Embed Size (px)
Citation preview
-deprenyl-D2 PET](https://reader042.dokumen.tips/reader042/viewer/2022020613/575091321a28abbf6b9c3ef0/html5/page/1.jpg)
iences 255 (2007) 17–22www.elsevier.com/locate/jns
Journal of the Neurological Sc
Evidence for astrocytosis in ALS demonstrated by[11C](L)-deprenyl-D2 PET☆
Anders Johansson a,⁎, Henry Engler b, Gunnar Blomquist d, Berit Scott c, Anders Wall b,Sten-Magnus Aquilonius a, Bengt Långström b, Håkan Askmark a
a Department of Neurology, University Hospital, S-751 85 Uppsala, Swedenb Uppsala Imanet AB, Box 967, S-751 09 Uppsala, Sweden
c Department of Psychology, Uppsala University, Box 1225, S-751 42 Uppsala, Swedend Department of Oncology, Radiology and Clinical Immunology, Section of Biomedial Radiation Sciences, Uppsala University, Sweden
Received 19 July 2006; received in revised form 19 January 2007; accepted 23 January 2007
Abstract
Objective: To use deuterium-substituted [11C](L)-deprenyl PET to depict astrocytosis in vivo in patients with amyotrophic lateral sclerosis(ALS).Background: In human brain, the enzyme MAO-B is primarily located in astrocytes. L-deprenyl binds to MAO-B and autoradiography with3H-L-deprenyl has been used to map astrocytosis in vitro. Motor neuron loss in ALS is accompanied by astrocytosis and astrocytes may playan active role in the neurodegenerative process. Deuterium-substituted [11C](L)-deprenyl PET provides an opportunity to localize astrocytosisin vivo in the brain of patients with ALS.Methods: Deuterium-substituted [11C](L)-deprenyl PET was performed in seven patients with ALS and seven healthy control subjects.Results: Increased uptake rate of [11C](L)-deprenyl was demonstrated in ALS in pons and white matter.Conclusion: This study provides evidence that astrocytosis may be detected in vivo in ALS by the use of deuterium-substituted [11C](L)-deprenyl PET though further studies are needed to determine whether deuterium-substituted [11C](L)-deprenyl binding tracks diseaseprogression and reflects astrocytosis.© 2007 Elsevier B.V. All rights reserved.
Keywords: Amyotrophic lateral sclerosis; ALS; Motor neuron disease; Astrocytosis; PET; MAO-B; Deprenyl
1. Introduction
Amyotrophic lateral sclerosis (ALS) is characterized bypreferential loss of motor neurons in the motor cortex,brainstem, and spinal cord. The cell loss is accompanied byastrocytosis commonly considered as secondary to the loss ofmotor neurons, but neither the temporal nor the spatialrelationship between astrocytosis and motor neuron degener-ation in the human disease is known [1–3]. In recent years
☆ Anders Johansson received financial support for this work from theUppsala University Research Foundation and The Swedish Association ofNeurologically Disabled.⁎ Corresponding author. Tel.: +46 186115038; fax: +46 186115027.E-mail address: [email protected] (A. Johansson).
0022-510X/$ - see front matter © 2007 Elsevier B.V. All rights reserved.doi:10.1016/j.jns.2007.01.057
interest in the role of astrocytes has increased because it hasbeen suggested that astrocytes play an active role in thedegenerative process [4,5]. For example, Clement et al.demonstrated that nonneuronal cells affect motor neuronsurvival and death in SOD1 mutant mice [6]. Furthermore, aclose temporal relationship exists between neuronal degener-ation and astrogliosis in other animal experiments [7,8]. Theenzyme monoamine oxidase (MAO) is involved in theoxidative deamination of endogenous and exogenous mono-amines. MAO-B is primarily located in astrocytes andserotonergic neurons in the normal as well as the lesionedbrain [9–12]. L-deprenyl binds irreversibly and quantitativelyto MAO-B and [3H]-L-deprenyl binding can therefore be usedtomeasureMAO-B proteinwith autoradiography postmortem[12]. Using this technique we have demonstrated increased
-deprenyl-D2 PET](https://reader042.dokumen.tips/reader042/viewer/2022020613/575091321a28abbf6b9c3ef0/html5/page/2.jpg)
Table 1Clinical characteristics of ALS patients
Patient/sex/age(years)
Onsettype
Diseaseduration(months)
BodyregionswithclinicallyaffectedUMN(number)
ALS-FRS
ALS-FRSbulbarsubscore
Medication
P1/m/40 Limb 30 5 20 6 Ril, CitP2/m/65 Limb 50 4 24 11 Ril, CitP3/f/51 Limb 15 5 26 10 0P4/f/26 Limb 39 5 25 10 Ril, Cit, OC,
BaclofenP5/m/68 Bulbar 11 3 30 4 Cit,
PropranololP6/m/50 Limb 24 3 30 12 RilP7/f/63 Limb 24 1 27 12 Ril, Cit,
Verapamil,Simvastatin,Oxazepam
P2 F-up Limb 60 5 17 8 Ril, Cit,Zolpidem
P3 F-up Limb 23 5 14 8 Ril,Diazepam,Zopiclone
UMN; Upper motor neuron. “Body regions” refer to the four limbs and thebulbar region. ALS-FRS; Amyotrophic Lateral Sclerosis Functional RatingScale score, (maximum score 40, lower numbers = more advanced disease).F-up = follow-up. Ril = Riluzole. Cit = Citalopram. OC = oral contraceptives.
18 A. Johansson et al. / Journal of the Neurological Sciences 255 (2007) 17–22
[3H]-L-deprenyl binding in regions of neurodegeneration inALS, e.g. motor neuron laminae and corticospinal tracts[13,14]. We have also found a high correlation between [3H]-L-deprenyl binding and glial cell count supporting astrocyticlocalization of MAO-B within these areas. PET allows manyfunctional and biochemical parameters to be determinedquantitatively in vivo and visualized in tomographic images.For example, L-deprenyl labeled with carbon-11 (half-life:20.4 min) has been used to image MAO-B in vivo in humanswith PET [15]. Sensitivity in human PET studies with [11C]L-deprenyl is limited in regions of high MAO-B concentrationby the rapid rate of radiotracer trapping, but the use ofdeuterium-substituted [11C](L)-deprenyl ([11C]-DED) mark-edly enhances sensitivity by reducing the rate of binding of thetracer to the enzyme [16]. Thus [11C]-DED is excellent for thevisualization of MAO-B in the brain, which provides anopportunity to indirectly depict astrocytosis [17]. The presentstudy was performed to investigate whether [11C]-DED PETcan be used to demonstrate astrocytosis in vivo in humanssuffering from ALS.
2. Methods
2.1. Patients and controls
Seven nonsmoking patients (age 52±15 years, mean±SD) with ALS, diagnosed according to the El Escorial
criteria [18] and clinically scored according to the ALSfunctional rating scale [19], were investigated with [11C]-DED PET of the brain. The clinical characteristics of thepatients are summarized (Table 1). Two of the patientswere reinvestigated, 8 and 10 months respectively, aftertheir first PET. Seven nonsmoking healthy subjects (age62±2 years, mean±SD) served as a control panel forassessment of normal [11C]-DED PET binding. Age andsex of control persons are presented (Table 2). Age ofpatients and control subjects did not differ significantly.No volunteers had a history of a medical or neurologicaldisease or drug abuse. All patients and control subjectsgave their informed consent to participate in the study,and the study was approved by the Ethics Committee ofthe Faculty of Medicine at Uppsala University and by theRadiation Hazard Ethics Committee of Uppsala Univer-sity Hospital.
2.2. PET scanning
[11C]-DED was produced according to the standardGMP at our laboratory. Radiochemical purity was greaterthan 95%. The specific activity at the time of injection was6.4 ± 2.9 GBq/μmol (mean ±SD). All subjects wereexamined in two Siemens ECAT HR+ whole body PETscanners with neuroinsert, providing 63 contiguous 2.46-mm slices with a 5.6-mm transaxial and 5.4-mm axialresolution (CTI PET Systems Inc. 1999). The orbito-meatal line was used to center the head of the subjects.Patients and healthy control subjects were administered arapid bolus of approximately 400 MBq of [11C]-DED in avenous catheter in the arm. PET measured the time-dependent uptake of radioactivity in the brain according toa predetermined set of measurements (frames of 4×30; 2–3×60; 1×300; and 5 × 600 s) for up to 60 min. The scanswere corrected for attenuation using transmission scans for10 min. Images were reconstructed for each sequentialmeasurement (ECAT software 7.2.1. CTI PET Systems Inc.2001) and subsequently resampled to 30 slices for imageanalysis with the IDA program (Images, Display andAnalysis; GE, 1994). Identical standardized regions ofinterest (ROIs) were placed on the activity images aspreviously described, with the addition of a ROI in themotor cortex, 25 mm above the level of thalami [20]. Inshort, two ROIs, 1.5 cm in diameter, were located in thepons, and the white matter was defined with a free-handROI at the location of the centrum semiovale. CorticalROIs with a width of 1 cm and a length of 3 cm were alsoplaced in the frontal (three slices), parietal (four slices),anterior cingulate cortex (three slices), and the temporallobe (five coronal slices). All regions drawn in more thanone slice were linked to volumes of interest (VOIs). In theoccipital and cerebellar cortices ROIs were drawn at thelevel of highest radioactivity uptake. For practical reasonsthe ROIs were drawn by a reviewer who could not beblinded to diagnosis.
-deprenyl-D2 PET](https://reader042.dokumen.tips/reader042/viewer/2022020613/575091321a28abbf6b9c3ef0/html5/page/3.jpg)
Table 2[11C]-DED slope×10−2 values
Controls and patients sex/age Pons Cerebellum White matter Frontal ctx Parietal ctx Temporal ctx Motor ctx
C1/F/61 1.38 0.79 0.44 1.10 1.02 1.05 0.93C2/M/64 1.43 0.97 0.43 1.16 1.04 1.05 1.00C3/F/60 0.94 0.86 0.47 1.08 0.95 0.91 0.95C4/F/62 0.96 0.77 0.33 1.00 0.86 0.95 0.88C5/M/63 1.31 1.06 0.57 1.18 1.09 1.18 0.97C6/M/61 1.43 0.87 0.31 1.00 0.87 0.96 0.83C7/F/60 1.40 1.08 0.57 1.22 1.05 1.17 0.99Mean controls 1.26 0.91 0.45 1.11 0.98 1.04 0.94±SD 0.22 0.13 0.10 0.09 0.09 0.11 0.06P1/M/40 1.57 0.92 0.73 1.10 0.88 1.08 0.96P2/M/65 1.61 0.88 0.62 1.10 0.99 0.99 1.10P3/F/51 2.20 0.83 1.06 1.38 1.14 1.35 0.99P4/F/26 1.32 0.92 0.54 1.22 1.12 1.19 1.08P5/M/68 1.46 0.87 0.61 1.02 0.84 0.95 0.86P6/M/50 1.68 1.09 0.56 1.12 1.02 1.08 0.94P7/F/63 1.52 1.10 0.75 1.00 0.89 1.09 0.80Mean patients 1.62⁎ 0.94 0.69⁎ 1.13 0.98 1.11 0.96±SD ±0.28 ±0.11 ±0.18 ±0.13 ±0.12 ±0.13 ±0.11P2 F-up 1.56 0.98 0.69 1.11 0.95 1.05 1.03P3 F-up 1.94 0.91 0.78 1.21 1.06 1.15 0.99
C: control. P: patient. F-up: follow-up. ⁎=pb0.01.
19A. Johansson et al. / Journal of the Neurological Sciences 255 (2007) 17–22
2.3. Kinetic analysis
This was a clinical study where it was not consideredfeasible to obtain blood samples. Therefore a reference tissuemodel, a modified “reference-Patlak”method, was used for thekinetic analysis [21–23]. Occipital cortex was chosen asreference region because it is a relatively spared region in ALS.Furthermore, in a post mortem study, L-deprenyl binding inoccipital cortex did not differ between controls and patientswhohad died from ALS [24]. Because of net tracer accumulation inall brain regions, including occipital cortex, no perfect referenceregion could be found. Therefore the reference-Patlak methodcould not be applied in its original form; the uptake in thereference region would never reach equilibrium with the idealinput function (arterial plasma concentration of tracer correctedfor labeled metabolites) and the data distribution in the Patlakplot would become concave, without any well-definedasymptotic part that could be approximated by a straight line.To overcome this problem the original assumption ofequilibrium between the tracer concentrations in the referenceregion and the arterial plasma was replaced by the assumptionthat the reversible (free) component of the tracer in the referenceregion would reach equilibrium with the input function at latetimes, after 20 min. We assumed that the model with onereversible and one irreversible compartment (three rateconstants) was applicable in all regions [21]. The followingvariables were used in the reference-Patlak model:
x ¼Z t
0CrefF ðxÞdx=Cref
F ðtÞ
and
y ¼ CtargS ðtÞ=Cref
F ðtÞ
In comparison with the variables used in the original reference-Patlakmodel, the total radioactivity concentration for each timeframe in the reference region (CS
ref(t)) was replaced by theconcentration of free tracer in the reference region (CF
ref(t)).CStarg(t) was the total radioactivity concentration in the target
region. At late times the distribution in the x- and y-variableswas expected to follow a straight line with a slope that would bean index of irreversible binding in the target region.CF
ref(t) wasrelated to the measured total radioactivity concentration CS
ref(t)in the reference region using the relation:
CrefF ðtÞ ¼ Cref
S ðtÞ � S 3
Z t
0eS 3ðx�tÞCref
S ðxÞdx:
The parameter ℓ3, which is the rate constant for irreversiblebinding in the reference region, was unknown but could beapproximately determined by gradually changing its value fromzero to higher values and observing how the originally concavedata distributions in the Patlak plot gradually became straighter.The smallest ℓ3-value that gave Patlak distributions that fellalong straight lines was chosen as correction parameter. Thesame value for ℓ3 was applied for patients and controls, i.e. itwas assumed that the rate constant for binding in the occipitalcortex was the same in the two groups. The value 0.01 min−1
was found appropriate.This modified reference-Patlak method has been prelimi-
narily reported [22]. A more detailed description of how themethod is applied is under preparation (Blomqvist et al.,Unidirectional influx and net accumulation of PittsburghCompound B, PIB).
In contrast to the relative rate of binding as measured bythe slope of the reference-Patlak method, standard uptakevalues (SUV) are simply the mean uptake normalized to the
-deprenyl-D2 PET](https://reader042.dokumen.tips/reader042/viewer/2022020613/575091321a28abbf6b9c3ef0/html5/page/4.jpg)
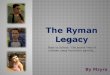
Fig. 1. Sagittal and transaxial 11C-DED PET parametric images of ALSpatient P3 and healthy control C3 (HC), demonstrating increased Patlakslope values in ALS. The transaxial images depict the levels where the whitematter and one of the pons regions of interest were located. The modifiedreference-Patlak method utilizing data from 20 to 60 min was used togenerate the parametrical images.
20 A. Johansson et al. / Journal of the Neurological Sciences 255 (2007) 17–22
injected dose and body weight. A simplification of thekinetic analysis is desirable for clinical introduction of [11C]-DED PET. Therefore, for comparison, we explored SUVfrom 20 to 60 min although SUV are more affected bydifferences in delivery of the tracer caused by other factorsthan MAO-B concentration, such as differences in bloodflow and body constitution, and should be inappropriate toestimate enzyme concentration. We also evaluated SUVnormalized to the corresponding uptake in the occipitalreference region.
2.4. Statistics
In order to reduce the number of comparisons slopevalues of the different ROIs and VOIs were summarizedresulting in the statistical evaluation of only the followingseven regions: pons, cerebellum, white matter, and frontal,parietal, temporal and motor cortex. The anterior cingulategyrus was included in the frontal cortex region. Left andright sides were evaluated together. To determine thepresence of differences in slope values between the groups
of control subjects and ALS, slope values for eachanatomical region were compared using the Kruskal–Wallistest followed by direct comparisons between groups usingMann Whitney U test (two-sided). Significance was set topb0.01. The non-parametric method was chosen becauseof the small sample size and because we could not assumethat our data were normally distributed. Identical statisticalanalysis was applied to the SUV data.
3. Results
The Kruskal–Wallis analysis confirmed the presence ofsignificant differences in slope values ( pb0.0001). Thesubsequent direct comparison between groups revealedincreased [11C]-DED slope in the ALS group in pons( pb0.01) and white matter ( pb0.01). Individual and meanslope values for the respective regions are shown (Table 2).The increased uptake rate in ALS was obvious on visualinspection of PET images (Fig. 1). The sample size was toolimited to permit a meaningful analysis of correlationbetween [11C]-DED slope and clinical characteristics. Thefollow-up scans of patient no 2 and 3 did not differ signi-ficantly from their first scans even though the patients hadprogressed clinically (Tables 1 and 2).
SUV was decreased in ALS in parietal and temporalcortex: The mean SUV±SD in parietal cortex was 3.5±0.45in ALS and 4.2±0.38 in control persons ( pb0.01). In tem-poral cortex it was 3.7±0.32 in ALS and 4.2±0.28 in controlpersons ( pb0.01). No other significant SUV differenceswere found although there was a trend towards a decrease inALS also in frontal and motor cortex ( pb0.05).
SUV normalized to the corresponding uptake in theoccipital reference region was in pons 1.4±0.12 in ALS and1.2±0.13 in control persons ( p 0.011). In white matter itwas 0.75±0.098 in ALS and 0.69±0.067 in control persons( p 0.32). These trends towards increased values in ALS didthus not reach the chosen significant level and there were noother differences between groups.
4. Discussion
This is the first study to demonstrate cerebral astrocytosisin vivo in ALS. The increased [11C]-DED binding rate inwhite matter in the patients accords well with previousneuropathological findings of widespread astrocytosis in thesubcortical white matter in ALS [2]. Astrocytosis in ALS hasalso been demonstrated post mortem in other parts of thecorticospinal tract but pons has not been included [3,13].Since we lack neuropathological support in this region, wemust interpret the increased binding rate in pons cautiously.Nevertheless, the increased binding rate in pons, where thecorticospinal tract fibers have converged, may reflectcorticospinal tract astrocytosis.
Uptake rate of [11C]-DED increases with age [25]. Theonly patient with a lower slope in pons than the highest valuein the control group was the youngest patient. Age did not
-deprenyl-D2 PET](https://reader042.dokumen.tips/reader042/viewer/2022020613/575091321a28abbf6b9c3ef0/html5/page/5.jpg)
21A. Johansson et al. / Journal of the Neurological Sciences 255 (2007) 17–22
differ significantly between groups, but the patients wereslightly younger than the controls. This further strengthensour findings of increased uptake rate in ALS.
While we cannot claim that the binding pattern in ourpatients with ALS is a specific finding for this disorder, wehave so far not found this type of binding pattern in otherpatients investigated with [11C]-DED PET [20]. Studies arenow also ongoing to map astrocytosis by the use of [11C]-DED PET in Alzheimer's disease.
It has not been studied whether riluzole or the othermedications our patients were taking affects [11C]-DEDkinetics. To minimize this risk, the patients were not allowedto take any medication on the day of examination. Plasmasamples were not taken, and therefore we do not know howmetabolism of [11C]-DED affected our results. It is known thatthe metabolism of nondeuterium-substituted 11C-deprenyl isaffected by treatment with antiepileptic drugs, consistent withinduction of hepatic microsomal enzymes by antiepilepticdrugs [26]. However, none of the patients was treated withantiepileptics or other similar enzyme-inducing medication.MAO-B is known to recover slowly after inactivation, butMAO-B inhibitory drugs are usually not used in this patientgroup, and a single challenge with trace amounts of [11C]-DED is unlikely to affect results of repeated scans [27].
The normalized SUV results were similar to the results ofthe modified reference-Patlak method, but failed to reachsignificance. The non-normalized SUVs were decreased inparietal and temporal cortex in ALS. This may be a reflectionof decreased regional cerebral blood flow in these areas inALS [28]. There are no previous publications using SUV toevaluate [11C]-DED, and our SUV results confirmed theneed for kinetic modeling to estimate MAO-B concentrationfrom [11C]-DED PET also in ALS [16].
Compared to PET, SPECT is a less expensive and morewidely accessible method though it is less sensitive. Given thekinetic properties of [11C]-DED it is unlikely that [11C]-DEDcan be modified for use in SPECT. Perhaps other ligands forMAO-B such as the iodinated MD-230254 derivate [123I]2-IBPO [29] or [123I]Ro-43-0463 [30] that have been used inSPECTcan become useful in the examination of ALS patients.
There are at present no specific PET markers for motorneurons, but previous PET studies in ALS patients haverevealed decreases in the binding of radiotracers fordopaminergic [31], GABA-ergic [32,33] and serotonergic[34] function, glucose metabolism [35,36] and regionalblood flow [28,37]. A “positive tracer” i.e. a tracer wheredisease causes increased rather than decreased uptake, wouldbe preferable for following disease progression. The firststudy with a positive PET marker in ALS was performed byTurner et al. who demonstrated microglial activation with theuse of PK11195 [38]. Our study represents the second PETstudy in ALS with a “positive tracer”.
Only two of our ALS patients underwent a second PET.Both patients had deteriorated clinically at the time of thesecond examination, but we saw no trend in the slope valuesthat cannot be explained by variability in the method [39].
Though our study suggests that [11C]-DED PET may be apotential surrogate marker of disease progress, the highbackground activity of MAO-B and our small sample sizelimit clinical introduction before longitudinal studies arepresented. Particularly troubling is that the two follow-upscans of patients who had deteriorated stayed the same. Thisshould dampen enthusiasm with respect to the use of [11C]-DED as a surrogate marker. In fact, it is not known whetherastrocytosis increases in a linear fashion as ALS progresses.Perhaps other imaging techniques, such as diffusion tensorimaging of the corticospinal tract, can prove to be moreuseful as a surrogate marker of disease progression [40].
Even though MAO-B is not strictly located in astrocytes,our findings emphasize the role of astrocytes in thepathological process [4,5]. Astrocytosis has been shown toprecede microglial activation in mouse models of motorneuron disease, but it is not known whether this is the casealso in humans suffering from ALS [41,42]. The combina-tion of [11C](R)-PK11195 and [11C]-DED PET to clarify thetemporal and spatial relationship between microglial activa-tion and astrocytosis in human disease merits furtherinvestigation.
In summary, [11C]-DED PET binding rate is increased inpons and white matter in patients with ALS, possiblyreflecting astrocytosis.
Acknowledgment
The control material on [11C]-DED PET binding in thismanuscript is used with kind permission from StéphaneNave, MD. F. Hoffmann-La Roche Ltd, PharmaceuticalsDivision.
References
[1] Kamo H, Haebara H, Akiguchi I, Kameyama M, Kimura H, McGeerPL. A distinctive distribution of reactive astroglia in the precentralcortex in amyotrophic lateral sclerosis. Acta Neuropathol (Berl)1987;74(1):33–8.
[2] Kushner PD, Stephenson DT, Wright S. Reactive astrogliosis iswidespread in the subcortical white matter of amyotrophic lateralsclerosis brain. J Neuropathol Exp Neurol 1991;50(3):263–77.
[3] Schiffer D, Cordera S, Cavalla P, Migheli A. Reactive astrogliosis ofthe spinal cord in amyotrophic lateral sclerosis. J Neurol Sci1996;139:27–33 (Suppl).
[4] Silani V, Ciammola A, Pizzuti A, Cardin V, Scarlato G. Motor neuronemetabolism. J Neurol Sci 1999;169(1–2):161–9.
[5] Barbeito LH, Pehar M, Cassina P, Vargas MR, Peluffo H, Viera L, et al.A role for astrocytes in motor neuron loss in amyotrophic lateralsclerosis. Brain Res Brain Res Rev 2004;47(1–3):263–74.
[6] Clement AM, Nguyen MD, Roberts EA, Garcia ML, Boillee S, RuleM, et al. Wild-type nonneuronal cells extend survival of SOD1 mutantmotor neurons in ALS mice. Science 2003;302(5642):113–7.
[7] Levine JB, Kong J, Nadler M, Xu Z. Astrocytes interact intimatelywith degenerating motor neurons in mouse amyotrophic lateralsclerosis (ALS). Glia 1999;28(3):215–24.
[8] Fischer LR, Culver DG, Tennant P, Davis AA, Wang M, Castellano-Sanchez A, et al. Amyotrophic lateral sclerosis is a distal axonopathy:evidence in mice and man. Exp Neurol 2004;185(2):232–40.
-deprenyl-D2 PET](https://reader042.dokumen.tips/reader042/viewer/2022020613/575091321a28abbf6b9c3ef0/html5/page/6.jpg)
22 A. Johansson et al. / Journal of the Neurological Sciences 255 (2007) 17–22
[9] Oreland L, Fowler CJ, Carlsson A, Magnusson T. Monoamine oxidase-A and -B activity in the rat brain after hemitransection. Life Sci1980;26(2):139–46.
[10] Levitt P, Pintar JE, Breakefield XO. Immunocytochemical demonstrationof monoamine oxidase B in brain astrocytes and serotonergic neurons.Proc Natl Acad Sci U S A 1982;79(20):6385–9.
[11] Nakamura S, Kawamata T, Akiguchi I, Kameyama M, Nakamura N,Kimura H. Expression of monoamine oxidase B activity in astrocytesof senile plaques. Acta Neuropathol (Berl) 1990;80(4):419–25.
[12] Jossan SS, Gillberg PG, d'Argy R, Aquilonius SM, Langstrom B,Halldin C, et al. Quantitative localization of human brain monoamineoxidase B by large section autoradiography using L-[3H]deprenyl.Brain Res 1991;547(1):69–76.
[13] Aquilonius SM, Jossan SS, Ekblom JG, Askmark H, Gillberg PG.Increased binding of 3H-L-deprenyl in spinal cords from patients withamyotrophic lateral sclerosis as demonstrated by autoradiography.J Neural Transm Gen Sect 1992;89(1–2):111–22.
[14] Ekblom J, Jossan SS, Bergstrom M, Oreland L, Walum E, AquiloniusSM. Monoamine oxidase-B in astrocytes. Glia 1993;8(2):122–32.
[15] Fowler JS, MacGregor RR, Wolf AP, Arnett CD, Dewey SL, SchlyerD, et al. Mapping human brain monoamine oxidase A and B with 11C-labeled suicide inactivators and PET. Science 1987;235(4787):481–5.
[16] Fowler JS, Wang GJ, Logan J, Xie S, Volkow ND, MacGregor RR, etal. Selective reduction of radiotracer trapping by deuterium substitu-tion: comparison of carbon-11-L-deprenyl and carbon-11-deprenyl-D2for MAO B mapping. J Nucl Med 1995;36(7):1255–62.
[17] Fowler JS, Logan J, Volkow ND, Wang GJ, MacGregor RR, Ding YS.Monoamine oxidase: radiotracer development and human studies.Methods 2002;27(3):263–77.
[18] Brooks BR. El Escorial World Federation of Neurology criteria for thediagnosis of amyotrophic lateral sclerosis. Subcommittee on MotorNeuron Diseases/Amyotrophic Lateral Sclerosis of the WorldFederation of Neurology Research Group on Neuromuscular Diseasesand the El Escorial “Clinical limits of amyotrophic lateral sclerosis”workshop contributors. J Neurol Sci 1994;124:96–107 (Suppl).
[19] The Amyotrophic Lateral Sclerosis Functional Rating Scale. Assess-ment of activities of daily living in patients with amyotrophic lateralsclerosis. The ALS CNTF treatment study (ACTS) phase I–II StudyGroup. Arch Neurol 1996;53(2):141–7.
[20] EnglerH, Lundberg PO, EkbomK,Nennesmo I,NilssonA,BergstromM,et al.Multitracer studywith positron emission tomography inCreutzfeldt–Jakob disease. Eur J Nucl Med Mol Imaging 2003;30(1):85–95.
[21] Patlak CS, Blasberg RG. Graphical evaluation of blood-to-braintransfer constants from multiple-time uptake data. Generalizations.J Cereb Blood Flow Metab 1985;5(4):584–90.
[22] Blomqvist G, Engler H, Wall A, Långström B. Graphical analysis oftime-activity data using a reference region with known irreversiblebinding. In: Knuuti J, NågrenK, editors. ANNALESUNIVERSITATISTURKUENSIS Ser. D: Medica - Odontologica. Turku PET Sympo-sium. Abstracts of the IX Turku PET Symposium, May 25–28, 2002,Turku, Finland. vol. 499. Turku University; 2002. p. 120.
[23] Lundquist P, Blomquist G, Hartvig P, Hagberg GE, Torstenson R,Hammarlund-Udenaes M, et al. Validation studies on the 5-hydroxy-L-[beta-11C]-tryptophan/PET method for probing the decarboxylase stepin serotonin synthesis. Synapse 2006;59(8):521–31.
[24] Ekblom J, Jossan SS, Gillberg PG, Oreland L, Aquilonius SM.Monoamine oxidase-B in motor cortex: changes in amyotrophic lateralsclerosis. Neuroscience 1992;49(4):763–9.
[25] Fowler JS, Volkow ND, Wang GJ, Logan J, Pappas N, Shea C, et al.Age-related increases in brain monoamine oxidase B in living healthyhuman subjects. Neurobiol Aging 1997;18(4):431–5.
[26] Cumming P, Yokoi F, Chen A, Deep P, Dagher A, Reutens D, et al.Pharmacokinetics of radiotracers in human plasma during positronemission tomography. Synapse 1999;34(2):124–34.
[27] Fowler JS, Volkow ND, Logan J, Wang GJ, MacGregor RR, SchylerD, et al. Slow recovery of human brain MAO B after L-deprenyl(Selegeline) withdrawal. Synapse 1994;18(2):86–93.
[28] Kew JJ, Leigh PN, Playford ED, Passingham RE, Goldstein LH,FrackowiakRS, et al. Cortical function in amyotrophic lateral sclerosis. Apositron emission tomography study. Brain 1993;116(Pt 3):655–80.
[29] Hirata M, Kagawa S, Yoshimoto M, Ohmomo Y. Synthesis andcharacterization of radioiodinatedMD-230254: a new ligand for potentialimaging of monoamine oxidase B activity by single photon emissioncomputed tomography. Chem Pharm Bull (Tokyo) 2002;50(5):609–14.
[30] Buck A, Frey LD, Blauenstein P, Kramer G, Siegel A, Weber B, et al.Monoamine oxidase B single-photon emission tomography with [123I]Ro 43-0463: imaging in volunteers and patients with temporal lobeepilepsy. Eur J Nucl Med 1998;25(5):464–70.
[31] Takahashi H, Snow BJ, Bhatt MH, Peppard R, Eisen A, Calne DB.Evidence for a dopaminergic deficit in sporadic amyotrophic lateralsclerosis on positron emission scanning. Lancet 1993;342(8878):1016–8.
[32] Lloyd CM, Richardson MP, Brooks DJ, Al-Chalabi A, Leigh PN.Extramotor involvement in ALS: PET studies with the GABA(A)ligand [(11)C]flumazenil. Brain 2000;123(Pt 11):2289–96.
[33] Turner MR, Hammers A, Al-Chalabi A, Shaw CE, Andersen PM,BrooksDJ, et al. Distinct cerebral lesions in sporadic and ‘D90A’ SOD1ALS: studies with [11C]flumazenil PET. Brain 2005;128(Pt 6):1323–9.
[34] TurnerMR, Rabiner EA, Hammers A, Al-Chalabi A, Grasby PM, ShawCE, et al. [11C]-WAY100635 PET demonstrates marked 5-HT1Areceptor changes in sporadic ALS. Brain 2005;128(Pt 4):896–905.
[35] Dalakas MC, Hatazawa J, Brooks RA, Di Chiro G. Lowered cerebralglucose utilization in amyotrophic lateral sclerosis. Ann Neurol1987;22(5):580–6.
[36] Ludolph AC, Langen KJ, Regard M, Herzog H, Kemper B, Kuwert T,et al. Frontal lobe function in amyotrophic lateral sclerosis:a neuropsychologic and positron emission tomography study. ActaNeurol Scand 1992;85(2):81–9.
[37] Tanaka M, Kondo S, Hirai S, Sun X, Yamagishi T, Okamoto K. Cerebralblood flow and oxygen metabolism in progressive dementia associatedwith amyotrophic lateral sclerosis. J Neurol Sci 1993;120(1):22–8.
[38] Turner MR, Cagnin A, Turkheimer FE, Miller CC, Shaw CE, BrooksDJ, et al. Evidence of widespread cerebral microglial activation inamyotrophic lateral sclerosis: an [(11)C](R)-PK11195 positron emis-sion tomography study. Neurobiol Dis 2004;15(3):601–9.
[39] Logan J, Fowler JS, Volkow ND, Wang GJ, MacGregor RR, Shea C.Reproducibility of repeated measures of deuterium substituted [11C]L-deprenyl ([11C]L-deprenyl-D2) binding in the human brain. Nucl MedBiol 2000;27(1):43–9.
[40] Wang S, Poptani H,BilelloM,WuX,Woo JH, ElmanLB, et al. Diffusiontensor imaging in amyotrophic lateral sclerosis: volumetric analysis of thecorticospinal tract. AJNR Am J Neuroradiol 2006;27(6):1234–8.
[41] Hall ED, Oostveen JA, Gurney ME. Relationship of microglial andastrocytic activation to disease onset and progression in a transgenicmodel of familial ALS. Glia 1998;23(3):249–56.
[42] Rathke-Hartlieb S, Schmidt VC, Jockusch H, Schmitt-John T, BartschJW. Spatiotemporal progression of neurodegeneration and gliaactivation in the wobbler neuropathy of the mouse. Neuroreport1999;10(16):3411–6.



![Parametric [11c]flumazenil images 3.pdf · Parametric [11C]flumazenil images | 51INTRODUCTION [11C]Flumazenil (FMZ) is a well known positron emission tomography (PET) tracer, which](https://img.dokumen.tips/doc/110x75/5e6cc96120477523c50be581/parametric-11cflumazenil-images-3pdf-parametric-11cflumazenil-images-51introduction.jpg)