Embed Size (px)
Citation preview
Evidence-based Medicine

Case Presentation
• 27 yo AA male presents to clinic with 3 days of pain and swelling in right leg
• First noted several spider bites on his leg – concerned they may be infected now
• Denies fever, chills, nausea, or other symptoms

Case Presentation
• PMH: HTN
• Meds: HCTZ, Adalat
• Allergies: NKDA
• Social: AD PO2 on shore duty at NI. Lives in Chula Vista with his wife.
• No recent antibiotics or hospital contacts

PE
• Vitals: BP - 132/82 P - 64 T - 98.1
• Gen: AAOX3, Appears well
• CV/Pulm: Unremarkable
• Right LE: Small, open pustule with surrounding edema, erythema. Scant thick, white discharge from lesion.
Diagnosis
• Uncomplicated cellulitis

Question
• What antibiotic is appropriate for uncomplicated cellulitis in an outpatient without risk factors for MRSA?

Choices…
• A) Any cephalosporin• B) vancomycin• C) linezolid• D) TMP-SMX• E) clindamycin• F) a fluoroquinolone• G) a tetracycline• H) An antistaphylococcal
PCN• I) Combination therapy
What bug is targeted?
a) MSSA
b) Streptococcus
c) MRSA
d) Pseudomonas
Is MRSA a concern?
• Emergence of CA-MRSA USA300 Clone as the Predominant Cause of Skin and Soft-Tissue Infections
• King, et al. Annals of Internal Medicine, 7 March 2006.

Background
• CA-MRSA known to be pathogen in select populations (prisons, military recruits)
• Is this an important community pathogen?

Methods
• Prospective study at single public inner-city hospital (Atlanta, GA) over 3.5 months in 2003.
• Retrospective review of records for all pts with S. aureus culture for HIV status, ESRD, hospitalization within 12 months, hx of MRSA, and cx within 72 hours of admission
• Reviewer was blinded to type of S. aureus infection

Genetic Analysis
• Pulse-field gel electrophoresis on most samples – compared to CDC samples
• Assessed for Panton-Valentine leukocidin gene by PCR


Statistical Analysis
• Univariate analysis of potential risk factors in MRSA USA 300/400 vs MSSA and MRSA USA 300/400 vs MRSA other.
• Then multivariate analysis of potential risk factors

Univariate Results

Multivariate Results

Discussion
• 72% of all S. aureus infections were caused by MRSA
• USA 300/400 clone accounted for 87% of ca-MRSA infections

Author’s conclusions
• MRSA coverage is essential to empiric coverage of skin and soft tissue infections
• I&D alone may be sufficient, but poor data
• USA 300 clone is usually sensitive to TMP-SMX, linezolid, tetracycline
• May have inducible clindamycin resistance

Study Weakness
• Only examined culture positive S. aureus infections, not all soft tissue infections
• All data from one hospital
• No evaluation of treatment
Surviving the New Killer Bug
• From Time Magazine; 26 June 2006
• “This is not bird flu or SARS or even the "flesh-eating bacteria" of tabloid fame. But it is every bit as dangerous, even if it goes by an uncommonly ungainly name: community-acquired methicillin-resistant Staphylococcus aureus (MRSA). Never heard of it? Neither have most doctors.”


CA-MRSA
• Typically USA 300 or USA 400 clone
• Normal resistance pattern includes resistance only to β-lactams and erythromycin
• Occasional resistance to levofloxacin, clindamycin, rifampin, and gentamycin
• Contains Panton-Valentine leukocidin gene (pvl) and SCCmec type IV gene
Panton-Valentine leukocidin gene
• Thought to be one of the major virulence factors for CA-MRSA
• Causes leukocyte destruction and tissue necrosis

Nosocomial MRSA
• Usually MDR
• Does not contain Panton-Valentine leukocidin gene

Is this applicable to our population?
• MRSA Infections among Patients in the Emergency Department
• Moran, et al. NEJM – 17 August 2006
Methods
• Prospective prevalence study
• Enrolled patients in 11 ERs with acute, purulent skin infections in August 2004
• Isolates typed with PFGE and PCR
Results
• S. aureus isolated in 76% of patients
• MRSA isolated in 59% of patients (78% of S. aureus cultures)
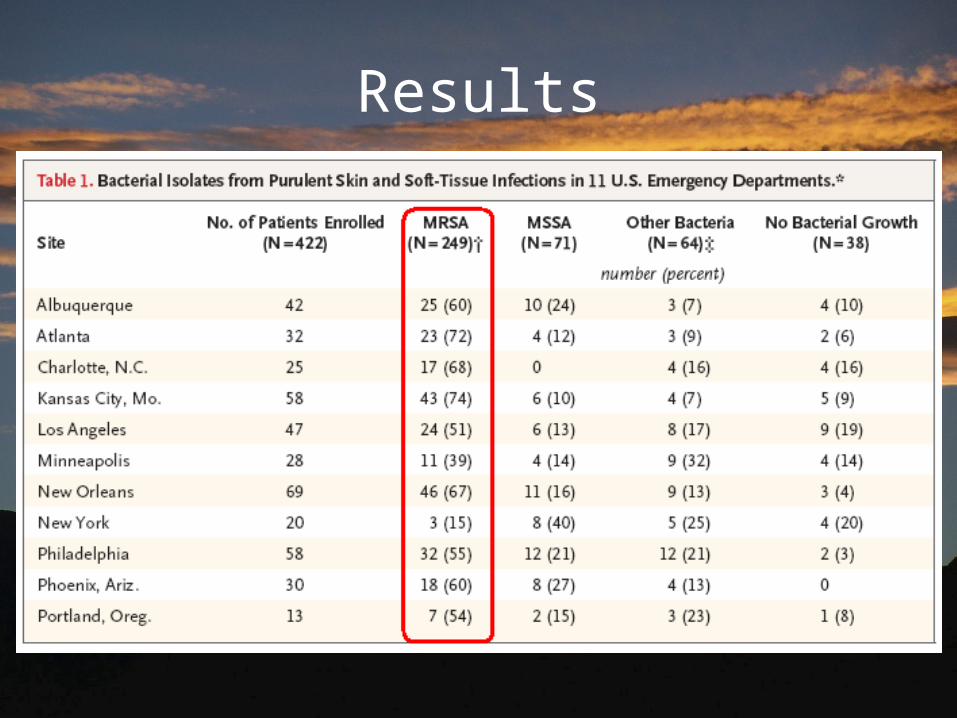
Results

Discussion
• 97% of MRSA was a USA 300 strain
• Susceptibilities: 100% TMP-SMX and rifampin; 95% clindamycin; 92% tetracycline
• Infectious organism resistant to antibiotic prescribed in 57% of patients (most common antibiotic was a β-lactam)
Discussion
• 59% of patients contacted for follow-up
• 96% of these patients reported the infection resolved or improved
• No association between antibiotic used and outcome in limited follow-up

Discussion
• 99% of MRSA had PFGE consistent with CA-MRSA, although 25% had risk factors for health-care associated MRSA

Study Weakness
• Poor follow-up – study not designed for treatment arm
• Only included purulent infections
• Only enrolled 42% of eligible patients

Question?
• What antibiotic is appropriate for uncomplicated cellulitis in an outpatient without risk factors for MRSA?


My Thoughts
• Treatment of any abscess requires drainage first
• Culture should always be performed on purulent infections
• Antibiotic coverage must include, at minimum, coverage for MRSA, MSSA, and group A streptococcus

My Thoughts
• A) Any cephalosporin – Will miss MRSA• B) vancomycin – Not appropriate for outpatient• C) linezolid – Very expensive; may induce resistance• D) TMP-SMX – Will likely miss streptococcus• E) clindamycin – May miss MRSA (inducible resistance)• F) A fluoroquinolone – Will miss MRSA, +/- vs strep• G) A tetracycline – Good coverage if tolerated• H) Antistaphylococcal PCN – Will miss MRSA• I) Combination therapy – More difficult, less compliance

My Thoughts
• Combination of TMP-SMX plus β-lactam until sensitivity results are available is appropriate empiric coverage
• Single coverage with a tetracycline is also appropriate
• Clindamycin not recommended as single therapy unless a “D-test” is performed

My Patient
• No culture performed
• Treated with clindamycin with full resolution of symptoms

Questions?
Sources• Fridkin, Scott, et al. MRSA Disease in Three Communities. NEJM
352;14• Graham, Philip, et al. A US Population-Based Survey of S. aureus
Colonization. Annals of Internal Medicine. 7MAR2006; 144:318-325• Grayson, M. The Treatment Triangle for Staphylococcal Infections.
NEJM; 355:724-726• King, Mark, et al. Emergence of CA-MRSA USA300 Clone as the
Predominant Cause of Skin and Soft-Tissue Infections. Annals of Internal Medicine. 7MAR2006; 144:309-317
• Moellering, Robert. The Growing Menace of CA-MRSA. Annals of Internal Medicine. 7MAR2006; 144:368-369
• Moran, G.J, et al. MRSA Infections among Patients in the Emergency Department. NEJM 355;7
• Pictures from: http://www.kcom.edu/faculty/chamberlain/