Embed Size (px)
Citation preview

Journal of Plastic, Reconstructive & Aesthetic Surgery (2011) 64, 1448e1453
Exceedingly expanded retroauricular flaps formicrotia reconstruction
Zhenyu Chen a, Weina Zhang a,b, Jinjun Huang b,*, Jizhen Ren a,Yuehua Zhu a
aDepartment of Plastic and Cosmetic Surgery, Affiliated Hospital of Medical Collage, Qingdao University, Qingdao, ChinabDepartment of Plastic and Cosmetic Surgery, ZhuJiang Hospital, Southern Medical University, Guangzhou 510282,Guangdong Province, China
Received 31 January 2011; accepted 21 June 2011
KEYWORDSTissue expander;Auricularreconstruction;Costal cartilage
* Corresponding author.E-mail address: surgeonhuangjj@1
1748-6815/$-seefrontmatterª2011Bridoi:10.1016/j.bjps.2011.06.025
Summary Background: Theauthorsproposehereanewstrategy toobtainexceedinglyexpandedretroauricular mastoid skin for sufficient coverage of the three-dimensional autogenous costalcartilage framework generally used in auricular reconstruction surgery. From February 2000 toSeptember 2009, 42 microtia reconstructions were performed using this new strategy.Methods: Auricular reconstructionwasperformed in three surgical stages. In thefirst stage, a 50-mlkidney-shaped expander was inserted subcutaneously in the retroauricular mastoid region. From 5to8mlsalinewas then injected into theexpanderevery4daysuntil thefinalvolumeoftheexpanderreached100e120ml. In the secondstage,wedivided theexpandedmastoid skin intoa superior two-third region (flap A) and an inferior one-third region (flap B, rotation flap). Autogenous costal carti-lage framework was then enveloped by these expanded flaps. Tragus construction and conchalexcavation was performed in the third stage.Results: All patients were followed up from 6 months to 4 years after reconstruction. A total of 36cases reported to be satisfied with the appearance of good shape, accurate size, right orientation,and duplication of well-detailed structures. Further revision was requested by six of the total.Complications in this series includes one case of haematoma, two cases of partial evection of theexpanded skin and two cases of partial skin necrosis of the helix. All the complicationswere treatedappropriately.Conclusion: Exceedingexpansion canprovide sufficient retroauricular non-hair-bearing skin tissuesfor draping the auricular cartilage framework. Skin grafts and retroauricular fascial flap are notneeded any more. Patients are usually satisfied with their reconstructive auricles as regards thesize, location, projection, convolution, skin-colourmatching, etc. Exceedinglyexpanded retroauri-cular flaps are the appropriate envelope for the auricular cartilage framework.ª 2011 British Association of Plastic, Reconstructive and Aesthetic Surgeons. Published byElsevier Ltd. All rights reserved.
63.com (J. Huang).
tishAssociationofPlastic,ReconstructiveandAestheticSurgeons.PublishedbyElsevierLtd.All rightsreserved.
Exceedingly expanded retroauricular flaps for microtia reconstruction 1449
Introduction removed 3 and 10 days after operation, respectively. The
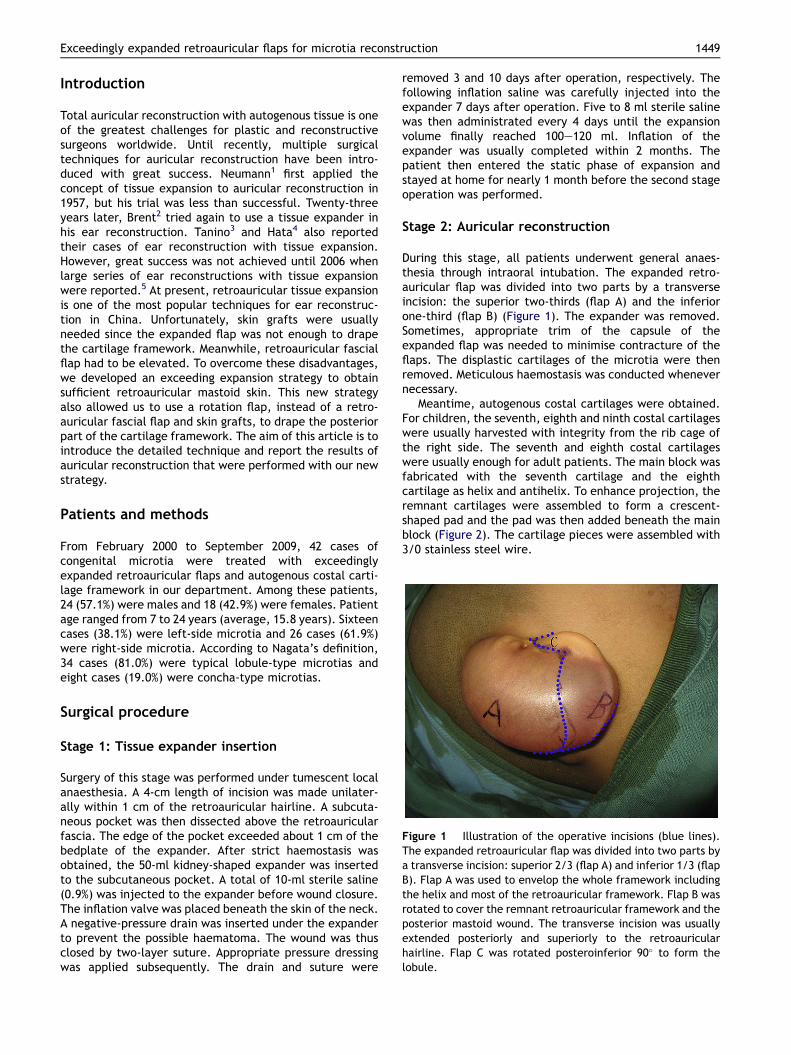
Figure 1 Illustration of the operative incisions (blue lines).The expanded retroauricular flap was divided into two parts bya transverse incision: superior 2/3 (flap A) and inferior 1/3 (flapB). Flap A was used to envelop the whole framework includingthe helix and most of the retroauricular framework. Flap B wasrotated to cover the remnant retroauricular framework and theposterior mastoid wound. The transverse incision was usuallyextended posteriorly and superiorly to the retroauricularhairline. Flap C was rotated posteroinferior 90� to form thelobule.
Total auricular reconstruction with autogenous tissue is oneof the greatest challenges for plastic and reconstructivesurgeons worldwide. Until recently, multiple surgicaltechniques for auricular reconstruction have been intro-duced with great success. Neumann1 first applied theconcept of tissue expansion to auricular reconstruction in1957, but his trial was less than successful. Twenty-threeyears later, Brent2 tried again to use a tissue expander inhis ear reconstruction. Tanino3 and Hata4 also reportedtheir cases of ear reconstruction with tissue expansion.However, great success was not achieved until 2006 whenlarge series of ear reconstructions with tissue expansionwere reported.5 At present, retroauricular tissue expansionis one of the most popular techniques for ear reconstruc-tion in China. Unfortunately, skin grafts were usuallyneeded since the expanded flap was not enough to drapethe cartilage framework. Meanwhile, retroauricular fascialflap had to be elevated. To overcome these disadvantages,we developed an exceeding expansion strategy to obtainsufficient retroauricular mastoid skin. This new strategyalso allowed us to use a rotation flap, instead of a retro-auricular fascial flap and skin grafts, to drape the posteriorpart of the cartilage framework. The aim of this article is tointroduce the detailed technique and report the results ofauricular reconstruction that were performed with our newstrategy.
Patients and methods
From February 2000 to September 2009, 42 cases ofcongenital microtia were treated with exceedinglyexpanded retroauricular flaps and autogenous costal carti-lage framework in our department. Among these patients,24 (57.1%) were males and 18 (42.9%) were females. Patientage ranged from 7 to 24 years (average, 15.8 years). Sixteencases (38.1%) were left-side microtia and 26 cases (61.9%)were right-side microtia. According to Nagata’s definition,34 cases (81.0%) were typical lobule-type microtias andeight cases (19.0%) were concha-type microtias.
Surgical procedure
Stage 1: Tissue expander insertion
Surgery of this stage was performed under tumescent localanaesthesia. A 4-cm length of incision was made unilater-ally within 1 cm of the retroauricular hairline. A subcuta-neous pocket was then dissected above the retroauricularfascia. The edge of the pocket exceeded about 1 cm of thebedplate of the expander. After strict haemostasis wasobtained, the 50-ml kidney-shaped expander was insertedto the subcutaneous pocket. A total of 10-ml sterile saline(0.9%) was injected to the expander before wound closure.The inflation valve was placed beneath the skin of the neck.A negative-pressure drain was inserted under the expanderto prevent the possible haematoma. The wound was thusclosed by two-layer suture. Appropriate pressure dressingwas applied subsequently. The drain and suture were
following inflation saline was carefully injected into theexpander 7 days after operation. Five to 8 ml sterile salinewas then administrated every 4 days until the expansionvolume finally reached 100e120 ml. Inflation of theexpander was usually completed within 2 months. Thepatient then entered the static phase of expansion andstayed at home for nearly 1 month before the second stageoperation was performed.
Stage 2: Auricular reconstruction
During this stage, all patients underwent general anaes-thesia through intraoral intubation. The expanded retro-auricular flap was divided into two parts by a transverseincision: the superior two-thirds (flap A) and the inferiorone-third (flap B) (Figure 1). The expander was removed.Sometimes, appropriate trim of the capsule of theexpanded flap was needed to minimise contracture of theflaps. The displastic cartilages of the microtia were thenremoved. Meticulous haemostasis was conducted whenevernecessary.
Meantime, autogenous costal cartilages were obtained.For children, the seventh, eighth and ninth costal cartilageswere usually harvested with integrity from the rib cage ofthe right side. The seventh and eighth costal cartilageswere usually enough for adult patients. The main block wasfabricated with the seventh cartilage and the eighthcartilage as helix and antihelix. To enhance projection, theremnant cartilages were assembled to form a crescent-shaped pad and the pad was then added beneath the mainblock (Figure 2). The cartilage pieces were assembled with3/0 stainless steel wire.

Figure 2 The picture of fabricated 3D costal cartilageauricular framework.
Figure 3 The appearance of the reconstructive ear imme-diately after operation. A, B and C represents the redistribu-tion of flap A, flap B and flap C, respectively.
1450 Z. Chen et al.
The cartilage framework was then inserted into thepocket of flap A and anchored to the fascia of the mastoidregion. An appendant longitudinal incision at the posterioredge of flap A was conducted to fix the framework to itsappropriate position. Flap A enveloped almost the wholeframework, including helix and most of the retroauricularbackbone. The transverse incision usually must beextended posteriorly and superiorly to the retroauricularhairline. Flap B was rotated backwards to cover theremnant retroauricular framework and retroauricularmastoid wounds. Sometimes, when flap A was insufficientto cover the anteroinferior part of the cartilage framework,we elevated flap C (Figure 1) and rotated it posteroinferior90� to help forming the lobule (Figure 3). Negative-pressuredrainage was produced by a 10-ml disposable syringe con-nected to a catheter which was inserted between the flapsand the cartilage framework. The appearance of thereconstructive ear was vivid immediately after suction(Figure 3). All wounds were closed by two-layer suture.Pressure dressing was applied on the operative region. Thedrain and suture was removed 5 and 10 days after opera-tion, respectively.
Stage 3: Modification of the reconstructed ear
Six months after the second stage, the reconstructed earwas further modified. Tragus reconstruction was the mostcommon procedure during the third stage. The tragus wasreconstructed by a doubled-up transverse flap from the
conchal area. The fascial tissue of the conchal floor wasexcised to deepen the concha. Meanwhile the helix rootwas prolonged to the appropriate region. Other works suchas repairing the retroauricular scar and excising theredundant remnant tissue were performed according to thepatient’s request.
Results
All patients were followed up from 6 months to 4 yearsafter the reconstruction. The reconstructed ears wereestimated by both patients (or their parents if under 18years old) and our surgical team. Thirty-six cases weresatisfied with the appearance of good shape, accurate size,right orientation and duplication of well-detailed structures(Figures 4e6), while six cases thought their reconstructedears needed further revision.
Complications in this series were as follows: One case ofhaematoma. However, skin expansion was successfullyaccomplished after evacuation of haematoma. Two cases ofpartial evection of the expanded skin, which appeared atthe early stage of inflation. Evection of the expanded skinwas probably due to fold and angulation of the expander instage one. It could be treated by regulation of inflationspeed and local massage of the salient skin. Two cases ofpartial skin necrosis of the helix and exposure of theframework. Noticeably, the wound was limited in those twocases and was cured by skim of the exposed cartilage,debridement and dressing changes (Figure 7). We did notexperience wound dehiscence, infection and partialnecrosis of the expanding flap and exposure of expander.
Discussion
Auricular reconstruction with autogenous costal cartilagewas first applied by Tanzer.6 Brent reviewed his 20 years’experience in auricular repair with autogenous rib cartilagegrafts in 1992.7 The technique of harvesting and fabricatingthe cartilage was refined by Nagata8 and Park,9 lately.

Figure 4 Example pictures of the case 1. A 22-year-old male patient with lobular microtia in right side. Left, A lateral view of theexpanded flap with a volume of 105 ml. Right, lateral view of the reconstructed ear one month after the operation. He was verysatisfied with the appearance of reconstructed ear.
Exceedingly expanded retroauricular flaps for microtia reconstruction 1451
Currently, autogenous costal cartilage for ear reconstruc-tion is a commonly used technique and it also achievedgreat success in China.10e12
Because the rib cartilage in Asians is thinner than that inCaucasians,12 Asian plastic surgeons preferred attachingover sculpting when fabricating the cartilage framework.Nagata8 used to harvest the sixth through ninth costalcartilages en bloc because they were much easier to beobtained and were usually in junction with each other. Theperichondrium was left completely intact in the donor side.This technique showed lower morbidity of haemopneumo-thorax and deformity of the chest wall. According to ourexperience, the seventh, eighth and ninth costal cartilageswere suitable to be harvested for fabrication of the mainblock, helix and antihelix. Those cartilage modules werethen assembled onto an integrity framework. We also leftthe perichondrium intact on the donor site. Chest-wall
Figure 5 Example pictures of the case 2. An 18-year-old boy wi(108 ml). Middle, lateral view of the reconstructed ear 10 days posthe symmetrical cranioauricular sulcus 10 days after operation.
deformity was not seen at present. Firmin13 categorisedthree types of frameworks used to correct microtia: type I(a complete framework), type II(no tragus) and type III (notragus or antitragus). The choice of these three types wasdictated by the presence or absence of the normal tragusand/or antitragus. According to Firmin’s principles, the earwas reconstructed in two stages and tragus was recon-structed concurrently. Our strategy is different from that ofFirmin. We do not excessively undermine under theexpanded flap anteroinferiorly to save the blood supply ofthe expanded flap. Hence, the tragus was not included inthe framework with our strategy. The tragus was recon-structed by an anteriorly based transverse flap from theconchal area doubled on itself in the third stage.
An adequate, excellent-quality skin envelope was crit-ical for a successful ear reconstruction. Tissue expansioncould provide additional retroauricular non-hair-bearing
th right-side microtia. Left, lateral view of the expanded flaptoperation. Right, posterior view of the reconstructed ear with

Figure 6 Example pictures of case 3. A 19-year-old boy with right-side microtia. Left, lateral view of the final expanded flap(116 ml). Right, anterolateral view of the reconstructed ear 4 months postoperation.
1452 Z. Chen et al.
skin soft tissue for the coverage of the framework. Anumber of surgeons had reported experience of tissueexpansion in reconstruction of congenital microtia andtraumatic auricular defects.14e16 Zhuang5 had successfullyapplied tissue expansion in over 2000 microtia reconstruc-tions with excellent results and relatively low morbidity ofcomplications. He preferred to make a blunt C-shapedincision on the expanded flap and then elevating thepedicled flap anteriorly to drape the anterior part of theframework. To cover the posterior part of the framework,the retroauricular mastoid fascial flap and skin grafts wereneeded. Park13 also reported his excellent reconstructionresults using subfascial expansion. The framework wasinserted between the expanded skin flap and the expandedfascial flap. Skin grafts were also needed to cover theretroauricular wounds. In our experiences, the redundanthair-bearing skin at the superior helix was embarrassingsometimes when using the methods mentioned above.Meanwhile, the reconstructive auricle was seen to be thick
Figure 7 Example pictures of Case 4. An 18-year-old girl with leftMiddle, lateral view of the reconstructed ear three month after opeRight, two years after operation.
and clumsy for adult male patients whose skins were thick.We here developed an exceedingly expanded retroauricularflaps technique to provide sufficient coverage for the three-dimensional autogenous costal cartilage framework. Thereconstructive auricle showed good shape, accurate sizeand duplication of well-detailed structures. Conspicuousretroauricular scars and reduction of the cranioauricularsulcus caused by contraction of skin grafts could be effi-ciently avoided. The unelevated retroauricular mastoidfascia could be used to resolve complications such asexposure of the cartilage framework. The following werethe key points in our technique:
1. The non-hair-bearing skin tissue of the mastoid region islimited. If the expander is too large, excessive hair-bearing skin tissue will be expanded. According to theauricular contour and the shape of the mastoid skin, weprefer to choose a kidney-shaped expander with 50 mlvolume.
-side microtia. Left, frontal view of the expanded flap (115 ml).ration. Partial skin necrosis and framework exposure occurred.

Exceedingly expanded retroauricular flaps for microtia reconstruction 1453
2. Over-injection to the expander is usually conducted toascertain the coverage of the cartilage framework. Anexpansion volume of 100 or 120 ml can be achieved.After inflation was completed, the patient was asked tostay at home for nearly one month. This ‘static phase’can prevent contracture of the expanded flap effec-tively. Sufficient retroauricular non-hair-bearing skintissues are obtained by this exceeding expansion.
3. The expanded flap is divided into two flaps: the supe-rior two-thirds (flap A) and the inferior one-third (flapB) during stage 2. The anterior side and majority of theposterior side of the framework are enveloped by flapA. The remnant wound of the posterior mastoid regionis covered by rotation flap B. Sometimes, when flap A isinsufficient to cover the anteroinferior part of thecartilage framework, flap C is rotated 90� poster-oinferiorly to form the lobule.
4. Moulding of the cranioauricular sulcus is accomplishedby postauricular gauze dressing after stage 2. Pressuredressing should not be too tight to avoid partial skinnecrosis over the helix.
5. Negative-pressure catheter is usually removed on thepostoperative fifth day after the oedema starts tosettle. Negative-pressure drainage helps to evacuatethe fluid in the operative area. It also ensures thesuccess of tight co-aptation between the skin flap andthe framework.12 This is very important to reconstructthe detailed structures of the auricle.
Conclusions
Exceeding expansion can offer sufficient retroauricularnon-hair-bearing skin tissues for draping the autogenousauricular cartilage framework. Skin grafts and retro-auricular fascial flap are not needed. Patients are usuallysatisfied with their reconstructive auricles as regards thesize, location, projection, convolution, skin-colour match-ing, etc. Exceedingly expanded postauricular flaps area suitable envelope for the auricular cartilage framework.
Conflict of interest statement
None of the authors has a financial interest in any of theproducts, devices or drugs mentioned in this article.
References
1. Neumann CG. The expansion of an area of skin by progressivedistention of a subcutaneous balloon; use of the method forsecuring skin for subtotal reconstruction of the ear. PlastReconstr Surg 1957;19:124e30.
2. Brent B. The correction of microtia with autogenous cartilagegrafts: II. Atypical and complex deformities. Plast ReconstrSurg 1980;66:13e21.
3. Tanino R, Miyasaka M. Reconstruction of microtia using tissueexpander. Clin Plast Surg 1990;17:339e53.
4. Hata Y, Hosokawa K, Yano K, Matsuka K, Ito O. Correction ofcongenital microtia using the tissue expander. Plast ReconstrSurg 1989;84:741e51. 752e753.
5. Zhuang HX, Jiang HY, Pan B, et al. Ear reconstruction using softtissue expander in the treatment of congenital microtia.Zhonghua Zheng Xing Wai Ke Za Zhi 2006;22:286e9.
6. Tanzer RC. Total reconstruction of the external ear. PlastReconstr Surg Transplant Bull 1959;23:1e15.
7. Brent B. Auricular repair with autogenous rib cartilage grafts:two decades of experience with 600 cases. Plast Reconstr Surg1992;90:355e74. 375e376.
8. Kawanabe Y, Nagata S. A new method of costal cartilageharvest for total auricular reconstruction: part I. Avoidanceand prevention of intraoperative and postoperative complica-tions and problems. Plast Reconstr Surg 2006;117:2011e8.
9. Park C. Modification of two-flap method and frameworkconstruction for reconstruction of atypical congenital auriculardeformities. Plast Reconstr Surg 1997;99:1846e57.
10. Dashan Y, Haiyue J, Qinghua Y, et al. Technical innovations inear reconstruction using a skin expander with autogenouscartilage grafts. J Plast Reconstr Aesthet Surg 2008;61(Suppl.1):S59e69.
11. Zhang Q, Quan Y, Su Y, et al. Expanded retroauricular skin andfascial flap in congenital microtia reconstruction. Ann PlastSurg 2010;64:428e34.
12. Zhang Q, Zhang R, Xu F, Jin P, Cao Y. Auricular reconstructionfor microtia: personal 6-year experience based on 350 microtiaear reconstructions in China. Plast Reconstr Surg 2009;123:849e58.
13. Firmin F. State-of-the-art autogenous ear reconstruction incases of microtia. Adv Otorhinolaryngol 2010;68:25e52.
14. Park C. Subfascial expansion and expanded two-flap methodfor microtia reconstruction. Plast Reconstr Surg 2000;106:1473e87.
15. Hata Y, Umeda T. Reconstruction of congenital microtia byusing a tissue expander. J Med Dent Sci 2000;47:105e16.
16. Park C, Mun HY. Use of an expanded temporoparietal fascialflap technique for total auricular reconstruction. PlastReconstr Surg 2006;118:374e82.




![HEAR MAPS a New Classification for Congenital Microtia ... · (Hearing, Ear [microtia], Atresia grade, Remnant earlobe, Mandible development, Asymmetry of soft tissue, Paralysis](https://img.dokumen.tips/doc/110x75/60e4c2c1d26f8d5c325501dd/hear-maps-a-new-classiication-for-congenital-microtia-hearing-ear-microtia.jpg)
























