Embed Size (px)
Citation preview
Ethical Problems in Ethical Problems in Pharmacogenomic ResearchPharmacogenomic Research
Dr. Fred Lombardo
Howard University
Basic BioethicsBasic Bioethics
Two predominate philosophies governing ethics in the Western world:– Deontological view-I. Kant (1724-1804)– Utilitarianism-John Locke (1632-1704) and
John Stuart Mill (1806-1873)
Deontology/UtilitarianismDeontology/Utilitarianism
Deontology– The study of duties
that persons have toward one another.
– The categorical imperative of Immanuel Kant
Utilitarianism– The view that actions
or policies are to be morally evaluated according to the extent to which they promote happiness or well-being

Clinical BioethicsClinical Bioethics
Principles:– Beneficence (To do Good)– Nonmaleficence (Primum non nocere)– Justice (Fairness)– Autonomy (Self-determination)– Veracity (Truth telling)– Utility (The greatest good for the greatest
number)

PharmacogenomicsPharmacogenomics
Pharmacogenomics: Social, Ethical, and Clinical Dimensions, ed. Mark A. Rothstein, 2003, John Wiley& Sons.– Challenges
Informed Consent Control over Research Materials and Data Confidentiality Return of Relevant Information to Individual Commercialism
DefinitionDefinition
Pharmacogenetics: The role of genetic variation in differential response to pharmaceuticals.
Pharmacogenomics: The use of genomic technologies in assessing differential response to pharmaceuticals.
From: Evans WE, Relling MV. Pharmacogenomics: Translating functional genomics into rational therapeutics. Science 286:487-491, 1999.
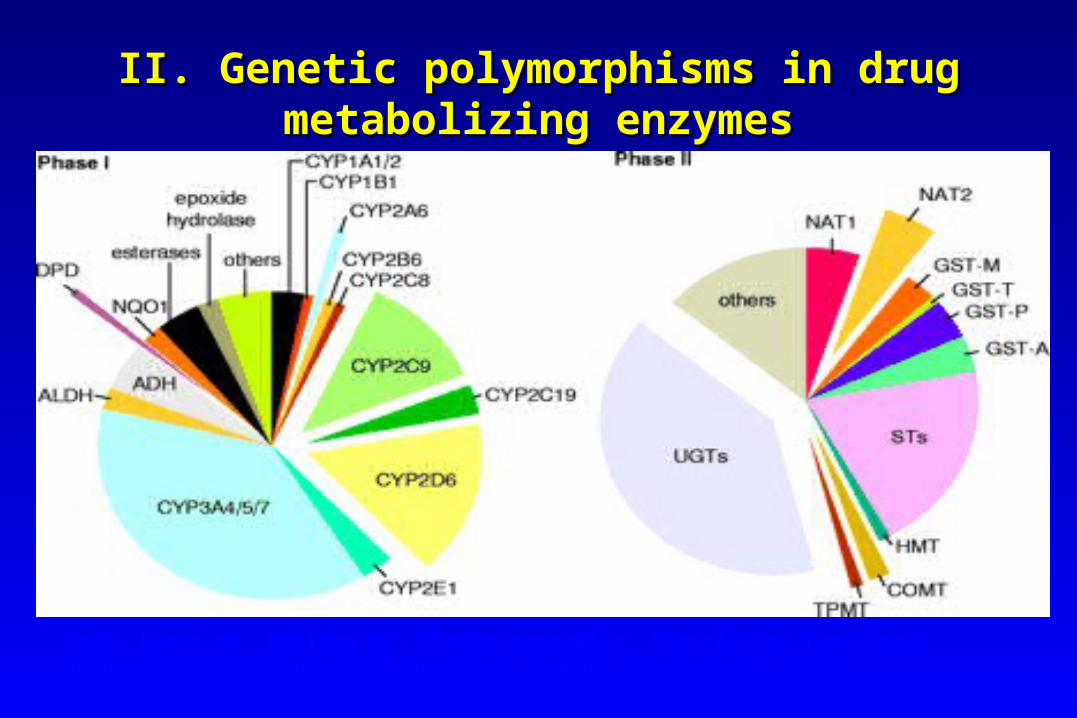
II. Genetic polymorphisms in drug II. Genetic polymorphisms in drug metabolizing enzymesmetabolizing enzymes
II. CLASSIFICATIONII. CLASSIFICATIONPhase IPhase I•AsyntheticAsynthetic•Introduce or expose a functional group increasing polarityIntroduce or expose a functional group increasing polarity•Includes oxidation, reduction and hydrolysisIncludes oxidation, reduction and hydrolysis
Phase IIPhase II•Synthetic (conjugation reaction)Synthetic (conjugation reaction)•Couples drug with an endogenous substrateCouples drug with an endogenous substrate•Conjugation with glucuronic acid, sulfate, acetic acid or Conjugation with glucuronic acid, sulfate, acetic acid or an amino acidan amino acid
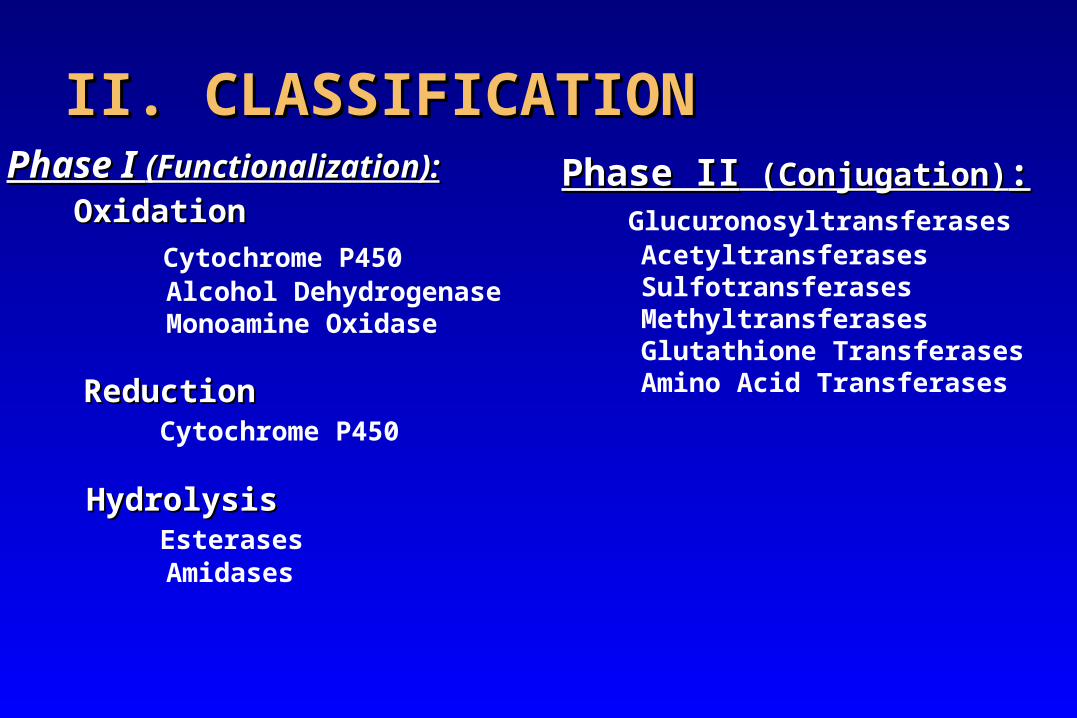
II. CLASSIFICATIONII. CLASSIFICATIONPhase I Phase I (Functionalization):(Functionalization):
OxidationOxidation
Cytochrome P450 Alcohol Dehydrogenase Monoamine Oxidase
ReductionReduction Cytochrome P450
HydrolysisHydrolysis Esterases Amidases
Phase IIPhase II (Conjugation) (Conjugation):: Glucuronosyltransferases Acetyltransferases Sulfotransferases Methyltransferases Glutathione Transferases Amino Acid Transferases
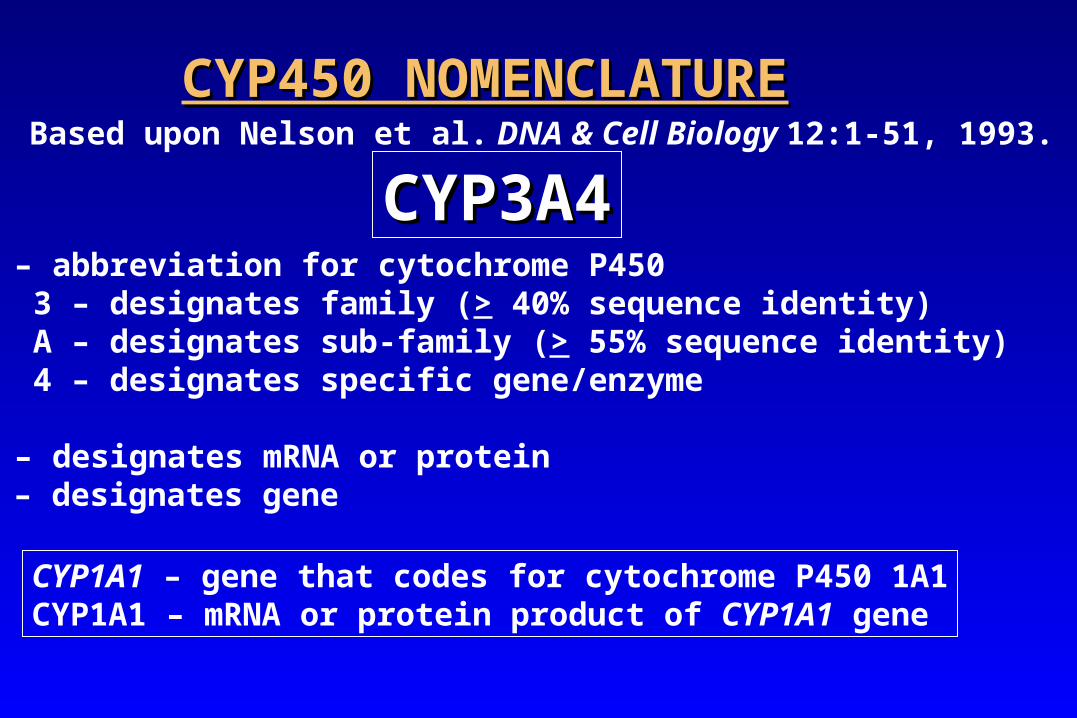
CYP450 NOMENCLATURECYP450 NOMENCLATUREBased upon Nelson et al. DNA & Cell Biology 12:1-51, 1993.
CYP3A4CYP3A4CYP – abbreviation for cytochrome P450 3 – designates family (> 40% sequence identity) A – designates sub-family (> 55% sequence identity) 4 – designates specific gene/enzyme
CYP – designates mRNA or proteinCYP – designates gene
CYP1A1 – gene that codes for cytochrome P450 1A1CYP1A1 – mRNA or protein product of CYP1A1 gene
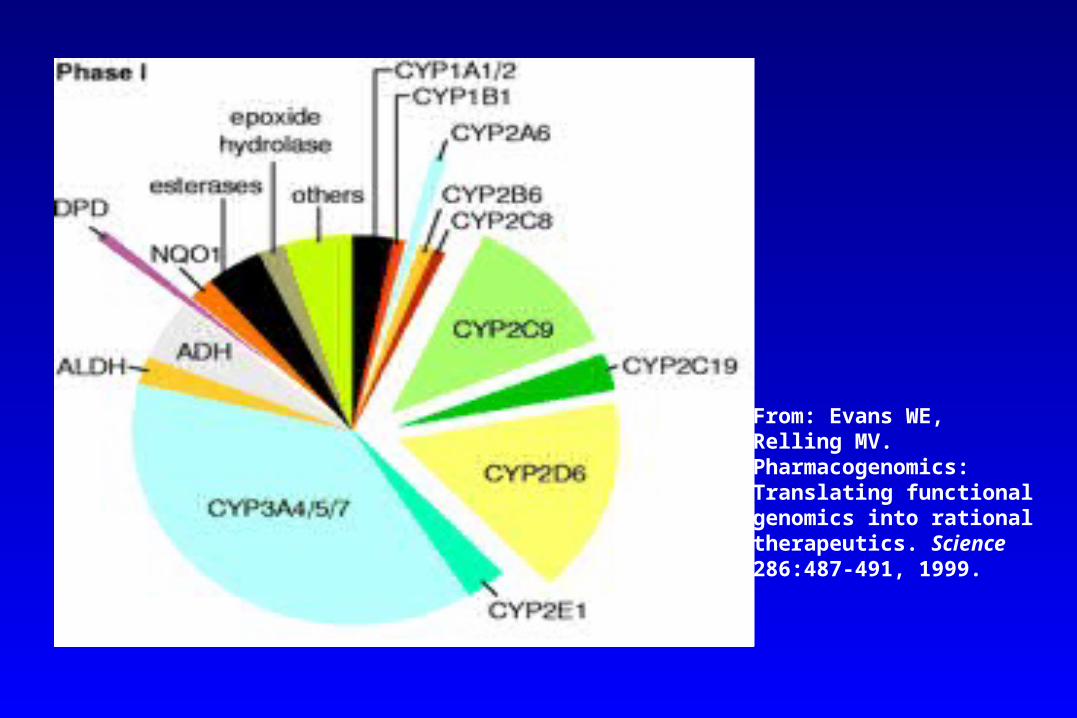
From: Evans WE, Relling MV. Pharmacogenomics: Translating functional genomics into rational therapeutics. Science 286:487-491, 1999.
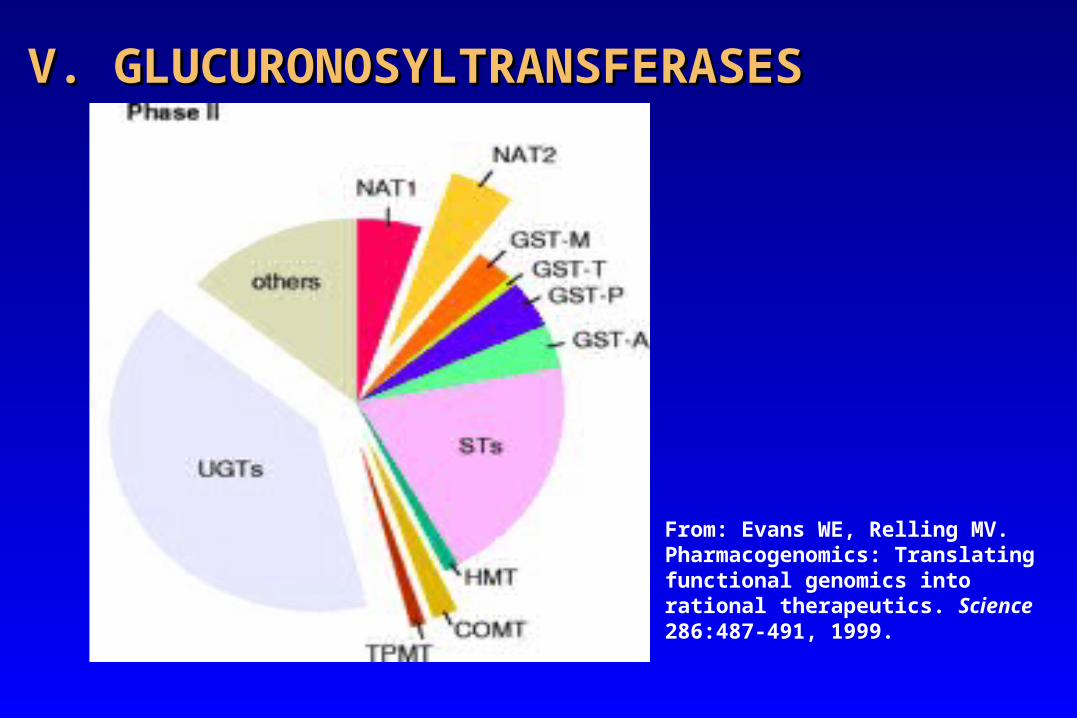
V. GLUCURONOSYLTRANSFERASESV. GLUCURONOSYLTRANSFERASES
From: Evans WE, Relling MV. Pharmacogenomics: Translating functional genomics into rational therapeutics. Science 286:487-491, 1999.
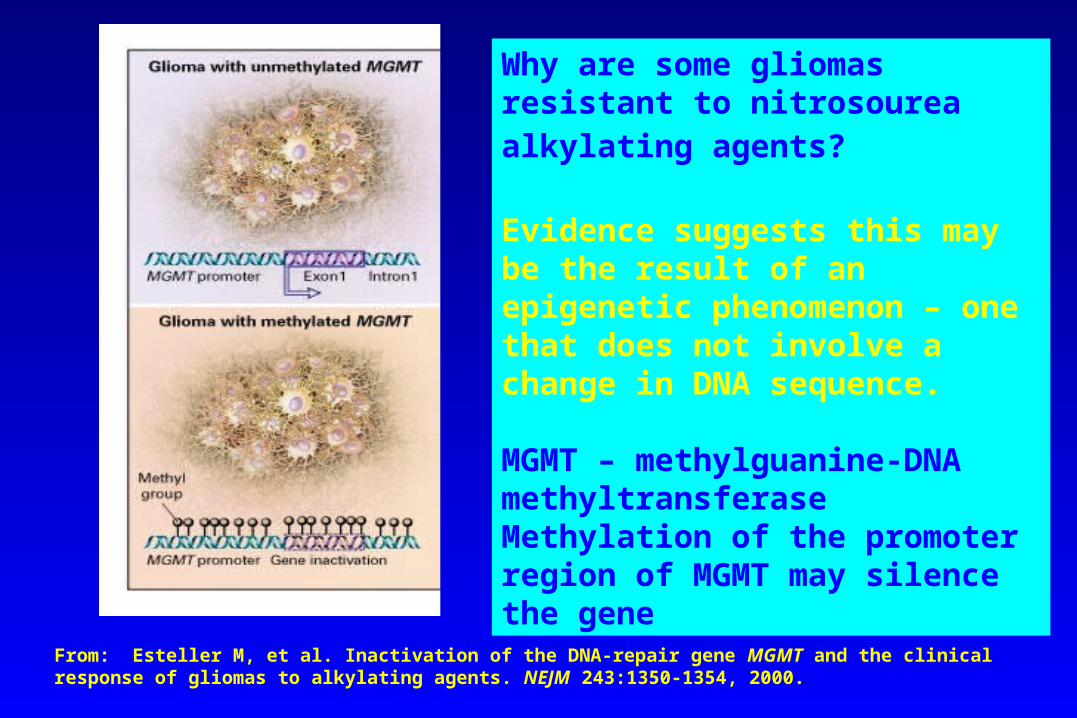
From: Esteller M, et al. Inactivation of the DNA-repair gene MGMT and the clinical response of gliomas to alkylating agents. NEJM 243:1350-1354, 2000.
Why are some gliomas resistant to nitrosourea alkylating agents?
Evidence suggests this may be the result of an epigenetic phenomenon – one that does not involve a change in DNA sequence.
MGMT – methylguanine-DNA methyltransferaseMethylation of the promoter region of MGMT may silence the gene
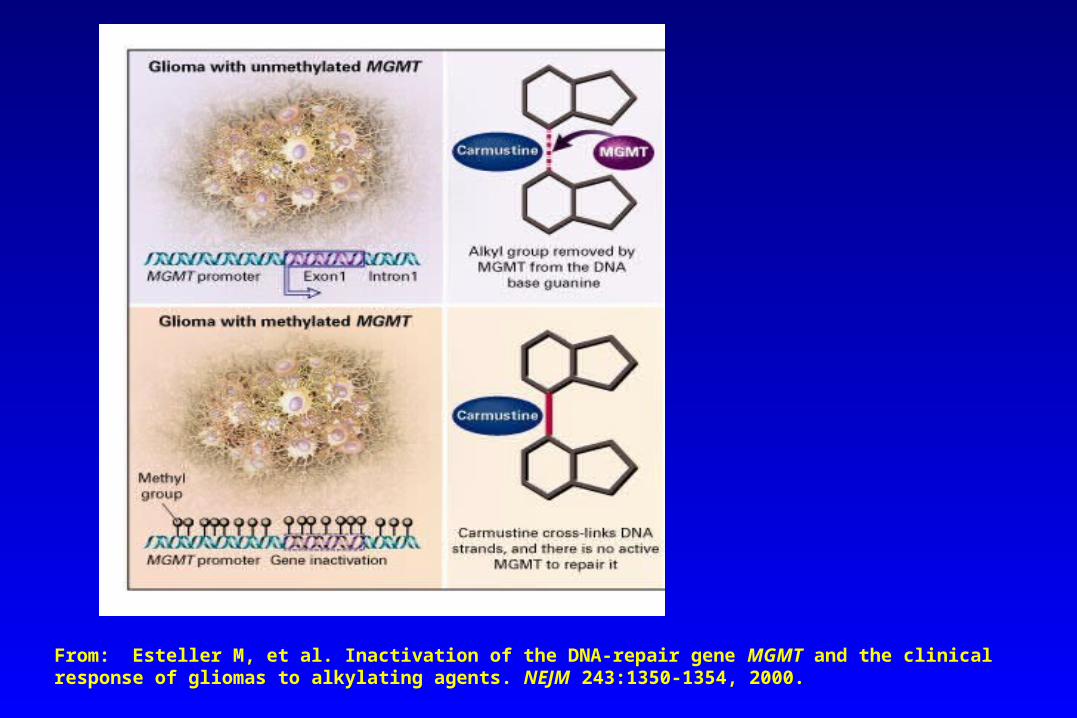
From: Esteller M, et al. Inactivation of the DNA-repair gene MGMT and the clinical response of gliomas to alkylating agents. NEJM 243:1350-1354, 2000.
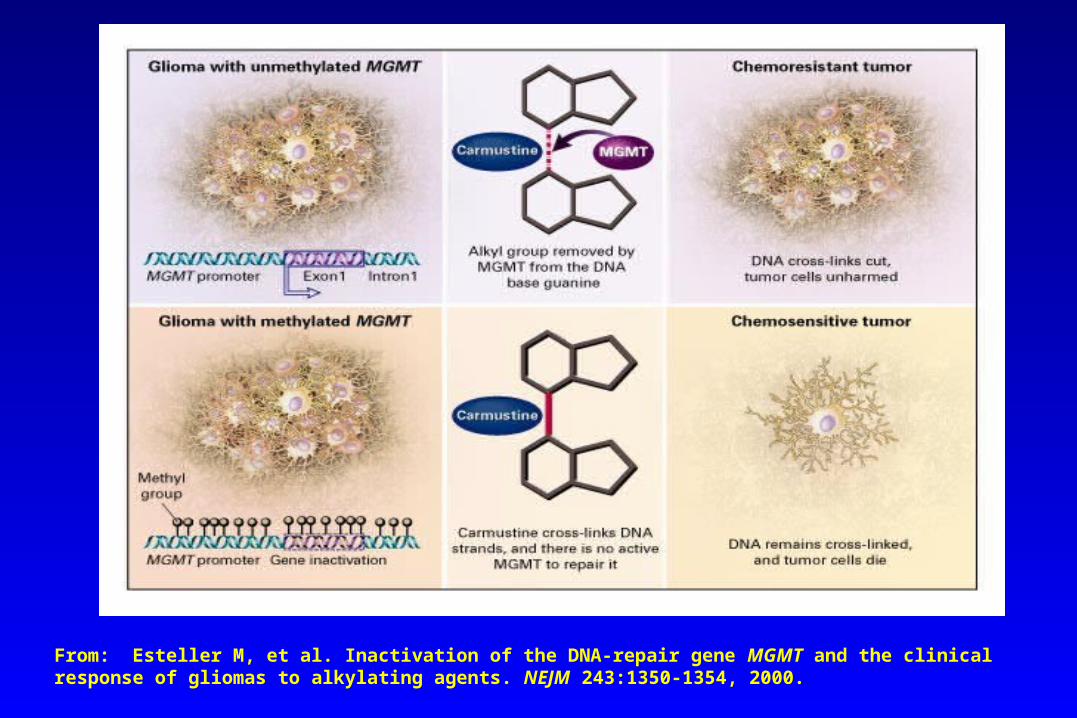
From: Esteller M, et al. Inactivation of the DNA-repair gene MGMT and the clinical response of gliomas to alkylating agents. NEJM 243:1350-1354, 2000.
Problems SeenProblems Seen
Inability to form 5-deoxyuridine monophosphate from 5-fluorouracil because of deficiency in dipyrimidine dehydrogenase has led to prolonged pancytopenia and severe mucositis in 2 patients at Howard University.
Test is now available to measure DPD activity.
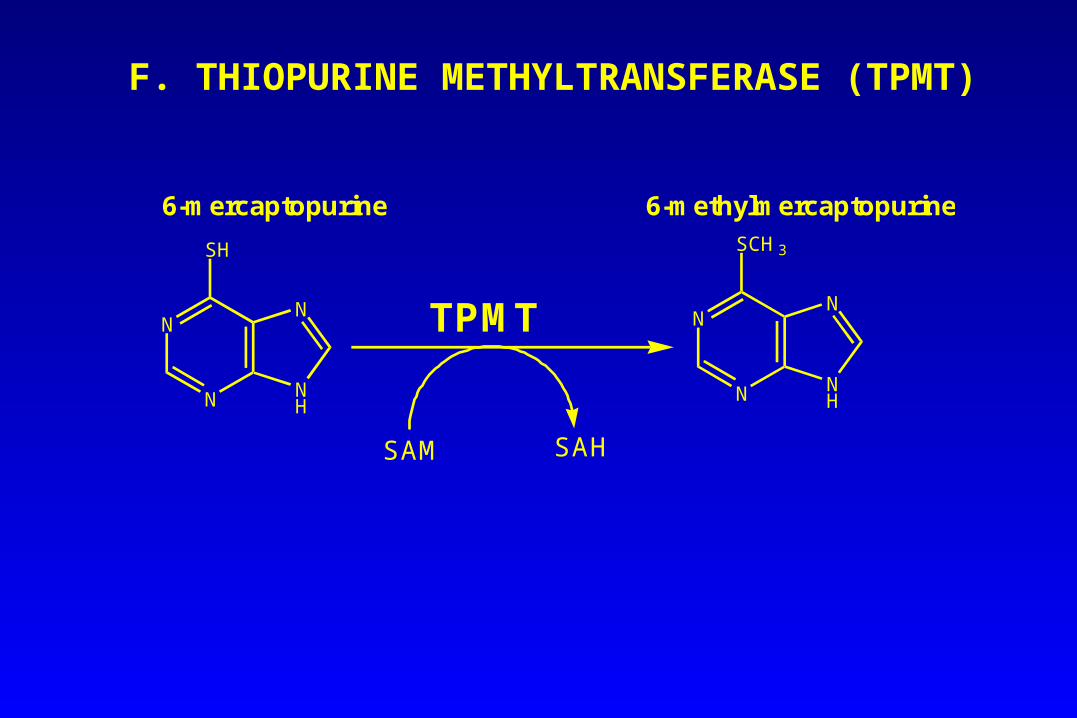
F. THIOPURINE METHYLTRANSFERASE (TPMT)
N
N NH
N
SH
N
N NH
N
SCH3
TPMT
SAM SAH
6-mercaptopurine 6-methylmercaptopurine
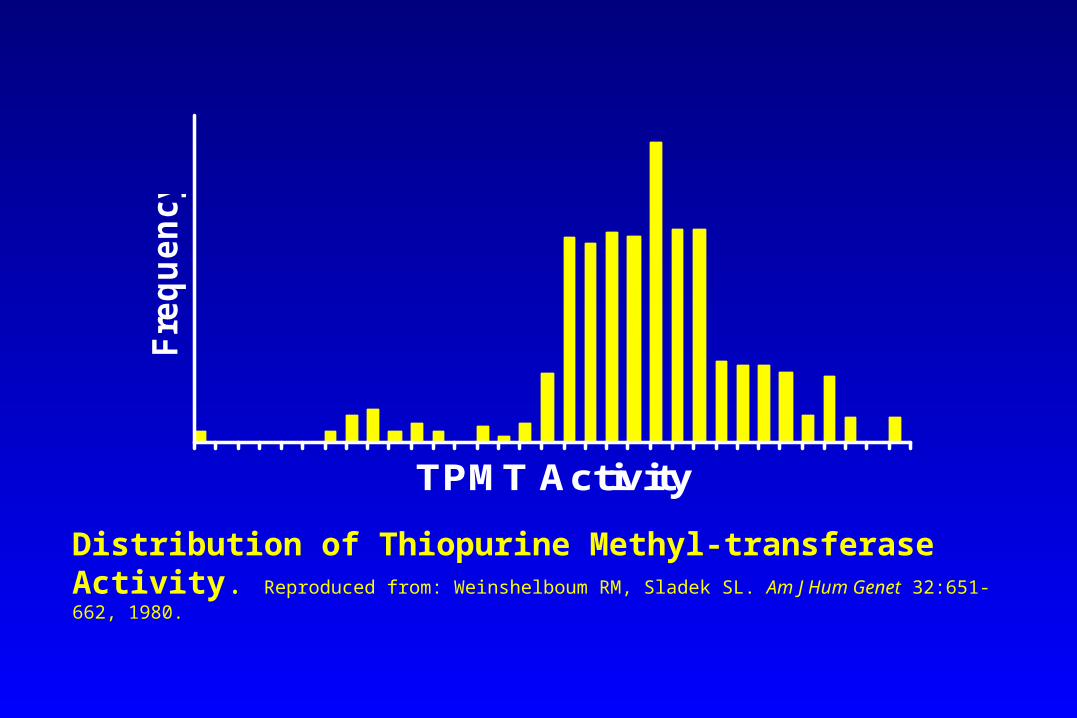
TPMT Activity
Fre
qu
en
cy
Distribution of Thiopurine Methyl-transferase Activity. Reproduced from: Weinshelboum RM, Sladek SL. Am J Hum Genet 32:651-662, 1980.
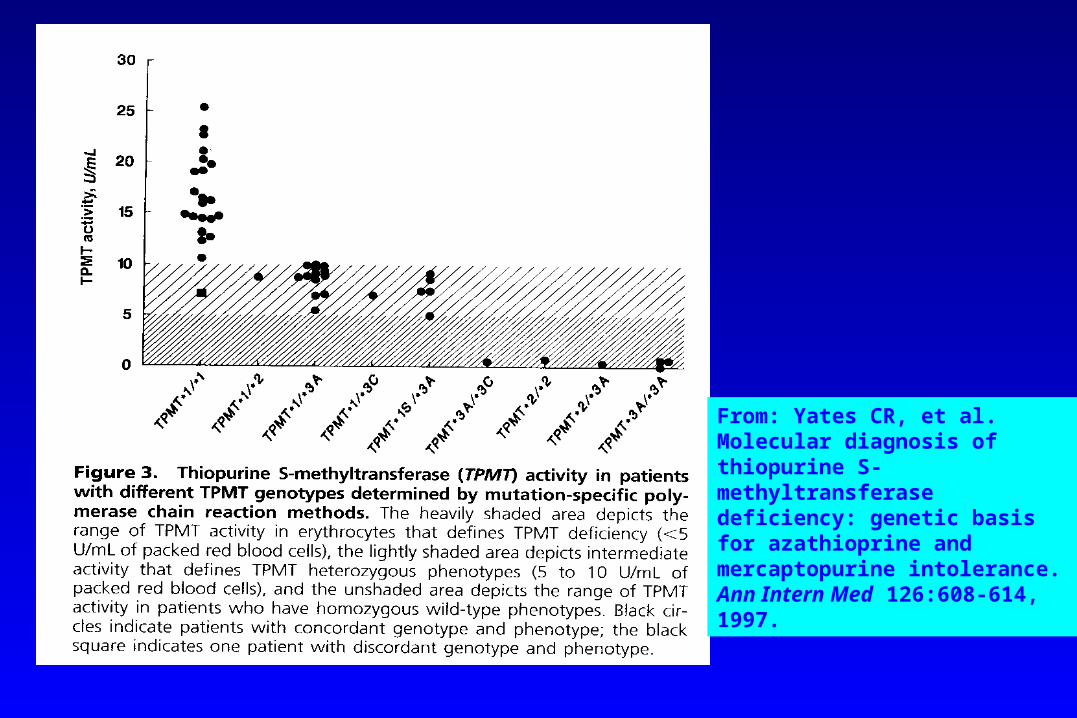
From: Yates CR, et al. Molecular diagnosis of thiopurine S-methyltransferase deficiency: genetic basis for azathioprine and mercaptopurine intolerance. Ann Intern Med 126:608-614, 1997.
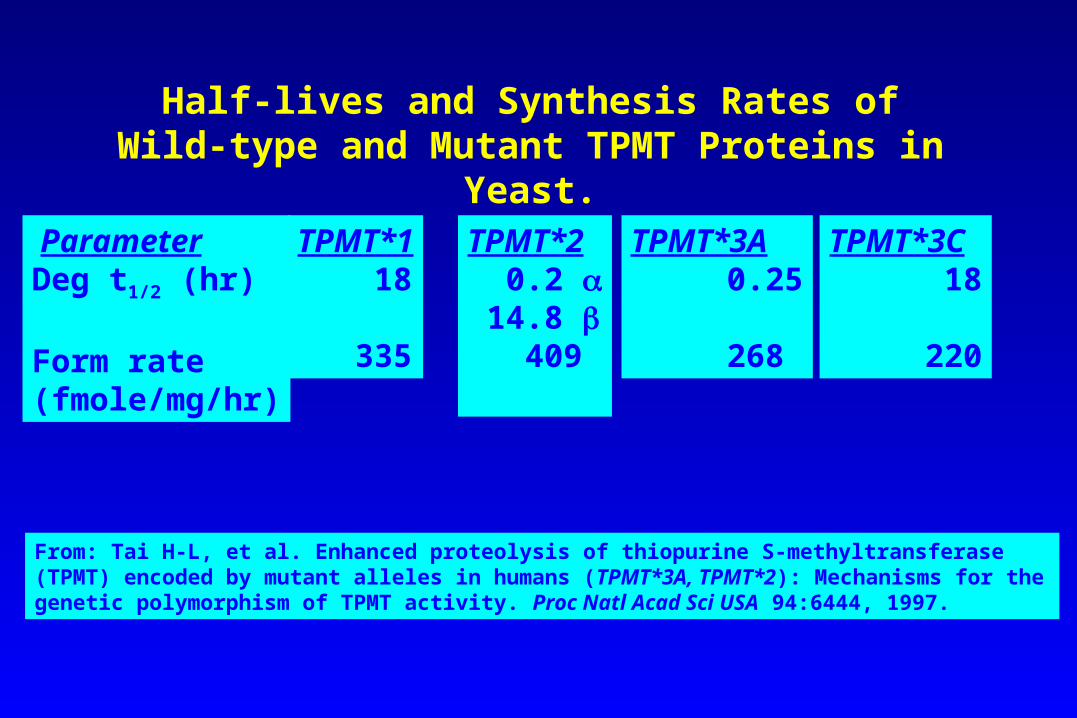
Half-lives and Synthesis Rates of Wild-type and Mutant TPMT Proteins in Yeast.
ParameterDeg t1/2 (hr)
Form rate(fmole/mg/hr)
TPMT*1 18
335
TPMT*2 0.2 14.8 409
TPMT*3A 0.25
268
TPMT*3C 18
220
From: Tai H-L, et al. Enhanced proteolysis of thiopurine S-methyltransferase (TPMT) encoded by mutant alleles in humans (TPMT*3A, TPMT*2): Mechanisms for the genetic polymorphism of TPMT activity. Proc Natl Acad Sci USA 94:6444, 1997.
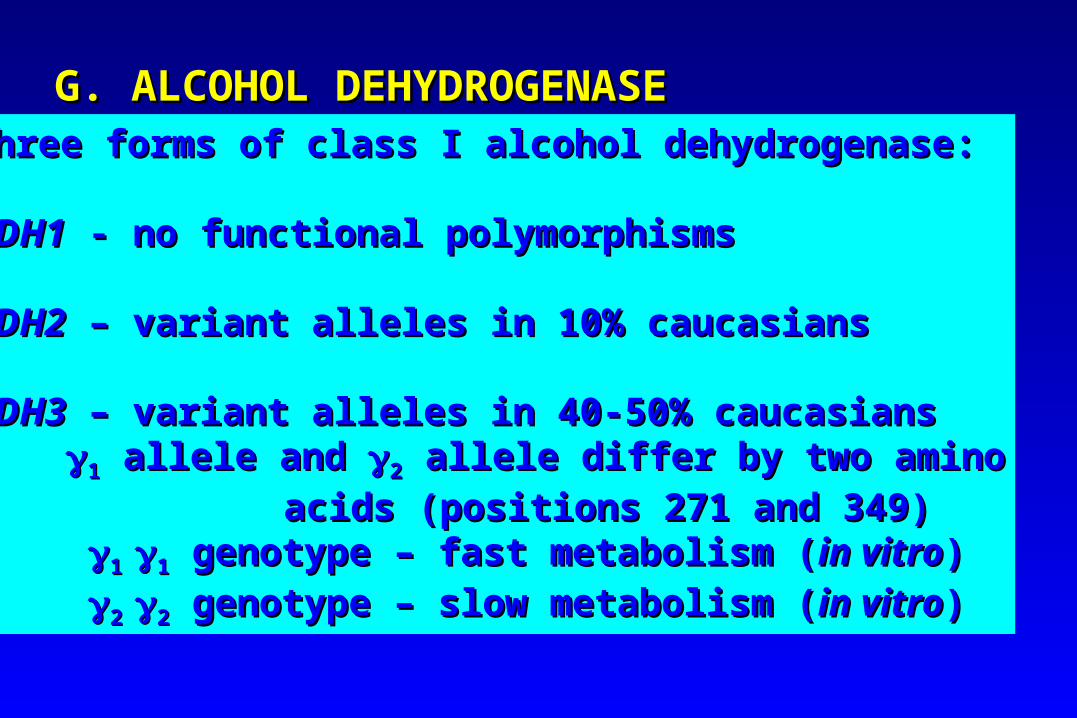
G. ALCOHOL DEHYDROGENASEG. ALCOHOL DEHYDROGENASEThree forms of class I alcohol dehydrogenase:Three forms of class I alcohol dehydrogenase:
ADH1ADH1 - no functional polymorphisms - no functional polymorphisms
ADH2ADH2 – variant alleles in 10% caucasians – variant alleles in 10% caucasians
ADH3ADH3 – variant alleles in 40-50% caucasians – variant alleles in 40-50% caucasians11 allele and allele and 22 allele differ by two amino allele differ by two amino
acids (positions 271 and 349)acids (positions 271 and 349) 1 1 11 genotype – fast metabolism ( genotype – fast metabolism (in vitroin vitro))
2 2 22 genotype – slow metabolism ( genotype – slow metabolism (in vitroin vitro))
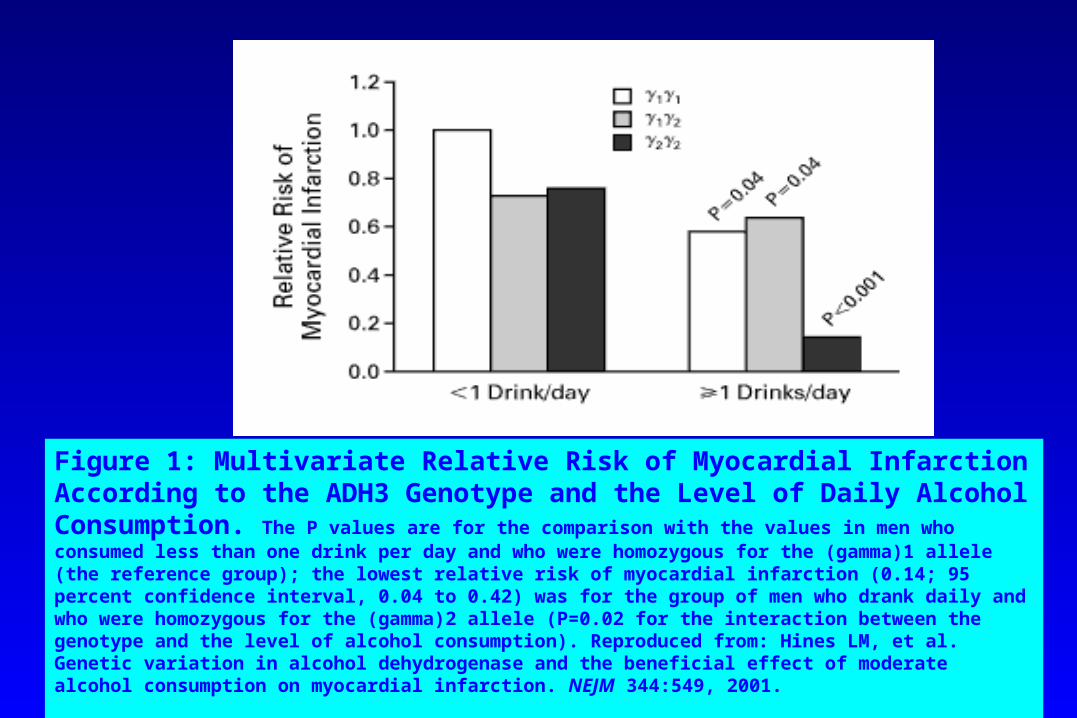
Figure 1: Multivariate Relative Risk of Myocardial Infarction According to the ADH3 Genotype and the Level of Daily Alcohol Consumption. The P values are for the comparison with the values in men who consumed less than one drink per day and who were homozygous for the (gamma)1 allele (the reference group); the lowest relative risk of myocardial infarction (0.14; 95 percent confidence interval, 0.04 to 0.42) was for the group of men who drank daily and who were homozygous for the (gamma)2 allele (P=0.02 for the interaction between the genotype and the level of alcohol consumption). Reproduced from: Hines LM, et al. Genetic variation in alcohol dehydrogenase and the beneficial effect of moderate alcohol consumption on myocardial infarction. NEJM 344:549, 2001.
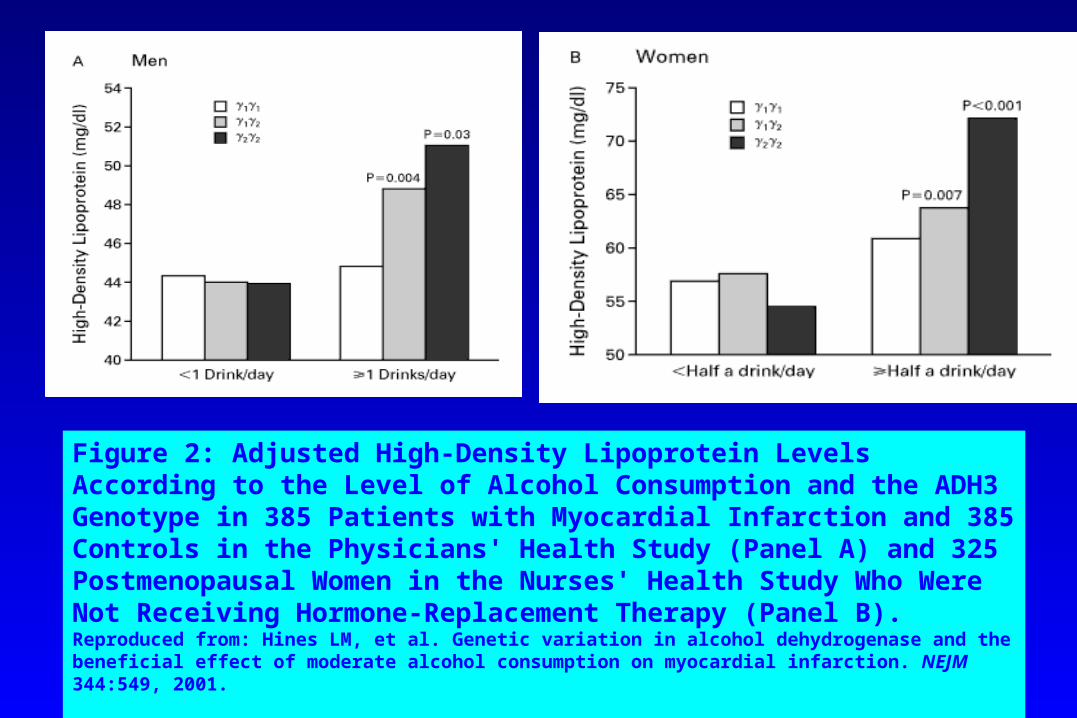
Figure 2: Adjusted High-Density Lipoprotein Levels According to the Level of Alcohol Consumption and the ADH3 Genotype in 385 Patients with Myocardial Infarction and 385 Controls in the Physicians' Health Study (Panel A) and 325 Postmenopausal Women in the Nurses' Health Study Who Were Not Receiving Hormone-Replacement Therapy (Panel B). Reproduced from: Hines LM, et al. Genetic variation in alcohol dehydrogenase and the beneficial effect of moderate alcohol consumption on myocardial infarction. NEJM 344:549, 2001.
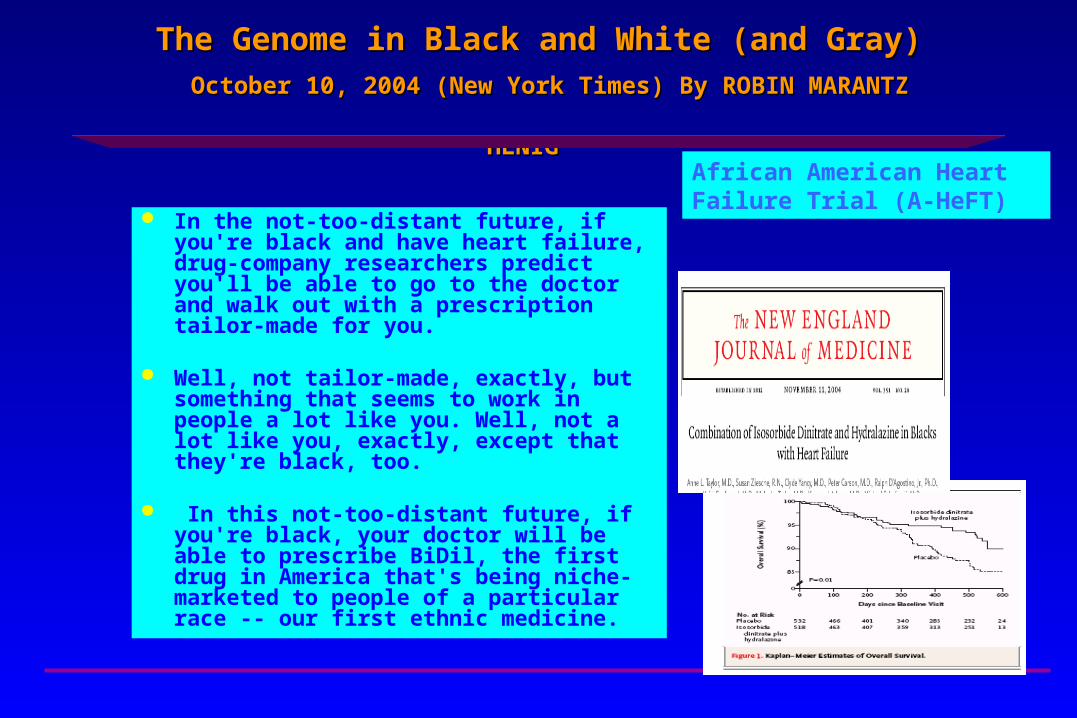
The Genome in Black and White (and Gray)The Genome in Black and White (and Gray)
October 10, 2004 (New York Times) By ROBIN MARANTZ HENIGOctober 10, 2004 (New York Times) By ROBIN MARANTZ HENIG
In the not-too-distant future, if you're black and have heart failure, drug-company researchers predict you'll be able to go to the doctor and walk out with a prescription tailor-made for you.
Well, not tailor-made, exactly, but something that seems to work in people a lot like you. Well, not a lot like you, exactly, except that they're black, too.
In this not-too-distant future, if you're black, your doctor will be able to prescribe BiDil, the first drug in America that's being niche-marketed to people of a particular race -- our first ethnic medicine.
African American Heart Failure Trial (A-HeFT)
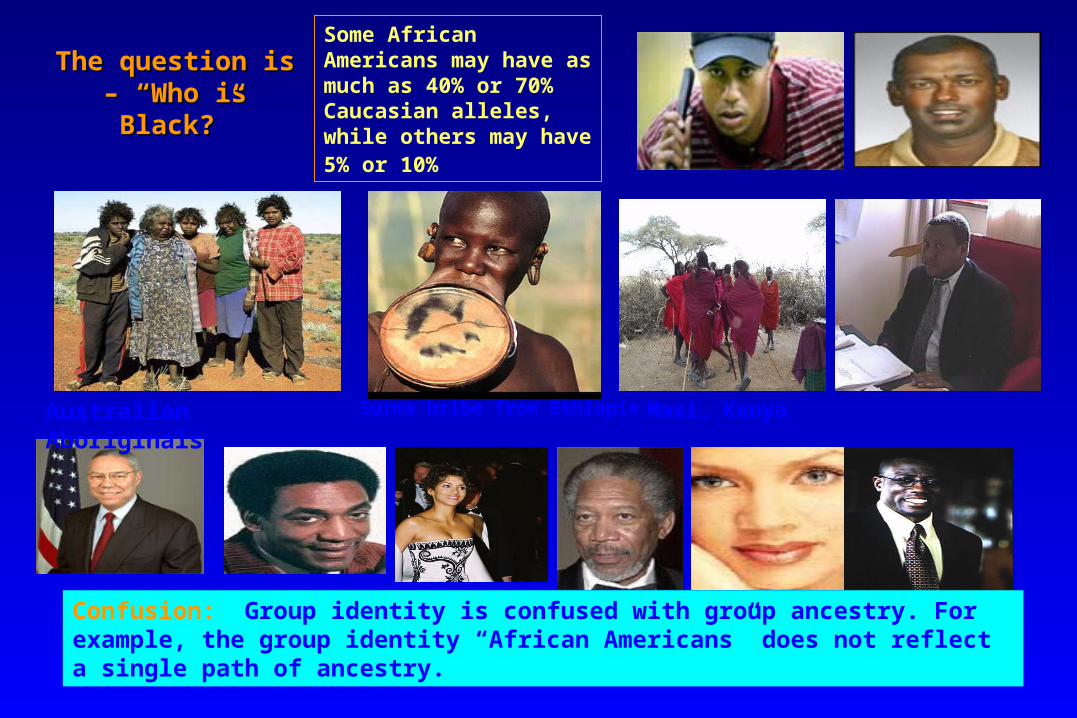
The question is – The question is – “Who is Black?”“Who is Black?”
Australian Aboriginals Masi, KenyaSurma bribe from Ethiopia
Confusion: Group identity is confused with group ancestry. For example, the group identity “African Americans” does not reflect a single path of ancestry.
Some African Americans may have as much as 40% or 70% Caucasian alleles, while others may have 5% or 10%
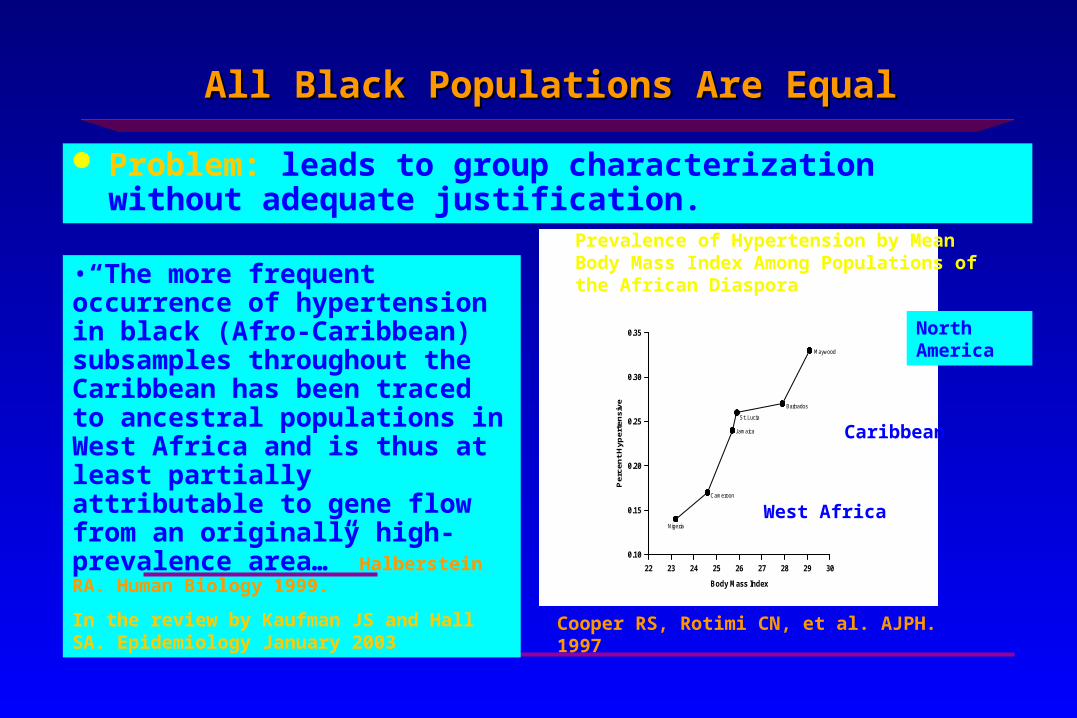
All Black Populations Are EqualAll Black Populations Are Equal
Problem: leads to group characterization without adequate justification.
Body Mass Index
22 23 24 25 26 27 28 29 30
Per
cen
t H
yper
ten
sive
0.10
0.15
0.20
0.25
0.30
0.35
Nigeria
Cameroon
Jamaica
St. Lucia
Barbados
Maywood
•“The more frequent occurrence of hypertension in black (Afro-Caribbean) subsamples throughout the Caribbean has been traced to ancestral populations in West Africa and is thus at least partially attributable to gene flow from an originally high-prevalence area…” Halberstein RA. Human Biology 1999.
In the review by Kaufman JS and Hall SA. Epidemiology January 2003
Prevalence of Hypertension by Mean Body Mass Index Among Populations of the African Diaspora
North America
Caribbean
West Africa
Cooper RS, Rotimi CN, et al. AJPH. 1997
N=85,000
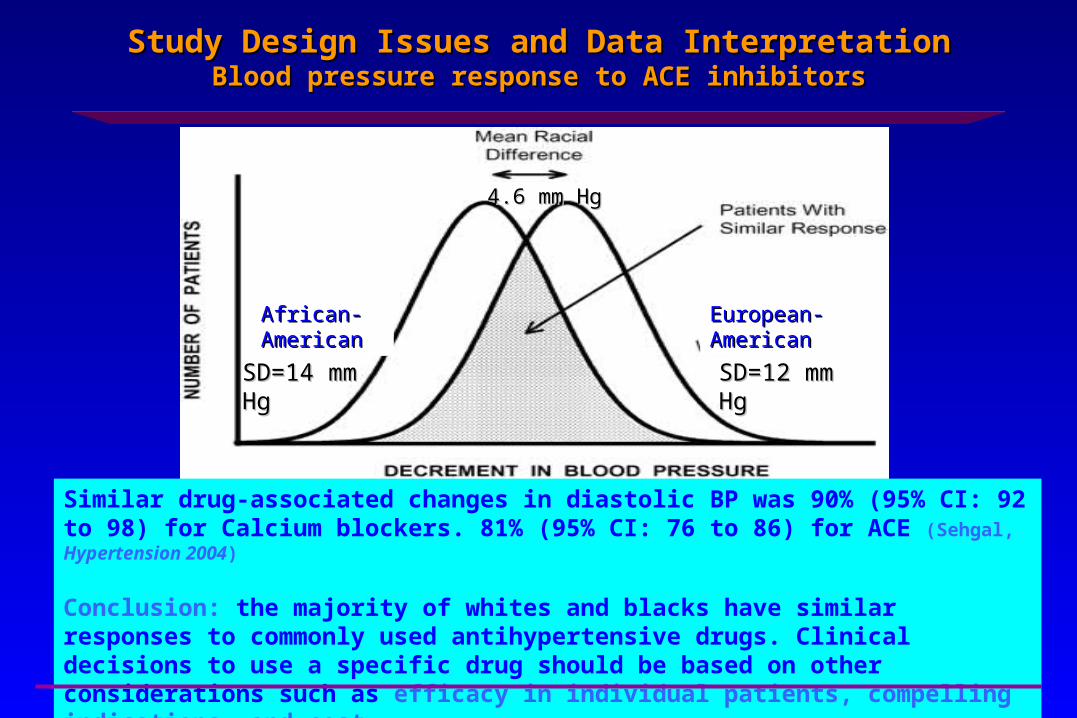
Study Design Issues and Data InterpretationStudy Design Issues and Data InterpretationBlood pressure response to ACE inhibitorsBlood pressure response to ACE inhibitors
4.6 mm Hg4.6 mm Hg
SD=14 mm SD=14 mm HgHg
SD=12 mm SD=12 mm HgHg
African-African-AmericanAmerican
European-European-AmericanAmerican
Similar drug-associated changes in diastolic BP was 90% (95% CI: 92 to 98) for Calcium blockers. 81% (95% CI: 76 to 86) for ACE (Sehgal, Hypertension 2004)
Conclusion: the majority of whites and blacks have similar responses to commonly used antihypertensive drugs. Clinical decisions to use a specific drug should be based on other considerations such as efficacy in individual patients, compelling indications, and cost.
We Advocate ForWe Advocate For
1. Labeling with language indicating the fact that BiDil does not replace existing drugs for the treatment of heart failure and that although it was tested only among African Americans, it may indeed be an effective treatment for heart failure patients who may not self identify (or be identified) as African Americans.
2. BiDil should not be approved as an African American ONLY drug (and by extension – all “black” people). The history of drug development and approval does not support ethnic labeling.
Due to political, social and economic forces, biomedical research was almost exclusively conducted in people, especially men, of European descent. Results of such studies were extrapolated to other groups without such labels as “White Drug”. In the end, the BiDil story will have similar outcome; if the drug continues to be effective in the treatment of heart failure, the global subset of individuals with heart failure who will benefit from the drug will not be accurately described by the label 'African American'.
We Advocate ForWe Advocate For
3. Strategies that promote overall health not simply the absence of disease (e.g, heart failure). What good is a drug that reduces mortality from heart failure by 43% if:
a. Because of patent, an otherwise cheap generically available therapeutics becomes
unaffordable;
b. It exacerbates racism with resulting increasedhypertension and associated complications,
including heart failure) due to increased psychosocial stressors;
c. It leads biomedical research down a wrong path by suggesting, without proper scientific justification, that the so-called racial categories are biological?
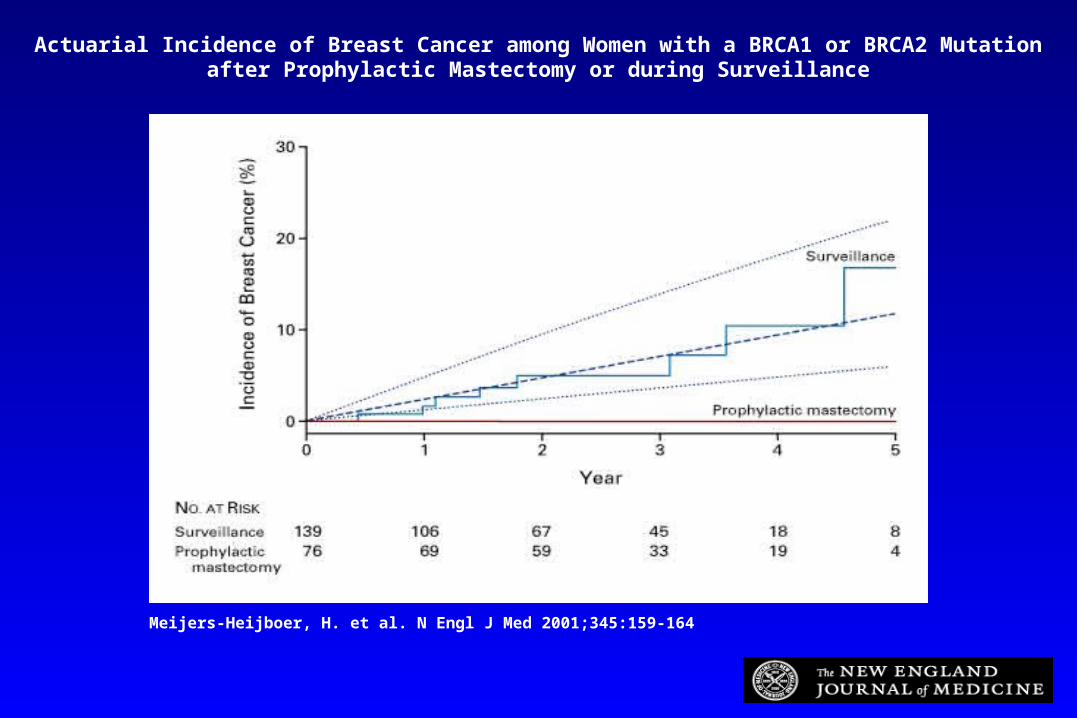
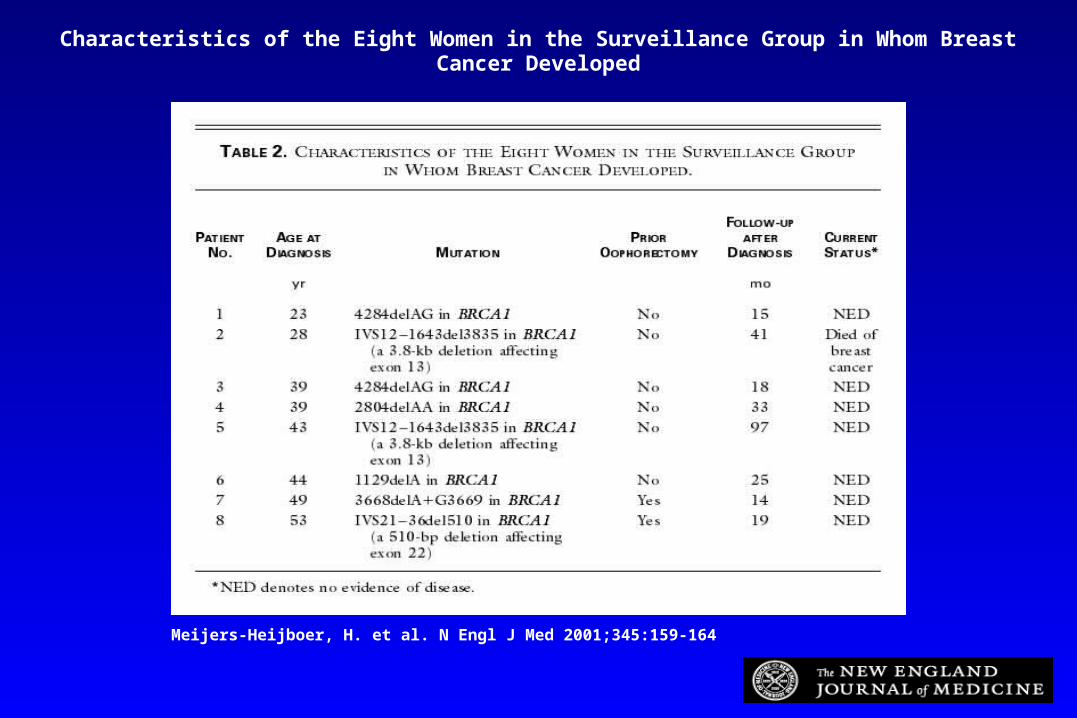
Meijers-Heijboer, H. et al. N Engl J Med 2001;345:159-164
Actuarial Incidence of Breast Cancer among Women with a BRCA1 or BRCA2 Mutation after Prophylactic Mastectomy or during Surveillance
Meijers-Heijboer, H. et al. N Engl J Med 2001;345:159-164
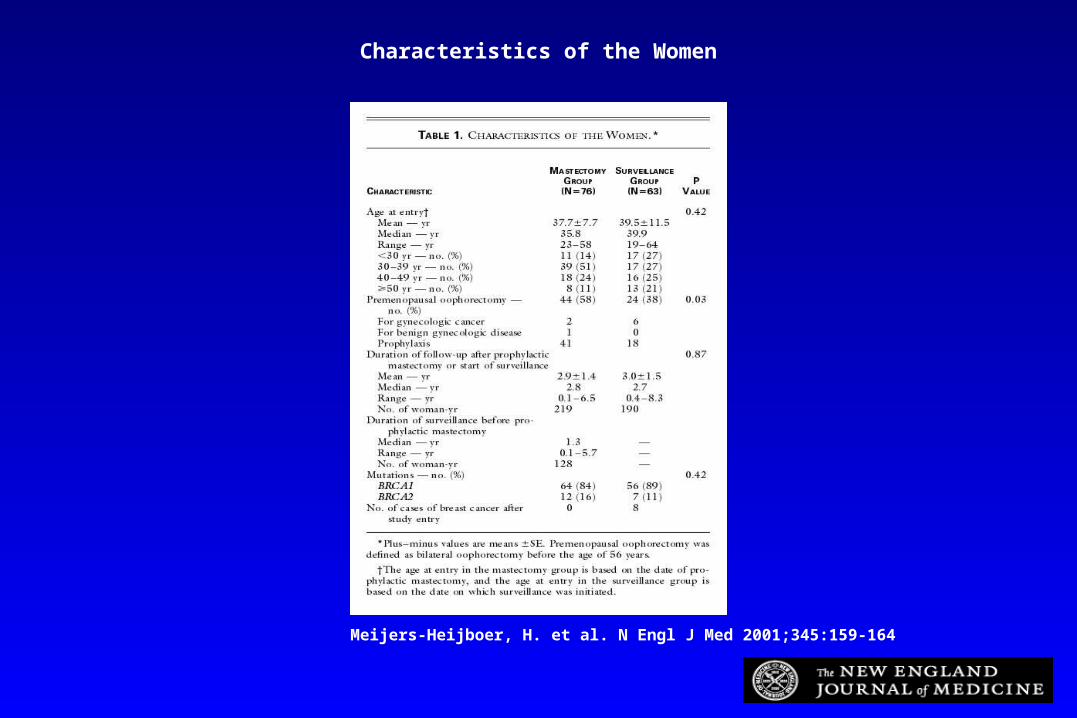
Characteristics of the Women
Meijers-Heijboer, H. et al. N Engl J Med 2001;345:159-164
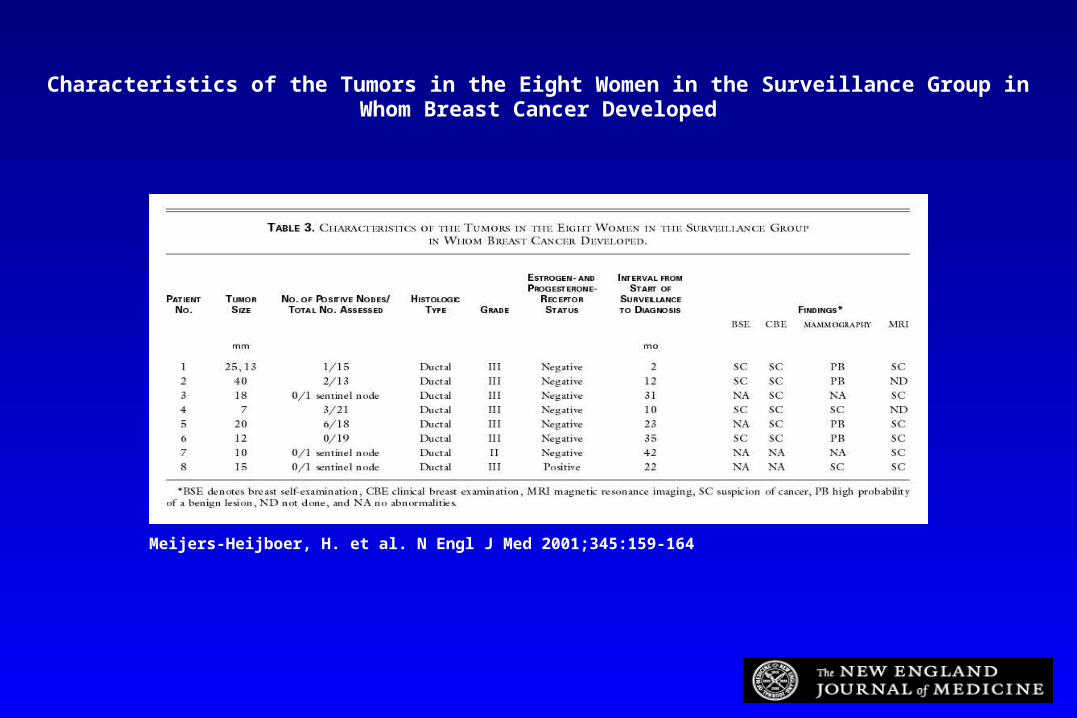
Characteristics of the Tumors in the Eight Women in the Surveillance Group in Whom Breast Cancer Developed
Meijers-Heijboer, H. et al. N Engl J Med 2001;345:159-164
Characteristics of the Eight Women in the Surveillance Group in Whom Breast Cancer Developed
Dr.Woo Suk HwangDr.Woo Suk Hwang
Dr. Hwang, veterinary scientist from Seoul National University cloned an Afghan hound named Snuppy (Seoul National University puppy).
Named Director, Stem-Cell Center, Seoul, Korea.
Branch labs planned for U.S. and U.K.

Dr. Hwang AftermathDr. Hwang Aftermath
Resigned as Director when it was reported that a member of his team had purchased human eggs from as many as 27 women for use in human stem cell experiments.
Two female members of his team had donated eggs to the cause.
Egg selling illegal in Korea Violation of scientific ethics for subordinates to
provide ova, even if free of charge.

Elements of Informed ConsentElements of Informed Consent
Threshold requirement: competence Information requirements
– Information– Understanding
Consent requirements– Consent– Authorization
Tuskegee Study (1932-1972)Tuskegee Study (1932-1972)
Reasons given for continuing study– Long-term benefits for African-Americans– Contribution to scientific knowledge– Benefits for subjects (would receive other
medical treatment)– Subjects were not harmed– Treatment might harm (Jarisch-Herxheimer)– Should not waste data collected
Tuskegee Study (1932-1972)Tuskegee Study (1932-1972)
Reasons given for not telling subjects the truth:– Subjects incapable of understanding– Scientists better equipped to determine what
would benefit the subjects (paternalism)– Better to sacrifice a few for the greater good of
the whole (utilitarianism)
Tuskegee Study (1932-1972)Tuskegee Study (1932-1972)
Reasons for breach of veracity tenet continued:– Subjects in the study were better off than those
not selected to participate.– Long-term scientific goals were of greater
importance than rights of an individual (Kant’s Categorical Imperative is breached)
Egregious Examples of Egregious Examples of Unethical ResearchUnethical Research
Tuskegee Syphilis Study (1932-1972) Nazi Experiments on Prisoners-WW II Willow Brook Study-1960’s Human Radiation Experiments 1950-1970 LSD Experiments 1930s Serratia marcescens experiments Bacillus subtilis experiments
Belmont ReportBelmont Report
Principles:– Respect for persons’ consent, privacy,
confidentiality– Beneficience (Benefits versus Risks)– Justice/Equality
45 Code of Federal 45 Code of Federal Regulations 46.111Regulations 46.111
Risks to subjects minimized Risks reasonable in relation to anticipated
benefits. Selection of subjects equitable Provision for safety monitoring Informed consent documented
45 CFR Part 46.11145 CFR Part 46.111
There is adequate provisions to protect the privacy of subjects and to maintain confidentiality of data
Where any of the subjects are likely to be vulnerable to coercion (“susceptible to kindness”) or undue influence, additional safeguards are incorporated to protect the subjects.
Informed ConsentInformed Consent
Benefits Risks Alternatives
The Nuremberg CodeThe Nuremberg Code
The voluntary consent of the human subject is absolutely essential.
The experiment should be such as to yield fruitful results for the good of society.
Experiment based on results of animal experiments and knowledge of the natural history of the disease or problem
The Nuremberg CodeThe Nuremberg Code
The experiment should be conducted as to avoid all unnecessary physical and mental suffering and injury.
No experiment should be conducted where there is an a priori reason to believe that death or disabling injury will occur;except in those experiments where the investigators serve as subjects.
The Nuremberg CodeThe Nuremberg Code
The degree of risk to be taken should never exceed that determined by the humanitarian importance of the problem to be solved by the experiment.
Proper preparations should be made and adequate facilities provided to protect the experimental subject against even remote possibilities of injury, disability, or death.
The Nuremberg CodeThe Nuremberg Code
The experiment should be conducted only by scientifically qualified persons.
During the course of the experiment the human subject should be at liberty to bring the experiment to an end (Intention to Treat Precepts)
The Nuremberg CodeThe Nuremberg Code
During the course of the experiment the scientist in charge must be prepared to terminate the experiment at any stage, if he/she has probable cause to believe, in the exercise of good faith, superior skill, and careful judgment that the continuation of the experiment is likely to cause injury, disability or death (Stopping Rules)