Embed Size (px)
Citation preview

lable at ScienceDirect
Chemico-Biological Interactions 256 (2016) 125e133
Contents lists avai
Chemico-Biological Interactions
journal homepage: www.elsevier .com/locate/chembioint
Evaluations of thyme extract effects in human normal bronchial andtracheal epithelial cell lines and in human lung cancer cell line
Marinelli Oliviero a, 1, Iannarelli Romilde a, 1, Morelli Maria Beatrice b, Valisi Matteo c,Nicotra Giovanna c, Amantini Consuelo d, Cardinali Claudio b, Santoni Giorgio a,Maggi Filippo a, **, Nabissi Massimo a, *
a School of Pharmacy, University of Camerino, Camerino, MC, Italyb Dept. Experimental Medicine, University Sapienza, Rome, Italyc Epo s.r.l., Istituto Farmochimico Fitoterapico, Milano, Italyd School of Biosciences and Veterinary Medicine, Camerino, MC, Italy
a r t i c l e i n f o
Article history:Received 10 April 2016Received in revised form6 June 2016Accepted 27 June 2016Available online 29 June 2016
Keywords:Thymus vulgarisAnti-inflammatoryNormal bronchial and tracheal epithelialcells (HBEpC/HTEpC)Lung cancerThymolNF-kB
Abbreviation: Abs, Antibodies; HBEpC/HTEpC,cells; CF, cystic fibrosis; COPD, chronic obstructiveglyceraldehydes-3-phosphate dehydrogenase; GCH,beta, interleukin-1 beta; LPS, lipopolysaccharide; PI,mor necrosis factor-alpha; NF-kB, Nuclear factor-kB.* Corresponding author. University of Camerino, Se
cine, School of Pharmacy, via Madonna delle Carceri 9** Corresponding author. University of Camerino, St’Agostino 1, 62032 Camerino, MC, Italy.
E-mail addresses: [email protected] (M.unicam.it (N. Massimo).
1 Contributed equally to this work.
http://dx.doi.org/10.1016/j.cbi.2016.06.0240009-2797/© 2016 Elsevier Ireland Ltd. All rights rese
a b s t r a c t
Thyme (Thymus vulgaris) is used traditionally to prepare herbal remedies possessing expectorant,mucolytic, antitussive and antispasmodic properties.
The aim of the present study was to investigate the effects of a standardized hydroalcoholic extract ofthyme on primary human airway (bronchial/tracheal) epithelial cell lines in a model of lung inflam-mation induced by LPS. In addition, the effects of thyme extract on human lung cancer cell line (H460)were analysed. Thyme extract showed significant anti-inflammatory properties by reducing the NF-kBp65 and NF-kB p52 transcription factors protein levels followed by the decrease of pro-inflammatorycytokines (IL-1 beta and IL-8), and Muc5ac secretion in human normal bronchial and tracheal epithe-lial cells. Moreover, the extract showed cytotoxic effects on H460 cancer cells, modulated the release ofIL-1 beta, IL-8 and down-regulated NF-kB p65 and NF-kB p52 proteins.
Taken together, these results substantiated the traditional uses of thyme in the treatment of respira-tory diseases. Thyme extract might be an effective treatment of chronic diseases based on inflammatoryprocesses when hypersecretion of mucus overwhelms the ciliary clearance and obstructs airways,causing morbidity and mortality. Moreover thyme extract, evaluated in H460 lung cancer cell line,demonstrated to induce cell cytotoxicity in addition to reduce inflammatory cell signals.
© 2016 Elsevier Ireland Ltd. All rights reserved.
1. Introduction
Inflammatory lung pathologies have become one of the mostprevalent diseases in Europe and are relevant cause of morbidity,
Bronchial/tracheal epithelialpulmonary disease; GAPDH,goblet cell hyperplasia; IL-1propidium iodide; TNF-a, tu-
ction of Experimental Medi-, 62032 Camerino, MC, Italy.chool of Pharmacy, via San-
Filippo), massimo.nabissi@
rved.
mortality and health care expenditure. Many lung diseases are ofinflammatory origin and the symptoms of these disorders aremediated by allergen-induced inflammatory reaction in the air-ways [1]. Whereby, the degranulation of resident mast cells and therelease of pro-inflammatory mediators from lung epithelial cells,trigger and increase vascular permeability and infiltration of acti-vated inflammatory cells [2]. As a consequence, chronic inflam-mation and destructive structural changes occur in the airways[3,4]. Despite the recommended therapy is based on inhalativeanti-inflammatory drugs such as glucocorticoids that suppress theinflammatory processes and bronchodilators that act on reversingmuscle contractility [5], the use of traditional herbal remedies inthe treatment of respiratory diseases is widely adopted by worldpopulation [6]. In this regard, one of the most used herbal drugs isdefinitely thyme, ecompassing several species belonging to thegenus Thymus L. (Lamiaceae family) that are used throughout the

M. Oliviero et al. / Chemico-Biological Interactions 256 (2016) 125e133126
world in the traditional medicine as well as in the food, cosmeticand pharmaceutical industries [7]. Actually, the most importantspecies of the genus used in therapeutic dosage forms is Thymusvulgaris L. This species is used as a spice in many regions of theworld and is one of the most important herbal drugs used asantibacterial agent [7-9]. In the traditional medicine, the floweringaerial parts of thyme are used to prepare infusions and decoctionspossessing expectorant, mucolytic, antitussive and antispasmodicproperties [10-13]. The most important bioactive compounds ofthyme are phenols (thymol and carvacrol) [7], phenolic acids(rosmarinic and caffeic acids) and flavonoids (luteolin, quercetinand apigenin derivatives) [14].
Given the traditional uses of thyme in the treatment of respi-ratory diseases, during which the inflammatory process plays amajor role, in this work we have evaluated whether a commercialstandardized thyme extract could mediate inflammatory cytokinesregulation. For the purpose, we studied the effects of thyme extracton primary human airway (bronchial/tracheal) epithelial cells(HBEpC/HTEpC) in a model of lung inflammation induced by lipo-polysaccharide (LPS). Indeed, exposure to LPS has been demon-strated to increase expression of several pro-inflammatorymediators, such as interleukin-1 beta (IL-1 beta) and tumor ne-crosis factor-alpha (TNF-a) [15], and mucin gene expression withmucus production in airway epithelial cells [16,17]. Furthermore,since inflammation signals often support lung oncogenesis [18], theeffects of thyme extract on human lung cancer cell line (H460) wereinvestigated. Since NF-kB pathway is considered a prototypical pro-inflammatory signaling pathway and an upstream regulator ofmucin gene expression [19], we evaluated thyme extract activity inregulating the canonical and non-canonical NF-kB pathways, withthe aim to identify the potential mechanisms by which thymeextract reduces the expression of pro-inflammatory signals in allcell line tested.
2. Materials and methods
2.1. Cell lines
Human Bronchial/Tracheal Epithelial Cells (HBEpC/HTEpC) arederived from the surface epithelium of normal human bronchi/trachea (Sigma Aldrich, Milan, Italy). HBEpC/HTEpC were grown inBronchial/Tracheal Epithelial Cell Growth medium (Sigma Aldrich),following the manufactoring protocol. Both cell lines were usedbetween passages three and six. Aliquots of passage three, for bothcell lines, were frozen in liquid nitrogen and cultured until passagesix. Medium was specifically designed to promote attachment,spreading and proliferation of HBEpC/HTEpC in culture. This me-dium was fully supplemented with growth factors, trace elements,and antibiotics. Bronchial/Tracheal Epithelial Cell Growth Mediumis serum-free. Media were changed every 48 h until cells were 90%confluent. H460 cells (carcinoma; large cell lung cancer; ATCC, LGCStandards, Milan, Italy) were grown in RPMI1640 medium (Lonza,Milan, Italy), supplemented with 10% foetal bovine serum (FBS),2 mM/L glutamine, 100 IU/ml penicillin, 100 mg streptomycin and1mM sodium pyruvate. All cell lines were maintained at 37 �C with5% CO2 and 95% humidity.
2.2. Reagents
A commercial standardized thyme hydroalcoholic extract(thymol 0.3% w/w) was kindly provided by EPO s.r.l., IstitutoFarmochimico Fitoterapico (Milan, Italy). Thyme extract was pre-pared in ethanol, sonicated and filtered (20 mm filter). Aliquotswere prepared and stored at �20 �C for single use. Lipopolysac-charide (LPS), the major component of the outer membrane of
Gram-negative bacteria, was purchased from Sigma Aldrich andprepared as fresh for each experiment. LPS was diluted in sterilizedwater at concentration of 2 mg/ml.
2.3. Sulforhodamine B (SRB) assay
Cells were seeded at a density of 3 � 104 cells/ml in 96-wellplates. After 24 h of incubation, extracts (up to 0.6% final concen-tration) or vehicles were added. Six replicates were used for eachtreatment. At the indicated time point, cell lines were fixed withcold trichloroacetic acid (TCA), stained by 0.4% SRB dissolved in 1%acetic acid. Bound stains were subsequently solubilized with10 mM Trizma, and the absorbance was read on the microplatereader at a wavelength of 520 nm using an ELISA reader microliterplate (BioTek Instruments, Winooski, VT).
2.4. Cell cycle analysis
Cells, at a density of 3 � 104 cells/ml, were incubated with theappropriate thyme extract (0.3%) for up to 72 h. Cells were fixed byadding ice-cold 70% ethanol for 1 h and then washed with stainingbuffer (PBS, 2% FBS and 0.01% NaN3). Next, cells were treated with100 mg/ml ribonuclease A solution (Sigma Aldrich), incubated for30min at 37 �C, stainedwith 20 mg/ml propidium iodide (PI) (SigmaAldrich) for 30 min at room temperature and finally analysed byflow cytometry using linear amplification.
2.5. Apoptosis assays and PI staining
Cell death was evaluated using Annexin V-FITC and PI stainingfollowed by biparametric FACS analysis. Cells, at a density of3 � 104 cells/ml, were treated with thyme extract (0.3%) for amaximum of 72 h and then incubated with 5 ml Annexin V-FITC(Enzo Life Sciences, Farmingdale, NY, USA) and 20 mg/ml PI (SigmaAldrich) for 10min at room temperature. The percentage of positivecells determined over 10,000 events was analysed on a FACScancytofluorimeter using the CellQuest software. PI-stained cells werealso evaluated by fuorescent microscope analysis.
2.6. DNA fragmentation assay
Electrophoresis of DNA extracts was performed to assess DNAfragmentation as a criterion for necrosis and apoptosis. Briefly,cells, at a density of 3 � 104 cells/ml, were treated with thymeextract (0.3%) and genomic DNA was extracted using a DNAextraction kit (Qiagen, Hilden, Germany). The purified sampleswere then subjected to electrophoresis on a 1.25% agarose gel, andDNA was stained with ethidium bromide. Ultraviolet spectroscopyat 302 nm was used to obtain the results.
2.7. Western blot analysis
HBEpC, HTEpC and H460 cell lines, treated with LPS, thymeextract alone (0.3%) and in combination for 3 h, were lysed and20 mg of the lysates were separated on a SDS polyacrylamide gel,transferred onto Hybond-C extra membranes (GE Healthcare),blocked with 5% low-fat dry milk in PBS-Tween 20, immunoblottedwith mouse monoclonal anti-Muc5ac (1:500, Thermo Scientific,Rockford, IL), anti-IL-1 beta (1:100, Novus, Littleton, CO), anti-IL-8(2 ml/ml, R&D System, Minneapolis, MN), antieNFekB p65(1:500, Santa Cruz, Dallas, TX), antieNFekB p52 (1:500, Santa Cruz)and anti-glyceraldehydes-3-phosphate dehydrogenase (GAPDH,1:8000, Origene, Rockville, MD) antibodies (Abs) overnight andthen incubated with HRP-conjugated anti-mouse secondary Ab(1:2000, Cell Signaling Technology, Danvers, MA) for 1 h.
M. Oliviero et al. / Chemico-Biological Interactions 256 (2016) 125e133 127
Peroxidase activity was visualized with the LiteAblot®PLUS orTURBO (EuroClone, Milan, Italy) kit and densitometric analysis wascarried out by a Chemidoc using the Quantity One software (Bio-Rad). For protein analysis in medium, proteins were precipitated bya modified TCA protocol and then analysed as described above.
2.8. Gene expression analysis
Total RNAwas extracted with the RNeasy Mini Kit (Qiagen), andcDNA was synthesized using the High-Capacity cDNA Archive Kit(Applied Biosystems, Foster City, PA) according to the manufac-turer’s instructions. Quantitative real-time polymerase chain re-actions (qRT-PCR) were performedwith RT2 qPCR Primer Assays forHuman Muc5ac, IL-1 beta and IL-8 (Qiagen) using the iQ5 Multi-color Real-Time PCR Detection System (Bio-Rad, Hercules, CA). ThePCR parameters were 10 min at 95 �C followed by 40 cycles at 95 �Cfor 15 s and 60 �C for 40 s. The relative amount of target mRNAwascalculated by the 2�DDCt method, using GAPDH as a housekeepinggene. All samples were assayed in triplicates in the same plate.Measurement of GAPDH levels was used to normalize mRNA con-tents, and target genes levels were calculated by the 2�DDCt method.
2.9. Statistical analysis
The data presented represent the meanwith standard deviation(SD) of at least 3 independent experiments. The statistical signifi-cance was determined by Student’s t-test and by one way ANOVA;*, #p < 0.01. The statistical analysis of IC50 levels was performedusing Prism 5.0a (Graph Pad).
3. Results
3.1. Thyme extract has no cytotoxic effect in HBEpC and HTEpC lines
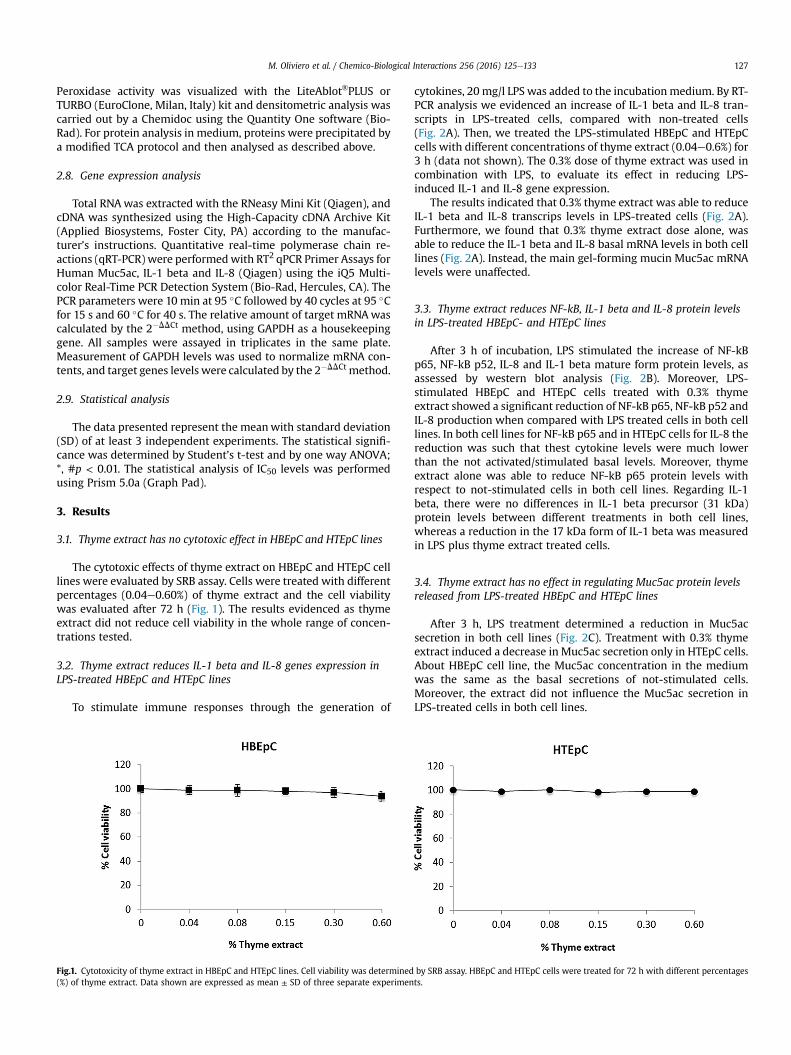
The cytotoxic effects of thyme extract on HBEpC and HTEpC celllines were evaluated by SRB assay. Cells were treated with differentpercentages (0.04e0.60%) of thyme extract and the cell viabilitywas evaluated after 72 h (Fig. 1). The results evidenced as thymeextract did not reduce cell viability in the whole range of concen-trations tested.
3.2. Thyme extract reduces IL-1 beta and IL-8 genes expression inLPS-treated HBEpC and HTEpC lines
To stimulate immune responses through the generation of
Fig.1. Cytotoxicity of thyme extract in HBEpC and HTEpC lines. Cell viability was determined(%) of thyme extract. Data shown are expressed as mean ± SD of three separate experimen
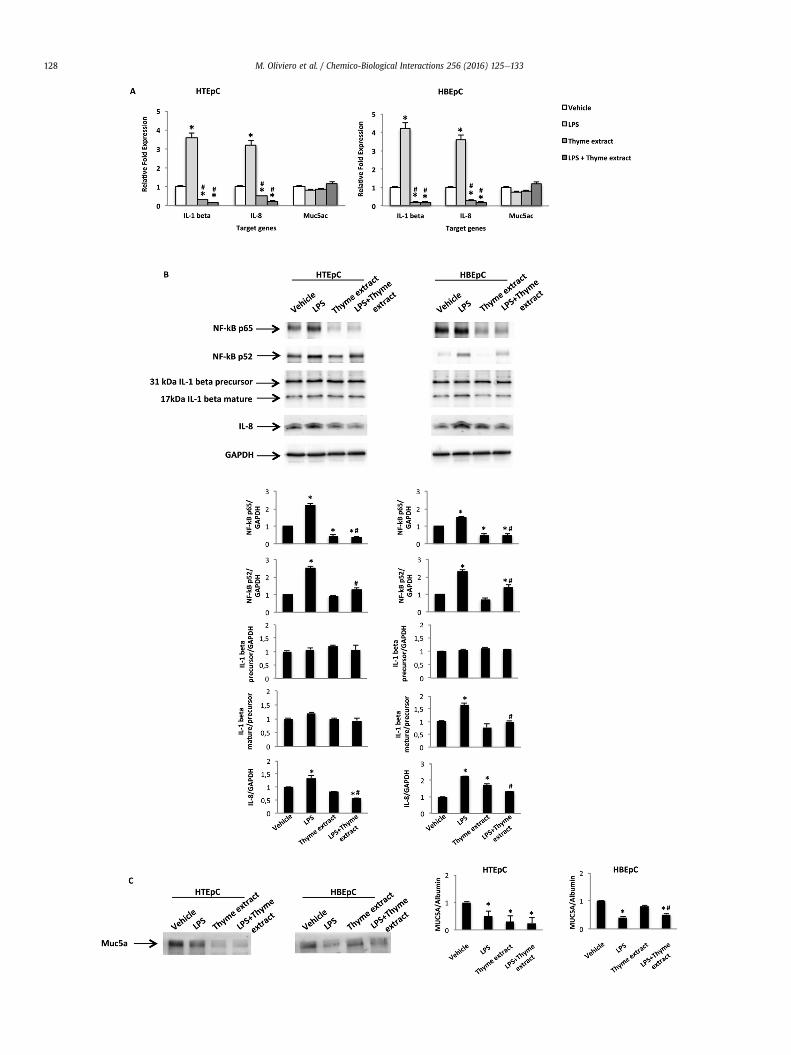
cytokines, 20 mg/l LPS was added to the incubationmedium. By RT-PCR analysis we evidenced an increase of IL-1 beta and IL-8 tran-scripts in LPS-treated cells, compared with non-treated cells(Fig. 2A). Then, we treated the LPS-stimulated HBEpC and HTEpCcells with different concentrations of thyme extract (0.04e0.6%) for3 h (data not shown). The 0.3% dose of thyme extract was used incombination with LPS, to evaluate its effect in reducing LPS-induced IL-1 and IL-8 gene expression.
The results indicated that 0.3% thyme extract was able to reduceIL-1 beta and IL-8 transcrips levels in LPS-treated cells (Fig. 2A).Furthermore, we found that 0.3% thyme extract dose alone, wasable to reduce the IL-1 beta and IL-8 basal mRNA levels in both celllines (Fig. 2A). Instead, the main gel-forming mucin Muc5ac mRNAlevels were unaffected.
3.3. Thyme extract reduces NF-kB, IL-1 beta and IL-8 protein levelsin LPS-treated HBEpC- and HTEpC lines
After 3 h of incubation, LPS stimulated the increase of NF-kBp65, NF-kB p52, IL-8 and IL-1 beta mature form protein levels, asassessed by western blot analysis (Fig. 2B). Moreover, LPS-stimulated HBEpC and HTEpC cells treated with 0.3% thymeextract showed a significant reduction of NF-kB p65, NF-kB p52 andIL-8 production when compared with LPS treated cells in both celllines. In both cell lines for NF-kB p65 and in HTEpC cells for IL-8 thereduction was such that thest cytokine levels were much lowerthan the not activated/stimulated basal levels. Moreover, thymeextract alone was able to reduce NF-kB p65 protein levels withrespect to not-stimulated cells in both cell lines. Regarding IL-1beta, there were no differences in IL-1 beta precursor (31 kDa)protein levels between different treatments in both cell lines,whereas a reduction in the 17 kDa form of IL-1 beta was measuredin LPS plus thyme extract treated cells.
3.4. Thyme extract has no effect in regulating Muc5ac protein levelsreleased from LPS-treated HBEpC and HTEpC lines
After 3 h, LPS treatment determined a reduction in Muc5acsecretion in both cell lines (Fig. 2C). Treatment with 0.3% thymeextract induced a decrease in Muc5ac secretion only in HTEpC cells.About HBEpC cell line, the Muc5ac concentration in the mediumwas the same as the basal secretions of not-stimulated cells.Moreover, the extract did not influence the Muc5ac secretion inLPS-treated cells in both cell lines.
by SRB assay. HBEpC and HTEpC cells were treated for 72 h with different percentagests.
M. Oliviero et al. / Chemico-Biological Interactions 256 (2016) 125e133128

Fig.3. Cytotoxicity of thyme extract in the human non small cell lung carcinomaH460 cells. H460 cell line was treated for 72 h with different concentrations of thymeextract. Cell viability was determined by SRB assay. Data shown are expressed asmean ± SD of three separate experiments. *p < 0.05 treated vs vehicle.
M. Oliviero et al. / Chemico-Biological Interactions 256 (2016) 125e133 129
3.5. Thyme extract reduces cell viability in H460 cancer cell line
The cytotoxic effects of thyme extract were also evaluated inH460 cancer cell line by SRB assay. Cells were treated with differentpercentages (0.04e0.6%) of thyme extract. After 72 h of incubation,thyme extract was able to reduce the cell viability in a dose-dependent manner with an IC50 of 0.11% (Fig. 3).
3.6. Thyme extract does not influence cell cycle in H460 cell line
We then evaluated the mechanisms through which thymeextract reduced cell viability. Thus, we performed cell cycle analysisin the presence of 0.3% thyme extract, the same dose used innormal cells treatments, for 24, 48 and 72 h of treatment. Weobserved that thyme extract treatment did not induce a significantmodulation of cell cycle profile in H460 cells (data not shown).Therefore, we decided to study whether extract treatment couldresult in cell death by DNA agarose gel electrophoresis. A DNAfragmentation was found from 24 h after treatment with 0.3%extract and increased during the time (Fig. 4A). By FITC-conjugatedAnnexin V/PI and cytofluorimetric analysis, we confirmed thatthyme extract treatment results in a significant increased per-centage of cells undergoing necrotic-like death (Annexin V�/PIþ)after 72 h of treatment (Fig. 4B). The PI incorporation was alsoconfirmed microscopically, by assessing the increased number ofpositive PI stained cells (Fig. 4C).
3.7. Thyme extract reduces IL-1 beta and IL-8 genes expression inH460 cells
H460 cells were treated with 0.3% thyme extract for 3 h andcytokines mRNA levels modulation was determined by qRT-PCR.Data demonstrated that thyme extract was able to reduce themRNA levels of both IL-1 beta and IL-8 (Fig. 5A).
Fig.2. Effects of thyme extract on IL-1beta, IL-8, and Muc5a levels in HBEpC and HTEpC celltime PCR. HBEpC and HTEpC cells were treated for 3 h with LPS (20 mg/l) and thyme extract (to GAPDH mRNA levels was calculated considering vehicle samples as calibrator. Values are mextract or LPS þ thyme extract vs LPS and vehicle. B. HBEpC and HTEpC were treated for 3 h wproduction of NF-kB p65, NF-kB p52, IL-1- beta and IL-8 proteins were evaluated in cell lyrepresentative of at least three different experiments. Values are the mean ± SD of three exproduction of Muc5a was measured using the culture supernatant of HBEpC and HTEpC cealone or in combination. Immunoblots are representative of at least three different expermean ± SD of three experiments. *p < 0.05 treated vs veihcle, #p < 0.05 LPS þ thyme extr
3.8. Thyme extract reduces NF-kB p65, NF-kB p52, IL-1 beta and IL-8 protein levels in H460 cells
After 3 h of incubation, 0.3% thyme extract decreased NF-kB p65,NF-kB p52, IL-8 and IL-1 beta mature (17 kDa) proteins production,in H460 cells (Fig. 5B). Regarding IL-1 beta, there were no differ-ences in IL-1 beta precursor (31 kDa) protein levels between vehicleand thyme extract treated cells.
4. Discussion
Extracts from thyme have been used in the traditional medicinefor the treatment of several respiratory diseases like asthma andbronchitis [13] and for the treatment of other pathologies thanks toseveral properties such as antiseptic, antispasmodic, antitussive,antimicrobial, antifungal, antioxidative, and antiviral [20-22].However, too much little is known about thyme anti-inflammatoryactivity. It has been reported that thyme oil reduces NO productionin J774A.1murinemacrophages [23] and reduces pro-inflammatorycytokines release in human THP-1 macrophage [24]. However, tothe best of our knowledge, there are no reports on the effects ofthyme extract on human lung epithelial cells. In this study, weanalysed the impact of a standardized thyme extract on pro-inflammatory response in a model of LPS-induced pulmonaryinflammation. We demonstrated that thyme extract acts as an in-hibitor of LPS-induced pro-inflammatory citokines IL-1 beta and IL-8, at both mRNA and protein levels in normal human epitelial cells.
The results obtained may be explained by the presence ofbioactive phytochemicals occurring in thyme extract such asthymol, although synergism with other minor constituents has tobe taken into account. Indeed, thymol was shown to exhibit mul-tiple biological activities including anti-inflammatory [25], immu-nomodulating [26], antioxidant [27], antibacterial [28], antifungal[29], and free radical scavenging properties [30].
Many studies have been conducted to elucidate the role ofvarious cytokines in mucus hypersecretion [31]. IL-1 beta is a pro-inflammatory cytokine that is secreted by immune cells in responseto bacterial or viral challenges [32] and has been shown to play arole in airway diseases characterized by increased mucus produc-tion [33]. Mucus is a gel that covers the airway epithelium and isconstituted by different glycoproteins called mucins, which aresecreted by goblet cells from submucosal glands and the airwayepithelium [34]. Mucus dissolves noxious gases and entraps foreignparticles and pathogens, facilitating their clearance by mucociliarytransport as a mechanism of innate defense [35]. However, inchronic inflammatory respiratory diseases, such as asthma, chronicobstructive pulmonary disease (COPD), and cystic fibrosis (CF),there is a pathological goblet cell hyperplasia (GCH) and mucushypersecretion that can generate airway occlusion, associated withmorbidity and death [34]. The main gel-forming mucins found inhuman airways areMuc5b andMuc5ac [34], which are large, highlyO-glycosylated macromolecules with a protein backbone. Inhealthy individuals, low levels of Muc5b and Muc5ac can bedetected in mucus; although Muc5b is mainly present in the sub-mucosal glands and Muc5ac is predominantly distributed in the
lines. A. The expression of IL-1beta, IL-8, and Muc5a mRNA was measured using real-final concentration 0.3%), alone or in combination. Relative gene expression normalizedean ± SD of three different experiments. *p < 0.05 treated vs vehicle, #p < 0.05 thymeith LPS (20 mg/l), thyme extract (final concentration 0.3%) alone or in combination. Thesates by western blot analysis. GAPDH was used as loading control. Immunoblots areperiments. *p < 0.05 treated vs veihcle, #p < 0.05 LPS þ thyme extract vs LPS. C. Thells stimulated for 3 h with LPS (20 mg/l) and thyme extract (final concentration 0.3%),iments. Albumin levels were used as loading control. The data are presented as theact vs thyme extract.

Fig.4. Effect of thyme extract on H460 cell cycle. H460 cell line was cultured in the presence of thyme extract (0.3% final concentration). A. Representative agarose gel electro-phoresis of DNA extracts after 24, 48 and 72 h of treatment for the assessment of DNA fragmentation. B. After 72 h of treatment, H460 cells were stained with PI and Annexin V-FITCto assess cell death. C. Fluorescent microscope analysis of PI incorporation after 72 h of treatment (magnification 20�).

Fig.5. Effects of thyme extract on IL-1beta, IL-8, and Muc5a levels in H460 cell line. A. The expression of IL-1beta, IL-8, and Muc5a mRNA was measured using real-time PCR. H460cells were treated thyme extract (final concentration 0.3%) for 3 h. Relative gene expression normalized to GAPDH mRNA levels was calculated considering vehicle samples ascalibrator. Values are mean ± SD of three different experiments. *p < 0.05 treated vs vehicle. B. H460 cells were treated for 3 h with thyme extract (final concentration 0.3%). Theproduction of NF-kB p65, NF-kB p52, IL-1- beta and IL-8 was evaluated in cell lysates by western blot analysis. GAPDH was used as loading control. Immunoblots are representativeof at least three different experiments. Values are the mean ± SD of three experiments. *p < 0.05 treated vs veihcle.

M. Oliviero et al. / Chemico-Biological Interactions 256 (2016) 125e133132
airway epithelium [36]. Mucins levels increased in patients withlung diseases [37]. Mucin gene expression is regulated by inflam-matory/immune response mediators, which are elevated in theairway secretions of patients with asthma, CF and COPD, at tran-scriptional [36,38] and/or post-transcriptional level [36]. TheMuc5ac gene is transcriptionally up regulated by LPS [39], IL-9 [40],neutrophil elastase (NE) [41], TNF-a, and IL-1 beta [42]. IL-8, whichis a predominant proinflammatory mediator activated in responseto pulmonary inflammation, regulates Muc5ac gene expression atthe post-transcriptional level to increase mucin mRNA stability inlung epithelial cells. Our findings are in agreement with these re-ports. Using primary HBEpC and HTEpC culture, supernatants fromcell lines treated with thyme extract, alone or LPS-stimulated,reduced the secretion of Muc5a at basal levels. Therefore, thesedata suggest that the use of thyme extract may be an effectiveapproach to decrease IL-1 beta and IL-8 during inflammation andmucin overproduction in CF, acute asthma, and chronic bronchitis.
Regarding the potential transcriptional pathways regulatinginflammatory state in lung, the activation of NF-kB transcriptionalfactors was identified in participating in cytokine and chemokineproduction [43]. Recently, as become clear that there are at leasttwo separate pathways for NF-kB activation, the canonical and thealternative pathway. The canonical NF-kB proteins, which comprisep65 and p50 members are triggered by LPS and pro-inflammatorycytokines (as IL-1), while the alternative NF-kBmembers consistingof p52 and RelB have been associated to normal lymphoid organdevelopment [43,44]. The findings about thyme extract as negativeregulator of p65 protein, strongly support its role in reducing aninflammatory environment in bronchial and tracheal cell after LPStreatment. Moroever, very recently, in lung tissue from patientswith acute respiratory distress syndrome, an increased expressionof p52 was found and its expressionwas associated to an enhancedlung injury, increased ephitelial apoptosis and reduced survivalafter LPS-treatment [45]. Our evidences regarding an inhibitoryrole of thyme extract in p52 expression, strengthens further itsprotective role in LPS-induced lung damages.
The most interesting observation made during our studies wasthat the same treatments with thyme extract that have no effect onviability of normal human epithelial cells, are capable to inducenecrotic cell death in H460 lung cancer cell line. Moreover, weobserved a significant expression modulation of the pro-inflammatory cytokines also in this model, with a reduction of IL-1 beta mature form and IL-8 levels. Notably, IL-1 influences tu-mor growth and metastases either through direct proliferative ef-fects or by promoting inflammatory and angiogenic pathways inhost cells [46], IL-8 signaling promotes angiogenic responses inendothelial cells, increases proliferation and survival of endothelialand cancer cells, and potentiates the migration of cancer cells,endothelial cells, and infiltrating neutrophils at the tumor site [47].Since elevated IL-1 and IL-8 concentrations have been identified innumerous types of solid tumors inwhich the prognoses is markedlyworse, our study highlight the potential beneficial effects of thymeextract on cancer cells. Furthermore, different studies have estab-lished a link between NF-kB and lung carcinogenesis, suggestingthat targeting NF-kB signaling pathway could be a novel approachin chemopreservation and lung cancer treatment [48,49]. Our data,in H460 lung cancer cells, suggest that the use of thyme extractshould be an interesting additional drug to reduce cancer cellviability for its interfering with the NF-kB p65 and NF-kB p52pathways in cancer cells.
5. Conclusions
Overall the present work substantiated the traditional uses ofthyme in the treatment of respiratory diseases during which
inflammatory processes play a key role. Thyme extract showedsignificant anti-inflammatory properties by reducing the release ofproinflammatory cytokines, NF-kB p65 and NF-kB p52 pathwaysand Muc5a secretion in human normal epithelial cells. These re-sults suggest that thyme extract could be used as an effectivetreatment of chronic diseases based on inflammatory processeseven when hypersecretion of mucus overwhelms the ciliary clear-ance and obstructs airways, causing morbidity and mortality.However, further studies should be carried out for this purpose. Ofparticular interest is the selective cytotoxic effect of thyme extracton H460 cancer cells with respect to normal cell lines and itscapability to modulate the cytokines IL-1 beta, IL-8 and NF-kB p65and NF-kB p52 pathways that are involved in promotion of angio-genesis, tumor growth, and metastasis in several experimentalmodels [47,50]. These results are interesting and deserve furtherinvestigations in order to verify the efficacy of thyme in the man-agement of lung cancer.
Acknowledgements
Authors thank EPO s.r.l., Istituto Farmochimico Fitoterapico(Milan, Italy), for the compound and FAR Unicam for financialsupport.
Transparency document
Transparency document related to this article can be foundonline at http://dx.doi.org/10.1016/j.cbi.2016.06.024.
References
[1] L.A. Weigand, B.J. Undem, Allergen-induced neuromodulation in the respira-tory tract, Chem. Immunol. Allergy 98 (2012) 142e162.
[2] H.J. Gould, B.J. Sutton, IgE in allergy and asthma today, Nat. Rev. Immunol. 8(3) (2008) 205e217.
[3] P.J. Barnes, Immunology of asthma and chronic obstructive pulmonary dis-ease, Nat. Rev. Immunol. 8 (3) (2008) 183e192.
[4] S.T. Holgate, Epithelium dysfunction in asthma, Dec, J. Allergy Clin. Immunol.120 (6) (2007) 1233e1244. quiz 1245e6.
[5] T. Rhen, J.A. Cidlowski, Antiinflammatory action of glucocorticoidsdnewmechanisms for old drugs, N. Engl. J. Med. 353 (16) (2005) 1711e1723.
[6] WHO Regional Office for the Western Pacific, Research Guidelines for Evalu-ating the Safety and Efficacy of Herbal Medicine, 1993. Manila, Republic of thePhilippines.
[7] S.M. Nabavi, A. Marchese, M. Izadi, V. Curti, M. Daglia, S.F. Nabavi, Plantsbelonging to the genus Thymus as antibacterial agents: from farm to phar-macy, Food Chem. 173 (2015) 339e347.
[8] I. Rasooli, S.A. Mirmostafa, Antibacterial properties of Thymus pubescens andThymus serpyllum essential oils, Fitoterapia 73 (2002) 244e250.
[9] B. Tepe, D. Daferera, M. S€okmen, M. Polissiou, A. S€okmen, In vitro antimicrobialand antioxidant activities of the essential oils and various extracts of Thymuseigii M. Zohary et P.H. Davis, J. Agric. Food Chem. 52 (2004) 1132e1137.
[10] B. Vanaclocha, S. Ca~nigueral, Fitoterapia: Vademecum de Prescripcion, 4th ed.,Masson Ed., Barcelona, Spain, 2003.
[11] F.A. Al-Bayati, Synergistic antibacterial activity between Thymus vulgaris andPimpinella anisum essential oils and methanol extracts, J. Ethnopharmacol.116 (2008) 403e406.
[12] D.A. Allen, G. Hatfield, Medicinal Plants in Folk Tradition. An Ethnobotany ofBritain and Ireland, Timber Press, Inc, Portland, Oregon, USA, 2004.
[13] J.R. Alonso, Tratado de Fitomedicina. Bases Clınicas y Farmacologicas, IsisEdiciones, Buenos Aires, Argentina, 1998.
[14] N. Martins, L. Barros, C. Santos-Buelga, S. Silva, M. Henriques, I.C.F.R. Ferreira,Decoction, infusion and hydroalcoholic extract of cultivated thyme: antioxi-dant and antibacterial activities, and phenolic characterisation, Food Chem.167 (2015) 131e137.
[15] D.S. Cheng, W. Han, S.M. Chen, T.P. Sherrill, M. Chont, G.Y. Park, J.R. Sheller,V.V. Polosukhin, J.W. Christman, F.E. Yull, T.S. Blackwell, Airway epitheliumcontrols lung inflammation and injury through the NF-kappa B pathway,J. Immunol. 178 (2007) 6504e6513.
[16] J.D. Li, A.F. Dohrman, M. Gallup, S. Miyata, J.R. Gum, Y.S. Kim, J.A. Nadel,A. Prince, C.B. Basbaum, Transcriptional activation of mucin by Pseudomonasaeruginosa lipopolysaccharide in the pathogenesis of cystic fibrosis lungdisease, Proc. Natl. Acad. Sci. U.S.A. 94 (1997) 967e972.
[17] K. Kohri, I.F. Ueki, J.J. Shim, P.R. Burgel, Y.M. Oh, D.C. Tam, T. Dao-Pick,J.A. Nadel, Pseudomonas aeruginosa induces Muc5ac production via epidermal

M. Oliviero et al. / Chemico-Biological Interactions 256 (2016) 125e133 133
growth factor receptor, Eur. Respir. J. 20 (2002) 1263e1270.[18] D.B. Vendramini-Costa, J.E. Carvalho, Molecular link mechanisms between
inflammation and cancer, Curr. Pharm. Des. 18 (2012) 3831e3852.[19] J.H. Kang, S.M. Hwang, I.Y. Chung, S100A8, S100A9 and S100A12 activate
airway epithelial cells to produce MUC5AC via extracellular signal-regulatedkinase and nuclear factor-kB pathways, Immunology 144 (1) (2015) 79e90.
[20] K.M. Soliman, R.I. Badeaa, Effect of oil extracted from some medicinal plantson different mycotoxigenic fungi, Food Chem. Toxicol. 40 (11) (2002)1669e1675.
[21] A. Bukovsk�a, S. Cikos, S. Juh�as, G. Il’kov�a, P. Reh�ak, J. Koppel, Effects of acombination of thyme and oregano essential oils on TNBS-induced colitis inmice, Mediat. Inflamm. (2007) 23296, http://dx.doi.org/10.1155/2007/23296.
[22] F. Begrow, J. Engelbertz, B. Feistel, R. Lehnfeld, K. Bauer, E.J. Verspohl, Impactof thymol in thyme extracts on their antispasmodic action and ciliary clear-ance, Planta Med. 76 (2010) 311e318.
[23] E. Vigo, A. Cepeda, O. Gualillo, R. Perez-Fernandez, In-vitro anti-inflammatoryeffect of Eucalyptus globulus and Thymus vulgaris: nitric oxide inhibition inJ774A.1 murine macrophages, J. Pharm. Pharmacol. 56 (2004) 257e263.
[24] A. Oca~na, G. Reglero, Effects of thyme extract oils (from Thymus vulgaris,Thymus zygis, and Thymus hyemalis) on cytokine production and geneexpression of oxldl-stimulated thp-1-macrophages, J. Obes. (2012) 104706.
[25] P.C. Braga, M. Dal Sasso, M. Culici, T. Bianchi, L. Bordoni, L. Marabini, Anti-inflammatory activity of thymol: inhibitory effect on the release of humanneutrophil elastase, Pharmacology 77 (2006) 130e136.
[26] Y. Suzuki, H. Furuta, Stimulation of guinea pig neutrophil superoxide anion-producing system with thymol, Inflammation 12 (1988) 575e584.
[27] R. Aeschbach, J. L€oliger, B.C. Scott, A. Murcia, J. Butler, B. Halliwell, O.I. Aruoma,Antioxidant actions of thymol, carvacrol, 6-gingerol, zingerone and hydrox-ytyrosol, Food Chem. Toxicol. 32 (1994) 31e36.
[28] N. Didry, L. Dubreuil, M. Pinkas, Activity of thymol, carvacrol, cinnamaldehydeand eugenol on oral bacteria, Pharm. Acta Helv. 69 (1994) 25e28.
[29] M. Segvi�c Klari�c, I. Kosalec, J. Masteli�c, E. Pieckov�a, S. Pepeljnak, Antifungalactivity of thyme (Thymus vulgaris L.) essential oil and thymol against mouldsfrom damp dwellings, Lett. Appl. Microbiol. 44 (2007) 36e42.
[30] S. Fujisawa, Y. Kadoma, Effect of phenolic compounds on the polymerizationof methyl methacrylate, Dent. Mater 8 (1992) 324e326.
[31] P. Jeffery, J. Zhu, Mucin-producing elements and inflammatory cells, NovartisFound. Symp. 248 (2002) 51e68 discussion 68-75, 277-282.
[32] C.A. Dinarello, Interleukin-1, Cytokine Growth Factor Rev. 8 (1997) 253e265.[33] J. Kadota, Y. Matsubara, Y. Ishimatsu, M. Ashida, K. Abe, R. Shirai, K. Iida,
K. Kawakami, H. Taniguchi, T. Fujii, M. Kaseda, S. Kawamoto, S. Kohno, Sig-nificance of IL-1beta and IL-1 receptor antagonist (IL-1Ra) in bronchoalveolarlavage fluid (BALF) in patients with diffuse panbronchiolitis (DPB), Clin. Exp.Immunol. 103 (1996) 461e466.
[34] D.J. Thornton, K. Rousseau, M.A. McGuckin, Structure and function of thepolymeric mucins in airways mucus, Ann. Rev. Physiol. 70 (2008) 459e486.
[35] S.H. Randell, R.C. Boucher, Effective mucus clearance is essential for respira-tory health, Am. J. Resp. Cell. Mol. Biol. 35 (2006) 20e28.
[36] M.C. Rose, J.A. Voynow, Respiratory tract mucin genes and glycoproteins inhealth and disease, Physiol. Rev. 86 (2006) 245e278.
[37] S. Kirkham, J.K. Sheehan, D. Knight, P.S. Richardson, D.J. Thornton, Heteroge-neity of airways mucus: variations in the amounts and glycoforms of themajor oligomeric mucins MUC5AC and MUC5B, Biochem J. 361 (2002)537e546.
[38] C. Basbaum, H. Lemjabbar, M. Longphre, D. Li, E. Gensch, N. McNamara,Control of mucin transcription by diverse injury-induced signaling pathways,Am. J. Respir. Crit. Care Med. 160 (1999) S44eS48.
[39] D. Li, M. Gallup, N. Fan, D.E. Szymkowski, C.B. Basbaum, Cloning of the amino-terminal and 5’-flanking region of the human MUC5AC mucin gene andtranscriptional up-regulation by bacterial exoproducts, J. Biol. Chem. 273(1998) 6812e6820.
[40] M. Longphre, D. Li, M. Gallup, E. Drori, C.L. Ordo~nez, T. Redman, S. Wenzel,D.E. Bice, J.V. Fahy, C. Basbaum, Allergen-induced IL-9 directly stimulatesmucin transcription in respiratory epithelial cells, J. Clin. Invest. 104 (1999)1375e1382.
[41] J.S. Koo, Y.D. Kim, A.M. Jetten, P. Belloni, P. Nettesheim, Overexpression ofmucin genes induced by interleukin-1 beta, tumor necrosis factor-alpha,lipopolysaccharide, and neutrophil elastase is inhibited by a retinoic acidreceptor alpha antagonist, Exp. Lung Res. 28 (2002) 315e332.
[42] K.S. Song, W.J. Lee, K.C. Chung, J.S. Koo, E.J. Yang, J.Y. Choi, J.H. Yoon, Inter-leukin-1 beta and tumor necrosis factor-alpha induce MUC5AC over-expression through a mechanism involving ERK/p38 mitogen-activatedprotein kinases-MSK1-CREB activation in human airway epithelial cells, J. Biol.Chem. 278 (2003) 23243e23250.
[43] T. Lawrence, The nuclear factor NF-kappaB pathway in inflammation, ColdSpring Harb. Perspect. Biol. 1 (6) (2009).
[44] Weih DS, Yilmaz ZB, Weih F. 2001. Essential role of RelB in germinal centerand marginal zone formation and proper expression of homing chemokines.67(4):1909e1919.
[45] J.A. Saxon, D.S. Cheng, W. Han, V.V. Polosukhin, A.G. McLoed, B.W. Richmond,L.A. Gleaves, H. Tanjore, T.P. Sherrill, W. Barham, F.E. Yull, T.S. Blackwell, p52overexpression increases epithelial apoptosis, enhances lung injury, and re-duces survival after lipopolysaccharide treatment, J. Immunol. 196 (4) (2016)1891e1899.
[46] A.M. Lewis, S. Varghese, H. Xu, H.R. Alexander, Interleukin-1 and cancerprogression: the emerging role of interleukin-1 receptor antagonist as a noveltherapeutic agent in cancer treatment, J. Transl. Med. 4 (2006) 48.
[47] D.J. Waugh, C. Wilson, The interleukin-8 pathway in cancer, Clin. Cancer Res.14 (2008) 6735e6741.
[48] W. Chen, X. Wang, L. Bai, X. Liang, J. Zhuang, Y. Lin, Blockage of NF-kappaB byIKKbeta- or RelA-siRNA rather than the NF-kappaB super-suppressor Ikap-paBalpha mutant potentiates adriamycin-induced cytotoxicity in lung cancercells, J. Cell Biochem. 105 (2) (2008) 554e561.
[49] G.M. Hur, J. Lewis, Q. Yang, Y. Lin, H. Nakano, S. Nedospasov, Z.G. Liu, Thedeath domain kinase RIP has an essential role in DNA damage-induced NF-kappa B activation, Genes Dev. 17 (7) (2003) 873e882.
[50] D.M. Elaraj, D.M. Weinreich, S. Varghese, M. Puhlmann, S.M. Hewitt,N.M. Carroll, E.D. Feldman, E.M. Turner, H.R. Alexander, The role of interleukin1 in growth and metastasis of human cancer xenografts, Clin. Cancer Res. 12(4) (2006) 1088e1096.







![Antioxidant Activity of Thyme Waste Extract in O/W Emulsions...In spite of emulsions O/W being largely used in food, pharmaceutical, cosmetic industries, and biomedical sciences [1],](https://img.dokumen.tips/doc/110x75/5fe4a53c6b0509197d17ff52/antioxidant-activity-of-thyme-waste-extract-in-ow-emulsions-in-spite-of-emulsions.jpg)