Embed Size (px)
Citation preview
Evidence-Based Treatment for Children with Autism 19 Copyright © 2014 Doreen Granpeesheh and
Jonathan Tarbox. Published by Elsevier Inc. All rights reserved.
C H A P T E R
3
Autism spectrum disorder (ASD) is a neurodevelopmental disorder. Neurodevelopmental disorders are characterized by onset in the devel-opmental period and the presence of deficits that produce impairment in personal, social, academic, or occupational functioning. The Diagnostic and Statistical Manual of Mental Disorders (DSM), published by the American Psychiatric Association, is the standard reference that is used for medical classification and diagnosis of ASD, among other disorders. The DSM has been revised several times over the past 60 years and is currently in its fifth edition (DSM-5; APA), released in May, 2013. The diagnostic criteria for ASD changed significantly from DSM-IV to DSM-5, and this chapter will describe these changes and what they mean for you as a treatment provider. We will also review who can give a diagnosis, as well as some of the standardized assessments used to diagnose ASD.
PROFESSIONALS WHO CAN DIAGNOSE ASD
The authority to give an official diagnosis of ASD is reserved for licensed medical doctors and psychologists. Most parents bring their child to a pediatrician when they first become alarmed that something may be awry with the child’s development. Pediatricians are allowed to give the ASD diagnosis, but, unless they have specialized training and experience in ASD, they should almost always refer the child to a specialist for a more thorough assessment. School psychologists are permitted to give the ASD diagnosis for use in school, but a diagnosis by a licensed medical doctor or psychologist is required for the diagnosis to be recognized outside of the
The Diagnosis of Autism Spectrum Disorder
Doreen Granpeesheh, Megan Maixner, Cecilia Knight, Monique Erickson

20 3. THE DIAGnoSIS of AuTISm SPECTRum DISoRDER
school setting. Regardless of who provides the diagnosis, no formal test-ing is required, but it is highly recommended. We provide descriptions of some of the more useful diagnostic assessments included in the Center for Autism and Related Disorders (CARD) Model at the end of the chapter.
DIAGNOSTIC CRITERIA
The diagnostic criteria for ASD 299.00, according to the DSM-5, consist of two sets of symptoms: 1) social communication and social interaction deficits, and 2) the presence of restrictive, repetitive patterns of behavior, interests, or activities. These symptoms must present in the early develop-ment period, although they may not fully manifest until social demands exceed capabilities, or they may be masked by learned strategies later in life. The symptoms together must cause significant impairment in other areas of everyday functioning and must not be better described by another DSM-5 diagnosis. These criteria are discussed in greater depth below.
Criterion 1: Social Communication and Social Interaction Deficits
The first criterion is persistent deficits in social communication and so-cial interaction across multiple contexts. To qualify for an ASD diagnosis, the child must meet the criteria for all three social communication and social interaction deficits described below:
1. Deficits in social-emotional reciprocity. These deficits may include abnormal social approach and failure of normal back-and-forth conversation; reduced sharing of interests, emotions, or affect; and failure to initiate or respond to social interactions. These deficits often become apparent when an individual 1) does not reciprocate social exchanges (e.g., greetings), 2) does not understand the emotions of others (e.g., keeps playing and shows no reaction when peer falls down and cries), and 3) lacks empathy for others (e.g., does not appear to feel sad when a peer or family member is sad).
2. Deficits in nonverbal communicative behaviors used for social interaction. These deficits include poorly integrated verbal and nonverbal communication, abnormalities in eye contact and body language (e.g., avoids eye contact with others), difficulty understanding and using gestures, and lacking understanding and use of appropriate facial expressions (e.g., does not react to peer’s angry facial expression).
3. Deficits in developing, maintaining, and understanding relationships. Deficits in this area include difficulties adjusting behavior to suit

DIAGnoSTIC CRITERIA 21
various social contexts, difficulties in sharing imaginative play or making friends, and an absence of interest in peers. Deficits of this nature may be exhibited when an individual does not develop friendships appropriate to a developmental level beyond those with caregivers (e.g., spends no time with peers outside of times prescribed by teachers). Children may also have great difficulty maintaining any existing peer relationships. This type of deficit may also be displayed by an individual who only plays with much younger children and does not have relationships with children of the same age.
Criterion 2: Restricted, Repetitive Patterns of Behavior, Interests, or Activities
In addition to Criterion 1, an individual must meet criteria for at least two of the following four symptom areas related to restricted and repeti-tive behaviors and interests to qualify for an ASD diagnosis:
1. Stereotyped or repetitive motor movements, use of objects, or speech. Examples of these behaviors include repeating sounds, words, or phrases out of context (ranging from single words or sounds to entire scripts of movies) and repeated movements, such as hand flapping, flipping a light switch on and off, twirling objects, lining up toys, and so on.
2. Insistence on sameness, inflexible adherence to routines, or ritualized patterns of verbal or nonverbal behavior. Children with these symptoms may display extreme distress at small changes in schedules or routines (e.g., becoming upset when classroom schedule changes), inflexibility with changes to the organization or placement of objects, difficulty with transitions, or rigid thinking patterns.
3. Highly restricted, fixated interests that are abnormal in intensity or focus. Children may display unreasonably strong attachment to or preoccupation with unusual objects, carry or hoard particular objects, or have excessively circumscribed or perseverative interests. Some children perseverate on specific topics (e.g., a child may turn every conversation into a discussion about mathematics).
4. Hyper- or hyporeactivity to sensory input or unusual interest in sensory aspects of the environment. Children with these symptoms may display apparent indifference to pain or extreme temperatures or may overreact to differences in temperature. They may have unreasonably adverse responses to specific sounds or textures, such as tantrumming whenever the family uses the kitchen blender or crying in terror upon handling sand or uncooked rice.

22 3. THE DIAGnoSIS of AuTISm SPECTRum DISoRDER
Symptoms Must Appear During Early Development
In addition to meeting the criteria described above, symptoms must be present in the early developmental period. In other words, if a child develops typically and then starts to show the symptoms described above during adolescence, she would not qualify for an ASD diagnosis. However, it is important to note that some symptoms are less likely to fully manifest until the child has greater social demands placed on her. For example, if a toddler has no siblings, does not attend daycare, and has very little inter-action with neighbors or peers, then her parents may not notice many of the signs of social deficits because the child has had little in the way of so-cial demands placed on her. As she begins to interact with other children more, the seriousness of her social deficits may become clearer.
Symptoms Must Cause Clinically Significant Impairment
In order to qualify for an ASD diagnosis, symptoms must cause clin-ically significant impairment in social, occupational, or other important areas of current functioning. Put simply, ASD does not simply mean that the child is different from other children but, rather, that his deficits are severe enough to affect his quality of life on a daily basis. For example, social deficits that result in the child making few or no meaningful peer relationships would qualify as clinically significant. Similarly, communi-cative deficits that are severe enough that the child cannot tell his parents what he wants, thereby leading to tantrums, would cause clinically sig-nificant distress for him and his family. Finally, if a child’s obsession with engaging in repetitive behavior takes up so much of his time that he never develops any other leisure skills, his quality of life is likely to suffer to a clinically significant degree.
As awareness of ASD has risen in recent decades, it has become a some-what popular topic in the general media. As a result, some people may casually declare themselves to have ASD or Asperger’s disorder if they are particularly good at using computers or are particularly socially awk-ward. It is important to keep in mind, however, that ASD is not the same as having a unique and quirky personality. If a person is highly socially awkward and would rather spend all of her time memorizing statistics, but she still engages in the social behaviors needed to make friends and function at work and at home, she likely does not qualify for an ASD di-agnosis. There are likely thousands of people who find social interaction annoying and/or terrifying and who would rather spend all of their time engaging in one or two particular hobbies, but this does not mean they have ASD. For diagnostic purposes, such traits must be so severe that they prevent people from succeeding independently in their social, family, or academic lives.

DIAGnoSTIC CRITERIA 23
Intellectual Disability and Global Developmental Delay
To receive an ASD diagnosis, the DSM requires that an individual’s symptoms cannot be better explained by intellectual disability (intellec-tual developmental disorder) or global developmental delay. Intellectual disability and ASD frequently co-occur. However, the symptoms of each disorder are distinct, and all must be present in order for both diagnoses to be made.
Specifiers
If an individual meets the full criteria for ASD described above, the diagnosis should also include specifiers. A specifier provides the etiology and/or other important features of the presenting symptoms that are rel-evant to the treatment of the diagnosed condition. Specifiers are not in-tended to be mutually exclusive or jointly exhaustive, and therefore, more than one specifier may be given for a particular diagnosis.
Comorbidity. The DSM-5 indicates that the diagnosis of ASD is to spec-ify the following comorbid (co-occurring) conditions:
• With or without accompanying intellectual impairment• With or without accompanying language impairment• Associated with a known medical or genetic condition or
environmental factor (e.g., sleep disorder or epilepsy)• Associated with another neurodevelopmental, mental, or behavioral
disorder• With catatonia
Age and pattern of onset. Although the symptoms of ASD are typi-cally identified during the second year of life (12–24 months of age), these symptoms may have been observed earlier than 12 months or later than 24 months, depending on the individual and the severity or subtleness of symptoms in day-to-day life. Additionally, some children with ASD demonstrate developmental plateaus or regression, with a gradual or rapid deterioration in social or language skills. This information is im-portant because these types of losses are rare in other disorders and can serve as a red flag for ASD, helping distinguish symptoms of ASD from other developmental delays and/or disorders (Table 3.1).
Severity. One of the most beneficial applications of the DSM-5 is that it allows the diagnostician to assign severity specifiers to the two main symptom areas. Severity specifiers rate the intensity, frequency, duration, symptom count, or other severity indicators of the social communication deficits and restricted, repetitive behaviors seen in ASD. Both symptom areas are assigned a severity, ranging from 1 (least severe) to 3 (most se-vere). Levels of severity are defined by how much support the symptoms
24 3. THE DIAGnoSIS of AuTISm SPECTRum DISoRDER
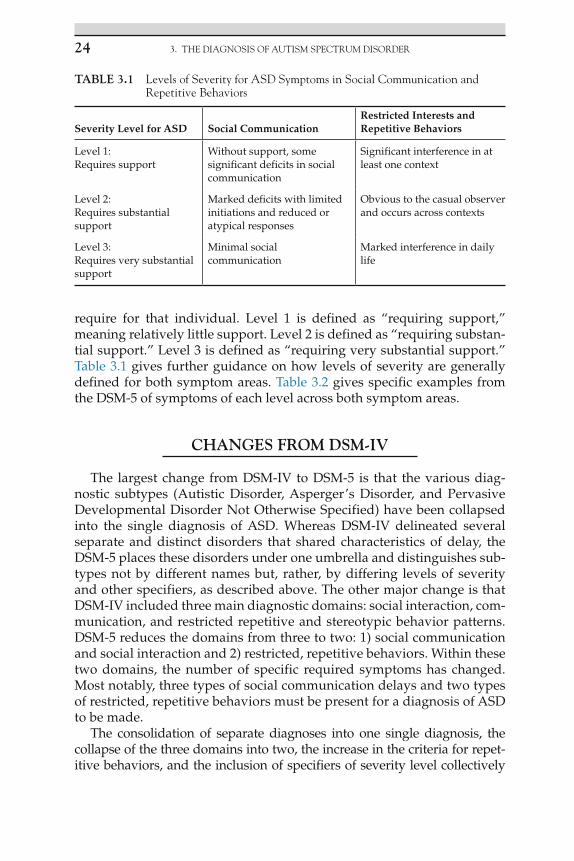
require for that individual. Level 1 is defined as “requiring support,” meaning relatively little support. Level 2 is defined as “requiring substan-tial support.” Level 3 is defined as “requiring very substantial support.” Table 3.1 gives further guidance on how levels of severity are generally defined for both symptom areas. Table 3.2 gives specific examples from the DSM-5 of symptoms of each level across both symptom areas.
CHANGES FROM DSM-IV
The largest change from DSM-IV to DSM-5 is that the various diag-nostic subtypes (Autistic Disorder, Asperger’s Disorder, and Pervasive Developmental Disorder Not Otherwise Specified) have been collapsed into the single diagnosis of ASD. Whereas DSM-IV delineated several separate and distinct disorders that shared characteristics of delay, the DSM-5 places these disorders under one umbrella and distinguishes sub-types not by different names but, rather, by differing levels of severity and other specifiers, as described above. The other major change is that DSM-IV included three main diagnostic domains: social interaction, com-munication, and restricted repetitive and stereotypic behavior patterns. DSM-5 reduces the domains from three to two: 1) social communication and social interaction and 2) restricted, repetitive behaviors. Within these two domains, the number of specific required symptoms has changed. Most notably, three types of social communication delays and two types of restricted, repetitive behaviors must be present for a diagnosis of ASD to be made.
The consolidation of separate diagnoses into one single diagnosis, the collapse of the three domains into two, the increase in the criteria for repet-itive behaviors, and the inclusion of specifiers of severity level collectively
TABLE 3.1 Levels of Severity for ASD Symptoms in Social Communication and Repetitive Behaviors
Severity Level for ASD Social CommunicationRestricted Interests and Repetitive Behaviors
Level 1:Requires support
Without support, some significant deficits in social communication
Significant interference in at least one context
Level 2:Requires substantial support
Marked deficits with limited initiations and reduced or atypical responses
Obvious to the casual observer and occurs across contexts
Level 3:Requires very substantial support
Minimal social communication
Marked interference in daily life

CHAnGES fRom DSm-IV 25
reflect changes that were made as part of the shift from a categorical ap-proach to a dimensional one. DSM-5 acknowledges the need to evolve in the context of other clinical research initiatives (e.g., cognitive neurosci-ence, brain imaging, epidemiology, genetics, and so forth) in the field. An important aspect of that transition is recognizing that the previous rigid cat-egorical classification system did not reflect clinical experience or scientific observations. The boundaries between the various symptoms associated with ASD are more fluid over the lifespan than the DSM-IV acknowledged, and many symptoms assigned to a single disorder may occur at varying lev-els of severity in many other disorders. Therefore, the DSM-5 attempts to accommodate these findings by adopting dimensional approaches to mental disorders that include dimensions that cut across categories. This approach is intended to produce more accurate descriptions of patient presentations and increase the validity of the diagnosis by presenting a thorough range of the symptoms present.
TABLE 3.2 Examples of Symptoms of ASD Across Both Symptom Areas and All Three Levels of Severity, from the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (APA, 2013)
Symptom AreaSeverity Level Examples
Social Communication and Social Interaction
1 Difficulty initiating and responding to social interactions. Decreased interest in others. Speaks in full sentences but difficulty with conversation. Attempts to make friends are often odd and unsuccessful.
2 Marked impairments noticeable even with supports in place. Limited response and initiations to social interactions.Speaks in simple limited sentences. Limited and odd nonverbal communication. Interactions are limited to narrow special interests.
3 Limited social initiations and minimal responding to others.Few words of intelligible speech. Rarely initiates and when does uses unusual approaches. Responds only to very direct social initiations.
Restricted and Repetitive Behavior and Interests
1 Marked inflexibility. Difficulty switching activities.Poor planning and organization skills that impactindependent functioning.
2 Inflexibility in behavior. Difficulty coping with change.
3 Extreme inflexibility and difficulty coping with changes. Marked distress when needing to change focus or action.Repetitive/restricted behaviors markedly interfere with all other areas of functioning.

26 3. THE DIAGnoSIS of AuTISm SPECTRum DISoRDER
It is also interesting to note that the DSM-5 specifically acknowledges the presence of abnormal responses to sensory experiences in individuals with ASD through the inclusion of hyper- or hyporeactivity to sensory input as one of the symptoms in the restricted, repetitive behavior do-main. Clinicians have widely acknowledged for years that many individ-uals with ASD have divergent reactions to sensory input, but the DSM-IV diagnostic criteria did not include this. We have observed repeatedly that some children with ASD are particularly challenged by sensory input of particular sorts (e.g., particular sounds or textures). On the other hand, some children have outstanding strengths in particular sensory areas, such as visual stimuli. Individual child sensory profiles must be consid-ered in order for treatment to be optimally effective (see Chapter 6 on visual and other sensory modifications). We hope that the inclusion of sensory abnormalities in the DSM-5 criteria will help bring greater atten-tion to the topic and, therefore, more research on how to customize treat-ment for sensory issues.
The inclusion of medical or genetic factors as a specifier in the DSM-5 criteria is new and interesting. To date, relatively few medical conditions have been associated with ASD. Fragile X and tuberous sclerosis are among the most well-known disorders that lead to autistic-like symp-toms. For the first time, DSM-5 acknowledges the existence of associations between ASD and medical conditions. We are hopeful that this acknowl-edgment will lead to further research that will enhance our understanding of the etiology of ASD.
It may be important to note that a new diagnosis in the DSM-5, Social Communication Disorder (SCD), may cause confusion for the inexperi-enced diagnostician, as it shares some characteristics with ASD. The SCD diagnosis is given to children who have difficulty in the social use of ver-bal or nonverbal communication to such an extent that it affects the devel-opment of their relationships, comprehension, academic achievement, or occupational performance. While SCD touches upon a very distinct com-monality with ASD (the lack of social communication), it does not account for the restricted, repetitive behaviors present in ASD. As such, it must be understood as a clearly distinct disorder.
Implications of Changes in DSM-5
The gold standard method for diagnosing ASD includes the use of standardized diagnostic assessments. The vast majority of these were developed using DSM-IV criteria, so they will need to be revised. At the time this manual goes to press, we have not yet seen the full effect of the changes in the DSM-5 on access to services and availability of third-party funding for treatment. Many are concerned that some children, who formerly would have been diagnosed with Asperger’s disorder and
DIAGnoSTIC ASSESSmEnTS 27
who suffer from clinically significant impairment in their daily lives, will no longer qualify for an ASD diagnosis according to the DSM-5. Still others are concerned that funding sources will intentionally influence diagnosticians to lean toward SCD, rather than ASD with low severity, because they will be less likely to have to provide funding for treatment, given that SCD has no treatment guidelines and insurance carriers are not mandated to pay for its treatment. Research addressing these top-ics is still under way, and the future will provide the answers to these questions.
DIAGNOSTIC ASSESSMENTS
Autism Diagnostic Observation Scale, Second Edition
The Autism Diagnostic Observation Scale (ADOS; Lord et al., 1989) is a widely regarded semi-structured assessment for diagnosing ASD. While direct clinical observation remains paramount in any assessment, some clinicians in the field now consider the ADOS to be the “gold standard” of autism observation measures. The ADOS consists of a standardized set of scenarios that a trained clinician presents to the individual being assessed. These scenarios are designed to produce situations in which the clinician can evaluate communication, social interaction, play, and imagination skills, as well as examine any potential symptomology of ASD. That is, the contrived scenarios give the child being evaluated the opportunity to behave or react as a typically developing child generally would. In this way, if the child being evaluated reacts to the situation by performing dif-ferently or demonstrating atypical behavior, differences are apparent to the clinician.
The ADOS is now in its second edition and includes revised algorithms. The ADOS-2 (Gotham, Risi, Pickles, and Lord, 2007) can be used to eval-uate almost anyone who is suspected to have ASD, from infants with no speech to adults who are verbally fluent. The ADOS-2 consists of five modules. An individual being assessed is only administered one module based on age and language abilities. Module 1 is designed for children 31 months and over who do not consistently use phrase speech; Module 2 is for children of any age who use phrase speech but are not verbally fluent; Module 3 is for verbally fluent children and young adolescents; and Module 4 is for verbally fluent older adolescents and adults. New to the ADOS is the Toddler Module, intended for use with children aged 12 to 30 months who do not consistently use phrase speech. The Toddler Module involves interacting with the child in minimally structured ac-tivities with reinforcing items. The goal is the same: to flag any behaviors consistent with an ASD diagnosis.

28 3. THE DIAGnoSIS of AuTISm SPECTRum DISoRDER
The time required to administer the ADOS-2 ranges from 40 to 60 minutes. Examiners need to have thorough knowledge of the exact ad-ministration and scoring procedures. A higher degree of training and ex-perience with ASD is required for competent interpretation of test results. The clinician administering the ADOS-2 requires extensive training and supervision. To score the ADOS-2 throughout the observation period, the examiner rates the child’s performance in each scenario. Items are rated on a three-point scale (0 = within normal limits, 1 = infrequent or possible abnormality, and 2 = definite abnormality). The scores on the ADOS are put into a diagnostic algorithm based on criteria for ASD. The revised scoring algorithms of the ADOS-2 reflect social and communication items as one social communication factor, and scores on the repetitive and re-stricted item scores are no longer included in the total score. The original algorithm cutoffs were 10 for autism and 7 for autism spectrum; the re-vised algorithm is 9 for autism and 7 for autism spectrum.
Autism Diagnostic Interview, Revised
The Autism Diagnostic Interview (ADI; Le Couteur et al., 1989) is a stan-dardized, semi-structured caregiver interview that was designed to aid in the assessment of a range of behaviors consistent with diagnoses of perva-sive developmental disorders. The Autism Diagnostic Interview – Revised (ADI-R; Lord, Rutter, and Le Couteur, 1994) was published in 1994. Compared to the ADI, the ADI-R is shorter, has modified items, and is in-tended for use with a younger population. The ADI-R can be used to assess children with a mental age of at least 18 months as opposed to the ADI, for which individuals had to be at least 5 years old to be assessed. The ADI-R consists of five sections. The sections include questions that evaluate con-cerns, communication skills, social development and play, repetitive and restricted behaviors, and general behavior problems. These topics address both current and previous functioning. There are three separate diagnostic algorithms that can be used to attain a diagnosis: lifetime, current behavior, and children under the age of 4 years. The ADI-R requires between 1.5 and 2.5 hours to administer. Examiners need to have thorough knowledge of the exact administration and scoring procedures. A higher degree of train-ing and experience with ASD is required for competent interpretation of test results. DVD training in the ADI-R is recommended.
SUMMARY
In conclusion, the process of diagnosing ASD is complex and changed significantly with the publication of the DSM-5. The new criteria require that an individual has impairment across three symptom areas in social

SummARy 29
communication and the presence of restricted, repetitive behavior, as ev-idenced by two or more symptom characteristics. The symptoms must have emerged during the early developmental period and, taken together, must represent a clinically significant challenge to the individual’s ability to function in daily life. DSM-5 criteria include specifiers that rate the se-verity of symptoms on a scale from level 1 to level 3, with 3 being most se-vere. It is also worth noting that challenging behaviors, such as tantrums, aggression, and property destruction, are still not part of the ASD diagno-sis, despite the fact that they are common in the ASD population. This fact reflects the position that the vast majority of these challenging behaviors in individuals with ASD are learned behaviors that result from deficits in communication, not core ASD symptoms in and of themselves. Finally, the diagnostic process is something with which most applied behavior analytic service providers are unfamiliar. A greater familiarity with the process will likely give treatment providers a richer source of informa-tion about their learner’s history and functioning level, thereby providing opportunities for customizing treatment programs to a greater degree.