Embed Size (px)
Citation preview

1
EXCELLENCE EXPERTISE INNOVATION
EthicsinPediatrics
JeffreyR.Starke,MDDecember02,2016
Medical Consultant MeetingDecember 02, 2016San Antonio, TX
• Member of a data safety monitoring board for Otsuka Pharmaceuticals concerning pediatric trials of Delamanid.
JeffreyR.Starke,MD,hasthefollowingdisclosurestomake:

2
Childhood Tuberculosis in 2016 – Ethics and Reality
Jeffrey R. Starke, M.D.Professor of Pediatrics
Baylor College of Medicine
Disclosures
Dr. Starke is a member of a Data Safety Monitoring Board for Otsuka Pharmaceuticals concerning pediatric trials of delamanid. This will not be discussed during this talk.
Dr. Starke will not discuss off-label use of drugs or diagnostic tests during this talk.

3
Tuberculosis is a social disease with medical implications
THE GREAT PARADOX OF TUBERCULOSIS – A CAUTIONARY TALE
By the use of drugs and BCG vaccines, we can
cure tuberculosis disease prevent progression of tuberculosis infection
into disease prevent a significant proportion of life-
threatening childhood tuberculosis [by BCG vaccination]
Yet, tuberculosis is AGAIN the #1 infectious disease killer of humans, and our inability to control it is our biggest public health failure.
4
When I started in TB [1983]… 23,846 cases of TB in the U.S.
Tine and multipuncture skin tests predominated
Only solid media for mycobacterial culture
9-12 months of daily isoniazid was the only treatment for TB infection
Treatment for TB disease was 9-12 months of isoniazid and rifampin with streptomycin given IM for the first 2-3 months
Pyrazinamide was not used
Ethambutol discouraged in children [possible ocular toxicity]
The link between TB and HIV was unrecognized
WHO 2016 Global TB Report 10.4 million new cases: 5.9 million in men,
3.5 million in women, 1.0 million in children
This is an increase from 2014, accounted for mostly by new surveillance and survey data from India
Only 6.1 million cases were detected and notified, a gap of 4.3 million cases
The gap is caused by underreporting of TB cases in countries with large unregulated private sectors, and under-diagnosis in countries with major barriers to accessing care
5
The Basic Conundrum of Childhood Tuberculosis
There has been a circular argument concerning childhood tuberculosis. Some have said that without evidence of under-diagnosis of tuberculosis in children there is no justification for allotting additional resources for diagnosis, treatment and prevention. However, the resources to adequately determine the burden of childhood tuberculosis [the evidence] have not been made available.
Why Are Obtaining Accurate Measures of Childhood TB So Important?
Allocation of resources within an NTP
Allocation of resources along the health care spectrum: community workers and programs, clinics, hospitals
Awareness among pediatric providers
Recognition of the issue among child survival experts and planners – MDG 4 and 5
Approaching and interesting funders for both grants and programs
Attracting the attention of researchers
Protect the human rights of children and families

6
HOW IS TUBERCULOSIS DIAGNOSED?
Adults – Mycobacterial-based diagnosis positive sputum AFB smear - 60% - 75% positive sputum culture - 90% positive tuberculin skin test - 80% [HIV < 50%]
Children positive sputum or gastric AFB smear - < 10% positive Xpert – 10% - 20% positive sputum or gastric culture - 10% - 40% positive tuberculin skin test - 50% - 80%
DIAGNOSIS OF TUBERCULOSIS IN CHILDREN
Even in developed countries, the “gold standard” for the diagnosis of tuberculosis in children is the triad of:
1. a positive TST
2. an abnormal CXR and/or physical exam
3. a history of recent contact to an infectious adult case of TB

7
The Implication of Using Sputum Microscopy
The decision to rely on sputum microscopy for the diagnosis of tuberculosis in high burden countries ensured the exclusion of children from tuberculosis control.
This is what happens when vulnerable groups are not represented when policy decisions are made.
GLOBAL ESTIMATES OF CHILDHOOD TUBERCULOSIS
WHO, 2012: 460,000 annual cases, 64,000 deaths in non-HIV-infected children [no estimate for HIV-infected]
Only 36% of estimated cases are actually reported
Jenkins et al 2014: Modeling study estimate –999,792 cases
Dodd et al 2014, 2016: Modeling study estimates in 22 high burden countries: 650,977 cases; 7,591,759 children annually infected; 53,234,854 total infected children, 100 MILLION GLOBALLY
WHO, 2015: 1 million annual cases, 210,000 deaths

8
CASE NOTIFICATIONS OF CHILDHOOD TUBERCULOSIS IN SELECTED HIGH-BURDEN
COUNTRIES - 2011
Total New < 15 smear + < 15 smear - Per cent of
Country Cases N [%] N [%] Total Cases
Afghanistan 26,853 669 [28] 1,753 [72] 9.0
Brazil 71,337 692 [36] 1,243 [64] 2.7
China 865,059 1,378 [25] 4,165 [75] 0.6
India 1,211,441 12,985 [26] 36,673 [74] 4.1
Pakistan 255,094 3,895 [22] 14,142 [78] 7.1
South Africa 325,321 3,404 [10] 32,080 [90] 10.9
Viet Nam 98,462 95 ------- ?
Zimbabwe 36,960 326 [11] 2,635 [89] 8.0
Total 2,890,527 23,444 92,691 4.0
Jenkins, et al. Mortality among children diagnosed with tuberculosis: a systemic review and meta-analysis. Lancet
Infect Dis, in press.Reviewed the literature in the pre- and post-chemotherapy eras to estimate mortality rates
Pre-chemotherapy
Pooled case fatality rate was 21.9%
Rate was 43.6% in children under age 5 years versus 14.9% in older children
Post-chemotherapy
Pooled case fatality rate was 0.9%
Rate was 1.9% in children under age 5 years
Case fatality rate in HIV-infected children prior to widespread use of ARV was 14.3% compared with 3.4% when ARV was given

9
Table: Estimated Tuberculosis Morbidity and Mortality in Children 0‐14 years of age by WHO Region ‐
2015
Children 0‐14 years of age
Region Estimated morbidity
Estimated mortality
% Mortality [CFR]
% of deaths occurring in HIV‐infected children
% Child contacts < 5 years of age given preventive therapy [Est.]
Africa 287,000 97,500 34 35 5
The Americas 26,000 2,370 9 8 67
Eastern Mediterranean 75,000 10,810 14 3 12
Europe 25,000 568 2 8 42
South‐East Asia 406,000 90,000 22 7 2
Western Pacific 138,000 8,570 6 < 1 13
Total 957,000 209,818 22 ‐‐‐‐
Source: World Health Organization Global Tuberculosis Report 2016 CFR – case fatality ratio

10
ECONOMIC AND SOCIAL BURDEN OF TUBERCULOSIS FOR CHILDREN
Direct treatment costs Inpatient or institutional treatment Lost earnings of the family Redirecting resources from other
needs Withdrawal from school Stigmatization and discrimination Creation of orphans
Tuberculosis Orphans

11
Some Issues for Foreign Children and Families
Language barriers
Lack of transportation
Lack of health insurance – immigrants [not refugees]
Lack of access to a medical home
Understanding the difficult concept of TB infection
Minimal or no orientation to prevention
Medication distribution – pharmacies, refills
Distrust of government agencies
Stigma of tuberculosis
New TB Tests Are Not Applied to Children
(as of 2013)
Test # of publishedstudies in children
FNA 140
Fluorescent microscopy 1
LED-FM 0
MODS 7
Line-probe assays 1
LAMP 0
GeneXpert 3

12
TB Studies on Adults & Children - 2013Modality Adult
Studies*
Pedi Studies
*
∆ Ratio adult to pedi
Year of 1st
publication
Culture: Solid
400 38 ‐362 11x 1967
Culture: Liquid
248 13 ‐235 19x 1966
MODS 37 7 ‐30 5x 2000
PPD/TST 6399 2031 ‐4368 3x 1907
IGRA 344 87 ‐257 4x 1999
Xpert 7 1 ‐6 7x 2010
PCR, all 1831 187 ‐1644 10x 1990
*: PubMed Queries

13
A Fundamental Question
Much of the attention for HIV and malaria has focused on children, but this has not happened for tuberculosis:
Why not?

14
SOME REASONS WHY CHILDHOOD TUBERCULOSIS HAS BEEN NEGLECTED
Inadequate data Difficulty confirming the diagnosis Children are rarely contagious
[public health “dead end”] Perception from TB policy makers that treating
adults is enough Government programs fail to address children Lack of family centered contact tracing Perceived lack of scientific study and scrutiny Misplaced faith in the BCG vaccines Lack of industry support Inadequate advocacy by pediatricians
Some Special Problems for Childhood TB
Lack of accurate diagnostic tests
Lack of pediatric dosing forms of medications
Dispersible pediatric dosage forms developed using U.S. funding but will not be available in the U.S. as FDA approval not being sought
Prevention of childhood TB depends on well-functioning local health departments that can rapidly investigate the contacts of new cases
Federal funding cuts have made these investigations be delayed or not occur at all, which will lead to more childhood TB cases

15
Availability of Tuberculosis Medications to Children RCT data are very difficult to obtain for children due
to lack of funding and small case loads at single centers
Childhood TB experts generally accept that “if it works in adults, it will work in children”
However, children may need fewer drugs and shorter durations than adults
PK data are essential in several age groups
Bedaquiline: U.S. approval, no pK data for children [orphan status]
Delamanid: European approval, de-escalated age pK data being determined for children
TRANSITIONS IN TUBERCULOSIS
Cured
Treated
Diagnosed
Susceptible
Exposed
Infected
Diseased
Sick
Prevent Disease
Register, Record, Report
Prevent Infection
16
Childhood TB Control Strategies in the U.S.
Never used a BCG vaccine
Slow, steady decline [~5%/Yr] until the mid-1980s when it recurred with a vengeance
Strategy of universal periodic testing [TST] for TB infection began in the late 1950s [when INH became available] and continued until the 1990s
Universal testing replaced with screening for risk factors and testing for risk
Heavy use of INH treatment for TB exposure and LTBI
Specific recording and reporting of childhood TB cases – each case is a “sentinel event”
Why is treating tuberculosis infection an essential part of getting to zero?
TB infections are not “latent” but are “active”
Vulnerable patients progress rapidly to life-threatening forms of TB: young children, immunocompromised persons, elderly
In some cases, can treat TB infection before the person becomes immunocompromised
Prevention of future cases = less transmission in the future to vulnerable persons
BCG vaccine prevents many but not all cases of life-threatening TB in children and adults
Treating MDR-TB infection may be safer and more effective than treating MDR-TB disease
Contact investigation: the most “bang” for the “buck” – high risk, high rate, motivation to treat, drug susceptibilities known, DOT and DOPT
17
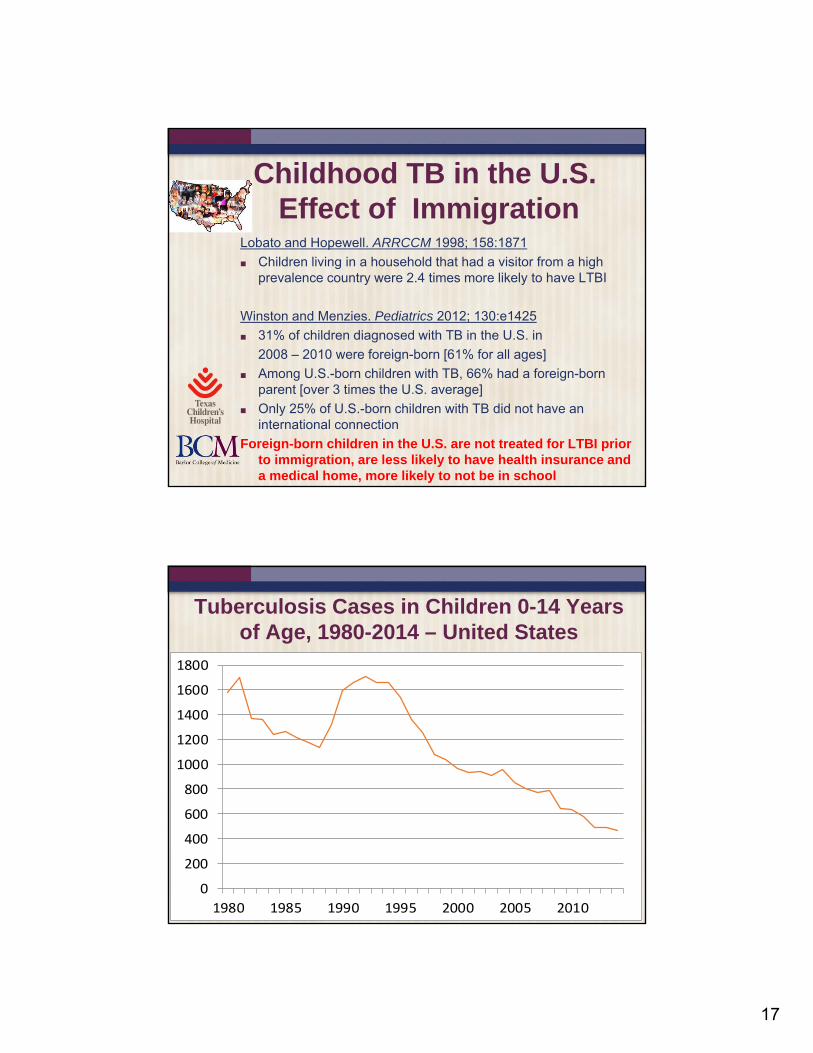
Childhood TB in the U.S.Effect of Immigration
Lobato and Hopewell. ARRCCM 1998; 158:1871
Children living in a household that had a visitor from a high prevalence country were 2.4 times more likely to have LTBI
Winston and Menzies. Pediatrics 2012; 130:e1425
31% of children diagnosed with TB in the U.S. in
2008 – 2010 were foreign-born [61% for all ages]
Among U.S.-born children with TB, 66% had a foreign-born parent [over 3 times the U.S. average]
Only 25% of U.S.-born children with TB did not have an international connection
Foreign-born children in the U.S. are not treated for LTBI prior to immigration, are less likely to have health insurance and a medical home, more likely to not be in school
Tuberculosis Cases in Children 0-14 Years of Age, 1980-2014 – United States
0
200
400
600
800
1000
1200
1400
1600
1800
1980 1985 1990 1995 2000 2005 2010
2014 - 460 cases

18
How Have We Lowered Childhood TB Rates in the U.S.?
Family-centered contact investigation
Use of the best available diagnostic modalities
Screening and treating high risk children and adolescents
Adequate funding of TB control programs
How Do We Find Children With Tuberculosis Disease?
1. Contact Investigation – Active Case-finding
50 % of cases in Houston
Milder disease, rarely need microbiologic confirmation
2. Ill Children – Passive Case-Finding
More severe disease, harder to treat
No source case, more difficult to diagnose
Broader differential diagnosis, esp. immunocompromise
3. Screening high risk children
Low yield, nonspecific findings in chest radiograph and physical examination because of other, more common, causes
19
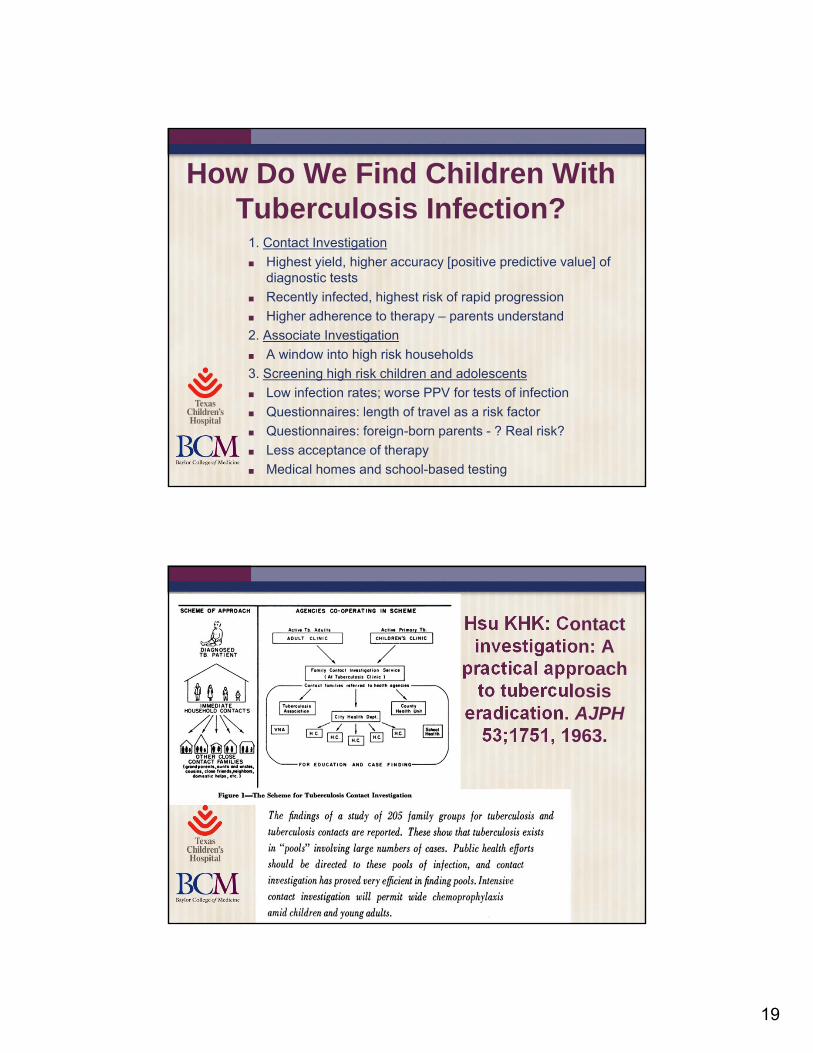
How Do We Find Children With Tuberculosis Infection?
1. Contact Investigation
Highest yield, higher accuracy [positive predictive value] of diagnostic tests
Recently infected, highest risk of rapid progression
Higher adherence to therapy – parents understand
2. Associate Investigation
A window into high risk households
3. Screening high risk children and adolescents
Low infection rates; worse PPV for tests of infection
Questionnaires: length of travel as a risk factor
Questionnaires: foreign-born parents - ? Real risk?
Less acceptance of therapy
Medical homes and school-based testing
Hsu KHK: Contact investigation: A
practical approach to tuberculosis
eradication. AJPH53;1751, 1963.
20
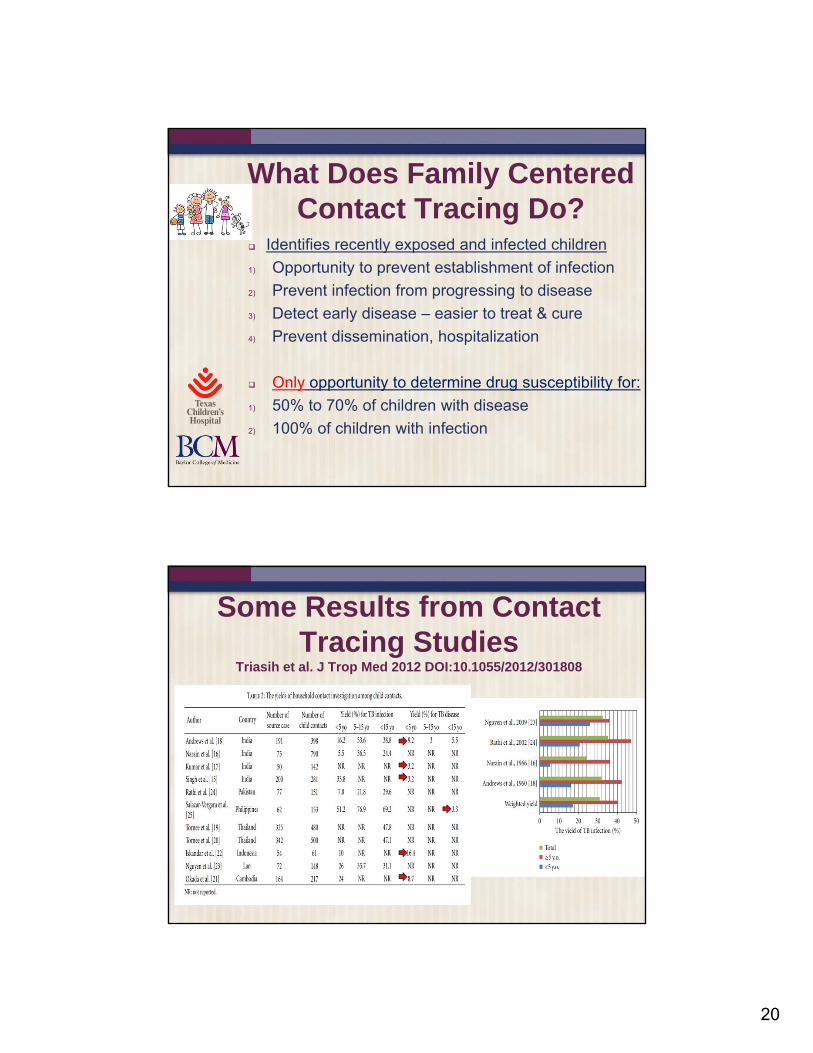
What Does Family Centered Contact Tracing Do?
Identifies recently exposed and infected children
1) Opportunity to prevent establishment of infection
2) Prevent infection from progressing to disease
3) Detect early disease – easier to treat & cure
4) Prevent dissemination, hospitalization
Only opportunity to determine drug susceptibility for:
1) 50% to 70% of children with disease
2) 100% of children with infection
Some Results from Contact Tracing Studies
Triasih et al. J Trop Med 2012 DOI:10.1055/2012/301808
21
ADVERSE EFFECTS IN CHILDREN OF NOT PERFORMING CONTACT TRACING
Missed cases
Misdiagnosis – tuberculosis not recognized
Diagnose cases later – increased morbidity and mortality
Missed drug resistance [need source case culture and drug susceptibility results]
Missed prevention – treating exposed or infected children
Graham and Triasih. More evidence to support screening of child contacts of
tuberculosis cases: If not now, then when? Clin Infect Dis 2013
“We already have the policy, the evidence and the tools we need to implement [contact tracing]; even the political will is beginning to emerge. It will not be easy, but this recent study [in Uganda] further highlights the consequences and missed opportunities of continued neglect.”

22

23
Educate 9-10th
graders at 2 public high schools in Houston, screen for risk factors, test those with risk factors via IGRAs
Provide short-course therapy with 12 weekly doses of INH/rifapentine (3HP) for IGRA+ children at school
Houston High School StudyLindsay Hatzenbuehler, Andrea Cruz, Jeffrey Starke
Piloted at a magnet high school for health sciences
Then rolled out at low-income school
Phlebotomy school students and TCH nurses volunteered for blood draws
Manufacturers of QuantiFERON (Qiagen) and T.SPOTTB (Oxford) donated test kits
Under programmatic conditions, only 1 IGRA would be used
Collaborator ran assays in his lab
TSTs not performed
Houston High School StudyLindsay Hatzenbuehler, Andrea Cruz, Jeffrey Starke

24
Variable IGRA positive(n = 16)
IGRAnegative(n = 399)
p-value
Student birth in a high-risk country 5 (31%) 106 (27%) 0.71
Student travel to a high-risk country in past year
7 (44%) 44 (11%) 0.001
Contact with TB disease 2 (13%) 4 (1%) 0.02
Household adult birth in a high-risk country
16 (100%)** 394 (99%)** 0.99
Houston High School StudyLindsay Hatzenbuehler, Andrea Cruz, Jeffrey Starke
Risk Factors & IGRA Results
Adolescents understood their risk They agreed to testing, even with a test
requiring venipuncture They and their parents were adherent with
therapy They discussed it with others in their
community
Take-Home Messages

25
Childhood TB: Lessons From a Low Burden Environment
Prevention of TB in children requires a system with central coordination and community activity
Linking a child to a source case improves the accuracy of diagnosis and effectiveness of treatment
Analysis of childhood tuberculosis is a window into the effectiveness of TB control – “yellow canaries”
Most childhood TB can be prevented with very little cost but better organization and emphasis
Migrating children are at high risk and have difficulty accessing central and community services
Young children with tuberculosis are rarely infectious to others
Main Challenges to TB Elimination in the U.S. Political commitment
As cases continue to decrease, seems less of a priority to general public and policymakers
Resources at risk – “U-shaped Curve of Concern”
Loss of expertise and experience
Clinical [nurses and MDs], laboratory, program
Drug and biologic shortages because of lack of market
Regulatory requirements (FDA) limit access to larger global market, e.g. child-friendly formulations
Concentration of remaining cases and outbreaks in more difficult-to-reach populations
Foreign-born, homeless, etc.
***How to address the large pool of persons with latent tuberculosis infection (LTBI)
<10 thousand TB cases; up to 13 million persons with LTBI
26
The Old Approach to Childhood Tuberculosis
Childhood TB has been relegated to National TB Control Programs, many of which have not had pediatric-specific guidelines or content in their educational and instructional materials
Children are identified only when they become sick, when TB is advanced and more difficult to manage
Because of the under-reporting of childhood TB, the disease has not been considered in discussions of child survival and the Millennium Development Goals
Childhood contacts of cases are rarely identified and given preventive therapy in the highest burden settings“Insanity is doing the same thing over and over again and expecting a different result!” – Albert Einstein
A New Approach
We need to decentralize care to people and organizations that will take the science of childhood tuberculosis and make it effective practice. Children and adolescents must be included in the three pillars of public health:
Scientific and operational research
Policy Development
Implementation of appropriate clinical practices
Science Guidelines Policy Practice
27
Childhood Tuberculosis: What Will Be The Tipping Point?
In his 2000 book, “The Tipping Point”, Malcolm Gladwell described the three basic elements of social “epidemics” that lead to fundamental change – the “tipping point”
how trends are often driven by a handful of exceptional people [The Law of the Few]
how to make a “contagious” message memorable [The Stickiness Factor]
the central importance of environment in changing behaviors [The Power of Context]
Tipping Point #1: The Law of the Few
We need to identify “connectors” – people and organizations that will take science and make it effective practice eg. the WHO for 35 years has recommended that asymptomatic children who live in households with a case of tuberculosis receive 6 months of INH. This simply is not done!
Science Guidelines Policy Practice
“Never doubt that a small group of thoughtful, committed, citizens can change the world. Indeed, it is the only thing that ever has.” ― Margaret Mead

28
Tipping Point #2: The Stickiness Factor
We need more effective messages
We need to tell patient and family stories
We need to market childhood tuberculosis to funders, scientists, clinicians and policy-makers
Little things matter
Tipping Point #3: The Power of Context
All public health is local: local data and need always trump global data and policies
Childhood tuberculosis should be linked with other perceived pressing needs – HIV, malnutrition, vaccination, MCH
The most expensive case of a disease will be the last one
Reichman’s U-shaped
curve of concern
29
So, are we at the Tipping Point for childhood tuberculosis?
30

31
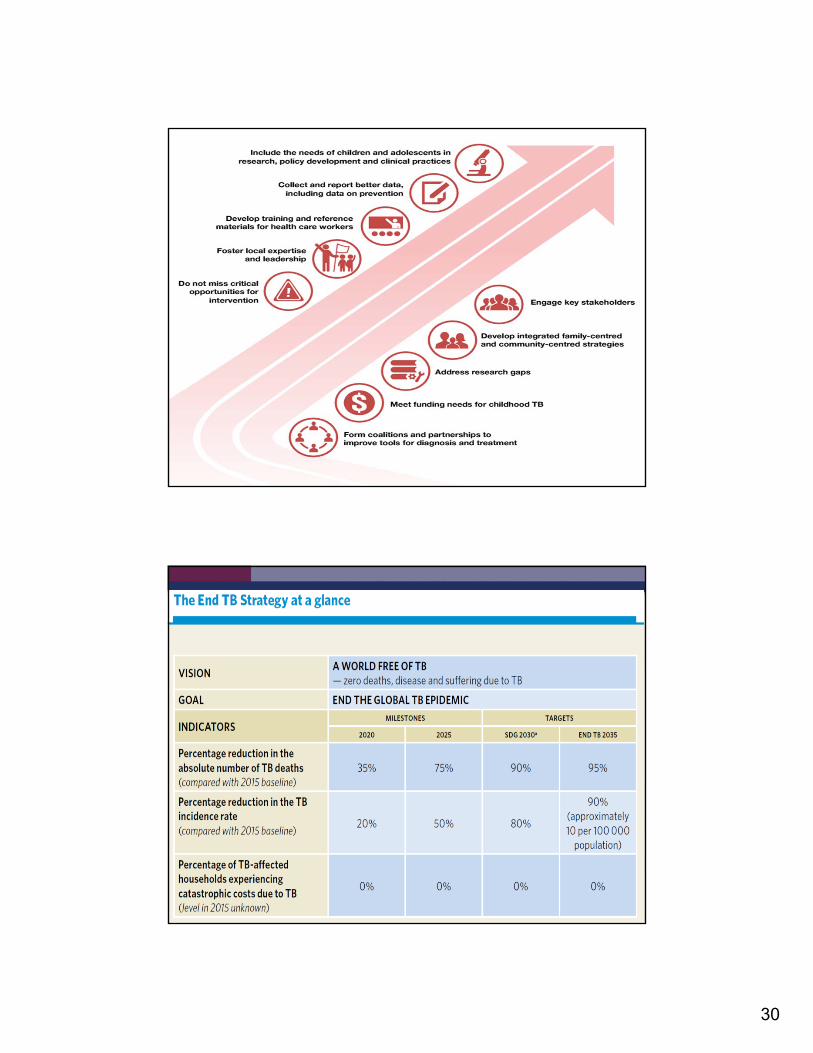
WHO End TB Strategy

32
Ten Truths About Childhood Tuberculosis
1. Adequate TB control for children requires a robust public health system.
2. We can prevent most childhood TB with simple, inexpensive measures.
3. Childhood TB can be found earlier when it is easier to treat.
4. Finding and treating adults with TB is notsufficient for controlling childhood TB.
5. BCG vaccines alone cannot control childhood TB.
Ten Truths About Childhood Tuberculosis
6. Some tests, like chest xray, are more important for children than adults.
7. Many adult TB cases arise from infection that occurred in childhood.
8. Childhood TB is a window into the effectiveness of tuberculosis control.
9. Almost all children with TB are treated with medications designed for adults.
10. Childhood TB is a neglected disease in most of the world.

33
CHILDHOOD TUBERCULOSIS: THE HIDDEN EPIDEMIC
Donald Int J Tuberc Lung Dis 2004; 8:627
“The time has come for the hidden epidemic of childhood tuberculosis to emerge from the shadow of adult tuberculosis and be seen as a neglected child health problem of considerable proportions in precisely those communities that do not have the resources to deal with it adequately.”





























