Embed Size (px)
Citation preview

CLINICAL ARTICLEJ Neurosurg 128:1235–1240, 2018
ChroniC neuropathic pain after peripheral nerve in-jury is a major clinical problem that is often misdi-agnosed, especially after iatrogenic insult. Severe
persistent neuropathic pain (score of > 5 of 10 on the visual analog scale [VAS]) is reported to occur in 5%–10% of pa-tients after thoracotomy, breast surgery, or sternotomy; in 2%–4% after inguinal hernia repair; and in 4% after cae-sarean section.15 However, physicians have little awareness of its occurrence. The diagnosis is often delayed, as is ap-
propriate therapeutic care.5 Etiologies of neuropathic pain are multiple and include compression syndromes, diabetes, and viral infections in addition to trauma.7 Development of severe and persistent pain due to a neuroma is unusual;23 the presence of a neuroma is thought to be necessary for the development of pain but the presence of a neuroma is not always associated with neuropathic pain.15,17 In cases of neuropathic pain, peripheral nociceptors are in a state of continual excitability that, in turn, induces chemical and
ABBREVIATIONS VAS = visual analog scale.SUBMITTED July 5, 2016. ACCEPTED January 5, 2017.INCLUDE WHEN CITING Published online June 16, 2017; DOI: 10.3171/2017.1.JNS161778.
Evaluation of surgical treatment for neuropathic pain from neuroma in patients with injured peripheral nervesValérie Decrouy-Duruz, MD, Thierry Christen, MD, and Wassim Raffoul, MD
Department of Plastic and Hand Surgery, University Hospital of Lausanne, Switzerland
OBJECTIVE Chronic neuropathic pain after peripheral nerve injury is a major clinical problem. Its management is dif-ficult, and therapeutic approaches vary and include oral medication, neurostimulation, and surgery. The aim of this study was to assess the adequacy of surgical nerve revision in a large series of patients with long-term follow-up.METHODS The authors reviewed the charts of 231 patients (335 nerve injuries) who experienced neuropathic pain after peripheral nerve injury and underwent surgery for nerve revision at the authors’ institution between 1997 and 2012. The following parameters were recorded for each patient: history, location, duration, and severity of the pain and details of nerve revision surgery. In addition, patients were invited to participate in a follow-up consultation and were asked to score their pain at that time. Current medications and examination findings were also documented.RESULTS Elective surgery was the source of nerve injury for 55.4% of the patients. The lower extremity was the most commonly involved anatomical region (54.3%), followed by the lower abdomen (16.4%) and the thoracic region (13%). The mean time between the onset of injury and revision surgery was 48 months. On average, 1.3 injured nerves per patient were explored, and surgery was performed 1.2 times per patient. Each nerve underwent revision 1.1 times on average. Neuromas-in-continuity and scar-tethered nerves were observed in 205 nerves (61%) and terminal neuromas were observed in 130 nerves (39%). The authors performed 186 (56%) neurolyses and 149 (44%) neuroma resections and translocations. The mean follow-up of the 127 (55%) patients who agreed to come back for a consultation was 68 months. These patients indicated an average pain decrease of 4 points in the visual analog scale (VAS) score. Pain relief greater than a 2-point decrease on the VAS, a criterion for a successful treatment according to the European Federation of Neurological Societies guidelines, was encountered in 80% of patients. Pain relief did not vary in a statistically signifi-cant way with regard to surgical technique, age and sex of the patient, affected nerve, or time between trauma and sur-gery. Before surgery, 76% of the patients were on a regimen of paracetamol and/or NSAIDs and 44% received opiates, while after nerve revision only 37% still required simple analgesia and 14% needed opiates.CONCLUSIONS Bearing in mind that medication achieves satisfying pain relief in only 30%–40% of patients with neuropathic pain, surgery must be considered as an effective alternative therapy. No objective criteria were shown to be factors of poor prognosis. Systematic preoperative clinical mapping of the injured nerves and diagnostic nerve blocks could improve the primary success rate of the surgery.https://thejns.org/doi/abs/10.3171/2017.1.JNS161778KEY WORDS peripheral nerve injury; neuroma; neuropathic pain; surgical management; neurolysis
J Neurosurg Volume 128 • April 2018 1235©AANS 2018, except where prohibited by US copyright law
Unauthenticated | Downloaded 06/01/20 06:52 AM UTC

V. Decrouy-Duruz, T. Christen, and W. Raffoul
J Neurosurg Volume 128 • April 20181236
anatomical changes in the cortical centers.5,15,22 Factors such as age and sex, genetic susceptibility, and psycho-social context might influence this central sensitization, a process leading to chronic pain.8,15
Therapeutic strategies are varied and often involve a multidisciplinary team (i.e., physical therapists, pain doc-tors, psychiatrists/psychologists, and surgeons). The first-line therapy is often medication (tricyclic antidepressants, selective serotonin norepinephrine reuptake inhibitors, and anticonvulsants). Stimulation of large afferent nerve fibers via a transcutaneous electrical nerve stimulator (TENS) or a spinal cord stimulator may help relieve pain in some patients.
Surgical management of neuropathic pain after pe-ripheral nerve injury is well known, and neurolysis and neuroma resection with translocation have been practiced for decades. Nonetheless, there are few scientific reports of neuromas after peripheral nerve injury, with the excep-tion of those involving the upper limb, for which Dellon and Mackennon9,18,19 as well as Elliot et al.2,3,10 have helped establish valuable recommendations regarding surgical techniques.
We have been regularly confronted at our institution with patients who experience neuropathic pain after pe-ripheral nerve injury in various body parts. We developed a treatment algorithm and wish to report our experience.
MethodsAfter obtaining institutional review board approval, we
reviewed the charts of all patients who experienced neu-ropathic pain after peripheral nerve injury and underwent surgery for nerve revision at our institution between 1997 and 2012. Neuropathic pain was defined as pain caused by a lesion or disease of the somatosensory nervous system.14
The quality of the pain had to be reported as one or more of the following terms: burning, tingling, sharp, or stabbing. Clinical examination had to show one or more of the following: anesthesia, hypesthesia, allodynia, hyperal-gesia, dysesthesia, or positive Tinel’s sign. The pain had to be resistant to pain medication. The intensity (scored on a VAS) and the duration of pain were not criteria. Patients with persistent pain after limb amputation were excluded because of the unclear boundary between painful neuro-ma and phantom pain.
In some instances, patients were referred by pain doc-tors after they responded to an anesthetic local nerve block, whereas others were selected after clinical exami-nation only. Preoperative nerve blocks were performed in a minority of patients; therefore, their efficiency as a pre-dictor of favorable outcome was not assessed.
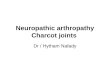
All operations were performed by the senior author. The following parameters were recorded for each patient: history, location, duration, and severity of the pain (VAS Score 0–10) and details of nerve revision surgery. Neuro-mas were classified as a terminal neuroma or a neuroma-in-continuity; the latter category included scar-tethered nerves as defined by Elliot and Sierakowski.10 Surgery consisted of either neurolysis or neuroma resection and translocation. All translocations were done in adjacent soft tissues (i.e., submuscular or subfascial) (Fig. 1).
All patients were informed of the present study by mail and were telephoned a few weeks later to invite them to participate at a follow-up consultation. This consultation was performed by an independent surgeon (first author). At the follow-up consultation, patients were asked to score their pain at that time, using a VAS, as well as their sat-isfaction with the treatment. As the linearity of the VAS is a subject of debate,20 we chose to report the number of points of improvement instead of the percentage of im-provement. Current medications and examination findings were also documented. When a patient required multiple operations for the same nerve or an adjacent one, the final result was considered to be the one after the last operation.
Descriptive data are expressed either as the mean or as the median with range values when adequate. Percentages are given when appropriate. Data were analyzed using the chi-square test, the Student t-test, and Fisher’s exact test.
ResultsTwo hundred thirty-one patients were included in the
study, representing a total of 335 nerve injuries. There were 132 women (57%) and 99 men (43%) with an average age of 47 years (range 13–85 years). The lower extremity was most commonly involved (54.3%), followed by the abdom-inal and groin regions (16.4%), thoracic region (13%), up-per extremity (11%), head (3%), back (1%), and perineum (1%) (Table 1). Nerve injury occurred after elective surgery in 128 patients (55.4%) and posttraumatic surgery in 65 pa-
FIG. 1. Case example. Branch of the superficial peroneal nerve with terminal neuroma (left) that is resected and translocated in adjacent submuscular tissue (right). Figure is available in color online only.
Unauthenticated | Downloaded 06/01/20 06:52 AM UTC

Evaluation of surgical treatment for painful neuroma
J Neurosurg Volume 128 • April 2018 1237
tients (28%). Crush injury with no associated surgery was noted in 38 patients (16.5%). Table 2 shows the distribution of the affected anatomical regions according to the cause of the nerve injury. The mean time between the onset of injury and revision surgery was 48 months (range 1–531 months, median 27 months). Patients underwent explora-tion of an average of 1.3 injured nerves and underwent surgery a mean of 1.2 times. More precisely, 194 (84%) patients underwent only 1 surgery, 31 (13.4%) had 2 sur-gical procedures, 3 (1.3%) had 3 surgeries, and 3 (1.3%) had 4 surgeries. Each nerve underwent revision surgery 1.1 times on average. Of the 335 nerves that were explored,
205 (61%) showed a neuroma-in-continuity or a scar-teth-ered nerve and 130 (39%) a terminal neuroma. One hun-dred eighty-six (56%) neurolyses and 149 (44%) neuroma resections and translocations were performed.
Patients With Follow-UpAmong the 231 patients, 127 (55%) came back for a
follow-up consultation. This sample is representative of the overall study population, in terms of both demograph-ic and operative criteria (Table 3). Among patients lost to follow-up, 93 were unreachable, 6 had died, and 5 refused to participate. The mean follow-up period was 68 months (range 6–191 months). Before revision surgery, 67 patients (53%) had consulted a pain doctor, 35 (28%) a neurologist, and 22 (17%) a psychiatrist. The median preoperative VAS score in these patients was 8 (range 2–10); at the time of the follow-up consultation, the score was 3 (range 0–10). The pain score improved by at least 4 points in 50% of the patients, by at least 3 points in 67%, and by at least 2 points in 80% (Table 4). Pain relief did not vary in a statistically significant way in relation to patient age and sex, affected nerve, or time between trauma and surgery. By studying a subset of the population including only the patients who underwent 1 operation on a single nerve (n = 80), pain relief (4-point decrease) was not significantly different be-tween patients after neurolysis or neuroma resection and translocation.
Two patients (1.6%) reported a higher postoperative score on the VAS (+1). Before surgery, 96 patients (76%) were on a regimen of paracetamol and/or NSAIDs and 56 (44%) required opiates, while after the nerve revision only 47 (37%) still required simple analgesia and 17 (14%) opi-ates. One hundred eighteen patients (93%) presented with local allodynia preoperatively versus 48 (38%) postoper-atively. The average satisfaction score out of 10 was 5.6 (range 0–10).
DiscussionThis series reflects the great diversity of patients suffer-
ing from neuropathic pain after nerve injury and the mul-tiple nerves that can be involved. Nerves of the lower ex-tremity were most commonly affected (54.5%), whether in the case of trauma or after elective surgery. This finding is similar to the number of iatrogenic injuries involving the lower extremity (41.3%) reported by Kretschmer et al.16 Neuromas in the upper extremities have been treated with
TABLE 1. Number of affected nerves that underwent surgical treatment, according to the anatomical region
Anatomical Region & Nerve No. of Nerves
Lower extremity Sural 49 Saphenous 37 Superficial peroneal 30 Lateral femoral cutaneous 23 Deep peroneal 18 Common peroneal 12 Femoral 7 Sciatic 4 Tibial 2Abdomen & groin Ilioinguinal 28 Iliohypogastric 15 Genitofemoral 12Upper extremity Radial 15 Ulnar 12 Median 5 Suprascapular 3 Musculocutaneous 2Thorax Intercostal 36 Intercostobrachial 7 Long thoracic 1Head Occipital 3 Mental 2 Hypoglossal 1 Great auricular 1 Supraorbital 1 Trigeminal 1Back Lumbar 4Perineum Pudendal 3 Coccygeal 1Total 335
TABLE 2. Distribution of anatomical regions according to the cause of the nerve injury
Anatomical Region
Elective Surgery
Posttraumatic Surgery
Crush Injury w/ No Associated
Surgery
Lower extremity 39.2 68.8 65.8Abdomen & groin 30.4 (17.6 + 12.8) 0 2.6Thorax 15.2 1.5 5.4Upper extremity 8 29.7 13.1Other 7.2 0 13.1
Values are percentages.
Unauthenticated | Downloaded 06/01/20 06:52 AM UTC

V. Decrouy-Duruz, T. Christen, and W. Raffoul
J Neurosurg Volume 128 • April 20181238
nerve revision for some time, and there has been increas-ing awareness of neuropathic pain in the lower extremi-ties. In contrast, it is likely that abdominal neuropathic pain is less frequently diagnosed and might be mistaken for psychosomatic pain. Selection bias due to underdiag-nosis cannot be excluded, and our numbers should not be interpreted as the actual incidence of painful neuromas related to an anatomical region.
The mean time between the onset of injury and revision surgery was 4 years, which might seem excessively long. However, Atherton et al. reported a latency of 3 years and 9 months in the management of 46 nerve injuries of the hand;3 Zacest et al. reported a similar period (3 years and 11 months) in a study of 26 patients with painful neuromas after inguinal hernia repair.24 There are several possible reasons for delay between injury and surgery, one of which is that neuropathic pain remains an unfamiliar entity, and another that physical therapy and pain medication are usu-ally the first line of treatment. Nath and Mackinnon have suggested surgical treatment if conservative treatment has failed after 6 months.21 Although this study does not show any correlation between the elapsed time before nerve re-vision and successful pain relief, one could only wish to shorten this delay.
An average of 1.3 nerves were explored per patient, each of which was revised an average of 1.1 times. Some patients harboring terminal neuromas that benefited from resection and translocation had to undergo revision sur-gery because of recurrent pain in the relocation site. El-liot and Sierakowski,10 in their experience, suggested that neuromas-in-continuity of small sensory nerves should be treated with resection and translocation because neurolysis alone is less effective. In cases of neuromas-in-continuity on larger nerves, the authors proposed fascial flap wrap-ping.10 Over the years, the senior author of our study has developed an algorithm based on his personal experience. Neurolysis is performed in cases of neuroma-in-continuity on a major nerve irrespective of the degree of severity of the lesion as well as on a small sensory nerve that appears mildly constricted and with preserved adjacent vascular-ization (probably corresponding to a “scar-tethered nerve,” as termed by Elliott and Sierakowski10). When sensory nerves appear to be severely damaged or the nerves are very superficial, neuroma resection and translocation is the preferred option. Our preferred surgical technique for each of the most commonly involved nerves is shown in Table 5.
In our study, since all affected nerves were not always explored during the first procedure, each patient had to un-dergo surgery an average of 1.2 times. Mackinnon and Del-lon have shown overlap of the innervated territories of the superficial radial nerve and lateral antebrachial cutaneous nerve in 75% of cadaveric and clinical dissections.18 In an-other study, they reported that their patients’ pain symptoms improved after simultaneous resection and relocation of both nerves into the brachioradialis muscle.9 Such overlap is found in other anatomical regions, such as the knee, groin, and thoracic regions. This could explain the necessity of performing multiple surgeries before achieving pain relief.
A subset of patients was available for a long-term fol-low-up consultation. Pain improvement in these patients was highly variable (10- to 0-point decrease on the VAS [in all but 1 patient]). However, half of the patients had pain relief scored as a decrease of 4 or more points and two-thirds a decrease of at least 3 points. This result cannot be directly compared with others because of a lack of similar studies. Burchiel et al. reported ≥ 50% pain relief in 40% of 40 patients with painful traumatic neuromas (information regarding location was not reported) who were treated by either neurolysis or neuroma resection and translocation.6 Another study reported partial or complete pain relief in VAS scores in 66.7% of 19 patients after neurectomy of ilioinguinal nerves for chronic pain.24 Finally, Kretschmer et al. reported pain relief or motor improvement in 70% of 126 patients with iatrogenic nerve injuries after repair.16 In evidence-based studies on pain, it is customary to consider “responders” to treatment to be the patients who report pain relief of greater than 50%. The European Federa-tion of Neurological Societies guidelines pointed out that only 30%–40% of the patients with chronic neuropathic pain achieved that target with pharmacotherapy.4,8,12 It was thereby proposed that a clinically meaningful reduc-tion of chronic pain in placebo-controlled trials would be a 2-point decrease or 30% pain reduction on a 0–10 nu-meric rating scale.4,11 Although the present study is neither
TABLE 3. Comparison between overall study population and the patients with follow-up
Variable
ValueOverall Study
PopulationPatients w/ Follow-Up
Sex Female 132 (57) 75 (59) Male 99 (43) 52 (41)Mean age in yrs 47.2 47Ratio no. nerves/no. patients 1.45 1.5Anatomical region Lower extremity 182 (54.5) 111 (57.5) Abdomen 55 (16.5) 35 (18.1) Thorax 44 (13) 20 (10.4) Upper extremity 37 (11) 16 (8.3) Head 9 (3) 5 (2.6) Back 4 (1) 3 (1.55) Perineum 4 (1) 3 (1.55)Nerve injury etiology Elective surgery 128 (55.5) 70 (55) Posttraumatic surgery 65 (28) 39 (31) Crush injury w/ no associated surgery 38 (16.5) 18 (14)Type of lesion Neuroma-in-continuity 205 (61) 127 (66) Terminal neuroma 130 (39) 66 (34)Surgical technique Neurolysis 186 (56) 112 (58) Neuroma resection & translocation 149 (44) 81 (42)Mean delay btwn lesion & surgery in mos 48 47
Values are presented as the number of patients (%) unless stated otherwise.
Unauthenticated | Downloaded 06/01/20 06:52 AM UTC

Evaluation of surgical treatment for painful neuroma
J Neurosurg Volume 128 • April 2018 1239
randomized nor placebo controlled, contribution of surgi-cal management to pain relief seems likely, as 80% of our patients experienced a minimum decrease of 2 points on the VAS. The other point supporting the relevance of sur-gery is that the treatment is aimed to be curative and not palliative (i.e., unlike treatment with pharmacotherapy and nerve stimulators). In our study, two-thirds of patients were able to stop receiving opiate medication, while half dis-continued simple analgesia. It should be kept in mind that neuropathic pain might be seen in association with pain related to other causes, such as orthopedic pathologies.
Our results are poorer than those reported by the groups of Elliot and Dellon in numerous homogeneous case series on neuromas of the upper extremity.2,3,10,13,19,23 Their results showed good-to-excellent outcomes in more than 80% of the cases. Statistical analysis of our data shows that suc-cess in pain relief did not vary depending on the site of the neuroma; that is, patients who underwent upper-extremity surgery had similar pain relief to that of patients who un-derwent surgery for a neuroma in a different anatomical region. However, in our case series, neuromas of the upper
extremity were all located on the sensory branch of the radial nerve, the dorsal branch of the ulnar nerve, or the palmar cutaneous branch of the median nerve. Surgery is known to be unpredictable and less successful for these nerves. Dellon and Mackinnon were able to improve sur-gery efficiency by stressing the importance of tracking a possible nerve territory overlap and performing nerve re-location in a muscle with reduced excursion.9,18
This study has not shown statistical superiority of one surgical technique over another. We see 2 possible ex-planations for this. First, there might be a selection bias due to the fact that neuroma resection and translocation was performed every time the neuroma was deemed to be severely pathological based on its appearance, except in cases of mixed nerves. Therefore, neuromas that were re-sected might have been those causing the worst symptoms with a potentially worse prognosis.
Second, failure of the surgery could be due to neuroma recurrence or to the lack of recognition of the multiplic-ity of the nerves involved. Preoperative local anesthesia of specific nerves is being performed more often to refine the diagnosis and evaluate the expected effectiveness of surgery.1,24 We have adopted this strategy, as all current pa-tients benefit from this diagnostic test. Interestingly, nega-tive findings on a preoperative local anesthesia test are not an absolute contraindication for Atherton and colleagues, who still perform surgery for neuropathic pain in the distal forearm.2 Furthermore, Mackinnon and Dellon19 pointed out that “excellent results” could still be achieved by reop-eration in patients who had undergone 3, or more, previous neuroma operations that had failed to completely relieve the problem of nerve pain. However, it remains unclear when one should discontinue performing additional nerve revisions in cases of persistent pain.
This study suffers from several limitations, the first of which is its retrospective nature. The large heterogene-ity of the nerves involved and the association of multiple variables are problematic since the outcomes of different nerves are compared. However, the variety of situations encountered reflects the reality and the need to propose treatment according to a case-by-case assessment, within a defined framework.
There is also a lack of systematic treatment since some patients underwent simple neurolysis while others under-went neuroma resection. Nevertheless we think that sur-gery should be tailored to each specific case.
TABLE 4. Rate of pain relief according to the preoperative VAS score
Preop VAS Score
Preop VAS Score − Postop VAS Score9–10 7–8 5–6 3–4 1–2 0 −1 Total (n = 127)
9–10 7.9% 2.4% 4.7% 6.3% 3.9% 3.1% — 29%7–8 — 7.9% 13% 12% 11% 5.5% — 49%5–6 — — 7.9% 1.6% 3.1% 0.8% 1.6% 15%3–4 — — — 3.1% 1.6% — — 4.7%1–2 — — — — 1.6% 1.6% — 3.1%
Total (n = 127) 7.9% 10% 25% 23% 21% 11% 1.6%
Values in the table correspond to the percentage of patients given their preoperative VAS score (grouped in 5 representative classes) and pain relief score (grouped in 7 representative classes).
TABLE 5. Algorithm of preferred surgery according to specific nerve
Nerve Preferred Op
Common peroneal NLDeep peroneal NLLateral femoral cutaneous NLSaphenous NL or R&TSuperficial peroneal R&TSural R&T (stripping)Iliohypogastric NL or R&T*Ilioinguinal NL or R&T*Genitofemoral NL or R&T*Median, palmar cutaneous branch R&TRadial, dorsal branch R&TUlnar, dorsal branch R&TIntercostal R&TIntercostobrachial R&T
NL = neurolysis; R&T = resection and translocation.* Resection and translocation was preferred after inguinal hernia repair with mesh.
Unauthenticated | Downloaded 06/01/20 06:52 AM UTC

V. Decrouy-Duruz, T. Christen, and W. Raffoul
J Neurosurg Volume 128 • April 20181240
A significant number of patients were not available for a follow-up visit (104 of 231, 45%). This might lead to a bias since it is possible that these patients might have had a poorer outcome and chose not to come back. Nevertheless, the patients who came for a follow-up visit were similar to the overall study population in terms of demographic and surgical criteria.
ConclusionsIf pain persists longer than usual after surgery, the neu-
ropathic origin of the pain should be investigated, as the treatment will differ. If pain is refractory to adequate con-servative treatment, nerve revision surgery should be sug-gested, as the outcome might be permanently favorable. No objective criteria were found to be associated with a poor prognosis. The potential overlap of several sensory nerves must be kept in mind, and systematic preoperative clinical mapping of the injured nerve(s) with diagnostic nerve blocks could improve the primary success rate of surgery.
References 1. Aasvang E, Kehlet H: Surgical management of chronic pain
after inguinal hernia repair. Br J Surg 92:795–801, 2005 2. Atherton DD, Fabre J, Anand P, Elliot D: Relocation of pain-
ful neuromas in Zone III of the hand and forearm. J Hand Surg Eur Vol 33:155–162, 2008
3. Atherton DD, Leong JCS, Anand P, Elliot D: Relocation of painful end neuromas and scarred nerves from the zone II territory of the hand. J Hand Surg Eur Vol 32:38–44, 2007
4. Attal N, Cruccu G, Baron R, Haanpää M, Hansson P, Jensen TS, et al: EFNS guidelines on the pharmacological treatment of neuropathic pain: 2010 revision. Eur J Neurol 17:1113–e88, 2010
5. Borsook D, Kussman BD, George E, Becerra LR, Burke DW: Surgically induced neuropathic pain: understanding the peri-operative process. Ann Surg 257:403–412, 2013
6. Burchiel KJ, Johans TJ, Ochoa J: The surgical treatment of painful traumatic neuromas. J Neurosurg 78:714–719, 1993
7. Ciaramitaro P, Mondelli M, Logullo F, Grimaldi S, Battiston B, Sard A, et al: Traumatic peripheral nerve injuries: epide-miological findings, neuropathic pain and quality of life in 158 patients. J Peripher Nerv Syst 15:120–127, 2010
8. Cruccu G, Aziz TZ, Garcia-Larrea L, Hansson P, Jensen TS, Lefaucheur JP, et al: EFNS guidelines on neurostimulation therapy for neuropathic pain. Eur J Neurol 14:952–970, 2007
9. Dellon AL, Mackinnon SE: Treatment of the painful neu-roma by neuroma resection and muscle implantation. Plast Reconstr Surg 77:427–438, 1986
10. Elliot D, Sierakowski A: The surgical management of painful nerves of the upper limb: a unit perspective. J Hand Surg Eur Vol 36:760–770, 2011
11. Farrar JT, Young JP Jr, LaMoreaux L, Werth JL, Poole RM: Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain 94:149–158, 2001
12. Finnerup NB, Otto M, McQuay HJ, Jensen TS, Sindrup SH:
Algorithm for neuropathic pain treatment: an evidence based proposal. Pain 118:289–305, 2005
13. Hazari A, Elliot D: Treatment of end-neuromas, neuromas-in-continuity and scarred nerves of the digits by proximal relocation. J Hand Surg [Br] 29:338–350, 2004
14. Jensen TS, Baron R, Haanpää M, Kalso E, Loeser JD, Rice AS, et al: A new definition of neuropathic pain. Pain 152:2204–2205, 2011
15. Kehlet H, Jensen TS, Woolf CJ: Persistent postsurgical pain: risk factors and prevention. Lancet 367:1618–1625, 2006
16. Kretschmer T, Antoniadis G, Braun V, Rath SA, Richter HP: Evaluation of iatrogenic lesions in 722 surgically treated cases of peripheral nerve trauma. J Neurosurg 94:905–912, 2001
17. Lewin-Kowalik J, Marcol W, Kotulska K, Mandera M, Klim-czak A: Prevention and management of painful neuroma. Neurol Med Chir (Tokyo) 46:62–68, 2006
18. Mackinnon SE, Dellon AL: The overlap pattern of the lateral antebrachial cutaneous nerve and the superficial branch of the radial nerve. J Hand Surg Am 10:522–526, 1985
19. Mackinnon SE, Dellon AL: Results of treatment of recurrent dorsoradial wrist neuromas. Ann Plast Surg 19:54–61, 1987
20. Myles PS, Troedel S, Boquest M, Reeves M: The pain vi-sual analog scale: is it linear or nonlinear? Anesth Analg 89:1517–1520, 1999
21. Nath RK, Mackinnon SE: Management of neuromas in the hand. Hand Clin 12:745–756, 1996
22. Stemkowski PL, Smith PA: Sensory neurons, ion channels, inflammation and the onset of neuropathic pain. Can J Neu-rol Sci 39:416–435, 2012
23. Watson J, Gonzalez M, Romero A, Kerns J: Neuromas of the hand and upper extremity. J Hand Surg Am 35:499–510, 2010
24. Zacest AC, Magill ST, Anderson VC, Burchiel KJ: Long-term outcome following ilioinguinal neurectomy for chronic pain. J Neurosurg 112:784–789, 2010
DisclosuresThe authors report no conflict of interest concerning the materi-als or methods used in this study or the findings specified in this paper.
Author ContributionsConception and design: all authors. Acquisition of data: Decrouy-Duruz. Analysis and interpretation of data: all authors. Draft-ing the article: Decrouy-Duruz. Critically revising the article: Christen, Raffoul. Reviewed submitted version of manuscript: all authors. Administrative/technical/material support: Raffoul.
Supplemental InformationPrevious PresentationsPortions of this work were presented at the XX Congress of Fed-eration of European Societies for Surgery of the Hand, Milano, Italy, June 20, 2015.
CorrespondenceValérie Decrouy-Duruz, Department of Plastic and Hand Surgery, CHUV, Rue du Bugnon 21, Lausanne CH-1011, Switzerland. email: [email protected].
Unauthenticated | Downloaded 06/01/20 06:52 AM UTC