Embed Size (px)
Citation preview

ANTIMICROBIAL AGENTS AND CHEMOTHERAPY, Aug. 1992, p. 1614-16180066-4804/92/081614-05$02.00/0Copyright © 1992, American Society for Microbiology
Evaluation of Cefuroxime Axetil and Cefadroxil Suspensionsfor Treatment of Pediatric Skin Infections
RICHARD F. JACOBS,`* WALLACE D. BROWN,2 STEPHEN CHARTRAND,3 PAUL DARDEN,4MARGARET A. DREHOBL,S ROBERT YETMAN,6 AND MICHAEL J. OSSI7
Arkansas Children's Hospital, Little Rock, Arkansas 722021; Raleigh Pediatric Association, Raleigh,North Carolina 276092; Creighton University School of Medicine, Omaha, Nebraska 681783;
Medical University of South Carolina, Charleston, South Carolina 294254; ScrippsClinic-Rancho Bernardo, San Diego, California 921015; University of Te-xas
Medical School, Houston, Texas 770256; and Glaxo Inc.,Research Triangle Park, North Carolina 277097
Received 7 October 1991/Accepted 15 May 1992
A randomized, single-blind, multicenter study was conducted to evaluate the safety and efficacy ofcefuroxime axetil and cefadroxil suspensions for the treatment of skin or skin structure infections in 287children. Each drug was given at a dosage of 30 mg/kg of body weight per day in two divided doses.Staphylococcus aureus and Streptococcus pyogenes, or a combination of the two, were the primary pathogensisolated from infected skin lesions. A satisfactory bacteriological response (cure or presumed cure) wasobtained in 97.1 and 94.3% of children in the cefuroxime axetil and cefadroxil groups, respectively (P > 0.05).Satisfactory clinical responses (cure or improvement) were more likely to occur in cefuroxime axetil recipientsthan in cefadroxil recipients (97.8 versus 90.3%; P < 0.05). Both regimens were equally well tolerated, withadverse events occurring in 7.9 and 6.1% of cefuroxime axetil and cefadroxil recipients, respectively. Therewere more patients who refused to take cefuroxime axetil (7 of 189) than there were who refused to takecefadroxil (0 of 98), but the difference was not statistically significant (P = 0.1). In this study, cefuroxime axetilwas at least as effective as cefadroxil in resolving skin and skin structure infections in children.
Cefuroxime is an expanded-spectrum cephalosporin withimproved P-lactamase stability and a broad spectrum ofactivity against clinically important gram-positive and gram-negative pathogens. The lowest concentrations that inhibitedthe growth of 90% of the Staphylococcus aureus and Strep-tococcus pyogenes strains tested are 1 to 2 and <0.125,ug/ml, respectively (2).Cefuroxime axetil, the acetyloxyethyl ester of cefuroxime,
is a prodrug that is suitable for oral administration. After oralingestion, cefuroxime axetil is deesterified in the intestinalmucosa and appears as cefuroxime in the blood. Peakconcentrations in serum increase in proportion to dose andare 3.3 and 5.1 ,ug/ml after oral doses of a cefuroxime axetilsuspension of 10 and 15 mg/kg of body weight, respectively(12). These results are comparable to those achieved inadults following administration of a 250-mg cefuroximeaxetil tablet (7). Thus, achievable concentrations in serumexceed the MICs for common cutaneous pathogens (2). Thetablet formulation of cefuroxime axetil has previously beenfound to be effective in the treatment of skin or skinstructure infections in adults (4, 5).The purpose of the study described here was to evaluate
the efficacy and safety of a new liquid suspension of cefur-oxime axetil in children with skin or skin structure infec-tions. Cefadroxil suspension was selected as the activecontrol because it has been proven to be effective in thetreatment of skin or skin structure infections and is suitablefor twice-daily administration.
* Corresponding author.
MATERIALS AND METHODS
Eligibility criteria. Children (ages 3 months to 12 years)with skin or skin structure infections requiring antibiotictreatment were eligible to participate in the study. Patientswere excluded if any of the following were present: infectionrequiring incision and drainage, hypersensitivity to cephalo-sporin or penicillin, previous systemic antibacterial drugtreatment (within 7 days), history of gastrointestinal disorderthat could alter drug absorption (within 3 months), unstableconcomitant disease, immunosuppression, or previous en-rollment in this study. Patients were to be withdrawn afterenrollment if, upon culture and susceptibility testing, nopathogen was isolated or the pathogen was not susceptible tothe study drugs (e.g., methicillin-resistant S. aureus). Pa-tients were discontinued from the study if any of the follow-ing occurred: adverse event necessitating discontinuation ofdrug therapy, treatment failure or recurrence of infection,patient refusal of further doses, or failure to return forfollow-up.
Study design. This was an evaluator-blinded, multicenterstudy. Patients were randomly chosen to receive eithercefuroxime axetil suspension (Ceftin; Glaxo Inc., ResearchTriangle Park, N.C.) or cefadroxil suspension (Duricef;Mead Johnson Pharmaceuticals, Evansville, Ind.) in a 2:1ratio according to a predetermined randomization schedule.Both drugs were administered orally at a dosage of 30mg/kg/day in two divided doses every 12 h (maximum dose,1 g/day) for 10 days. Cefuroxime axetil was given aftermorning and evening meals, because postprandial adminis-tration of cefuroxime axetil (in the tablet form) has beenshown to enhance absorption (3). Cefadroxil was givenwithout regard to mealtimes, as recommended by the man-ufacturer. Compliance was assessed by assay of antibioticactivity in urine during treatment and by the volume of drug
1614
Vol. 36, No. 8
on May 7, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

CEFUROXIME AXETIL AND CEFADROXIL SUSPENSION EVALUATION 1615
returned upon completion of the treatment period. Theabsence of detectable antibacterial activity in a during-treatment urine sample excluded a patient from the efficacyanalyses. Written informed consent was obtained from allpatients' parents or legal guardians. This protocol wasapproved by the institutional review boards of the respectiveinvestigators' institutions.
Efficacy assessment. Response to treatment was assessedbacteriologically and clinically. Although 10 days is thestandard length of therapy for most infections in children, forpurposes of efficacy assessments, 5 days (10 doses) waspredetermined as the minimum length of treatment neces-
sary to effect clinical improvement and eradication of thecausative organism(s) from superficial skin infections.Specimens from the involved skin lesion(s) were obtained
for bacterial culture and susceptibility testing at the initialvisit and, if culturable material was present, at the during-and posttreatment visits. Material for culture was obtainedby needle aspiration or sterile swab of a lesion(s). Crustedmaterial was partially unroofed. The culture material ob-tained was processed at an accredited laboratory accordingto that laboratory's standard protocol for wound or surfacespecimen culture. Standard disk or dilution methods wereused for susceptibility testing; the current criteria of theNational Committee for Clinical Laboratory Standards wereused to interpret the results (10). Bacteriological outcomewas determined at the completion of the study or when thepatient's condition dictated the need for alternate antibiotictherapy. Bacterial responses were rated as cure (initialpathogen eradicated), failure (identification of the originalpathogen in a follow-up culture), or relapse (eradication withsubsequent isolation of the original pathogen). Presumptivebacterial responses were made on the basis of the clinicalresponse when follow-up cultures were not obtainable be-cause of healing of the lesion(s) (e.g., presumed cure). Forstatistical analysis, bacteriological outcomes were groupedas satisfactory (cure or presumed cure) or unsatisfactory(failure or relapse).
Patients underwent at least three clinical evaluations at thefollowing intervals: at the start of therapy (initial visit), at 4to 6 days after the initiation of therapy (during treatment),and at 5 to 7 days after the completion of therapy (posttreat-ment). If complete healing did not occur at 5 to 7 days, anadditional visit was required at 14 to 20 days posttreatment.Clinical response was rated as cure (resolution of clinicalsigns and symptoms of infection), improvement (resolutionof signs and symptoms with incomplete lesion healing;further antibacterial therapy required), failure (no improve-ment after 25 days of treatment or discontinuation oftreatment because of adverse event; alternate antibacterialtherapy required), or recurrence (initial diminution of signsand symptoms but recurrence by the posttreatment visit;further or alternate antibacterial therapy required). Forstatistical analysis, a satisfactory clinical response was de-fined as cure or improvement; an unsatisfactory clinicalresponse was defined as failure or recurrence.
Safety assessment. All patients were monitored for adverseevents. Each patient's parent or guardian was interviewed ateach visit to determine the presence of adverse events. Inorder to avoid bias in eliciting adverse events, the initialquestioning was restricted to "Is your child having anyproblems?" In addition, physical findings that were detectedby the physician observer but that were not present at theinitial visit were recorded as adverse events and were
assessed as to their possible relationship to treatment. Forthe purpose of monitoring laboratory safety, blood was
TABLE 1. Patient enrollment and demographic dataa
Parameter Cefuroxime Cefadroxil Paxetil value
Enrollment dataTotal enrolled (no.) 189 98Population for analysis 156 (82.5) 82 (83.7)
(no. [%])Age (mo)b 69.6 + 3.3 65.6 ± 4.8 NSc
Wt (kg)b 25.2 ± 1.0 24.8 ± 1.6 NS
No. (%) of females 72 (46.2) 39 (47.6) NS
Ethnic origin (no. [%])Caucasian 71 (45.5) 48 (58.5) 0.007Black 74 (47.4) 26 (31.7)Hispanic 9 (5.8) 7 (8.5)Other 2 (1.3) 1 (1.2)
DiagnosisdImpetigo 126 (80.8) 66 (80.5) NSCellulitis 14 (9.0) 8 (9.8)Injury-induced wound 13 (8.3) 6 (7.3)Paronychia 10 (6.4) 4 (4.9)Other' 7 (4.5) 5 (6.1)
TherapyMean dose (mg/kg/day)b 28.6 ± 0.4 28.4 ± 0.4 NSMean duration (days) 10.3 ± 0.2 10.5 ± 0.2 NS
a Demographic data of the population used for analysis.b Data are means ± standard errors.c NS, not significant.d There was more than one primary diagnosis for some patients.Other diagnoses were furunculosis (for the cefuroxime axetil and ce-
fadroxil treatment groups, 2 and 0 patients, respectively), pyoderma (1 and 3patients, respectively), carbunculosis (1 and 0 patients, respectively), buttockabscess (1 and 0 patients, respectively), folliculitis (1 and 0 patients, respec-tively), skin infection began as contact dermatitis (1 and 0 patients, respec-tively), lymphangitis (0 and 1 patient, respectively), and nonspecific skin rashwith exudates (0 and 1 patient, respectively).
collected for complete blood count with differential, plateletcount, prothrombin time, and the direct Coomb's test andfor evaluation of hepatic enzymes, blood urea nitrogen, andserum creatinine. Urine was obtained for evaluation ofalbumin and glucose and a microscopic examination. Thesetests were performed at the initial and posttreatment visits.
Statistical analysis. Two-sided statistical tests were used.Demographic data were summarized by using a van Elterenstatistic (13) (patient age and weight), a Mantel-Haenszelstatistic (9) controlling for investigational center (sex andethnic origin), or a Fisher exact test (8) (allergy, significantmedical history, and abnormal physical finding) to examinethe comparabilities of treatment groups. Summary statisticswere performed on bacteriological and clinical assessments;the Mantel-Haenszel test was used to evaluate differencesbetween treatment groups. The incidence rates of adverseevents were compared between treatment groups by using aFisher exact test. A P value of 0.05 or less was consideredstatistically significant.
RESULTS
A total of 287 patients from 11 centers were enrolled in thestudy (Table 1). Forty-nine patients were excluded from theanalyses because of the following prespecified protocolviolations: inability to isolate a pathogen from the pretreat-
VOL. 36, 1992
on May 7, 2018 by guest
http://aac.asm.org/
Dow
nloaded from
1616 JACOBS ET AL.
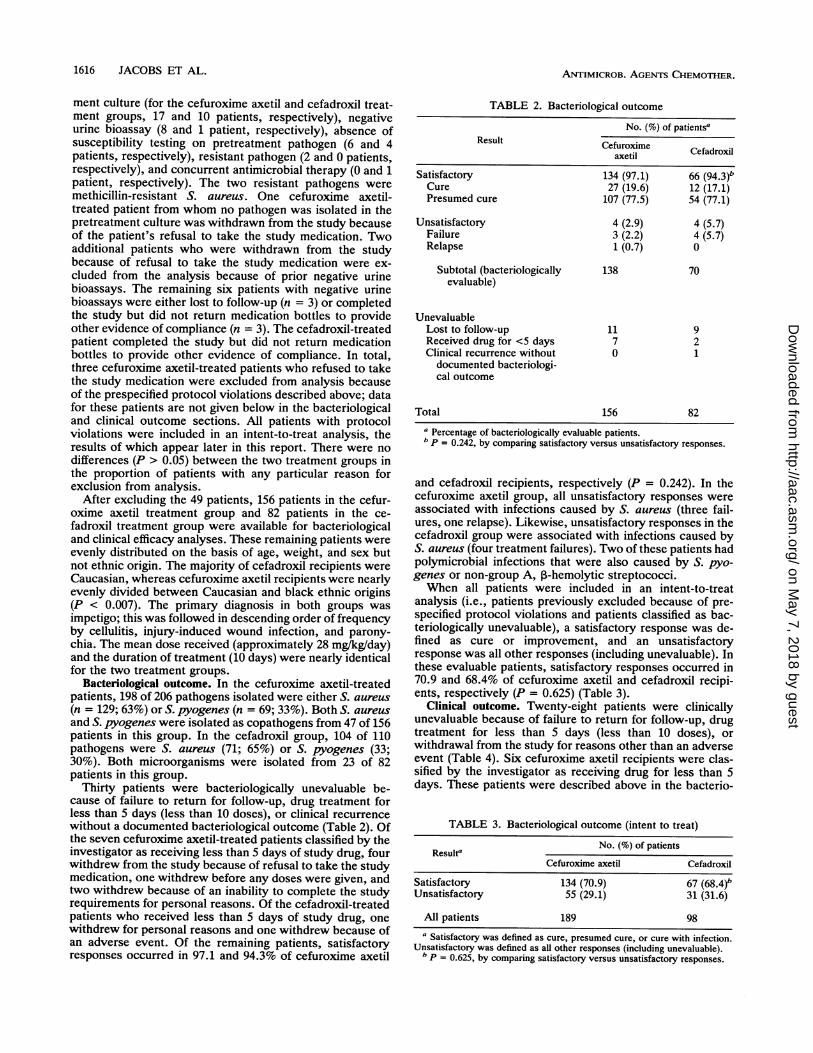
ment culture (for the cefuroxime axetil and cefadroxil treat-ment groups, 17 and 10 patients, respectively), negativeurine bioassay (8 and 1 patient, respectively), absence ofsusceptibility testing on pretreatment pathogen (6 and 4patients, respectively), resistant pathogen (2 and 0 patients,respectively), and concurrent antimicrobial therapy (0 and 1patient, respectively). The two resistant pathogens weremethicillin-resistant S. aureus. One cefuroxime axetil-treated patient from whom no pathogen was isolated in thepretreatment culture was withdrawn from the study becauseof the patient's refusal to take the study medication. Twoadditional patients who were withdrawn from the studybecause of refusal to take the study medication were ex-cluded from the analysis because of prior negative urinebioassays. The remaining six patients with negative urinebioassays were either lost to follow-up (n = 3) or completedthe study but did not return medication bottles to provideother evidence of compliance (n = 3). The cefadroxil-treatedpatient completed the study but did not return medicationbottles to provide other evidence of compliance. In total,three cefuroxime axetil-treated patients who refused to takethe study medication were excluded from analysis becauseof the prespecified protocol violations described above; datafor these patients are not given below in the bacteriologicaland clinical outcome sections. All patients with protocolviolations were included in an intent-to-treat analysis, theresults of which appear later in this report. There were nodifferences (P > 0.05) between the two treatment groups inthe proportion of patients with any particular reason forexclusion from analysis.
After excluding the 49 patients, 156 patients in the cefur-oxime axetil treatment group and 82 patients in the ce-fadroxil treatment group were available for bacteriologicaland clinical efficacy analyses. These remaining patients wereevenly distributed on the basis of age, weight, and sex butnot ethnic origin. The majority of cefadroxil recipients wereCaucasian, whereas cefuroxime axetil recipients were nearlyevenly divided between Caucasian and black ethnic origins(P < 0.007). The primary diagnosis in both groups wasimpetigo; this was followed in descending order of frequencyby cellulitis, injury-induced wound infection, and parony-chia. The mean dose received (approximately 28 mg/kg/day)and the duration of treatment (10 days) were nearly identicalfor the two treatment groups.
Bacteriological outcome. In the cefuroxime axetil-treatedpatients, 198 of 206 pathogens isolated were either S. aureus(n = 129; 63%) or S. pyogenes (n = 69; 33%). Both S. aureusand S. pyogenes were isolated as copathogens from 47 of 156patients in this group. In the cefadroxil group, 104 of 110pathogens were S. aureus (71; 65%) or S. pyogenes (33;30%). Both microorganisms were isolated from 23 of 82patients in this group.
Thirty patients were bacteriologically unevaluable be-cause of failure to return for follow-up, drug treatment forless than 5 days (less than 10 doses), or clinical recurrencewithout a documented bacteriological outcome (Table 2). Ofthe seven cefuroxime axetil-treated patients classified by theinvestigator as receiving less than 5 days of study drug, fourwithdrew from the study because of refusal to take the studymedication, one withdrew before any doses were given, andtwo withdrew because of an inability to complete the studyrequirements for personal reasons. Of the cefadroxil-treatedpatients who received less than 5 days of study drug, onewithdrew for personal reasons and one withdrew because ofan adverse event. Of the remaining patients, satisfactoryresponses occurred in 97.1 and 94.3% of cefuroxime axetil
TABLE 2. Bacteriological outcome
No. (%) of patientsaResult Cefuroxime
axetil Cefadrox
Satisfactory 134 (97.1) 66 (94.3)bCure 27 (19.6) 12 (17.1)Presumed cure 107 (77.5) 54 (77.1)
Unsatisfactory 4 (2.9) 4 (5.7)Failure 3 (2.2) 4 (5.7)Relapse 1 (0.7) 0
Subtotal (bacteriologically 138 70evaluable)
UnevaluableLost to follow-up 11 9Received drug for <5 days 7 2Clinical recurrence without 0 1documented bacteriologi-cal outcome
Total 156 82
a Percentage of bacteriologically evaluable patients.b p = 0.242, by comparing satisfactory versus unsatisfactory responses.
and cefadroxil recipients, respectively (P = 0.242). In thecefuroxime axetil group, all unsatisfactory responses wereassociated with infections caused by S. aureus (three fail-ures, one relapse). Likewise, unsatisfactory responses in thecefadroxil group were associated with infections caused byS. aureus (four treatment failures). Two of these patients hadpolymicrobial infections that were also caused by S. pyo-genes or non-group A, ,3-hemolytic streptococci.When all patients were included in an intent-to-treat
analysis (i.e., patients previously excluded because of pre-specified protocol violations and patients classified as bac-teriologically unevaluable), a satisfactory response was de-fined as cure or improvement, and an unsatisfactoryresponse was all other responses (including unevaluable). Inthese evaluable patients, satisfactory responses occurred in70.9 and 68.4% of cefuroxime axetil and cefadroxil recipi-ents, respectively (P = 0.625) (Table 3).
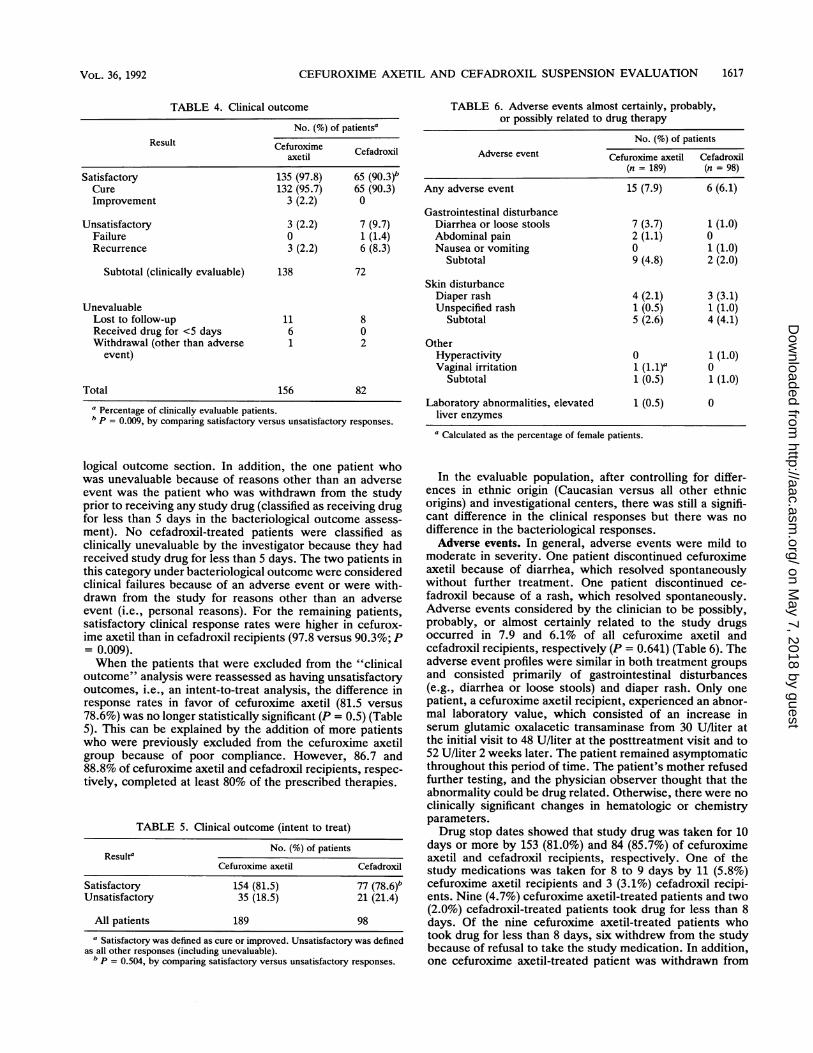
Clinical outcome. Twenty-eight patients were clinicallyunevaluable because of failure to return for follow-up, drugtreatment for less than 5 days (less than 10 doses), orwithdrawal from the study for reasons other than an adverseevent (Table 4). Six cefuroxime axetil recipients were clas-sified by the investigator as receiving drug for less than 5days. These patients were described above in the bacterio-
TABLE 3. Bacteriological outcome (intent to treat)
No. (%) of patientsResulta
Cefuroxime axetil Cefadroxil
Satisfactory 134 (70.9) 67 (68.4)bUnsatisfactory 55 (29.1) 31 (31.6)
All patients 189 98a Satisfactory was defined as cure, presumed cure, or cure with infection.
Unsatisfactory was defined as all other responses (including unevaluable).b p = 0.625, by comparing satisfactory versus unsatisfactory responses.
ANTimICROB. AGENTS CHEMOTHER.
on May 7, 2018 by guest
http://aac.asm.org/
Dow
nloaded from
CEFUROXIME AXETIL AND CEFADROXIL SUSPENSION EVALUATION 1617
TABLE 4. Clinical outcome
No. (%) of patientsaResult Cefuroxime Cefadroxil
axetil
Satisfactory 135 (97.8) 65 (90.3)bCure 132 (95.7) 65 (90.3)Improvement 3 (2.2) 0
Unsatisfactory 3 (2.2) 7 (9.7)Failure 0 1 (1.4)Recurrence 3 (2.2) 6 (8.3)
Subtotal (clinically evaluable) 138 72
UnevaluableLost to follow-up 11 8Received drug for <5 days 6 0Withdrawal (other than adverse 1 2
event)
Total 156 82
a Percentage of clinically evaluable patients.b P = 0.009, by comparing satisfactory versus unsatisfactory responses.
logical outcome section. In addition, the one patient whowas unevaluable because of reasons other than an adverseevent was the patient who was withdrawn from the studyprior to receiving any study drug (classified as receiving drugfor less than 5 days in the bacteriological outcome assess-ment). No cefadroxil-treated patients were classified asclinically unevaluable by the investigator because they hadreceived study drug for less than 5 days. The two patients inthis category under bacteriological outcome were consideredclinical failures because of an adverse event or were with-drawn from the study for reasons other than an adverseevent (i.e., personal reasons). For the remaining patients,satisfactory clinical response rates were higher in cefurox-ime axetil than in cefadroxil recipients (97.8 versus 90.3%; P= 0.009).When the patients that were excluded from the "clinical
outcome" analysis were reassessed as having unsatisfactoryoutcomes, i.e., an intent-to-treat analysis, the difference inresponse rates in favor of cefuroxime axetil (81.5 versus78.6%) was no longer statistically significant (P = 0.5) (Table5). This can be explained by the addition of more patientswho were previously excluded from the cefuroxime axetilgroup because of poor compliance. However, 86.7 and88.8% of cefuroxime axetil and cefadroxil recipients, respec-tively, completed at least 80% of the prescribed therapies.
TABLE 5. Clinical outcome (intent to treat)
No. (%) of patientsResulta
Cefuroxime axetil Cefadroxil
Satisfactory 154 (81.5) 77 (78.6)bUnsatisfactory 35 (18.5) 21 (21.4)
All patients 189 98a Satisfactory was defined as cure or improved. Unsatisfactory was defined
as all other responses (including unevaluable).b p = 0.504, by comparing satisfactory versus unsatisfactory responses.
TABLE 6. Adverse events almost certainly, probably,or possibly related to drug therapy
No. (%) of patientsAdverse event Cefuroxime axetil Cefadroxil
(n = 189) (n = 98)
Any adverse event 15 (7.9) 6 (6.1)
Gastrointestinal disturbanceDiarrhea or loose stools 7 (3.7) 1 (1.0)Abdominal pain 2 (1.1) 0Nausea or vomiting 0 1 (1.0)
Subtotal 9 (4.8) 2 (2.0)
Skin disturbanceDiaper rash 4 (2.1) 3 (3.1)Unspecified rash 1 (0.5) 1 (1.0)
Subtotal 5 (2.6) 4 (4.1)
OtherHyperactivity 0 1 (1.0)Vaginal irritation 1 (1.1)a 0
Subtotal 1 (0.5) 1 (1.0)
Laboratory abnormalities, elevated 1 (0.5) 0liver enzymes
a Calculated as the percentage of female patients.
In the evaluable population, after controlling for differ-ences in ethnic origin (Caucasian versus all other ethnicorigins) and investigational centers, there was still a signifi-cant difference in the clinical responses but there was nodifference in the bacteriological responses.Adverse events. In general, adverse events were mild to
moderate in severity. One patient discontinued cefuroximeaxetil because of diarrhea, which resolved spontaneouslywithout further treatment. One patient discontinued ce-fadroxil because of a rash, which resolved spontaneously.Adverse events considered by the clinician to be possibly,probably, or almost certainly related to the study drugsoccurred in 7.9 and 6.1% of all cefuroxime axetil andcefadroxil recipients, respectively (P = 0.641) (Table 6). Theadverse event profiles were similar in both treatment groupsand consisted primarily of gastrointestinal disturbances(e.g., diarrhea or loose stools) and diaper rash. Only onepatient, a cefuroxime axetil recipient, experienced an abnor-mal laboratory value, which consisted of an increase inserum glutamic oxalacetic transaminase from 30 U/liter atthe initial visit to 48 U/liter at the posttreatment visit and to52 U/liter 2 weeks later. The patient remained asymptomaticthroughout this period of time. The patient's mother refusedfurther testing, and the physician observer thought that theabnormality could be drug related. Otherwise, there were noclinically significant changes in hematologic or chemistryparameters.Drug stop dates showed that study drug was taken for 10
days or more by 153 (81.0%) and 84 (85.7%) of cefuroximeaxetil and cefadroxil recipients, respectively. One of thestudy medications was taken for 8 to 9 days by 11 (5.8%)cefuroxime axetil recipients and 3 (3.1%) cefadroxil recipi-ents. Nine (4.7%) cefuroxime axetil-treated patients and two(2.0%) cefadroxil-treated patients took drug for less than 8days. Of the nine cefuroxime axetil-treated patients whotook drug for less than 8 days, six withdrew from the studybecause of refusal to take the study medication. In addition,one cefuroxime axetil-treated patient was withdrawn from
VOL. 36, 1992
on May 7, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

1618 JACOBS ET AL.
the study because of refusal to take the study medication,but the drug stop date was not recorded. In total, seven(3.7%) cefuroxime axetil-treated patients were withdrawnfor this reason. The disposition of these patients for analysiswas discussed above. No cefadroxil-treated patients with-drew from the study because of refusal to take the studydrug. Drug stop dates were not available for 33 patients (16cefuroxime axetil recipients, 9 cefadroxil recipients), ofwhich 14 (7.4%) cefuroxime axetil recipients and 7 (7.1%)cefadroxil recipients were lost to follow-up. Of the remainingpatients, none were withdrawn because of refusal to takestudy medication.
DISCUSSION
This is the first comparative study of a new formulation ofcefuroxime axetil suitable for oral administration to childrenwith skin or skin structure infections. Clinical (97.1%) andbacteriological (97.8%) response rates in the current studyapproximated those reported in adults receiving the tabletformulation. The overall clinical improvement rate was 95%in 97 patients who participated in a noncomparative study(5). In a study with a design similar to that of the studydescribed here, cefuroxime axetil in the tablet formulationproduced clinical and bacteriological response rates (97 and96%, respectively) higher than those of cephalexin (89 and85%, respectively; P < 0.05) and similar to those of ce-fadroxil (94 and 93%, respectively; P > 0.05) (4). In othercomparative studies, the authors concluded that cefuroximeaxetil is as effective as amoxicillin-clavulanate (14) andcefaclor (11). In those trials, clinical and bacteriologicalresponse rates from 92 to 97% were achieved.
In the study described here, bacteriological response rateswere comparable to those achieved with the cefadroxilsuspension (approximately 97% in each group), but clinicalresponses were higher in cefuroxime axetil recipients (97.8versus 90.3%; P = 0.009). The difference between treatmentgroups did not appear to be due to a spuriously low responserate in the cefadroxil group, because the response rate wasconsistent with those previously reported in comparativetrials of patients with skin or skin structure infections (1, 6).The new cefuroxime axetil suspension was well tolerated
in the study described here. The incidence and profile ofadverse events of the cefuroxime axetil suspension closelyresembled that of the cefadroxil suspension. Only 7.9% ofchildren experienced adverse events during cefuroxime ax-etil therapy; these adverse events were primarily manifestedas gastrointestinal disturbances (e.g., diarrhea or loosestools) or diaper rash. No episodes of nausea or vomitingwere reported in the cefuroxime group.
In this single-blind, randomized study, a suspension for-mulation of cefuroxime axetil produced bacteriological re-sponse rates comparable to those of the cefadroxil suspen-sion (97.1 versus 94.3%) in children with skin or skinstructure infections. The clinical response rate was higher inthe cefuroxime axetil group (97.8 versus 90.3%; P < 0.05).
Both regimens were well tolerated. These results indicatethat the cefuroxime axetil suspension is safe and efficaciousin the treatment of skin and skin structure infections inchildren.
ACKNOWLEDGMENTS
We thank Joseph Quinn for performing statistical analyses andNancy E. Powell for assisting with the execution of this study andpreparation of the manuscript.
This study was supported by a grant from Glaxo Inc.
REFERENCES1. Ballantyne, F. N. 1985. Comparative efficacy of cefadroxil and
cefaclor in the treatment of skin and soft-tissue infections. Clin.Ther. 7:487-491.
2. Dornbusch, K., G. Kronvall, G. E. Goransson, and E. Mortsell.1989. In vitro activity of FCE 22101 against respiratory patho-gens with reference to production of P-lactamases. J. Antimi-crob. Chemother. 23(Suppl. C):31-41.
3. Finn, A., A. Straughn, M. Meyer, and J. Chubb. 1987. Effect ofdose and food on the bioavailability of cefuroxime axetil.Biopharm. Drug Dispos. 8:519-526.
4. Gooch, W. M., III, L. Kaminester, G. W. Cole, et al. 1991.Clinical comparison of cefuroxime axetil, cephalexin and ce-fadroxil in the treatment of patients with primary infections ofthe skin or skin structures. Dermatologica 183:36-43.
5. Gudgeon, A. C., M. J. Vandenburg, L. J. Wight, G. K. Griffiths,and M. Kelsey. 1987. Is oral cefuroxime axetil suitable for thetreatment of unidentified bacterial infection of skin and softtissue? Br. J. Clin. Pract. 41:954-956.
6. Hains, C. S., S. E. Johnson, and K. G. Nelson. 1989. Once dailycefadroxil therapy for pyoderma. Pediatr. Infect. Dis. J. 8:648-649.
7. Harding, S. M., P. E. 0. Williams, and J. Ayrton. 1984.Pharmacology of cefuroxime as the 1-acetoxyethyl ester involunteers. Antimicrob. Agents Chemother. 25:78-82.
8. Kendall, M., and A. Stuart. 1979. The advanced theory ofstatistics, vol. 2, p. 580-585. Macmillan Publishing Company,Inc., New York.
9. Mantel, N., and W. Haenszel. 1959. Statistical aspects of theanalysis of data from retrospective studies of disease. J. Natl.Cancer Inst. 22:719-748.
10. National Committee for Clinical Laboratory Standards. 1984.Performance standards for antimicrobial disk susceptibilitytests. Approved standard M2-A3. National Committee for Clin-ical Laboratory Standards, Villanova, Pa.
11. Parish, L. C., D. M. Cocchetto, K. Werner, D. L. Jungkind, andJ. Witkowski. 1987. Cefuroxime axetil in the treatment ofcutaneous infections. Int. J. Dermatol. 26:389-393.
12. Powell, D. A., N. C. James, M. Ossi, M. C. Nahata, and K. H.Donn. 1991. Pharmacokinetics of cefuroxime axetil suspensionin infants and children. Antimicrob. Agents Chemother. 35:2042-2045.
13. van Elteren, P. H. 1960. On the combination of independenttwo-sample tests of Wilcoxon. Bull. Int. Stat. Inst. 37:351-361.
14. Watts, H. F., A. H. Williams, and D. M. Cox. 1987. A pilot studyof cefuroxime axetil (Zinnat) and Augmentin in the treatment ofskin and soft tissue infections in general practice. Clin. Trials J.24:356-362.
ANTimICROB. AGENTS CHEMOTHER.
on May 7, 2018 by guest
http://aac.asm.org/
Dow
nloaded from





























