Embed Size (px)
Citation preview

Seminars in Surgical Oncology 10:242-248 (1994)
Etiology, Biology, and Epidemiology of Ovarian Cancer
TRUDY R. BAKER, MD, AND M. STEVEN PIVER, MD
From the Roswell Park Cancer Institute, Department of Gynecologic Oncology, Buffalo, New York
~~
Epithelial ovarian cancer kills more women per year than all other gynecologic cancers combined. Pregnancy, oral contraceptive use, and tuba1 ligation decrease the risk of the disease, whereas risk is increased for women whose family history is consistent with one of the familial ovarian cancer syndromes. Several theories have been postulated con- cerning the etiology of ovarian cancer, including the incessant ovula- tion theory and that based on the model of hypergonadotropic hypo- gonadism. Chromosomal abnormalities and allele losses have been described in ovarian cancers. Involvement of oncogenes and tumor suppressor genes has been investigated as well. Genetic linkage studies are ongoing in families whose history is consistent with one of the familial ovarian cancer syndromes. @ 1994 WiIey-Liss. Inc.
KEY WORDS: epithelial ovarian cancer, epidemiology, etiology, genetics, family studies
INTRODUCTION Ovarian cancer is the second most common malig-
nancy of the female genital tract; however, it kills more women per year than cancers of all other genital sites combined. Of the estimated 22,000 new cases occurring in the United States in 1993, 13.300 women are expected to die from their disease [I] . Age-specific incidence rates increase from 2 to 3/100,000 in the third decade to 59/ 100,000 in the eighth decade, level- ing off at that point [2]. It is estimated that 1 in every 70 females born in the United States will develop this disease at some point in their life [3].
Ovarian cancer is most frequently seen in Northern and Western Europe and in North America (Fig. 1). The highest annual incidence rates of 141 100,000 occur in the Scandinavian countries, while slightly lower rates of 12/100,000 are found in the United States [4]. The lowest incidence rates are observed in developing countries, as well as in India and China (2-51 100,000). Because ovarian cancer is found more frequently in industrialized nations, environmental factors, diet, and reproductive events have all been implicated as possible etiologic factors. The one excep- tion to this trend is highly industrialized Japan, which has a low annual incidence rate of 3/100,000. Inci- dence rates are noted to rise among those Japanese
women who migrate to the United States [ 5 ] , lending strength to the suggestion that environmental factors influence the development of this disease.
ENVIRONMENTAL FACTORS Asbestos and talc are the two main chemicals im-
plicated in the development of ovarian cancer. Not only is talc chemically similar to asbestos, but both substances are found together in their natural states. It is postulated that asbestos-contaminated talcum powder used in the genital area could migrate up the genital tract to reach the ovaries, where it would act as a carcinogen. That carbon particles deposited in the vagina prior to hysterectomy have been retrieved in fallopian tubes [6] and that talc particles have been found embedded in both normal and malignant ovaries [7] lend support to this theory. Indeed, Cramer et al. [8] noted a relative risk of 1.9 (P < 0.003) for developing ovarian cancer associated with perineal talc exposure, and more recently Rosenblatt et al. [9] reported a relative risk of 4.8 (95% CI = 1.3-17.8) for talc use on sanitary napkins. Whittemore et al. [lo], however, failed to show a
Address reprint requests to Trudy R. Baker. M.D.. Roswell Park Cancer Institute. Department of Gynecologic Oncology, Elm and Carlton Streets, Buffalo, NY 14263.
0 1994 Wiley-Liss, Inc.

Etiology, Biology, and Epidemiology 243
Swadan
0 ! - - . -- -. . I
Israel, Born Europe, America I I
Norway I I
USA, Bay Area, White 1 I
USA. Alameda. White I I USA. El Paso. Spanish I I
New Zealand, Maori I I Israel, All Jews I 1
Germany, Democratic Republic I I Canada. Newfoundland UK. Oxford Canada, Manitoba New Zeland, Non-Maori Germany. FRG, Hamburg Poland, Warsaw City UK, Birmingham Canada, Saskatchewan Switzerland, Geneva USA. New Mexico, Spanish USA, Detroit, Black UK, Liverpool Yugoslav, Slovenia Canada, Alberta USA, Alameda, Black Canada, Quebec USA, Utah Hungary, Vas Israel, Born Israel USA, Bay Area, Black Malta Bulawyao, African Colombia, Cali Finland USA, New Mexico, Indian USA, Bay Area, Chinese Poland, Warsaw Rural Brazil, Sao Paulo Israel, Born Afr. Asia USA. Puerto Rico Hungary, Szabolcs India, Bombay Spain, Zaragoza Israel, Non-Jews Japan, Osaka Japan, Miyagi
U
0 L 5
Fig. 1. Age-adjusted worldwide annual ovarian cancer incidence per 100,000 women. (Data from Waterhouse et al. (1976) [37], with permission of Lyon International Agency for Research on Cancer.)
strong association between genital talc exposure and ovarian cancer (RR1.4, P = 0.06). Further study is needed before the precise role of talc as an etiologic agent in ovarian cancer is known.
DIETARY FACTORS One of the most pronounced differences between
the diets of industrialized and nonindustrialized coun- tries is the higher intake of animal fat by the former. Case-control studies have demonstrated significant di- rect associations between ovarian cancer and fat in- take [11,12]. Shu et al. [12] noted that the effect of fat
intake persisted even after adjustment for total calo- ries.
Mettlin and Piver [ 131 have evaluated another source of dietary fat and its association with ovarian cancer. Their case-control study demonstrated a rela- tive risk of 3.1 for developing ovarian cancer for those women who drank more than one glass of whole milk each day, compared to those who never drank whole milk. Women who drank skim or 2% milk were not found to be at increased risk, suggesting that the fat content of milk may be responsible for the increased risk. Cramer et al., [14] however, postulated that the
244 Baker and Piver
component of milk that was the likely etiologic factor was galactose, derived from the milk carbohydrate, lactose. In that case-control study, regular use of yo- gurt and cottage cheese resulted in an increased rela- tive risk of ovarian cancer (1.7, P=O.O1 and 1.4, P = 0.08, respectively). Women with high lactose con- sumption and low concentrations of the enzyme galac- tose-1-phosphate-uridyl transferase, which converts galactose to glucose, had a relative risk of 2.2 (P = 0.03) for ovarian cancer. Cramer and co-workers postulated that not only is lactose intake a dietary factor in the development of ovarian cancer, but that low transferase activity could represent a genetic risk factor for the disease.
REPRODUCTIVE AND ENDOCRINE FACTORS Most epidemiologic studies indicate that the risk of
developing ovarian cancer is decreased by pregnancy or by oral contraceptive use [15]. Wu et al. [16] noted a protective effect of pregnancy of 40% for women who had had two children, while Kvale et al. [I71 noted a decrease in risk of 50% for those women hav- ing five or more children. A study from the Centers for Disease Control (CDC) on oral contraceptive use and ovarian cancer revealed a relative risk reduction to 0.6 (40% decrease in incidence) for women 20-54 years of age who had used oral contraceptives and indicated that the risk decreased the longer the pill was used [ 181.
Tuba1 ligation has also been associated with a re- duced risk of ovarian cancer. In a recent prospective cohort study, an age-adjusted relative risk of 0.29 (95% CI, 0.15-0.55) was noted among women who had undergone that procedure [ 191. This reduction in risk persisted even after adjustment for other ovarian cancer risk factors. Hankinson et al. [19] also noted an inverse association between hysterectomy and ovarian cancer (RR 0.67; 95% CI, 0.45- 1 .OO), although not as substantial a risk reduction as that noted for tuba1 ligation [ 191.
Long periods of unprotected intercourse without pregnancy have been associated with an increased risk of ovarian cancer. Whittemore et al. [20] found that women having 2 10 years of unprotected intercourse had a risk of 1.8 relative to women with < 2 years of the same. The increase in risk associated with many years of unprotected intercourse applied regardless of previous oral contraceptive use or parity. Whittemore and colleagues suggested that ovarian cancer may be caused by a physiological disorder that affects ovula- tion and results in an inability to conceive.
More recently, a report by the Collaborative Ova- rian Cancer Group noted an increased risk of ovarian cancer (odds ratio 2.8; 95% CI, 1.3-6.1) for women who had used fertility drugs, compared to women with
no history of infertility [I 51. However, these results were based on a small number of patients, and infor- mation on specific fertility drugs used was not com- plete.
HEREDITARY FACTORS While most cases of ovarian cancer are considered
sporadic events, approximately 5-10% of cases fall into a pattern of familial occurrence [21]. Pedigree analysis of these family members suggests an autoso- ma1 dominant mode of inheritance with incomplete penetrance and variable expression. Three types of familial cancer syndromes involving ovarian cancer have been described [22]. Site-specific ovarian carci- noma syndrome involves a risk of developing ovarian cancer. Ovarian-breast carcinoma syndrome, the most common of the three, describes families in which both breast and ovarian cancers are identified. Finally, the cancer family syndrome is characterized by a predominance of cancer in the proximal colon plus the frequent occurrence of other primary adenocar- cinomas including breast, ovarian, and endometrial. However, recent reports found no support for the the- ory that the cancer family syndrome is a nonrandom occurrence, as no significant increase in clustering of colon, breast, uterine, and ovarian cancers was noted [2 3,241.
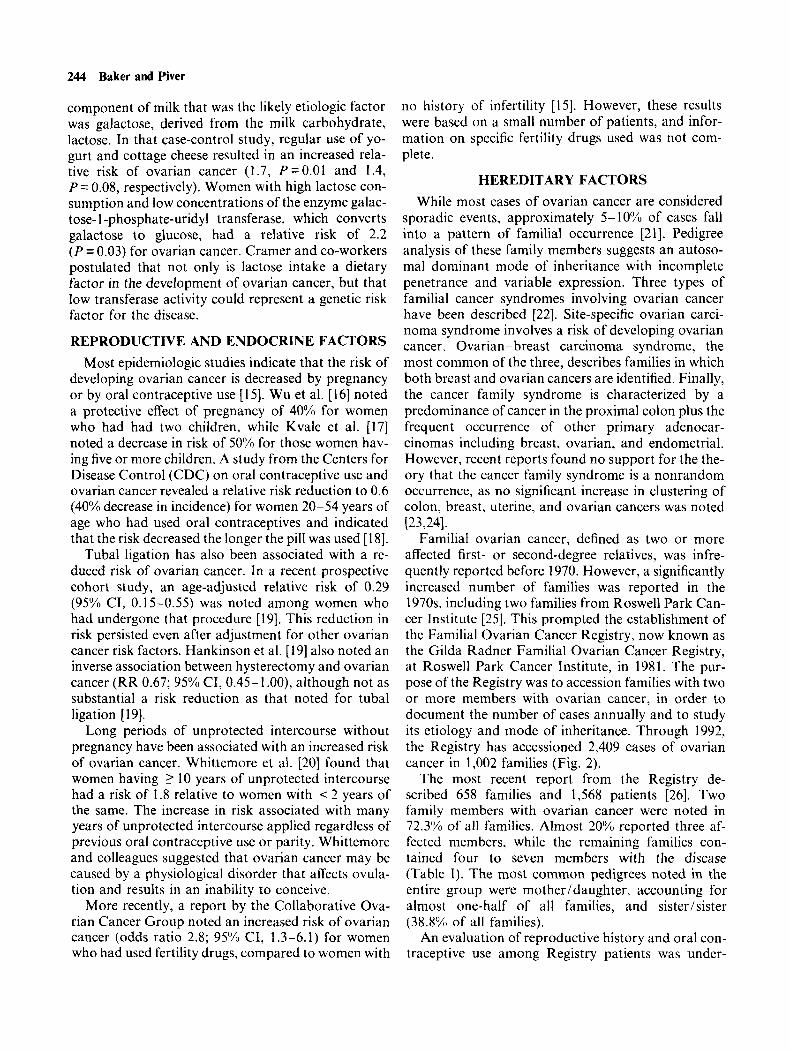
Familial ovarian cancer, defined as two or more affected first- or second-degree relatives, was infre- quently reported before 1970. However, a significantly increased number of families was reported in the 1970s, including two families from Roswell Park Can- cer Institute [25]. This prompted the establishment of the Familial Ovarian Cancer Registry, now known as the Gilda Radner Familial Ovarian Cancer Registry, at Roswell Park Cancer Institute, in 1981. The pur- pose of the Registry was to accession families with two or more members with ovarian cancer, in order to document the number of cases annually and to study its etiology and mode of inheritance. Through 1992, the Registry has accessioned 2,409 cases of ovarian cancer in 1,002 families (Fig. 2).
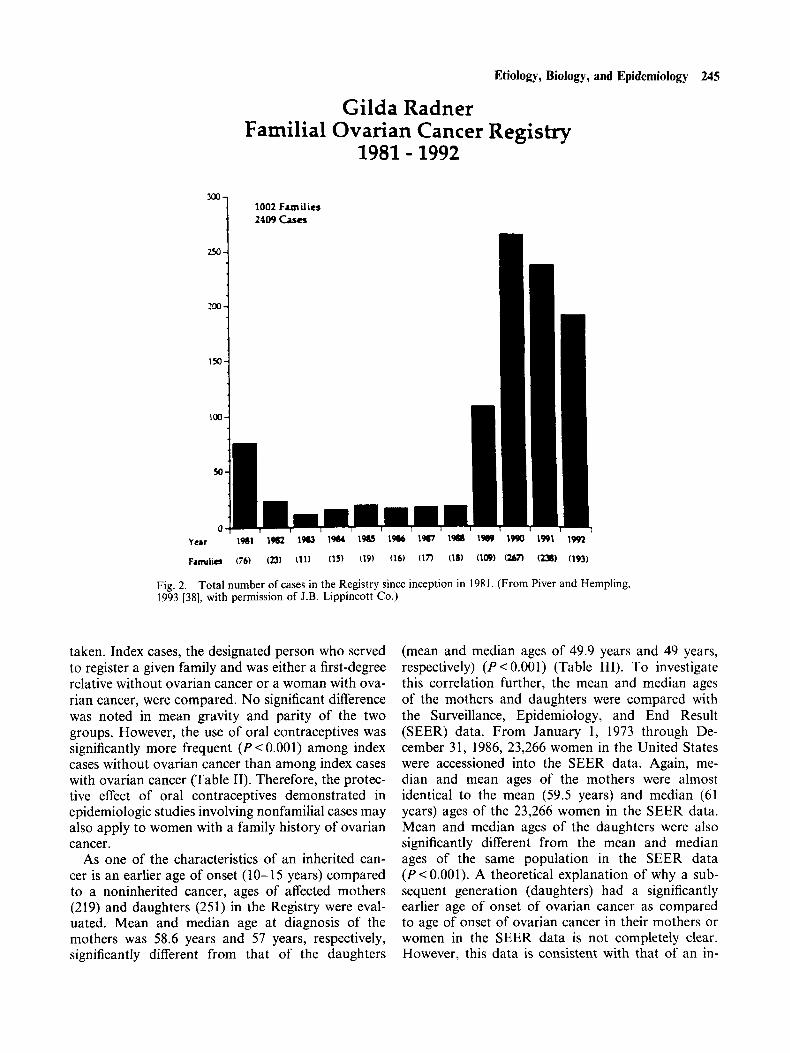
The most recent report from the Registry de- scribed 658 families and 1,568 patients [26]. Two family members with ovarian cancer were noted in 72.3% of all families. Almost 20% reported three af- fected members, while the remaining families con- tained four to seven members with the disease (Table I). The most common pedigrees noted in the entire group were motherldaughter, accounting for almost one-half of all families, and sister/sister (38.8% of all families).
An evaluation of reproductive history and oral con- traceptive use among Registry patients was under-
Etiology, Biology, and Epidemiology 245
Gilda Radner Familial Ovarian Cancer Registry
1981 - 1992
1002 Families 2409 Cases
year 1%1 19@2 1w 1964 1w 1% 1987 19M 1w 1990 1991 1992
Famlm (76) (23) (11) (15) (19) (16) (1I) (18) (10s) (m (-1 (193)
Fig. 2 . 1993 [38], with permission of J.B. Lippincott Co.)
Total number of cases in the Registry since inception in 1981. (From Piver and Hempling.
taken. Index cases, the designated person who served to register a given family and was either a first-degree relative without ovarian cancer or a woman with ova- rian cancer, were compared. No significant difference was noted in mean gravity and parity of the two groups. However, the use of oral contraceptives was significantly more frequent ( P < 0.001) among index cases without ovarian cancer than among index cases with ovarian cancer (Table 11). Therefore, the protec- tive effect of oral contraceptives demonstrated in epidemiologic studies involving nonfamilial cases may also apply to women with a family history of ovarian cancer.
As one of the characteristics of an inherited can- cer is an earlier age of onset (10-15 years) compared to a noninherited cancer, ages of affected mothers (219) and daughters (251) in the Registry were eval- uated. Mean and median age at diagnosis of the mothers was 58.6 years and 57 years, respectively, significantly different from that of the daughters
(mean and median ages of 49.9 years and 49 years, respectively) (P < 0.001) (Table 111). To investigate this correlation further, the mean and median ages of the mothers and daughters were compared with the Surveillance, Epidemiology, and End Result (SEER) data. From January 1, 1973 through De- cember 31, 1986, 23,266 women in the United States were accessioned into the SEER data. Again, me- dian and mean ages of the mothers were almost identical to the mean (59.5 years) and median (61 years) ages of the 23,266 women in the SEER data. Mean and median ages of the daughters were also significantly different from the mean and median ages of the same population in the SEER data (P < 0.001). A theoretical explanation of why a sub- sequent generation (daughters) had a significantly earlier age of onset of ovarian cancer as compared to age of onset of ovarian cancer in their mothers or women in the SEER data is not completely clear. However, this data is consistent with that of an in-
246 Baker and Piver
TABLE I. The Gilda Radner Familial Ovarian Cancer Registrv*
No. of cases in one family
2 3 4 5 6 7 Total:
Frequency
476 129 40 10
I 658
7 - -
No. of cases % of total
families
952 387 160 50 19 7
1.568 -
72.3 19.6 6. I 1.5 0.3 0.2
100.0 -
*Number of relatives diagnosed with ovarian cancer within indi- vidual families. From Piver et al. (1993) [26], with permission of J.B. Lippincott Co.
TABLE 11. The Gilda Radner Familial Ovarian Cancer Registry Use of Oral Contraceotion
Index cases Index cases with without
ovarian ovarian cancer cancer P -value
I06 I42 < 0.00 1 Yes 49 (46.2%)) 104 (73.1%) No 57 (53.7"YU) 38 (26.7'Yu)
Adapted from Piver et al. (1993) [26]. with permission of J.B. Lippincott Co.
TABLE 111. The Gilda Radner Familial Ovarian Cancer Registry Analysis of the Difference Between Mean and Median Ages for Mothers and Daughters With Ovarian Cancer in the Gilda Radner Familial Ovarian Cancer Reeistrv
Relationship to be analyzed
Mothers 58.566 57 Daughters 49.865 49 P P < 0.001 P < 0.001
Medianb ~- .~ Meana
______~_.
"Analysis of the difference between the means was done with two- tailed t-tests. bAnalysis of the difference between the medians was done with Z-tests. Adapted from Piver et al. (1993) [76], with permission of J.B. Lippincott Co.
herited cancer which is seen at an earlier age of onset compared to its noninherited counterpart.
The pattern of inheritance among Registry patients is consistent with an autosomal dominant transmis- sion with variable penetrance. Therefore, sisters and daughters in families with two or more first-degree relatives affected could have as high as a 50% chance of developing the disease. Risk of developing ovarian cancer with one first- and one second-degree or two or more second-degree relatives is likely less than 50%. but still higher than that of women without a family history of the disease ( 1.4%1, or 1 in 70).
ETIOLOGY Several theories have been proposed to explain the
cause of ovarian cancer. Fathalla [27] in 1971 postu- lated that the greater the number of ovulations during a woman's lifetime, the greater the chance of develop- ing ovarian cancer. This incessant ovulation theory suggested that the epithelial ovarian surface suffers repeated trauma with each ovulatory event, predispo- sing it to malignant changes. A modification of Fa- thalla's theory [27] has been suggested that proposes that disorders of ovulation, resulting in impaired abil- ity to conceive, play a role in the development of ova- rian cancer [20]. It is proposed that such disorders of ovulation could result in the development of epithelial inclusion cysts, which may play a role in the process of malignant transformation [28]. Another abnormality of ovulation known as luteinized unruptured follicle syndrome [20], which results in elevated midcycle folli- cle-stimulating hormone (FSH) levels compared to that of normal ovulatory cycles along with high local concentrations of estradiol, progesterone, andros- tenedione, and luteinizing hormone (LH) in the un- ruptured follicle, could also play a role in the develop- ment of neoplasia according to this theory. These hypotheses are supported by epidemiologic data sug- gesting a decreased risk of the development of ovarian cancer related to oral contraceptive use or pregnancy, both of which suppress ovulation. Conversely, ova- rian hyperstimulation and promotion of ovulation, as seen with the use of fertility drugs, reported to increase the risk of ovarian cancer, is also consistent with the incessant ovulation theory.
A second theory proposes that ovarian cancer is induced through the mechanism of hypergonado- tropic hypogonadism [29]. This state is characterized by elevated levels of gonadotropins, which exist sec- ondary to loss of negative feedback on the pituitary. Ovarian failure induced by any means, including drugs, infection, or environmental toxins, could theoretically result in a hypergonadotropic state, plac- ing one at risk of ovarian cancer. The protective effects seen with oral contraceptive use and pregnancy, both of which are associated with decreased gonadotropin levels, are consistent with this model. Furthermore, a hypergonadotropic state exists in menopausal women, who exhibit the highest rates of ovarian cancer. The finding of an increased risk of ovarian cancer with the use of fertility drugs is also compatible with the model, as fertility drugs either contain various gonadotropins or increase their production.
BIOLOGY Malignant transformation develops from a series of
genetic alterations that lead to abnortnal growth and

Etiology, Biology, and Epidemiology 247
differentiation [30]. Cytogenetic studies of ovarian cancers have shown various chromosomal abnormali- ties involving chromosome 1, 3, 6, 7, and 11 [31]. Allele losses involving 3p, 6q, 1 Ip, 17p, and 17q have been observed as well [32].
In general, genetic changes in one of two categories of normal cellular genes can occur, leading to malig- nant transformation. If activated, proto-oncogenes, which normally encode proteins involved in growth regulatory pathways, can produce an altered or over- expressed gene product that can facilitate malignant change. Activation can occur by mutation, deletion, amplification, or translocation. Expression of several proto-oncogenes, including Ki-ras, H-ras, c-myc, fms, and HER-2-neu, has been noted in epithelial ovarian cancers [33]. The significance of the activation of these proto-oncogenes’ and their role in the development of ovarian cancer is unclear. However, it has been noted that overexpression of HER-2-neu is found in 30% of ovarian cancers and has been associated with a poor prognosis [34]. The second category of normal cellular genes that can undergo genetic alteration to induce malignancy is tumor suppressor genes. As these genes normally inhibit growth, activation or loss of both alleles of the gene is necessary to lead to the develop- ment of cancer. The most completely studied of these genes is p53, reportedly overexpressed or mutated in approximately 50% of advanced epithelial ovarian cases [35]. Mutation of p53 in ovarian cancer has not been associated with a poor prognosis [35].
While it is likely that the genetic alterations that lead to the development of ovarian cancer are more complex than the occurrence of a single genetic muta- tion, it is noteworthy that for at least a subset of ovarian cancer patients, the genetic puzzle is becoming more clear. A recent genetic linkage study involving hereditary breast-ovarian cancer families found link- age to the genetic marker D17S74 on chromosome 17q in three out of five families studied [36]. Narod et al. [36] suggest that the chromosomal region previously determined to contain a gene (BRCA-I) for early- onset breast cancer may also be associated with some hereditary ovarian cancer cases. Our laboratory in col- laboration with B.J. Ponder of the University of Cam- bridge, United Kingdom, has localized the breast/ ovarian susceptibility gene (BRCA-1) on 17q12-21 to an interval of 5 1 cM (S. Smith, personal communica- tion). Elucidation of the exact genetic region and clon- ing of the gene involved awaits further study.
REFERENCES I . Boring CC. Squires TS, Tong T: Cancer Statistics. 1993. Ca
2. Frey CM: Ovary. In Miller BA, Gloeckler Ries LA, Hankey Cancer J Clinicians 427-26, 1993.
BF, Kosary CL. Edwards BK (eds): “Cancer Statistics Review 1973-1989.” Vol. XX. Bethesda: National Cancer Institute. 1992. 1-7.
3. Cutler SJ, Young JL: Third National Cancer Survey: Incidence data, National Cncer Institute Monograph no. 41. DHEW Publication (NIH) 75-787. Washington, DC: US Government Printing Office, 1975.
4. Tomatis L: Cancer: Causes, Occurrence and Control. Oxford, UK: International Agency for Research on Cancer, 1990.
5 . Dunn JE: Cancer epidemiology in populations of the United States with emphasis on Hawaii and California and Japan. Cancer Res 35:3240-3245. 1975.
6. Egli GE, Newton M: The transport of carbon particles in the human female reproductive tract. Fertil Steril 12: 15 I - 155, 1961.
7. Henderson WJ, Hamilton TC, Griffiths K: Talc in normal and malignant ovarian tissue. Lancet 1:499, 1979.
8. Cramer DW, Welch, WR, Scully RE, Wojciechowski CA: Ovarian cancer and talc. A case-control study. Cancer 50: 372-376. 1982.
9. Rosenblatt KA, Szklo M, Rosenshein NB: Mineral fiber expo- sure and the development of ovarian cancer. Gynecol Oncol 45:20-25, 1992.
10. Whittemore AS, Wu ML, Paffenbarger RS Jr, et al: Personal and environmental characteristics related to epithelial ovarian cancer. Am J Epidemiol 128:1228-1240, 1988.
11. Cramer DW. Welch WR, Hutchinson GB. et al: Dietary ani- mal fat in relation to ovarian cancer risk. Obstet Gynecol
12. Shu XO, Gao TG, Yuan JM, et al: Dietary factors and epi- thelial ovarian cancer. Br J Cancer 59:92-96, 1989.
13. Mettlin C, Piver MS: A case-control study of milk drinking and ovarian cancer risk. Am J Epidemiol 132:871-876. 1990.
14. Cramer DW, Willett WC, Bell DA, et al: Galactose consump- tion and metabolism in relation to the risk of ovarian cancer. Lancet 2:66-71, 1989.
15. Whittemore AS, Harris R, Intyre J, and the Collaborative Ovarian Cancer Group: Characteristics relating to ovarian cancer risk: Collaborative analysis of I2 US case-control stud- ies. 11. Invasive epithelial ovarian cancers in white women. Am J Epidemiol 136: I 184- 1203, 1992.
16. Wu ML, Whittemore AS, Paffenbarger RS Jr. et al: Personal and environmental characteristics related to epithelial ovarian cancer. I. Reproductive and menstrual events and oral contra- ceptive use. Am J Epidemiol 128:1216-1227. 1988.
17. Kvale G, Heuch I, Nilssen S, Beral V: Reproductive factors and risk of ovarian cancer: A prospective study. Int J Cancer
18. Cancer and Steroid Hormone Study of the Centers for Disease Control and the National Institute of Child Health and Human Development: The reduction in risk of ovarian cancer associated with oral contraceptive use. N Engl J Med 316: 650-655, 1987.
19. Hankinson SE, Hunter DJ, Colditz GA, et al: Tuba1 ligation, hysterectomy, and risk of ovarian cancer: A prospective study. JAMA 270:28 13-28 18, 1993.
20. Whittemore AS, Wu ML, Paffenbarger RS Jr, el al: Epithelial ovarian cancer and the ability to conceive. Cancer Res 49: 4047-4052, 1989.
21. Lynch HT, Conway T, Lynch J: Hereditary ovarian cancer. In Sharp F, Mason WP, Leake RE (eds): “Ovarian Cancer: Bio- logical and Therapeutic Challenges.” London: Chapman & Hall, 1990, 7-19.
22. Lynch HT, Bewtra, Lynch JT: Familial ovarian carcinoma. Am J Med 81:1073-1076, 1986.
23. Nelson CL, Sellers TA, Rich SS, et al: Familial clustering of colon. breast, uterine, and ovarian cancers as assessed by fam- ily history. Genet Epidemiol 10:235-244. 1993.
24. Houlston RC, Bourve TH, Collins WP, et al: Risk of ovarian cancer and genetic relationship to other cancers in families. Hum Hered 43:111-115. 1993.
63:833-838, 1984.
42:246-251, 1988.

248 Baker and Piver
25. Piver MS, Barlow JJ, Sawyer DM: Familial ovarian cancer: Increasing in frequency? Obstet Gynecol 60:397-400, 1982.
26. Piver MS, Baker TR, Jishi MF, et al: Familial Ovarian Cancer. A report of 658 families from the Gilda Radner Familial Ova- rian Cancer Registry 1981-1991. Cancer 71:582-588.
27. Fathalla MF: Incessant ovulation-A factor in ovarian neo- plasia? Lancet 2:163. 1971.
28. Zajicek J: Ovarian cystomas and ovulation, a histogenetic con- cept. Tumori 63:429-435. 1977.
29. Cramer DW: Epidemiologic Aspects of Gynecologic Oncol- ogy. In Knapp RC Berkowitz RS (eds): “Gynecologic Oncol- ogy.” Vol. 8. 2nd Ed. McGraw-Hill, New York, 1993, 145- 150.
30. Weinberg RA: The genetic origins of human cancer. Cancer
31. Amos CI, Struewing JP: Genetic epidemiology of epithelial
32. DiCioccio RA, Piver MS: The genetics of ovarian cancer. Can-
61:1963-1968, 1988.
ovarian cancer. Cancer 71566-572, 1993.
cer Invest 10:135-141, 1992.
33. Bast RC Jr, Boyer CM, Jacobs I , et al: Cell growth regulation in epithelial ovarian cancer. Cancer 71:1597-601, 1993.
34. Berchuck A, Kame1 A, Whitaker R, et al: Overexpression of HER-2ineu is associated with poor survival in advanc- ed epithelial ovarian cancer. Cancer Res 50:4087-4091, 1990.
35. Marks JR, Davidoff AM, Kerns BJ, et al: Overexpression and mutation of p53 in epithelial ovarian cancer. Cancer Res 51:
36. Narod SA, Feunteun J, Lynch HT. et al: Familial breast- 2979-2984, 1991.
ovarian cancer locus on chromosome 17ql2-q23. Lancet 338: 82-83, 1991.
37. Waterhouse J, Muir C, Correa P, et al: “Cancer Incidence in Five Continents.” Vol. 2. No. 15. Lyon: Lyon International Agency for Research on Cancer, 1976.
38. Piver MS. Hempling RE: Etiology and Screening of ovarian cancer. In Thompson JD, Rock JA (eds): “Telinde’s Operative Gynecology Updates.” Vol. I, No. 9. Philadelphia: JB Lippin- cott, 1993, 1-13.