-
EVALUATION'OF THERAPEUTIC SUBSTANCESEMPLOYEDFORTHERELIEF OF
BRONCHOSPASM.V. ADRENERGICAGENTS
By ELLIOTT BRESNICK,2 JOHN F. BEAKEY,3 LEON LEVINSON,'AND
MAURICES. SEGAL5
(From the Department of Inhalational Therapy, Boston City
Hospital, and the Department ofMedicine, Tufts College Medical
School, Boston)
(Received for publication March 31, 1949)
Many laboratory techniques have been em-ployed in the study of
sympathomimetic amines,particularly in an attempt to correlate
chemicalstructure with pharmacological activity (1-7).In Table I
are shown the structural formulae ofthe preparations dealt with in
this report.
The technique of protection studies in asthmatichuman subjects
appears to offer an additionalmethod of investigating and
evaluating these andother substances in the ultimate test object,
man.The technique essentially consists of the measure-ment of the
protection afforded by any substanceagainst the dyspnea and
bronchospasm induced byrepeated administrations of histamine,
methacho-line, or allergens, as measured, in part at least,by
changes in vital capacity.
METHODS
The methods we have employed and their historicaldevelopment
have been extensively presented elsewhere(8, 9).
In the experiments reported at this time, the broncho-spastic
agents used were histamine diphosphate 6 andmethacholine chloride
employed intravenously or asaerosols. The protecting ability of the
therapeutic agentunder examination was determined by serial
observationsof the reduction in vital capacity produced by
repeatedadministration of a constant dose (predetermined as
cap-able of producing a consistent reduction in vital capacity
1 This study was supported by a grant from the UnitedStates
Public Health Service.
2 Out-Patient Physician, Boston City Hospital; FormerCharlton
Research Fellow and now Assistant in Medi-cine, Tufts College
Medical School.
8 Research Fellow in Medicine, Tufts College MedicalSchool.
4Assistant in Medicine, Tufts College Medical School.6 Director,
Department of Inhalational Therapy, Boston
City Hospital; Assistant Professor of Medicine, TuftsCollege
Medical School.
* Kindly supplied by Abbott Laboratories, Inc., Chi-cago,
Illinois.
7Kindly supplied by Merck and Company, Rahway,New Jersey.
of at least 25 per cent) of histamine or methacholine atvarying
intervals after the protecting agent was admin-istered. The degree
of protection may be described interms of the following
equation:
p CC E X 100,Cwhere P is the degree of protection in per cent, C
thecontrol drop in vital capacity produced by administrationof the
bronchospastic substance (before the protectingdrug is given), and
E the drop similarly produced at anytime after the protecting agent
has been administered.These percentage values may then be massed
into aver-ages derived from several experiments on different
asth-matic subjects. Determination of such averages is neces-sary,
for we have repeatedly encountered single protec-tion studies, or
even repeated studies in the same indi-vidual, which were at
variance with the average of resultsobtained by employing the same
drugs in many experi-ments carried out on many individuals.
RESULTS
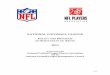
1. Epinephrine hydrochloride. Epinephrine hy-drochloride 1:
1000, 0.5 cc. subcutaneously, causethe usual side-reactions of
throbbing in the chestand head, uneasiness, tremor, etc. Protection
wasstriking, however, in that this dose afforded 100per cent
"immediate" (five to ten minutes afterinjection) protection against
intravenous hista-mine. This decreased gradually reaching a levelof
40 per cent after 143 minutes (Figure 1).This 40 per cent level has
previously (9) beenproposed as the minimum at which protectionmay
be considered significant, in view of the er-rors inherent in any
technique of clinical assay.Against the bronchospastic effects of
methacho-line, epinephrine hydrochloride 1: 1000, 0.5
cc.subcutaneously, provided 90 per cent immediateprotection and
maintained a significant level, over40 per cent, for 83 minutes.
These results arepresented in tabular form in Table II.
Subcutaneously administered epinephrine wasalso assayed against
the bronchospastic effect ofaerosols of histamine and methacholine
and dis-
1182
-
STUDY OF ADRENERGICAGENTSFOR RELIEF OF BRONCHOSPASM
TABLE I
Structural relationships of the sympathomimetic agents studied.
(Modifiedfrom Gunn [3])
CH-CH-NH
NEOSYNEPHRIN H OH H OH H CH3
EPINEPHRINE OH OH H OH H CH3
VAPONEFRIN OH OH H| OH H CH3
ISUPREL OH OH H OH H HCeCH3EPHEDRINE H H H OH CH3 CH3ORTHOXINE H
H OCH3 H CH3 CH3
Vaponefrin is a specially prepared racemic epinephrine.
played somewhat less, though still very effectiveprotecting
ability. Against histamine it showed70 per cent immediate
protection, which rose to apeak of 86 per cent at 40 minutes, and
maintaineda level greater than 40 per cent for 127 minutes.Less
protection against methacholine was againobserved; there was an
immediate level of 40 percent, rising to a peak of 51 per cent at
38 minutes,and remaining at a significant level for 72 minutes.
The 1: 100 dilution of epinephrine hydrochloride(10) was
dispensed in a glycerine-water solution,as were all other agents
employed as aerosolizedmists. Deep inhalations at ten-second
intervals
EPINEPHRINE HCL 1:100005CC. SC.
---SuSTAMINE IV CT~tIALS)-IECHOLYL IV (IT*ALLS-*.-"STAM1NC
AERCWAiALS)-X -ECHOLYL AZRC4TMIALS)
100-
U
° 0: so-0
V ~~ ~~~~.S,jl %, '4
N 0%+ 41
were administered with a standard Vaponefrinhand-bulb nebulizer
until six were completed.Against intravenous histamine 75 per cent
im-mediate protection was observed. The signifi-cant level of 40
per cent lasted for 28 minutes.Against intravenous methacholine
there was 56per cent immediate protection and an 18 minuteduration
of the 40 per cent level (Figure 2).
The protective capacity of epinephrine aerosolappeared slightly
greater when assayed againstnebulized bronchospastic agents. There
was 89per cent immediate protection and 36-minuteduration of the 40
per cent level against histamine;
100-
z0F-U
0IL -
-4
I I I I I I *- I I I I I I I
30 00 90 120 ISO 30 60MINUTES P PROTECTING DRUG
1% NEOSYNEPHRINCQ3 CC. S.C.)___ MSTAMPICMCSTRIALSW- MECHOLYLK(4
TWALS
-I I IN ,I I '-.I Z 3 4
HOURSF PROTECTING DRUG
FIG. 1. THE PROTECTION AFFORDEDAGAINST HISTAMINE AND
METHACHOLINE (REFERRED TO ABOVE ASMECHOLYL) BY 0.5 CC. OF
EPINEPHRINE HYDROCHLORIDE1: 1000, AND 0.3 CC. OF 1 PER CENT
NEOSYNEPHRINADMINISTERED SUBCUTANEOUSLY
1183
-
ELLIOTT BRESNICK, JOHN F. BEAKEY, LEON LEVINSON, AND MAURICE S.
SEGAL
TABLE II
Summary of the pertinent data obtained with the
phenylethylamines when tested against the bronchospastic effectsof
histamine and methacholine (referred to below as mecholyl)
BRONCHOCONSTRICTINGAGENTI *1 7
PROTECTING IMMEDIATE DURATION OF IMMEDIATE DURATION OF IMMEDIATE
DURATION OF IMMEDIATE DURATION orPROTEING PROTECTION IGNiFICANT (40
PROTECTION NIFICANT C40 PROTECTION SIGNIFICANT C40V PROTECTION
SIGNIFICANT (4¢X,DRUG (96) PROTECTION C(%) PROTECTION (96)
PROTECTION (26) PROTECTIONDRUG (6) I(MINUTES) (MINUTEs) (MINUTES)
(MINUTES)
PINEPHRINE 100 143 90 83 70 127 40 72EPINEPHRINE 75 28 56 IS 89
36 66 17
1:100 AER. __ _ _ _ __ _ _ _ __ _ _ _ _ _ _ _ _VAPONEFRIN 93 27
74 18 90 53 87 402.25 %_AER._____ ____NEOSYNEPHRIN 13 0 13 0
1:100, 0.3CC., S .NEOSYNEPHRIN 52 16 32 0
1:100 AER. __________
ISUPREL ~~98 82 91 811:100 AER. __________
| ISUPREL 708 22 69s 42 | 84 | 21 65s 25ISUPREL
I.200A HISTAMINE IVMEH 4YI2 HITAIEE.4EHOY2AR
1:00,oSUPRELs 100 30 56 1 8 ___
and 66 per cent immediate and 17-minute dura-tion of the 40 per
cent level against methacholine.These data are not, however,
significantly dif-ferent from those obtained with the
intravenousbronchospastics.
2. Vaponefrin.8 This is a 2.25 per cent solu-tion of a specially
prepared synthetic racemic epi-nephrine. Richards, Barach and
Cromwell (11)considered it preferable to the official 1: 100
solu-tion of epinephrine hydrochloride, which is thelevo-rotatory
isomer. We have compared theseaerosols elsewhere (12).
Using histamine intravenously we found thatsix deep inhalations
of Vaponefrin aerosol pro-vided 93 per cent immediate protection
and sig-nificant protection (over 40 per cent) lasting 27minutes.
Against intravenous methacholine weobtained an immediate level of
74 per cent and aduration of a significant level of 18 minutes.
Em-ploying the bronchospastics by nebulization re-sulted in no
greatly significant difference in in-tensity of action, 90 per cent
against histamine and87 per cent against methacholine. However,
the40 per cent level was maintained definitely longer,53 minutes
with histamine and 40 minutes withmethacholine (Figure 2). The
explanation forthis discrepancy is obscure; it may simply be dueto
inadequate sampling.
8 Kindly supplied by the Vaponefrin Co., Upper
Darby,Pennsylvania.
3. Neosynephrin. As may be seen from TableI, this drug differs
from epinephrine only in theabsence of the para-hydroxyl group on
the aro-matic portion of the molecule. The compoundsresulting from
removal of one or both hydroxylgroups are more stable but have
greatly decreasedinhibitory effects. Various investigators (11,
13-15) have found neosynephrin of little value as abronchodilator
although it may be an efficientbronchovasoconstrictor (14, 15).
Utilizing the 1: 100 solution of neosynephrin,we have studied
the protecting effect of the drugadministered by nebulizer and by
hypodermic in-jection. Our studies were limited to intravenoususe
of the bronchospastic agents. Figure 1 por-trays the
ineffectiveness of 0.3 cc. subcutane-ously, the level of protection
never exceeding 20per cent. Neosynephrin aerosol, 1: 100, in
theusual dose of six deep inhalations, proved some-what more
effective (Figure 2), displaying againsthistamine 52 per cent
immediate protection whichdropped below 40 per cent within 16
minutes.Against methacholine no significant protectivelevels were
attained, 32 per cent being the highestobserved.
4. Isuprel.9 This sympathomimetic amine,1- (3,4-dihydroxyphenyl)
-2-isopropylaminoethanoldiffers from epinephrine only in the alkyl
group
9Kindly supplied by Winthrop-Stearns, Inc., NewYork, New
York.
1184
HISTAMINE AER.HISTAMINE I.V MECHOLYL I.V. MECHOLYL AER.
-
1185STUDY OF ADRENERGICAGENTSFOR RELIEF OF BRONCHOSPASM
VAPONEFRIN6 INHALATIONS
---NHISTAIAR IV CS TRIALS I-MCC"OLYL IV CS TRTALS )-.-ViSTASMIC
AMCR4TRIALS )
-SICCOLVL ACR.C4 TMALS )
NEOSYNEPHRIN1% AEROSOL 6 INHAL-- STAMIrC 4soC4Tt^ALS )-MCCHOLVL
tV CS XIALS)
100-
z2I.- -u
50-0
U1
I4
I' I I I I T2 3 4 5 6
MMRI P PROTECTiNG MOU
.4.%16
+
+ 0
%%
I 9I I -I- I - I I 130 60 90
EPINEPPHRINE HCL 1 1006 INHALATIONS-"TAM.N *IV CS *WALS )
-"tEC'o"L IVCv MA*^S X--_ STAMM Atlt(4TM-ALS I_"tM-CcoOlVL AtKt4
**MALS 7A
100-
z
0
So
IL -
%0'0
*,'I
%
0%0%lp44
to.., %%"
I I* II* I * I I I30 00 00 120 ISO 30 a
MIurts f PRorECTING DRUG
FIG. 2. THE PROTECTIONNOTEDAGAINST HISTAMINE AND
METHACHOLINE(REFERRED TO ABOVE AS MECHO-LYL) BY NEBULIZED SOLUTIONS
OF EPINEIHRINE HYDROCHLORIDE(1: 100), VAPONEFRIN (2.25 PER CENT)
ANDNEOSYNEPHRIN(1 PER CENT)
attached to the nitrogen atom (Table I). It hasbeen demonstrated
that substitution on the aminonitrogen of branched alkyl groups,
particularlyisopropyl (as in Isuprel) and terbutyl,
producescompounds with enhanced sympathin I-mimeticproperties (4-7,
16). The specific structure ofthe substituted alkyl group is also
important ininfluencing the inhibitory potency of such
com-pounds.
The clinical efficacy of Isuprel has been previ-ously reviewed
by Segal and Beakey (17, 18),who introduced its use in this
country. Cohenand Van Bergen (19) have found Isuprel a
mosteffective antagonist of methacholine-inducedbronchospasm in
animals and of spontaneousasthma in man.
Wehave employed a 1: 50,000 dilution of Isu-prel intravenously
in a few subjects with variableresults. Occasionally the most
dramatic possiblecomplete relief of clinical asthma has been
noted,while a dose of 0.25 cc. (0.005 mgm.) was still be-ing
administered. The effect persisted for a mat-ter of hours. In other
instances relief was onlypartial and transient after intravenous
administra-tion of 0.25 cc. (0.005 mgm.) to 0.5 cc. (0.01mgm.),
even in repeated doses. The 0.25 cc.dose caused a uniform increase
of 20-30 beatsper minute in the heart rate. All patients
ex-perienced unpleasant, although not alarming, pal-pitations. The
0.5 cc. dose, on the other hand,accelerated the pulse by 50 beats
per minute andcaused uneasiness and alarming palpitations. The
100-
so-
.4'
'4
'4'4
'4'4
4.4.
I * I120 Iso 30 6o0
MINUTES P PROTECTING DRUGIo I
-
ELLIOTT BRESNICK, JOHN F. BEAKEY, LEON LEVINSON, AND MAURICE S.
SEGAL
effect on blood pressure was minimal. The doseof 0.005 mgm.
appeared to cause a small increasein systolic pressure
(approximately 10 mm. ofmercury), probably due mainly to the
increasedrate. There appeared to be, in general, a tend-ency toward
a slight fall in the diastolic level.The larger dose, 0.01 mgm.
(0.5 cc.), caused atransient drop in systolic and diastolic levels
si-multaneous with the greatest increase in heartrate. We performed
several protection studiesusing this very dilute solution of
Isuprel intra-venously. Doses of 0.25 cc. (0.005 mgm.) and0.5 cc.
(0.01 mgm.) failed to demonstrate any pro-tective ability against
histamine or methacholinefor long enough periods to be measured by
themethod employed.
Isuprel 1:100, the dilution commonly employed
with epinephrine, provided essentially completeimmediate
protection against intravenous hista-mine and methacholine (98 and
91 per cent re-spectively). Not only did it maintain a signifi-cant
(40 per cent) protection against histaminefor 62 minutes, but it
also afforded a surprising81-minute duration against methacholine
(Figure3). However, this dilution of Isuprel frequentlycaused
unpleasant epinephrine-like side-effects.
Isuprel 1:200 is the dilution in common usefor nebulization. It
is, of course, one-half as con-centrated as the usual epinephrine
solution andequivalent to approximately one-third the
con-centration of levo-epinephrine in Vaponefrin.This dilution of
Isuprel displayed (Figure 3) 70per cent immediate protection
against intrave-nous histamine with a duration of 22 minutes
for
ISUPRELt5OOO 05C.C. SC.--4IISTAMIN AI.V. (6 TRIALS )-MECHOLYL
1.1 C( TRIALS )
z0F
A
o\
II
II ' WII I I- F I I90 120 ISO ISO
PROTECTING DRUG
ISUPR EL1IOOAEROSOL 6 INHAL---HISTAMINE I.V. (RTAIALS )-MCCHOLYL
IV. (6 TRIALS )
100-
2
0 o
6IW
2 3 4
HSP PROTECTING DRUG
ISUPREL20XMGMSUBUNGUAL---HISTMAGNE IV. (S TUALS)-MECMYL I.V. (4
TRIALS)
HOURS PROTECTING DRUG
ISUPREL 1:2006 INHALATIONS
-01VAMINE I.V. C? TNALS )-MECt4OLL LV. C(TRCALS )_-tgtSTAMIKE
AEft (4TRIAL S)
z ~~~~~~~-X-MiCC HOLES ACR CS TWA&LS
so4
0% ''b
\ %.
30 60 90 30
MINUTES P PROTECTING DRUG
FIG. 3. THE PROTECTIVE CAPACITY OF ISUPREL ADMINISTERED BY
VARIED ROUTESAND IN VARIED AMOUNTSAGAINST HISTAMINE AND
METHACHOLINE(REFERRED TO ABOVE AS MECHOLYL)
1186
100-
z
I- -v
10
z2I-1
0
30 60MINUTES F
I
-
STUDY OF ADRENERGICAGENTSFOR RELIEF OF BRONCHOSPASM
significant levels. Against intravenous metha-choline, there was
a 69 per cent immediate leveland significant levels persisted for
42 minutes.As may be seen in Table II, the data were, withone
exception, essentially equivalent when thebronchospastics were
employed in the form ofaerosols. An immediate level of 84 per cent
anda 21-minute duration of significant protection werefound against
histamine; and 65 per cent with 25minutes were the comparable
values for metha-choline. The only discrepancy appears in
theduration of levels over 40 per cent against metha-choline
administered intravenously and as anaerosol. This, again, may be
due to inadequatesampling and the consequent chance inclusion
ofpatients with extreme differences in responsive-ness to
Isuprel.
An average dose of the 1: 5000 dilution ofIsuprel for
subcutaneous injection is 0.5 cc. Thisdose was assayed against
intravenous histamineand methacholine (Figure 3). Weobtained
com-plete (100 per cent) immediate protection againsthistamine and
a continuation of significant levelsfor 30 minutes. Less
anticholinergic effect wasnoted with this preparation, for the
initial inten-sity was only 56 per cent, and it dropped to 40
percent in 18 minutes.
Sublingual tablets of Isuprel, although they havebeen moderately
effective clinically in occasionalpatients, have not proved to be
an adequate sub-stitute for a nebulizer in most cases. We
haveperformed protection studies with these tabletsin doses of 20
mgm. (two tablets) against hista-mine and methacholine administered
intrave-nously. Against histamine, significant levels ofprotection
were not attained, and a peak of 38 percent was reached in 27
minutes. Against metha-choline the results were very similar
although the40 per cent level was reached in 12 minutes afterthe
tablets dissolved under the tongue. (Time fordissolution was
usually two to three minutes.)The total duration of levels over 40
per cent was23 minutes. However, the peak level, attained24 minutes
after dissolution of the tablets, wasonly 44 per cent. These data
are presentedgraphically in Figure 3.
5. Ephedrine. From Table I it may be seenthat ephedrine is
lacking in the hydroxyl groupson the benzene ring, and possesses an
additionalmethyl group attached to the alpha-carbon atom.
Clinically it has longer, less intense action thanepinephrine;
it is active orally.
In our studies, employing the usual oral doseof 25 mgm.
(administered several hours after thesubject's last meal), there
was a delay of 81 min-utes before a protection level of 40 per cent
wasreached against histamine (Figure 4). A peaklevel of 57 per cent
was attained at 120 minutes.Significant levels of 40 per cent or
over weremaintained for 108 minutes, or until slightly overthree
hours after the drug was taken. Againstmethacholine, no significant
levels of protectionwere reached. The peak level was only 32
percent, occurring 60 minutes after ingestion of thetherapeutic
agent.
100-
2
- -85-530-0
O0.
100-
z2_I5-UhI0 .
EPHEDRINE SULFATE(25 MGM. PO.)----HISTAMINE SV (4
TRIALS)-MCCHOLYL LV. -(4 TRIALS)
I 44
I I I I I I1 2 3 4
HOURS P PROTECTING DRUG
I I I I5 6
ORTHOXINE200 MGM. P.O.--4HISTAMINC IVI4TRIALS-%CCHOLYI. IV
(6TRIALS)
_-_
*4%
5%4%
", -1 I I I I I I I I I I |' I1 2 3 4 5 6
HOURSP PROCTING DLIG
FIG. 4. THE PROTECTINGABILITY OF ORALLY ADMIN-ISTERED
EPHEDRINESULFATE (25 MGM.) AND ORTHOXINE(200 MGM.) AGAINST
HISTAMINE AND METHACHOLINE(REFERRED TO ABOVE AS MECHOLYL)
1187
-
ELLIOTT BRESNICK, JOHN F. BEAKEY, LEON LEVINSON, AND MAURICE S.
SEGAL
6. Orthoxine.10 This synthetic amine differsfrom ephedrine in
the absence of the beta-hydroxylgroup and the presence of a methoxy
radical in theortho position.
Wehave made a clinical trial in approximately20 patients with a
dose of 100-200 mgm. three tofour times daily. In general it proved
to be oflittle benefit in preventing severe asthmatic at-tacks,
although one patient obtained moderate re-lief and one noted marked
improvement. Side-effects were observed by many patients and
variedamong anorexia, nausea, light-headedness, dizzi-ness and
drowsiness. Only one patient complainedof the ephedrine-like effect
of insomnia. Thesyrup of orthoxine has been tolerated fairly
welland appears to give clinical relief from troublesomecough in
some patients.
In protection studies against intravenous hista-mine, orthoxine,
in a dose of 200 mgm. orally,was apparently rapidly absorbed, for
it displayed49 per cent protection at 57 minutes. In addition,this
proved to be the peak level attained inasmuchas the protective
capacity dropped very graduallyto 40 per cent at 165 minutes after
ingestion ofthe drug. The total measured duration of signifi-cant
protection was 108 minutes. Against metha-choline, a 40 per cent
level was never reached.The peak attained was 38 per cent at 120
minutes.These figures for orthoxine, graphically presentedin Figure
4, obviously are very closely similar tothose for ephedrine.
SUMMARYAND CONCLUSIONS
1. Five well-known sympathomimetic aminesand one new one have
been studied with respectto their protective capacity against the
broncho-spastic effects of histamine and methacholine insensitive
asthmatic patients.
2. No consistent difference in results was ob-served whether the
bronchospastic agents wereadministered intravenously or as
aerosols.
3. Epinephrine hydrochloride 1: 1000, 0.5 cc.subcutaneously,
protected as well as or better thanthe other agents tested and
afforded greater dura-tion of significant protection. However, its
cardi-ovascular and central nervous stimulating side-reactions
proved disagreeable.
10 Kindly supplied by The Upjohn Co., Kalamazoo,Michigan.
4. Isuprel 1: 100 aerosol (double the usualstrength), six
inhalations, was comparable to thesubcutaneously administered
epinephrine, particu-larly in anticholinergic effect, although it
protectedless than half as long against histamine. This,too, caused
undesirable side-effects.
5. Of the three most commonly employed solu-tions for
nebulization, Vaponefrin, 2.25 per cent,appeared to have a slightly
greater antihistaminicprotecting ability than Isuprel 1: 200 and
epi-nephrine 1: 100. The latter two were of approxi-mately equal
efficacy as antihistaminics. Isuprel1: 200 demonstrates greater
anticholinergic pro-tecting ability than either of the other two
prepa-rations.
6. Neosynephrin was quite ineffective when in-jected
parenterally and of only slight value by theinhalatory route.
7. Sublingually administered Isuprel, in a doseof 20 mgm.,
proved to have little protective ca-pacity against the
bronchospastic effects of hista-mine and methacholine. It was
occasionally ofmoderate value clinically when administered bythis
route.
8. Isuprel 1: 5000, 0.5 cc. subcutaneously, dis-played excellent
though brief protecting abilityagainst the bronchospastic effects
of histamine andconsiderably less effectiveness against
metha-choline.
9. Isuprel 1: 50,000 could not, because of cardi-ovascular
side-effects, be injected intravenouslyin doses sufficient to
effect measurable protection.Doses of 0.25 cc. and 0.5 cc. (0.005
to 0.01 mgm.)occasionally proved dramatically effective in
allevi-ating clinical asthma, although it usually was lesseffective
and quite transiently so.
10. A new sympathomimetic amine,
orthometh-oxy-beta-phenylisopropyl methylamine hydrochlo-ride
(Orthoxine, Upjohn), of the class of ephed-rine, was studied and
appeared quite similar to thelatter in protecting capacity. Brief
clinical trialindicated that the ortho-methoxy group may
oc-casionally reverse the central stimulation of ephed-rine.
ACKNOWLEDGMENT
We are indebted to Dr. H. J. Rubitsky for carryingout several
protection study tests in this series.
1188
-
STUDY OF ADRENERGICAGENTSFOR RELIEF OF BRONCHOSPASM
BIBLIOGRAPHY
1. Goodman, L., and Gilman, A., The PharmacologicalBasis of
Therapeutics. The Macmillan Co., NewYork, 1941.
2. Barger, G., and Dale, H. H., Chemical structure
andsympathomimetic action of amines. J. Physiol.,1910, 41, 19.
3'. Gunn, J. A., The pharmacological actions and thera-peutic
uses of some compounds related to adrena-line. Brit. M. J., 1939,
2, 155.
4. Siegmund, 0. H., Granger, H. R., and Lands, A. M.,The
bronchodilator action of compounds struc-turally related to
epinephrine. J. Pharmacol. &Exper. Therap., 1947, 90, 254.
5. Lands, A. M., Nash, V. L., McCarthy, H. M.,Granger, H. R.,
and Dertinger, B. L., The pharma-cology of N-alkyl homologues of
epinephrine. J.Pharmacol. & Exper. Therap., 1947, 90, 110.
6. Marsh, D. F., Pelletier, M. H., and Ross, C. A.,The
comparative pharmacology of the N-alkyl-arterenols. J. Pharmacol.
& Exper. Therap., 1948,92, 108.
7. Lands, A. M., Nash, V. L., Dertinger, B. L.,Granger, H. R.,
and McCarthy, H. M., Thepharmacology of compounds structurally
related tohydroxytyramine. J. Pharmacol. & Exper. Therap.,1948,
92, 369.
8. Segal, M. S., Beakey, J. F., Bresnick, E., and Levin-son, L.,
Evaluation of therapeutic substances em-ployed for the relief of
bronchospasm. Bull. NewEngland M. Center, 1948, 10, 21.
9. Levinson, L., Beakey, J. F., Bresnick, E., and Segal,M. S.,
Evaluation of therapeutic substances em-ployed for the relief of
bronchospasm. II. His-torical development and methods. Ann.
Allergy,1948, 6, 705.
10. Graeser, J. B., and Rowe, A. H., Inhalation of epi-nephrine
for the relief of asthmatic symptoms.J. Allergy, 1935, 6, 415.
11. Richards, D. W., Jr., Barach, A. L., and Cromwell,H. A., Use
of vaporized bronchodilator solutions inasthma and emphysema. A
continuous inhalationmethod for severe asthmatic states. Am. J.
M.Sc., 1940, 199, 225.
12. Segal, M. S., Beakey, J. F., Bresnick, E., and Levin-son,
L., A comparison of various sympathomimeticamines in counteracting
the dyspnea and broncho-spasm induced by histamine and
acetyl-beta-methyl-choline. J. Allergy, 1949, 2G, 97.
13. Graeser, J. B., Inhalation therapy of bronchialasthma. J. A.
M. A., 1939, 112, 1223.
14. Barach, A. L., Physiological methods in the diagnosisand
treatment of asthma and emphysema. Ann.Int. Med., 1938, 12,
454.
15. Burrage, W. S., Recent therapeutic trends in allergy.New
England J. Med., 1948, 238, 181.
16a. Konzett, H., Neue broncholytisch hochwirksameKbrper der
Adrenalinreihe. Arch. f. exper. Path.u. Pharmakol., 1940, 197,
27.
b. Konzett, H., Zur Pharmakologie neuer adrenalin-verwandter
K6rper. Ibid., 1940, 197, 41.
17. Segal, M. S., and Beakey, J. F., The use of isuprelfor the
management of bronchial asthma. Bull.New England M. Center, 1947,
9, 62.
18.ISegal, M. S., and Beakey, J. F., Management ofbronchial
asthma; the use of 1- (3',4'-dihydroxy-phenyl)
-2-isopropylaminoethanol. Ann. Allergy,1947, 5, 317.
19. Cohen, E. N., and Van Bergen, F., Isuprel, a
newbronchodilating agent. Bull. Univ. of Minn. Hos-pitals &
Minn. Med. Foundation, 1948, 19, 424.
1189