Embed Size (px)
Citation preview

Presented by Dr. Raymond Chu at
Idaho Optometric Physicians Annual Congress 2016
Evidence-based myopia
management, what
works and what doesn’t
DISCLOSURE STATEMENT
I certify:
I have no proprietary interest in the tested
product
I have no equity interest or significant
payments by the sponsor of a covered study
Lecture content and format is free from
commercial bias
Lecture content was independently prepared
by myself
Arch Ophthalmol.
2009;127(12):1632-1639 2523 children in grades 1 to 8 (age 5-17 years)
White (n=1035)
African American (n=534)
Asian (n=491)
Hispanic (n=463)
Overall
Myopia (≥ 0.75 D)
4.4% 6.6% 18.5% 13.2% 9.2%
Hyperopia (≥ 1.25 D)
19.3% 6.4% 6.3% 12.7% 12.8%
Astigmatism (≥ 1.00D)
26.4% 20.0% 33.6% 36.9% 28.4%
Arch Ophthalmol. 2003; 121(8):1141-7.
Atropine in the Treatment
of Myopia Study (ATOM)
RATIONALE
Animal studies
myopia retardation is
independent of
accommodative effect
STUDY DESIGN
Randomized, placebo-controlled trial
400 children 6-12 years
-1.00 to -6.00D
1% atropine / placebo drops to 1 eye
1° outcome: Cycloplegic autorefraction
Opthalmol 2006;113(12): 2285-2291

Presented by Dr. Raymond Chu at
Idaho Optometric Physicians Annual Congress 2016
RESULTS
1 year (n=359)
Placebo eyes = -0.76 D ± 0.44 D
Atropine eyes = +0.30 D ± 0.50 D
2 years (n=346)
Placebo eyes = -1.20 D ± 0.69 D
Atropine eyes = -0.25 D ± 0.92 D
Opthalmol 2006;113(12): 2285-2291 Opthalmol 2006;113(12): 2285-2291
1 year after cessation
1.14 ± 0.80
0.38 ± 0.39 D
1 year after cessation
Atropine
treated eye
Atropine
untreated eye
Initial amps 13.76 ± 3.45 13.86 ± 3.58
3 yr amps 14.64 ± 2.56 15.22 ± 2.63
Initial near
VA
0.50 ± 0.11 0.50 ± 0.11
3 yr near VA 0.38 ± 0.06 0.38 ± 0.06
ATOM 2
Three concentrations of atropine eye drops to
be applied once nightly in both eyes:
0.5% atropine (n=161)
0.1% atropine (n=155)
0.01% atropine (n=84)
Ophthalmology 2012;119:347–354

Presented by Dr. Raymond Chu at
Idaho Optometric Physicians Annual Congress 2016
0.01%: -0.43 (0.52)
0.1%: -0.31 (0.50)
0.5%: -0.17 (0.47)
0.01%: -0.49 (0.63)
0.1%: -0.38 (0.60)
0.5%: -0.30 (0.60)
Atropine
0.01%
Atropine
0.1%
Atropine
0.5%
P value
Spherical Equivalent
∆ over 1
yr
-0.43
(0.52)
-0.31
(0.50)
-0.17
(0.47)
<0.001
∆ over 2
yrs
-0.49
(0.63)
-0.38
(0.60)
-0.30
(0.60)
0.07
Axial Length
∆ over 1
yr
0.24 (0.19) 0.13 (0.18) 0.11 (0.17) <0.001
∆ over 2
yrs
0.41 (0.32) 0.28 (0.27) 0.27 (0.25) 0.002
Atropine
0.01%
Atropine
0.1%
Atropine
0.5%
P value
Mesopic pupil size (mm)
∆ over 1
yr
1.15 (0.78) 2.77 (1.03) 3.50 (1.05) <0.001
∆ over 2
yrs
1.15 (0.71) 2.71 (1.12) 3.56 (1.14) <0.001
Near vision (logMAR)
∆ over 1
yr
-0.01
(0.10)
0.10 (0.16) 0.32 (0.19) <0.001
∆ over 2
yrs
-0.02
(0.08)
0.06 (0.13) 0.25 (0.19) <0.001
Am J Ophthalmol 2014;157:451–457
Ophthalmology 2016; 123:391-399 Near
Viewing
Accommodative Lag Axial Elongation
Blur is a critical component
in development of myopia
IOVS 1993; 34(3): 690-694
Presented by Dr. Raymond Chu at
Idaho Optometric Physicians Annual Congress 2016
Near
Viewing
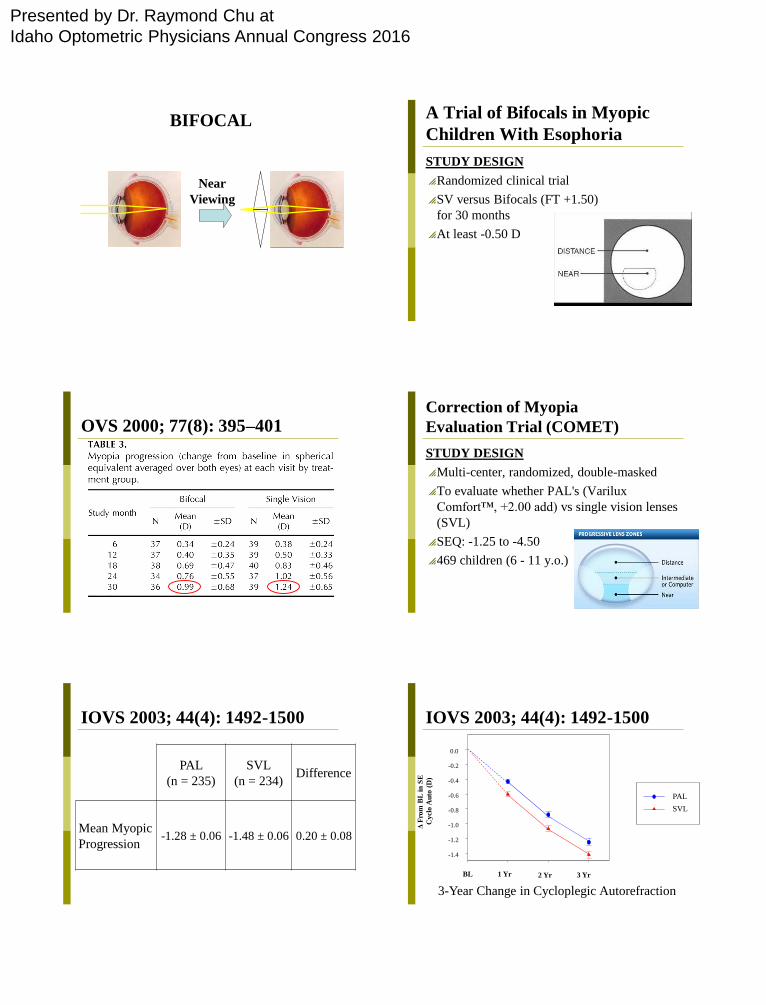
BIFOCAL
STUDY DESIGN
Randomized clinical trial
SV versus Bifocals (FT +1.50)
for 30 months
At least -0.50 D
A Trial of Bifocals in Myopic
Children With Esophoria
OVS 2000; 77(8): 395–401 Correction of Myopia
Evaluation Trial (COMET)
STUDY DESIGN
Multi-center, randomized, double-masked
To evaluate whether PAL's (Varilux
Comfort™, +2.00 add) vs single vision lenses
(SVL)
SEQ: -1.25 to -4.50
469 children (6 - 11 y.o.)
PAL
(n = 235)
SVL
(n = 234) Difference
Mean Myopic
Progression -1.28 ± 0.06 -1.48 ± 0.06 0.20 ± 0.08
IOVS 2003; 44(4): 1492-1500
PAL
SVL
-1.4
-1.2
-1.0
-0.8
-0.6
-0.4
-0.2
0.0
Δ F
rom
BL
in
SE
Cy
clo
Au
to (
D)
1 Yr 2 Yr 3 Yr BL
3-Year Change in Cycloplegic Autorefraction
IOVS 2003; 44(4): 1492-1500

Presented by Dr. Raymond Chu at
Idaho Optometric Physicians Annual Congress 2016
PAL SVL Difference
≥0.43D Lag
& Eso -1.08 (n=42) -1.72 (n=34) 0.64
≥0.43D Lag
& ≤-2.25D -1.11 (n=44) -1.59 (n=60) 0.48
≥0.43D Lag
& <31.2 cm -1.24 (n=64) -1.68 (n=52) 0.44
IOVS 2003; 44(4): 1492-1500 COMET 2
To evaluate whether PAL's (Varilux
Comfort™, +2.00 addition) slow the rate of
myopic progression in children with near-point
eso, a lag of accommodation, and low amounts
of myopia vs single vision lenses (SVL)
IOVS. 2011 Apr 25;52(5):2749-5
-0.29
-0.58
-0.87 -0.42
-0.80
-1.15
Contact Lens and Myopia
Progression Study (CLAMP)
Rationale
Previous studies have suggested that RGP’s
may slow the progression of myopia in
children
STUDY DESIGN
Run-in period before randomization
RGP’s versus soft contact lenses
Children 8-11 yrs
-0.75 to -4.00 SEQ
No previous CL wear
Arch Ophthalmol 2004;
122(12):1760-66
Arch Ophthalmol 2004;
122(12):1760-66
0.81

Presented by Dr. Raymond Chu at
Idaho Optometric Physicians Annual Congress 2016
Arch Ophthalmol 2004;
122(12):1760-66
Arch Ophthalmol 2004;
122(12):1760-66
Conclusions
RGP lenses are a viable choice for refractive
correction in patients 8 to 11 years of age
(CLAMP: 78.6% of subjects)
A portion of the treatment effect is likely to be
temporary and due to corneal flattening
Children’s Overnight
Orthokeratology Investigation
GOAL
To examine the safety and effectiveness orthokeratology lens in children
STUDY DESIGN
A prospective case series
Children 8-11 yrs
-0.75 to -5.00 SEQ
No RGP use
OVS 2004; 81(6): 407–413
OVS 2004; 81(6): 407–413
Visit High Contrast
(Mean ±SD)
Baseline 0.67 ± 0.22 (20/94)
1 Day 0.50 ± 0.22 (20/63)
1 Week 0.28 ± 0.21 (20/38)
2 Weeks 0.16 ± 0.21 (20/29)
1 Month 0.14 ± 0.15 (20/28)
3 Months 0.14 ± 0.22 (20/28)
6 Months 0.08 ± 0.15 (20/24)
OVS 2004; 81(6): 407–413
CONCLUSION
Mean reduction: -2.48 ± 1.57 D (98%)
~2 weeks of wear, subjects were able to see
clearly throughout the entire day
~1 month of wear, some were able to wear
every other night
~3/5 of the subjects had corneal staining

Presented by Dr. Raymond Chu at
Idaho Optometric Physicians Annual Congress 2016
CRAYON Pilot Study
8 to 11 years old
Between -0.75 D and -4.00 D
Primary outcome: difference in the 2-year
change in axial length
Compared to a control group randomized to
soft CL
Br J Ophthalmol 2009; 93:1181–1185.
Eye growth
is slowed
by 55%
STUDY DESIGN
Prospective Case-Controlled Trial
35 children 7-12 years
SEQ: -0.25 to -4.50D (< 2.00 DC)
1° outcome: Axial Length
Longitudinal Orthokeratology
Research in Children (LORIC) Curr Eye Res 2005; 30(1):71–80
Control Ortho-K
AL Change
(p value:<0.001) 0.54 ± 0.27 0.29 ± 0.27
RE Change −1.20 ± 0.61 2.09 ± 1.34
Curr Eye Res 2005; 30(1):71–80
CONCLUSION
Ortho-k may have both a
corrective and
preventive/control effect in
childhood myopia.
Retardation of Myopia in
Orthokeratology (ROMIO) Study
Single-masked randomized clinical trial
(Ortho-k lenses or SV glasses)
Ages from 6 to 10 years
Between -0.50 and -4.00 diopters

Presented by Dr. Raymond Chu at
Idaho Optometric Physicians Annual Congress 2016
IOVS 2012;53:7077–7085 IOVS 2012;53:7077–7085
Optom Vis Sci 2013;90:530-539
partial reduction ortho-k and spectacles for residual refractive
errors in the daytime
Bifocal Contact Lens
Based on a case report involving
identical twins
Clin Exp Optom 2008; 91(4):
394–399
Baseline Year 1 Year 2
Twin A
BFL/BFL
-1.50
-1.50-0.25 x 110
-1.25 -0.25 x 160
-1.50 DS
-1.75 -0.50 x 165
-1.50 DS
Twin B
SVL/BFL
-1.25 -0.25 x 085
-1.50
-2.50 DS
-2.75 DS
-1.75 -0.50 x 162
-2.00 -0.50 x 012
DIMENZ
STUDY DESIGN
RCT 20-month clinical trial
with crossover
One eye bifocal SCL and
SV contact lens on other
eye for 10 months
Lens assignment swapped
between eyes from 11-20
months

Presented by Dr. Raymond Chu at
Idaho Optometric Physicians Annual Congress 2016
DIMENZ
11–14 years old
-1.25 to -4.50 on non-cycloplegic subjective
refraction
myopia progression ≥ 0.50 D in the previous
12 months
1o outcome: cycloplegic autorefraction
Ophthalmology 2011;118:
1152–1161
With SVD With DF
lens
Difference
Period 1: Baseline to 10 months
Change in
refraction
-0.69 ± 0.38 -0.44 ± 0.33 0.25 ± 0.27
Period 2: Crossover to 20 months
Change in
refraction
-0.38 ± 0.38 -0.17 ± 0.35 0.20 ±0.34
Contact Lens Designed to Reduce
Relative Peripheral Hyperopia
Chinese children, aged 7 to 14 years, with
baseline myopia from sphere −0.75 to −3.50 D
Silicone hydrogel lens with a central zone that
corrected for the refractive error of the eye
Outside the central zone, the refracting power
of the lens increased progressively to +2.00 D
at the edge of the peripheral treatment zone
Relative peripheral refractive
error profile
IOVS 2011;52: 9362–9367 Multifocal Contact Lens Myopia Control
8 to 11 years old
Between -1.00 D and -6.00D
Fit with Proclear Multifocal with the distance
center design in both eyes and a +2.00 D add

Presented by Dr. Raymond Chu at
Idaho Optometric Physicians Annual Congress 2016
Optometry and Vision Science,
Vol. 90, No. 11, November 2013
Multifocal (n) Single Vision (n)
Baseline -2.24 ± 0.06 (32) -2.26 ± 0.06 (32)
Year 1 -2.57 ± 0.06 (32) -2.86 ± 0.06 (32)
Year 2 -2.75 ± 0.06 (27) -3.28 ± 0.06 (27)
2-year change -0.51 ± 0.06 -1.03 ± 0.06
(p<0.0001)
Optometry and Vision Science,
Vol. 90, No. 11, November 2013
Slowed the growth of
the eye by ~29%