Embed Size (px)
Citation preview

EVIDENCE BASED HEALTH EVIDENCE BASED HEALTH CARE CARE
and BEST PRACTICES at and BEST PRACTICES at Northwestern Health Northwestern Health Sciences UniversitySciences University
Gert Bronfort DC, PhD; Gert Bronfort DC, PhD; Michele Maiers, DC, MPHMichele Maiers, DC, MPH; Roni Evans DC, ; Roni Evans DC, MSMS

Northwestern Health Sciences Northwestern Health Sciences University (NWHSU)University (NWHSU)
Six clinics in Twin Cities areaSix clinics in Twin Cities area Conservative health care services, Conservative health care services,
including including – chiropractic chiropractic – acupuncture/ Oriental medicine acupuncture/ Oriental medicine – massage therapy massage therapy – healing touch healing touch – naturopathy naturopathy
Teaching clinics for upper term studentsTeaching clinics for upper term students

Best Practices at NWHSU:Best Practices at NWHSU:Precipitating EventsPrecipitating Events
Council on Chiropractic Guidelines Council on Chiropractic Guidelines and Practice Parametersand Practice Parameters
MN State Legislative InitiativeMN State Legislative Initiative NWHSUNWHSU
– MissionMission– Guiding principles and valuesGuiding principles and values– Strategic goalsStrategic goals

Our MissionOur MissionTo advance and promote natural approaches to To advance and promote natural approaches to
health through education, research, clinical health through education, research, clinical services and community involvementservices and community involvement
Best Practices affect our ability to fulfill our Best Practices affect our ability to fulfill our missionmission
EducationEducation: providing students with the tools : providing students with the tools they need to be effective and competitive they need to be effective and competitive providersproviders
ResearchResearch: accurately documenting clinical : accurately documenting clinical practicepractice
Clinical ServicesClinical Services: optimizing patient care : optimizing patient care Community InvolvementCommunity Involvement: providing consistent : providing consistent
message of our standards of care and our message of our standards of care and our effectivenesseffectiveness

Several advantages Several advantages for our providers:for our providers:
Easier Easier access to researchaccess to research pertinent pertinent to their practice to their practice
An An opportunity to evaluate opportunity to evaluate themselvesthemselves before others do before others do
The ability to change and The ability to change and improve improve their systems of caretheir systems of care
Provide Provide standardized documentationstandardized documentation of effectivenessof effectiveness

Several advantages Several advantages to our stake-holders:to our stake-holders:
Evaluation system based on Evaluation system based on accurate accurate analysis of clinical outcomesanalysis of clinical outcomes– Internal assessmentInternal assessment
– Patients can see progress over timePatients can see progress over time
Provides the ability for standardized Provides the ability for standardized documentation of the effectivenessdocumentation of the effectiveness of our providers’ interventionsof our providers’ interventions
Standards of care = consistent public Standards of care = consistent public message about chiropracticmessage about chiropractic

Best Practices Pilot ProjectBest Practices Pilot Project
Specific Aims:Specific Aims: To optimize the quality of To optimize the quality of diagnosis and therapeutic diagnosis and therapeutic management of patients through: management of patients through:
application of evidence-based health application of evidence-based health carecare
within the context of a quality within the context of a quality assurance systemassurance system
……in the NWHSU clinic systemin the NWHSU clinic system

Implementation: Implementation: Effective Transfer StrategiesEffective Transfer Strategies
Educational outreach visitsEducational outreach visits– trained personnel visit providers in their practice
settings - information / support Interactive educational sessionsInteractive educational sessions
– health care providers participating in interactive, problem-based learning sessions (adult learning principles)
Decision support and reminder systemsDecision support and reminder systems – automated or manual prompts to perform clinical
tasks Multifaceted interventionsMultifaceted interventions
– any combination of audit & feedback, reminders, local consensus processes, or marketing
Bero et al (1998); Davis et al (1995); Freemantle et al (1998)Bero et al (1998); Davis et al (1995); Freemantle et al (1998)

Outline of Pilot ProjectOutline of Pilot Project
Assessment of Clinical EnvironmentAssessment of Clinical Environment Development of Quality Assurance Development of Quality Assurance
SystemSystem ImplementationImplementation Evaluation of Pilot ProjectEvaluation of Pilot Project

Assess Clinic EnvironmentAssess Clinic Environment
Choose pilot sites and providersChoose pilot sites and providers Identify representative clinicians to Identify representative clinicians to
serve on project teamserve on project team Survey current practice behaviorsSurvey current practice behaviors
– Case vignettes (exam, imaging, Case vignettes (exam, imaging, treatment)treatment)
– Record keepingRecord keeping– Use of guidelines, outcome measuresUse of guidelines, outcome measures

Interactive Workshop IInteractive Workshop I Teach the concepts of Best Practices Teach the concepts of Best Practices
and Quality Assuranceand Quality Assurance Outline/ timeline for pilot projectOutline/ timeline for pilot project Present and discuss of results of Present and discuss of results of
practice behavior surveypractice behavior survey Identify facilitating factors for Identify facilitating factors for
implementation implementation Identify barriers against Identify barriers against
implementationimplementation

Development of QA SystemDevelopment of QA System Select clinical indicatorsSelect clinical indicators
– structure, process, outcome (Kristensen 2001)structure, process, outcome (Kristensen 2001) Select standards for clinical indicatorsSelect standards for clinical indicators
– Research evidenceResearch evidence– Consensus by participantsConsensus by participants
Develop specific elementsDevelop specific elements– Integrate access to information within QA systemIntegrate access to information within QA system– Finalize content of QA databaseFinalize content of QA database– Develop data collection protocolsDevelop data collection protocols– Develop test electronic patient record systemDevelop test electronic patient record system– Develop centrally located database for all clinicsDevelop centrally located database for all clinics

Quality DatabaseQuality Database
Electronic Patient RecordElectronic Patient Record– Standardized documentation Standardized documentation – Prompts to ensure complete data collectionPrompts to ensure complete data collection– Link to resourcesLink to resources
Centralized databaseCentralized database– Collection of quality indicatorsCollection of quality indicators– Compare actual outcomes to standardsCompare actual outcomes to standards
Access for clinicians, researchers, administratorsAccess for clinicians, researchers, administrators

Interactive Workshop IIInteractive Workshop II
Select quality indicators and standardsSelect quality indicators and standards– Participant driven (rank consensus)Participant driven (rank consensus)– Minimal set of data to be included in QA databaseMinimal set of data to be included in QA database
Introduce EPRIntroduce EPR Electronic access to best practices Electronic access to best practices
documentsdocuments– Updated internet web-sitesUpdated internet web-sites
hyper-links to additional information, reference hyper-links to additional information, reference materials, guidelinesmaterials, guidelines
– ““Bedside” with use of tablet PCs, etc.Bedside” with use of tablet PCs, etc. Problem solve perceived barriersProblem solve perceived barriers

ImplementationImplementation
Identify implementation strategies Identify implementation strategies – Minimize staff, provider and patient Minimize staff, provider and patient
burdenburden– Maximize efficiencyMaximize efficiency
Train clinicians to use Best Practices Train clinicians to use Best Practices and QA systemand QA system– Case study vignettesCase study vignettes– Data collection processesData collection processes– On-site visitsOn-site visits

Implementation: Implementation: How would this look in How would this look in
practice?practice?Initial PresentationInitial Presentation Patient presents to NWHSU ClinicPatient presents to NWHSU Clinic
– Completes intake formsCompletes intake forms Standardized questions, entered into data Standardized questions, entered into data
collection system for QA purposescollection system for QA purposes– Clinician performs history, exam, treatmentClinician performs history, exam, treatment
Clinician has access to best practice Clinician has access to best practice informationinformation
– may inform choices of exam procedures, may inform choices of exam procedures, imaging, treatmentimaging, treatment
Exam, treatment decisions entered into data Exam, treatment decisions entered into data collection system for QA purposescollection system for QA purposes

Implementation:Implementation:How would this look in How would this look in
practice?practice?Follow-up visitsFollow-up visits Patient returns to clinic for next Patient returns to clinic for next
appointment(s)appointment(s)– Completes follow-up questionnaire, entered into Completes follow-up questionnaire, entered into
data collection system for QA purposesdata collection system for QA purposes– Clinician manages case as usualClinician manages case as usual
Subsequent exam, treatment decisions entered Subsequent exam, treatment decisions entered into data collection system for QA purposesinto data collection system for QA purposes
Established benchmarks and Best Practice Established benchmarks and Best Practice recommendations help clinician make decisions recommendations help clinician make decisions for subsequent treatment plan, care for subsequent treatment plan, care
Questionnaire mailed to patientQuestionnaire mailed to patient– Sent back to clinic, entered into data collection Sent back to clinic, entered into data collection
systemsystem

Evaluation of Pilot ProjectEvaluation of Pilot Project
Compliance assessmentCompliance assessment Best practices utilizationBest practices utilization Results of 3 months follow up of careResults of 3 months follow up of care Assess clinicians’ experiencesAssess clinicians’ experiences Determine overall feasibilityDetermine overall feasibility Report to NWHSU Office of Report to NWHSU Office of
Institutional EffectivenessInstitutional Effectiveness

Results: Results: Assessment of Clinical Assessment of Clinical
EnvironmentEnvironment Who: 12 clinicians Who: 12 clinicians Where: 2 multidisciplinary NWHSU Where: 2 multidisciplinary NWHSU
clinicsclinics What: Each clinician follows 5 What: Each clinician follows 5
consecutive LBP patients for 3 monthsconsecutive LBP patients for 3 months How: Outcomes tracked in centralized How: Outcomes tracked in centralized
database with quality indicatorsdatabase with quality indicators

Results: Develop Quality Results: Develop Quality Assurance Selection of Quality Assurance Selection of Quality
IndicatorsIndicators Timely collection of quality indicator dataTimely collection of quality indicator data Diagnostic classificationsDiagnostic classifications Patient/ clinic recordsPatient/ clinic records Patient educationPatient education Patient knowledgePatient knowledge Pain severityPain severity DisabilityDisability Global improvementGlobal improvement Patient satisfactionPatient satisfaction Quality of life/ general health statusQuality of life/ general health status

Results: Develop Quality Results: Develop Quality Assurance Selection of Assurance Selection of
StandardsStandards Global improvement (DC or ET for Global improvement (DC or ET for
LBP)LBP)1 month1 month
N=195N=195PercentPercent Cumulative Cumulative
PercentPercent
Completely Completely GoneGone
11 11
Much BetterMuch Better 2121 2222
Moderately Moderately BetterBetter
2727 4949
A Little BetterA Little Better 3333 8282
SameSame 1616 9898
A Little Worse A Little Worse 11 9999
Much WorseMuch Worse 11 100100
3 months3 months
N=192N=192PercentPercent Cumulative Cumulative
PercentPercent
Completely Completely GoneGone
55 55
Much BetterMuch Better 4646 5252
Moderately Moderately BetterBetter
2020 7272
A Little BetterA Little Better 1818 9090
SameSame 77 9797
A Little WorseA Little Worse 1.51.5 98.598.5
Much WorseMuch Worse 1.51.5 100100
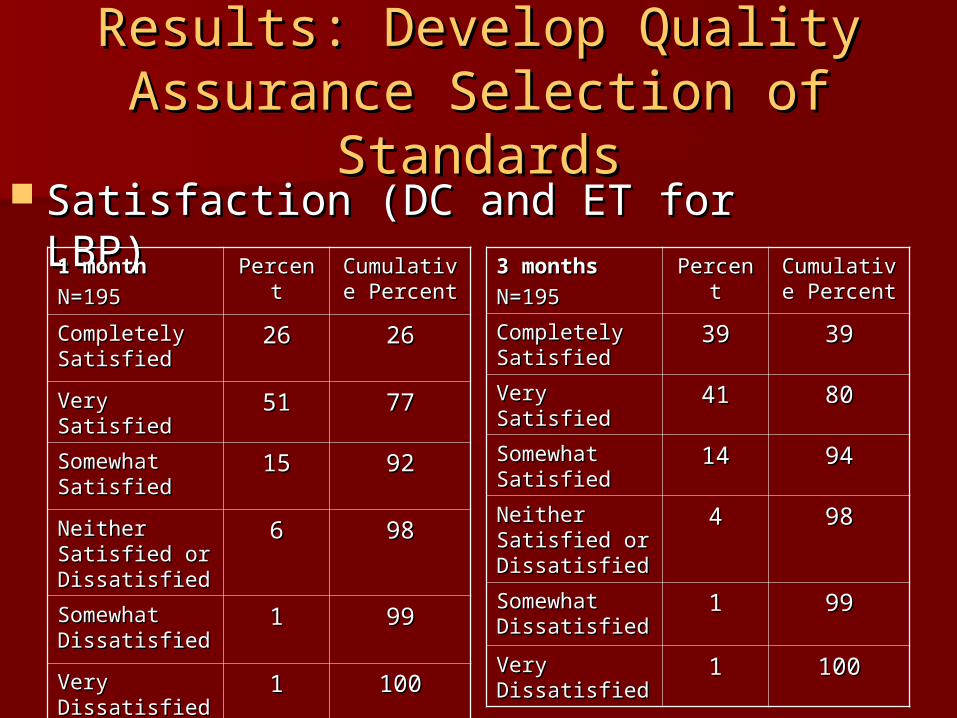
Results: Develop Quality Results: Develop Quality Assurance Selection of Assurance Selection of
StandardsStandards Satisfaction (DC and ET for LBP)Satisfaction (DC and ET for LBP)
1 month1 month
N=195N=195PercentPercent Cumulative Cumulative
PercentPercent
Completely Completely SatisfiedSatisfied
2626 2626
Very SatisfiedVery Satisfied 5151 7777
Somewhat Somewhat SatisfiedSatisfied
1515 9292
Neither Neither Satisfied or Satisfied or DissatisfiedDissatisfied
66 9898
Somewhat Somewhat DissatisfiedDissatisfied
11 9999
Very Very DissatisfiedDissatisfied
11 100100
3 months3 months
N=195N=195PercentPercent Cumulative Cumulative
PercentPercent
Completely Completely SatisfiedSatisfied
3939 3939
Very SatisfiedVery Satisfied 4141 8080
Somewhat Somewhat SatisfiedSatisfied
1414 9494
Neither Neither Satisfied or Satisfied or DissatisfiedDissatisfied
44 9898
Somewhat Somewhat DissatisfiedDissatisfied
11 9999
Very Very DissatisfiedDissatisfied
11 100100

Next StepsNext Steps
Select measurement tools for quality Select measurement tools for quality indicatorsindicators– Established instrumentsEstablished instruments– ConsensusConsensus
Agree to standards for quality Agree to standards for quality indicatorsindicators– Research literature Research literature – Consensus standardsConsensus standards
Choose and implement EPRChoose and implement EPR
Perceived BarriersPerceived Barriers Appropriate allocation of resourcesAppropriate allocation of resources
– FinancialFinancial– Administrative Administrative
Multi-disciplinary settingMulti-disciplinary setting– Access to literatureAccess to literature– EPR and classification system EPR and classification system
Burden (staff, providers, patients)Burden (staff, providers, patients)– Minimal set of quality indicatorsMinimal set of quality indicators– Benefits outweigh burdenBenefits outweigh burden

Educational ImpactEducational Impact
Evidence based curriculum translates Evidence based curriculum translates to clinical experienceto clinical experience
Expose students in controlled Expose students in controlled environment to:environment to:– Electronic patient recordsElectronic patient records– Standardized data collectionStandardized data collection– Pragmatic use of research literaturePragmatic use of research literature
Develop habits for evidence based Develop habits for evidence based practicepractice