Embed Size (px)
Citation preview

EstablishmentandclinicalapplicationoftheRapidInterventionScreeningTestforAutismin
Toddlers(RITA-T)Roula Choueiri, MD
NeurodevelopmentalDisabilitiesPediatricianAssociateProfessorofPediatrics
Chief,DivisionofDevelopmentalandBehavioralPediatricsCDCActearlyCampaignAmbassadortoMAUniversityofMassachusettsMedicalSchool
NewTwoLevelScreeningModel

CurrentScreeningMethodsforASD• Level1oruniversalscreensuchastheMCHAT-R:
• Verygoodatpickingupchildrenwhoneedmoreworkup• HighfalsepositiveforASD
• Level2– Disorder-specificscreener• DifferentiatesbetweenASDandotherdelays
• ReferralsforASDevaluationsmoreappropriate
vInteractiveLevel2ASDscreenerspreferredtoquestionnaires
èTriggersatypicalbehaviors

Two-LevelASDScreeningModel
RiskASD+++
RiskforDevelopmentalDelays/ASD
WellChildVisitsorhighrisk(ex:EarlyIntervention)
Level1
Level2

IdealASDLevel2screenerThismodelwouldallowimprovedaccess
ToddlerswithhighriskofASDwouldnotbedelayedfordiagnosticconfirmation
EarlyIntervention,EarlyChildhoodeducators,Pediatricians,nurses,NP,canbetrainedonit
Reliablein18-36monthsold
Easytotrainandlearn
DiscriminateswellbetweentoddlerswithASDandthosewithDelaysthatarenonASD
Andmostimportantly:FITSWELLINTOBUSYPRACTICEFLOW

CurrentInteractiveLevel2ASDscreenersSTAT:ScreeningforAutismin
Toddlers• 20minutestoadminister• Difficulttraining• Goodpsychometricsfor2-3y
old• Lessgoodfor<2y• Missesmildtomoderate
formsofASD• HighCosts
RITA-T:RapidInteractiveScreeningTestforAutisminToddlers
• 5-10minutestoadminister• Reliabletrainingin3hours• Goodpsychometricsfor18-39
months• Trainingandaccesstobe
accessible

DESCRIPTIONoftheRITA-T@UMassMed

DescriptionoftheRITA-T(JournalofPediatrics,August2015)
• 9interactivepresses• Assessesdevelopmental
constructsdelayedinearlyASDsuchas:• JointAttention(JA)• ReactiontoEmotions• AwarenessofHumanAgency
• Eachitemcodedfrom0to2,3or4(typicaltoatypical)
• Totalscoregenerated;maximum:30
• Thelower thescore,themoretypicalthereaction
vAdministrationandscoringtime:10minutes

RITA-T- Description
• Scoringalgorithm,Manualandtrainingdevelopedandtested.
• Resultsofvalidationstudies
• CorrelatesverywellwithAutismDiagnostictests

EyeContactandJA
“Checking in” to share interest/surprise to a magical change in colors or to disappearing ball

HumanAgency&preferenceforfaces
Child aware of person blocking object not just “the hand”
Preference for faces
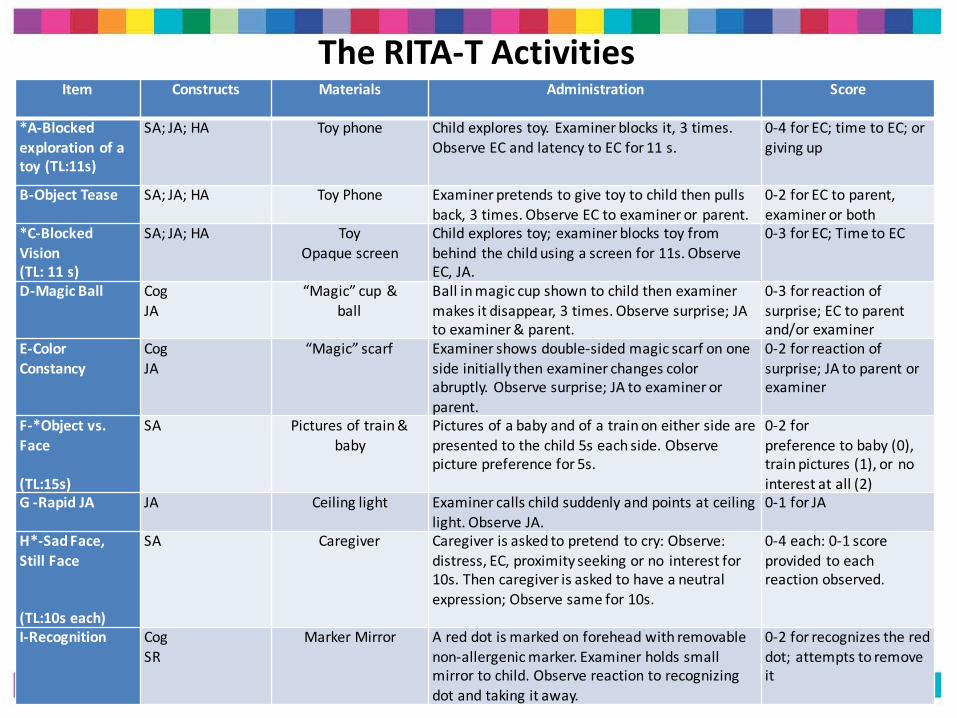
TheRITA-TActivitiesItem Constructs Materials Administration Score
*A-Blockedexplorationofatoy(TL:11s)
SA;JA;HA Toyphone Childexplorestoy.Examinerblocksit,3times.ObserveECandlatencytoECfor11s.
0-4 forEC;timetoEC;orgivingup
B-ObjectTease SA;JA;HA ToyPhone Examinerpretendstogivetoytochildthenpullsback,3times.ObserveECtoexaminerorparent.
0-2forECtoparent,examinerorboth
*C-BlockedVision(TL:11s)
SA;JA;HA ToyOpaquescreen
Childexplorestoy;examinerblockstoyfrombehind thechildusingascreenfor11s.ObserveEC,JA.
0-3forEC;TimetoEC
D-MagicBall CogJA
“Magic”cup&ball
Ballinmagiccupshowntochildthenexaminermakesitdisappear,3times.Observesurprise;JAtoexaminer&parent.
0-3forreactionofsurprise;ECtoparentand/orexaminer
E-ColorConstancy
CogJA
“Magic”scarf Examinershowsdouble-sidedmagicscarfononesideinitiallythenexaminerchangescolorabruptly.Observesurprise;JAtoexaminerorparent.
0-2forreactionofsurprise;JAtoparentorexaminer
F-*Objectvs.Face
(TL:15s)
SA Picturesoftrain&baby
Picturesofababyandofatrainoneithersidearepresentedtothechild5seachside.Observepicturepreferencefor5s.
0-2forpreferencetobaby(0),trainpictures(1),ornointerestatall(2)
G-RapidJA JA Ceilinglight Examinercallschildsuddenlyandpointsatceilinglight.ObserveJA.
0-1forJA
H*-SadFace,StillFace
(TL:10seach)
SA Caregiver Caregiverisaskedtopretend tocry:Observe:distress,EC,proximityseekingorno interestfor10s.Thencaregiverisaskedtohaveaneutralexpression;Observesamefor10s.
0-4each:0-1scoreprovided toeachreactionobserved.
I-Recognition CogSR
MarkerMirror Areddotismarkedonforeheadwithremovablenon-allergenicmarker.Examinerholdssmallmirrortochild.Observereactiontorecognizingdotandtakingitaway.
0-2forrecognizesthereddot;attemptstoremoveit
RITA-TScoringSheet

InitialvalidationSample(JofPediatrics,2015)
• 74 toddlerswereenrolled• 13 wereexcluded
»61 continuedthestudy
• 23 hadASD
• 19hadDD(DevelopmentalDelay)/Non-ASDdiagnoses
• LanguageDelay(LD)in12• GlobalDevelopmentalDelay(GDD)in7
• 19 were“TD”(NCR:NoConcernsRaised)

Results- Demographics
ASD(N=23)
NonASD(N=19)
NCR(N=19)
P-value
FemaleN(%) 1(4) 8(36) 12(63) <0.001AgemonthsMean(SD)
27.77(5.7) 29.46(6) 21.7(6.5) 0.001
RaceN(%) 0.07WhiteN(%) 11(47.8) 15(79) 8(42.1)
Hispanic 8(34.7) 3(15.8) 4(21)Other 4(17.3) 1(5.2) 7(36.8)
IncomeN(%) NS>$50,000 7(30.4) 8(42.1) 6(31.5)<$50,000 16(69.5) 11(58) 13(68.4)
P-valuesforgroupdifferencesarebasedonANOVAforcontinuousvariablesandchi-squaretestsforcategoricalvariables.

Results- MeanScores(SD)byDiagnoses
ASD DD/NON-ASD NCR P-VALUERITA-T 20.8(3.6) 13(2.5) 10.9(2.12) <0.0001M-CHAT
TotalItemsfailed(SD) 8.7(4.9) 4(3.6) 1.3(1.6) <0.0001M-CHAT
Meancriticalfailed(SD) 2.87(2.3) 1.42(1.6) 0.11(0.31) <0.0001DSMIV 8.96(1.99) 0.89(1.15) N/A <0.0001DSM5 6.04(0.88) 0.75(1.15) N/A <0.0001
MULLENReceptiveLanguage 29.7(12.3) 33.8(15.2) N/A NS
MULLENExpressiveLanguage 28.4(13.2) 29.6(13.4) N/A NS
MULLENVisual Reception 32.8(10.7) 40(14.65) N/A NS

Results- CorrelationsofRITA-TwithAutismmeasures
CorrelationsDSMIVcriteria
checkedDSM5criteria
checkedADOS
CompositeScore
r= 0.78 0.76 0.79
N= 42 42 25
t= 7.81 7.37 6.14
p=(two-tailed) <0.0001 <0.0001 <0.0001
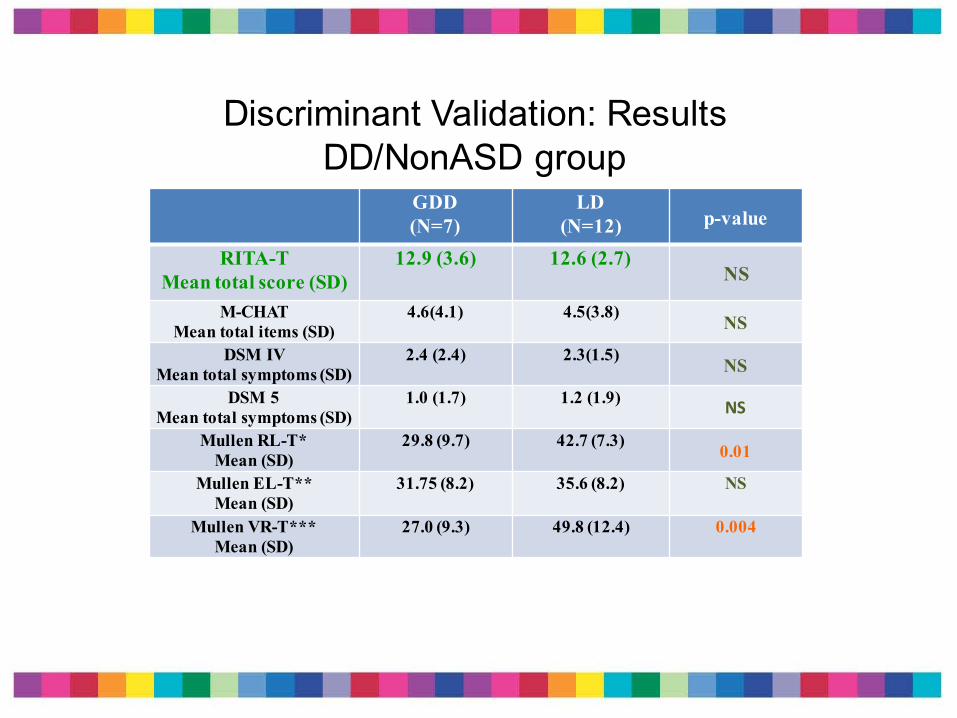
Discriminant Validation: Results DD/NonASD group
GDD(N=7)
LD(N=12) p-value
RITA-TMean total score (SD)
12.9 (3.6) 12.6 (2.7)NS
M-CHAT Mean total items (SD)
4.6(4.1) 4.5(3.8) NS
DSM IVMean total symptoms (SD)
2.4 (2.4) 2.3(1.5) NS
DSM 5 Mean total symptoms (SD)
1.0 (1.7) 1.2 (1.9) NS
Mullen RL-T*Mean (SD)
29.8 (9.7) 42.7 (7.3) 0.01
Mullen EL-T**Mean (SD)
31.75 (8.2) 35.6 (8.2) NS
Mullen VR-T***Mean (SD)
27.0 (9.3) 49.8 (12.4) 0.004

DISCRIMINANT VALIDATION: RESULTS
•RITA-T & MCHAT total score: Positive Correlation
– Spearman Rho: 0.65; p < 0.001
•RITA-T mean total score BY ADOS classification (t-test)
MeanRITA-TScorep<0.01
ADOS(Autism) ADOS(ASD)22(SD:3.3) 16.25(SD:3.8)

Measures of test validity
•Sensitivity:– Positivesaretruepositives
•Specificity:• Negativesaretrulynegatives
•PPV:PositivePredictiveValue– Proportionofpatientswithpositivetestresultswhoarecorrectlydiagnosed
•NPV:NegativePredictiveValue– Proportionofpatientswithnegativetestresultswhoarecorrectlyexcluded

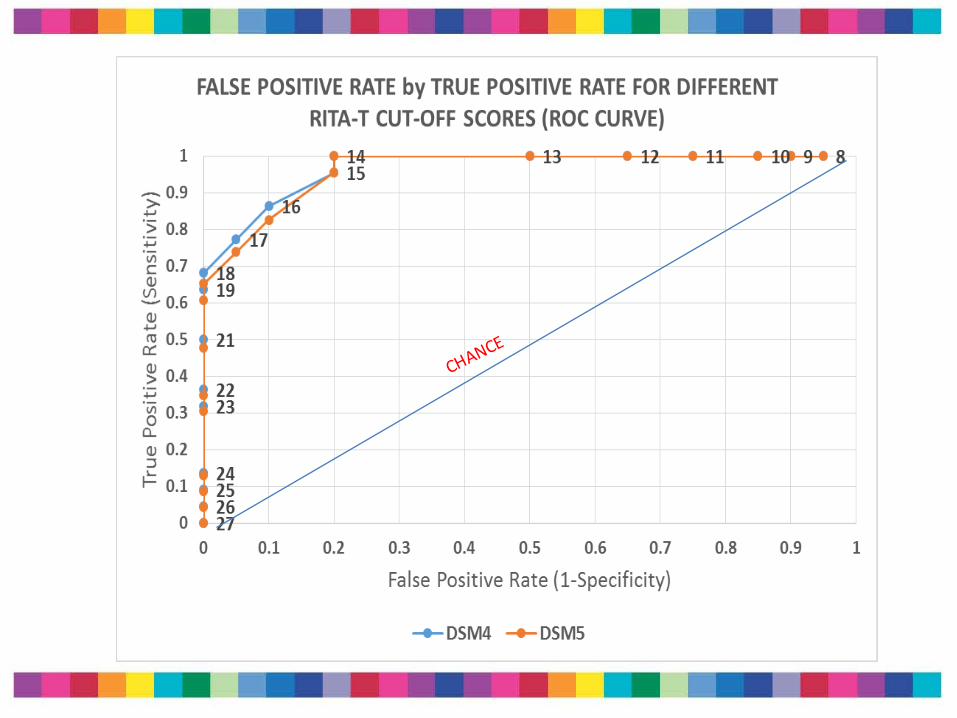
RITA-TTotalscore Sensitivity Specificity PPV NPV
8 1 0.05 0.56 19 1 0.11 0.58 110 1 0.16 0.59 111 1 0.26 0.62 112 1 0.37 0.66 113 1 0.53 0.72 114 1 0.84 0.88 115 0.96 0.84 0.88 0.9416 0.83 0.89 0.90 0.8117 0.74 0.95 0.94 0.7518 0.65 1 1 0.7019 0.61 1 1 0.6821 0.48 1 1 0.6122 0.35 1 1 0.5623 0.30 1 1 0.5424 0.13 1 1 0.4925 0.09 1 1 0.4826 0.04 1 1 0.4627 0 1 1 0.45
Sensitivity&Specificityforallcut-offscores
SUMMARY– CorrelateswellwiththeADOS– Reliability inadministrationandscoringiseasilyobtained– Differentiateswellbetween“TD”&toddlerswithASD– Discriminatessensitivelyandspecificallybetween
toddlerswithDD/NonASD&toddlerswithASDatcutoffscoreof14
– At5-10minutes,itfitsverywell intoclinicflow
ØTheRITA-Tisareliable,valid,Level2interactiveASDscreeningtestfortoddlers
18-36months

OtherValidationStudiesGeneralization&Newmodels

• DivisionofDevelopmentalandBehavioralPediatrics:teamtrainedontheRITA-T(JeanFrancoisLemay,MDFRCPC;twospeechtherapists,andapsychologist)
• Goal:Reducepatientwait-listtimefortoddlers18- 39monthsreferredfordiagnosticevaluationsforpossibleASD
• October,2013:waittobeevaluatedfora0-3ywas12months
• NewmodelandtriagewithRITA-T:– Parentmeeting– MCHAT&RITA-Tadministrationthentriagetospecifictestinggroup(Lowrisk,moderateriskandhighrisk)withdiagnosticevaluations,
treatmentandfollowupprovided.
a- CalgaryAlbertaChildren’sHospitalReplicationStudy-Results

ResultsofNewTriageProtocolContinuesafterstudycompletion
DATE WAITTIMETODIAGNOSTICVISIT
OCT,2013 12-13MONTHS
MAY,2014 6MONTHS
SEPT,2014 2MONTHS
JAN,2016 28days


• This quality improvement (QI) project incorporated evidence-based practice with process improvement methodology.
• The model included: – a) an initial mandatory parent education session followed one week later by – b) a child visit using the face-to-face level II screening tool (RITA-T) + completion
of M-CHAT questionnaire by parents followed in 7-21 days by – c) an ASD diagnostic evaluation appointment (type dependent on score obtained
in screening appointment) and finally the opportunity to attend in the next 2-3 weeks
– d) an “After the ASD Diagnosis” parent group session with a positive diagnosis of ASD.
TriageGroupsBasedonRITA–TScore
LowRisk: score<under12
MediumRisk: scoreisbetween12-16
HighRisk: score>above16

Results• A total of 173 patients were assessed (81% male; mean age 30.74
months +/- 5.53 months, interval 15.4-39.0). Of those 143 children (82.7%) were diagnosed with ASD
• The diagnostic process was completed within a max 30-day cycle (previously >4 months with high variation) and required less hours/child (12 vs 20 hours – overall 40% net gain)
• Waitlist was reduced to <1 month by August 2014 compared to >12 months in October 2013
• The discriminative properties of RITA-T at a cut off score of 12 were calculated: Sensitivity 0.99; Specificity 0.67; Positive Predictive Value 0.91; Negative Predictive Value 0.94.

RESULTS:
ASD NON-ASD
N=133 N=20
MEAN S.D MEAN S.Dp-
VALUE
RITA-TTOTAL 22.3 4.3 10.9 2.9 <.0001
#OFDSM-5CRITERIAHITS 6.2 1.4 3.2 4 <.0001
M-CHATTOTAL 8.81 4.88 3.7 3.83 <.0001
AGE 29.5 4 30.1 5 0.56

CORRELATIONS(CALGARY)
• RITA-TIsuncorrelatedwithageacrossallagegroups
• ModeratelycorrelatedwithM-CHAThits(r=.53)
• ModeratelycorrelatedwithtotalDSM-5criteriaendorsedbyclinician(r=.6)
• WithfemalesRITA-ThighercorrelationwithDSM-5hits(r=.8)

RITA-TSCORESbyDx(0%False-Negatives,2.6%False-Positives)

SummaryCalgaryProject
•Our ASD diagnostic approach of toddlers [12-39 months], a blend of quality improvement and evidence-based practice, has led to innovation in developing an efficient ASD diagnostic assessment process
•Reduced the wait times from 12+ months to 1 month and decreased capacity hours by 40%
•The RITA-T was very useful in the overall process and showed very good discriminative properties comparable to previous results
•This sustainable diagnostic approach promoted practice innovation
•Patients are now able to access critical community supports and resources in a timely manner.
b- OngoingStudiesatUMassinWorcester(DevelopmentalandBehavioralPediatrics- DBP)
a- EarlyInterventionReplicationStudy
TheTHOMEarlyInterventionprograminWorcester:- EIprovidersalltrainedontheMCHAT-R/F- FourEIprovidersfromAutismteamtrainedreliablyontheRITA-T
- Pediatricclinicsinformedaboutstudy.MCHATR/Fcompletedbypediatricians.
- AlltoddlersenrolledinEIprogramreceiveMCHAT-R/F- ThosewithconcernsonMCHATR/ForconcernsclinicallyareadministeredtheRITA-T
- TheyarethenreferredtodiagnosticteaminDBPatUMassinWorcester
36

-DBPUMassWorcesterDiagnosticTeamandTesting
DiagnosticevaluationteamatUMass(phase1)andinEI(Phase2):- TheAutismDiagnosticObservationSchedule(ADOS)-2- TheMullenScalesofEarlyLearning
- Diagnosesdiscussedwithfamilies
- StudyapprovedbyIRB
- Followupprovided

RESULTS• Pilot:BetweenFebruary2016andJune2016:(otherongoingJanuary2017-December2017- noresultsyet)
– 68toddlersenrolled:NonASDin13;ASDin55– Waittime:within4weeks
• Females:15andMales:53• Averageage:29.91months(19-36months)• Ethnicity:
– White:29– Hispanic:15– Other:12– Multiple:3– NA:9
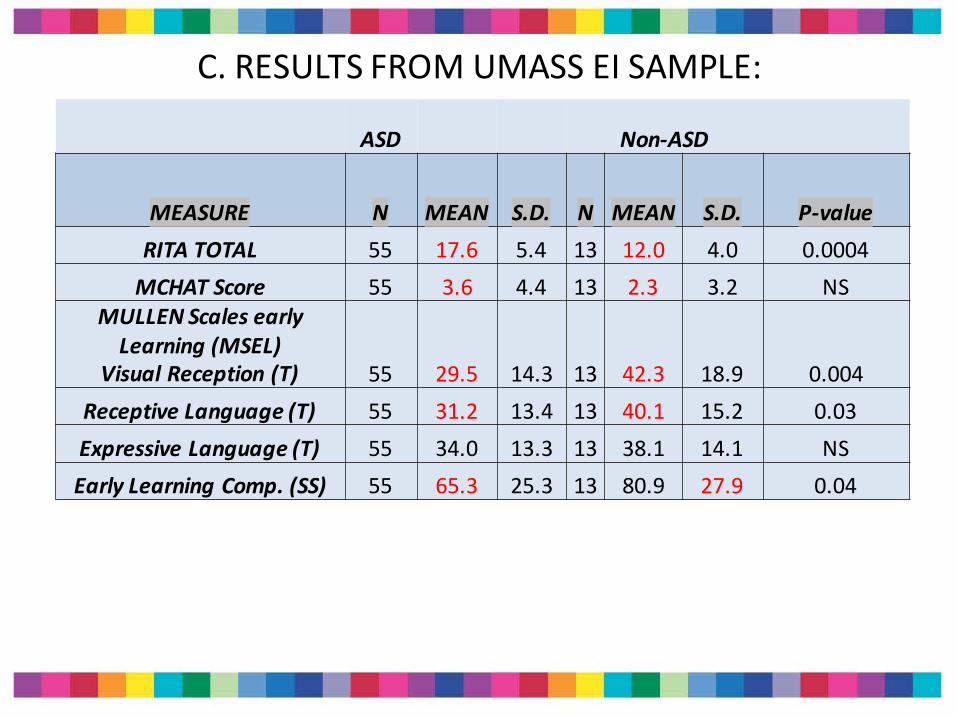
C.RESULTSFROMUMASSEISAMPLE:
ASD Non-ASD
MEASURE N MEAN S.D. N MEAN S.D. P-valueRITATOTAL 55 17.6 5.4 13 12.0 4.0 0.0004MCHATScore 55 3.6 4.4 13 2.3 3.2 NS
MULLENScales earlyLearning(MSEL)
VisualReception(T) 55 29.5 14.3 13 42.3 18.9 0.004ReceptiveLanguage(T) 55 31.2 13.4 13 40.1 15.2 0.03ExpressiveLanguage(T) 55 34.0 13.3 13 38.1 14.1 NSEarlyLearningComp.(SS) 55 65.3 25.3 13 80.9 27.9 0.04

EICORRELATIONS
ASD NON-ASD
WITHASDRITATOTAL CORRELATION WITHNON-ASDRITATOTAL CORRELATION
MCHATScore 0.34 MCHATScore 0.64
MULLEN VR(T) -0.31 MULLEN VR(T) 0.01
Receptive Language(T) -0.36 Receptive Language(T) -0.19
ExpressiveLanguage (T) -0.46 ExpressiveLanguage (T) 0.09
CognitiveTScoreSum -0.11 CognitiveTScoreSum -0.06
ELCompositeSS -0.28 ELCompositeSS -0.08
MullenPercentileRank -0.30 MullenPercentileRank -0.18
ADOSMod1TOTAL(SA+RRB) 0.63 ADOSMod1TOTAL(SA+RRB) 0.67
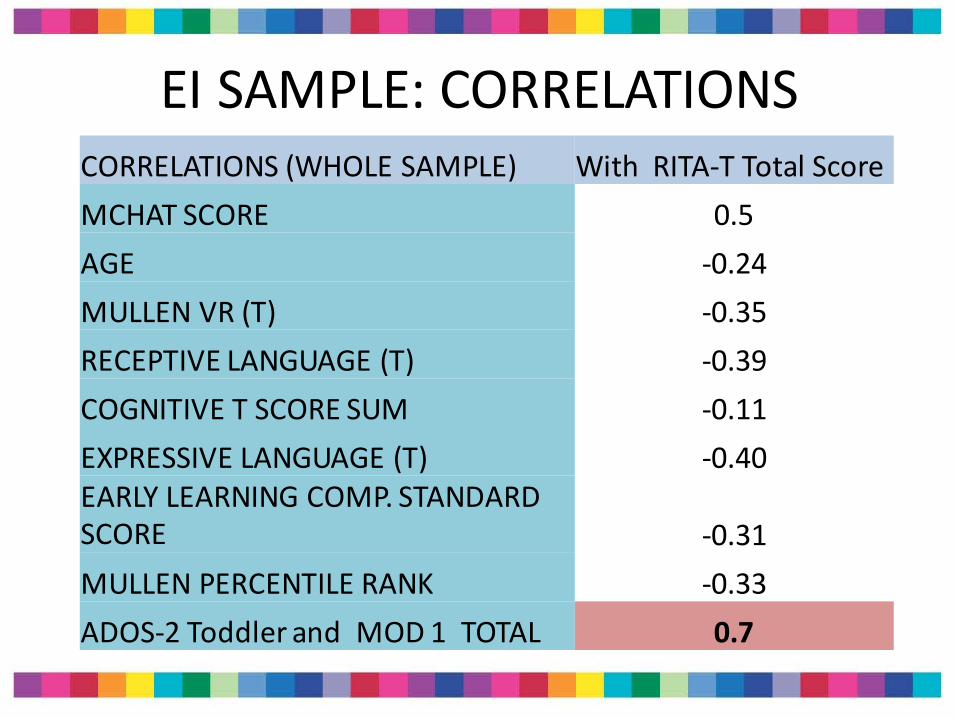
EISAMPLE:CORRELATIONSCORRELATIONS(WHOLESAMPLE) WithRITA-TTotalScoreMCHATSCORE 0.5AGE -0.24MULLENVR(T) -0.35RECEPTIVELANGUAGE(T) -0.39COGNITIVETSCORESUM -0.11EXPRESSIVELANGUAGE(T) -0.40EARLYLEARNINGCOMP.STANDARDSCORE -0.31MULLENPERCENTILERANK -0.33ADOS-2ToddlerandMOD1TOTAL 0.7
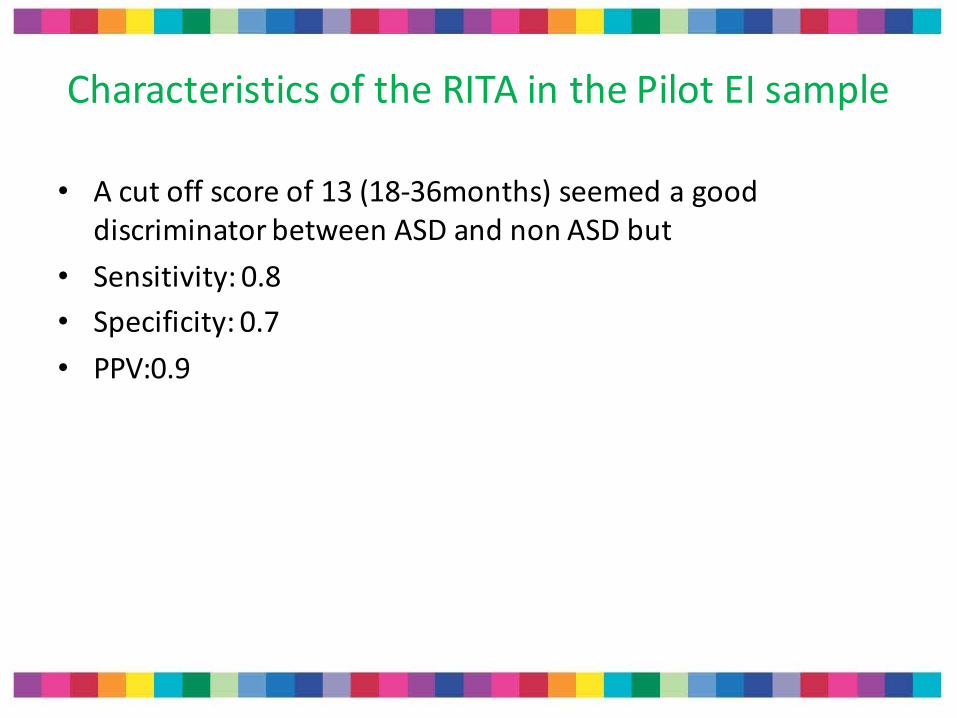
CharacteristicsoftheRITAinthePilotEIsample
• Acutoffscoreof13(18-36months)seemedagooddiscriminatorbetweenASDandnonASDbut
• Sensitivity:0.8• Specificity:0.7• PPV:0.9
b- FurtherEIreplicationandnewmodels
• PediatricpracticestobetrainedontheRITA-T
• OtherEIprograms
• Generalizetoothersettingsandothercultures

SUMMARY:TheRITA-T• CorrelateswellwithAutismdiagnosticmeasures
• Reliabletrainingiseasilyobtained
• DiscriminateswellbetweentoddlerswithDD/NonASD&ASDatcutoffscoreof12(greyarea12-14)
• At5-10minutes,itfitsverywell intoclinicflow
• TheRITA-TisareliableandreasonablyvalidLevel2interactiveASDscreeningtestfortoddlers
• Facilitatesearlierdetectionandtwo-levelscreeningmodels
Futuresteps• Validationpapers• ContinuingtocollectdatafromEIprojectandotherpractices• TwopediatricpracticeswilltrainontheRITA-Tand
establishingaclinicatUMassforfasttrackdiagnosis• PhysiciantrainerinChinaandstudyimplementationofRITA-T
inscreeninganddiagnosticclinicsin2areasinChina• Generalizeitsuseindifferentsettingsandculturesandby
differentproviders.• Forinformationorquestions:

Futuresteps:RITA-Thttp://www.umassmed.edu/AutismRITA-T/rita-t/

AcknowledgementsRITA-TResearchTeams
TuftsTeam:SheldonWagner,PhD;SusanParsons,MD;
KarenMiller,MD;NicolaSmith,MD;KathleenReilly,CCC-SLP;KrishnaBanerjee,MD;SherylLevy,MD;NaomiSteiner,MD;ChristinaSakai,MD;CarminaErdei,MD;SusanMangan,MS;EricStern,BS;LaurenBrodsky,MS;
Calgaryteam:• JeanFrancoisLemay,MDChinateam:JuneKong,MDUMassteam:• AsherLindenbaum,MS;RoksanaSasanfar,
MD;MargaretManning,PhD;RyanShafer,BS.
• THOMWorcesterEarlyInterventionprogram(JeanineMindrum;ChantalRoyer-Haig;KellyBrennan)
• ITdepartmentandCMEdepartment
Grants1- PlanningGrantTuftsClinical andTranslationalScienceInstitute(CTSI)20102- CVScharitabletrademark(Autismoutcomeresearchproject)3- TuftsSusanSaltonstallPilotGrant20124- UMassPediatricDepartmentSeedgrant5- UMassScholaraward6- WorcesterFairlawnFoundation
ALLTHEFAMILIES





























