Embed Size (px)
Citation preview
Educational Partner
Accredited Provider
This activity is supported by an educational grant from
Novartis Pharmaceuticals Corporation.
Wednesday, April 8, 20152:00 pm – 3:15 pm
Anaheim, California
Evolving Issues and New Treatment
Approaches to Psoriasis: What the PCP Needs to Know
Session 5
Session 5: Evolving Issues and New Treatment Approaches to Psoriasis: What the PCP Needs to Know Learning Objectives
1. Incorporate therapeutic strategies that manage the systemic manifestations and comorbidities associated with psoriasis
2. Assess the risk-benefit profiles of conventional and emerging treatments for psoriasis to assist in therapeutic decision making
3. Recognize the physiological and psychological impacts of psoriasis, counsel patients accordingly, and incorporate care coordination and active patient engagement to improve outcomes in patients with psoriasis
Faculty Sylvia Hsu, MD Professor of Dermatology Baylor College of Medicine Chief of Dermatology Ben Taub General Hospital Houston, TX
Dr Sylvia Hsu graduated cum laude from Rice University in 1985 and Baylor College of Medicine in 1989. She did her internship at the University of Pennsylvania and her dermatology residency at Jefferson Medical College. After her training, she stayed at Jefferson as an assistant professor of dermatology. Dr Hsu moved back to Houston in 1997 to be on faculty in the department of dermatology at Baylor College of Medicine. Dr Hsu is professor of dermatology and chief of dermatology at Ben Taub General Hospital. She has a special interest in autoimmune bullous diseases, psoriasis, and acne. Dr Hsu was president of the Houston Dermatological Society in 2006. She was a member of the editorial board for the Journal of the Academy of Dermatology and the Medical Board of the National Psoriasis Foundation. She is also a member of the advisory board for Dermatology World.
Paul S. Yamauchi, MD, PhD Clinical Assistant Professor Division of Dermatology David Geffen School of Medicine at UCLA Adjunct Associate Professor John Wayne Cancer Institute Medical Director Dermatology Institute and Skin Care Center Santa Monica, CA
Dr Paul Yamauchi practices at the Dermatology Institute and Skin Care Center and is on staff at St. John’s Hospital, Santa Monica and the Ronald Reagan Hospital at the UCLA Medical Center. He is a clinical assistant professor of medicine at the David Geffen School of Medicine at UCLA and adjunct associate professor at the John Wayne Cancer Institute. Dr Yamauchi serves as a principle investigator in several studies of psoriasis, skin cancer, rejuvenation, rosacea, eczema, and acne. He is a key opinion leader in psoriasis and speaks extensively on new advances in the treatment of psoriasis and other dermatologic conditions. He has written several articles on the use of botulinum toxins and fillers for rejuvenation and other indications as well as advances in laser treatment. Dr Yamauchi serves on the editorial board of the Scientific World Journal and has authored numerous publications. He has published extensively on new advances in the treatment of psoriasis as well as on topics of acne, eczema, skin manifestations associated with rheumatologic conditions, and hyperhidrosis.

Session 5
Planning Committee and Faculty Financial Disclosure Statements The planning committee reported the following: Alan Menter, MD: Advisory Board for AbbVie, Allergan, Amgen, Boehringer Ingelheim, Genentech, Janssen Biotech, Inc., LEO Pharma and Pfizer, Consultant for AbbVie, Allergan, Amgen, Convoy Therapeutics, Inc., Eli-Lilly, Janssen Biotech, Inc., LEO Pharma, Novartis, Pfizer, Syntrix, Wyeth and XenoPort, Investigator for AbbVie, Allergan, Amgen, ApoPharma, Boehringer Ingelheim, Celgene, Convoy Therapeutics, Eli-Lilly, Genentech, Janssen Biotech, Inc., LEO Pharma, Merck, Novartis, Pfizer, Symbio/Maruho, Syntrix and Wyeth and Speaker for AbbVie, Amgen, Janssen Biotech, Inc., LEO Pharma and Wyeth. The presenting faculty reported the following: Dr Hsu: No relevant financial relationships to disclose. Dr Yamauchi: Consultant for AbbVie, Amgen, Baxter, Janssen-Ortho, Inc., Novartis and Pfizer, Inc., Speaker for AbbVie, Amgen, Galderma USA, Janssen-Ortho, Inc., Leo Pharma, Inc., Novartis Pharmaceuticals Corporation, Investigator for Amgen, Celgene Corporation, Galderma USA, Janssen-Ortho, Inc., Leo Pharma, Inc., Lilly ICOS, LLC, Pfizer, Inc. and Advisory Board for Lilly ICOS, LLC. Education Partner Financial Disclosure Statement The content collaborators at Vindico Medical Education no relevant financial relationships to disclose. Suggested Reading List Armstrong AW, Schupp C, Bebo B. Psoriasis comorbidities: results from the National Psoriasis Foundation surveys 2003 to 2011. Dermatology. 2012;225(2):121-126. Armstrong AW, Robertson AD, Wu J, et al. Undertreatment, treatment trends, and treatment dissatisfaction among patients with psoriasis and psoriatic arthritis in the United States: findings from the National Psoriasis Foundation surveys, 2003-2011. JAMA Dermatol. 2013;149(10):1180-1185. Hsu S, Papp KA, Lebwohl MG, et al. Consensus guidelines for the management of plaque psoriasis. Arch Dermatol. 2012;148(1):95-102. Menter A, Gottlieb A, Feldman SR, et al. Guidelines of care for the management of psoriasis and psoriatic arthritis: Section 1. Overview of psoriasis and guidelines of care for the treatment of psoriasis with biologics. J Am Acad Dermatol. 2008;58(5):826- 850. A, Korman NJ, Elmets CA, et al. Guidelines of care for the management of psoriasis and psoriatic arthritis: section 6. Guidelines of care for the treatment of psoriasis and psoriatic arthritis: case-based presentations and evidence-based conclusions. J Am Acad Dermatol. 2011;65(1):137-174. Villaseñor-Park J, Wheeler D, Grandinetti L. Psoriasis: evolving treatment for a complex disease. Cleve Clin J Med. 2012;79(6):413-423. Rustin MH. Long-term safety of biologics in the treatment of moderate-to-severe plaque psoriasis: review of current data. Br J Dermatol. 2012;167(Suppl 3):3-11. Chan SA, Hussain F, Lawson LG, Ormerod AD. Factors affecting adherence to treatment of psoriasis: comparing biologic therapy to other modalities. J Dermatolog Treat. 2013;24(1):64-69. Bewley A, Page B. Maximizing patient adherence for optimal outcomes in psoriasis. J Eur Dermatol Venerol. 2011;25(Suppl 4):9-14.
2 – 3:15pm
Evolving Issues and New
Treatment Approaches to Psoriasis: What the PCP
Needs to Know
SPEAKERS
Paul S. Yamauchi, MD, PhD
Sylvia Hsu, MD
Presenter Disclosure Information
►Sylvia Hsu, MD: No relevant financial relationships to disclose.
►Paul S. Yamauchi, MD, PhD: Consultant for AbbVie, Amgen, Baxter,
Janssen-Ortho, Inc., Novartis and Pfizer, Inc., Speaker for AbbVie, Amgen, Galderma USA, Janssen-Ortho, Inc., Leo Pharma, Inc.,
Novartis Pharmaceuticals Corporation, Investigator for Amgen,
Celgene Corporation, Galderma USA, Janssen-Ortho, Inc., Leo Pharma, Inc., Lilly ICOS, LLC, Pfizer, Inc. and Advisory Board for
Lilly ICOS, LLC.
The following relationships exist related to this presentation:
Off-Label/Investigational Discussion
► In accordance with pmiCME policy, faculty have been asked to
disclose discussion of unlabeled or unapproved use(s) of drugs or devices during the course of their presentations.
Management of Psoriasis
Patients: What the PCP Needs to Know
Objectives
• Improve management of systemic manifestations of psoriasis and its comorbidities
• Learn about the risks and benefits of conventional and emerging psoriasis treatments
• Recognize the psychological impacts of psoriasis and incorporate care coordination to improve patient outcomes
Defining the Need for a Systemic Treatment for a Systemic Disease
Sylvia Hsu, MD
Professor of Dermatology
Baylor College of Medicine
Chief of Dermatology
Ben Taub General Hospital
Houston, TX
Psoriasis (sō-rī’ǎ-sĭs)
[Gr., an itching]
A common, genetically-determined
dermatosis most commonly consisting of discrete erythematous plaques with a
characteristic silvery scale.
An inflammatory arthritis is associated with
psoriasis in approximately 30% of patients.
Taber's Cyclopedic Medical Dictionary. Philadelphia: F.A. Davis Co.; 2013.
Epidemiology
• Age of onset– Bimodal – 1st peak – age 15-20 years, 2nd peak
- age 55-60 years– Onset earlier than 15 years of age may indicate
more severe disease
• Family history– Up to 33% patients report family history– HLA-Cw6, B13, B17, Bw57
Psoriasis: Clinical Features
• Chronic immune-mediated disease• Psoriatic plaques
– Erythema (redness)
– Induration (thickness)– Desquamation (scaling)
• Affected areas of the body– Symmetric
– Extensors (elbows, knees)– Scalp
– Trunk
• No permanent cure
Psoriasis: Differential Diagnosis
• Plaque psoriasis1
• Well-demarcated, erythematous plaques with thick, silvery scale
Photo courtesy of Sylvia Hsu, M.D.1. Chen, FJ. Can Fam Physician. 2011 Aug; 57(8): 903–904.
• Eczema2
• Pruritic dry skin with poorly defined erythematous patches, papules, and plaques, with fine
scale.1
1. Chen, FJ. Can Fam Physician. 2011 Aug; 57(8): 903–904. 2. Wolff K, Johnson R, Saavedra AP. Section 2. Eczema/Dermatitis. In: Wolff K, Johnson R, Saavedra AP. eds.
Fitzpatrick's Color Atlas and Synopsis of Clinical Dermatology, 7e. New York, NY: McGraw-Hill; 2013. Photo courtesy of Sylvia Hsu, M.D.
Psoriasis: Differential Diagnosis
• Tinea Corporis
• Flat, scaly patch with a raised, palpable border. Enlarges by advancing outer border, leaving a
clear center1
Photo courtesy of Sylvia Hsu, M.D.1. Azadi K, Burns B. Chapter 48. Dermatologic Emergencies. In: Stone C, Humphries RL. eds. CURRENT Diagnosis & Treatment Emergency Medicine, 7e. New York, NY: McGraw-Hill; 2011.
Psoriasis: Differential Diagnosis
• Contact Dermatitis1
• Erythematous, edematous plaques with linear or geometric patterns
Photo courtesy of Sylvia Hsu, M.D.1. Urman CO, Loo DS. Common Skin Disorders. In: Williams BA, Chang A, Ahalt C, Chen H, Conant R, Landefeld C, Ritchie C,
Yukawa M. eds. Current Diagnosis & Treatment: Geriatrics, Second Edition. New York, NY: McGraw-Hill; 2014.
Psoriasis: Differential Diagnosis

• Mycosis fungoides1
• Scale is not thick
• More common on trunk and
proximal extremities
Photo courtesy of Sylvia Hsu, M.D1. Usatine RP, Smith MA, Chumley HS, Mayeaux EJ, Jr.. Chapter 152. Psoriasis. In: Usatine RP, Smith MA, Chumley HS, Mayeaux EJ, Jr.. eds. The Color Atlas of Family Medicine, 2e. New York, NY: McGraw-Hill; 2013.
Psoriasis: Differential Diagnosis
• Drug Eruptions1
• Many presentations, but may be exanthematous, urticarial, blistering, or pustular.
Photo courtesy of Sylvia Hsu, M.D.1. Shear NH, Knowles SR. Chapter 41. Cutaneous Reactions to Drugs. In: Goldsmith LA, Katz SI,
Gilchrest BA, Paller AS, Leffell DJ, Wolff K. eds. Fitzpatrick's Dermatology in General Medicine, 8e. New York, NY: McGraw-Hill; 2012
Psoriasis: Differential Diagnosis
Types of Psoriasis
• Plaque Psoriasis: Comprises 80% of all psoriasis cases.
• DDx: eczema, tinea corporis, mycosis fungoides
Photo courtesy of Sylvia Hsu, M.D.
Types of Psoriasis
• Guttate Psoriasis: Small droplet lesions. Frequently first
manifestation of psoriasis, can develop into plaque psoriasis. Often precipitated by streptococcus throat
infection.
• DDx: pityriasis rosea, secondary
syphilis, morbilliform drug eruption
Photo courtesy of Sylvia Hsu, M.D.
Types of Psoriasis
• Scalp Psoriasis:
• DDx: seborrheic dermatitis, allergic contact dermatitis, dermatomyositis
Photo courtesy of Sylvia Hsu, M.D.
Types of Psoriasis
• Palmoplantar Psoriasis: Scaly plaques on palms and soles.
• DDx: dyshidrosis, keratoderma
Photo courtesy of Sylvia Hsu, M.D.
Types of Psoriasis
• Pustular Psoriasis: Sterile pustules. Can be precipitated by withdrawal of
systemic steroids.
Photo courtesy of Sylvia Hsu, M.D.
Types of Psoriasis
• Erythrodermic Psoriasis: Generalized erythema with scale. Can
be precipitated by withdrawal of systemic steroids.
• DDx: pityriasis rubra pilaris, mycosis fungoides, drug eruption
Photo courtesy of Sylvia Hsu, M.D.
Types of Psoriasis
• Inverse Psoriasis: Psoriasis in the flexural (intertriginous) areas
• DDx: Candidal intertrigo, dermatophytosis, erythrasma
Photo courtesy of Sylvia Hsu, M.D.
Psoriasis-associated Comorbidities
Associated Comorbidities
1. Psoriatic arthritis1
2. Obesity/metabolic syndrome1,2
3. Cardiovascular disease1
4. Cancer/lymphoma1,3
5. Psychiatric diseases1
6. Increased mortality1
All statistically validated
1. Reich K. JEADV. 2012;26(Suppl. 2):3-11.2. Carrascosa JM, et al. Actas Dermosifiliogr. 2014;105(1):31-44.3. Gelfand JM, et al. J Invest Dermatol. 2006;126:2194-2201.
Associated Comorbidities
7. Personal behaviors, e.g. smoking1
8. Autoimmune diseases2
9. Nonalcoholic steatohepatitis (NASH)3
10. COPD4
11. Sleep apnea5
All statistically validated
1. Asokan N, et al. Indian J Dermatol. 2014 May-Jun; 59(3): 237–240.2. Wu JJ, et al. J Am Acad Dermatol. 2012;67:924-930, 1076-1083.3. Roberts KK, et al. Aliment Pharmacol Ther. 2014 Dec 18. doi: 10.1111/apt.13042. [Epub ahead of print].4. Chiang YY, Lin HW. J Eur Acad Dermatol Venereol. 2012 Jan;26(1):59-65.5. Karaca S, et al. Sleep Breath. 2013 Mar;17(1):275-80.

Risk of Cardiovascular Disease in
Patients with More Severe Psoriasis
1. Increased risk of MI, stroke,
cardiovascular death, diabetes, chronic kidney disease
2. 5 years of life lost
3. 10-year risk of major CV event attributable to psoriasis = 6%
4. Risk of cardiovascular disease
in patients with severe psoriasis similar to risk
conferred by diabetes mellitus
Outcome Adj. RR Mild
Adj. RR Severe
MI1 1.05 1.5
Stroke2 1.06 1.4
CV Death3 Not done 1.6
MACE4 Not done 1.5
Diabetes5 1.11 1.5
CKD6 0.99 (NS) 1.9
1. Gelfand JM, et al. JAMA. 2006;296:1735.2. Gelfand JM, et al. J Invest Derm. 2009;129:2411.3. Mehta NN, et al. Eur Heart J. 2010;31:1000.4. Mehta NN, et al. Am J Med. 2011;124:775.e1-6.5. Azfar R, et al. Arch Derm. 2012;148:995-1000.6. Wan J, et al. BMJ. 2013;347;f5691.
Clinical Significance:
MI=Myocardial Infarction. CV=Cardiovascular. MACE=Major Adverse Cardiac Events. CKD=Chronic Kidney Disease.
Comorbidities:
Cardiovascular Disease
• Risk factor evaluation and interventions1,2:
1. Federman DG, et al. Br J Dermatol. 2009;160(1):1-7.2. Kremers HM, et al. J Am Acad Dermatol. 2007;57:347-354.
• Obesity • Smoking
• Hypertension • Dyslipidemia
• Diabetes mellitus • Cardiovascular Disease
Psoriasis: An Opportunity to Identify Cardiovascular Risk1,2
Comorbidities:
Psoriatic Arthritis (PsA)
• An inflammatory arthritis in approx 30% of patients with psoriasis1
• Temporal relationship between psoriasis and PsA
– 70% have psoriasis prior to onset of PsA2,3
– 20% have PsA before psoriasis2,3
– 10%-15% report simultaneous onset 2,3
• Severity of psoriasis is not predictive of severity of PsA3
1. Gladman D, et al. Ann Rheum Dis. 2005; 64 (Suppl II): ii14-7. 2. Leung Y, et al. J Postgrad Med. 2007; 53: 63-71. 3. Cohen M, et al. J Rheumatol. 1999; 26: 1752-6.
Psoriasis: Unmet Needs and Undertreatment
Patient Satisfaction
with Treatment
• National Psoriasis Foundation study1
– Physician unwillingness to prescribe systemic therapy was the 3rd most common reason why patients were on topical monotherapy (1st – fewer adverse effects than other options, 2nd – psoriasis not severe enough)
• Netherlands study (N=1293)2
– Patients receiving biologic therapy were most satisfied and those receiving topical treatment were least satisfied of all groups
1. Armstrong AW, et al. JAMA Dermatol. 2013;149(10):1180-1185.2. van Cranenburgh OD, et al. Br J Dermatol. 2013;169(2):398-405.
Case Presentation
Case
• A 45-year-old woman
• PMH: Type 2 diabetes mellitus, asthma
• Treatment History:
– Recently completed a 7-day course of oral steroids for an acute
asthma exacerbation.
– She is taking metformin for her diabetes.
• HPI: She presents to your office with a 4-day history of erythematous
patches, plaques, and multiple pustules over most of her body surface area.
• Vitals/Labs: Temperature: 99.5oF. BP: 124/84 mm HG bilaterally. CBC:
normal.
Psoriasis is Not Simply a Skin
Disease
Psoriasis is not just a cosmetic disfigurement or skin disease.
Psoriasis significantly impacts QOL comparable to, if not more,
than most other systemic diseases.
Summary: Psoriasis Treatment,
Inflammation, and Comorbidities
Mercy KM, et al. JAMA. 2014;312(24):2676-2677.MTX: Methotrexate, CV: Cardiovascular, TNF: Tumor Necrosis Factor, CVD: Cardiovascular Disease, QOL: Quality of Life
• With inflammation as a common link, systemic treatment of psoriasis may also mitigate
comorbidities
– anti-TNF therapy may decrease CV morbidity and mortality
• Understanding risks of psoriasis � better treatment decisions � improved QOL and outcomes
Examining the Risk-Benefit Profiles of Current and Emerging Treatments
Paul S. Yamauchi, MD, PhD
Clinical Assistant Professor
Division of Dermatology
David Geffen School of Medicine at UCLA
Adjunct Associate Professor
John Wayne Cancer Institute
Medical Director
Dermatology Institute and Skin Care Center
Santa Monica, CA
Agenda
• Discuss:
– Safety concerns with conventional systemic agents
– Biologics and their place in management
– Novel oral systemic agents
– Development of biosimilars
Assessing Severity of Psoriasis
• Imagine 1 palm equal to 1% of your body surface area.
• Mild : 1-3%
• Moderate: 3-10%
• Severe: More than 10%
• Location also determines severity
• Scalp
• Hands and feet
• Groin and skin folds
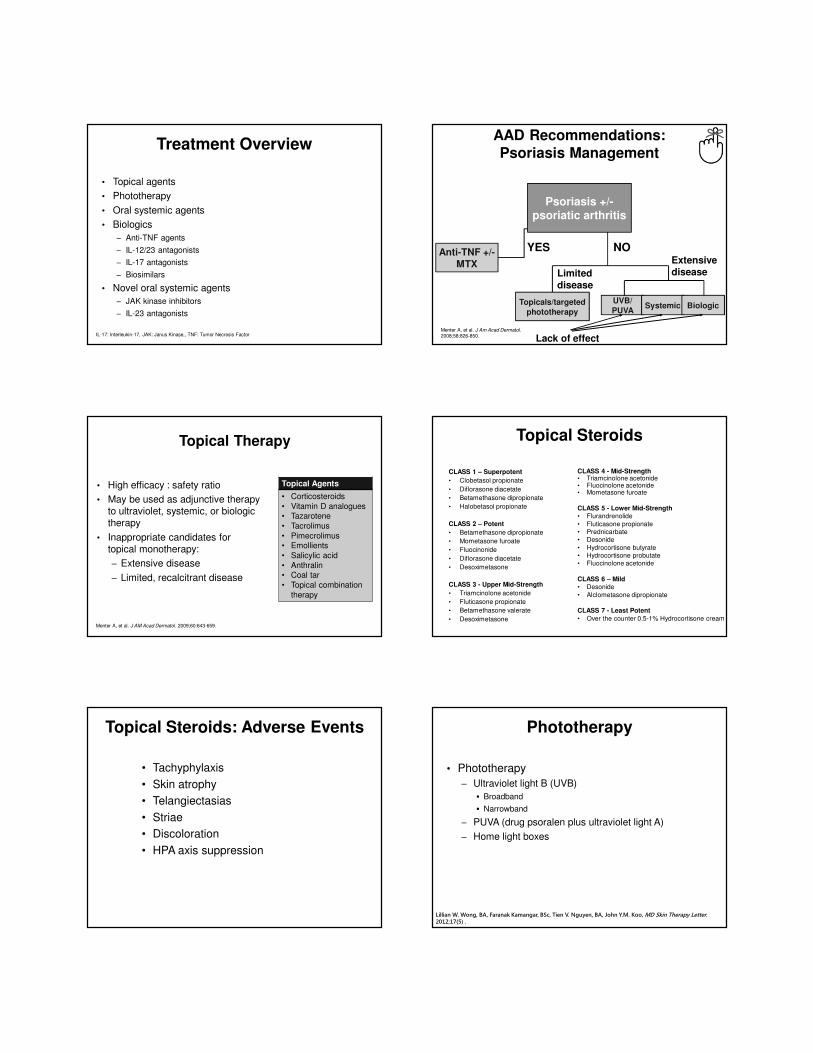
Treatment Overview
• Topical agents
• Phototherapy
• Oral systemic agents
• Biologics
– Anti-TNF agents
– IL-12/23 antagonists
– IL-17 antagonists
– Biosimilars
• Novel oral systemic agents
– JAK kinase inhibitors
– IL-23 antagonists
IL-17: Interleukin-17, JAK: Janus Kinase,, TNF: Tumor Necrosis Factor
AAD Recommendations:
Psoriasis Management
Anti-TNF +/-MTX
UVB/
PUVASystemic BiologicTopicals/targeted
phototherapy
YES NO
Limited disease
Extensive disease
Lack of effectMenter A, et al. J Am Acad Dermatol. 2008;58:826-850.
Psoriasis +/-psoriatic arthritis
Topical Therapy
• High efficacy : safety ratio
• May be used as adjunctive therapy to ultraviolet, systemic, or biologic therapy
• Inappropriate candidates for topical monotherapy:
– Extensive disease
– Limited, recalcitrant disease
Topical Agents
• Corticosteroids
• Vitamin D analogues• Tazarotene
• Tacrolimus
• Pimecrolimus• Emollients
• Salicylic acid
• Anthralin• Coal tar
• Topical combination
therapy
Menter A, et al. J AM Acad Dermatol. 2009;60:643-659.
Topical Steroids
CLASS 1 – Superpotent
• Clobetasol propionate
• Diflorasone diacetate
• Betamethasone dipropionate
• Halobetasol propionate
CLASS 2 – Potent
• Betamethasone dipropionate
• Mometasone furoate
• Fluocinonide
• Diflorasone diacetate
• Desoximetasone
CLASS 3 - Upper Mid-Strength
• Triamcinolone acetonide
• Fluticasone propionate
• Betamethasone valerate
• Desoximetasone
CLASS 4 - Mid-Strength• Triamcinolone acetonide• Fluocinolone acetonide• Mometasone furoate
CLASS 5 - Lower Mid-Strength• Flurandrenolide
• Fluticasone propionate• Prednicarbate• Desonide
• Hydrocortisone butyrate• Hydrocortisone probutate• Fluocinolone acetonide
CLASS 6 – Mild• Desonide
• Alclometasone dipropionate
CLASS 7 - Least Potent
• Over the counter 0.5-1% Hydrocortisone cream
Topical Steroids: Adverse Events
• Tachyphylaxis
• Skin atrophy
• Telangiectasias
• Striae
• Discoloration
• HPA axis suppression
Phototherapy
• Phototherapy
– Ultraviolet light B (UVB)
� Broadband
� Narrowband
– PUVA (drug psoralen plus ultraviolet light A)
– Home light boxes
Lillian W. Wong, BA, Faranak Kamangar, BSc, Tien V. Nguyen, BA, John Y.M. Koo, MD Skin Therapy Letter. 2012;17(5) .
Phototherapy
• Exposure to ultraviolet light
– Continuous, intermittent therapy
• Meaningful response in 60% to 70% of
patients
• Risks:
– Burning
– Skin cancer
– Premature aging
• Does not treat psoriatic arthritis
• Labor intensive and usually impractical →requires frequent visits to office (3 visits per week),
but can be self-administered at home by
appropriate patient
When to Initiate Systemic or
Biologic Therapy
Reasons for Systemic Treatment• Poor or no response to topicals, UVB, PUVA therapy
• Received maximum “safe” cumulative PUVA dose
• Psoriasis covers > 10% BSA
• More inflammatory forms of psoriasis
• Localized/recalcitrant disease
• Physical restrictions
• Negative impact on QOL
• Status of disease
– (PASI > 10, BSA > 10, DLQI > 10)
Menter A, et al. J Am Acad Dermatol. 2009;61:451-485.
BSA: Body Surface Area, DLQI: Dermatology Life Quality Index, PASI: Psoriasis Area and Severity Index, PUVA: Psoralen + Ultraviolet A, QOL: Quality of Life
Traditional Oral Systemic Therapy
Methotrexate
Cyclosporine
Acitretin
Methotrexate: Efficacy/Safety
• Most commonly prescribed
traditional systemic agent globally for psoriasis
– Dramatically effective, even in the most severe cases
• Can be used in combination
with all approved biologics for psoriasis, especially the anti-
TNFs
– Can be used to suppress anti-drug antibodies against
adalimumab and infliximab
• Pregnancy issues
• Clinical efficacy relative to
biologics
• Drug interactions
• Polymorphisms2
• Liver biopsies and amino-
terminal propeptide of type III collagen (PIIINP)
• Bone marrow
suppression
• Lifetime dose restriction
1. Menter A, et al. J Am Acad Dermatol. 2009;61:451-485.2. Warren RB, et al. Clin Exp Dermatol. 2008;33(5):551-554.
Efficacy1 Safety
Cyclosporine: Efficacy/Safety
1. Menter A, et al. J Am Acad Dermatol. 2009;61:451-485.2. Ellis CN, et al. N Engl J Med. 1991;324:277-284.3. Faerber L, et al. Am J Clin Dermatol. 2001;2:41-47.4. Wolverton SE. Comprehensive Dermatologic Drug Therapy. 2nd ed. Philadelphia, PA: WB Saunders; 2007.5. Ryan C, et al. J Am Acad Dermatol. 2010;63(6):949-972.
Efficacy Safety1,4-5
• One of the most effective
interventional therapies1
• Rapid response in 80-90% of patients2,3
• Induces rapid remission in
patients with severe flares1
• Can prevent rebound flares
in patients discontinuing
systemic steroids1
• Irreversible
nephrotoxicity/hypertension with continued usage
• Malignancy – rare
• Dyslipidemia and metabolic
issues
• Infections, including TB – rare
• Use limited to 1 year in the
U.S. due to nephrotoxicity
Acitretin: Efficacy/Safety
• Least effective as
monotherapy
• Often used with UVB or PUVA phototherapy
• Acitretin is may be
effective in patients with
palm-sole psoriasis
• Not immunosuppressive
and can be used in combination with
biologics
• Teratogenicity
– Limits use
• High doses associated with mucocutaneous effects, including hair loss
• Hyperlipidemia
Menter A, et al. J Am Acad Dermatol. 2009;61:451-485.
PUVA: Psoralen + Ultraviolet A, UVB: Ultraviolet B
Efficacy Safety

Conventional Agents:
End-Organ Toxicity
• End-organ toxicity is a major concern common to conventional systemic therapy
• Toxicities of individual agents can be decreased by rotating from one conventional agent to
another
• Biologics have decreased the incidence of end-
organ toxicity
– Use of biologics has decreased the need for rotational therapy
Menter A, et al. J Am Acad Dermatol. 2009;61:451-485.
Newer Oral Agent:
Apremilast: Efficacy/Safety
• Inhibits PDE4
(phosphodiesterase-4) and increases cAMP
levels intracellularly
• Indirectly
immunomodulatesproduction of
inflammatory cytokines
• Approved for psoriasis
and psoriatic arthritis
• No lab monitoring required
• Diarrhea
• Headache
• Weight loss
• Depression/suicide
Efficacy Safety
Apremilast [package insert]. Summit, NJ: Celgene; 2014.
Current and Emerging Biologics
Drug Class Agent Indication (Psoriasis, PsA)
Anti-TNF Etanercept Psoriasis, PsA
Infliximab Psoriasis, PsA
Adalimumab Psoriasis, PsA
IL-12/23 antagonist Ustekinumab Psoriasis, PsA
IL-17 antagonist Secukinumab Psoriasis, in Phase III for PsA
Brodalumab In Phase III for Psoriasis and PsA
Ixekizumab In Phase III for Psoriasis and PsA
TNF: Tumor Necrosis Factor, IL: Interleukin, PsA: Psoriatic Arthritis
Trends in Biologic Use in
Psoriasis in the United States
“Step therapy”– Phototherapy
– Then oral systemics
– Then biologics
Phototherapy or oral systemics or biologics
Both AAD and NPF support the use of biologic as a first-line agent for moderate to severe patients
Menter A, et al. J Am Acad Dermatol. 2008;58:826-850.Hsu S, et al. Arch Dermatol. 2012;148(1):95-102.
Biologic Agents: Safety Profile
Considerations in Psoriasis
• Key considerations
– Infections: Bacterial, viral, mycobacterial
– Malignancy (Solid tumors and non-melanoma skin cancer)
• Other considerations
– Infusion/injection-site reactions
– Contraindications/cautions� Tuberculosis
� Hepatitis B (TNF inhibitors)
� Demyelinating diseases (TNF inhibitors)
� Congestive heart failure (TNF inhibitors)
Wolverton SE. Comprehensive Dermatologic Drug Therapy. 3rd ed. Philadelphia, PA: WB Saunders; 2012.Menter A, et al. J Am Acad Dermatol. 2008;58:826-850.
When a Patient is on a
Biologic Agent
• Avoid administering live vaccines1
– Intranasal flu vaccine, herpes zoster, varicella,
measles/mumps/rubella, oral polio, rotavirus, yellow fever,
rabies, BCG, typhoid
• Inactivated or subunit vaccines are generally considered safe but efficacy may be compromised1
• Monitor for signs or symptoms of infection
– Opportunistic fungal infections
– Reactivation of latent TB, underlying hepatitis B/C, shingles
• What if a patient becomes pregnant?
• Surgery
1. Hsu S, et al. Arch Dermatol. 2012;148(1):95-102.BCG: Bacillus Calmette–Guérin, HBV: Hepatitis B Virus, HCV: Hepatitis C Virus, HZV: Herpes Zoster Virus, TB: Tuberculosis
Prior to Initiating an Anti-
TNF-α Biologic Agent
• Ensure patient is up-to-date on all vaccinations
• Verify negative TB test
• Assess underlying cancer risk
• Verify absence of demyelinating disease
• Verify absence of current infection
• Screen for Hepatitis B and C viral infections
• Use caution in patients with active CHF
TB: Tuberculosis, CHF: Congestive Heart Failure
Current and Emerging Oral
Therapies
Drug Class Agent Indication (Psoriasis, PsA)
JAK inhibitor Tofacitinib Phase III: Psoriasis/PsA
ASP015K Phase IIb: Psoriasis
LY3009104 Phase IIb: Psoriasis
PsA: Psoriatic Arthritis
Biosimilars
• Not to be interchanged with the term “generics”
• They are not exact protein copies of the originators (the branded biologic)
• Although the mechanism of action is similar to the originator, they are manufactured by a different cell line.
• TNF inhibitors being considered first
Case Presentation
Case: Overview
• 51 year-old male
• Height: 5 ft 11in, Weight: 245 lbs
• BMI = 33.2 kg/m2
• History of psoriasis since age 22 yrs
• Occupation – college professor
• Family history of psoriasis
– Father
• Family history of cancer
– Leukemia: Mother
– Colon cancer: Father
• Social history
– Social drinker (1 glass wine per day with dinner)
– Smoking - 1 pack per day
Case: Overview
• Past medical history
– Hypertension
– Hyperlipidemia
• Medications
– Atorvastatin
– Hydrochlorothiazide
• Prior therapies for psoriasis
– Topical steroids
– Phototherapy
• Physical exam
– Psoriatic plaques on scalp, elbows, arms, knees, legs
– 40% body surface area
– No evidence of dactylitis,
– No tender or swollen joints
– No signs of enthesitis
Case: Laboratory Values
• Quantiferon Gold: Negative
• CBC – WNL
• LFTs – 1.5x higher than upper limit of normal
• Hepatitis B panel – Negative
• Hepatitis C panel – Negative
• Total cholesterol – 202 mg/dL
• Triglycerides – 175 mg/dL
Summary
• Conventional systemic agents can be effective in managing psoriasis and inducing remission, but their use is limited by teratogenicity and toxicity.
• Psoriasis treatment strategies are moving away from step therapy and more towards first-line use of biologics in patients with moderate to severe disease.
• Patients on biologics are immunosuppressed which must be taken into consideration when administering vaccines and monitoring for infections and possible malignancy
Incorporating Shared Decision Making With PatientsPaul S. Yamauchi, MD, PhD
Clinical Assistant Professor
Division of Dermatology
David Geffen School of Medicine at UCLA
Adjunct Associate Professor
John Wayne Cancer Institute
Medical Director
Dermatology Institute and Skin Care Center
Santa Monica, CA
Agenda
• Review the psychosocial impacts of
psoriasis
• Identify adherence-improving methods
• Discuss the importance of the coordination of care and referrals
Psoriasis and Quality of Life (QOL)
• Nearly half of patients with psoriasis prefer a different serious medical condition (e.g. hypertension, asthma)
• 83% need to hide their psoriasis
• 74% with lowered self confidence
• 46% chronically depressed
• 83% avoid sports activities (swimming)
• 35% inhibited in sexual relationships
• 23% affected choice of career
• 10% between the ages of 18-34 years contemplated suicide
Weiss, S et al, Dermatol Nurs 2003;47:512.
What Role Do Quality-of-Life Issues Play in the Decision-
making Process before Initiating a Plan of Treatment?
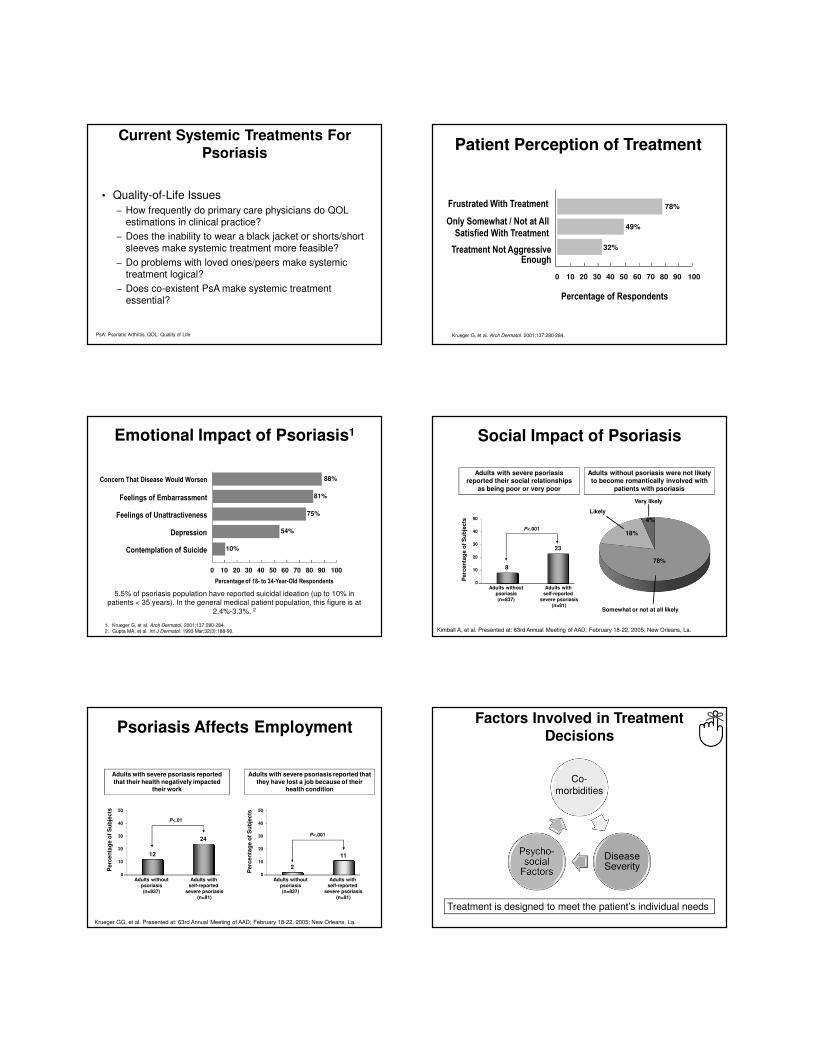
Current Systemic Treatments For
Psoriasis
• Quality-of-Life Issues
– How frequently do primary care physicians do QOL estimations in clinical practice?
– Does the inability to wear a black jacket or shorts/short sleeves make systemic treatment more feasible?
– Do problems with loved ones/peers make systemic treatment logical?
– Does co-existent PsA make systemic treatment essential?
PsA: Psoriatic Arthritis, QOL: Quality of Life
Patient Perception of Treatment
Krueger G, et al. Arch Dermatol. 2001;137:280-284.
78%
49%
32%
0 10 20 30 40 50 60 70 80 90 100
Percentage of Respondents
Treatment Not Aggressive Enough
Frustrated With Treatment
Only Somewhat / Not at All
Satisfied With Treatment
1. Krueger G, et al. Arch Dermatol. 2001;137:280-284.2. Gupta MA, et al. Int J Dermatol. 1993 Mar;32(3):188-90.
Emotional Impact of Psoriasis1
88%Concern That Disease Would Worsen
81%Feelings of Embarrassment
75%Feelings of Unattractiveness
54%Depression
10%Contemplation of Suicide
0 10 20 30 40 50 60 70 80 90 100
Percentage of 18- to 34-Year-Old Respondents
5.5% of psoriasis population have reported suicidal ideation (up to 10% in patients < 35 years). In the general medical patient population, this figure is at
2.4%-3.3%. 2
Social Impact of Psoriasis
78%
18%
4%
Somewhat or not at all likely
Likely
Very likely
Adults without psoriasis were not likely to become romantically involved with
patients with psoriasis
Adults with severe psoriasis reported their social relationships
as being poor or very poor
8
23
0
10
20
30
40
50
Adults withoutpsoriasis(n=837)
Adults with self-reported
severe psoriasis(n=81)
Perc
en
tag
e o
f S
ub
jects
Kimball A, et al. Presented at: 63rd Annual Meeting of AAD; February 18-22, 2005; New Orleans, La.
P<.001
Adults with severe psoriasis reported that
they have lost a job because of their health condition
Adults with severe psoriasis reported
that their health negatively impacted their work
12
24
0
10
20
30
40
50
Adults withoutpsoriasis(n=837)
Adults with self-reported
severe psoriasis(n=81)
Perc
en
tag
e o
f S
ub
jects
Krueger GG, et al. Presented at: 63rd Annual Meeting of AAD; February 18-22, 2005; New Orleans, La.
2
11
0
10
20
30
40
50
Adults withoutpsoriasis(n=837)
Adults with self-reported
severe psoriasis(n=81)
Perc
en
tag
e o
f S
ub
jects
P<.01
P<.001
Psoriasis Affects EmploymentFactors Involved in Treatment
Decisions
Treatment is designed to meet the patient’s individual needs
Disease Severity
Co-morbidities

Summary: Psoriasis Challenges
and Quality-of-Life Issues
• We have many challenges!
• We must consider QOL issues at each visit.
• We owe it to our psoriasis patients and our
colleagues to use systemic therapies appropriately!
• We must consider the full list of comorbidities at each visit, including PsA evaluation.
Adherence and Adherence Improving Methods
The Problem of Non-adherence
• Maintenance therapy is required for long-term treatment success1
• Discontinuation rates for conventional systemic and phototherapy range from 15%-25%1
• First-year attrition rates for biologics range from 10%-15%1
• Patients most likely to be non-adherent tend to be: Men, unmarried patients, those who are unemployed, patients who drink or smoke, and patients with more severe disease2
1. Yeung H, et al. J Am Acad Dermatol. 2013;68(1):64-72.2. Bewley A, Page B. J Eur Acad Dermatol Venereol. 2011;25(Supp. 4):9-14.
The Most Common Reasons Cited
for Discontinuation
• Loss of efficacy
• Lack of initial response
• Adverse events
• Inconvenient administration
Yeung H, et al. J Am Acad Dermatol. 2013;68(1):64-72.
Practical Strategies to Improve
Adherence
• Schedule a follow-up visit shortly after treatment initiation
• Ask patients about preferred vehicle for topical therapy– Gels and creams vs ointments
• Build patient trust by:– Being empathetic, listening to the patient, physically examining
their skin, practicing good communication skills
• Clarify treatment goals in the context of patient expectations
• Provide cues to medication administration (e.g., setting a phone reminder, environmental cues, behavioral cues)
Bewley A, Page B. J Eur Acad Dermatol Venereol. 2011;25(Supp. 4):9-14.
Practical Strategies to Improve
Adherence
• Educate patients about psoriasis as a disease state
• Provide information about diagnosis, drug dosing, and treatment duration
• Provide an in-office demonstration showing how to properly apply/administer the prescribed medication
– Assure patient understanding by asking them to repeat back
treatment instructions
• Provide information about alternative treatment options
Bewley A, Page B. J Eur Acad Dermatol Venereol. 2011;25(Supp. 4):9-14.
Coordination of Care
• Involve other healthcare providers in the education, follow-up, and long-term care of patients1
• Study was conducted on patients with psoriasis or eczema2
– Patients randomized to standard of care or receiving an
additional session with a dermatology specialist nurse immediately after their physician consultation
– At 6 weeks:
� Both groups showed similar improvement in QOL� Patients who saw the nurse:
♦ Had significantly more knowledge about treatment
duration*♦ Knew how to obtain a repeat prescription*
♦ Knew who to contact for support**
1. Bewley A, Page B. J Eur Acad Dermatol Venereol. 2011;25(Supp. 4):9-14.2. Gladwell C, et al. Br J Dermatol. 2002;147:513-517.
*P<0.01**P<0.001
When to Refer to a Dermatologist
• Defined treatment goals are not met
• Patient dissatisfaction with treatment
outcomes
• Discomfort with treating moderate to severe disease
• Psoriasis patients with multiple comorbidities
Case Presentation
Case: Palmoplantar Psoriasis
• 66-year-old male
• History of psoriasis since age 51 years
• Comorbidities:
– Depression
– Hyperlipidemia
• Physical Exam:
– Significant involvement of palms and soles
– 40% of both palmar and plantar aspects affected
– Face, scalp, genitalia, groin
– Significant impact on patient’s quality of life, i.e., pain when
walking and limitation of the use of his hands
Treatment
• Scalp and genital
area responded well to topical
agents:
- Corticosteroids
- Tacrolimus
• Palmoplantar areas were recalcitrant
to topicals and photochemotherapy. Examples of agents tried:
– Corticosteroids
– Vitamin D3
– Combination topical treatment, including occlusion
– Topical PUVA
• Acitretin was initiated at dose of 25 mg daily; moderate degree muco-
cutaneous side effects noted
• Acitretin dose reduced to 25 mg on alternate days
– Improvement maintained with reduction in cheilitis
Prior Therapies
Treatment Decision:
Summary
• Psoriasis is a systemic inflammatory disease often requiring systemic treatment
• Conventional systemic agents are limited by safety concerns such as teratogenicity and end-organ toxicity
• New oral and biologic agents are safe and effective treatment options
• Biologics may be used first-line in moderate-severe psoriasis
• Psychosocial concerns must be taken into account when determining treatment regimens
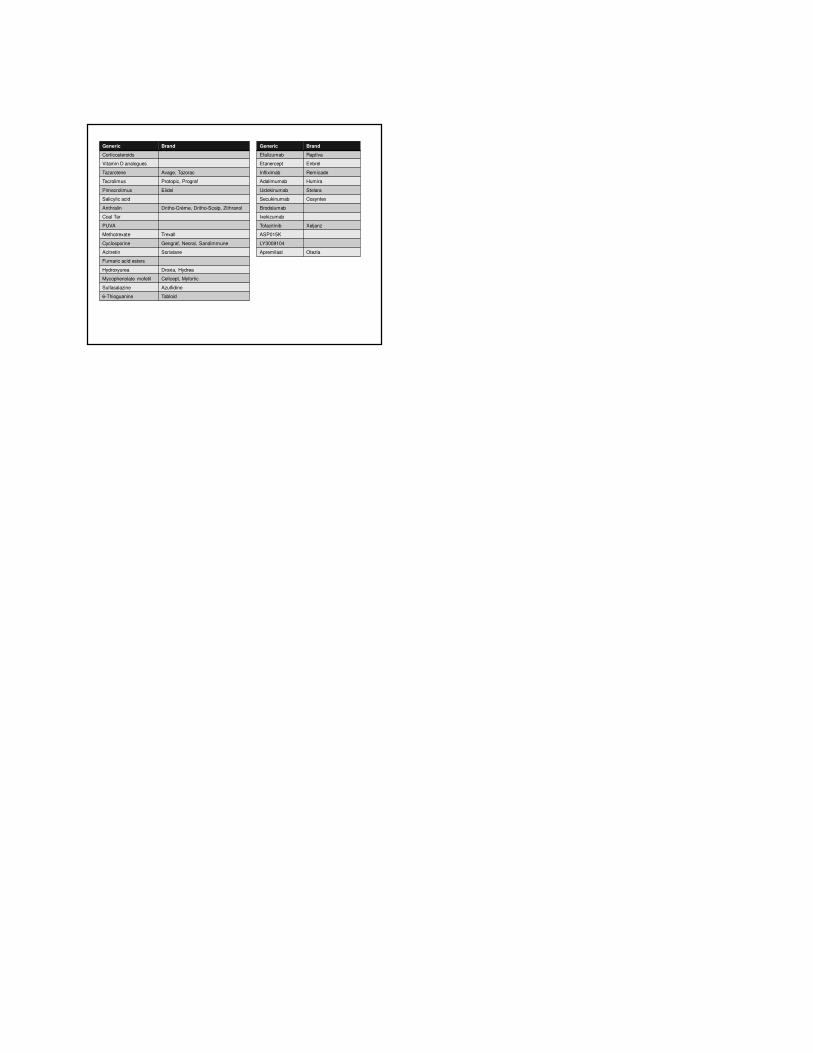
Generic Brand
Corticosteroids
Vitamin D analogues
Tazarotene Avage, Tazorac
Tacrolimus Protopic, Prograf
Pimecrolimus Elidel
Salicylic acid
Anthralin Dritho-Crème, Dritho-Scalp, Zithranol
Coal Tar
PUVA
Methotrexate Trexall
Cyclosporine Gengraf, Neoral, Sandimmune
Acitretin Soriatane
Fumaric acid esters
Hydroxyurea Droxia, Hydrea
Mycophenolate mofetil Cellcept, Myfortic
Sulfasalazine Azulfidine
6-Thioguanine Tabloid
Generic Brand
Efalizumab Raptiva
Etanercept Enbrel
Infliximab Remicade
Adalimumab Humira
Ustekinumab Stelara
Secukinumab Cosyntex
Brodalumab
Ixekizumab
Tofacitinib Xeljanz
ASP015K
LY3009104
Apremilast Otezla