Embed Size (px)
Citation preview

Everything a PCP Needs to Know About Lab Testing
(Rheum & Otherwise)
PSVMC MEDICAL GRAND ROUNDSMay 20, 2014
Richard Wernick, M.D.

Testing for Rheumatic Disease:A (PCP) Consumer’s Guide - Outline
• Synovial fluid analysis• RF/a-CCP• ANA/a-DS DNA & a-Smith• ESR/CRP• Temporal artery bx• ANCAs
Testing for Rheumatic Disease:A (PCP) Consumer’s Guide - Outline
• Synovial fluid analysis• RF/a-CCP• ANA/a-DS DNA & a-Smith• ESR/CRP• Temporal artery bx• ANCAs
• Bayes’ for PCPs• Spectrum effect• Reliability

Conflicts of Interest
• Industry• Financial• Personal

A Case of Acute Monoarthritis(File #1141) : “ZZ”
• 50 y/o M rock drummer• 3 d severe pain & swelling left knee• PMH – MI, DM-2, STDs, ETOH, cigs• Meds – simva, metformin, prn oxy/Ambien• PE – tender, warm, swollen knee; obese
Acute Monoarthritis: Differential Diagnosis
Inflammatory• Gout• Pseudogout• Bacterial• (DFKA “Reiter’s”)
Non-inflammatory• Internal
mechanical derangement
• Avascular necrosis• Hemarthrosis• Osteoarthritis

Acute Monoarthritis: Differential Diagnosis
Inflammatory• Gout• Pseudogout• Bacterial• (DFKA “Reiter’s”)
Non-inflammatory• Internal
mechanical derangement
• Avascular necrosis• Hemarthrosis• Osteoarthritis
A Case of Acute Monoarthritis(File #1141) : “ZZ”
• 50 y/o M rock drummer• 3 d severe pain & swelling left knee• PMH – MI, DM-2, STDs, ETOH, cigs• Meds – simva, metformin, prn oxy/Ambien• PE – tender, warm, swollen knee; obese
• Which test(s)? CBC, uric acid, SF, X-ray . . .• Discuss
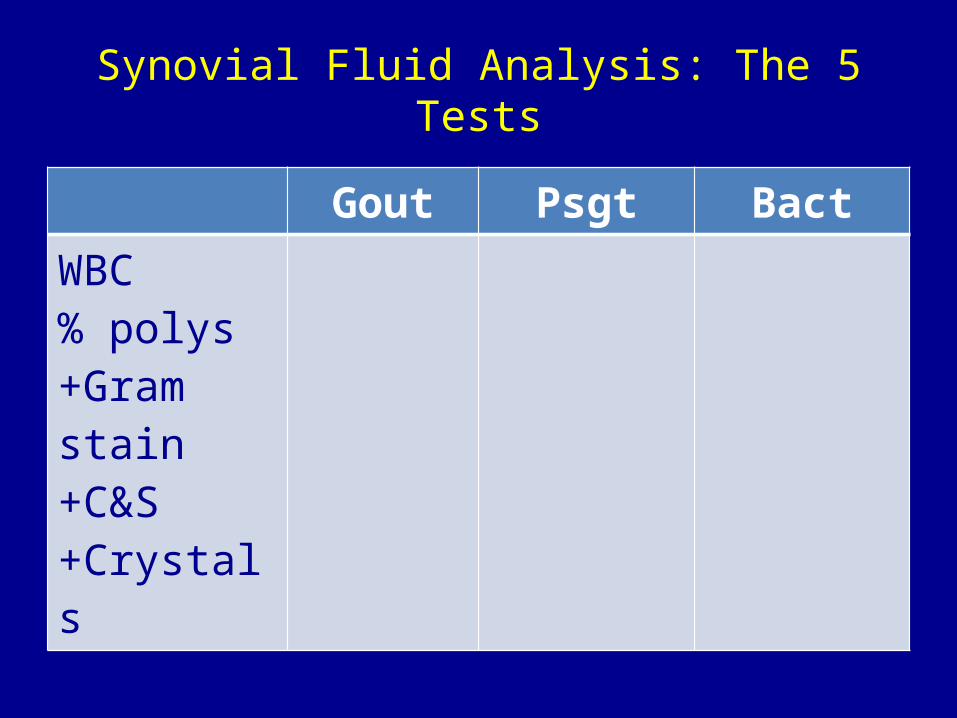
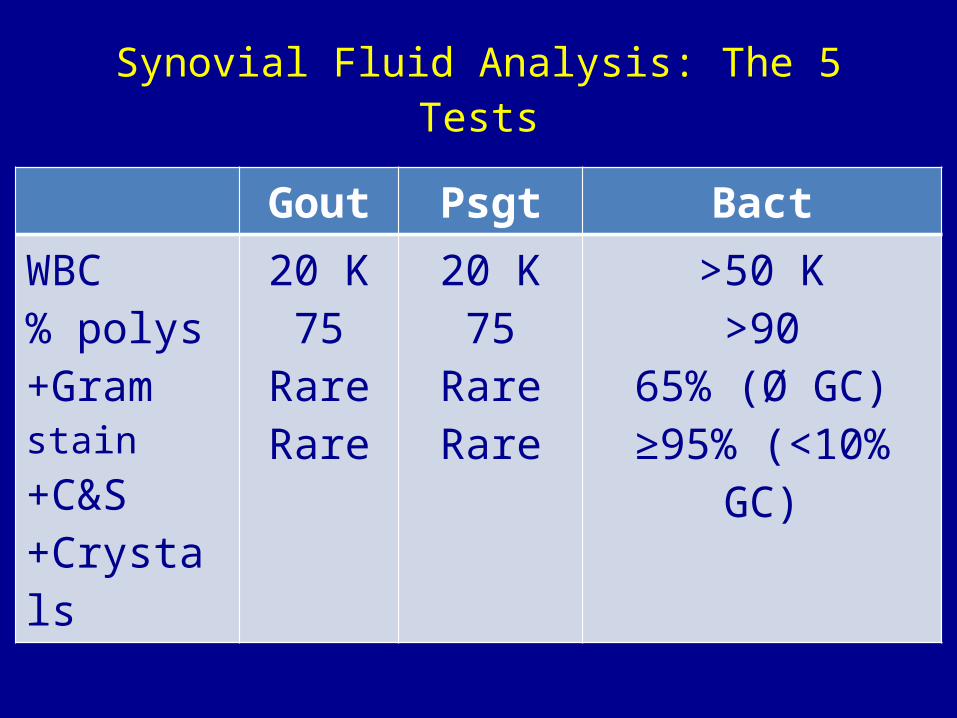
Synovial Fluid Analysis: The 5 Tests
Gout Psgt BactWBC% polys+Gram stain+C&S+Crystals
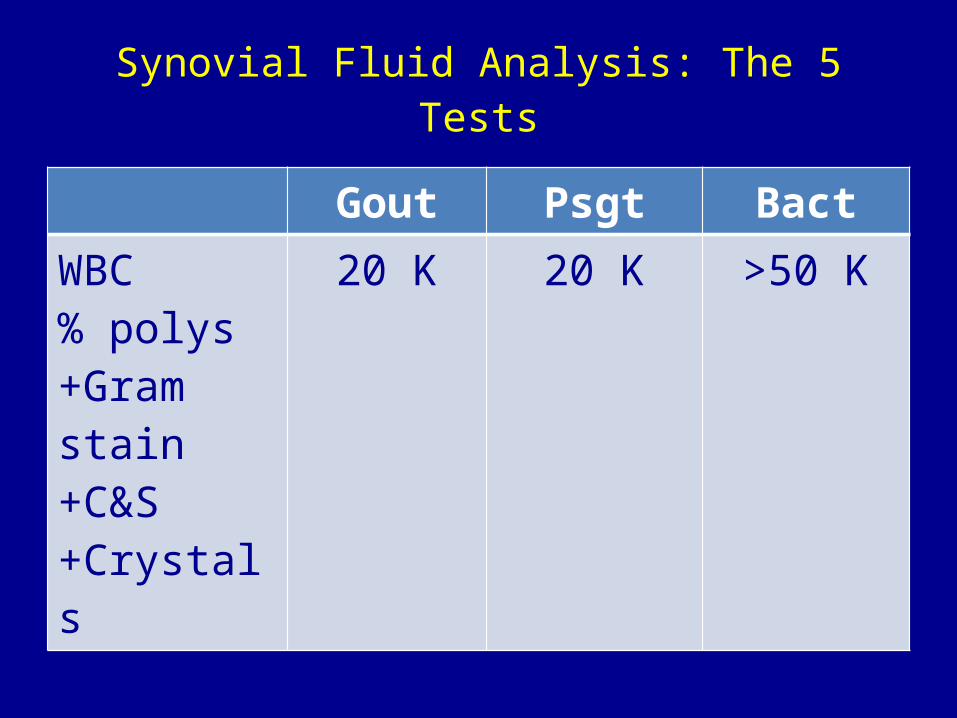
Synovial Fluid Analysis: The 5 Tests
Gout Psgt BactWBC% polys+Gram stain+C&S+Crystals
20 K 20 K >50 K
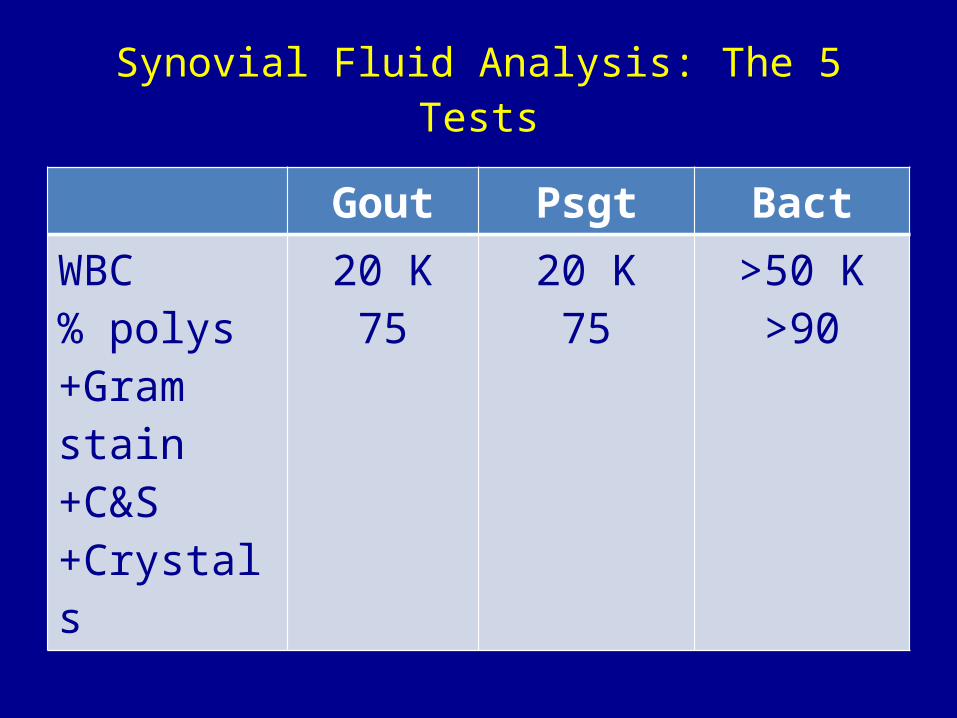
Synovial Fluid Analysis: The 5 Tests
Gout Psgt BactWBC% polys+Gram stain+C&S+Crystals
20 K75
20 K75
>50 K>90
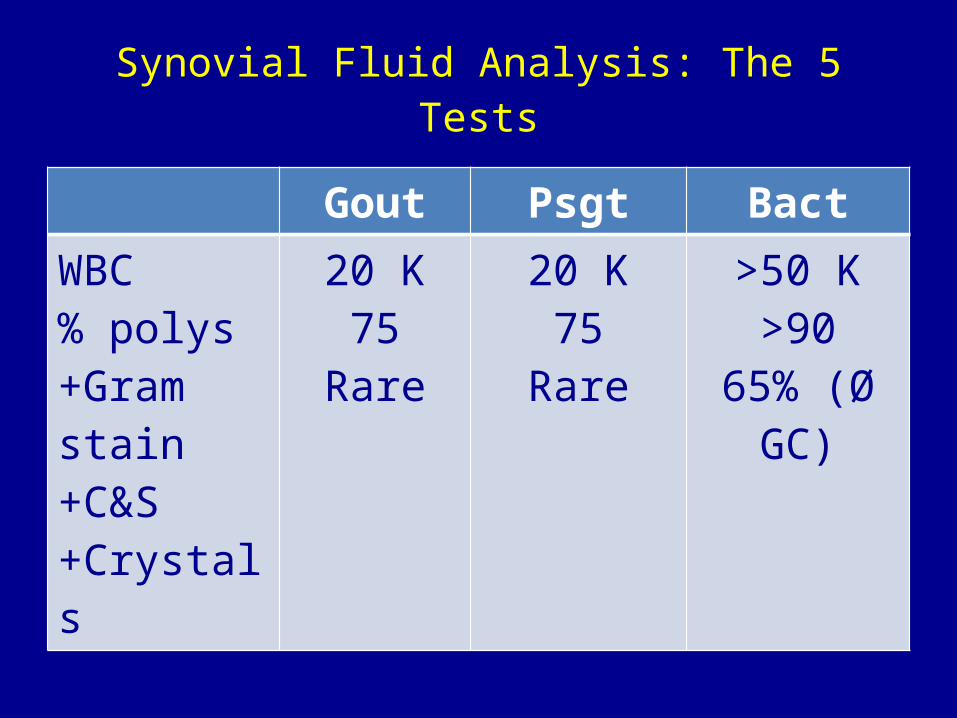
Synovial Fluid Analysis: The 5 Tests
Gout Psgt BactWBC% polys+Gram stain+C&S+Crystals
20 K75
Rare
20 K75
Rare
>50 K>90
65% (Ø GC)
Synovial Fluid Analysis: The 5 Tests
Gout Psgt BactWBC% polys+Gram stain+C&S+Crystals
20 K75
RareRare
20 K75
RareRare
>50 K>90
65% (Ø GC)≥95% (<10% GC)

Synovial Fluid Analysis: The 5 Tests
Gout Psgt BactWBC% polys+Gram stain+C&S+Crystals
20 K75
RareRare
80-90%
20 K75
RareRare~70%
>50 K>90
65% (Ø GC)≥95% (<10% GC)
5-10%
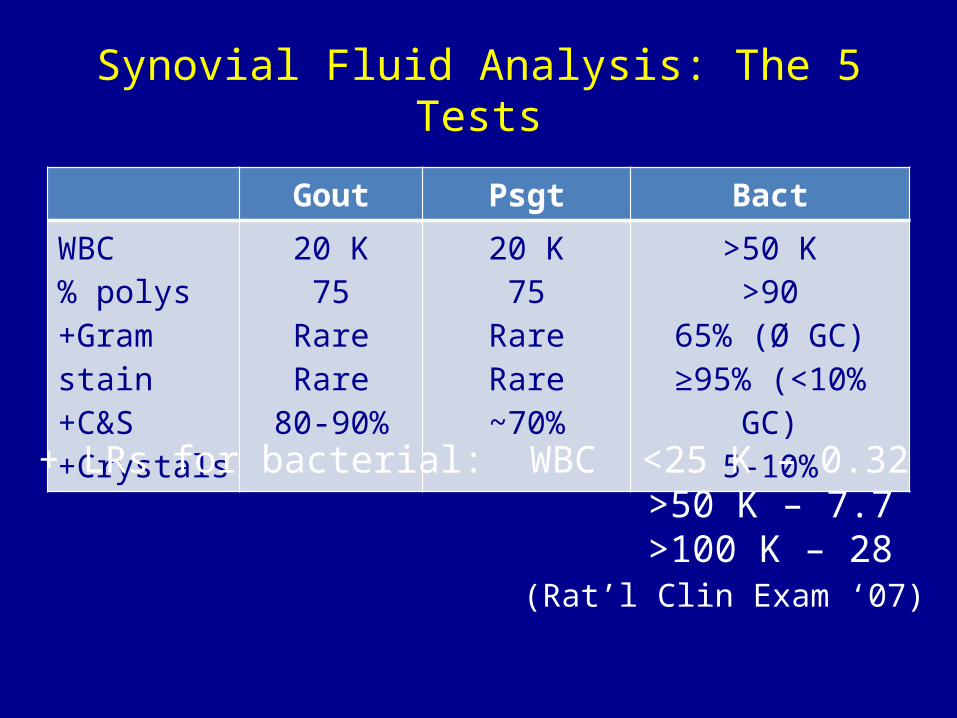
Synovial Fluid Analysis: The 5 Tests
Gout Psgt BactWBC% polys+Gram stain+C&S+Crystals
20 K75
RareRare
80-90%
20 K75
RareRare~70%
>50 K>90
65% (Ø GC)≥95% (<10% GC)
5-10%
+ LRs for bacterial: WBC <25 K – 0.32 >50 K – 7.7 >100 K – 28
(Rat’l Clin Exam ‘07)

Bayes’ for PCPs
• Sensitivity = % pts with disease who test positive (the way they should)
• Specificity = % pts without disease who test negative (the way they should)
• FP rate = 1- specificity• TP rate = sensitivity
Bayes’ for PCPs (2)
• Post-test probability depends on– Sensitivity– Specificity– Pretest probability
• As the sensitivity 100%, post-test prob 0 if negative– SNOut
• As the specificity 100%, post-test prob 100% if positive– SpPIn
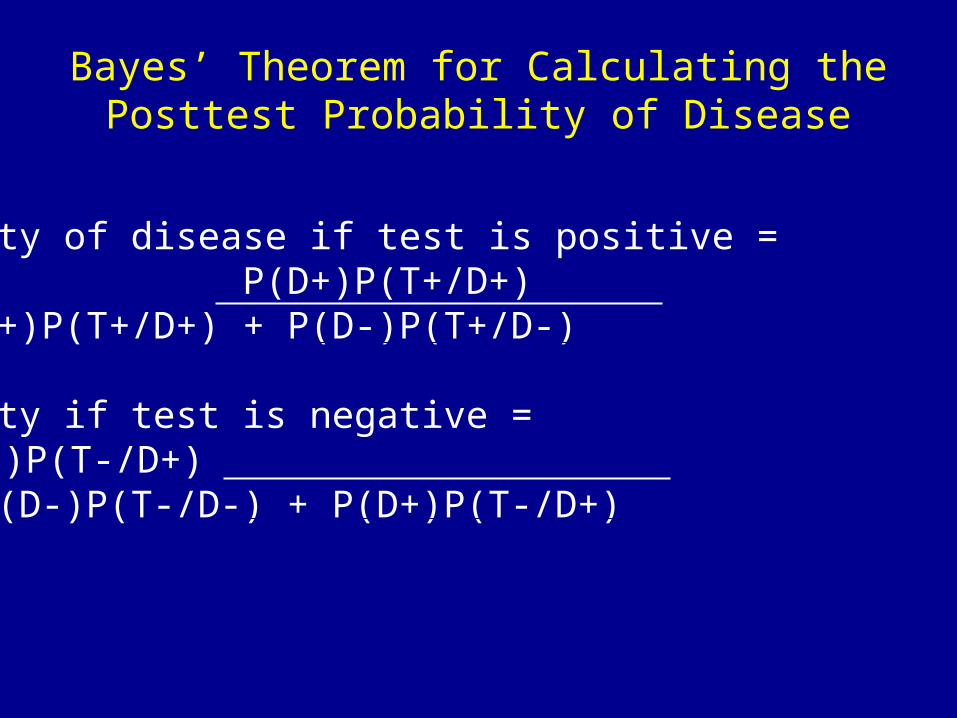
Bayes’ Theorem for Calculating thePosttest Probability of Disease
Probability of disease if test is positive = P(D+)P(T+/D+) P(D+)P(T+/D+) + P(D-)P(T+/D-)
Probability if test is negative = P(D+)P(T-/D+)
P(D-)P(T-/D-) + P(D+)P(T-/D+)

MSU Crystals

Synovial Fluid Analysis Miscellany
• When to tap? Bugs or crystals still in DD?• Clotting falsely lowers WBC
– So does IR saline insertion• A dry tap does not exclude effusion• A negative G stain can’t r/o septic etiology• Crystal analysis not so reliable

A Case of Acute Monoarthritis(File #1141) : “ZZ”
• 50 y/o M rock drummer• 3 d severe pain & swelling left knee• PMH – MI, DM-2, STDs, ETOH, cigs• Meds – simva, metformin, prn oxy/Ambien• PE – tender, warm, swollen knee; obese• SF pos for urate crystals• Rx’d with IA TAC 40 mg
The “Diamond-Shaped Algorithm”
Test
Positive Negative
Management (Rx, education, . . .)
(eg, serum uric acid/CBC for ZZ)

Pitfalls in Testing: Reliability
• Reproducibility, precision• Prerequisite for widespread use of a test• Most important for subjective or
unstandardized tests• Gap between research lab & community
– Are community labs concordant?– Measured by Kappa (K) for categorical
results– K=0-chance; <0.4-poor; 0.4-0.7-fair; >0.7-
good

A Case of Acute Polyarthritis (File #777): “Polly R”
• 32 y/o F PCP• 6 days of pain & swelling PIPs, MCPs,
wrists and knees• PMH – Ø• SH – single, wine, recreational weed, 4+
travel• Meds – prns• PE – tender, swollen jts
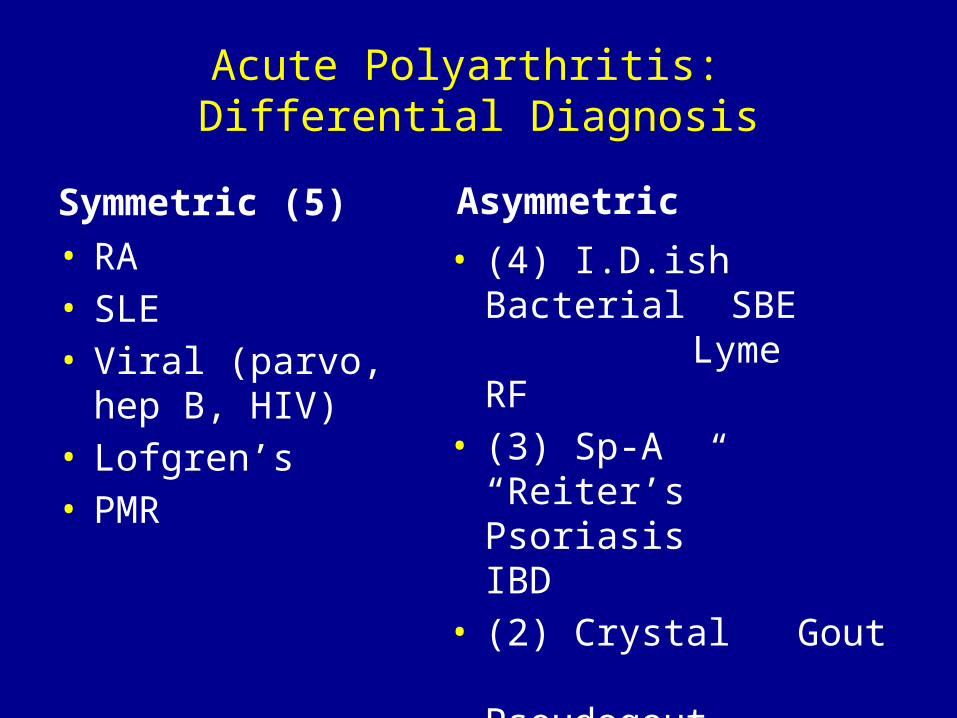
Acute Polyarthritis: Differential Diagnosis
Symmetric (5)• RA• SLE• Viral (parvo, hep B,
HIV)• Lofgren’s• PMR
Asymmetric
• (4) I.D.ish Bacterial SBE Lyme RF
• (3) Sp-A “Reiter’s”
Psoriasis IBD
• (2) Crystal Gout
Pseudogout
A Case of Acute Polyarthritis (File #777): “Polly R”
• 32 y/o F PCP• 6 days of pain & swelling PIPs, MCPs, wrists
and knees• PMH – Ø• SH – single, wine, recreational weed, 4+
travel• Meds – prns• PE – tender, swollen jts
• What workup?
Which Test(s) Would You Order for Polly R (acute poly)?
1) ANA, reflexive2) ANA, quantitative3) RF & a-CCP4) ESR &/or CRP5) Tap/SF analysis6) Lyme titer
Vote for one or more now !

Acute Poly Tests
ANA reflex ANA quant RF/CCP ESR/CRP SF Lyme0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
83%
22%
58%
87%
15%10%

Does Polly R Have Lupus if ANA + ?
1000 clones pretest = 10%
100 SLE 900 Non-SLE
95% TP 5% FP
95 TP 45 FP
Posttest Prob = 95 = 68% 95 + 45

Does Polly R Have Lupus if ANA + ?
1000 clones pretest = 10%
100 SLE 900 Non-SLE
800 RA 100 Misc 95% TP
30% FP 5% FP
95 TP 240 FP 5 FP Posttest Prob = 95 = 28%
95 + 240 And if ANA - ?

Does Polly R Have MI if TROPONIN + ? 1000 clones pretest = 10%
100 MI 900 Non-MI
800 PE 100 Misc 95% TP
30% FP 5% FP
95 TP 240 FP 5 FP
MI Posttest Prob = 95 = 28% 95 + 240
And if Trop - ?
Pitfalls in Testing: Spectrum Effect (Bias)
• Variability in test sensitivity or specificity in different patient subgroups or clinical settings
• e.g.’s of specificity spectrum effect– ANA FP in 5% young normals, but 15%
>65 1/3 RA
– RF FP in 5% young normals, but 15% >65 75% hep C
• e.g.’s of sensitivity spectrum effect– UTI and dipstick– MS & MRI
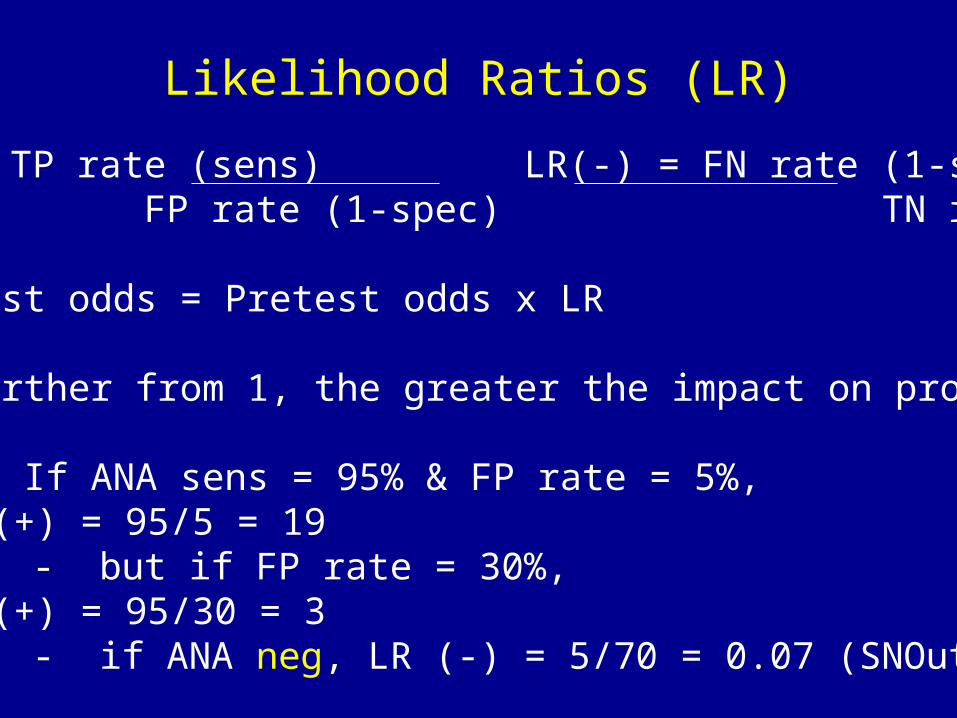
Likelihood Ratios (LR)
LR(+) = TP rate (sens) LR(-) = FN rate (1-sens) FP rate (1-spec) TN rate (spec)
• Posttest odds = Pretest odds x LR
• The further from 1, the greater the impact on prob
• e.g.: If ANA sens = 95% & FP rate = 5%, LR (+) = 95/5 = 19
- but if FP rate = 30%, LR (+) = 95/30 = 3
- if ANA neg, LR (-) = 5/70 = 0.07 (SNOut)

Anti-Nuclear Antibody (ANA): The Basics
• Screen for many possible Abs v. NAs• IFA v. EIA (screen v. reflexive)• Sensitivity (SLE) ~ 95% (at 5% FP cut pt)• FP rate varies – Spectrum Effect (Bias)
– ~1/3 RA, 15% >65, AI thyroid disease, meds, . . .• Supports dx of SLE if prior prob reasonable• Better at R/O than R/I
– Chronic poly + ANA = RA• Reliability (reproducibility) issues• $65 for quantitative screen• The charge for reflexive?

ANAs: The Basics (2)
• Anti-DS DNA sens = 50%, spec >95%• Anti-Smith 25% >95%
– R/I > R/O• “Reflexive ANA”? (a-DNA, Sm, RNP, Ro, La,
Blah, Blah, Blah)– Charge = $752.50
• What is the FIRST stage of testing for SLE?

ANAs: The Basics (2)
• Anti-DS DNA sens = 50%, spec >95%• Anti-Smith 25% >95%
– R/I > R/O• “Reflexive ANA”? (a-DNA, Sm, RNP, Ro, La,
Blah, Blah, Blah)– Charge = $752.50
• What is the FIRST stage of testing for SLE?– CBC & UA


Rheumatoid Factor (RF): The Basics
• a-IgG Fc• Sens (RA) = 70% (at 5% FP cut pt)• FP rate (spec) varies
– ~ 1/3 SLE, 15% >65, 2/3 Hep C• Supports RA Dx if pretest prob reasonable• Small % with +RF have/will get RA• Reliability (reproducibility) issues• Worthless without arthritis (PE)• $60

Anti-Cyclic Citrullinated Protein (a-CCP):The Basics
• Citrulline is an a.a., modified arginine residue• Sens (RA) 70%, spec (in rheum clinic) 95%• 34% of RF neg “RA” pts• Predicts persistence of early inflammatory arthritis
– OR = 38 at 3 yr f/u– OR = 10 for new erosions over 5 yrs (3.4 for +RF)
• But also in 1/4 a-CCP neg pts & not in 1/5 a-CCP+
• It’s ok to do both RF & a-CCP if RA suspected• $49

A Case of Acute Polyarthritis (File #777): “Polly R”
• 32 y/o F PCP• 6 days of pain & swelling PIPs, MCPs, wrists and knees• PMH – Ø• SH – single, wine, recreational weed, 4+ travel• Meds – prns• PE – tender, swollen jts
• ANA 1:160, neg a-DS DNA & a-Smith• RF 1:160, neg a-CCP• Naproxen 500 mg b.i.d.• Resolved over 3 wks

Questions?

The Sed Rate (& CRP): Facts, Fancy & Fiction
• Facts– Cheap, quick & reproducible– RBC fall in 1 hr (mm)– Function of RBC aggregation– with inflammation, tissue injury– >30 in 98% GCA, >80% PMR, 50% RA– >100? - ?90% prob of dxable disease– CRP more direct, changes faster– CRP and ESR may be discrepant
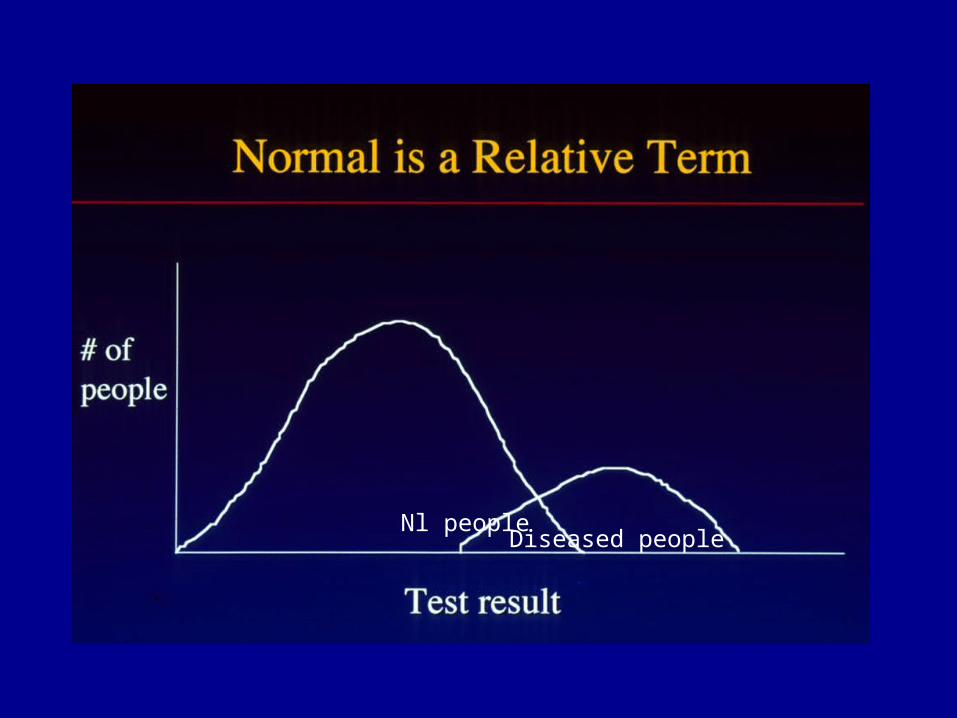
Nl peopleDiseased people

The Sed Rate (& CRP): Facts, Fancy & Fiction (2)
• Fancy– Follow in GCA, PMR– CRP better– Increase with normal aging
• Fiction– If >100, think GCA (TB, MM)– Normal R/O PMR– Increase implies illness

ANCA: Facts, Fancy & Fiction
• Facts– Serologic marker for pauci-immune
necrotizing vasculitides• WG, MPA, C-S, drug-induced
– IFA: c-ANCA & p-ANCA (nonspecific)– ELISA: a-PR3(c) & a-MPO(p)– Sensitivity (c,a-PR3) 80-90%, spec >98%
for WG– Sensitivity if localized– a-MPO in 70% MPA

ANCA: Facts, Fancy & Fiction (2)
• Fancy–Replaces need for bx–Predicts flare
• Fiction–Reliable–p-ANCA helpful
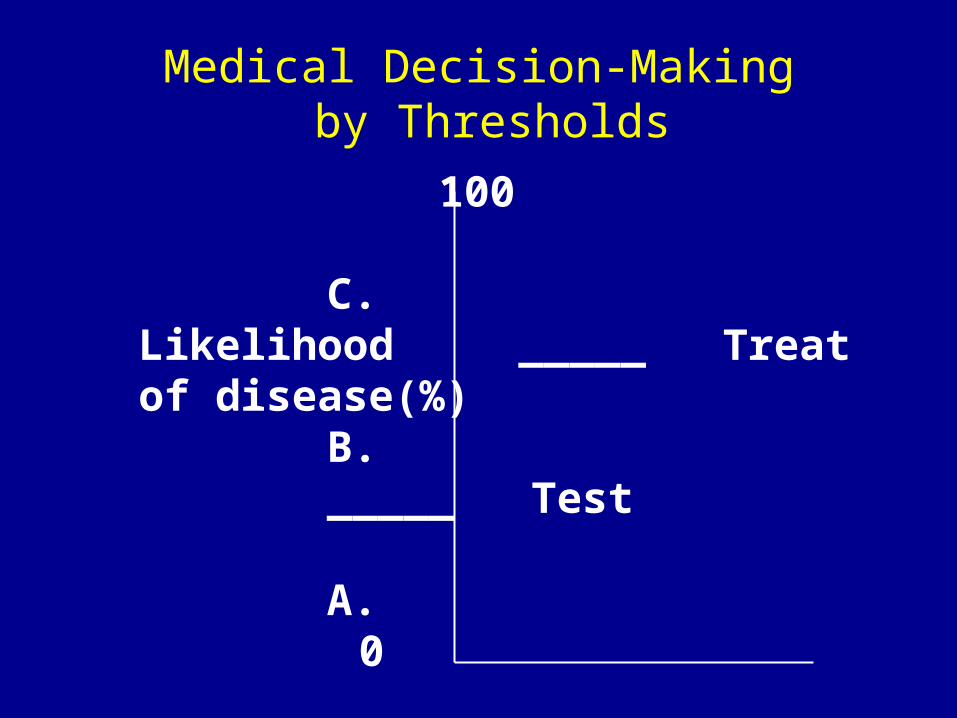
Medical Decision-Making by Thresholds
100
C. Likelihood _____ Treat of disease(%)
B._____ Test
A. 0

Which Diagnostic Strategy is Better?The 4 Determinants
1.Sensitivity2.Specificity3.Cost ($ & morbidity)4.Reliability
A Case of Recurrent Herpes Labialis in a 24 y/o Musician (“Ritchie W”)
• Is he more likely a piano or a tuba player?
piano
tuba
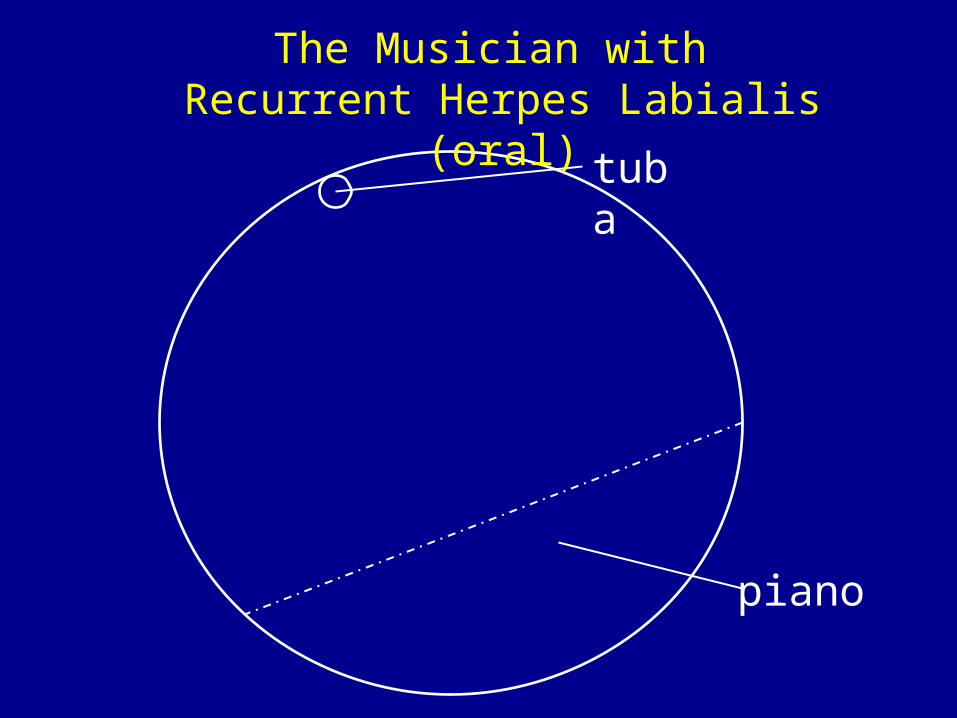
The Musician with Recurrent Herpes Labialis (oral)
piano+ herpes
tuba + herpes
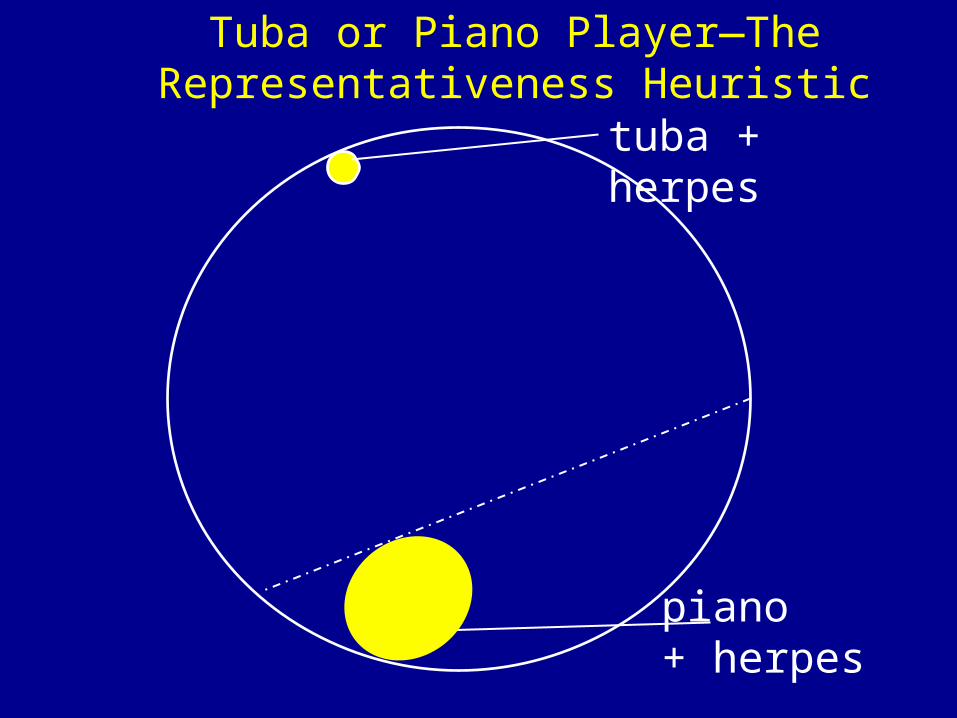
Tuba or Piano Player—The Representativeness Heuristic
A Case of Recurrent Herpes Labialis in a 24 y/o Musician (“Ritchie W”)
• Is he more likely a piano or a tuba player?• The question was NOT “Do tuba players
get more herpes labialis than piano players”
• Human brains substitute an easier, yet wrong question
• The representativeness heuristic

A Case of a Positive ANA
• Joan Smith has a positive ANA at 1:320• 3% of normal women have such an ANA• What can we say about Joan and her ANA?
A Case of a Positive ANA
• Joan Smith has a positive ANA at 1:320• 3% of normal women have such an ANA• What can we say about Joan and her ANA?• “There is a 3% chance this occurred by
chance” ?
A Case of a Positive ANA
• Joan Smith has a positive ANA at 1:320• 3% of normal women have such an ANA• What can we say about Joan and her ANA?• “There is a 3% chance this occurred by
chance” ?• “There is a 97% chance Joan has SLE” ?

A Case of a Positive ANA
• Joan Smith has a positive ANA at 1:320• 3% of normal women have such an ANA• What can we say about Joan and her ANA?• “There is a 3% chance this occurred by
chance” ?• “There is a 97% chance Joan has SLE” ? • “If Joan does NOT have SLE, there is a 3%
chance of getting this result”.
Multiple Testing Error
• A 31 y/o F with polyarthritis x 1 wk, macular rash x 2 days
• CXR (n=?) - possible opacity left base• RF slightly positive, a-CCP neg• Nl/neg CBC (n=≥6), CMP (n=20), UA (n=5?),
ANA, IgM a-parvo, Lyme titer, uric acid, APLA panel (n=6?), ANCA (n=2), C3/C4/CH50– Alk phos 132
• Nl hx (n=?) and PE (n=?) otherwise

Multiple Testing Error (2)• Normal range for most continuous tests = mean ±
2 SDs of healthy controls → 5% FP rate• FP rate may be higher in competing diseases• Chem 20 – 5% FP x 20 = 1 FP/normal
– 40% nls pass, some have > 1 FP• ~ studies & endpoints
– Try to minimize, prespecify primary endpoints– Likelihood of true pos ↑ if . . .
• More abnl• ↑ prior prob• Biologically plausible• Higher specificity• Fewer tests done
(Rheumatologic) Lab Testing for PCPs: Conclusions
• Optimal diagnostic testing is difficult– even more so with rapidly progressing disease, meter
running• Anticipate and avoid tests that lead to a diamond algorithm• Estimate prior probability; avoid “base case neglect”• SNOut, SpPIn• Don’t confuse sensitivity with NPV, specificity with PPV• Beware spectrum effect
– Sens and/or spec may vary• In rheum, few tests are diagnostic
– Observation over time may be the best test (uncertainty!!)– Reliability issue– H&P much more helpful

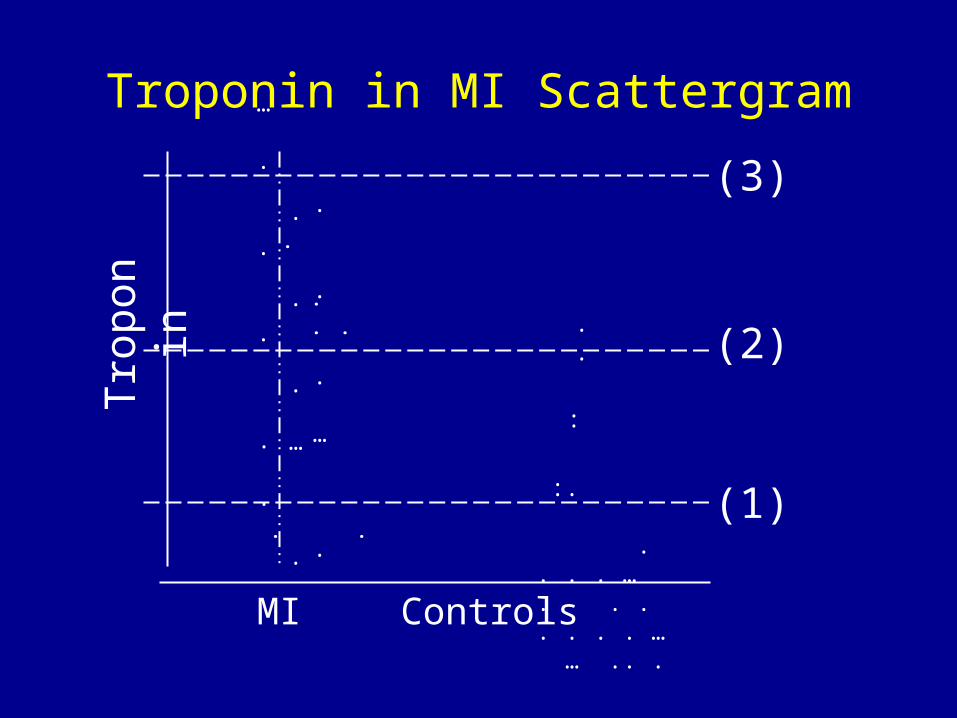
Troponin in MI ScattergramTr
opon
in
:.
. . . . … . . . . . . . … … .. .
(3)
(2)
(1)
MI Controls
. .
.
.
.
.
. … .
.
.
. … .
.
.
. … . .
.
. .
:
.
.

The Case of the Increasingly Sensitive Troponin
• Sensitivity 83% (4th gen cTn T, Roche) 95% (HS)• Specificity 93% 80%• PPV 72% 50%• NPV 97% 99%• Not specific for type of myocardial injury
– HF, PE, demand ischemia, sepsis, myocarditis, KD, . . .• ↑ sens → ↓ spec
– Ok for ED, not for inpatient• Prob of MI in a typical U.S. chest pain observation unit=<5%• HS cTnT above MI threshold in 15% U.S. CP pts; only 2% had
MI (Januzzi, Circ ‘10)– ↑ cost/tests, anxiety
de Lemos. JAMA 2013:2262-9
A Case of Amaurosis Fugax (File #533): “George C”
• 75 y/o M with 15 minutes of R eye blindness yesterday
• PMH – DM2, PAD, ↑ BP• SH – s/p cigs• Meds – ASA 81, metformin, lisinopril, simva• PE – wnl• Lab – ESR 83• Workup ?
– 1) carotid US, 2) TA Bx, 3) CRP, 4) TA color duplex US, 5) 25-OH vit D
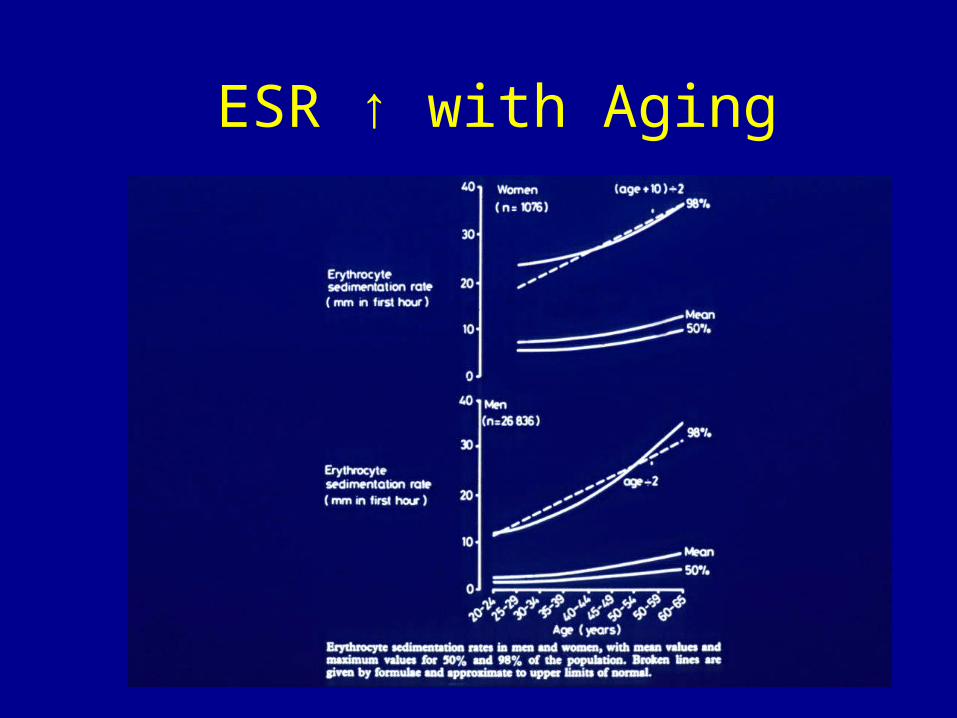
ESR ↑ with Aging

The Temporal Artery Biopsy:Facts, Fancy & Fiction
• Facts– Skip lesions– Take 4 cm– Sens (GCA) ? 75%– 2nd side adds 3% sens– Most will be negative– Hypoechoic halo (US) sens=69%, spec 82%
(Karassa’05)• Only helps by r/o if low prob; reliability ?
• Fancy - a negative bx rules out GCA• Fiction - Can wait 2 wks to bx after pred Rx
A Case of Amaurosis Fugax (File #533): “George C”
• 75 y/o M with 15 minutes of R eye blindness yesterday
• PMH – DM2, PAD, ↑ BP• SH – s/p cigs• Meds – ASA 81, metformin, lisinopril, simva• PE – wnl• Lab – ESR 83• Pred 60 mg/d• TA Bx positive 3 days later
A Case of Pulmonary-Renal Syndrome (File #277): MM
• 50 y/o F with 2 wks of cough & worsening SOB• PMH – neg• PE – diffuse crackles, T 100.8• Hgb 12.1, WBC 7.8 (nl diff), platelets 535K• Creatinine 4.3, UA-2+ pro, 30-40 RBC, 10-15
WBC• CXR – diffuse hazy opacities• Kidney Bx pending• DDx? • Wkup?
A Case of Pulmonary-Renal Syndrome (File #277): MM (2)
• Workup? (vote for one or more)1) ESR/CRP2) ANCA by IFA3) ANCA by EIA4) ANA5) Anti-GBM6) Lung Bx

ESR/CRP ANCA,IFA ANCA,EIA ANA a-GBM Lung Bx0%
20%
40%
60%
80%
100%
120%
63%
90%
80%
100%
85%
25%
Pulm-Renal Syndrome Tests

A Case of Pulmonary-Renal Syndrome (File #277): MM(3) - Test Results
• ESR 63• c-ANCA 1:640• ↑ anti-Pr3• ANA 1:80, homogeneous• Neg a-GBM• DIF of kidney Bx – “pauci-immune”• Dx – GPA (WG)• Pred + cyclo

Questions?





























