Embed Size (px)
Citation preview

566 JCOM December 2015 Vol. 22, No. 12 www.jcomjournal.com
Pancreatic cystic Lesions
AbstrAct• Objective:Toreviewthediagnosisandmanagement
ofpancreaticcysticlesions.• Methods:Narrativereviewoftheliterature.• Results: Pancreatic cystic lesions are clinically rel-
evant as some are precursor lesions to pancreaticadenocarcinoma. Mucinous cystic neoplasms andintraductalpapillarymucinousneoplasmsare2com-monly encountered pre-cancerous pancreatic cysts.Manycystsareidentifiedincidentallyduetofrequentuseofhigh-resolutionCTandMRIimagingtechnol-ogy. Proposed diagnostic and management algo-rithmsexisttoguideclinicalpracticebutarelimitedbya lack of evidence and discordance among variousguidelines.Newcyst fluidbiomarkersareunderde-velopmenttodiagnosecysttypesandriskofcancer.
• Conclusion: Pancreatic cysts are increasingly en-counteredinclinicalpracticeandrepresentagrowingproblem.Diagnosticandmanagementalgorithmsareavailabletoassistpracticebutarelimitedbytheavail-ableevidence.Amultidisciplinaryapproachisrecom-mended.
In the United States there were an estimated 46,420 new cases of pancreatic cancer in 2014 [1]. Of all major cancers, pancreatic cancer had the lowest 5-year
survival rate at 6% [1]. Of the 3 known precursor lesions to pancreas adenocarcinoma, 2 are pancreatic cysts [2]. Correctly identifying those with cancer, those with cancer potential (premalignant), and those that are benign (har-boring no malignant potential) can be difficult.
The estimated prevalence of pancreatic cysts is ap-proximately 2.6% [3]. In some case series using mag-netic resonance imaging (MRI), higher rates of detection of approximately 13.5% have been observed [4]. The prevalence increases with age reaching nearly 10% by the 8th decade of life [3,4]. Mucinous cystic neoplasms (MCNs) and intraductal papillary mucinous neoplasms (IPMNs) account for about 30% of pancreatic cysts [5].
These cysts are defined as mucinous cysts and are known precursor lesions to pancreatic adenocarcinoma [6]. The other most common types of cysts are serous cystic neo-plasms (SCNs), comprising 20% of pancreatic cysts, and pseudocysts, comprising 30% [5]. These cysts are con-sidered nonmucinous cysts and are almost always benign [7,8]. There are multiple other pancreatic cyst types to consider, which are summarized in Table 1 [9,10,11]. In this review, we will cover the diagnosis and management of the most common pancreatic cysts in a case-based format.
Case 1A 57-year-old male had a 1.5-cm pancreatic cyst located in the head that was found on computed
tomography (CT) imaging for suspected renal colic. He had no history or complaints suspicious for pancre-atic disease. A CT pancreas protocol scan was obtained, which demonstrated a simple appearing cyst with no mural nodules. The pancreatic and biliary ducts were normal. His laboratory evaluations including liver func-tion testing and lipase were normal.
• What is the approach to incidentally discov-eredpancreaticcysts?
While many pancreatic cysts are first discovered by cross sectional imaging (CT or MRI), the diagnostic accuracy of defining cyst type and the presence of malignancy is imperfect. The area under the curve (AUC) for dif-ferentiating malignant from benign pancreatic cysts ranges from 0.64 to 0.82 for CT and 0.73 to 0.91 for MRI, and no difference between the 2 were observed
Evaluation and Management of Pancreatic Cystic LesionsThomas Zikos, MD, and Walter G. Park, MD, MS
From the Department of Medicine, Stanford University School of Medicine, Stanford, CA.

www.jcomjournal.com Vol. 22, No. 12 December 2015 JCOM 567
[12,13]. Several guidelines are currently available to offer guidance on management [6,14,15,16,17]. Much of the current evidence includes retrospective case series with no randomized control trials. The guidelines, therefore, mostly represent consensus-based expert extrapolation of available data.
The second iteration of guidelines put forth by an international panel of experts is perhaps the most widely accepted among pancreatologists. Published in 2012, the panel narrowed the criteria from their first guidelines (2006) regarding surgical resection of a pancreatic cyst [6,17]. Patients with a pancreatic cyst who have any of the following 3 features (or “high-risk stigmata”) warrant immediate consideration of surgical resection. These features are (1) obstructive jaundice in the setting of a head cyst, (2) presence of an enhancing solid component within the cyst, and (3) main pancreatic ductal dilation of 10 or more mm [6]. The presence of other “worrisome” features should prompt further investigation with endo-scopic ultrasound (EUS) and these include (1) presenta-tion of a cyst with pancreatitis, (2) cysts 3 cm or greater in size, (3) thickened or enhancing cyst walls, (4) nonen-hancing mural nodules, and (5) tapering of the pancreatic duct with distal pancreatic atrophy (Table 2)[6].
The American Gastroenterological Association (AGA) recently produced guidelines in 2015 [14]. In compari-son to the international consensus guidelines, there are a few key differences, which have now become a point of vigorous debate and disagreement among pancreatolo-gists and confusion among general gastroenterologists and surgeons in the community. Where the international consensus guidelines have stricter criteria to define the appropriateness of surgery, the AGA guidelines are more liberal. AGA defined cysts appropriate for surgery as hav-
ing 2 out of 3 of the following features: (1) cyst size ≥ 3 cm, (2) presence of a solid component in the cyst, and (3) dilation of the main pancreatic duct. Those having 1 out of 3 criteria were defined as needing further inves-tigation with EUS [14]. These criteria are more relaxed and will likely lead to more surgical resections.
Another difference involves surveillance recommen-dations. The international consensus guidelines do not define a period when surveillance can be safely stopped. The AGA guidelines define 5 years as the period where if there is no significant change in the cyst from surveil-lance MRIs performed every 1 to 2 years, then surveil-lance can be stopped [14]. As the natural history of these cysts remain substantially uncertain, with evidence that malignant transformation occurs after 5 years, this particular recommendation by the AGA remains highly controversial [18,19]. Other differences between these 2 guidelines are summarized in Table 2 [6,14].
Until the surveillance recommendations by the AGA are validated with further studies, we generally follow the 2012 international consensus guidelines. We generally prefer MRI for initial and surveillance evaluations of pan-creatic cysts. Besides the lack of radiation exposure, some studies show MRI to have better inter-reader variability [20], better resolution to show cyst communication with the main pancreatic duct [21], and better characteriza-tion of peripheral pancreatic cysts [22]. At our center, when a solid mass is suspected, a CT pancreas protocol is preferred in lieu of an MRI by our surgical team.
Case1Continued
Given the smaller size and absence of high-risk stigmata or worrisome features, surveillance of his
cyst was recommnded. He unfortunately did not follow up
Case-based review
Table 1. DifferentialDiagnosisofPancreaticCysts
Malignant/Premalignant Benign
•Intraductalpapillarymucinousneoplasms(IPMNs) •Serouscysticneoplasms(SCNs)*•Mucinouscysticneoplasms(MCNs) •Pancreaticfluidcollections(includingpseudocysts)
•Solidpseudopapillaryneoplasms(SPNs) •Abscesses
•Cysticdegenerationof: •Congenitalcysts
•Pancreaticadenocarcinoma •Retentioncysts
•Metastaticdisease •Squamouscysts
•Neuroendocrinetumors •Lymphangiomas
•Mucinousnon-neoplasticcysts
*SCNscanrarelyundergomalignanttransformation.

568 JCOM December 2015 Vol. 22, No. 12 www.jcomjournal.com
Pancreatic cystic Lesions
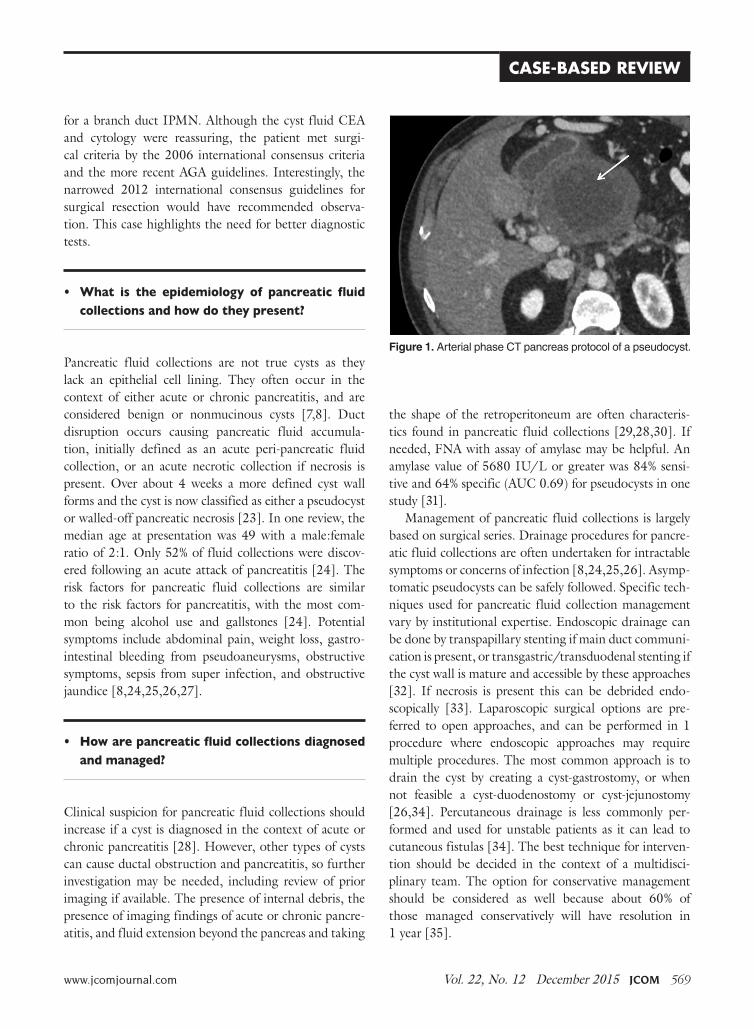
and presented 7 years later with several months of abdomi-nal pain and esophageal reflux symptoms. A CT scan was repeated which showed that the cyst had grown to 10.7 x 8.8 x 8.9 cm with an adjacent smaller cyst (Figure 1). The cyst was surrounded by a thick rind of enhancing tis-sue and had occluded the splenic and superior mesenteric veins, and was encasing the splenic artery. The main pan-creatic duct was dilated at 7 mm with pancreatic body and tail atrophy. There was no evidence of metastatic disease or pathological lymph nodes. An EUS was performed and showed a large complex cyst with thick walls of up to 2 cm. Fine-needle aspiration (FNA) yielded a carcinoembryonic antigen (CEA) value of 2.3 ng/mL and cytology showed “bland epithelial cells.”
Despite the reassuring CEA and cytology results, a high concern for a malignant cystic lesion remained based on cyst size, main pancreatic duct dilation, and atrophy noted in the distal pancreas. The patient under-went surgical resection including subtotal pancreatec-tomy, splenectomy, subtotal gastrectomy, and superior mesenteric and portal vein resection with reconstruction. Pathology revealed the cyst to be a benign pseudocyst.
This case reflects some of the critical challenges in current management of pancreatic cysts. By history, this patient had no suspicion for pancreatitis, making a pseudocyst less likely in a differential diagnosis. When the patient presented 7 years later, again with no re-ported history of pancreatitis, there was clinical concern
Table 2. ComparisonofguidelinesforManagementofPancreaticCysts
2012 International Consensus Guidelines [6]
2015 American Gastroenterological Association Guidelines [14]
Preferredimaging: •PancreaticprotocolCTOR •MRIwithMRCP
•MRIwithMRCP
Considersurgeryifthefollowinghigh-riskfeaturesarepresent:
•Obstructivejaundiceinthesettingofapancreaticheadcyst
•2of3riskfactors:cyst≥3cm,presenceofasolidcomponentinthecyst,dilationofthemainpancreaticduct•Enhancingsolidcomponentinthecyst
•Mainpancreaticductdilation≥10mm
ConsiderEUSwithFNAifthefollowingconcerningfeaturesarepresent:
SurgeryifEUS/FNAconcerning*
•Presentationwithpancreatitis •1of3riskfactors:cyst≥3cm,presenceofasolidcomponentinthecyst,dilationofthemainpancreaticduct
•Cyst≥ 3cm
•Thickened/enhancingcystwalls
•Mainpancreaticduct5–9mm
•Non-enhancingmuralnodules
•Abrupttaperingofthepancreaticductwithdistalpancreaticatrophy
•Abrupttaperingofthepancreaticductwithdistalpancreaticatrophy
Ifsurgeryisnotundertaken,surveillanceisrecommendedifthepatientisasurgi-calcandidate:
•Cyst≥ 3cmorinconclusiveEUS:alter-natingEUSandMRIevery3–6months
•SurveillancewithMRIevery1–2years.Stopafter5yearsifnochange.
•Cyst2–3cm:EUSin3–6months,thenalternateEUSwithMRIatlengtheningintervalsifstable
•Cyst1–2cm:CTorMRIyearlyfor2years,thenlengthenintervalifnochange
•Cyst<1cm:CT/MRIin2–3years
Surveillanceafteroperation: •Surveillanceidenticaltopancreaticadeno-carcinomaifinvasivediseasepresent
•IfdysplasiaorinvasivediseaseispresentrecommendyearlyMRI.Nodefinitivestopdate.•Ifnon-invasiveIPMNobtainCTorMRIin
6months(considerincreasingintervalsifstable
*The2012InternationalConsensusGuidelinesdefineconcerningEUS/FNAfindingsasmuralnodules,mainpancreaticduct involve-ment,orpositivecytology.TheAmericanGastroenterologicalAssociationdoesnotspecificallycommentonthisintheirreview.
www.jcomjournal.com Vol. 22, No. 12 December 2015 JCOM 569
for a branch duct IPMN. Although the cyst fluid CEA and cytology were reassuring, the patient met surgi-cal criteria by the 2006 international consensus criteria and the more recent AGA guidelines. Interestingly, the narrowed 2012 international consensus guidelines for surgical resection would have recommended observa-tion. This case highlights the need for better diagnostic tests.
• What is the epidemiology of pancreatic fluidcollectionsandhowdotheypresent?
Pancreatic fluid collections are not true cysts as they lack an epithelial cell lining. They often occur in the context of either acute or chronic pancreatitis, and are considered benign or nonmucinous cysts [7,8]. Duct disruption occurs causing pancreatic fluid accumula-tion, initially defined as an acute peri-pancreatic fluid collection, or an acute necrotic collection if necrosis is present. Over about 4 weeks a more defined cyst wall forms and the cyst is now classified as either a pseudocyst or walled-off pancreatic necrosis [23]. In one review, the median age at presentation was 49 with a male:female ratio of 2:1. Only 52% of fluid collections were discov-ered following an acute attack of pancreatitis [24]. The risk factors for pancreatic fluid collections are similar to the risk factors for pancreatitis, with the most com-mon being alcohol use and gallstones [24]. Potential symptoms include abdominal pain, weight loss, gastro-intestinal bleeding from pseudoaneurysms, obstructive symptoms, sepsis from super infection, and obstructive jaundice [8,24,25,26,27].
• Howarepancreaticfluidcollectionsdiagnosedandmanaged?
Clinical suspicion for pancreatic fluid collections should increase if a cyst is diagnosed in the context of acute or chronic pancreatitis [28]. However, other types of cysts can cause ductal obstruction and pancreatitis, so further investigation may be needed, including review of prior imaging if available. The presence of internal debris, the presence of imaging findings of acute or chronic pancre-atitis, and fluid extension beyond the pancreas and taking
the shape of the retroperitoneum are often characteris-tics found in pancreatic fluid collections [29,28,30]. If needed, FNA with assay of amylase may be helpful. An amylase value of 5680 IU/L or greater was 84% sensi-tive and 64% specific (AUC 0.69) for pseudocysts in one study [31].
Management of pancreatic fluid collections is largely based on surgical series. Drainage procedures for pancre-atic fluid collections are often undertaken for intractable symptoms or concerns of infection [8,24,25,26]. Asymp-tomatic pseudocysts can be safely followed. Specific tech-niques used for pancreatic fluid collection management vary by institutional expertise. Endoscopic drainage can be done by transpapillary stenting if main duct communi-cation is present, or transgastric/transduodenal stenting if the cyst wall is mature and accessible by these approaches [32]. If necrosis is present this can be debrided endo- scopically [33]. Laparoscopic surgical options are pre-ferred to open approaches, and can be performed in 1 procedure where endoscopic approaches may require multiple procedures. The most common approach is to drain the cyst by creating a cyst-gastrostomy, or when not feasible a cyst-duodenostomy or cyst-jejunostomy [26,34]. Percutaneous drainage is less commonly per-formed and used for unstable patients as it can lead to cutaneous fistulas [34]. The best technique for interven-tion should be decided in the context of a multidisci-plinary team. The option for conservative management should be considered as well because about 60% of those managed conservatively will have resolution in 1 year [35].
Figure 1.ArterialphaseCTpancreasprotocolofapseudocyst.
Case-based review

570 JCOM December 2015 Vol. 22, No. 12 www.jcomjournal.com
Pancreatic cystic Lesions
Case 2A 65-year-old male had a CT scan of the abdo-men and pelvis for hematuria. While no clear
source of hematuria was identified, a pancreatic cyst was described prompting a dedicated CT pancreas proto-col scan. This showed a 3.4 x 4.0 x 5.5 cm multicystic lesion in the head of the pancreas with mural nodules but no dilation of the main pancreatic duct or biliary ducts (Figure 2). He had no correlating symptoms and lab test results were normal.
• WhatistheroleofendoscopicultrasoundwithFNAinthediagnosisofpancreaticcysts?
While more invasive than CT or MRI, EUS provides detailed imaging to characterize relevant clinical features and allows fine needle aspiration of the cyst fluid and tissue of intra-cystic masses (Table 2) [6,14]. While MRI imaging resolution is continuing to improve [22,36,37], EUS is generally considered superior [38] for diagnosing high-risk lesions. A limitation of EUS, however, is signifi-cant inter-observer variability when compared with MRI [37,39,40].
EUS enables FNA of the cyst, which offers unique oppor-tunities for diagnosis. Cyst fluid cytology un-fortunately has limited diagnostic yield, with a recent meta-analysis showing sensitivity 63%, specificity 88%, and AUC of 0.89 in differentiating mucinous from non-mucinous cysts [41]. The low sensitivity is likely because cyst fluid is paucicellular. Techniques that include target-ing the cyst wall are under investigation and may improve
the diagnostic yield of cytological analysis [42]. Tumor markers such as CEA have been widely used in the cyst fluid, with a value > 192 ng/mL having 63% sensitivity and 88% specificity (AUC of 0.79) for mucinous pancre-atic cysts [43]. Other cyst fluid markers have been or are being developed including mutated KRAS DNA [44], mutated GNAS DNA [45,46], micro RNA [47,48], glucose [49], proteomic analysis [50], and multiple other molecules [51]. At this time, many of these markers are under investigation.
Case2Continued
An endoscopic ultrasound was performed and showed normal main pancreatic and common bile
ducts. No intra-cystic mural nodules were observed. FNA was performed. Cytology showed “paucicellular fluid” and the cyst fluid CEA was 319 ng/mL. Having met the original consensus criteria for surgical resection [17] based on size, the presence of mural nodules, and due to suspicion for a mucinous cyst based on the CEA level, the patient underwent a Whipple procedure. The final pathol-ogy was a branch-duct IPMN with moderate dysplasia.
• What interventionsexist fortreatingpancre-aticcysts?
Surgery is the mainstay of treatment for pancreatic cysts. The most common surgical procedure for worri-some cysts in the head of the pancreas is a pancreato-duodenectomy (Whipple procedure). For cysts in the distal pancreas, a laparoscopic distal pancreatectomy can be performed [52,53]. Middle pancreatectomy, total pancreatectomy, and enucleation are less commonly performed and remain under investigation. The most common complications after surgery are surgical site and nonsurgical site infection, bleeding, pancreatic fistula, and delayed gastric emptying [52,53]. Overall complica-tion rate for pancreatic cyst surgery is 27% to 39%, and perioperative mortality is 0.5% to 4% at high-volume centers [52,53].
An area of active investigation involves EUS-directed chemical cyst ablation. Prior studies using ethanol intra-cystic injection alone showed cyst resolution in 33% of patients [54]. A combination of ethanol and paclitaxel showed cyst resolution in 62% of patients [55]. Though these techniques offer a less invasive alternative to sur-
Figure 2. Left panel:CTscanshowingabranchduct intra-ductalpapillarymucinousneoplasm.Right panel:Endoscopicultrasoundimageofthesamecyst.

www.jcomjournal.com Vol. 22, No. 12 December 2015 JCOM 571
gery, the complete eradication of dysplastic cystic epithe-lium remains uncertain and long-term efficacy is unclear. Thus, these techniques should only be considered in the context of a clinical trial or perhaps in patients who are not surgical candidates [56].
Case 3A 72-year-old male with a history of pancreatitis 23 years ago complicated by a pseudocyst, who
is status post cyst jejunostomy and cholecystectomy pre-sented for evaluation. He was having colicky abdominal pain consistent with prior episodes of nephrolithiasis, and a non-contrast CT scan was obtained that showed a cystic mass in the head of the pancreas. His labora-tory test results including liver function tests and lipase were normal. A CT pancreas protocol was obtained and showed a 2.4 x 4.6 cm cystic lesion without mural nod-ules in the head of pancreas (Figure 3). The cyst was continuous with the main duct, which was dilated to 0.9 cm and the common bile duct was dilated to 1.4 cm. There was severe atrophy of the pancreas upstream of the cyst, and small mesenteric lymph nodes. An endo-scopic ultrasound with FNA showed similar findings to the CT, but a CEA was measured at 2298 ng/mL (Figure 3). Given the concerning imaging findings and an elevated CEA, a Whipple procedure was performed and final pathology showed a main-duct IPMN with in situ carcinoma.
• WhatistheepidemiologyofIPMNsandhowdotheypresent?
IPMNs are mucin-producing lesions (mucinous cysts) of the exocrine pancreas involving either the main or branch ducts that have the potential to develop into pancreatic adenocarcinoma [57]. The mean age at presentation for both branch duct IPMNs (BD-IPMNs) and main duct IPMNs (MD-IPMNs) is around 65 years [58,59]. In the United States, the male to female prevalence ratio is equal, though there is some geographic variation among different countries [58]. Risk factors for IPMN forma-tion include diabetes, chronic pancreatitis, and a family history of pancreatic adenocarcinoma [60]. Presentation is often asymptomatic but may present with pancreatitis, abdominal pain, weight loss, jaundice, and pancreatic exocrine insufficiency [61]. They tend to occur in the
pancreatic head [29]. IPMNs involve either the main pancreatic duct or branch duct or both [62], but this is not always visible by imaging [21]. MRI with MRCP is considered superior to CT in characterizing these lesions, specifically in identifying a connection with the pancre-atic ducts [21].
• HowareIPMNsdiagnosedandmanaged?
MD-IPMNs harbor a higher risk of malignancy than BD-IPMNs. In one series, 64% of MD-IPMN resected specimens contained cancer [63]. Because of the high cancer risk, all guidelines recommend surgical resection for appropriate patients [6,14,15,16,17]. BD-IPMNs have a lower risk of cancer at diagnosis, present in 19.5% of resected specimens in one study [63]. As a surgical series, this may overstate the true prevalence, which is supported by another study. A cohort of 103 suspected BD-IPMNs patients were observed and those with high-risk features were resected. The overall rate of cancer at 5 years was 2.6%, and only 1 of 103 patients developed non-resectable disease [64]. For these reasons, suspected BD-IPMNs can often be safely monitored if they do not harbor any high risk stigmata as defined by the in-ternational consensus criteria (Table 2)[6]. Otherwise, suspected BD-IPMNs are managed in a similar manner to other pancreatic cysts (Table 2) [6,14].
Prognosis after resection is more favorable for IPMNs than for pancreatic adenocarcinoma, possibly due to ear-lier stage of detection. The 5-year survival for BD-IPMN
Case-based review
Figure 3. Left panel:CTscanshowingamainductintraductalpapillarymucinousneoplasm.Right panel:Endoscopicultra-soundshowingadilatedpancreaticduct(labeledPD)causedbythecystseenintheCTscan.

572 JCOM December 2015 Vol. 22, No. 12 www.jcomjournal.com
Pancreatic cystic Lesions
is 90% after resection, and 47% for MD-IPMN after resection [62]. Survival rates for IPMNs with invasive adenocarcinoma are lower with a combined overall sur-vival 24% to 42% at 5 years. Survival rates are similar to the survival rate for non-cystic pancreatic adenocarci-noma when controlling for size, invasiveness, and lymph node metastasis [65,66].
Guidelines for surveillance after resection have even fewer applicable studies. The 5-year postoperative recur-rence rate is 0 to 20% for IPMNs [6]. The revised inter-national consensus guidelines recommends surveillance 6 months after resection with CT or MRI for all IPMNs, but with no recommendation given on how long to con-tinue surveillance [6]. For patients with invasive disease, the same follow up is recommended as for standard inva-sive adenocarcinoma [6]. The AGA recommends yearly MRI only for only patients with high-grade dysplasia or invasive disease, with consideration for lifelong surveil-lance [14].
Case 4A 44-year-old previously healthy female presents with 2 months of epigastric pain. Her laboratory
test results, including liver function testing, were nor-mal. A CT of the abdomen and pelvis showed an 11-cm unilocular cyst in the tail of the pancreas (Figure 4). Since the imaging findings were highly suggestive of a MCN, no further workup was done and a laparoscopic spleen preserving distal pancreatectomy was performed. Pathology confirmed a mucinous cystic neoplasm with low-grade dysplasia.
• WhatistheepidemiologyofMCNsandhowdotheypresent?
MCNs are mucin-producing lesions (mucinous cysts) of the exocrine pancreas histologically defined by the pres-ence of ovarian stroma [67]. They have the potential to develop into pancreatic adenocarcinoma. Unlike IPMNs, MCNs occur almost exclusively in women, and patients are generally younger. In one series, 99.7% of MCNs oc-curred in females, with a mean age of 47 [67]. Presenting symptoms, as with other cysts, are often vague. These include abdominal pain, fatigue, weight loss, pancreatitis, and a palpable mass. Only 25% of patients are asymptom-atic [68].
• HowareMCNsdiagnosedandmanaged?
Approximately 95% of MCNs are located in the body or tail of the pancreas [67]. These lesions do not com-municate with the pancreatic ducts unlike IPMNs, though they may still cause ductal obstruction and dilation [29]. They are often one large unilocular cyst with a thick cyst wall, but in 20% of cases they can have multiple septations [29]. Peripheral eggshell calcifica-tion on CT is present in roughly 25% of cases, which is sometimes helpful in differentiating these lesions from serous cystic neoplasms, which often have central calcification [69].
When diagnosed, MCNs are surgically removed [6,14]. A recent surgical series found that the rate of high-grade dysplasia in resected specimens was 5.5%, and the risk of invasive disease was 4.4% [70]. This data suggests that a more conservative approach of observa-tion rather than immediate resection may be reasonable for some patients [70]. The prognosis is very good after MCN resection, with a 5-year survival of 97% to 100% for all comers [68,70]. However, invasive MCNs have a lower 5-year survival rate ranging from 15% to 75% [70,71]. Per the AGA guidelines, patients with invasive disease or dysplasia should undergo yearly surveillance with MRI [14]. This recommendation is based on a potential field defect described with IPMNs. However, the international consensus guidelines only recommends surveillance if invasive disease is present [6,68,71,72].
Figure 4. ArterialphasepancreasprotocolCTofamucinouscysticneoplasm.

www.jcomjournal.com Vol. 22, No. 12 December 2015 JCOM 573
Case 5A 59-year-old male presents for evaluation of sudden onset abdominal pain and an 8-pound
weight loss over the past few months. Seven years ago a pancreatic cyst was diagnosed and has since been ob-served by serial imaging. His lipase was 400 U/L (nor-mal < 82) with normal liver function tests. A CT scan of the abdomen and pelvis showed peri-pancreatic stranding consistent with pancreatitis and a large complex cyst in the head of the pancreas.
After the acute pancreatitis resolved, a CT pancreas protocol was performed for better characterization of the cyst. This showed a 5.9 x 5.3 x 1.5 cm, multiloculated cystic lesion without mural nodules, with multiple ad-ditional subcentimeter lesions. He underwent an EUS, which confirmed the CT findings (Figure 5). FNA was performed and the cytology showed “paucicellular fluid” and the CEA was 0.9 ng/mL. Due to his weight loss and presentation with pancreatitis, a Whipple procedure was performed and pathology showed a serous cystic neoplasm.
• WhatistheepidemiologyofSCNsandhowdotheypresent?
SCNs are benign non–mucin-producing cystic lesions that are characterized by a glycogen-rich epithelium on histology [73]. Of patients with SCNs, 74% are female, with a median age 58 [10]. When diagnosed, most pa-tients are usually asymptomatic (61%), but 27% present with abdominal pain. Other symptoms include jaundice, pancreatitis, nausea, and presence of a palpable abdomi-nal mass. SCNs are more common in patients with von Hippel-Lindau syndrome [74].
• HowareSCNsdiagnosedandmanaged?
These cysts have fairly even distribution when discovered in the pancreas [53]. About 74% of lesions have smaller micro-cystic components [75]. About 20% of lesions have a characteristic honeycomb appearance, which is highly suggestive of an SCN [76]. About 30% of pa-tients have a characteristic central stellate scar on CT which is also highly suggestive of an SCN [76]. Unlike
mucinous neoplasms, peripheral calcification is usually not seen [69].
Malignancy associated with these cysts is very rare, with the largest cohort study reporting a rate of 0.1% [10]. The diagnosis can commonly be made by its unique imaging appearance [10]. Diagnostic biomarkers that may identify such cysts with more certainty are under ac-tive investigation [77]. Resection is reasonable and often performed for SCNs when they cause debilitating symp-toms including refractory abdominal pain or pancreatitis. When resected and confirmed by pathology, no surveil-lance is required [14,78].
Conclusion
Pancreatic cysts are common incidental findings in clini-cal practice today. Many cause anxiety due to their asso-ciation with pancreas cancer, but most are indolent and safe to observe. Even those cysts with malignant potential grow slowly and immediate surgery is often unneces-sary. Several guidelines have been developed, and while there are similarities between them, there are enough critical differences unfortunately to cause some confu-sion among practitioners today. Further robust research is needed to help address and reconcile these differences. In the meantime, a multidisciplinary approach is highly recommended at dedicated centers of excellence for pan-creatic diseases.
Corresponding author: Walter G. Park, MD, MS, 300 Pasteur Drive, MC: 5187, Stanford, CA 94305, [email protected].
Funding/support: Dr. Park is funded by an American College of Gastroenterology Junior Faculty Development Award and is a subcontinent for the National Cancer Institute's Early Detection Research Network.
Case-based review
Figure 5. Left panel: ArterialphasepancreasprotocolCTofaserouscysticneoplasm.Right panel: Endoscopicultrasoundimages of the same serous cystic neoplasm, labeled cysticmass.

574 JCOM December 2015 Vol. 22, No. 12 www.jcomjournal.com
Pancreatic cystic Lesions
Financial disclosures: None.
Author contributions: conception and design, TZ, WGP; analysis and interpretation of data, WGP; drafting of article, TZ, WGP; critical revision of the article, TZ, WGP.
References1. DeSantis CE, Lin CC, Mariotto AB, et al. Cancer treat-
ment and survivorship statistics, 2014. CA Cancer J Clin 2014;64:252–71.
2. Hruban RH, Maitra A, Kern SE, Goggins M. Precur-sors to pancreatic cancer. Gastroenterol Clin North Am 2007;36:831–49.
3. Laffan TA, Horton KM, Klein AP, et al. Prevalence of un-suspected pancreatic cysts on MDCT. Am J Roentgenol 2008;191:802–7.
4. Lee KS, Sekhar A, Rofsky NM, Pedrosa I. Prevalence of inci-dental pancreatic cysts in the adult population on MR imag-ing. Am J Gastroenterol 2010;105:2079–84.
5. Volkan Adsay N. Cystic lesions of the pancreas. Mod Pathol 20(1 Suppl):S71–93.
6. Tanaka M, Fernández-del Castillo C, Adsay V, et al. In-ternational consensus guidelines 2012 for the manage-ment of IPMN and MCN of the pancreas. Pancreatology 2012;12:183–97.
7. Galanis C, Zamani A, Cameron J, et al. Resected serous cystic neoplasms of the pancreas: a review of 158 patients with recommendations for treatment. J Gastrointest Surg 2007;11:820–6.
8. Vitas G, Sarr M. Selected management of pancreatic pseu-docysts: operative versus expectant management. Surgery 1992;111:123–30.
9. Jani N, Bani Hani M, Schulick RD, et al. Diagnosis and man-agement of cystic lesions of the pancreas. Diagn Ther Endosc 2011;2011:478913.
10. Jais B, Rebours V, Malleo G, et al. Serous cystic neoplasm of the pancreas: a multinational study of 2622 patients under the auspices of the International Association of Pancreatology and European Pancreatic Club (European Study Group on Cystic Tumors of the Pancreas). Gut 2015 Jun 4.
11. Kim YS, Cho JH. Rare nonneoplastic cysts of pancreas. Clin Endosc 2015;48:31–8.
12. Visser BC, Yeh BM, Qayyum A, et al. Characterization of cys-tic pancreatic masses: relative accuracy of CT and MRI. Am J Roentgenol 2007;189:648–56.
13. Lee H-J, Kim M-J, Choi J-Y, et al. Relative accuracy of CT and MRI in the differentiation of benign from malignant pan-creatic cystic lesions. Clin Radiol 2011;66:315–21.
14. Scheiman JM, Hwang JH, Moayyedi P. American Gastroen-terological Association technical review on the diagnosis and management of asymptomatic neoplastic pancreatic cysts. Gastroenterology 2015;148:824–48.
15. Berland LL, Silverman SG, Gore RM, et al. Managing incidental findings on abdominal CT: white paper of the ACR Incidental Findings Committee. J Am Coll Radiol 2010;7:754–73.
16. Khalid A, Brugge W. ACG practice guidelines for the diag-nosis and management of neoplastic pancreatic cysts. Am J Gastroenterol 2007;102:2339–49.
17. Tanaka M, Chari S, Adsay V, et al. International consensus guidelines for management of intraductal papillary mucinous neoplasms and mucinous cystic neoplasms of the pancreas. Pancreatol Off J Int Assoc Pancreatol IAP Al 2006;6(1-2).
18. Ahn D-W, Lee SH, Kim J, et al. Long-term outcome of cystic lesions in the pancreas: a retrospective cohort study. Gut Liver 2012;6:493–500.
19. Khannoussi W, Vullierme MP, Rebours V, et al. The long term risk of malignancy in patients with branch duct intraductal papillary mucinous neoplasms of the pancreas. Pancreatol Off J Int Assoc Pancreatol IAP Al 2012;12:198–202.
20. Grieser C, Heine G, Stelter L, et al. Morphological analysis and differentiation of benign cystic neoplasms of the pancreas using computed tomography and magnetic resonance imag-ing. Fortschr Röntgenstr 2013;185:219–27.
21. Waters J, Schmidt CM, Pinchot J, et al. CT vs MRCP: optimal classification of IPMN type and extent. J Gastrointest Surg 2008;12:101–9.
22. Duconseil P, Turrini O, Ewald J, et al. “Peripheric” pancreatic cysts: performance of CT scan, MRI and endoscopy according to final pathological examination. HPB 2015;17:485–9.
23. Banks PA, Bollen TL, Dervenis C, et al. Classification of acute pancreatitis—2012: revision of the Atlanta classification and definitions by international consensus. Gut 2013;62:102–11.
24. Sanfey H, Aguilar M, Jones R. Pseudocysts of the pancreas, a review of 97 cases. Am Surg 1994;60:661–8.
25. Cheruvu CVN, Clarke MG, Prentice M, Eyre-Brook IA. Conservative treatment as an option in the management of pancreatic pseudocyst. Ann R Coll Surg Engl 2003;85:313–6.
26. Usatoff V, Brancatisano R, Williamson RCN. Operative treat-ment of pseudocysts in patients with chronic pancreatitis. Br J Surg 2000;87:1494–9.
27. Marshall G, Howell DA, Hansen BL, et al. Multidisci-plinary approach to pseudoaneurysms complicating pancreatic pseudocysts: Impact of pretreatment diagnosis. Arch Surg 1996;131:278–83.
28. Sahani DV, Kadavigere R, Saokar A, et al. Cystic pancreatic le-sions: a simple imaging-based classification system for guiding management. RadioGraphics 2005;25:1471–84.
29. Tirkes T, Aisen A, Cramer H, et al. Cystic neoplasms of the pancreas; findings on magnetic resonance imaging with patho-logical, surgical, and clinical correlation. Abdom Imaging 2014;39:1088–101.
30. Macari M, Finn ME, Bennett GL, et al. Differentiating Pancreatic cystic neoplasms from pancreatic pseudocysts at MR Imaging: value of perceived internal debris. Radiology 2009;251:77–84.
31. Park WG, Mascarenhas R, Palaez-Luna M, et al. Diagnostic performance of cyst fluid carcinoembryonic antigen and amylase in histologically confirmed pancreatic cysts. Pancreas 2011;40:42–5.
32. Braden B, Dietrich CF. Endoscopic ultrasonography-guided endoscopic treatment of pancreatic pseudocysts and walled-off necrosis: New technical developments. World J Gastroenterol

www.jcomjournal.com Vol. 22, No. 12 December 2015 JCOM 575
WJG 2014;20:16191–6. 33. van Brunschot S, Fockens P, Bakker O, et al. Endoscopic
transluminal necrosectomy in necrotising pancreatitis: a sys-tematic review. Surg Endosc 2014;28:1425–38.
34. Pan G, Wan MH, Xie K-L, et al. Classification and man-agement of pancreatic pseudocysts. Medicine (Baltimore). 2015;94:e960.
35. Yeo CJ, Bastidas JA, Lynch-Nyhan A, et al. The natural his-tory of pancreatic pseudocysts documented by computed tomography. Surg Gynecol Obstet 1990;170:411–7.
36. Chebib I, Yaeger K, Mino-Kenudson M, Pitman MB. The role of cytopathology and cyst fluid analysis in the preop-erative diagnosis and management of pancreatic cysts >3 cm. Cancer Cytopathol 2014;122:804–9.
37. Kim JH, Eun HW, Park H-J, et al. Diagnostic performance of MRI and EUS in the differentiation of benign from malignant pancreatic cyst and cyst communication with the main duct. Eur J Radiol 2012;81:2927–35.
38. Khashab MA, Kim K, Lennon AM, et al. Should we do EUS/FNA on patients with pancreatic cysts? the incremental diag-nostic yield of EUS over CT/MRI for prediction of cystic neoplasms. Pancreas 2013;42:717–21.
39. de Jong K, Verlaan T, Dijkgraaf MG, et al. Interobserver agreement for endosonography in the diagnosis of pancreatic cysts. Endoscopy 2011;43:579–84.
40. Harinck F, Konings ICAW, Kluijt I, Poley JW, van Hooft JE, van Dullemen HM, et al. A multicentre comparative prospec-tive blinded analysis of EUS and MRI for screening of pancre-atic cancer in high-risk individuals. Gut 2015 May 18.
41. Thosani N, Thosani S, Qiao W, et al. Role of EUS-FNA based cytology in diagnosis of mucinous pancreatic cystic lesions: a systematic review and meta-analysis. Dig Dis Sci 2010;55:2756–66.
42. Hong S-KS, Loren DE, Rogart JN, et al. Targeted cyst wall puncture and aspiration during EUS-FNA increases the diag-nostic yield of premalignant and malignant pancreatic cysts. Gastrointest Endosc 2012;75:775–82.
43. Thornton G, McPhail M, Nayagam S, et al. Endoscopic ultrasound guided fine needle aspiration for the diagnosis of pancreatic cystic neoplasms: a meta-analysis. Pancreatology 2013;13:48–57.
44. Khalid A, Zahid M, Finkelstein SD, et al. Pancreatic cyst fluid DNA analysis in evaluating pancreatic cysts: a report of the PANDA study. Gastrointest Endosc 2009;May;69:1095–102.
45. Wu J, Matthaei H, Maitra A, et al. Recurrent GNAS muta-tions define an unexpected pathway for pancreatic cyst devel-opment. Sci Transl Med 2011;3:92ra66.
46. Springer S, Wang Y, Molin MD, et al. A Combination of mo-lecular markers and clinical features improve the classification of pancreatic cysts. Gastroenterology 2015 Aug 4.
47. Ryu JK, Matthaei H, dal Molin M, et al. Elevated microRNA miR-21 Levels in Pancreatic cyst fluid are predictive of muci-nous precursor lesions of ductal adenocarcinoma. Pancreatol-ogy 2011;11:343–50.
48. Matthaei H, Wylie D, Lloyd MB, et al. miRNA Biomarkers in cyst fluid augment the diagnosis and management of pancre-atic cysts. Clin Cancer Res 2012;18 :4713–24.
49. Zikos T, Pham K, Bowen R, et al. Cyst fluid glucose is rapidly feasible and accurate in diagnosing mucinous pancreatic cysts. Am J Gastroenterol 2015;110:909–14.
50. Corcos O, Couvelard A, Dargère D, et al. Proteomic as-sessment of markers for malignancy in the mucus of intra-ductal papillary mucinous neoplasms of the pancreas. Pancreas 2012;41:169–74.
51. Thiruvengadam N, Park W. Systematic review of pancreatic cyst fluid biomarkers: the path forward. Clin Transl Gastroen-terol 2015;11:e88.
52. Plichta JK, Brosius JA, Pappas SG, et al. The changing spec-trum of surgically treated cystic neoplasms of the pancreas. HPB Surg 2015;2015:791704.
53. Valsangkar NP, Morales-Oyarvide V, Thayer SP, et al. 851 resected cystic tumors of the pancreas: A 33-year experience at the Massachusetts General Hospital. Surgery 2012;152: S4–12.
54. DeWitt J, McGreevy K, Schmidt CM, Brugge WR. EUS-guided ethanol versus saline solution lavage for pancreatic cysts: a randomized, double-blind study. Gastrointest Endosc 2009;70:710–23.
55. Oh H-C, Seo DW, Song TJ, et al. Endoscopic ultrasonography-guided ethanol lavage with paclitaxel injection treats patients with pancreatic cysts. Gastroenterology 2011;140:172–9.
56. Gavini H, Lee JH. Endoscopic ultrasound-guided endothera-py. J Clin Gastroenterol 2015;49:185–93.
57. Grutzmann R, Niedergethmann M, Pilarsky C, et al. Intra-ductal papillary mucinous tumors of the pancreas: biology, diagnosis, and treatment. Ooncologist 2010;15:1294–309.
58. Ingkakul T, Warshaw AL, Fernández-Del Castillo C. Epidemi-ology of intraductal papillary mucinous neoplasms of the pan-creas: sex differences between 3 geographic regions. Pancreas 2011;40:779–80.
59. Brugge WR, Lauwers GY, Sahani D, et al. Cystic neoplasms of the pancreas. N Engl J Med 2004;351:1218–26.
60. Capurso G, Boccia S, Salvia R, et al. Risk factors for intra-ductal papillary mucinous neoplasm (IPMN) of the pan-creas: a multicentre case-control study. Am J Gastroenterol 2013n;108:1003–9.
61. Lubezky N, Ben-Haim M, Nakache R, et al. Clinical presen-tation can predict disease course in patients with intraductal papillary mucinous neoplasm of the pancreas. World J Surg 2010;34:126–32.
62. Kobari M, Egawa S, Shibuya K, et al. Intraductal papillary mucinous tumors of the pancreas comprise 2 clinical subtypes: differences in clinical characteristics and surgical management. Arch Surg Chic Ill 1960. 1999;134:1131–6.
63. Serikawa M, Sasaki T, Fujimoto Y, et al. Management of intraductal papillary-mucinous neoplasm of the pancreas: treatment strategy based on morphologic classification. J Clin Gastroenterol 2006;40:856–62.
64. Sawai Y, Yamao K, Bhatia V, et al. Development of pancreatic cancers during long-term follow-up of side-branch intraductal papillary mucinous neoplasms. Endoscopy 2010;42:1077–84.
65. Poultsides GA, Reddy S, Cameron JL, et al. Histopathologic basis for the favorable survival after resection of intraductal papillary mucinous neoplasm-associated invasive adenocarci-
Case-based review
576 JCOM December 2015 Vol. 22, No. 12 www.jcomjournal.com
Pancreatic cystic Lesions
noma of the pancreas. Ann Surg 201 Mar;251:470–6. 66. Worni M, Akushevich I, Gloor B, et al. Adjuvant radiotherapy
in the treatment of invasive intraductal papillary mucinous neoplasm of the pancreas: an analysis of the surveillance, epidemiology, and end results registry. Ann Surg Oncol 2012;19:1316–23.
67. Goh BKP, Tan Y-M, Chung Y-FA, et al. A review of muci-nous cystic neoplasms of the pancreas defined by ovarian-type stroma: clinicopathological features of 344 patients. World J Surg 2006;30:2236–45.
68. Crippa S, Salvia R, Warshaw AL, et al. Mucinous cystic neo-plasm of the pancreas is not an aggressive entity: lessons from 163 resected patients. Ann Surg 2008;247:571–9.
69. Curry CA, Eng J, Horton KM, et al. CT of primary cystic pancreatic neoplasms: can CT be used for patient triage and treatment? AJR Am J Roentgenol 2000;175:99–103.
70. Park JW, Jang J-Y, Kang MJ, et al. Mucinous cystic neoplasm of the pancreas: Is surgical resection recommended for all surgically fit patients? Pancreatology 2014;14:131–6.
71. Sakorafas GH, Smyrniotis V, Reid-Lombardo KM, Sarr MG. Primary pancreatic cystic neoplasms revisited: Part II. Muci-nous cystic neoplasms. Surg Oncol 2011;20:e93–101.
72. Sarr MG, Carpenter HA, Prabhakar LP, et al. Clinical and pathologic correlation of 84 mucinous cystic neoplasms of
the pancreas: can one reliably differentiate benign from ma-lignant (or premalignant) neoplasms? Ann Surg 2000;231: 205–12.
73. Reid MD, Choi H, Balci S, et al. Serous cystic neoplasms of the pancreas: Clinicopathologic and molecular characteristics. Pancreat Neoplasms 2014;31:475–83.
74. Charlesworth M, Verbeke CS, Falk GA, et al. Pancreatic le-sions in von Hippel-Lindau disease? A systematic review and meta-synthesis of the literature. J Gastrointest Surg Off J Soc Surg Aliment Tract 2012;16:1422–8.
75. Kimura W, Moriya T, Hirai I, et al. Multicenter study of se-rous cystic neoplasm of the Japan pancreas society. Pancreas 2012;41):380–7.
76. Sarr MG, Murr M, Smyrk TC, et al. Primary cystic neoplasms of the pancreas. Neoplastic disorders of emerging importance-current state-of-the-art and unanswered questions. J Gastroin-test Surg Off J Soc Surg Aliment Tract 2003;7:417–28.
77. Yip-Schneider MT, Wu H, Dumas RP, et al. Vascular endo-thelial growth factor, a novel and highly accurate pancreatic fluid biomarker for serous pancreatic cysts. J Am Coll Surg 2014;218:608–17.
78. Del Chiaro M, Verbeke C, Salvia R, et al. European experts consensus statement on cystic tumours of the pancreas. Dig Liver Dis 2013;45:703–11.
Copyright 2015 by Turner White Communications Inc., Wayne, PA. All rights reserved.





























