Embed Size (px)
Citation preview

Dis Manage Health Outcomes 2007; 15 (4): 215-224LEADING ARTICLE 1173-8790/07/0004-0215/$44.95/0
© 2007 Adis Data Information BV. All rights reserved.
Evaluation of an Online Relapse PreventionProgram for Bipolar DisorderAn Overview of the Aims and Methodology of a RandomizedControlled Trial
Caryl Barnes,1 Robin Harvey,2 Philip Mitchell,1 Michael Smith2 and Kay Wilhelm1
1 Black Dog Institute, School of Psychiatry, University of New South Wales, Sydney, New South Wales, Australia2 Sentiens Pty Ltd, University of Western Australia, Perth, Western Australia, Australia
Bipolar disorder is a chronic relapsing remitting illness affecting 1–2% of the general adult population.AbstractAwareness of the limitations of pharmacological treatment for this disorder has encouraged the development ofpsychological treatments and a large body of evidence now exists demonstrating the effectiveness of severaltypes of psychosocial interventions in the treatment and prevention of relapse for bipolar disorder. Unfortunate-ly, it is difficult for many individuals with bipolar disorder to access such programs due to financial constraintsand restricted roll-out. One solution to this difficulty is to use Internet-based delivery of targeted psycho-education, cognitive behavior management and online medication monitoring to improve relapse prevention forthose with bipolar disorder.
The focus of this article is to discuss the aims and methodology of this unique, collaborative randomizedcontrol trial that evaluates the effectiveness of an Internet-based disease management program (termed RecoveryRoad [RR]). The RR program incorporates both symptom monitoring with feedback, and targeted psychosocialtreatment for adults with bipolar disorder delivered over a 12-month period. The overall aim was to determinewhether this web-based adjunctive relapse prevention program can improve mental health outcomes. Uponsuccessful enrolment, participants were automatically randomized into either the intervention (RR) or controlgroup. The control group received some relevant information but did not include program componentsconsidered to be active parts of the experimental intervention.
This article also describes a recruitment, enrolment and randomization process that maximizes the potentialof the Internet for research and data collection purposes. At the time of writing full results were not yet availableand, thus, were not reported in this article. Interim outcomes indicate that the online enrolment has beensuccessful and participants are making full use of all online features of the active program included by thesupport facility. The difficulties with maintaining individuals on the control program are described and samplesof typical anecdotal comments provided by participants to the research group via the support facility arepresented.
1. Research Rationale WHO in 1990 rated bipolar disorder as the sixth leading cause of
disability-adjusted life-years in the world amongst people agedBipolar disorder is a chronic relapsing remitting illness that
15–44 years.[3] The economic burden to society is also high,affects 1–2% of the general adult population.[1,2] Despite advancesestimated to be approximately 70% of that linked to schizophre-in the pharmacological treatment of this disorder, rates for recov-
ery and return to normal level of functioning remain poor. The nia.[4]

216 Barnes et al.
A high level of adherence to effective medication regimens is support for a range of chronic conditions including mental healthrecognized as a key factor in the successful management of bipolar difficulties.[18] In particular, programs delivering varying types ofdisorder and the prevention of relapse.[5] However, poor adherence CBT have been developed for post-traumatic stress disorder, so-to prescribed medication has been consistently reported for indi- cial phobia, depression, and anxiety. CBT is a proven efficaciousviduals diagnosed with bipolar disorder, with studies demonstrat- treatment intervention for these last two high-prevalence disor-ing adherence rates between 12% and 60%.[6] Another important ders, but accessibility has been reduced by the lack of availabilityissue is the finding that even when adherence rates are high, the of a trained therapist to deliver such programs face to face and themajority of people with bipolar disorder continue to experience relatively high cost of training such therapists.high levels of ‘sub-syndromal’ symptoms or inter-episode mood A recent review by Titov[19] reported on eight randomizeddisturbances across the lifespan. Such symptoms have been shown controlled trials looking at computerized cognitive behavioralto impact on an individual’s daily functioning and persist even therapy (CCBT) for depression. This included the randomizedwhen pharmacological interventions are maximized.[7-9] controlled study by Christensen et al.,[20] which demonstrated that
both a web-delivered CBT program (Mood Gym) and a psycho-Awareness of the limitations of pharmacological treatment haseducational program (Blue pages) led to statistically significantturned the attention of researchers and clinicians to understandingreductions in the symptoms of depression in the general popula-the role and impact of psychological treatments in the manage-tion compared with the attention placebo control. Interestingly,ment of bipolar disorder. A large body of evidence now existsalthough both programs showed reduction in symptoms, only thedemonstrating the effectiveness of several types of psychosocialMood Gym program showed sustained improvement after 12interventions in the treatment and prevention of relapse for bipolarmonths. A subsequent study by the same authors showed thatdisorder, such as individual and group psycho-education pro-multiple sessions of mood gym were more effective than a singlegrams, cognitive behavioral therapy (CBT), family focused ther-session.apy and interpersonal social rhythms therapy.[10-14] Such interven-
tions are now regarded as part of best practice standards for the Not all studies have been positive; Clarke et al.[21] reported nomanagement of bipolar disorder. For example, psychosocial inter- difference in groups on depressive scores or on frequency or use ofvention now forms an important part of the treatment guidelines health services. A subsequent revised study by the same researchfor bipolar disorder produced by the Royal Australian and New group[22] also found no difference between intervention condi-Zealand College of Psychiatrists[15] and those developed by the tions, but those who were more depressed showed a greaterAmerican Psychiatric Association.[16] Unfortunately, many of reduction in depressive symptoms relative to controls. Limitationsthese interventions are labor intensive and therefore expensive, with this type of intervention include the fact that participantswith services mostly restricted to large teaching/research faculties accessed the website infrequently, possibly because participantsor accessed on a fee-for-service basis through private health prov- with higher levels of depression found it more difficult to motivateiders. Accessibility to these treatment options is therefore limited themselves to use such an intervention. The key to the most of theto only a small proportion of individuals living with bipolar successful studies seems to be the retention of some sort ofdisorder. clinician contact with the participant, keeping them motivated and
engaged in the program. This is reflected in the fact that thoseEffective management of this disorder clearly requires thestudies that did not have any therapist contact tended to have lowerdevelopment of efficacious, cost effective, and accessible inter-completion rates, which then impacted on the effect size of anyventions that provide the recommended adjunctive psychologicalimprovements.[19] Other researchers have used the Internet totherapy for people with bipolar disorder and supports good adher-deliver successful psycho-education programs for post-traumaticence to medication regimes. The Internet provides one possiblestress disorder,[23] eating disorders,[24] and obesity.[25]pathway for disseminating targeted and standardized psychosocial
programs, due to its accessibility and versatility. Self-help groups Sentiens, a mental health service provider in Perth (WA, Aus-and mental health consumers have increasingly used the Internet tralia), has developed an Internet-based, disease management plat-to obtain information about their disorder and treatment options as form known as ‘Recovery Road’ (RR).[26] Through this secure andwell as gaining comfort and support through consumer driven personalized online platform, mental health consumers can bewebsites and chat rooms.[17] In the past 5 years, clinicians and linked with their treating clinicians using asynchronous messag-researchers have also begun to recognize the potential of the ing. The platform provides consumers and clinicians with accessInternet to provide treatment interventions and self-management to self-report monitoring tools, utilizing a range of online mental
© 2007 Adis Data Information BV. All rights reserved. Dis Manage Health Outcomes 2007; 15 (4)

Online Relapse Prevention for Bipolar Disorder 217
health, medication adherence and quality-of-life questionnaires. 1. To evaluate an online enrolment platform as a tool to obtainThis allows consumers to receive immediate and ongoing feed- informed consent and complete enrolment into the study throughback on progress, risk of relapse and level of medication adher- improving utility of the Internet-based program.ence. In addition, the platform allows consumers to access a 2. To evaluate an automated, Internet -based strategy to random-12-month program of psychosocial treatment for a variety of ize participants into one of two online programs representing thechronic mental health conditions. The primary author of this paper study or ‘active’ intervention (RR) and control intervention (VH).authored and developed a relapse prevention program for peoplewith bipolar disorder to be used on this platform. This was then 3. Methodologyadapted for the purposes of a study with the inclusion of severalvalidated measures. This trial only involves the consumer side of
3.1 Participantsthe overall program.
In order to determine treatment efficacy and utilize the research Participants for the trial were primarily recruited via publicityefficiency of the Internet, individuals experiencing bipolar disor- generated from a news release from the Black Dog Instituteder were recruited via the web to a randomized controlled trial of (Sydney, NSW, Australia), an internationally recognized, clinical,the relapse prevention program for bipolar disorder. This article research and educational body dedicated to improving understand-discusses the aims and methodology of this unique, collaborative ing, diagnosis and treatment of mood disorders. Participants wereproject to evaluate the effectiveness of an Internet-based program also recruited via a number of mental health websites that publi-that incorporates both symptom monitoring with feedback, and cized the trial. In addition, newsletters describing the trial werepsychosocial therapy, including ten sessions of CBT, in the man- sent to community-based mental health services, general practi-agement of bipolar disorder. It also describes a recruitment and tioners, and psychiatrists within Australia.randomization process that maximizes the potential of the Internetas a research tool. It is important to note that the results of the 3.2 Enrolmentstudy are not reported here, but will be published elsewhere.
In order to maximize accessibility, interested individuals, ini-tially local and then by default, international, were invited to2. Design and Aims of the Projectcomplete an online screening instrument, the Bipolar DisorderScreening Questionnaire (BDSQ), which identified suitability forThe trial of the relapse prevention program for bipolar disorderenrolment into the project and obtained informed consent online.was designed as a longitudinal, prospective randomized controlledThe BDSQ is a 109-item self-report questionnaire specificallytrial of an online program. The overall aim was to determinedesigned to identify people with bipolar disorder, as defined by thewhether a web-based adjunctive relapse prevention program, RRDiagnostic and Statistical Manual of Mental Disorders (DSM-for adults with a clinical diagnosis of bipolar affective disorder,IV[27]), who met the study’s inclusion criteria (table I).scheduled over 12 months at fixed intervals can improve mental
The BDSQ was developed by researchers at the Black Doghealth outcomes. The main outcome measure was time to relapseInstitute (more details of the development of the BDSQ are report-over the 12-month period, symptom severity and sub-syndromaled in section 3.3) and was validated previously in a pilot studysymptomatology, level of functioning and medication compliancewith attendees at the Bipolar Clinic, headed by one of the authorswhen compared with adults randomized to a control program
termed ‘Virtual Highway Program for Bipolar Disorder’ (VH),with both groups receiving ‘treatment as usual.’ A prerequisite toinclusion into the study is that all participants were seeing aclinician for ongoing management of their bipolar disorder, andwere currently taking medication for the management of theirillness. They may have also been receiving other conventionalpsychological/psychosocial therapy as part of this ‘treatment asusual.’ As individuals within each group have equal chance ofreceiving such therapy, it is felt that this did not need to becontrolled for statistically. Additional aims include:
Table I. Inclusion criteria for participants enrolling in the Online BipolarProgram
Over 18 years of age with a current diagnosis of bipolar disorder madeby a mental health professional
Meets criteria for bipolar disorder as confirmed by self-report responseson the BDSQ
Currently under care of psychiatrist or general practitioner and takingmedication for bipolar disorder
Access to the Internet, a printer and an e-mail account, and is able tounderstand written English
© 2007 Adis Data Information BV. All rights reserved. Dis Manage Health Outcomes 2007; 15 (4)

218 Barnes et al.
(PM) at the Black Dog Institute.[28] The last 100 attendees in be calculated from the point at which the symptomatic participantSeptember 2005 were invited, via a letter, to go online and becomes euthymic, as measured by the Internal State Scale (ISS).complete the draft version of BDSQ. Sixteen of 100 did so and
3.3 Measurestheir responses were then cross matched with their earlier clinicalassessment. The assessment and subsequent diagnosis of a clinic The BDSQ was developed from a number of resources includ-attendee was based on several face-to-face assessments by an ing the DSM[27] and a number of validated questionnaires, includ-experienced psychiatrist and psychologist. It included the use of a ing Brief Psychiatric Rating Scale,[30] Young Mania scale,[31]
battery of standardized questionnaires and the clinicians had ac- Mood Disorder Questionnaire,[32] Depression Anxiety Stresscess to the patient’s medical file. At the end of the pilot study, the Scales,[33] Hamilton Rating Scale for Depression,[34] Montgomery-BDSQ was revised to correct for the users’ tendencies to underrate Asberg Depression Rating Scale,[35] Beck Depression Inventory-IIthe length of time they had been manic or hypomanic. This had the (BDI-II),[36] and the Structured Clinical Interview for Depres-effect of increasing the BDSQ’s false-negative rate for Bipolar I. sion.[37] It was also informed by the clinical experience of theThis underestimation is in keeping with literature in this area, authors and the clinical assessment process that occurs at thewhich has established the validity of using self-report tools in the Bipolar Clinic. As mentioned in section 3.2, the BDSQ wasbipolar population.[29] The authors are confident of the BDSQ’s validated in an earlier pilot study with attendees at the Bipolarability to correctly identify individuals meeting the study’s inclu- Clinic at the Black Dog Institute.sion criteria. To further reduce the risk of false-negative or false-
The mood monitoring section of the two online programs waspositives, the chief investigator for the study (CB) reviewed each
made up of a battery of questionnaires, some were validatedset of data from the BDSQ analysis and compared the outcome
measures used with permission of the publishers/authors andwith raw data file for each person completing the BDSQ. Data
others were developed specifically for the program. Validatedwere only analyzed from those users who had completed the
measures used included the BDI-II,[36] the ISS,[38] and the SheehanBDSQ in full and who had provided a contact e-mail address.
Disability Scale.[39]
The consent protocol also provided participants with the oppor- Two new bipolar measures were developed for the programtunity to print off clinician information sheets to provide to their from the resources described above and are known as the ‘Bipolartreating doctor. The BDSQ was accessed from the Black Dog Depression Severity Scale’ and ‘Bipolar Mania Severity Scale’.Institute and Sentiens’ websites and, after its completion, individu- Two other new scales, the ‘General Symptom Scale’; developed asals were informed by e-mail of their eligibility to enrol in the means of identifying and monitoring medication adverse effectsprogram and provided with the appropriate security codes in order and the ‘Risk and Safety Check List.’ These scales were only usedto access the online enrolment. By accessing the online enrolment in the study program (RR) and were excluded from the controlparticipant’s consented to allowing their clinician to be contacted program (VH) as participants were not receiving feedback fromduring the study to inform them about their patient’s involvement these scales, which rendered them superfluous.in the trial.
The initial protocol required participants to be asymptomatic at 3.4 Procedure and Description of Active and
commencement of the study (i.e. that they did not meet DSM-IV Control Programs
criteria for either major depressive, mixed or hypomanic/manicUpon successful enrolment, participants were automatically
episode). As the BDSQ data were being evaluated it becamerandomized into either the intervention (RR) or control group
apparent that significant numbers were in fact meeting the criteria(VH). Each participant was provided with a user ID and password
for a current mood episode. We were concerned that excludingthat allowed them access to the allocated program and ensure all
these people from the study would have significantly reduced thedata collected were secure and de-identified.
power of the study. We therefore revised the mood severity3.4.1 Active Program: Recovery Road for Bipolar Disorderentrance criteria, which then allowed participants to be experienc-
ing a current mood episode at commencement of the study. This The study or active intervention is a relapse prevention programwas subsequently confirmed at end of recruitment with only 29% for bipolar disorder designed and authored by the primary author.of completers being asymptomatic, according to the BDSQ. This After logging on using their personalized user ID and password,change in protocol will impact on the analysis of data at the end of participants randomized to the intervention program proceededstudy; as time to relapse (our main outcome measure) will have to into the first of 21 scheduled sessions. At the start of the first
© 2007 Adis Data Information BV. All rights reserved. Dis Manage Health Outcomes 2007; 15 (4)

Online Relapse Prevention for Bipolar Disorder 219
session, participants were led through a series of automated steps active parts of the experimental intervention. In all respects, theto set up a personal ‘medical record,’ which details their current procedure for accessing sessions remained the same, the schedul-treatment, medication details and adherence. They were then re- ing of new sessions was the same, and participants were requiredquired to complete a set of questionnaires (see section 3.3 for to complete the same range of evaluative questionnaires, butdetails of measures included). The last questionnaire the ‘Appoint- without the graphical and report type feedback from the BDSS andments Diary’ asked about frequency and nature of contact with BMSS. However, the online home page of the control group didmental health services since the last session; this Appointments not give participants access to the psycho-education material orDiary section, in combination with scores on symptom severity the therapy sessions. Instead, for each of their 21 sessions, theycan be used to establish point of relapse. Participants were provid- were taken on a ‘Virtual Tour’ to a variety of publicly availableed with access to new sessions, which were weekly for the first 2 websites that focused on healthy living. These included websitesmonths, then fortnightly for the next 2 months and then monthly teaching the viewer how to meditate, to recognize and deal withfor the remainder of the 12-month period. stress, and about the health benefits of healthy nutrition and
exercise. If interested, the participant could record their assess-Once the evaluation procedure for each session is complete,ment of each website they visit by completing a short optionalparticipants were taken to their personalized ‘Bipolar Recoverysurvey called the ‘Website Diary.’ This was developed fromRoad Home Page.’ From here they could access a variety ofstudies that described how to assess the quality of health informa-psycho-educational materials (referred to as Sessions) and, whention on the Internet. Participants in the study program (RR) couldscheduled, ten sessions of CBT, specifically designed to assistalso access these websites through a feature called ‘Website of theparticipants to identify early warning signs of relapse. The psycho-Week’ housed in the ‘Suggested Reading’ section on theireducational material changes for each session and covers thehomepage. It should be noted that, in order to keep controlfollowing areas:participants motivated, they have been placed in a ‘wait list• dealing with symptomscontrol’ position and will be able to access the active and updated• medication issuesRR program once the study is completed.• psychological approaches
Although both groups undertake mood monitoring, only those• lifestyle and relationshipsin the active program received detailed feedback on the results of• staying safe.these; this combined with the psycho-education and CBT compo-More detailed information about treatment and specific man-nents of the study program are felt to be the ‘active ingredients’ ofagement issues could be accessed through information brochuresthe program. Our hypothesis is that those in the active programcalled ‘Suggested Readings.’ In addition, each home page showedwill show better outcome with improved adherence to medicationa graphical summary of results from the self-reported Bipolar(as recorded in the ‘Medication diary’ of both programs), and willDepression Severity Scale (BDSS), Bipolar Mania Severity scaleshow longer time to relapse compared with the control group. We(BMSS) and General Symptom Scale. This provided each partici-will be using the three validated scales used in this study: (i) thepant with immediate feedback about progress and adverse effects.BDI-II; (ii) the ISS; and (iii) the Sheehan Disability Scale toIf there was an increase in symptom severity, participants wereestablish level of symptoms and functioning. The ‘Appointmentsdirected to access more detailed psycho-educational material toDiary’ section of the two programs records the amount of contactfind out about the types of issues/problems that might underlie thewith mental health services and admissions to hospital betweenidentified changes and what approaches may assist them to im-each session and this combined with the mood questionnaires willprove. The intervention also allowed participants to keep an onlineenable us to measure ‘time to relapse’ – the main outcome measurediary and to track changes and the timing of such changes to theirfor the study.medications through a section ‘My Medication.’ Each participant
received several e-mail reminders for each session to log on andcould choose to set up a daily e-mail reminder to take medication. 3.5 Ethical Considerations
3.4.2 Control Program: Virtual Highway for Bipolar Disorder Numerous concerns were raised about duty of care towardsThe control intervention was designed to form an online ‘atten- participants during the development of the study protocol. Several
tion placebo.’ It provided information of some interest to partici- safety nets were built into the programs as a result. These includedpants but did not include program components considered to be establishing strict inclusion criteria to ensure that all participants
© 2007 Adis Data Information BV. All rights reserved. Dis Manage Health Outcomes 2007; 15 (4)

220 Barnes et al.
were under the care of a mental health professional and providing and was a resident in Australia, a research officer contacted themparticipants with the capacity to access information about seeking by phone. Once the allotted time for a session had passed, partici-help in an emergency through the ‘In Emergency’ button, which pants were still able to access the information contained within theappeared at the top of the computer screen when in the program session, but had to wait until a new session was due before being(both for the control and active groups). This section listed emer- able to complete the next set of monitoring questionnaires.gency contact numbers for each state of Australia and containedgeneric information on how to seek help. The active program also 4. Interim Findingshad a ‘Staying Safe’ section, which contained tips on how to staysafe when manic or depressed. Finally, an automated system of Prior to commencement of the study, statistical advice was‘Red Flags’ was developed and built into the system based on two sought and a sample size calculation performed, which indicatedof the outcome measures (the BDI-II and the ISS). If total scores that approximately 100 participants per group (200 in total) wason these two scales indicated a clinically significant level of required. Our plans to use survival analysis (log rank test) as thesymptoms and/or the presence of serious suicidal intentions, a main outcome measure increased this estimate to 120 per group,‘Red Flag’ report is generated. This is reviewed by a clinician assuming 12-month follow-up and median survival of 6 months(CB) who sent an e-mail encouraging him or her to see their for the controls.clinician for review. In addition, if the appropriate consents were Despite only limited advertising, at the completion of thegiven, either an e-mail or letter was sent to the treating clinician enrolment period there have been 559 individuals attempting theinforming him or her about their patient’s ‘Red Flag’ and what this online screening instrument (BDSQ) at least once. One personmeant. All participants were treated in the same manner. attempted the questionnaire twice, she had initially been excluded
from the study based on her responses and we believe that in anattempt to get enrolled she attempted it again with different3.6 Case Management
responses; however, she was again excluded. This only becameThe study and control programs were designed to be an adjunct apparent at the close of the enrolment period and when the BDSQ
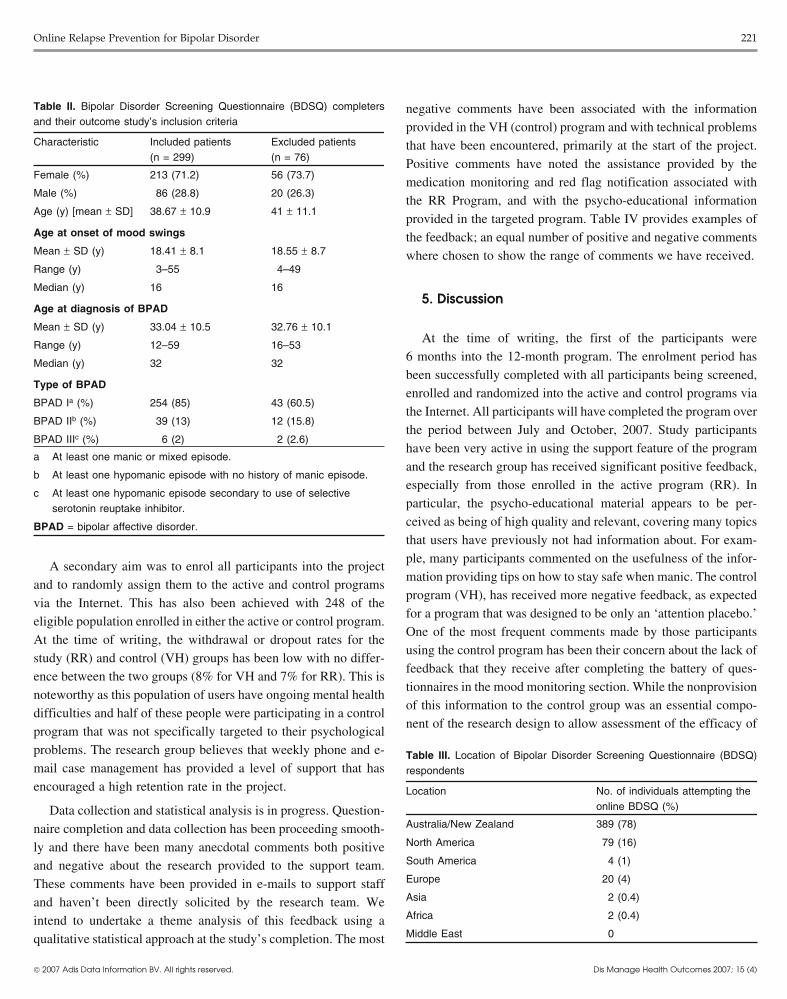
to ‘treatment as usual’ and were not viewed as a replacement for data were analyzed. The BDSQ is made up of 106 items and takesstandard treatment by a qualified medical practitioner. Participants >30 minutes to finish; therefore, significant effort is required by awere encouraged to keep in regular contact with their treating potential participant to complete it. Only those who have complet-clinician throughout the program. As stated in section 3.2, when a ed the BDSQ in full and provided an active e-mail address haveparticipant provided the appropriate consent at enrolment, a letter their answers evaluated. Indeed, out of the 559 who accessed theor e-mail was sent to their treating clinician, informing them about online screening questionnaire, 67% (n = 375) completed the fullthe study and their patient’s participation in it. Once enrolled into assessment with 80% (n = 299) of these individuals identified asthe study, any enquires from participants were managed through e- eligible for participation. These individuals were sent an e-mailmail to the [email protected] portal. The goal of ‘support’ inviting them to enrol into the study, of whom 83% subsequentlywas to supply technical support for participants having problems did. At the end of the enrolment period, 248 participants wereaccessing their program and, whenever possible, standardized enrolled into the study. Table II illustrates some of the demograph-replies were used and no direct treatment advice or comment on ic statistics for this group.treatment was given. This was in order to ensure the fidelity of the The initial research protocol was to exclude non-Australian/program and to allow evaluation of the standard online program. New Zealand residents; however, 107 overseas residents accessedAs all participants were treated in the same manner, this support is the BDSQ despite the lack of broad publicity and those who metnot expected to require statistical correction. the study’s inclusion criteria have now been included. We intend
Each new session was scheduled with participants having a to now include county of origin as a variable in the end analysis if‘window of opportunity’ lasting 5 days, during which they could numbers remain significant. Although the results of this study willcomplete the set of monitoring questionnaires for that session. not be reported in this article, initial comparison of the BDSQParticipants (both study and control groups) were sent an e-mail completers has not revealed any significant differences betweenreminder prior to this ‘window’ opening, a second e-mail when these two groups. Table III provides a full breakdown of thethis ‘window’ opened and a third when it closed. If a participant number of respondents accessing the BDSQ from various conti-failed to complete the monitoring section after the first two e-mails nents.
© 2007 Adis Data Information BV. All rights reserved. Dis Manage Health Outcomes 2007; 15 (4)
Online Relapse Prevention for Bipolar Disorder 221
negative comments have been associated with the informationprovided in the VH (control) program and with technical problemsthat have been encountered, primarily at the start of the project.Positive comments have noted the assistance provided by themedication monitoring and red flag notification associated withthe RR Program, and with the psycho-educational informationprovided in the targeted program. Table IV provides examples ofthe feedback; an equal number of positive and negative commentswhere chosen to show the range of comments we have received.
5. Discussion
At the time of writing, the first of the participants were6 months into the 12-month program. The enrolment period hasbeen successfully completed with all participants being screened,enrolled and randomized into the active and control programs viathe Internet. All participants will have completed the program overthe period between July and October, 2007. Study participantshave been very active in using the support feature of the programand the research group has received significant positive feedback,especially from those enrolled in the active program (RR). Inparticular, the psycho-educational material appears to be per-ceived as being of high quality and relevant, covering many topics
Table II. Bipolar Disorder Screening Questionnaire (BDSQ) completersand their outcome study’s inclusion criteria
Characteristic Included patients Excluded patients(n = 299) (n = 76)
Female (%) 213 (71.2) 56 (73.7)
Male (%) 86 (28.8) 20 (26.3)
Age (y) [mean ± SD] 38.67 ± 10.9 41 ± 11.1
Age at onset of mood swings
Mean ± SD (y) 18.41 ± 8.1 18.55 ± 8.7
Range (y) 3–55 4–49
Median (y) 16 16
Age at diagnosis of BPAD
Mean ± SD (y) 33.04 ± 10.5 32.76 ± 10.1
Range (y) 12–59 16–53
Median (y) 32 32
Type of BPAD
BPAD Ia (%) 254 (85) 43 (60.5)
BPAD IIb (%) 39 (13) 12 (15.8)
BPAD IIIc (%) 6 (2) 2 (2.6)
a At least one manic or mixed episode.
b At least one hypomanic episode with no history of manic episode.
c At least one hypomanic episode secondary to use of selectiveserotonin reuptake inhibitor.
BPAD = bipolar affective disorder.that users have previously not had information about. For exam-ple, many participants commented on the usefulness of the infor-
A secondary aim was to enrol all participants into the projectmation providing tips on how to stay safe when manic. The control
and to randomly assign them to the active and control programsprogram (VH), has received more negative feedback, as expected
via the Internet. This has also been achieved with 248 of thefor a program that was designed to be only an ‘attention placebo.’
eligible population enrolled in either the active or control program.One of the most frequent comments made by those participants
At the time of writing, the withdrawal or dropout rates for theusing the control program has been their concern about the lack of
study (RR) and control (VH) groups has been low with no differ-feedback that they receive after completing the battery of ques-
ence between the two groups (8% for VH and 7% for RR). This istionnaires in the mood monitoring section. While the nonprovision
noteworthy as this population of users have ongoing mental healthof this information to the control group was an essential compo-
difficulties and half of these people were participating in a controlnent of the research design to allow assessment of the efficacy of
program that was not specifically targeted to their psychologicalproblems. The research group believes that weekly phone and e-mail case management has provided a level of support that hasencouraged a high retention rate in the project.
Data collection and statistical analysis is in progress. Question-naire completion and data collection has been proceeding smooth-ly and there have been many anecdotal comments both positiveand negative about the research provided to the support team.These comments have been provided in e-mails to support staffand haven’t been directly solicited by the research team. Weintend to undertake a theme analysis of this feedback using aqualitative statistical approach at the study’s completion. The most
Table III. Location of Bipolar Disorder Screening Questionnaire (BDSQ)respondents
Location No. of individuals attempting theonline BDSQ (%)
Australia/New Zealand 389 (78)
North America 79 (16)
South America 4 (1)
Europe 20 (4)
Asia 2 (0.4)
Africa 2 (0.4)
Middle East 0
© 2007 Adis Data Information BV. All rights reserved. Dis Manage Health Outcomes 2007; 15 (4)

222 Barnes et al.
Table IV. Examples of positive and negative responses to the online bipolar program
Positive responses
Response to ‘red flag’ e-mail Many thanks for your e-mail. I have been having extra sessions with my psychologist to work through thislow. My regular GP is on leave until next week, but will see her as soon as I can. She wants to re-evaluatemy medication. I’m a bit scared of coming off Prozac and trying other meds though …Thank you for your kind concern
Response to support provision Many thanks, I am able to follow you no problem. That makes perfect sense! I am enjoying the programThank you for the e-mail. Yes, it makes perfect sense about the changes to the program. I will wait till nextweek to complete Session 9. I sound a little too eager I think. The program has been wonderful though andI am slowly learning and applying many new and valuable ideas
Negative responses
Participant not understanding a I have not received an e-mail reminder for this week’s session and cannot access it when I log in – thoughchange to scheduling the homepage identifies the Week 9 Session. I wonder if this is because I changed my e-mail contact after
the last session?Thank you for your help
Technical glitches I have now tried four times to access my program Road to Recovery, but I have mislaid my password etc.so I can’t get in to it. As it is now Wednesday I need assistance please or I’ll fall behind in the Road toRecovery program
The team learning more about I know I am being a pain, but is there an opportunity to leave the survey open all day Saturday?scheduling This is the third occasion I have missed doing the survey by a matter of hours
I know I have all week to do this, but being self employed my priority is to work
Lack of efficacy of control program I would appreciate if you could pass this e-mail onto the medical staff as I wish to drop out of this study.(virtual highway) Basically because I can not see how this program is meant to help me in any size shape or form and am
finding it a chore with no positive outcomes for me. The websites are generic and only helpful if you don’thave the forethought and the proactivity (sic) to be able to help yourself when researching alternatives toliving in and with madness (not that there is anything wrong with that, that being madness). Basically I ambored with the repetitive (sic) questions that lack feedback, except for a number that means nothing to meseeing as it lacks explanation. For me personally, this program is useless
all components of the active program, it is clearly a significant issues and using standardized e-mails as templates to responses toqueries. It appears that all users view themselves as being part ofsource of frustration for those in the control group.an ‘online community.’ The regular automated individualized e-Another limitation of the study, as supported by feedbackmail reminders seemed to quickly establish a rapport with eachreceived from participants, has been the structure of the controlparticipant. This added to the way in which each query is handledprogram. Limitations with the IT platform software made it diffi-in an empathic and individualized manner and may have assistedcult to personalize certain aspects of program delivery, whichin its development. This aspect of the study may have added
proved to be confusing for the VH users who thought they couldsignificantly to the user experience of the program and may makes
access their progress graphs when in fact they couldn’t. Althoughit difficult to identify the components of the active program that
the current rate of drop out for both groups remains comparable, ithave contributed to its success when the results are analyzed.
is predicted that there will be a higher rate of drop out in the VH
group over time. This pattern is likely to reflect the challenges6. Conclusions
noted previously in clinical research studies when a control group
is not provided with targeted support. This is particularly the caseOne of the big challenges for both Australian and overseas
in the area of relapse prevention when follow-up and case manage- mental health services is providing psychological interventionsment occurs over a reasonably long period of time (in this case 12 that are effective, easily accessible and cost effective. An ongoingmonths). challenge for clinicians is how to best support people on long-term
A further limitation of the current research design is in assess- medication and to reduce the incidence of the common ‘stop-start’ing the impact of the support facility to participants in both pattern of medication use, which has been shown to have aprograms. Despite all efforts to keep this purely based on technical profoundly negative impact on both the severity and course of
© 2007 Adis Data Information BV. All rights reserved. Dis Manage Health Outcomes 2007; 15 (4)

Online Relapse Prevention for Bipolar Disorder 223
bipolar disorder. If this study shows that a computerized Internet- References1. Kessler RC, McGonagle KA, Zhoa S. Lifetime and 12-month prevalence of DSM-delivered program like RR can improve outcome, even modest
III-R psychiatric disorders in the United States: results from the National Co-ones, in regards to health service utilization or an improvement in Morbidity Survey. Arch Gen Psychiatry 1994; 51: 8-19
functioning, then it will be the first such study for bipolar disorder 2. Angst J. The emerging epidemiology of hypomania and bipolar-II disorder. J Af-fect Disord 1998; 50: 143-51to show that such an approach has merit. A positive result will
3. Murray CJL, Lopez AD. The global burden of disease. The World Health Organi-indicate that computerized programs delivered over the Internet zation. Cambridge (MA): Harvard University Press, 1996
have the potential to help mental health services, clinicians, and 4. Woods SW. The economic burden of bipolar disease. J Clin Psychiatry 2000; 61Suppl. 13: 38-41consumers alike in meet these challenges.
5. Goodwin FK, Jamison KR. Manic-depressive illness. New York: Oxford Universi-Online delivery of information and psychological interventions ty Press, 1990
6. Keck PE, McElory SL, Strakowski SM, et al. Compliance with maintenancemay also be more attractive to some users who may have been puttreatment in bipolar disorder. Psychopharmacol Bull 1997; 33 (1): 87-91off by more conventional methods. Such a medium certainly
7. Coryell W, Scheftner W, Keller M, et al. The enduring psychosocial consequencesallows such information and therapeutic interventions to be deliv- of mania and depression. Am J Psychiatry 1993; 150: 720-7
8. Gitlin MJ, Swendsen J, Heller TL, et al. Relapse and impairment in bipolarered in a format that is more dynamic than any paper-based self-disorder. Am J Psychiatry 1995; 152 (11): 1635-40help manual. Information in computerized programs can also be
9. Judd LL, Akiskal HS, Schettler PJ, et al. The long-term natural history of theupdated more easily to reflect the advancements being made in the weekly symptomatic status of bipolar I disorder. Arch Gen Psychiatry 2002; 59:
530-7understanding of bipolar disorder and in its treatment. Computer-10. Huxley NA, Parikh SV, Baldessarini RJ. Effectiveness of psychosocial treatmentsized programs themselves encourage compliance due to their
in bipolar disorder: state of the evidence. Harvard Rev Psychiatry 2000; 8: 126-interactive structure and instantaneous feedback. 40
11. Colom F, Vieta E, Reinares M, et al. Psychoeducation efficacy in bipolar disorders:At this point in this study, the usefulness and effectiveness of anbeyond compliance enhancement. J Clin Psychiatry 2003; 64: 1101-5
Internet-based process for recruiting participants into a clinical12. Miklowitz DJ. Review of evidence-based psychosocial interventions for bipolar
research study has been established. Given previous research disorder. J Clin Psychiatry 2006; 67 Suppl. 11: 28-33
13. Scott J. Psychotherapy for bipolar disorders: efficacy and effectiveness. J Psy-experiences, it has been estimated that the recruitment of a similarchopharmacol 2006; 20 (2 Suppl.): 46-50
number of participants using established clinical research tech-14. Colom F, Lam D. Psychoeducation: improving outcomes in bipolar disorder. Eur
niques and limited to one site would take 12 months. Furthermore, Psychiatry 2005; 20: 359-64
15. Mitchell PM, Malhi GS, Redwood BL, et al. For the RANZCP Clinical Practicethe accessibility of this study to the bipolar population has led toGuideline Team for Bipolar Disorder. Summary of the guidelines for the
the recruitment of participants not only from all parts of Australia treatment of bipolar disorder. Aust Psychiatry 2003; 11: 39-53
but also from the international community. This has become an 16. American Psychiatric Association. Practice guideline for the treatment of patientswith bipolar disorder. Am J Psychiatry 2002; 159 Suppl. 4: 1-50international study, which is applying established research meth-
17. Taylor CB, Jobson KO, Winzelberg AJ, et al. The use of the Internet to provideodology to evaluate an innovative approach to delivering evidence-based integrated treatment programs for mental health. Psychiatric
Ann 2002; 32: 671-7psychosocial interventions for people with bipolar disorder.18. Christensen H, Griffiths KM. The internet and mental health practice. Evid Based
Ment Health 2003; 6 (3): 66-9
19. Titov N. Status of computerized cognitive behavioural therapy for adults. Aust N ZAcknowledgmentsJ Psychiatry 2007; 41: 95-114
20. Christensen H, Griffiths KM, Jorm A. Delivering interventions for depression byusing the internet; randomised controlled trial. BMJ 2004; 328 (7434): 265The authors wish to thank the following individuals: Gavin Pinto, IT
21. Clarke G, Redi E, Eubanks D, et al. Overcoming Depression on the InternetArchitect and designer of web-based platform, Sentiens Pty Ltd, Perth, West-(ODIN): a randomised control trial of an Internet depression skills interventionern Australia; Dr Dennis Tannenbaum, Consulting Psychiatrist and Executiveprogram. J Med Internet Res 2002; 4: e14
Chair, Sentiens Pty Ltd, Perth, Western Australia; Professor Gordon Parker,22. Clarke G, Eubanks D, Reid E, et al. Overcoming Depression on the Internet
Executive Director, Black Dog Institute, Sydney, New South Wales; and Sue (ODIN) (2): a randomised trial of a self-help depression skills program withGrdovic, Project Manager Community and Consumer Programs, Black Dog reminders. J Med Internet Res 2005; 7: e16Institute, Sydney, New South Wales, Australia. 23. Lange A, Schrieken B, van de Ven JP, et al. ‘Interapy’: the effects of a short
protocolled treatment of posttraumatic stress and pathological grief through theDr Barnes has received a scholarship grant from the University of Newinternet. Behav Cognitive Psychother 2000; 28: 175-92South Wales. Professors Mitchell and Wilhelm have received a NH&MRC
24. Celio AA, Winzelberg AJ, Wilfley DE, et al. Reducing risk factors for eatingprogram grant 230802 and NSW Centre for Mental Health Infrastructuredisorders; comparison of internet and classroom delivered psychoeducation.
grant. Dr Barnes was a past employee of Sentiens Pty Ltd (formally In-J Consulting Clin Psychol 2000; 68: 650-7
frapsych). Dr Harvey is employed as the Research and Development Manager25. Tate DF, Wing RR, Winette RA. Using technology to deliver a behavioural weight
for Sentiens Pty Ltd. Mr Smith is employed as a research officer at Sentiens loss program. JAMA 2001; 285: 1172-7Pty Ltd. Professors Mitchell and Wlihelm have no conflicts of interest relevant 26. Tannenbaum D, Barnes C. Infrapsych bipolar affective disorder recovery roadto the content of this article. program. Bipolar Disord 2004; 6 Suppl. 1: 24
© 2007 Adis Data Information BV. All rights reserved. Dis Manage Health Outcomes 2007; 15 (4)

224 Barnes et al.
27. American Psychiatric Association. Diagnostic and statistical manual of mental 37. First MB, Spitzer RL, Gibbon M. Structured clinical interview for DSM-IV-TRdisorders. 4th rev ed. Washingtion, DC: American Psychiatric Association, Axis I disorders, research version, patient edition (SCID-1/P). New York:2000 Biometrics Research Department, Columbia University, 2001
28. Barnes C, Mitchel P, Wilhelm K. Preventing relapse in people with bipolar 38. Bauer MS, Vojta C, Kinosian B, et al. The internal state scale; replication of itsdisorder using the www-interim results of a RCT [abstract]. ANZ J Psych 2005; discriminating abilities in a multisite, public sector sample. Bipolar Disord39 Suppl. 2: A30-1 2000; 2: 340-6
29. Bauer M, Grof P, Gyulai L, et al. Using technology to improve longitudinal studies: 39. Sheehan DV, Harnett-Sheehan K, Raj BA. A measurement of disability. Int Clinself-reporting with ChronoRecord in bipolar disorder. Bipolar Disord 2004; 6 Psychopharmacol 1996; 11 Suppl. 3: 89-95(1): 67-74
30. Overall JE, Gorham DR. The brief psychiatric rating scale. Psychol Rep 1962; 10:799-812 About the Author: Dr Caryl Barnes is a Conjoint Lecturer and Doctoral
31. Young RC, Biggs JT, Ziegler VE, et al. A rating scale for mania; reliability, Fellow at the School of Psychiatry, University of New South Wales, Sydney,validity, sensitivity. Br J Psychiatry 1978; 133: 429-35 and a Consultant Psychiatrist affiliated to the Black Dog Institute, Sydney.
32. Hirschfeld R, Holzer C, Calabrese C. Validity of the Mood Disorder Questionnaire:She is also a lecturer for the Western Australian Postgraduate Training ina general population study. Am J Psychiatry 2003; 160: 170-80Psychiatry Program. Her research interests include the biological and33. Antony MM, Bieling PJ, Cox BJ, et al. Psychometric properties of the 42-item andpsychological treatment of mood disorders, in particular bipolar disorder21-item versions of the Depression Anxiety Stress Scales (DASS) in clinical
groups and a community sample. Psychol Assessment 1998; 10: 176-81 and its management in women. Her current MD thesis is on the role of the34. Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiatry 1960; Internet in the management of bipolar disorder.
23: 56-62Correspondence: Dr Caryl Barnes, UNSW School of Psychiatry, Room G30,
35. Montgomery SA, Asberg M. A new depression scale designed to be sensitive toBlack Dog Institute Building, Hospital Road, Prince of Wales Hospital,change. Br J Psychiatry 1979; 134: 382-9Randwick, Sydney, NSW 2031, Australia.36. Beck AT, Ward CH, Mendelson M, et al. An inventory measuring depression. Arch
Gen Psychiatry 1961; 4: 561-71 E-mail: [email protected]
© 2007 Adis Data Information BV. All rights reserved. Dis Manage Health Outcomes 2007; 15 (4)











