 ms. This level of sensitivity wasmore than adequate to address the issues of interest,since mean heart rate over the intermittent exposurenights was 56.3 beats per minute, which corresponds toa cardiac cycle duration of 1066 ms.
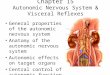
Custom software automated the data selectionand comparison process. A total of 17 280 ®eldtransitions occurred in the 18 intermittent exposuresessions analyzed. The software ®rst selected the timewhen each ®eld transition occurred (measured in mselapsed from midnight). The cardiac cycle was de®nedas the time between successive R waves in the ECG.The software determined the time of occurrence of theR-waves in the ECG for the ®ve heart beats thatpreceded each ®eld transition and the ®ve heart beatsthat followed each transition. Figure 1 illustrates thisprocess by using a segment of the continuous ECGrecording from one volunteer. As can be seen, a ®eld-on transition point is identi®ed as well as the ®vecycles preceding and following the ®eld change. Thetiming for each cycle is indicated by a small trianglecoinciding with the R wave.
Analysis terms were operationally de®ned asfollows. The time of each ®eld transition within a
Fig. 1. The electrocardiogram (ECG) of the18 volunteers and thewaveform of the intermittent magnetic field were simultaneouslysampled at 256 Hz.The time of each field-on or field off transition(N�17280), andthedurationoffive cardiaccycles (R^R intervals)beforeandaftera transition,were calculated.InthisexampleoftheECG from one volunteer, the five cardiac cycles of interest sur-roundinga field-on transition ( $) are indicatedbyan~over the Rwaves.
416 Graham et al.

cardiac cycle was expressed as a percent of the elapsedtime between successive R waves (T%). For example,the value T1 represented a ®eld transition that occurredimmediately after an R wave, at 1% of the time fromthat R wave to the next. Likewise, a value of T99
represented a ®eld transition that took place just beforean R wave, and a value of T50 represented a ®eldtransition that occurred exactly halfway between twoconsecutive R waves. The quantity D was used toidentify the difference between the duration in ms of acardiac cycle after the ®eld transition and the durationof the corresponding cardiac cycle before the ®eldtransition. Thus, the quantities D1 through D5 repre-sented the timing differences associated respectivelywith the ®ve pairs of heart beats surrounding each ®eldtransition.
RESULTS
Quality Control Measures
Analysis of the FSQ rating data indicated thatneither the subjects (chi-square� 3.51, df 2, P� 0.17)nor the investigators (chi-square� 1.12, df 2, P�0.57) were able to judge when the magnetic ®elds werepresent. These results con®rm the effectiveness of thedouble-blind control procedures. Ambient temperature(mean 22.2� 0.1 �C) and relative humidity (mean45.7%,� 8.9%) in the test room did not changesigni®cantly over the night, and neither was affectedby exposure type. Monitoring of ®eld intensity insidethe test room con®rmed that exposure conditions weremaintained as planned for each subject.
Heart Rate
The expected slowing of heart rate over the nightwas observed (F� 35.30, df 5, 105, P < 0.001). Therewas also a signi®cant Hour by Period interaction(F� 2.53, df 10,210, P� 0.007) indicating thatdecreases in heart rate were greatest during the ®rsthour of the night. However, these decreases did notdiffer under either exposure condition when comparedwith the control condition.
Heart Rate Variability
Following the recommendations of the consensusguidelines [Anonymous, 1996], data are presented forboth percent and absolute power in the Low and Highfrequency bands of the HRV spectrum. Table 1presents hourly values for percent power in each testcondition for the 18 subjects. Table 2 presents similardata for absolute power. Analysis of variance failed toreveal any ®eld-related differences in percent poweramong the three test conditions. Speci®cally, percent T
AB
LE
1.
Per
cen
tP
ow
erV
alu
esin
the
Lo
wa
nd
Hig
hH
RV
Fre
qu
ency
Ba
nd
sin
All
Tes
tC
on
dit
ion
sfo
r1
8M
ale
Volu
nte
ers
Ho
ur
1H
ou
r2
Ho
ur
3H
ou
r4
Hour
5H
our
6(0
0:0
0±
01
:00
ho
urs
)(0
1:0
0±
02
:00
ho
urs
)(0
2:0
0±
03
:00
ho
urs
)(0
3:0
0±
04
:00
ho
urs
)(0
4:0
0±
05:0
0hours
)(0
5:0
0±
06:0
0hours
)
Tes
tco
nd
itio
nM
ean
SE
Ran
ge
Mea
nS
ER
ang
eM
ean
SE
Ran
ge
Mea
nS
ER
ange
Mea
nS
ER
ange
Mea
nS
ER
ange
Low
HR
Vb
and
(0.0
4±
0.1
5H
z)S
ham
con
tro
l1
1.7
0.4
5±
21
11
.30
.44
±2
01
1.9
0.4
4±
24
11
.80
.54
±22
11.2
0.5
4±
25
11.4
0.4
5±
22
Co
nti
nu
ou
sex
po
sure
12
.10
.56
±2
41
1.0
0.4
4±
19
11
.70
.46
±2
11
0.9
0.3
5±
18
11.2
0.4
5±
18
11.0
0.4
4±
20
Inte
rmit
ten
tex
posu
re1
2.2
0.4
7±
22
10
.80
.45
±1
91
1.1
0.4
5±
22
11
.20
.54
±23
10.8
0.4
4±
22
11.5
0.4
5±
22
Hig
hH
RV
ban
d(0
.15
±0
.40
Hz)
Sh
amco
ntr
ol
14
.51
.14
±4
21
3.5
0.7
4±
26
13
.70
.94
±3
61
4.6
0.9
3±
43
14.1
1.1
4±
46
11.7
0.7
4±
38
Co
nti
nu
ou
sex
po
sure
12
.50
.74
±3
01
3.1
0.9
4±
41
12
.90
.73
±2
91
3.2
0.8
3±
33
14.7
1.0
4±
37
13.2
0.7
4±
35
Inte
rmit
ten
tex
posu
re1
3.2
0.9
3±
31
14
.81
.03
±3
81
3.1
0.8
4±
33
14
.20
.94
±49
13.7
0.7
4±
27
13.2
0.7
4±
35
Cardiac Autonomic Control Under Magnetic Fields 417

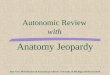
power in the Low HRV band (F� 0.86, df 10, 210,P� 0.57) and in the High HRV band (F� 1.17, df 10,210, P� 0.31) was not different across the night ineither ®eld condition when compared with the controlcondition. Hourly values for percent power in the Lowband across the night are plotted for all test conditionsin Figure 2. As can be seen, no consistent patternof ®eld-related changes in power is apparent in thisclinically-relevant portion of the HRV frequencyspectrum.
Absolute power in the Low band also was notin¯uenced by ®eld exposure. The pattern of hourlychanges in absolute power in the High band, however,was found to differ under continuous exposure,compared with either sham or intermittent exposureconditions (F� 2.43, df 10,210, P� 0.03). This effectappears to be a spurious statistical interaction arisingfrom an unexplained increase in High band power atonly one point in the night (05:00±06:00 hours) in thecontinuous exposure condition, but not in the other twoconditions. No coherent pattern of ®eld-relatedchanges in High band power was observed over thenight.
Phase Resetting Analysis
We determined whether cardiac cycle durationfor heart beats 1±5 immediately before and immedi-ately after each ®eld transition differed as a function ofwhen in the cardiac cycle the ®eld transition occurred.Thus, for the ®rst heart beat immediately following a®eld transition, the quantity D1 was plotted for eachsubject as a function of all percent values from T1 toT99 across all 960 ®eld transitions per exposure night.If phase-resetting was operative in the data set, the plotof D1 vs. T% should exhibit a markedly nonlinearshape, with positive values of D1 corresponding to aspeci®c T% range, and negative values of D1
corresponding to a complementary T% range. Table 3summarizes the linear regressions performed for D1 for
Fig. 2. Percent power in the LowHRV frequencybandwasnot dif-ferent during continuous or intermittent magnetic field exposure(60 Hz,127.3 mT), compared to controlconditions.
TA
BL
E2
.A
bso
lute
Po
wer
(s2)
Va
lues
inth
eL
ow
an
dH
igh
HR
VF
req
uen
cyB
an
ds
inA
llT
est
Co
nd
itio
ns
for
18
Male
Volu
nte
ers
Ho
ur
1H
ou
r2
Ho
ur
3H
ou
r4
Hour
5H
our
6(0
0:0
0±
01
:00
ho
urs
)(0
1:0
0±
02
:00
ho
urs
)(0
2:0
0±
03
:00
ho
urs
)(0
3:0
0±
04
:00
ho
urs
)(0
4:0
0±
05:0
0hours
)(0
5:0
0±
06:0
0hours
)
Tes
tco
nd
itio
nM
ean
SE
Ran
ge
Mea
nS
ER
ang
eM
ean
SE
Ran
ge
Mea
nS
ER
ange
Mea
nS
ER
ange
Mea
nS
ER
ange
Low
HR
Vb
and
(0.0
4±
0.1
5H
z)S
ham
con
tro
l3
48
31
18
±1
07
33
16
34
27
±1
80
03
38
26
34
±1
14
33
45
32
31
±1126
358
28
33
±1239
352
26
33
±1227
Co
nti
nu
ou
sex
po
sure
37
23
32
5±
14
61
31
52
93
0±
15
09
32
72
43
9±
11
29
31
32
95
2±
1196
320
37
32
±1977
382
26
60
±934
Inte
rmit
ten
tex
po
sure
32
12
53
4±
99
92
61
25
16
±8
93
28
32
63
1±
10
56
31
62
43
1±
1068
317
22
37
±881
348
25
39
±1210
Hig
hH
RV
ban
d(0
.15
±0
.40
Hz)
Sh
amco
ntr
ol
38
94
74
9±
22
65
38
65
14
7±
20
81
42
66
07
1±
26
17
43
75
43
5±
2252
485
64
57
±2507
368
36
64
±1546
Co
nti
nu
ou
sex
po
sure
40
95
24
2±
20
90
41
86
34
8±
31
91
41
35
32
9±
22
95
39
45
14
0±
2095
434
67
47
±3512
534
61
44
±2182
Inte
rmit
ten
tex
po
sure
33
23
74
4±
18
10
34
34
94
0±
28
12
36
04
44
0±
16
53
42
54
63
0±
2072
450
52
72
±2284
437
45
68
±1939
418 Graham et al.

the 18 subjects. Each regression for each subject wasbased on 480 ®eld-on and 480 ®eld-off transitions. Noevidence of phase-resetting was found. Values for D1
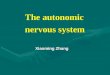
are uniformly distributed around zero, and they ®t theT% line with a slope of zero. Figure 3 illustrates thisnegative pattern of results using ®eld-on and ®eld-offtransition data from one volunteer. Similar analyses ofthe quantities D2 through D5 did not alter the aboveresults, nor did analyses of the successive averages for2, 3, 4, and 5 cardiac cycles before a ®eld transitioncompared to similar averages following the ®eldtransition. Finally, examination of individual plots forthe 18 men revealed no nonzero slopes or otherdeviations from linearity.
DISCUSSION
HRV spectral analysis measures were not chan-ged in this group of healthy young men during all-night exposure to 60 Hz magnetic ®elds at highoccupational intensity levels, when compared withsimilar measures obtained under equivalent no-expo-sure, sham control conditions. Extensive analyses ofthe ECG also failed to reveal any evidence that thehuman cardiac rhythm is altered through the operationof a phase-resetting mechanism during intermittentmagnetic ®eld exposure. These results are notconsistent with earlier laboratory-based observationsof ®eld-related reductions in HRV [Sastre et al., 1998].
The present study was not designed as a strictreplication of the earlier research reported by Sastreet al. [1998], and several major differences are worthnoting. First, the present volunteers were exposed tomagnetic ®elds at a much higher intensity (127.3mTvs. 28.3mT) than in the previous studies. Reports ofnonlinear dose±response relationships and of intensityor frequency selectivity effects, are not at all un-common in bioelectromagnetics research [see Grahamet al., 1994 for review]. To our knowledge, all suchreports involve exposure to an electric ®eld alone or toa combined electric and magnetic ®eld; however, theydo raise the possibility that alterations in HRV mayoccur at lower, but not at higher, magnetic ®eldintensities.
TABLE 3. Summary of Linear Regressions for Delta1 Phase-Resetting Analysis; Each Regression is Based on 480 Field-onand 480 Field-off Transitions
Variable Field-on transitions Field-off transitions
Slope (ms/T%)Mean (18 subjects) ÿ0.05 0.02SEM 0.08 0.0495% CL ÿ0.21 to 0.12 ÿ0.06 to 0.10
Intercept (ms)Mean 0.34 0.02SEM 4.30 1.9495% CL ÿ0.87 to 0.94 ÿ0.41 to 0.41
Fig. 3. Effects of switching on (A) and switching off (B) a 60 Hz magnetic field at 127.3 mT on thehuman cardiac rhythm. D1 (the time difference between the R^R interval immediately before andafter a field transition) is plotted in seconds for one volunteer as a function of T% (the point in thecardiac cyclewhena field transitionoccurred, expressedasapercent of the elapsed timebetweensuccessive R waves). Data from 480 field-on and 480 field-off transitions are presented. D1 wasuniformlydistributedaroundzero, and fit theT% linewithaslopeof zero.
Cardiac Autonomic Control Under Magnetic Fields 419

Two additional studies that bear directly on thisissue have now been performed. Graham et al. [1997]repeated the present study using the earlier 28.3 mT®eld intensity and again found no effects on HRV.In a second study [Graham et al., 1998], HRV wasevaluated during intermittent exposure to the 28.3mTmagnetic ®eld, but this time the ®eld was presentedat three different frequencies (16 Hz, 40 Hz, 60 Hz).The 16 Hz frequency was selected because HRV iscontrolled from centers in the brain and this frequencyis well within the electrophysiological range of fre-quencies recorded from the human brain; 40 Hzprovided an intermediate comparison frequency.Exposure to the 16 Hz ®eld (but not to the other ®eldconditions) was associated with a signi®cant(P� 0.02) reduction in percent power in the Low bandof the HRV frequency spectrum. Taken together, theseresults provide some support for the notion offrequency selectivity.
One difference between the present study and theSastre et al. [1998] studies may be relevant. Volunteersin the present study slept undisturbed through the testnights. In the Sastre et al. [1998] studies, a nurseentered the exposure room each hour through the nightto obtain a blood sample for hormonal analysis. Bloodsamples were obtained through an indwelling catheterinserted into an arm vein, so that disturbance to thevolunteers was minimal. Nonetheless, many volun-teers were somewhat aroused from sleep by thisprocedure, and individuals differed in their degree ofresponsiveness. Physiological arousal level duringsleep, as indexed by EEG-de®ned sleep stages, isknown to be linked to alterations in HRV [Malik andCamm, 1995; Vaughn et al., 1995; Otzenbergeret al.,1998]; thus, these protocol differences betweenstudies could potentially lead to variable or insuf®cientadaptation to the laboratory environment. Under suchcircumstances, the changing demands placed oncardiac control mechanisms, through altered levels ofsympathetic nervous system activity or disruption ofthe natural patterns of sleep, might also lead todivergent HRV results across studies.
The negative results obtained in the phase-resetting analysis are of particular interest. Little isknown about possible biological mechanisms thatcould provide the necessary link between exposure topower-frequency magnetic ®elds and alterations inhuman physiology. A biophysically plausible hypoth-esis is that cellular activity or function may bemodulated by the electric ®elds induced in the bodyby exposure to the ambient magnetic ®eld. Of course,the issue here is whether ambient magnetic ®eldexposure, particularly at the present high level ofintensity, provides an exogenous stimulus of suf®cient
strength to compete with and alter the endogenous®elds generated by the heart. Calculations derivedfrom the detailed, whole body dosimetric model ofDawson et al. [1999] indicate that the 127.3mT ®eldwould induce an average electric ®eld across heartmuscle at an intensity between 1.3 and 1.7 mV/munder in situ exposure conditions; local maxima areonly four-fold higher. This is far below the intensity ofthe endogenous ®elds measured in the heart of the dog.Hart and Gandhi [1998] report these endogenous ®eldsin the 40±70 Hz band range from 7.7 to 25 mV/m,depending on the method of calculation used.
Taken together, these earlier reports suggest thatdirect excitation of the human heart by the present127.3mT ®eld is extremely unlikely. The uniformlynegative effects observed with human volunteers in thepresent study demonstrate that phase-resetting in not acredible physiological mechanism for the reportedalterations in HRV, and they provide direct experi-mental support for the earlier model- and animal-basedcalculations. Induced electric ®eld effect on braincenters, however, is still a plausible explanation for theSastre et al. [1998] results. Calculations indicate thatthe earlier exposure conditions would induce anelectric ®eld of about 1.8 mV/m in the cortical areasof brain. This magnitude of induced electric ®eld isabove the reported threshold for biological responses[Gailey et al., 1997].
The previous results by Sastre et al. [1998]formed the basis for the epidemiologic hypothesis ofSavitz et al. [1999] that, if workplace exposure alteredthe autonomic nervous system's control of cardiacfunction in a clinically important manner, thenincreased mortality associated with exposure wouldoccur for arrhythmias and acute myocardial infarction,but not for chronic coronary heart disease or athero-sclerosis. The epidemiological results were consistentwith the hypothesis, using as exposure measures bothlength of employment in exposed occupations (e.g.,electrician) and integrated magnetic ®eld exposure(mT±years) derived from a job-exposure matrix. Giventhese results, it is important to resolve the reasons forthe inconsistencies in the laboratory series of studiesand to understand whether and how acute responsesrelated to cardiac control mechanisms may havechronic implications.
ACKNOWLEDGMENTS
We wish to thank Dr. Paul Gailey for initiallysuggesting the idea for the phase-resetting analysis,Richard Ulrich for creating the custom software usedin ECG signal processing and the phase-resettinganalyses, and project staff members Steven J.
420 Graham et al.

Hoffman (programming), Jeffrey L. Hackman (ECGsignal processing), and Brian E. Peterson (datamanagement).
REFERENCES
Akselrod S, Gordon D, Ubel FA, Shannon DC, Berger AC. 1981.Power spectrum analysis of heart rate ¯uctuation: aquantitative probe of beat-to-beat cardiovascular control.Science 213:220±222.
Anonymous. 1996. Heart rate variability: standards of measure-ment, physiological interpretation and clinical use. Specialreport, Task Force of the European Society of Cardiologyand the North American Society of Pacing and Electro-physiology. Circulation 93:1043±1065.
Anumonwo JM, Delmar M, Vinet A, Michaels DC, Jalife J. 1991.Phase resetting and entrainment of pacemaker activity insingle sinus nodal cells. Circ Res 68:1138±1153.
Bigger JT, Fleiss JL, Rolnitzky LM, Steinman RC. 1993.Frequency domain measures of heart rate variability toassess risk late after myocardial infarction. Circulation88:927±934.
Chay TR, Lee YS. 1985. Phase resetting and bifurcation in theventricular myocardium. Biophys J 47:641±651.
Clay JR, Guevara MR, Shrier A. 1984. Phase resetting of therhythmic activity of embryonic heart cell aggregates.Experiment and theory. Biophys J 45:699±714.
Clay JR, Brochu RM, Shrier A. 1990. Phase resetting of embryonicchick atrial heart cell aggregates. Experiment and theory.Biophys J 58:609±621.
Cook MR, Graham C, Cohen HD, Gerkovich MM. 1992. Areplication study of human exposure to 60-Hz Fields:Effects on neurobehavioral measures. Bioelectromagnetics13:261±285.
Becker JM, Schouten EG, Klootwijk P, Pool J, Swenne CA,Kromhout D. 1997. Heart rate variability from shortelectrocardiographic recordings predicts mortality from allcauses in middle-aged and elderly men. Am J Epidemiol145:899±908.
Dawson TW, Caputa K, Stuchly MA. 1999. Magnetic induction at60 Hz in the human heart: A comparison between the in situand isolated scenarios. Bioelectromagnetics 20:233±243.
Demir SS, Clark JW, Giles WR. 1999. Parasympathetic modula-tion of sinoatrial node pacemaker activity in rabbit heart: aunifying model. Am J Physiol 276:H2221±H2244.
Doynov P, Cohen HD, Cook MR, Graham C. 1999. Test facility forhuman exposure to AC and DC magnetic ®elds. Bioelec-tromagnetics 20:101±111.
Gailey P, Sastre A, McGaughy RE. 1997. Internal electric ®eldsproduced by EMF, dosimetry, and endogenous ®elds. In:Portier C, Wolfe M, editors. EMF Science ReviewSymposium Breakout Group Reports for TheoreticalMechanisms and In Vitro Research Findings. NationalInstitute of Environmental Health Sciences, Durham, NC. p55±70. www.niehs.nih.gov/emfrapid/home.htm
Graham C, Cook MR, Cohen HD, Gerkovich MM. 1994. A doseresponse study of human exposure to 60-Hz electric andmagnetic ®elds. Bioelectromagnetics 15:447±463.
Graham C, Sastre A, Cook MR. 1997. Effects of magnetic ®elds oncardiac control mechanisms. EPRI Report No. TR-108251.
Graham C, Sastre A, Cook MR, Rif¯e DW. 1998. Variation inmagnetic ®eld frequency: effects on heart rate variability.Paper presented at the 20th annual Meeting of theBioelectromagnetics Society, St. Pete Beach, FL (AbstractP-54B).
Hart RA, Gandhi OP. 1998. Comparison of cardiac-inducedendogenous ®elds and power-frequency induced exogenous®elds in an anatomical model of the human body. Phys MedBiol 43:3083±3099.
Hayano J, Sakakibara Y, Yamada M, Ohte N, Fujinami T,Yokoyama K, Watanabe Y, Takata K. 1990. Decreasedmagnitude of heart rate spectral components in coronaryartery disease: its relation to angiographic severity. Circula-tion 81:1217±1224.
International Commission on Non-Ionizing Radiation Protection,ICNIRP. 1998. Guidelines for limiting exposure to time-varying electric, magnetic, and electromagnetic ®elds (up to300 GHz). Health Phys 74:494±522.
Liao D, Cai JC, Rosamond WD, Barnes RW, Hutchinson RG,Whitsel EA, Rautaharju P, Heiss G. 1997. Cardiacautonomic function and incident coronary heart disease: apopulation-based case-cohort study. Am J Epidemiol145:696±706.
Malik M, Farrell T, Camm AJ. 1990. Circadian rhythm of heart ratevariability after acute myocardial infarction and its in¯uenceon the prognostic value of heart rate variability. Am JCardiol 66:1049±1054.
Malik M, Camm AJ. 1995. Heart rate variability. Armonk, NewYork: Futura Publishing Co.
Martin GJ, Magid NM, Myers G, Barnett PS, Schaad JW, Weiss JS,Lesch M, Singer DH. 1987. Heart rate variability and suddendeath secondary to coronary artery disease during ambula-tory electrocardiographic monitoring. Am J Cardiol 60:86±89.
Otzenberger H, Gron®er C, Simon C, Charloux A, Ehrhart J,Piquard F, Brandenberger G. 1998. Dynamic heart ratevariability: a tool for exploring sympathovagal balancecontinuously during sleep in men. Am J Physiol 275:H946±H950.
Sastre A, Cook MR, Graham C. 1998. Nocturnal exposure tointermittent 60-Hz magnetic ®elds alters human cardiacrhythm. Bioelectromagnetics, 19:98±106.
Savitz DA, Liao D, Sastre A, Kleckner RC, Kavet R. 1999.Magnetic ®eld exposure and cardiovascular disease mortal-ity among electric utility workers. Am J Epidemiol149:135±142.
Tsuji H, Venditti FJ, Manders ES, Evans JC, Larson MG, FeldmanCL, Levy D. 1994. Reduced heart rate variability andmortality risk in an elderly cohort: the Framingham HeartStudy. Circulation 90:878±883.
Tsuji H, Martin G, Larson MG, Venditti FJ, Manders ES, Evans JC,Feldman CL, Levy D. 1996. Impact of reduced heart ratevariability on risk for cardiac events: the Framingham HeartStudy. Circulation 94:2850±2855.
Vaughn BV, Quint SR, Messenheimer JA, Robertson KR. 1995.Heart period variability in sleep. Electroencephalogr ClinNeurophysiol 94:155±162.
Cardiac Autonomic Control Under Magnetic Fields 421