Embed Size (px)
Citation preview
Evaluation of Abnormal BleedingAmbulatory Medicine Clerkship
01/11/2010Kofi-Buaku Atsina
YSM III
Learning ObjectivesList the differential diagnoses of abnormal bleeding in an adult.
Describe the appropriate diagnostic evaluation for abnormal bleeding in an adult.
Interpret coagulation assays and understand their role in refining differential diagnosis
Understand the coagulation cascadeDescribe the physiologic role of von Willebrand factor in clotting

Case 1 HPI: A 62 y/o mildly overweight black woman with h/o hypertension presents with gingival bleeding after periodontal scaling of her lower-right second molar 5 hours prior to the episode. Her bleeding had persisted despite application of ice and pressure. She reports a similar episode 6 months earlier, also after a periodontal procedure, in which bleeding stopped only after the application of firm pressure for 6 hours. She is otherwise in her USOH and denies any easy bruising, epistaxis, rectal bleeding, hemturia, weakness, fatigue, lightheadedness, fever, arthralgia, dyspnea, jaundice, adbominal pain, back pain, rash or confusion.

PMH/PSH Deep-vein thrombosis in the legs (20 years ago) Cosmetic blepharoplasty, w/o bleeding complications (@ age 20)
Arthroscopic repair of meniscal tear in the left knee without bleeding complications (1 year ago)
Uncomplicated vaginal delivery SH
Former smoker, quit 30 years ago Consumes alcohol infrequently
FH Father died of lung cancer at age 62 Mother still living and in good health at age 88 Brother had colorectal cancer at age 57 No h/o bleeding diathesis
MedsThiazide diuretic
Allergies NKDA

Physical Exam Gen: NAD Vitals: BP: 128/76 mm Hg, P: 80 and regular, RR: 16, O2
saturation 98% on ambient air. HEENT: Oral cavity revealed blood slowly oozing from the
vicinity of the lower-right second molar, with no visible mucosal laceration. But no oral petechiae, bullae, or ulcers. Mild conjunctival pallor was noted, but no scleral icterus. There was no lymphadenopathy.
RESP: Clear to auscultation and percussion. Cor: Mild lateral apical displacement; RRR, no murmur,
rub, or gallop. Abd: Soft and not tender; normal bowel sounds and no
hepatosplenomegaly or masses detected. Rectal examination revealed no masses and a scant amount of brown stool that was negative for occult blood.
EXT: Her extremities were warm, with brisk capillary refill, and no clubbing, cyanosis, or edema. No rashes, petechiae, ecchymoses, or telangiectasias were noted.
Neuro: cranial nerves intact, 5/5 muscle strength, normal sensation, 3/5 deep-tendon reflexes, normal coordination, and gait.

Differential diagnosis?AcquiredTraumaDrugs: Aspirin, wafarin, heparinPlatelet disorder: ITP, TTP/HUS, HITClotting factor deficiency
Liver disease, malnutrition, clotting factor inhibitor, acquired von willebrand disease
Combined platelet and clotting factor disorder: DICVessel wall disease: acquired vasculitides
GeneticPlatelet disorder
Bernard Soulier syndrome, Glanzmann’s thrombasthenia, storage pool disorders
Clotting factor deficiencyHemophilia A, Hemophilia B, von Willebrand disease
Vessel wall abnormalities: Ehlers-Danlos syndrome
Acquired or Genetic?
AcquiredBased on history:Generally healthy personPMH/PSH
Cosmetic blepharoplasty, w/o bleeding complications
Arthroscopic repair of meniscal tear in the left knee without bleeding complications
Uncomplicated vaginal delivery
Nature of Bleeding
Mucosal Bleeding (petechiae, purpura), menorrhagia, prolonged bleeding from minor wounds --> Platelet disorder/ vWF disorder
Deep Tissue Bleeding (Hemathrosis, hematomas, ecchymosis, prolonged post-surgical bleeding ) --> Coagulation factor defect/deficiency

Platelet/vWF disorder or Coagulation disorder?Acquired:
Platelet DisorderQuantitative:
Bone marrow diseases e.g. aplastic anemia, marrow infiltration (leukemia), drug induced e.g alcohol, thiazides, infection (HIV, measles)
Infections eg. HIV, CMV, infectious mononucleosisImmunological e.g. ITPNonimmunologic e.g.TTP/HUSDrug induced e.g. Heparin, quinidine, sulfa compoundsHypersplenism
Qualitative: Aspirin/NSAIDUremia
Acquired von Willebrand DiseaseHypothyroidism, Mechanical/Shear stress, Lymphoproliferative diseases, Pancreatitis, DIC,Decompensated cirrhosis

Effectors of HemostasisVessel Wall IntegrityvWFPlatelet adhesion, activation and aggregation
Coagulation CascadeAnticoagulants and fibrinolytic factors
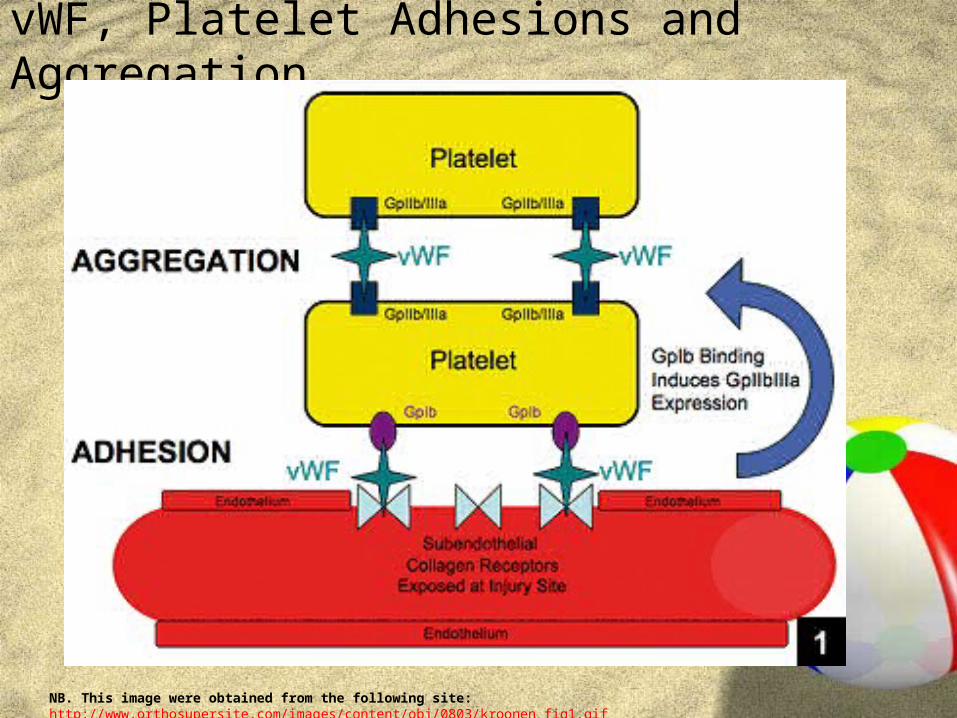
vWF, Platelet Adhesions and Aggregation
NB. This image were obtained from the following site: http://www.orthosupersite.com/images/content/obj/0803/kroonen_fig1.gif

Coagulation cascade

PT/PTTPT PTT Differential Diagnosis
Normal Prolonged Factor VIII, IX, XI, or XII deficiency Lupus anticoagulant Spurious
Prolonged Normal Factor VII deficiency Lupus anticoagulant Spurious
Prolonged Prolonged Factor II, V, X deficiency Abnormalities in fibrin ogen Disseminated intravascular coagulation Lupus anticoagulant Spurious
Normal Normal von Willebrand disease Platelet function abnormality Factor XIII deficiency

Assays for Von Willebrand factor Quantitative or qualitative defects:von Willebrand Ristocetin Cofactorvon Willebrand AntigenFactor VIII levelQualitative defects:Von Willebrand multimer gel analysisRistocetin-induced platelet aggregation (RIPA)

Case 1: Labs
NB. Normal chemistry panel and normal LFT
Variable Results Normal Range
WBC (per mm3 ) 6200 4,000 - 10,000
PMN (%) 49 49 - 79
Lymph (%) 37 11 - 38
Monocytes (%) 13 1 - 12
Hematocrit 31.8 36 - 48
Mean corpuscular vol (µm3)
93 80 - 95
Platelet count (per m m3)
352,000 150,000 - 450,000
BUN (mg/dl) 18 9 - 25
Creatinine (mg/dl) 1.4 0.7 - 1.3
Total protein (g/dl) 8.6 6 - 8
Albumin (g/dl) 3.9 3.7 - 5.4
Thyrotropin (µU/ml) 1.7 0.5 - 5.0
Prothrombin time (sec) 13.7 11.8 - 14.6
Activated thromboplastin time (sec)
49.6 23.8 - 36.6

LabsLab Test Results Normal Range
Erythropoietin Level (mU/ml)
13.3 4.1 - 19.5
Factor VIII activity assay (%)
20 50 - 150
Fibrinogen level (mg/dl) 387 200 - 450
aPTT after mixing of patient’s plasma in 1:1 ratio (sec)
49, corrected to 32 after mixing
23.6 - 36.6
Ristocetin cofactor assay (%)
14 50 - 160
Von Willebrand factor antigen level
22 50 - 160
Von Willebrand factor multimer gel electrophoresis
Loss of high- molecular-weight forms
Normal Pattern
Other data: The serum iron level was 27 µg per deciliter (4.8 µmol per liter), the ferritin level 76 ng per milliliter, and the total iron-binding capacity 314 µg per deciliter (56.2 µmol per liter). Levels of vitamin B12 and folate were normal. The reticulocyte count was 2.7%, and the peripheral-blood smear showed mild erythrocyte anisocytosis but was otherwise normal.
What is your refined DDx?
Acquired Von Willebrand disease
Acquired Von Willebrand disease
Causes:HypothyroidismMechanical/Shear stress, Lymphoproliferative diseases/ collagen vascular diseases
Pancreatitis, DIC, Decompensated cirrhosis
Tumor

Von Willebrand disease
QuantitativeType 1 partial vWF deficiencyType 3: complete vWF deficiency
QualitativeType 2:
2A: decreased affinity of vWF for platelet2B: increased affinity of vWF for platelet2M: decreased platelet dependent function2N: defective factor VIII binding site
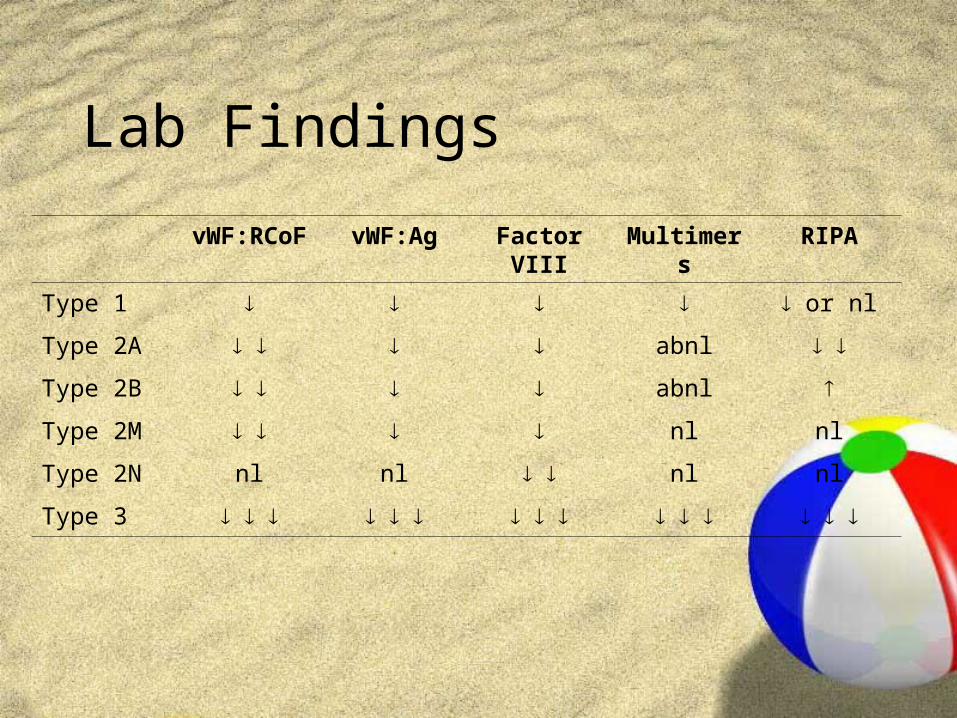
Lab Findings
vWF:RCoF vWF:Ag Factor VIII
Multimers
RIPA
Type 1 or nl
Type 2A abnl
Type 2B abnl
Type 2M nl nl
Type 2N nl nl nl nl
Type 3

Case 2 HPI: A 2-year old boy was brought to the emergency department by his mother for oozing blood from his mouth following a fall nearly 6 hours ago. His mother related that he tended to bleed for prolonged periods from his immunization sites, but there was no history of bruising or hematomas. The patient was on antibiotics for a recent ear infection. There was no known family history of a bleeding disorder.
PE:Gen: Alert, in no apparent distress, development appropriate for age
HEENT: Two small lacerations on the inside of lower lip, oozing bloodRemainder of exam within normal limits (notably, no petechia, bruises, joint swelling)

What is your DDx?
Von Willebrand diseaseFactor VIII and IX deficiency (Hemophilia A, B)
Lupus anticoagulant, factor VIII inhibitor (rare)
Factors XI and XII deficiency (rare)

Initial lab results
Hemoglobin 12.3 g/dl 10.5 - 13.5
Hematocrit 35.4 % 33.0 - 39.0
WBC 7.9*10^9/L 6.0 - 17.5
Platelet 368*10^9/L 156 - 369
PT 11.3s 10.0 - 12.8
aPTT 37.2s 24.4 - 33.2

Additional Work upaPTT 49.6s 28.0 - 38.0
aPTT after mix
35.7s 28.0 - 38.0
Factor VIII 0.16 U/ml 0.60 - 1.50
Factor IX 0.82 U/ml 0.60 - 1.50
Thrombin time
17.3s 16.0 - 22.0
vWF Ag 0.16s 0.78 - 1.53
RCOF <0.10 U/ml 0.50 - 1.50

Final Diagnosis
Von Willebrand Disease

References Cuker A, Connors JM, Katz JT, Levy BD, Loscalzo J; A
Bloody Mystery, N Engl J Med 2009; 361:1887 - 94 Haberichter SL, Balistreri M, Christopherson P,
Morateck P,Gavazova S, Bellissimo DB, Manco-Johnson MJ, Gill JC, Montgomery RR; With type 1 von Willebrand disease with decreased VWF survival Assay of the von Willebrand factor (VWF) propeptide to identify patients, Blood 2008; 108:3344 - 3351
Robbins and Cotran Pathological Basis of Human Disease, 7th ed. Chapter 13 (pg 649 - 659)
Harrison’s Principles of Internal Medicine, 16th ed. Chapter 102
http://path.upmc.edu/cases/case325.html Kroonen LT, Gillingham BL Provencher MT, Orthopedic
Manifestations and Management of Patients With von Willebrand Disease, Orthopedics 2008; 31:263